Embed Size (px)
Citation preview

DepartOdense Unogy, AalbNuclear MEconomicsSouthernGentofte HHealth, UhDepartmeManuscripaccepted J
See pa*CorreE-mail
0002-9149http://dx.do
Comparison of Mortality in Patients With AcuteMyocardial Infarction Accidentally Admitted to
Non-cardiology Departments Versus That in PatientsAdmitted to Coronary Care Units
Maria D’Souza, BScmeda, Lotte Saaby, MDa, Tina S. Poulsen, MD, PhDa,Axel C.P. Diederichsen, MD, PhDa, Susanne Hosbond, MDa, Søren Z. Diederichsen, BScmeda,
Torben B. Larsen, MD, PhDb, Henrik Schmidt, MD, DMScc, Oke Gerke, MSc, PhDd,Jesper Hallas, MD, DMSce, Gunnar Gislason, MD, PhDf,g, Kristian Thygesen, MD, DMSch,
and Hans Mickley, MD, DMSca,*
The aim of this study was to prospectively investigate the clinical characteristics including
ments oiversityorg UnedicineResearDenmaospitalniversitynt of Cat receivuly 16,ge 1156spondinaddres
/14/$ -i.org/1
symptoms and long-term mortality in patients with acute myocardial infarction (AMI)accidentally admitted to non-cardiology departments (NCDs). For comparison, similarobservations in patients admitted to the coronary care unit (CCU) were collected. During a1-year period, consecutive patients having cardiac troponin I measured at the OdenseUniversity Hospital were considered. The hospital has 27 clinical departments. Patients wereclassified as having an AMI if the diagnostic criteria of the universal definition were met.Follow-up was at least 1 year with mortality as the clinical end point. Of 3,762 consecutivepatients, an AMI was diagnosed in 479, of whom 114 patients (24%) were hospitalized inNCDs and 365 (76%) in the CCU. Chest pain or chest discomfort more frequently occurredin patients from the CCU (83%) than in patients from the NCDs (45%, p <0.0001). Atmedian follow-up of 2.1 years, 150 patients had died: 73 (64%) of patients from the NCDsand 77 (21%) of the patients from the CCU. In the multivariable Cox regression analysis, theadjusted hazard ratio of mortality for patients from the NCDs versus CCU was 2.0 (95%confidence interval 1.3 to 3.2). In conclusion, chest pain/discomfort was absent in more thanhalf of the patients with AMI admitted to NCDs, and admission to NCDs was an inde-pendent predictor of a 2 times higher long-term mortality in comparison with admission tothe CCU. � 2014 Elsevier Inc. All rights reserved. (Am J Cardiol 2014;114:1151e1157)
It occurs that patients with acute myocardial infarction(AMI) accidentally are referred to non-cardiology de-partments (NCDs)—even at hospitals with highly special-ized cardiology services available. Potential causes for thismay be low suspicion of AMI because of not only atypicalsymptoms and/or discrete electrocardiographic changes1 butalso triaging through low-volume emergency departments.2
Moreover, severe co-morbidity at hospitalization mayoverrule the diagnosis of AMI when deciding on theappropriate triage.1,3 The clinical characteristics and
f aCardiology and cAnesthesiology and Intensive Care,Hospital, Odense, Denmark; bDepartment of Cardiol-
iversity Hospital, Aalborg, Denmark; dDepartment of, Odense University Hospital and Center of Healthch, eDepartment of Clinical Pharmacology, University ofrk, Odense, Denmark; fDepartment of Cardiology,, Hellerup, Denmark; gThe National Institute of Publicof Southern Denmark, Copenhagen, Denmark; and
rdiology, Aarhus University Hospital, Aarhus, Denmark.ed April 23, 2014; revised manuscript received and2014.for disclosure information.g author: Tel: (þ452) 857-1431; fax: (þ456) 311-0497.s: [email protected] (H. Mickley).
see front matter � 2014 Elsevier Inc. All rights reserved.0.1016/j.amjcard.2014.07.035
prognosis of patients with AMI treated by non-cardiologistshave been investigated in a number of retrospective,observational multicenter studies, and inconsistent conclu-sions have been reached.1,4e9 To the best of our knowledge,only 1 prospective study has been published so far, but onlyselected patients with ST-elevation AMI were addressed.10
The objectives of this prospective study were to investi-gate the clinical characteristics and long-term mortality inpatients with AMI, who were admitted to NCDs in a largeuniversity hospital. For comparison, similar observations inpatients admitted directly to the coronary care unit (CCU)were collected.
Methods
This is a substudy of the DEF-AMI study (“Consequencesof the universal Definition of Acute Myocardial Infarctionstudied prospectively in a Danish consecutive hospital pop-ulation”).11,12 Odense University Hospital has 1,000 bedsand serves not only as a tertiary referral center for a region of1.2 million inhabitants but also as the local hospital for acatchment area of 300,000 residents. The hospital has 27clinical departments including a CCU with an intensive caresection and round-the-clock facilities for primary percuta-neous coronary intervention (PCI). During the inclusion
www.ajconline.org
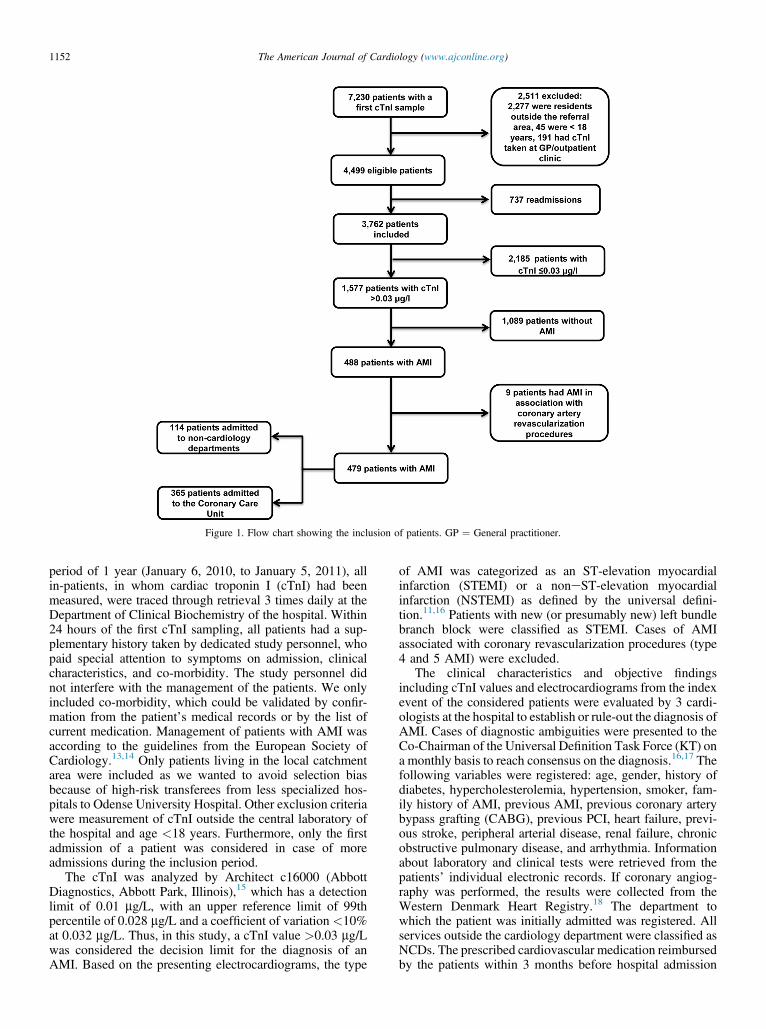
Figure 1. Flow chart showing the inclusion of patients. GP ¼ General practitioner.
1152 The American Journal of Cardiology (www.ajconline.org)
period of 1 year (January 6, 2010, to January 5, 2011), allin-patients, in whom cardiac troponin I (cTnI) had beenmeasured, were traced through retrieval 3 times daily at theDepartment of Clinical Biochemistry of the hospital. Within24 hours of the first cTnI sampling, all patients had a sup-plementary history taken by dedicated study personnel, whopaid special attention to symptoms on admission, clinicalcharacteristics, and co-morbidity. The study personnel didnot interfere with the management of the patients. We onlyincluded co-morbidity, which could be validated by confir-mation from the patient’s medical records or by the list ofcurrent medication. Management of patients with AMI wasaccording to the guidelines from the European Society ofCardiology.13,14 Only patients living in the local catchmentarea were included as we wanted to avoid selection biasbecause of high-risk transferees from less specialized hos-pitals to Odense University Hospital. Other exclusion criteriawere measurement of cTnI outside the central laboratory ofthe hospital and age <18 years. Furthermore, only the firstadmission of a patient was considered in case of moreadmissions during the inclusion period.
The cTnI was analyzed by Architect c16000 (AbbottDiagnostics, Abbott Park, Illinois),15 which has a detectionlimit of 0.01 mg/L, with an upper reference limit of 99thpercentile of 0.028 mg/L and a coefficient of variation <10%at 0.032 mg/L. Thus, in this study, a cTnI value >0.03 mg/Lwas considered the decision limit for the diagnosis of anAMI. Based on the presenting electrocardiograms, the type
of AMI was categorized as an ST-elevation myocardialinfarction (STEMI) or a noneST-elevation myocardialinfarction (NSTEMI) as defined by the universal defini-tion.11,16 Patients with new (or presumably new) left bundlebranch block were classified as STEMI. Cases of AMIassociated with coronary revascularization procedures (type4 and 5 AMI) were excluded.
The clinical characteristics and objective findingsincluding cTnI values and electrocardiograms from the indexevent of the considered patients were evaluated by 3 cardi-ologists at the hospital to establish or rule-out the diagnosis ofAMI. Cases of diagnostic ambiguities were presented to theCo-Chairman of the Universal Definition Task Force (KT) ona monthly basis to reach consensus on the diagnosis.16,17 Thefollowing variables were registered: age, gender, history ofdiabetes, hypercholesterolemia, hypertension, smoker, fam-ily history of AMI, previous AMI, previous coronary arterybypass grafting (CABG), previous PCI, heart failure, previ-ous stroke, peripheral arterial disease, renal failure, chronicobstructive pulmonary disease, and arrhythmia. Informationabout laboratory and clinical tests were retrieved from thepatients’ individual electronic records. If coronary angiog-raphy was performed, the results were collected from theWestern Denmark Heart Registry.18 The department towhich the patient was initially admitted was registered. Allservices outside the cardiology department were classified asNCDs. The prescribed cardiovascular medication reimbursedby the patients within 3 months before hospital admission
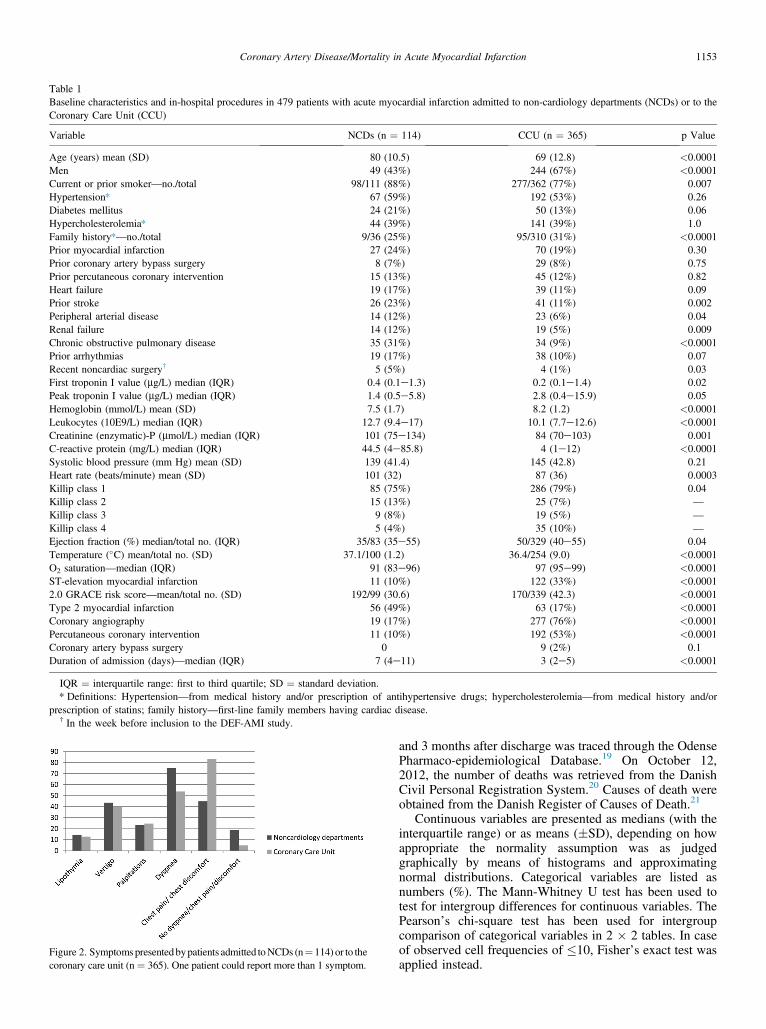
Table 1Baseline characteristics and in-hospital procedures in 479 patients with acute myocardial infarction admitted to non-cardiology departments (NCDs) or to theCoronary Care Unit (CCU)
Variable NCDs (n ¼ 114) CCU (n ¼ 365) p Value
Age (years) mean (SD) 80 (10.5) 69 (12.8) <0.0001Men 49 (43%) 244 (67%) <0.0001Current or prior smoker—no./total 98/111 (88%) 277/362 (77%) 0.007Hypertension* 67 (59%) 192 (53%) 0.26Diabetes mellitus 24 (21%) 50 (13%) 0.06Hypercholesterolemia* 44 (39%) 141 (39%) 1.0Family history*—no./total 9/36 (25%) 95/310 (31%) <0.0001Prior myocardial infarction 27 (24%) 70 (19%) 0.30Prior coronary artery bypass surgery 8 (7%) 29 (8%) 0.75Prior percutaneous coronary intervention 15 (13%) 45 (12%) 0.82Heart failure 19 (17%) 39 (11%) 0.09Prior stroke 26 (23%) 41 (11%) 0.002Peripheral arterial disease 14 (12%) 23 (6%) 0.04Renal failure 14 (12%) 19 (5%) 0.009Chronic obstructive pulmonary disease 35 (31%) 34 (9%) <0.0001Prior arrhythmias 19 (17%) 38 (10%) 0.07Recent noncardiac surgery† 5 (5%) 4 (1%) 0.03First troponin I value (mg/L) median (IQR) 0.4 (0.1e1.3) 0.2 (0.1e1.4) 0.02Peak troponin I value (mg/L) median (IQR) 1.4 (0.5e5.8) 2.8 (0.4e15.9) 0.05Hemoglobin (mmol/L) mean (SD) 7.5 (1.7) 8.2 (1.2) <0.0001Leukocytes (10E9/L) median (IQR) 12.7 (9.4e17) 10.1 (7.7e12.6) <0.0001Creatinine (enzymatic)-P (mmol/L) median (IQR) 101 (75e134) 84 (70e103) 0.001C-reactive protein (mg/L) median (IQR) 44.5 (4e85.8) 4 (1e12) <0.0001Systolic blood pressure (mm Hg) mean (SD) 139 (41.4) 145 (42.8) 0.21Heart rate (beats/minute) mean (SD) 101 (32) 87 (36) 0.0003Killip class 1 85 (75%) 286 (79%) 0.04Killip class 2 15 (13%) 25 (7%) —
Killip class 3 9 (8%) 19 (5%) —
Killip class 4 5 (4%) 35 (10%) —
Ejection fraction (%) median/total no. (IQR) 35/83 (35e55) 50/329 (40e55) 0.04Temperature (�C) mean/total no. (SD) 37.1/100 (1.2) 36.4/254 (9.0) <0.0001O2 saturation—median (IQR) 91 (83e96) 97 (95e99) <0.0001ST-elevation myocardial infarction 11 (10%) 122 (33%) <0.00012.0 GRACE risk score—mean/total no. (SD) 192/99 (30.6) 170/339 (42.3) <0.0001Type 2 myocardial infarction 56 (49%) 63 (17%) <0.0001Coronary angiography 19 (17%) 277 (76%) <0.0001Percutaneous coronary intervention 11 (10%) 192 (53%) <0.0001Coronary artery bypass surgery 0 9 (2%) 0.1Duration of admission (days)—median (IQR) 7 (4e11) 3 (2e5) <0.0001
IQR ¼ interquartile range: first to third quartile; SD ¼ standard deviation.* Definitions: Hypertension—from medical history and/or prescription of antihypertensive drugs; hypercholesterolemia—from medical history and/or
prescription of statins; family history—first-line family members having cardiac disease.† In the week before inclusion to the DEF-AMI study.
Figure 2. Symptomspresentedbypatients admitted toNCDs (n¼ 114) or to thecoronary care unit (n¼ 365). One patient could report more than 1 symptom.
Coronary Artery Disease/Mortality in Acute Myocardial Infarction 1153
and 3 months after discharge was traced through the OdensePharmaco-epidemiological Database.19 On October 12,2012, the number of deaths was retrieved from the DanishCivil Personal Registration System.20 Causes of death wereobtained from the Danish Register of Causes of Death.21
Continuous variables are presented as medians (with theinterquartile range) or as means (�SD), depending on howappropriate the normality assumption was as judgedgraphically by means of histograms and approximatingnormal distributions. Categorical variables are listed asnumbers (%). The Mann-Whitney U test has been used totest for intergroup differences for continuous variables. ThePearson’s chi-square test has been used for intergroupcomparison of categorical variables in 2 � 2 tables. In caseof observed cell frequencies of �10, Fisher’s exact test wasapplied instead.
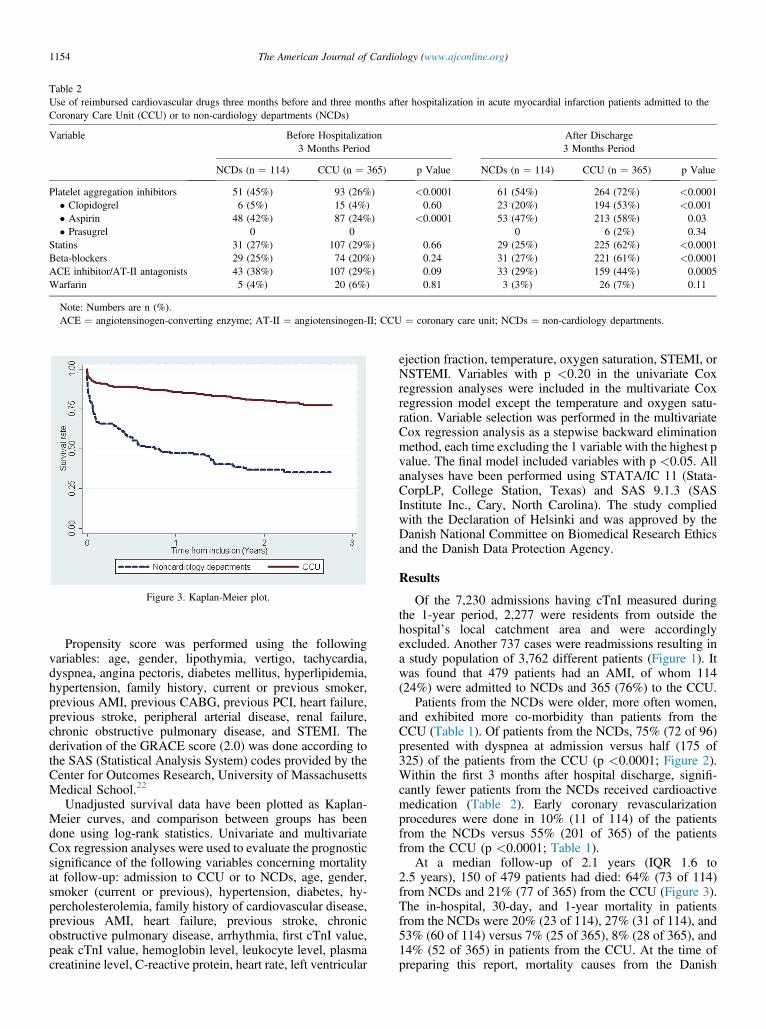
Table 2Use of reimbursed cardiovascular drugs three months before and three months after hospitalization in acute myocardial infarction patients admitted to theCoronary Care Unit (CCU) or to non-cardiology departments (NCDs)
Variable Before Hospitalization3 Months Period
After Discharge3 Months Period
NCDs (n ¼ 114) CCU (n ¼ 365) p Value NCDs (n ¼ 114) CCU (n ¼ 365) p Value
Platelet aggregation inhibitors 51 (45%) 93 (26%) <0.0001 61 (54%) 264 (72%) <0.0001� Clopidogrel 6 (5%) 15 (4%) 0.60 23 (20%) 194 (53%) <0.001� Aspirin 48 (42%) 87 (24%) <0.0001 53 (47%) 213 (58%) 0.03� Prasugrel 0 0 0 6 (2%) 0.34
Statins 31 (27%) 107 (29%) 0.66 29 (25%) 225 (62%) <0.0001Beta-blockers 29 (25%) 74 (20%) 0.24 31 (27%) 221 (61%) <0.0001ACE inhibitor/AT-II antagonists 43 (38%) 107 (29%) 0.09 33 (29%) 159 (44%) 0.0005Warfarin 5 (4%) 20 (6%) 0.81 3 (3%) 26 (7%) 0.11
Note: Numbers are n (%).ACE ¼ angiotensinogen-converting enzyme; AT-II ¼ angiotensinogen-II; CCU ¼ coronary care unit; NCDs ¼ non-cardiology departments.
Figure 3. Kaplan-Meier plot.
1154 The American Journal of Cardiology (www.ajconline.org)
Propensity score was performed using the followingvariables: age, gender, lipothymia, vertigo, tachycardia,dyspnea, angina pectoris, diabetes mellitus, hyperlipidemia,hypertension, family history, current or previous smoker,previous AMI, previous CABG, previous PCI, heart failure,previous stroke, peripheral arterial disease, renal failure,chronic obstructive pulmonary disease, and STEMI. Thederivation of the GRACE score (2.0) was done according tothe SAS (Statistical Analysis System) codes provided by theCenter for Outcomes Research, University of MassachusettsMedical School.22
Unadjusted survival data have been plotted as Kaplan-Meier curves, and comparison between groups has beendone using log-rank statistics. Univariate and multivariateCox regression analyses were used to evaluate the prognosticsignificance of the following variables concerning mortalityat follow-up: admission to CCU or to NCDs, age, gender,smoker (current or previous), hypertension, diabetes, hy-percholesterolemia, family history of cardiovascular disease,previous AMI, heart failure, previous stroke, chronicobstructive pulmonary disease, arrhythmia, first cTnI value,peak cTnI value, hemoglobin level, leukocyte level, plasmacreatinine level, C-reactive protein, heart rate, left ventricular
ejection fraction, temperature, oxygen saturation, STEMI, orNSTEMI. Variables with p <0.20 in the univariate Coxregression analyses were included in the multivariate Coxregression model except the temperature and oxygen satu-ration. Variable selection was performed in the multivariateCox regression analysis as a stepwise backward eliminationmethod, each time excluding the 1 variable with the highest pvalue. The final model included variables with p <0.05. Allanalyses have been performed using STATA/IC 11 (Stata-CorpLP, College Station, Texas) and SAS 9.1.3 (SASInstitute Inc., Cary, North Carolina). The study compliedwith the Declaration of Helsinki and was approved by theDanish National Committee on Biomedical Research Ethicsand the Danish Data Protection Agency.
Results
Of the 7,230 admissions having cTnI measured duringthe 1-year period, 2,277 were residents from outside thehospital’s local catchment area and were accordinglyexcluded. Another 737 cases were readmissions resulting ina study population of 3,762 different patients (Figure 1). Itwas found that 479 patients had an AMI, of whom 114(24%) were admitted to NCDs and 365 (76%) to the CCU.
Patients from the NCDs were older, more often women,and exhibited more co-morbidity than patients from theCCU (Table 1). Of patients from the NCDs, 75% (72 of 96)presented with dyspnea at admission versus half (175 of325) of the patients from the CCU (p <0.0001; Figure 2).Within the first 3 months after hospital discharge, signifi-cantly fewer patients from the NCDs received cardioactivemedication (Table 2). Early coronary revascularizationprocedures were done in 10% (11 of 114) of the patientsfrom the NCDs versus 55% (201 of 365) of the patientsfrom the CCU (p <0.0001; Table 1).
At a median follow-up of 2.1 years (IQR 1.6 to2.5 years), 150 of 479 patients had died: 64% (73 of 114)from NCDs and 21% (77 of 365) from the CCU (Figure 3).The in-hospital, 30-day, and 1-year mortality in patientsfrom the NCDs were 20% (23 of 114), 27% (31 of 114), and53% (60 of 114) versus 7% (25 of 365), 8% (28 of 365), and14% (52 of 365) in patients from the CCU. At the time ofpreparing this report, mortality causes from the Danish
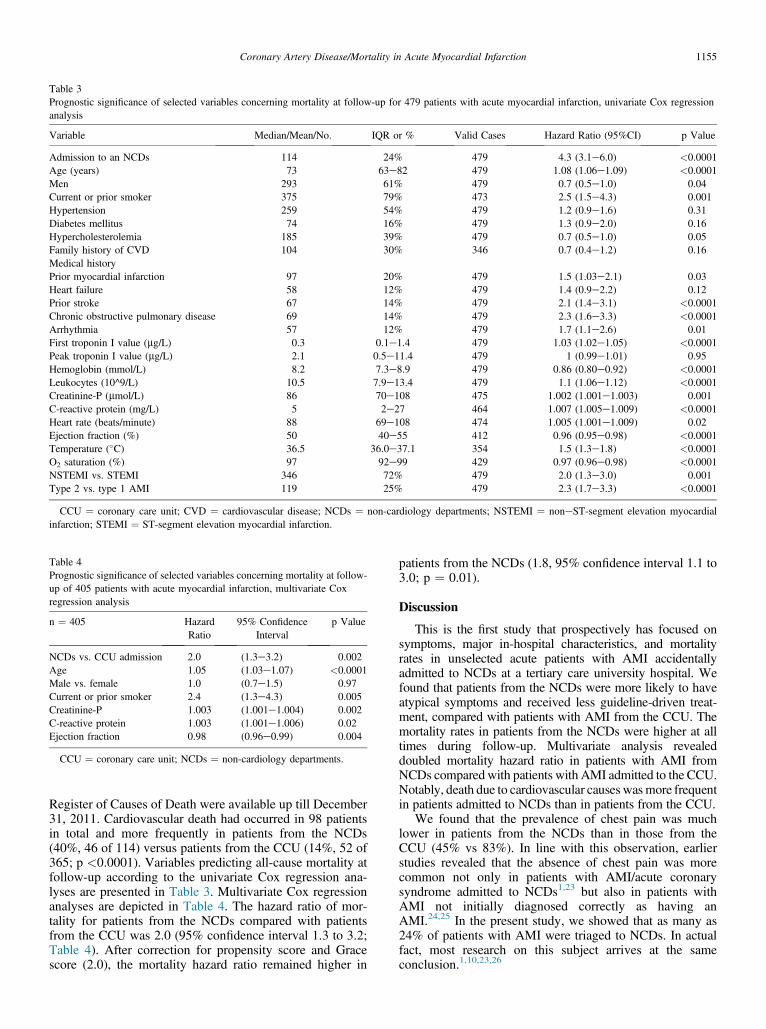
Table 3Prognostic significance of selected variables concerning mortality at follow-up for 479 patients with acute myocardial infarction, univariate Cox regressionanalysis
Variable Median/Mean/No. IQR or % Valid Cases Hazard Ratio (95%CI) p Value
Admission to an NCDs 114 24% 479 4.3 (3.1e6.0) <0.0001Age (years) 73 63e82 479 1.08 (1.06e1.09) <0.0001Men 293 61% 479 0.7 (0.5e1.0) 0.04Current or prior smoker 375 79% 473 2.5 (1.5e4.3) 0.001Hypertension 259 54% 479 1.2 (0.9e1.6) 0.31Diabetes mellitus 74 16% 479 1.3 (0.9e2.0) 0.16Hypercholesterolemia 185 39% 479 0.7 (0.5e1.0) 0.05Family history of CVD 104 30% 346 0.7 (0.4e1.2) 0.16Medical historyPrior myocardial infarction 97 20% 479 1.5 (1.03e2.1) 0.03Heart failure 58 12% 479 1.4 (0.9e2.2) 0.12Prior stroke 67 14% 479 2.1 (1.4e3.1) <0.0001Chronic obstructive pulmonary disease 69 14% 479 2.3 (1.6e3.3) <0.0001Arrhythmia 57 12% 479 1.7 (1.1e2.6) 0.01First troponin I value (mg/L) 0.3 0.1e1.4 479 1.03 (1.02e1.05) <0.0001Peak troponin I value (mg/L) 2.1 0.5e11.4 479 1 (0.99e1.01) 0.95Hemoglobin (mmol/L) 8.2 7.3e8.9 479 0.86 (0.80e0.92) <0.0001Leukocytes (10^9/L) 10.5 7.9e13.4 479 1.1 (1.06e1.12) <0.0001Creatinine-P (mmol/L) 86 70e108 475 1.002 (1.001e1.003) 0.001C-reactive protein (mg/L) 5 2e27 464 1.007 (1.005e1.009) <0.0001Heart rate (beats/minute) 88 69e108 474 1.005 (1.001e1.009) 0.02Ejection fraction (%) 50 40e55 412 0.96 (0.95e0.98) <0.0001Temperature (�C) 36.5 36.0e37.1 354 1.5 (1.3e1.8) <0.0001O2 saturation (%) 97 92e99 429 0.97 (0.96e0.98) <0.0001NSTEMI vs. STEMI 346 72% 479 2.0 (1.3e3.0) 0.001Type 2 vs. type 1 AMI 119 25% 479 2.3 (1.7e3.3) <0.0001
CCU ¼ coronary care unit; CVD ¼ cardiovascular disease; NCDs ¼ non-cardiology departments; NSTEMI ¼ noneST-segment elevation myocardialinfarction; STEMI ¼ ST-segment elevation myocardial infarction.
Table 4Prognostic significance of selected variables concerning mortality at follow-up of 405 patients with acute myocardial infarction, multivariate Coxregression analysis
n ¼ 405 HazardRatio
95% ConfidenceInterval
p Value
NCDs vs. CCU admission 2.0 (1.3e3.2) 0.002Age 1.05 (1.03e1.07) <0.0001Male vs. female 1.0 (0.7e1.5) 0.97Current or prior smoker 2.4 (1.3e4.3) 0.005Creatinine-P 1.003 (1.001e1.004) 0.002C-reactive protein 1.003 (1.001e1.006) 0.02Ejection fraction 0.98 (0.96e0.99) 0.004
CCU ¼ coronary care unit; NCDs ¼ non-cardiology departments.
Coronary Artery Disease/Mortality in Acute Myocardial Infarction 1155
Register of Causes of Death were available up till December31, 2011. Cardiovascular death had occurred in 98 patientsin total and more frequently in patients from the NCDs(40%, 46 of 114) versus patients from the CCU (14%, 52 of365; p <0.0001). Variables predicting all-cause mortality atfollow-up according to the univariate Cox regression ana-lyses are presented in Table 3. Multivariate Cox regressionanalyses are depicted in Table 4. The hazard ratio of mor-tality for patients from the NCDs compared with patientsfrom the CCU was 2.0 (95% confidence interval 1.3 to 3.2;Table 4). After correction for propensity score and Gracescore (2.0), the mortality hazard ratio remained higher in
patients from the NCDs (1.8, 95% confidence interval 1.1 to3.0; p ¼ 0.01).
Discussion
This is the first study that prospectively has focused onsymptoms, major in-hospital characteristics, and mortalityrates in unselected acute patients with AMI accidentallyadmitted to NCDs at a tertiary care university hospital. Wefound that patients from the NCDs were more likely to haveatypical symptoms and received less guideline-driven treat-ment, compared with patients with AMI from the CCU. Themortality rates in patients from the NCDs were higher at alltimes during follow-up. Multivariate analysis revealeddoubled mortality hazard ratio in patients with AMI fromNCDs compared with patients with AMI admitted to the CCU.Notably, death due to cardiovascular causeswasmore frequentin patients admitted to NCDs than in patients from the CCU.
We found that the prevalence of chest pain was muchlower in patients from the NCDs than in those from theCCU (45% vs 83%). In line with this observation, earlierstudies revealed that the absence of chest pain was morecommon not only in patients with AMI/acute coronarysyndrome admitted to NCDs1,23 but also in patients withAMI not initially diagnosed correctly as having anAMI.24,25 In the present study, we showed that as many as24% of patients with AMI were triaged to NCDs. In actualfact, most research on this subject arrives at the sameconclusion.1,10,23,26

1156 The American Journal of Cardiology (www.ajconline.org)
Our study demonstrated a higher mean age and preva-lence of other major risk factors and co-morbidities in pa-tients from the NCDs. NSTEMI was the most frequent AMItype in patients from the NCDs and was significantly moreprevalent than in patients from the CCU. These findings arein accordance with previous research.5,6,26 It appeared thatpatients from the NCDs had a higher initial cTnI value,which may be a consequence of the atypical symptomsfound in patients from the NCDs implying a delay introponin blood sampling compared with patients from theCCU. In contrast, patients from the NCDs had lower peakcTnI concentrations, also reported in 1 earlier study of pa-tients with STEMI,10 indicating that this proxy for AMI sizeis not useful in predicting the prognosis in these patients.The longer hospital stay observed in patients from the NCDsmost likely reflects more co-morbidity and more complexhospitalizations.
In our study, the patients from the NCDs, compared withpatients from the CCU, were less often managed accordingto the contemporary guidelines.13,14 This observation is inaccordance with the results from most earlier studies1,5e8
although occasional studies have reported no significantdifference.4,10 However, the populations in the latter studieswere heavily selective toward younger age or patients withSTEMI only. Additionally, the higher age and prevalence ofco-morbidity in patients from the NCDs in our study mayhave led to more obstacles to guideline-recommendedtreatment.27,28 The larger proportion of patients with type2 AMI in the NCDs may partly explain the observed lowerpostdischarge use of contemporary guideline-recommendedmedication compared with patients in the CCU. It should beborne in mind that no specific guidelines for the treatment oftype 2 AMI are available. Clinical research involving pa-tients with type 2 AMI is urgently needed to help determinewhat, if any, specific treatment is needed.29 Anotherimportant piece of information from our study is theobservation that significantly fewer patients from the NCDshad diagnostic procedures like echocardiography and coro-nary angiography performed. This imbalance has beenobserved in other studies as well.1,5e8,10
We found an increased short- and long-term mortality inpatients with AMI from NCDs compared with patients fromthe CCU. In 1 prospective10 and a few retrospective1,6,8,9
studies, a similar negative prognostic effect of admission toNCDs have previously been demonstrated. Moreover, theseearlier studies found that the observed association wasstrongly attenuated when adjusted for baseline characteristicsof the patients and/or the hospitals. In only 2 earlier studies,the adjustment for baseline characteristics eliminated theassociation between mortality and the type of department.4,7
In the present study, the mortality rate in patients from theNCDs was higher at any time through the follow-up periodcompared with patients admitted to the CCU (Figure 3).Based on our data, it appears that the group of patientsadmitted to NCDs with an AMI is rather complex andcharacterized by a large burden of risk factors, mixedinfarction types, and a high frequency of extra-cardiac mor-bidities, suggesting the need for a broad-spectrum of treat-ments in addition to the specific cardiac care. The prognosisin these patients might be improved by an intensified coop-eration between cardiology and non-cardiology services.
The present study has a number of limitations. First, thisis an everyday hospital study explaining why completecardiac examinations were not performed in all patients.Thus, diagnostic procedures and supplementary bloodsampling were done at the discretion of the treating physi-cians. Second, our observations reflect the management ofpatients with suspected or definite acute AMI in a largertertiary care university hospital, which may not mirror thetreatment elsewhere in the world. One of the strengths of ourstudy is the thorough case ascertainment. All patients wereevaluated by both a 3-member local diagnosis committeeand 1 external expert. Additionally, all mortality data wereobtained from a national registration system linked to aunique civil registration number (records on all Danish cit-izens, living and diseased).20 Moreover, we had informationon dispensed medication 3 months before and 3 months afterdischarge, which account for a quite precise registration ofthe medication actually taken by the patients and appears tobe superior to information on medication on discharge.
Disclosures
The authors have no conflicts of interest to disclose.
1. Herlitz J, Dellborg M, Karlsson T, Evander MH, Berger A, Luepker R.Epidemiology of acute myocardial infarction with the emphasis onpatients who did not reach the coronary care unit and non-AMIadmissions. Int J Cardiol 2008;128:342e349.
2. Schull MJ, Vermeulen MJ, Stukel TA. The risk of missed diagnosis ofacute myocardial infarction associated with emergency departmentvolume. Ann Emerg Med 2006;48:647e655.
3. Arbelle JE, Porath A, Cohen E, Gilutz H, Garty M. Triage dispositionof patients with acute myocardial infarction—ACSIS 2000. Isr MedAssoc J 2003;5:786e790.
4. Amit G, Goldman S, Ore L, Low M, Kark JD. The association betweenhospital department, medical treatment and outcome in acute myocar-dial infarction. Isr Med Assoc J 2003;5:255e259.
5. Birkhead JS, Weston C, Lowe D. Impact of specialty of admittingphysician and type of hospital on care and outcome for myocardialinfarction in England and Wales during 2004e5: observational study.BMJ 2006;332:1306e1311.
6. Chen J, Radford MJ, Wang Y, Krumholz HM. Care and outcomes ofelderly patients with acute myocardial infarction by physician specialty:the effects of comorbidity and functional limitations. Am J Med2000;108:460e469.
7. Frances CD, Go AS, Dauterman KW, Deosaransingh K, Jung DL,Gettner S, Newman JM, Massie BM, Browner WS. Outcome followingacute myocardial infarction: are differences among physician spe-cialties the result of quality of care or case mix? Arch Intern Med1999;159:1429e1436.
8. Jollis JG, DeLong ER, Peterson ED, Muhlbaier LH, Fortin DF, CaliffRM, Mark DB. Outcome of acute myocardial infarction according tothe specialty of the admitting physician. N Engl J Med 1996;335:1880e1887.
9. Alcalai R, Planer D, Culhaoglu A, Osman A, Pollak A, Lotan C.Acute coronary syndrome vs nonspecific troponin elevation: clinicalpredictors and survival analysis. Arch Intern Med 2007;167:276e281.
10. Bang A, Grip L, Herlitz J, Kihlgren S, Karlsson T, Caidahl K, HartfordM. Lower mortality after prehospital recognition and treatmentfollowed by fast tracking to coronary care compared with admittancevia emergency department in patients with ST-elevation myocardialinfarction. Int J Cardiol 2008;129:325e332.
11. Saaby L, Poulsen TS, Hosbond S, Larsen TB, Pyndt Diederichsen AC,Hallas J, Thygesen K, Mickley H. Classification of myocardialinfarction: frequency and features of type 2 myocardial infarction. Am JMed 2013;126:789e797.
12. Saaby L, Poulsen TS, Pyndt Diederichsen AC, Hosbond S, Larsen TB,Schmidt H, Gerke O, Hallas J, Thygesen K, Mickley H. Mortality rate
Coronary Artery Disease/Mortality in Acute Myocardial Infarction 1157
in type 2 myocardial infarction: observations from an unselectedhospital cohort. Am J Med 2014;127:295e302.
13. Van de Werf F, Bax J, Betriu A, Blomstrom-Lundqvist C, Crea F, FalkV, Filippatos G, Fox K, Huber K, Kastrati A, Rosengren A, Steg PG,Tubaro M, Verheugt F, Weidinger F, Weis M. Management of acutemyocardial infarction in patients presenting with persistent ST-segmentelevation: the Task Force on the Management of ST-Segment ElevationAcute Myocardial Infarction of the European Society of Cardiology.Eur Heart J 2008;29:2909e2945.
14. Bassand JP, Hamm CW, Ardissino D, Boersma E, Budaj A,Fernandez-Aviles F, Fox KA, Hasdai D, Ohman EM, Wallentin L,Wijns W. Guidelines for the diagnosis and treatment of non-ST-segment elevation acute coronary syndromes. Eur Heart J2007;28:1598e1660.
15. Lam Q, Black M, Youdell O, Spilsbury H, Schneider HG. Performanceevaluation and subsequent clinical experience with the AbbottAutomated Architect STAT Troponin-I assay. Clin Chem 2006;52:298e300.
16. Thygesen K, Alpert JS,White HD, Jaffe AS, Apple FS, GalvaniM, KatusHA, Newby LK, Ravkilde J, Chaitman B, Clemmensen PM, Dellborg M,Hod H, Porela P, Underwood R, Bax JJ, Beller GA, Bonow R, Van derWall EE, Bassand JP, Wijns W, Ferguson TB, Steg PG, Uretsky BF,WilliamsDO,Armstrong PW,Antman EM, FoxKA,HammCW,OhmanEM, Simoons ML, Poole-Wilson PA, Gurfinkel EP, Lopez-Sendon JL,Pais P, Mendis S, Zhu JR, Wallentin LC, Fernandez-Aviles F, Fox KM,Parkhomenko AN, Priori SG, Tendera M, Voipio-Pulkki LM, VahanianA, CammAJ, De CR,Dean V, Dickstein K, Filippatos G, Funck-BrentanoC, Hellemans I, Kristensen SD, McGregor K, Sechtem U, Silber S,TenderaM,Widimsky P, Zamorano JL,Morais J, Brener S, Harrington R,Morrow D, Lim M, Martinez-Rios MA, Steinhubl S, Levine GN, GiblerWB, Goff D, Tubaro M, Dudek D, Al-Attar N. Universal definition ofmyocardial infarction. Circulation 2007;116:2634e2653.
17. Thygesen K, Mair J, Katus H, Plebani M, Venge P, Collinson P,Lindahl B, Giannitsis E, Hasin Y, Galvani M, Tubaro M, Alpert JS,Biasucci LM, Koenig W, Mueller C, Huber K, Hamm C, Jaffe AS.Recommendations for the use of cardiac troponin measurement in acutecardiac care. Eur Heart J 2010;31:2197e2204.
18. Schmidt M, Maeng M, Jakobsen CJ, Madsen M, Thuesen L, NielsenPH, Botker HE, Sorensen HT. Existing data sources for clinicalepidemiology: the western Denmark heart registry. Clin Epidemiol2010;2:137e144.
19. Gaist D, Sorensen HT, Hallas J. The Danish prescription registries.Dan Med Bull 1997;44:445e448.
20. Pedersen CB. The danish civil registration system. Scand J PublicHealth 2011;39:22e25.
21. Helweg-Larsen K. The danish register of causes of death. Scand JPublic Health 2011;39:26e29.
22. Granger CB, Goldberg RJ, Dabbous O, Pieper KS, Eagle KA, CannonCP, Van de Werf F, Avezum A, Goodman SG, Flather MD, Fox KA.Predictors of hospital mortality in the global registry of acute coronaryevents. Arch Intern Med 2003;163:2345e2353.
23. Katz DA, Aufderheide TP, Bogner M, Rahko PS, Hillis SL, Selker HP.Do emergency department patients with possible acute coronarysyndrome have better outcomes when admitted to cardiology versusother services? Ann Emerg Med 2008;51:561e570.
24. Herlitz J, Karlson BW, Karlsson T, Svensson L, och Bjorn Kalin EZ.A description of the characteristics and outcome of patients hospital-ized for acute chest pain in relation to whether they were admitted tothe coronary care unit or not in the thrombolytic era. Int J Cardiol2002;82:279e287.
25. Canto JG, Shlipak MG, Rogers WJ, Malmgren JA, Frederick PD,Lambrew CT, Ornato JP, Barron HV, Kiefe CI. Prevalence, clinicalcharacteristics, and mortality among patients with myocardialinfarction presenting without chest pain. JAMA 2000;283:3223e3229.
26. Roe MT, Chen AY, Mehta RH, Li Y, Brindis RG, Smith SC Jr,Rumsfeld JS, Gibler WB, Ohman EM, Peterson ED. Influence ofinpatient service specialty on care processes and outcomes for patientswith non ST-segment elevation acute coronary syndromes. Circulation2007;116:1153e1161.
27. Krumholz HM, Radford MJ, Wang Y, Chen J, Heiat A, Marciniak TA.National use and effectiveness of beta-blockers for the treatment ofelderly patients after acute myocardial infarction: national CooperativeCardiovascular Project. JAMA 1998;280:623e629.
28. Dziewierz A, Siudak Z, Rakowski T, Zdzienicka J, Dykla D, MieleckiW, Dubiel JS, Dudek D. In-hospital management and mortality inelderly patients with non-ST-segment elevation acute coronarysyndromes treated in centers without on-site invasive facilities. CardiolJ 2008;15:451e457.
29. Alpert JS, Thygesen KA, White HD, Jaffe AS. Diagnostic andtherapeutic implications of type 2 myocardial infarction: review andcommentary. Am J Med 2014;127:105e108.





























