Embed Size (px)
Citation preview
COMPARISON OF MOTHER-FATHER PERCEPTIONS OF THEIR CHILD’S SELF-MANAGEMENT OF DIABETES
BARBARA J. LEONARD, PhD, Rh’ School of Nursing, University of Minnesota, Minneapolis, Minnesota, USA
BARBARA J. KRATZ, MS, CPNP Park Nicollet Clinic-HealthSystem Minnesota, Bloomington, Minnesota, USA
CAROL L. SKAY, PhD MARGUERITE M. RHEINBERGER, JD, MPH School of Nursing, University of Minnesota, Minneapolis, Minnesota, USA
This study compared mothers’ and fathers’ perceptions of their children’s self- management of diabetes. Participants included a subsample of 29 paired parents of children and youth with diabetes, ages 8-14, who attended a diabetes camp in the Midwest. Parents completed a self-report structured questionnaire that included content specific to self-management. Results showed high ratings for child responsibility for self-management, style of care delivery, and mother-father self-efficacy in managing specific tasks of diabetes self-management. Although overall ratings were similar, in the majority of measures mothers’ ratings were higher than fathers’ ratings. Areas of similarity and significant differences in perceptions are identified with implications for practice stated.
Diabetes mellitus is the most common metabolic disorder of childhood, affecting 1 in 500 individuals under age 20 (Giordano, Petrila, Banion, & Neuenkirchen, 1992). Most of the responsibility for care of youth with any chronic illness is initially placed on their parents. The transition to self-care is a progressive process that is ideally started in childhood, with adolescents assuming increased responsibility commensurate with their developmental capacities (Giordano et al., 1992).
Transferring responsibility for self-care to the adolescent is complex and requires assessment of the interplay of a variety of factors, including knowledge, performance, cognitive complexity, locus of control, family factors, and perceptions (Follansbee, 1989; Giordano et a]., 1992). The
Address correspondence to Barbara J. Leonard, University of Minnesota School of Nursing, 6-101 Weaver Densford Hall, 308 Harvard St. SE, Minneapolis, MN 55455.
Issues in Comprehensive Pediatric Nursing, 20:6e87, 1997 Copyright 0 1997 Tqlor & Francis
0146-0862/97 $12.00 -+ .OO 69
Issu
es C
ompr
Ped
iatr
Nur
s D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y SU
NY
Sta
te U
nive
rsity
of
New
Yor
k at
Sto
ny B
rook
on
10/2
7/14
For
pers
onal
use
onl
y.
70 B. J. Leonard et al.
family has been identified as the primary social context of a young person with a disability (Patterson, 1991). Families, specifically parents, play a critical role in the child’s self-care of a chronic illness (Deatrick, Angst, & Madden, 1994; Follansbee, 1989; Saucier & Clark, 1993). Family func- tioning will have either an enhancing or an undermining effect on the accomplishment of critical developmental tasks and transitions (Patterson, 1991).
Although the concept of self-care and the interchangeable concept of self-management have received increased attention in the literature in relation to youth with a chronic illness, less attention has been given to the roles of parents and families in relation to self-care with children and adolescents. A paucity of literature exists specific to each parent’s per- ceptions of self-care (Eiser, Havermans, Pancer, & Eiser, 1992).
There is support for exploring the difference in parental perceptions and the need to define the meaning any differences may have in rela- tionship to management of care for children with chronic illness or developmental disabilities (Beckman, 199 1 ; Copeland & Clements, 1993; Cummings, 1976; Eiser et al., 1992). Eiser et al. found differences in the way mothers and fathers perceived their children and their self-manage- ment of diabetes. In an analysis of paired data, fathers were found to perceive their children as more dependent and more likely to have diffi- culty with peers compared with mothers; however, there were no overall differences in parents’ ratings (Eiser et al., 1992).
Allen, Tennen, McGrade, Affleck, and Ratzan (1 983) found that par- ents’ perceptions of increased independence in various aspects of diet management were related to more successful coping by parents and their children and improved compliance.
Mothers’ and fathers’ perceptions of diabetes in adolescent daughters and its impact on the family were examined in a study by Dashiff (1993). Most parents felt unprepared for the periods of poor diabetic control encountered as their daughters entered adolescence. Parents described periods of emotional distress for themselves due to the metabolic insta- bility that commonly occurs during adolescence. Mothers reported more worry and intermittent feelings of guilt when contrasted with fathers (Dashiff, 1993).
The purpose of this study was to compare mothers’ and fathers’ per- ceptions of their children’s self-management of diabetes. Specific inquir- ies included mothers’ and fathers’ perceptions about the amount of responsibility their children assume for diabetes self-management, dimen- sions of care delivery style among their health care providers, their own level of self-efficacy in independent self-management of diabetes tasks, and the way tasks or situations specific to diabetes management are handled in the family. In addition, we examined factors influencing mothers
Issu
es C
ompr
Ped
iatr
Nur
s D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y SU
NY
Sta
te U
nive
rsity
of
New
Yor
k at
Sto
ny B
rook
on
10/2
7/14
For
pers
onal
use
onl
y.
Self-Management of Diabetes 71
and fathers in deciding how much responsibility their children should assume in diabetes self-management.
METHOD
The survey respondents for this study were a subsample of a larger study of 120 parents of children and youth aged 8-17 years who were attending two sessions of a diabetes camp in the Midwest. The subsample con- sisted of 29 matched sets of parents (mothers and fathers) of children and youth aged 8-14 years. Parents were recruited to complete surveys at the camp registration and product information fairs that were held the first day of each of two 1-week camp sessions. All available matched pairs of parents were included in this study. In all 29 cases, both mother and father lived with the child with diabetes.
The authors of the study developed all but one section of the survey, the Diabetes Family Responsibility Questionnaire (DFRQ; Anderson, Auslander, Jung, Miller, & Santiago, 1990). The 17 questions on the DFRQ make up three subscales: General Health Maintenance, Regimen Tasks, and Social Presentation of Diabetes, Anderson et al. found internal consistency, with alphas ranging from .69 for the shortest scale, Social Presentation of Diabetes, to .85 for the total DFRQ scale. Concurrent validity was found for the Regimen Task subscale and the total DFRQ when correlations were performed between the mothers’ scores on the DFRQ and the mothers’ scores on the Moos Family Environment Scale (FES; Moos, 1986; Anderson et al., 1990). For the sections other than the DFRQ, face and content validity were established by two parents of chil- dren with diabetes and three nurse practitioners reviewing and comment- ing on the questions. The instrument was rewritten incorporating their suggestions. Reliability was not established.
RESULTS
The analysis compared mothers’ and fathers’ perceptions of care regard- ing their children’s self-management of diabetes. These comparisons in- clude mothers’ and fathers’ perceptions as they related to (a) the amount of responsibility their children assumed for diabetes self-management compared with the average child with diabetes of the same age, (b) how certain factors influenced mothers and fathers in deciding how much responsibility their children should assume in diabetes self-management, (c) ratings of the children’s health care providers along specific dimen- sions of style of care delivery, (d) mothers’ and fathers’ ratings of their own self-efficacy in independently managing specific tasks related to self- management of diabetes, and (e) how tasks or situations related to dia- betes management were handled in the family.
Issu
es C
ompr
Ped
iatr
Nur
s D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y SU
NY
Sta
te U
nive
rsity
of
New
Yor
k at
Sto
ny B
rook
on
10/2
7/14
For
pers
onal
use
onl
y.
72 B. J. Leonard et al.
We used McNemar's chi-square for dependent proportions and paired t tests in the analysis. Both of these methods adjust for the dependence or correlation expected owing to mothers and fathers being paired subject units within a family.
Family Demographics
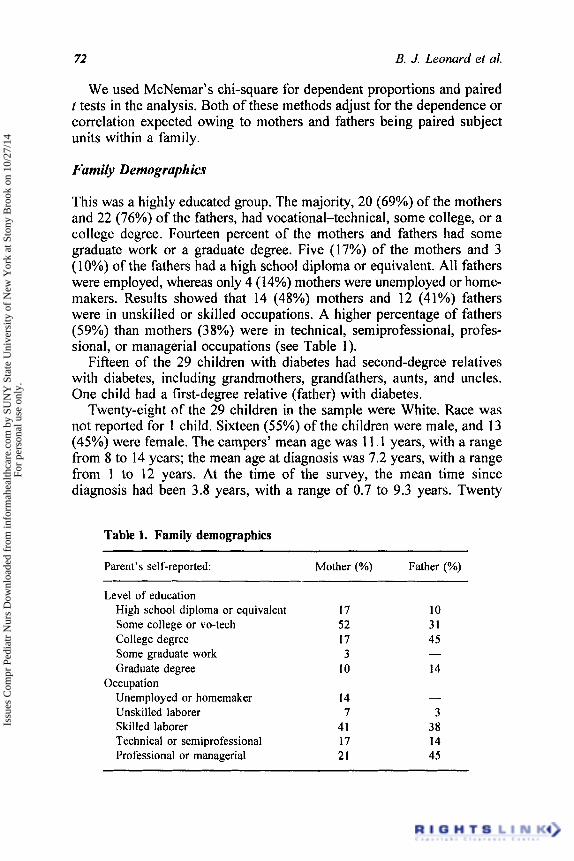
This was a highly educated group. The majority, 20 (69%) of the mothers and 22 (76%) of the fathers, had vocational-technical, some college, or a college degree. Fourteen percent of the mothers and fathers had some graduate work or a graduate degree. Five (1 7%) of the mothers and 3 (10%) of the fathers had a high school diploma or equivalent. All fathers were employed, whereas only 4 (14%) mothers were unemployed or home- makers. Results showed that 14 (48%) mothers and 12 (41%) fathers were in unskilled or skilled occupations. A higher percentage of fathers (59%) than mothers (3 8%) were in technical, semiprofessional, profes- sional, or managerial occupations (see Table 1 ) .
Fifteen of the 29 children with diabetes had second-degree relatives with diabetes, including grandmothers, grandfathers, aunts, and uncles. One child had a first-degree relative (father) with diabetes.
Twenty-eight of the 29 children in the sample were White. Race was not reported for 1 child. Sixteen (55%) of the children were male, and 13 (45%) were female. The campers' mean age was 11.1 years, with a range from 8 to 14 years; the mean age at diagnosis was 7.2 years, with a range from I to 12 years. At the time of the survey, the mean time since diagnosis had been 3.8 years, with a range of 0.7 to 9.3 years. Twenty
Table 1. Family demographics
Parent's self-reported: Mother (YO) Father (YO)
Level of education High school diploma or equivalent 17 10
College degree 17 45 Some graduate work 3
Some college or vo-tech 52 31
- Graduate degree 10 14
Unemployed or homemaker 14 Unskilled laborer 7 3 Skilled laborer 41 38 Technical or semiprofessional 17 14
Occupation -
Professional or managerial 21 45
Issu
es C
ompr
Ped
iatr
Nur
s D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y SU
NY
Sta
te U
nive
rsity
of
New
Yor
k at
Sto
ny B
rook
on
10/2
7/14
For
pers
onal
use
onl
y.
Self-Management of Diabetes 73
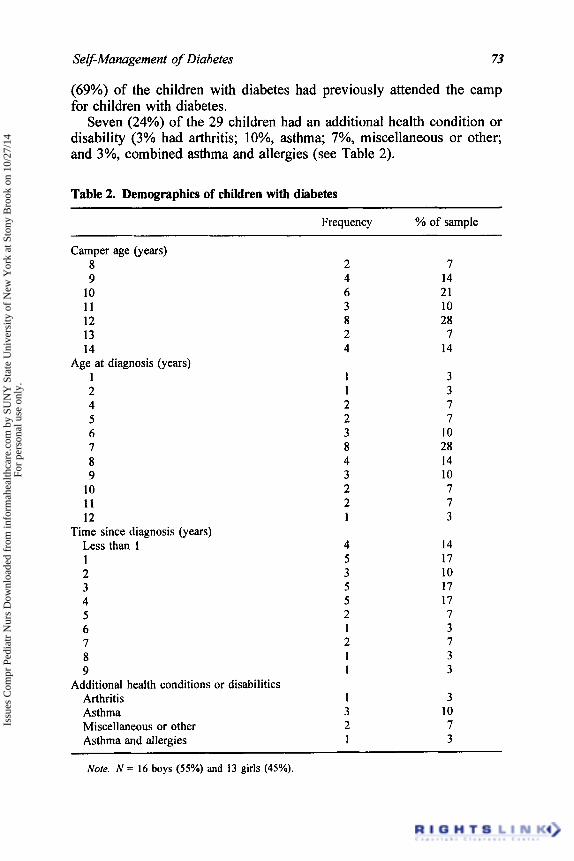
(69%) of the children with diabetes had previously attended the camp for children with diabetes.
Seven (24%) of the 29 children had an additional health condition or disability (3% had arthritis; lo%, asthma; 7%, miscellaneous or other; and 3%, combined asthma and allergies (see Table 2).
Table 2. Demographics of children with diabetes
Frequency YO of sample
Camper age (years) 8 9
10 11 12 13 14
1 2 4 5 6 7 8 9
10 11 12
Less than 1 1 2 3 4 5 6 7 8 9
Age at diagnosis (years)
Time since diagnosis (years)
2 4 6 3 8 2 4
I 1 2 2 3 8 4 3 2 2 1
4 5 3 5 5 2 1 2 1 I
Additional health conditions or disabilities Arthritis 1 Asthma 3 Miscellaneous or other 2 Asthma and allergies 1
7 14 21 10 28
7 14
3 3 7 7
10 28 14 10 7 7 3
14 17 10 17 17 7 3 7 3 3
3 10 7 3
Note. N = 16 boys (550/,) and 13 girls (45%).
Issu
es C
ompr
Ped
iatr
Nur
s D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y SU
NY
Sta
te U
nive
rsity
of
New
Yor
k at
Sto
ny B
rook
on
10/2
7/14
For
pers
onal
use
onl
y.
74 B. J. Leonard et al.
Responsibility for Diabetes Self-Management
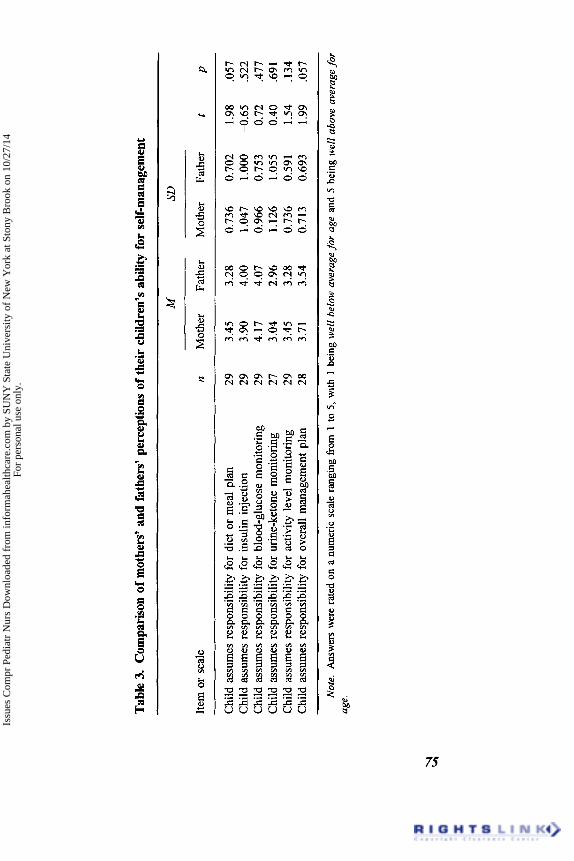
We computed means for both mothers’ and fathers’ perceptions of the amount of responsibility their children assume for diabetes self-manage- ment compared with the parents’ perception of what an average child with diabetes was like. The mothers’ perceptions (means) were slightly higher than the fathers’ in all areas except one. Fathers’ ratings were slightly higher in the area of responsibility for insulin injection. Mothers and fathers both perceived their children as being well above average for age in the areas of responsibility for insulin injection (mother mean = 3.90, father mean = 4.00, on a 5-point numeric scale) and responsibility for blood glucose monitoring (mother mean = 4.17, father mean = 4.07, on a 5-point scale). In only two of six areas, the child assumed responsi- bility for diet or meal plan and the child assumed responsibility for over- all management plan; p values of .057 showed close to significant results when comparing mother and father means (see Table 3).
Children ’s Responsibility in Diabetes Self-Management
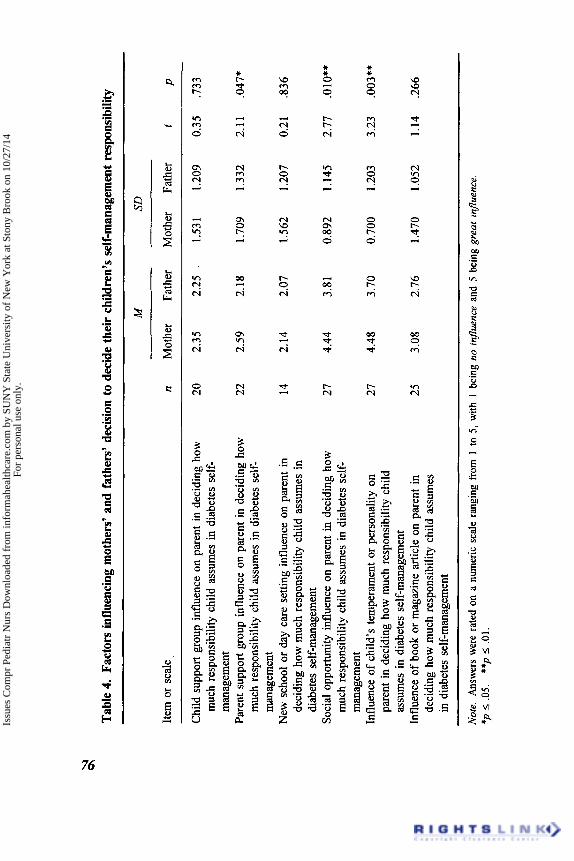
Parents were asked to rate how the following factors influenced them in deciding how much responsibility their children should assume in self- management: child support group, parent support group, new school or day care setting, social opportunity (meals, sleepovers, day trips), child’s temperament and personality, and book or magazine articles. Answers were rated on a 5-point numeric scale, with 1 being no influence and 5 being great influence. Mothers perceived social opportunities (mothers’ mean = 4.44, fathers’ mean = 3.81) and child’s temperament and person- ality (mothers’ mean = 4.48, fathers’ mean = 3.70) as having a strong influence (i.e., a mean greater than 4.0, with 5.0 being the highest). In all areas, mothers’ perceptions of the amount of influence of specific factors was slightly higher than fathers’. Differences between mothers and fathers were found for the following three factors: parent support group influence, 422) = 2.1 1, p = .047; social opportunity influence, t(27) = 2.77, p = 010; and child’s temperament or personality influence, t(27) 3.23, p = .003 (see Table 4).
Style of Care Delivery
Mothers and fathers rated their health care providers (those who assisted parents and children in managing diabetes) on 5-point numeric scales for four dimensions: (a) 1 being authoritarian and 5 being acknowledging family authority, (b) 1 being having a disease orientation and 5 being having a health orientation, (c) 1 being narrowly focused with an interest
Issu
es C
ompr
Ped
iatr
Nur
s D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y SU
NY
Sta
te U
nive
rsity
of
New
Yor
k at
Sto
ny B
rook
on
10/2
7/14
For
pers
onal
use
onl
y.
Tab
le 3
. C
ompa
riso
n of
mot
hers
’ and
fath
ers’
per
cept
ions
of th
eir
child
ren’
s ab
ility
for
self-
man
agem
ent
Item
or
scal
e
M
SD
n M
othe
r Fa
ther
M
othe
r Fa
ther
t
P
Chi
ld a
ssum
es r
espo
nsib
ility
for
die
t or
mea
l pla
n 29
3.
45
3.28
0.
736
0.70
2 1.
98
.057
C
hild
ass
umes
resp
onsi
bilit
y fo
r in
sulin
inj
ectio
n 29
3.
90
4.00
1.
047
1.00
0 4
.65
,5
22
Chi
ld a
ssum
es re
spon
sibi
lity
for
bloo
d-gl
ucos
e m
onito
ring
29
4.17
4.
07
0.96
6 0.
753
0.72
.4
77
Chi
ld a
ssum
es re
spon
sibi
lity
for u
rine-
keto
ne m
onito
ring
27
3.04
2.
96
1.12
6 1.
055
0.40
,6
91
Chi
ld a
ssum
es r
espo
nsib
ility
for
act
ivity
lev
el m
onito
ring
29
3.45
3.
28
0.73
6 0.
591
1.54
.1
34
Chi
ld a
ssum
es re
spon
sibi
lity
for
over
all m
anag
emen
t pla
n 28
3.
71
3.54
0.
713
0.69
3 1.
99
.057
~
~~
Not
e. A
nsw
ers w
ere
rate
d on
a n
umer
ic s
cale
rang
ing from 1
to 5
, with
1 b
eing
wel
l bel
ow a
vera
ge fo
r ag
e and
5 be
ing
wel
l abo
ve a
vera
ge fo
r ag
e.
Issu
es C
ompr
Ped
iatr
Nur
s D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y SU
NY
Sta
te U
nive
rsity
of
New
Yor
k at
Sto
ny B
rook
on
10/2
7/14
For
pers
onal
use
onl
y.
Tabl
e 4.
Fact
ors i
nflu
enci
ng m
othe
rs’ a
nd fa
ther
s’ d
ecisi
on to
dec
ide
thei
r ch
ildre
n’s
self-
man
agem
ent
resp
onsib
ility
Item
or
scal
e
M
SD
n M
othe
r Fa
ther
M
othe
r Fa
ther
t
P
Chi
ld s
uppo
rt gr
oup
influ
ence
on
pare
nt i
n de
cidi
ng h
ow
20
2.35
2.
25 -
1.53
1 1.
209
0.35
.7
33
muc
h re
spon
sibi
lity
child
ass
umes
in d
iabe
tes
self-
m
anag
emen
t
muc
h re
spon
sibi
lity
child
ass
umes
in
diab
etes
sel
f-
man
agem
ent
deci
ding
how
muc
h re
spon
sibi
lity
child
ass
umes
in
diab
etes
sel
f-m
anag
emen
t
muc
h re
spon
sibi
lity
child
ass
umes
in d
iabe
tes
self-
m
anag
emen
t
pare
nt in
dec
idin
g ho
w m
uch
resp
onsi
bilit
y ch
ild
assu
mes
in d
iabe
tes
self-
man
agem
ent
deci
ding
how
muc
h re
spon
sibi
lity
child
ass
umes
in
dia
bete
s se
lf-m
anag
emen
t
Pare
nt s
uppo
rt gr
oup
influ
ence
on
pare
nt in
dec
idin
g ho
w
22
2.59
2.
18
1.70
9 1.
332
2.11
.0
47*
New
sch
ool o
r day
car
e se
tting
influ
ence
on
pare
nt i
n 14
2.
14
2.07
1.
562
1.20
7 0.
21
,836
Soci
al o
ppor
tuni
ty i
nflu
ence
on
pare
nt i
n de
cidi
ng h
ow
27
4.44
3.
81
0.89
2 1.
145
2.77
.0
10**
Influ
ence
of c
hild
’s te
mpe
ram
ent
or p
erso
nalit
y on
27
4.
48
3.70
0.
700
1.20
3 3.
23
.003
**
Influ
ence
of b
ook
or m
agaz
ine
artic
le o
n pa
rent
in
25
3.08
2.
76
1.47
0 1.
052
1.14
.2
66
~
Nof
e A
nsw
ers
wer
e ra
ted
on a
num
eric
sca
le r
angi
ng fr
om 1
to
5, w
ith 1
bei
ng no
rnflu
ence
and
5 b
eing
gre
at r
nji’u
ence
*p
I 0
5 **
p 5
01
Issu
es C
ompr
Ped
iatr
Nur
s D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y SU
NY
Sta
te U
nive
rsity
of
New
Yor
k at
Sto
ny B
rook
on
10/2
7/14
For
pers
onal
use
onl
y.
Self-Management of Diabetes 77
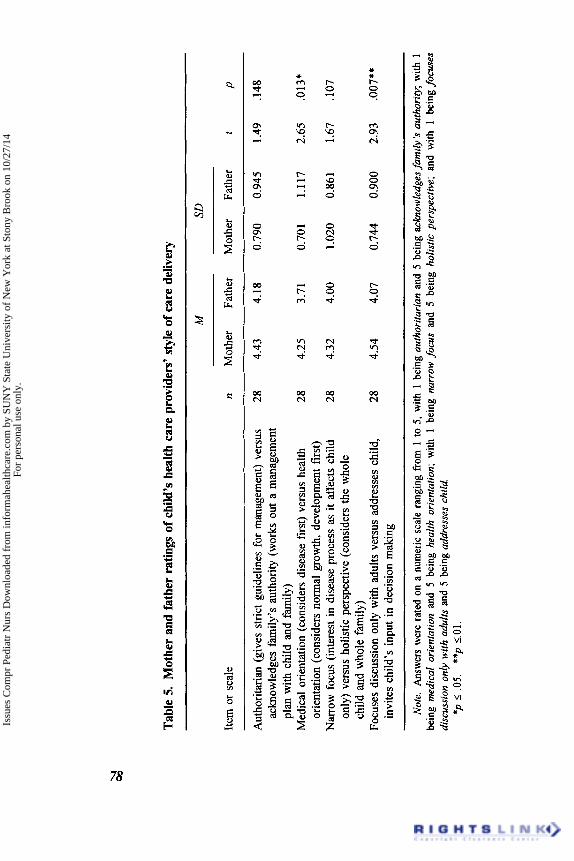
in the disease process as it affects the child oniy and 5 being having a holistic focus, and (d) 1 being having adult-focused discussions and 5 being inviting child’s input in decision making. Mothers and fathers rated health care providers as acknowledging family authority, having a health orientation with a primary focus on growth and development, having a holistic perspective that considers the whole child and the whole family, and inviting the child’s input with decision making. In all areas, mothers’ perspectives of these dimensions were slightly higher than fathers’. Two of the areas showed differences between mothers and fathers: disease orientation versus health orientation, t(28) = 2.65, p = .013, and discus- sion focus with adults versus addresses child, invites child’s input in decision making, t(28) = 2.93, p = .007 (see Table 5) .
Mothers’ and Fathers’ Serf-Efjcacy
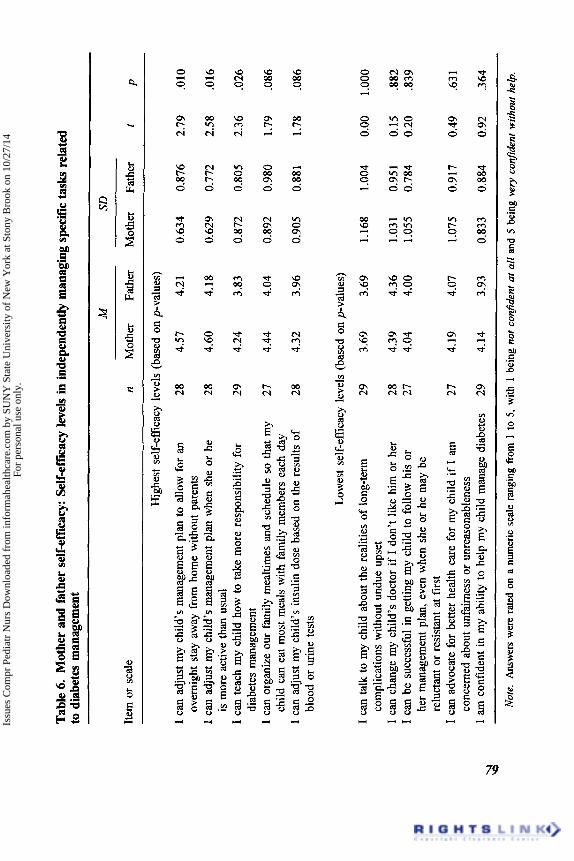
Mothers and fathers were asked to rate their level of confidence in man- aging specific tasks related to diabetes management. Answers were rated on a 5-point numeric scale, with 1 being not confident at all and 5 being vevy conJident. In 15 of 17 areas identified in Table 6 mothers felt very confident in their ability to manage tasks (ie.’ a mean greater than 4.00). Fathers also felt very confident in 12 of the 17 areas. In the item “I can adjust my child’s management plan if s h e gets a cold or flu,” mothers’ mean was 3.83 and fathers’ mean was 3.59, and in the item “I can talk to my child about the realities of long-term complications without undue upset,” mother’ mean 3.69 was equal to fathers’. In these two items, mothers and fathers felt least confident. In all areas, mothers’ level of confidence was slightly higher than fathers’. The following three items showed significant differences between mothers and fathers: ‘‘I can adjust child’s management plan when she is more active than usual,” t(28) = 2.58, p = .016; “ I can teach my child how to take more responsibility for diabetes management,” t(29) = 2.36, p = .026; and “I can adjust my child’s management plan to allow for an overnight stay away from home without parents,” t(28) = 2.79, p = .010 (see Table 6).
Handling of Tasks or Situations Related to Diabetes Management
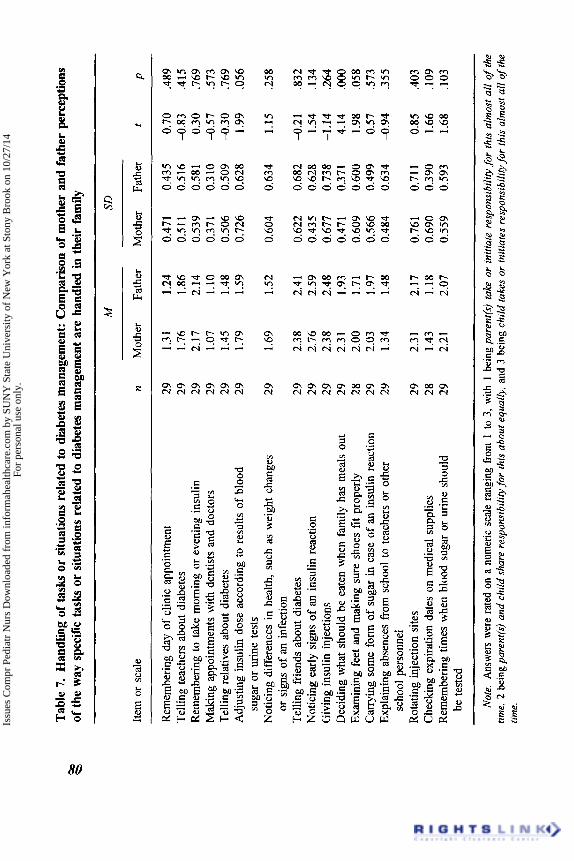
Parents were given a list of tasks or situations relating to diabetes man- agement in their family and were asked to identify whether (a) the parent(s) takes or initiates responsibility for this almost all the time, (b) parent(s) and child share responsibility for this equally, or (c) the child takes or initiates responsibility for this almost all the time. We computed statistics on a scale ranging from 1 to 3, with 1 being the parent($ taking respon-
Issu
es C
ompr
Ped
iatr
Nur
s D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y SU
NY
Sta
te U
nive
rsity
of
New
Yor
k at
Sto
ny B
rook
on
10/2
7/14
For
pers
onal
use
onl
y.
Tab
le 5
. M
othe
r an
d fa
ther
rat
ings
of c
hild
’s h
ealth
car
e pr
ovid
ers’
sty
le o
f car
e de
liver
y
Item
or
scal
e
M SD
n M
othe
r Fa
ther
M
othe
r Fa
ther
t
P
Aut
horit
aria
n (g
ives
stri
ct g
uide
lines
for m
anag
emen
t) ve
rsus
28
4.
43
4.18
0.
790
0.94
5 1.
49
.I48
ac
know
ledg
es fa
mily
’s a
utho
rity
(wor
ks o
ut a
man
agem
ent
plan
with
chi
ld a
nd f
amily
)
orie
ntat
ion
(con
side
rs n
orm
al g
row
th,
deve
lopm
ent f
irst)
only
) ver
sus
holis
tic p
ersp
ectiv
e (c
onsi
ders
the
who
le
child
and w
hole
fam
ily)
invi
tes c
hild
’s in
put i
n de
cisi
on m
akin
g
Med
ical
orie
ntat
ion
(con
side
rs d
isea
se fi
rst)
vers
us h
ealth
28
4.
25
3.71
0.
701
1.11
7 2.
65
.013
*
Nar
row
foc
us (i
nter
est i
n di
seas
e pr
oces
s as
it a
ffec
ts c
hild
28
4.
32
4.00
1.
020
0.86
1 1.
67
.lo7
Focu
ses
disc
ussi
on o
nly
with
adu
lts v
ersu
s ad
dres
ses c
hild
, 28
4.
54
4.07
0.
744
0.90
0 2.
93
.007
**
Not
e. Answers w
ere
rate
d on
a n
umer
ic s
cale
rang
ing
from
1 to
5,
with
1 b
eing
aut
hori
tari
an an
d 5
bein
g ac
know
ledg
esfa
mily
’s au
thor
iwy;
with
1
bein
g m
edic
al o
rien
tatio
n an
d 5
bein
g he
alth
ori
enta
tion;
with
1 b
eing
nar
row
focus a
nd 5
bei
ng h
olis
tic p
ersp
ectiv
e; a
nd w
ith 1
bei
ng fo
cuse
s di
scus
sion
onl
y w
ith a
dults
and
5 b
eing
add
ress
es c
hild
. *p
I .05.
**p
5.01
.
Issu
es C
ompr
Ped
iatr
Nur
s D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y SU
NY
Sta
te U
nive
rsity
of
New
Yor
k at
Sto
ny B
rook
on
10/2
7/14
For
pers
onal
use
onl
y.
Tab
le 6
. M
othe
r an
d fa
ther
sel
f-effi
cacy
: Sel
f-effi
cacy
leve
ls in
inde
pend
ently
man
agin
g sp
ecifi
c tasks r
elat
ed
to d
iabe
tes m
anag
emen
t
M
SD
n M
othe
r Fa
ther
M
othe
r Fa
ther
t
P Ite
m o
r sc
ale
Hig
hest
sel
f-ef
ficac
y le
vels
(ba
sed
on p
-val
ues)
I ca
n ad
just
my
child
’s m
anag
emen
t pla
n to
allo
w f
or a
n 28
4.
57
4.21
I ca
n ad
just
my
child
’s m
anag
emen
t pla
n w
hen
she
or h
e 28
4.
60
4.18
I ca
n te
ach
my
child
how
to ta
ke m
ore
resp
onsi
bilit
y fo
r 29
4.
24
3.83
I ca
n or
gani
ze o
ur fa
mily
mea
ltim
es a
nd s
ched
ule
so th
at m
y 27
4.
44
4.04
I ca
n ad
just
my
child
’s i
nsul
in d
ose
base
d on
the
resu
lts o
f 28
4.
32
3.96
over
nigh
t st
ay a
way
fro
m h
ome
with
out
pare
nts
is m
ore
activ
e th
an u
sual
diab
etes
man
agem
ent
child
can
eat
mos
t mea
ls w
ith f
amily
mem
bers
eac
h da
y
bloo
d or
urin
e te
sts
Low
est
self-
effic
acy
leve
ls (
base
d on
p-v
alue
s)
I ca
n ta
lk to
my
child
abo
ut th
e re
aliti
es o
f lo
ng-te
rm
29
3.69
3.
69
I ca
n ch
ange
my
child
’s d
octo
r if
I do
n’t
like
him
or
her
28
4.39
4.
36
I can
be
succ
essf
ul in
get
ting
my
child
to
follo
w h
is o
r 27
4.
04
4.00
he
r m
anag
emen
t pla
n, e
ven
whe
n sh
e or
he
may
be
relu
ctan
t or
resi
stan
t at
firs
t I c
an a
dvoc
ate
for
bette
r he
alth
car
e fo
r m
y ch
ild i
f I
am
conc
erne
d ab
out u
nfai
rnes
s or
unr
easo
nabl
enes
s
com
plic
atio
ns w
ithou
t und
ue u
pset
27
4.19
4.
07
I am
con
fiden
t in
my
abili
ty to
hel
p m
y ch
ild m
anag
e di
abet
es
29
4.14
3.
93
\1
0.63
4
0.62
9
0.87
2
0.89
2
0.90
5
1.16
8
1.03
1 1.
055
1.07
5
0.83
3
0.87
6
0.77
2
0.80
5
0.98
0
0.88
1
1.00
4
0.95
1 0.
784
0.91
7
0.88
4
2.79
2.58
2.36
1.79
1.78
0.00
0.15
0.
20
0.49
0.92
.010
.016
.026
.086
.086
1 .ooo
.882
.8
39
.63 1
.364
\d
N
ote.
Ans
wer
s w
ere
rated
on
a nu
mer
ic s
cale
rang
ing from 1
to 5
, with
1 b
eing
not
con
fiden
t at
all
and
5 be
ing
very
con
fiden
t wi
thou
t he
lp.
Issu
es C
ompr
Ped
iatr
Nur
s D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y SU
NY
Sta
te U
nive
rsity
of
New
Yor
k at
Sto
ny B
rook
on
10/2
7/14
For
pers
onal
use
onl
y.
Tabl
e 7.
Han
dlin
g of
task
s or
situ
atio
ns re
late
d to
dia
bete
s man
agem
ent:
Com
pari
son
of m
othe
r an
d fa
ther
per
cept
ions
of
the
way
spe
cific
task
s or
situ
atio
ns re
late
d to
dia
bete
s m
anag
emen
t are
han
dled
in t
heir
fam
ily
Item
or
scal
e
Rem
embe
ring
day
of c
linic
app
oint
men
t Te
lling
teac
hers
abo
ut d
iabe
tes
Rem
embe
ring
to ta
ke m
orni
ng o
r ev
enin
g in
sulin
M
akin
g ap
poin
tmen
ts w
ith d
entis
ts a
nd d
octo
rs
Telli
ng r
elat
ives
abo
ut d
iabe
tes
Adj
ustin
g in
sulin
dos
e ac
cord
ing
to re
sults
of
bloo
d su
gar o
r ur
ine
test
s N
otic
ing
diff
eren
ces
in h
ealth
, suc
h as w
eigh
t cha
nges
or
sig
ns o
f an i
nfec
tion
Telli
ng f
riend
s ab
out d
iabe
tes
Not
icin
g ea
rly s
igns
of
an in
sulin
rea
ctio
n G
ivin
g in
sulin
inj
ectio
ns
Dec
idin
g w
hat s
houl
d be
eat
en w
hen
fam
ily h
as m
eals
out
Ex
amin
ing
feet
and
mak
ing
sure
sho
es fi
t pro
perly
C
arry
ing
som
e fo
rm of
suga
r in
cas
e of
an
insu
lin r
eact
ion
Expl
aini
ng a
bsen
ces
from
sch
ool t
o te
ache
rs o
r ot
her
scho
ol p
erso
nnel
R
otat
ing
inje
ctio
n si
tes
Che
ckin
g ex
pira
tion
date
s on
med
ical
sup
plie
s R
emem
berin
g tim
es w
hen
bloo
d su
gar
or u
rine
shou
ld
be te
sted
M SD
n M
othe
r Fa
ther
~ Mot
her
Fath
er
t P
29
29
29
29
29
29
29
29
29
29
29
28
29
29
29
28
29
1.31
1.
24
1.76
1.
86
2.17
2.
14
1.07
1.
10
1.45
1.
48
1.79
1.
59
1.69
1.
52
2.38
2.
41
2.76
2.
59
2.38
2.
48
2.3 1
1.
93
2.00
1.
71
2.03
1.
97
1.34
1.
48
2.3
1 2.
17
1.43
1.
18
2.21
2.
07
0.47
1 0.
435
0.51
1 0.
516
0.53
9 0.
581
0.37
1 0.
310
0.50
6 0.
509
0.72
6 0.
628
0.60
4 0.
634
0.62
2 0.
682
0.43
5 0.
628
0.67
7 0.
738
0.47
1 0.
371
0.60
9 0.
600
0.56
6 0.
499
0.48
4 0.
634
0.76
1 0.
711
0.69
0 0.
390
0.55
9 0.
593
0.70
-0
.83
0.30
-0
.57
-0.3
0 1.
99
1.15
-0.2
1 1.
54
-1.1
4 4.
14
1.98
0.
57
4.9
4
0.85
1.
66
1.68
.489
,4
15
.769
.5
73
.769
.0
56
.258
.832
.1
34
.264
.oo
o .0
58
.573
.3
55
.403
.1
09
.103
Not
e. A
nsw
ers w
ere r
ated
on a
num
eric
scal
e ra
ngin
g fro
m 1
to 3
, with
1 b
eing
pare
nt($
tak
e or
ini
tiate
res
pons
ibili
ty fo
r th
is a
lmos
t al
l of
the
trine
, 2 b
eing p
aren
t@) a
nd c
hild
sha
re r
espo
nsib
ility
for
this
abo
ut e
qual
ly, a
nd 3
bei
ng c
hild
take
s or
initi
ates
res
pons
ibili
ty fo
r th
is a
lmos
t aN
ofth
e tim
e.
Issu
es C
ompr
Ped
iatr
Nur
s D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y SU
NY
Sta
te U
nive
rsity
of
New
Yor
k at
Sto
ny B
rook
on
10/2
7/14
For
pers
onal
use
onl
y.
Self-Management of Diabetes 81
sibility; 2, the parent and child sharing responsibility, and 3, the child taking responsibility. The following ranges were used to interpret the results: (a) less than 1.5, parent taking or initiating responsibility; (b) 1.5 to 2.5, shared responsibility between parents and child; and (c) greater than 2.5, child taking or initiating responsibility.
The following areas had parents taking or initiating responsibility: (a) remembering day of clinic appointment, (b) making appointments with dentists and doctors, (c) telling relatives about diabetes, (d) explaining absences from school to teachers or other school personnel, and (e) checking expiration dates on medical supplies. The majority of the tasks or situa- tions related to diabetes management were perceived to have shared re- sponsibility between parent(s) and child. The only area where the child was perceived to initiate or take responsibility was in noticing early signs of an insulin reaction (see Table 7).
DISCUSSION
The matched sets of parents (mothers and fathers) allowed comparisons of areas of similarities and differences between parents as they related to their children’s self-management of diabetes. Mothers and fathers in this study were actively involved in the care and management of their chil- dren.
Throughout, the results of mothers’ and fathers’ ratings (means) were high. Specifically, their overall ratings were high related to the children’s responsibility for self-management, style of care delivery, and mothers’ and fathers’ self-efficacy related to independently managing the specific tasks related to diabetes management. Mothers’ ratings (means) were similar but slightly higher than fathers’ ratings (means) in 11 of the 17 areas, with the 1 area of significant difference being deciding what should be eaten when the family has meals out. Eiser et al. (1992) demonstrated a similar pattern in investigating age and gender differences in adjustment to chronic disease in children suffering from one of five conditions, in- cluding diabetes. Their ratings of adjustment and disease-related restric- tions, obtained separately from mothers and fathers, found that fathers’ ratings did not contradict mothers’ ratings, although they were less dif- ferentiated. We would concur with Eiser et al. in their postulation that the differences may reflect fathers’ decreased involvement with the children and less realistic expectations about behavior and are characteristic of parents’ views of their children with or without chronic disease.
In all areas, mothers and fathers perceived that their children were average or above average for the amount of responsibility their children assumed for diabetes self-management compared with the average child
Issu
es C
ompr
Ped
iatr
Nur
s D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y SU
NY
Sta
te U
nive
rsity
of
New
Yor
k at
Sto
ny B
rook
on
10/2
7/14
For
pers
onal
use
onl
y.
82 B. J. Leonard el al.
with diabetes of the same age. In five of the six areas, mothers’ means were higher than fathers’ means, with no areas of significant difference. Of interest, the two areas rated highest by parents for children’s respon- sibility for self-management compared with the average child with diabe- tes the same age were the following: child assumes responsibility for insulin injection and child assumes responsibility for blood-glucose mon- itoring. Allen et a]. (1983) found in their study that parents attached particular significance to giving insulin injections as an indication of their children’s independence in diabetes management. Although results show that parents perceive their children as average or above average for re- sponsibility, it is important that the parents stay actively involved in their support to their children and that the children are comfortable with the level of responsibility they have assumed (Follansbee, 1989; Frey & Fox, 1990).
The two factors that showed the most influence for both mothers’ and fathers’ perceptions in deciding how much responsibility their children should assume for diabetes self-management were social opportunity (meals, sleepovers, and day trips) and children’s temperament or personality. The fact that social opportunity was rated high as a motivating factor is a positive finding supportive of normal development for the age group studied. Parents may seek ways to normalize life for their children with diabetes, thus the children would need to assume responsibility for self- management in order for them to participate in age-appropriate social opportunities.
Although mothers’ perceptions were always greater than fathers’ per- ceptions, areas of significant difference in their perceptions of diabetes self-management for their children included how parent support group, social opportunity, and child’s temperament or personality influenced them in deciding how much responsibility their children should assume in self- management. The significant difference in mothers’ and fathers’ percep- tions of support group influence is documented by Copeland and Clements (1 993), who identified that fathers used reasoning strategies more than mothers and mothers used releasing and relating (support groups) strate- gies more than fathers. McKeever (1981) also identified fathers’ hesi- tancy to use support groups.
Parents’ perceptions about the style of care delivery by the child’s health care providers were very similar. These are positive findings in that this type of health care experience could facilitate the process for transfer of care from parent to child both by role modeling and providing support to parents. Dashiff (1993) found that parents perceived the health care provider as supportive when the provider permitted them to express feelings and still recognized the parents’ competence and primacy in overseeing care. Again, although in all areas mothers’ perceptions were
Issu
es C
ompr
Ped
iatr
Nur
s D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y SU
NY
Sta
te U
nive
rsity
of
New
Yor
k at
Sto
ny B
rook
on
10/2
7/14
For
pers
onal
use
onl
y.
Self-Management of Diabetes 83
higher than fathers’ perceptions, the two areas that showed significant difference were disease orientation versus health orientation and focuses discussion only with adults versus addresses child (invites child’s input in decision making). The significant areas of difference may be explained by the fact that mothers usually have more interaction with health care providers and may be more sensitive to the style of care delivery. Copeland and Clements (1993) found that mothers used relating strategies more than fathers. Mothers are often more focused on day-to-day management, which may include health care encounters (McKeever, 1981). These highly favorable results invite closer examination of the health care delivery system philosophy and components and the health care provider and fam- ily interactions and relationships that are supportive of parents.
Overall findings showed that both mothers and fathers felt very confi- dent in their ability to independently manage specific identified tasks related to diabetes management. This is a positive finding specific to their parental ability to independently manage the identified tasks related to their children’s diabetes. The high levels of perceived self-efficacy may affect which activities are attempted, the amount of effort put into the specific task, and the length of persistence when difficulties are en- countered (O’Leary, 1985). Adolescence is a time when the routine of diabetes management may be disrupted, and mothers’ and fathers’ posi- tive perceptions of self-efficacy may be a strength supporting their per- sistence and involvement with the process of successfully transferring care.
In all areas except one (“I can talk to my child about the realities of long-term complications without undue upset”), where mothers’ and fathers’ ratings were equal, mothers’ ratings were higher than fathers’ ratings. The areas having significant difference were adjusting child’s management plan based on activity level, teaching child to take increased responsibility for self-management, and adjusting child’s management plan to allow for overnight stay. A possible explanation for these signifi- cant differences is that mothers may do more day-to-day planning for their children with diabetes.
The two lowest rated areas for both mothers and fathers were I can adjust my child’s management plan when s/he gets a cold or the flu (mothers’ mean = 3.83, fathers’ mean = 3.59) and I can talk to my child about the realities of long-term complications without undue upset (mothers’ and fathers’ means = 3.69). It would not be unusual to expect parents to seek guidance for how to adjust the management plan when their chil- dren are sick, and therefore this may be one possible reason for a lower rating. One might expect that talking to children about the realities of long-term complications without undue upset may be difficult and possi- bly not even appropriate depending on the children’s developmental level
Issu
es C
ompr
Ped
iatr
Nur
s D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y SU
NY
Sta
te U
nive
rsity
of
New
Yor
k at
Sto
ny B
rook
on
10/2
7/14
For
pers
onal
use
onl
y.
84 B. J. Leonard et al.
and status of disease. Canam (1987) conducted a study that explored ways parents coped with the adaptive task of communicating their children’s chronic illness within the family. She found that although 74% of parents identified feelings they thought their children were experiencing about having a chronic illness, 81% said they did not talk to their children about their feelings. Reasons for this included that it did not occur to parents to talk to their children about their feelings, their lack of aware- ness of the need to explore the children’s feelings, and they did not want to make their children feel worse. Ninety-one percent of parents stated they had received no guidance related to talking to children about feel- ings related to their chronic illness (Canam, 1987).
When given a list of specific tasks or situations related to diabetes management, parents in this study perceived that they initiated or took primary responsibility for the following most of the time: (a) remember- ing day of clinic appointment, (b) making appointments with dentists and doctors, (c) telling relatives about diabetes, (d) explaining absences from school to teachers or other school personnel, and (d) checking expiration dates on medical supplies. Considering the sample age range of the chil- dren in this study was 8-14, parents would routinely assume responsibil- ity for health care encounters for their children, for checking expiration dates on medical supplies, and for telling relatives about diabetes. It also would not be unusual for a parent to be the person responsible for ex- plaining absences to school personnel, and it is likely they would be expected to relay the reason. The majority (10 out of 16) of the tasks or situations related to diabetes management were perceived to have shared responsibility between parent(s) and child. This is important as we look at self-care capacity for adolescents. The only area where the child was perceived to initiate or take responsibility was noticing early signs of an insulin reaction. This is an important area for the child to assume re- sponsibility so that appropriate intervention can occur in a timely way. Children in this sample would be at a developmental age where one would expect them to be spending timc alone or with friends; therefore, being able to recognize signs of an insulin reaction would be a necessary survival skill.
This study had a homogeneous sample in terms of race, education, and occupation that may represent the children with Type I diabetes in this region. It should be noted that more than half of the children came from outside major metropolitan areas in the upper Midwest and were identi- fied as rural. The factors contributing to their high ratings by both parents were not specifically identified but may be the result of the highly edu- cated sample. Twenty mothers and 22 fathers had vocational-technical, some college, or a college education. In addition, children who attend camp may comprise a highly motivated group that is more likely to
Issu
es C
ompr
Ped
iatr
Nur
s D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y SU
NY
Sta
te U
nive
rsity
of
New
Yor
k at
Sto
ny B
rook
on
10/2
7/14
For
pers
onal
use
onl
y.
Self-Management of Diabetes 85
exhibit self-care behaviors (Saucier & Clark, 1993). The cross-sectional nature of the study should also be noted, specifically recognizing that these parent perceptions were obtained at one point in time and may vary over time (Rodrigue, Geffken, Clark, & Hunt, 1994). Using a larger sample would allow age group comparisons in terms of age at diagnosis and time since diagnosis and other potential influencing factors. Further, although mothers and fathers in this study had more areas of similarity than differ- ence, we continue to support analyses of separate results in future studies as families are becoming increasingly diverse.
CONCL USION
The transfer of care from mothers and fathers to their children with any chronic illness is a complex process. Health care providers have the potential to affect this process and positively influence child outcomes. This study found both similarities and differences in the perceptions of mothers and fathers specific to their children’s self-management of dia- betes. Health care providers can influence child outcomes by (a) realizing that parents may have different perceptions related to the care of their chijdren with diabetes and assisting parents in identifying the differences so improved spousal communication may enhance mutual support (Cope- land & Clements, 1993); (b) providing opportunities for both parents to express their feelings and to acknowledge their differences (Dashiff, 1993); (c) recognizing and supporting the role of the family in developing ado- lescent self-care abilities; (d) informing parents of the necessity to remain involved in the care of their children or adolescents with diabetes and providing them support while they negotiate the transfer of specific self- care tasks and management (Deatrick et al., 1994); (e) carefully assessing each individual child’s ability to take on self-care responsibilities and negotiating with families the gradual transfer of these responsibilities to the child (Giordano et al., 1992); and ( f ) encouraging a partnership rela- tionship with the child where control by both are high and the partner- ship is characterized by collaboration and mutual support (Roter & Hall, 1992).
The parents in this study had high levels of perceived self-efficacy, which may have affected their high ratings. By planning strategies where parents can increase their skills and competence, perceived self-efficacy may become enhanced. For example, health professionals can encour- age parents to openly discuss concerns with them so they can address and alleviate these concerns and offer guidance in identifying and using parental strengths in the management of their children’s illness (Rodrigue et al., 1994). Family-centered care can be fostered when health professionals assess mothers’ and fathers’ perceptions rather than
Issu
es C
ompr
Ped
iatr
Nur
s D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y SU
NY
Sta
te U
nive
rsity
of
New
Yor
k at
Sto
ny B
rook
on
10/2
7/14
For
pers
onal
use
onl
y.
86 B. J. Leonard et al.
basing interventions on what they themselves perceive as best (Copeland, 1993).
REFERENCES
Allen, D. A., Tennen, H., McGrade, B., Affleck, G., & Ratzan, S. (1983). Parent and child perceptions of the management of juvenile diabetes. Journal of Pediatric Psy-
Anderson, B. J., Auslander, W. F., Jung, K. C., Miller, J. P., & Santiago, J. V. (1990). Assessing family sharing of diabetes responsibilities. Journal of Pediatric Psychol- ogy, 15(4), 477-492.
Beckman, P. J. (1991). Comparison of mothers’ and fathers’ perceptions of the effect of young children with and without disabilities. American Journal on Mental Retarda- tion, 95(5), 585-595.
Canam, C. (1987). Coping with feelings: Chronically ill children and their families. Nursing Papers, I9(3), 9-2 I .
Copeland, L. G. (1993). Caring for children with chronic conditions: Model of critical times. Holistic Nurse Practitioner, 8( I) , 45-55.
Copeland, L. G., & Clements, D. B. (1993). Parental perceptions and support strategies in caring for a child with a chronic condition. Issues in Comprehensive Pediatric Nursing, 16, 109-1 2 1.
Cummings, S. T. (1976). The impact of the child’s deficiency on the father: A study of fathers of mentally retarded and of chronically ill children. American Journal of Orthopsychiatry, 46( 2), 246-255,
Dashiff, C. J. (1993). Parents’ perceptions of diabetes in adolescent daughters and its impact on the family. Journal of Pediatric Nursing, 8(6), 361-369.
Deatrick, J. A., Angst, D. B., & Madden, M. (1994). Promoting self-care with adoles- cents. Capsules & Comments in Pediatric Nursing, 1(2), 11-20.
Eiser, C., Havermans, T., Pancer, M., & Eiser, I. R. (1992). Adjustment to chronic disease in relation to age and gender: Mothers’ and fathers’ reports of their childrens’ behavior. Journal of Pediatric Psychology, I7(3), 261-275.
Follansbee, D. S. (1989). Assuming responsibility for diabetes management: What age? what price? The Diabetes Educator, 15(4), 347-353.
Frey, M. A., & Fox, M. A. (1990). Assessing and teaching self-care to youths with diabetes mellitus. Pediatric Nursing, 16(6), 597-599.
Giordano, B. P., Petrila, A,, Banion, C. R., & Neuenkirchen, G. (1992). The challenge of transferring responsibility for diabetes management from parent to child. Journal of Pediatric Health Care, 6, 235-239.
Johnston, C. E., & Marder, L. R. (1994). Parenting the child with a chronic condition: An emotional experience. Pediatric Nursing, 20(6), 61 1 4 1 4 .
McKeever, P. T. (1981). Fathering the chronically ill child. MCN, 6, 124-128. Moos, R. H., & Moos, B. S. (1986). Family environment scale manual (2nd ed.). Palo
O’Leary, A. (1985). Self-efficacy and health. Behavior Research and Therapy, 23(4),
chology, 8(2), 129-141.
Alto, CA: Consulting Psychologists Press.
437-451.
Issu
es C
ompr
Ped
iatr
Nur
s D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y SU
NY
Sta
te U
nive
rsity
of
New
Yor
k at
Sto
ny B
rook
on
10/2
7/14
For
pers
onal
use
onl
y.

Self-Management of Diabetes 87
Patterson, J. M. (1991). Family systems perspective for working with youth with disabil- ity. Pediatrician, 18. 129-1 4 1.
Rodrigue, J. R., GeMten, G. R., Clark, J. E., & Hunt, F. (1994). Parenting satisfaction and efficacy among caregivers of children with diabetes. Children’s Health Cure
Roter, D. L., & Hall, J. A. (1 992). Doctors talking with patients/putients talking with doctors. Westport, CT: Auburn Health.
Saucier, C. P., & Clark, L. M. (1993). The relationship between self-care and metabolic control in children with insulin-dependent diabetes rnellitus. The Diabetes Educator,
23(3), 181-191.
19(2), 133-135.
Issu
es C
ompr
Ped
iatr
Nur
s D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y SU
NY
Sta
te U
nive
rsity
of
New
Yor
k at
Sto
ny B
rook
on
10/2
7/14
For
pers
onal
use
onl
y.





























