-
Original Article
Comparison of Outcomes of Percutaneous Endoscopic Lumbar
Discectomy
and Open Lumbar Microdiscectomy for Young Adults: A
Retrospective MatchedCohort Study
Sang-Soak Ahn1, Sang-Hyeon Kim2, Dong-Won Kim2, Byung-Hun
Lee3
-OBJECTIVE: There have been only a few studies onsurgical
treatment of lumbar disc herniation (LDH) in youngadults. In
addition, previous studies do not provide detailedinformation on
the surgical outcomes for young adults withLDH. The purpose of this
study was to compare theoutcome of transforaminal percutaneous
endoscopic lum-bar discectomy (PELD) and open lumbar
microdiscectomyfor active, young adults (age 20e25 years).
-METHODS: We performed retrospective chart and radi-ography. The
patients were divided into 2 groups accordingto the surgical
methods. Group A included the patients whounderwent transforaminal
PELD, and Group B included thepatients who underwent open lumbar
microdiscectomy forLDH at L4/5. After we matched for several
factors, 32 youngpatients in group A and 34 young patients in group
B wereanalyzed. We compared the outcomes between the 2groups in
terms of clinical, radiologic, perioperative out-comes, and
surgery-related complications.
-RESULTS: The clinical results for leg pain and
radiologicresults for decompression were the same in both
groups.Most of complications in the PELD group occurred in theearly
phase. The recurrence rate and operation failure ratewas no
difference between the groups. The PELD broughtsignificant
advantages in the following areas: back pain,operation time, blood
loss, hospital stay, and return-to-work.
Key words- Diskectomy- Percutaneous- Endoscopy- Intervertebral
disc displacement- Young adult
Abbreviations and AcronymsDSCSA: Dural sac cross-sectional
areaLDH: Lumbar disc herniationMRI: Magnetic resonance imagingODI:
Oswestry Disability IndexOLM: Open lumbar microdiscectomyPELD:
Percutaneous endoscopic lumbar diskectomyPLL: Posterior
longitudinal ligamentSF-12: 12-item short form health survey
250 www.SCIENCEDIRECT.com WORLD NEU
-CONCLUSIONS: Although a learning curve is needed inorder to
become familiar with PELD, PELD seemed to be agood choice for disc
herniation in the lumbar spine foractive, young adults.
INTRODUCTION
umbar disc herniation (LDH) is a relatively common causeof
sciatica in young adults.1-5 Most young adults with LDH
Lcan be managed properly with conservative treatment;
however, a small number of patients do not respond effectively
toconservative treatment and eventually require surgical
treatment.There are 2 main surgical options: open lumbar
microdiscectomy(OLM) and percutaneous endoscopic lumbar discectomy
(PELD).OLM has been considered to be the gold standard procedure
forsymptomatic lumbar disc diseases1,6-9; however, open
surgeryresults in muscle damage, the removal of the yellow
ligament, andnerve retraction. This can cause instability and
scarring of theepidural space, which becomes clinically symptomatic
in 10% ormore of patients.6,7,9,10 PELD has been performed as an
alternativeto classic open discectomy with comparable results.
There arepotential downsides of the tranforaminal PELD, such as
transientparesthesias, a larger annular defect, and difficulties
accessingL5/S1 in patients with a prominent iliac crest. In
addition, thelearning curve is perceived to be steep. However, it
has severaladvantages over open discectomy, including (1) the
ability to beperformed under local anesthesia; (2) minimal
postoperative pain
VAS: Visual analog scale
From the 1Department of Neurosurgery, Spine and Spinal Cord
Institute, Gangnam SeveranceSpine Hospital, Yonsei University
College of Medicine, Seoul; 2Department of Radiology,Dong-A
University Medical Center, Busan; and 3Department of Neurosurgery,
The ArmedForces Capital Hospital, Seongnam, Korea
To whom correspondence should be addressed: Sang-Soak Ahn,
M.D.[E-mail: [email protected]]
Citation: World Neurosurg. (2016)
86:250-258.http://dx.doi.org/10.1016/j.wneu.2015.09.047
Journal homepage: www.WORLDNEUROSURGERY.org
Available online: www.sciencedirect.com
1878-8750/$ - see front matter ª 2016 Elsevier Inc. All rights
reserved.
ROSURGERY, http://dx.doi.org/10.1016/j.wneu.2015.09.047
http://crossmark.crossref.org/dialog/?doi=10.1016/j.wneu.2015.09.047&domain=pdfmailto:[email protected]://dx.doi.org/10.1016/j.wneu.2015.09.047http://www.WORLDNEUROSURGERY.orgwww.sciencedirect.com/science/journal/18788750www.sciencedirect.com/science/journal/18788750http://dx.doi.org/10.1016/j.wneu.2015.09.047
-
ORIGINAL ARTICLE
SANG-SOAK AHN ET AL. PELD VERSUS OLM FOR YOUNG ADULTS
and preservation of the normal para-spinal muscles; and (3)
aminimization of the risk of postoperative epidural scar
formationand instability.4,11-18 A consensus on the preferred
surgical methodin young patients has not been established, however,
and therehave only been a few studies in which the authors examined
thesurgical treatment of LDH in young adults.1,2,4,5
We conducted this study to compare the clinical, radiologic,and
perioperative outcomes of transforaminal PELD and OLM foryoung
adults (age 20e25 years) with LDH, as well as the surgery-related
complications. To the best of our knowledge, this is thefirst study
to compare the outcomes of PELD and OLM in youngadults by the use
of a retrospective matched cohort design.
MATERIALS AND METHODS
Study DesignThis study was carried out after we obtained
approval from theinstitutional review board (The Armed Forces
Capital Hospital[AFMC-15041-IRB-15-057]). Between May 2012 and
January 2014,178 consecutive patients with LDH who underwent
surgical treat-ment were considered for this study. The inclusion
criteria were asfollows: (1) a soft LDH within the spinal canal in
L4�5 (including
Figure 1. Flowchart depicting patient selection. OLM, lumbar
mdiscectomy.
WORLD NEUROSURGERY 86: 250-258, FEBRUARY 2016
the sequestering of material located cranially below the lower
edgeof the cranial pedicle or caudally not over the middle of the
caudalpedicle), with lumbar spine radiographs, computed
tomography,and magnetic resonance image (MRI) corresponding to the
clinicalsymptoms; (2) age between 20 and 25 years; (3) nonresponse
to atleast 8 weeks of conservative treatment, including
medication,physical therapy, and injections; (4) a surgical
procedure performedby the designated spine surgeon (S.S.A.); and
(5) follow-up of atleast 1 year. Those who met any of the following
criteria wereexcluded: (1) lateral recess stenosis, hard disc
herniation, foraminaland extraforaminal disc herniations, and
spinal instability; (2)follow-up of less than 1 year; and (3) an
inability to accuratelycomplete the pre- and postoperative
questionnaires. Ninety-sevenpatients were excluded because of these
criteria.The patients were divided into 2 groups according to the
sur-
gical methods. Group A included the patients who underwentPELD
for disc herniation, and Group B included those who un-derwent OLM.
After we matched for tobacco smoking and bodymass index between the
2 groups, 32 patients in group A and 34patients in group B were
analyzed (Figure 1). All of these patientswere Korean military
serviceman at the time of their operations.Before surgery, all
patients were informed of the details of the
icrodiscectomy; PELD, percutaneous endoscopic lumbar
www.WORLDNEUROSURGERY.org 251
http://www.WORLDNEUROSURGERY.org
-
ORIGINAL ARTICLE
SANG-SOAK AHN ET AL. PELD VERSUS OLM FOR YOUNG ADULTS
surgery, including the anesthesia process,
potentialcomplications, and benefits of the procedures. One
spinesurgeon with 4 years of surgical experience was involved in
thestudy. The selection of the surgical method was based on
thissurgeon’s recommendation as well as patient preference.
Clinical AssessmentClinical and demographic data were recorded
prospectively. Thepatients completed a questionnaire consisting of
a 10-pointvisual analog scale (VAS) for low back pain and leg pain
pre-operatively and at each follow-up visit. The patients
alsocompleted the Oswestry Disability Index (ODI) and a
12-itemshort form health survey (SF-12) for their quality of life
preop-eratively and at each follow-up visit. The physical
componentsummary and mental component summary of the SF-12
wererecorded separately. Follow-up visits occurred at 6 and
12months after surgery. Patients were not allowed to review
theirprevious results. The operation time, blood loss, hospital
stay,return-to-work time, complication rate, failure rate, and
12-month reherniation rate were evaluated to assess the outcomesof
the procedures.
Radiologic AssessmentAll patients underwent MRI preoperatively
and at 12 months aftersurgery. The change in the dural sac
cross-sectional area (DSCSA)between the preoperative and the
postoperative MRI was evaluatedto demonstrate the extent of
decompression. This space wasdrawn by an imaginary area at the
narrowest lesion on the T2-weighted axial MRI (Figure 2). The MRI
scans were performedusing a 1.5-T MRI system (Signa Excite scanner,
General ElectricCompany, Milwaukee, Wisconsin, USA) with a slice
thickness of 5mm. To evaluate the radiologic parameters, two
radiologists(S.H.K. and D.W.K.) independently measured the
preoperativeand postoperative parameters using a picture archiving
commu-nication system feature (Marosis 5.0 PACS viewer,
Marotech,Seoul, Korea).
Figure 2. Dural sac cross-sectional area between the
preopera(MRI). The space was drawn by an imaginary area at the
narrowpicture archiving communication system.
252 www.SCIENCEDIRECT.com WORLD NEU
Surgical ProcedureIn group A, we used the “in-and-out-and-in”
technique. All op-erations were performed under local anesthesia
after sedation ofthe patient with the intramuscular administration
of midazolam(0.1 mg/kg) in the prone position. Before surgery, we
checked thelateral view of the C-arm image and determined the entry
point,which was between the tip of the spinous process and the
spi-nolaminar junction on the lateral view. The entry point was
usually10�15 cm from the midline. The entry point was projected to
have20�25 degrees of access (from the coronal plane) for L4�5. An
18-gauge spinal needle was introduced under the biplanar guidanceof
fluoroscopy. The final target point of the needle was the
medialpedicular line on the anteroposterior view and the
posteriorvertebral line on the lateral view.At this point,
epidurography was performed with contrast me-
dium and local anesthesia was carried out using 1%
lidocaine.After the insertion of the needle into the disc,
evocative chro-modiscography was performed with contrast medium and
indigo-carmine. A guide wire was then inserted through the needle,
andthe needle was removed. A linear skin incision about 8 mm
longwas made at the entry point, and an obturator (YESS
system;Richard Wolf, Knittlingen, Germany) was gently introduced by
atwisting maneuver. A bevel-ended working sheath was insertedinto
the disc space along the obturator, and then the obturator
wasremoved. After we placed the endoscope within the workingsheath,
the disc fragment at the base of the herniated mass wasremoved with
a high-voltage bipolar probe manufactured by Ell-man (Ellman
Innovation, Hicksville, New York, USA) and pituitaryforceps. After
the removal of the central disc fragment, theworking sheath was
moved back to the epidural space and theposterior longitudinal
ligament (PLL) was removed in the half-and-half view (Figure 3).
After removal of the PLL, while weconfirmed the pulsation of the
dura with direct visualization, theposterolateral target fragment
was removed by introducing theworking sheath from the lateral to
the medial area. After allprocedures were complete, the endoscope
was removed, and
tive and the postoperative magnetic resonance imagingest lesion
on the T2-weighted axial MRI by the use of a
ROSURGERY, http://dx.doi.org/10.1016/j.wneu.2015.09.047
www.sciencedirect.com/science/journal/18788750http://dx.doi.org/10.1016/j.wneu.2015.09.047
-
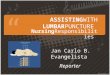
Figure 3. Intraoperative endoscopic view in transforaminal
approach with the posterior longitudinal ligament (A), whichis
removed by cutter (B). D, herniated disc stained by indigocarmine;
F, epidural fat; P, posterior longitudinal ligament).
Table 1. Demographic Data
Characteristics Group A Group B P Value
Number of patients 32 34
Mean age, year* 22.41 � 1.68 22.18 � 1.51 0.56Sex, male/female
32/0 34/0 1.00
Height, cm* 173.09 � 5.90 172.56 � 5.89 0.71Weight, kg* 66.53 �
6.60 67.03 � 6.24 0.75BMI, kg/m2* 22.16 � 1.22 22.46 � 0.90
0.26Smoking, %y 10 (31.2) 10 (29.4) 0.87Follow-up, mo* 13.69 � 1.26
13.41 � 1.02 0.33BMI, body mass index.*Student t test.yc2 test.
ORIGINAL ARTICLE
SANG-SOAK AHN ET AL. PELD VERSUS OLM FOR YOUNG ADULTS
a sterile dressing was performed with a one-point suture.
Thepatients were able to communicate with the surgeon during
theentire procedure.In group B, the procedure was performed under
general anes-
thesia in the prone position on a Wilson frame. A 3-cm
posteriormidline skin incision was made over the appropriate disc
space. Alimited laminotomy was performed using a high-speed drill.
Bythe use of a small annulotomy if needed, the disc fragment
wasremoved in the conventional manner under microscopic view.
Theforamen was then routinely probed for residual fragments or
bonylesions. After confirming the decompression of the nerve root,
theclosure was performed in the conventional manner.8
StatisticsStatistical analyses were performed using SPSS version
20.0 (SPSSInc., Chicago, Illinois, USA). The mean values � standard
de-viations or the medians with the interquartile ranges are
shown.Student t tests were conducted to confirm intergroup
differencesin cases with normal distributions. Mann-Whitney U tests
wereused to compare variables between two groups with
non-normaldistributions. For the categorical variables, c2 tests
and Fischerexact tests were performed between 2 independent groups.
AllP-values less than .05 were considered statistically
significant.
RESULTS
DemographicsWe reviewed 32 patients in group A (PELD) and 34
patients ingroup B (OLM) who met the inclusion and exclusion
criteria.Patient demographics including the follow-up period were
notsignificantly different between the 2 groups (Table 1).
Clinical OutcomesPreoperatively, the back and leg VAS scores
were 4.41 � 0.98 and7.53 � 0.92, respectively, in group A and, 4.74
� 1.08 and 7.50 �0.93, respectively, in group B. These results
revealed no significantdifferences. After surgery, the VAS scores
for the back and leg
WORLD NEUROSURGERY 86: 250-258, FEBRUARY 2016
decreased significantly in both groups. At 12 months after
surgery,the back and leg VAS scores were 2.50 � 0.62 and 2.06 �
0.84,respectively, in group A and 2.91 � 0.67 and 2.32 �
1.01,respectively, in group B. There were significant differences
be-tween the groups for back VAS score at 6 months and 12
monthsafter surgery (P < 0.001, P ¼ 0.012, respectively).
However, therewas no significant difference between the groups for
leg VAS scoreafter surgery (Figure 4).The mean ODI scores
significantly improved from baseline at
the final follow-up in both groups (Figure 5). As depicted
inFigure 5, there was a significant difference in ODI scoresbetween
the groups at 6 months after surgery (P ¼ 0.004). Themean physical
component summary score and mentalcomponent summary score in the
SF-12 improved at the finalfollow-up time as compared to the
baseline in both groups(Figure 6). As depicted in Figure 6, there
was a significant
www.WORLDNEUROSURGERY.org 253
http://www.WORLDNEUROSURGERY.org
-
Figure 4. Clinical outcomes using visual analog scale (VAS)
scores. There were significant differences between thegroups for
the back VAS at 6 and 12 months after surgery (yP < 0.013,
z0.012, respectively).
ORIGINAL ARTICLE
SANG-SOAK AHN ET AL. PELD VERSUS OLM FOR YOUNG ADULTS
difference in mental parameters between the groups at 6
monthsafter surgery (P ¼ 0.002) (Table 2).
Radiologic OutcomesThe preoperative DSCSA was 58.60 � 23.07 mm2
in group A and57.30 � 22.13 mm2 in group B. The postoperative DSCSA
was 75.25� 23.10 mm2 in group A and 75.83 � 22.00 mm2 in group B.
Theexpansion in DSCSA between the preoperative and the
post-operative MRI was 16.65 � 6.58 mm2 in group A and 18.53 �
6.19mm2 in group B. However, there was no significant
differencebetween the groups (P ¼ 0.092) (Table 3, Figure 7).
Perioperative OutcomesThe mean operating time was significantly
shorter in group A(48.66 � 6.45 minutes) as compared with group B
(53.71 � 8.49minutes) (P ¼ 0.009). There was no measurable blood
loss ingroup A; the mean intraoperative blood loss was 41.26 �
31.88 mL
Figure 5. Clinical outcomes using Oswestry Disability Index
(ODI) scores.*Statistically significant differences between scores
in each follow-uptime (P < 0.05). Preop, preoperative.
254 www.SCIENCEDIRECT.com WORLD NEU
(15e167 mL) in group B. However, both groups had negligibleblood
loss with no clinical significance. The mean hospital staywas
significantly shorter in group A (7.50 � 2.63 days) ascompared with
group B (15.65 � 4.80 days) (P < 0.001). The meanreturn-to-work
time was significantly shorter in group A (13.94 �3.72 days) as
compared with group B (29.26 � 5.80 days)(P < 0.001) (Table
4).
ComplicationsComplications occurred in 4 patients (12.5%) in
group A and 4patients (11.8%) in group B. Four patients complained
of dyses-thesia on the posterolateral thigh, which spontaneously
improved2�3 days after surgery (2 cases in group A and 2 cases in
group B).A dural tear occurred in 1 patient in group B, which was
suc-cessfully managed with direct repair. One patient with the
longestoperative time in group A complained of headache during
surgery,especially near the end of the procedure, which
spontaneouslyimproved after bed rest for 1 day. One patient
presented with asymptomatic pseudocyst 2 months after PELD, which
slowlyimproved after an epidural block. Postoperative epidural
hema-toma occurred in one patient in group B, which was
successfullyremoved with evacuation. There were no major
complicationssuch as neurovascular injury, retroperitoneal
hematoma, andsurgical-site infections in either group, and there
were no signif-icant differences in the complication rate between
the 2 groups(Table 4).
Operation Failures and RecurrencesIncomplete removal of the
target fragment occurred in 2 patientsin group A, which we
considered surgical failures. Because thesepatients complained of
leg pain after surgery, we performed a MRIin the immediate
postoperative period and detected the residualfragments. However,
no patients underwent reoperations due topatient preference and
were instead managed with conservativetreatment. There was no
significant difference in the failure ratebetween the 2 groups (P ¼
0.231). Reherniation at 12 monthsoccurred in one patient in group A
(3.1%) and one patient in groupB (2.9%). The patient in the PELD
group with reherniationoccurred at 6 months after surgery and was
managed with
ROSURGERY, http://dx.doi.org/10.1016/j.wneu.2015.09.047
www.sciencedirect.com/science/journal/18788750http://dx.doi.org/10.1016/j.wneu.2015.09.047
-
Figure 6. Clinical outcomes using 12-item short form health
survey (SF-12) scores. *Statistically significant
differencesbetween scores in each follow-up time (P < 0.05).
PCS, physical component summary; MCS, mental componentsummary.
Table 2. Clinical Outcomes According to the Parameters
Parameters Group A (n [ 32) Group B (n [ 34) P Value
VAS (back)
Preop 4.41 � 0.98 4.74 � 1.08 0.2016 months 2.66 � 0.70 3.53 �
0.71
-
Figure 7. Expansion of the dural sac cross-sectional area
(DSCSA). yTherewas no significant difference between the groups (P
¼ 0.092).
ORIGINAL ARTICLE
SANG-SOAK AHN ET AL. PELD VERSUS OLM FOR YOUNG ADULTS
in the ODI score was considered to reflect clinical
improvement,as proposed by the Food and Drug Administration.7 ODI
scorereductions were similar to those reported previously by
Ruettenet al.18 using the PELD and OLM techniques. However, both
theODI and mental SF-12 scores tended to worsen after 6
monthspostoperatively in the OLM group. There are several reasons
forthe worse outcomes in the OLM group 6 months after
surgerycompared with the PELD group: (1) OLM requires further
muscledissection and the removal of posterior structures such as
thelamina, yellow ligament, and facet joint, which might
affectpostoperative back pain as well as physical and mental
statuses;and (2) all patients were active young men who returned to
a
Table 4. Summary of Perioperative Outcomes,
Complications,Failure, and Recurrence Rate
Group A (n [ 32) Group B (n [ 34) P Value
Op time, min* 48.66 � 6.45 53.71 � 8.49 0.009EBL, mL Not
measureable 41.26 � 31.88Hospital stay, daysy 7.50 � 2.63 15.65 �
4.80 0.05Op, operation; EBL, estimated blood loss.*Student t
test.yMann-Whitney U test.zFisher’s exact test.
256 www.SCIENCEDIRECT.com WORLD NEU
military environment after surgery, with intense physical
trainingand duties.It is difficult to predict the outcomes for
patients in both groups
in the next 10�20 years. However, we would expect lower rates
ofdegeneration and recurrence in the PELD group given its
relativelyminimally invasive approach. Studies with longer
follow-up pe-riods are needed to address this question.
Comparison of Radiologic OutcomesMany previous studies have
measured the DSCSA to evaluate theseverity of spinal stenosis.20-22
However, the relationship betweenthe DSCSA and clinical symptoms
has been uncertain, with poorcorrelation in most published
studies.21,22 In addition, to the bestof our knowledge, there has
been no study that has used theDSCSA to evaluate the extent of
decompression in LDH. Becausethere is as of yet no alternative
measurement technique to assessthe extent of decompression, we used
the DSCSA to measure theexpansion ratio of the dural sac. Despite
improvements in theDSCSA after surgery in both groups, there were
no statisticallysignificant differences between the groups. We did
not investigatethe correlation of the DSCSA to clinical outcomes
because we onlywanted to assess the amount of decompression between
the 2groups. To compare the extent of decompression in LDH as
wellas its clinical correlations, advancements in measurement
tech-niques are necessary.
Comparison of Perioperative OutcomesThe mean operative time in
the PELD group was significantlyshorter than that of the OLM group.
Blood loss was not meas-ureable in the PELD group and was
negligible in the OLM group.Despite the fact that the mean
operative time in our study waslonger than previously reported
times, the intergroup results weresimilar.18
Comparison of ComplicationsAlthough the published complication
rate for PELD was lowerthan that for OLM,13,18,23 there were 4
complications after PELD(12.5%) and 4 complications after OLM
(11.8%) in the presentstudy. Like any other technique, PELD has its
own learning curve.Most of the complications in the PELD group,
such as transientdysesthesia and intraprocedure headache, occurred
in the earlyphases of the study. Sairyo et al.24 reported that an
elevation inintracranial pressure may occur if the irrigation
pressure is toohigh or if the endoscopic maneuvers take too long.
In thepresent case, one patient complained of headache
duringsurgery and also had the longest operative time in our
study’searly phases.Choi et al.11 reported that the working sheath
may compress the
exiting root during surgery, and thus a prolonged operation
timemay contribute to nerve irritation. In the present study,
weexperienced2 such cases, both of which also occurred in theearly
phases. In addition, there was 1 case of a
symptomaticpostdiscectomy pseudocyst after PELD. Kang and
Park25
reported that symptomatic postdiscectomy pseudocyst wasdetected
within 2 months postoperatively in about 1% of cases.The authors
suggested that there was no difference in treatmentoutcomes between
the surgical and conservative management ofsymptomatic pseudocysts.
The pseudocyst in the present study
ROSURGERY, http://dx.doi.org/10.1016/j.wneu.2015.09.047
www.sciencedirect.com/science/journal/18788750http://dx.doi.org/10.1016/j.wneu.2015.09.047
-
ORIGINAL ARTICLE
SANG-SOAK AHN ET AL. PELD VERSUS OLM FOR YOUNG ADULTS
was detected at 2 months postoperatively, and slowly
improvedafter epidural injection. Although the complication rates
in bothgroups were greater than those described in previous
studies,there were no major complications.13,18 These results
showedthat with proper patient selection, PELD is a safe and
effectiveprocedure after overcoming its learning curve.
Comparison of Hospital Stay and Return to WorkThe length of the
hospital stay and return-to-work time are veryimportant parameters
in the assessment of a patient’s quality oflife. Although the
relationship between these measures and apatient’s overall health
is uncertain, these factors may be related toimprovements in
patient outcome and productivity by reducingthe duration of their
disability.6 In the present study, similar to theresults of
previous studies,13,17-19 the mean hospital stay in thePELD group
was shorter than that of the OLM group. However,the mean hospital
stays for the patients in both the PELD andOLM groups were longer
than those reported in previousstudies.13,18 This may have occurred
because all patients wereactive young men who were required to
maintain weight standardsand physical readiness even though they
had recently undergonesurgery, and therefore, the hospital stay in
the present study mayhave included some period of time even after
the relief fromsymptoms. In the present study, similar to the
results of previousstudies, the mean return-to-work time for the
PELD group wasshorter than that for the OLM group.13,17-19
Comparison of Operation Failures and RecurrencesAs previously
described, incomplete removal of the target frag-ment occurred in 2
patients in the PELD group, which we regardedas surgical failures.
All of these cases occurred in the early phasesof our study and may
be the result of technical limitations. Nopatients underwent
reoperation due to patient preference andwere instead managed with
conservative treatment. We hypothe-sized that the recurrence rate
in young patients would be greaterthan those reported in previous
studies; however, 12-month discreherniation was only observed in 1
case (3.1%) in the PELD groupand 1 case (2.9%) in the OLM group, a
rate comparable with thosereported in a previous study (5.7% and
6.6% for PELD and OLM,respectively).18 In previous studies, a large
annular defect inpatients in the OLM group resulted in
significantly greater ratesof recurrence than smaller or covered
defects.18,26,27 However, inthe present study, sequestrotomy with
partial extirpation wasperformed in OLM cases involving small or
covered annular de-fects. Therefore, we could not examine the
relationship between
WORLD NEUROSURGERY 86: 250-258, FEBRUARY 2016
the sizes of the annular defects and the clinical outcomes.
Leeet al.4 hypothesized that their study’s relatively high
reherniationrate may be attributable to limited target
fragmentectomy in thePELD group. In the present study, we could not
only remove thetarget fragment but also the central fragment using
an “in-and-out-and-in” technique. Through this technique, we could
checkon the target fragment while re-introducing a working
channelfrom the lateral to medial area after removal of the
PLL.
LimitationsIt is important to note that the present study has
several limita-tions. First, it was a retrospective matched cohort
study with asmall sample size (32 and 34 patients for the PELD and
OLMgroups, respectively), short follow-up periods (1 year),
limitedoperative levels (L4�5), and limited indications (excluding
harddiscs and foraminal/extraforaminal disc herniations). To
investi-gate the efficacy of the surgical methods, prospective
randomizednoninferiority or superiority studies are necessary.
Second, thestudy participants were limited to men who were
recruited from anarmed forces hospital. Because this study was
conducted in alimited population, statistical analysis was
difficult because of anon-normal distribution, and this study’s
conclusions might notbe valid for general populations. However,
because this studyincluded a homogeneous population of young
patients from anarmed forces hospital, we could reduce selection
bias and per-formance bias. In addition, because we could match
several fac-tors (sex, age, height, weight, body mass index, and
tobaccosmoking) between the 2 groups, we could also reduce
confound-ing bias. However, prospective double-arm parallel studies
withlonger follow-up times and larger sample sizes are necessary
toprovide more useful information on the outcomes of PELD andOLM
for LDH.
CONCLUSION
In our opinion, the use of PELD in young adults has several
ad-vantages, including: (1) a simpler surgical procedure due to
theavailability of local anesthesia, a short operative time, and a
shorthospital stay; (2) more efficacy for back pain and quality of
life ascompared to OLM, especially in active patients; and (3) a
relativelylow recurrence rate, even in patients undergoing intense
physicalactivity. Although surgeons need to overcome a learning
curve tobecome familiar with PELD, the procedure seems to be a
goodchoice for the treatment of LDH in young and active
patients.
REFERENCES
1. Dewing CB, Provencher MT, Riffenburgh RH,Kerr S, Manos RE.
The outcomes of lumbarmicrodiscectomy in a young, active
population:correlation by herniation type and level. Spine(Phila Pa
1976). 2008;33:33-38.
2. Kumar R, Kumar V, Das NK, Behari S,Mahapatra AK. Adolescent
lumbar disc disease:findings and outcome. Childs Nerv Syst.
2007;23:1295-1299.
3. Lagerback T, Elkan P, Moller H, Grauers A,Diarbakerli E,
Gerdhem P. An observational studyon the outcome after surgery for
lumbar discherniation in adolescents compared with adultsbased on
the Swedish Spine Register. Spine J. 2015;15:1241-1247.
4. Lee DY, Ahn Y, Lee SH. Percutaneous endo-scopic lumbar
discectomy for adolescent lumbardisc herniation: surgical outcomes
in 46consecutive patients. Mt Sinai J Med. 2006;73:864-870.
ww
5. Wang H, Cheng J, Xiao H, Li C, Zhou Y.Adolescent lumbar disc
herniation: experiencefrom a large minimally invasive treatment
centrefor lumbar degenerative disease in Chongqing,China. Clin
Neurol Neurosurg. 2013;115:1415-1419.
6. Angevine PD, McCormick PC. Outcomes researchand lumbar
discectomy. Neurosurg Focus. 2002;13:E8.
7. Casal-Moro R, Castro-Menendez M, Hernandez-Blanco M,
Bravo-Ricoy JA, Jorge-Barreiro FJ.Long-term outcome after
microendoscopic dis-kectomy for lumbar disk herniation: a
prospective
w.WORLDNEUROSURGERY.org 257
http://refhub.elsevier.com/S1878-8750(15)01210-3/sref1http://refhub.elsevier.com/S1878-8750(15)01210-3/sref1http://refhub.elsevier.com/S1878-8750(15)01210-3/sref1http://refhub.elsevier.com/S1878-8750(15)01210-3/sref1http://refhub.elsevier.com/S1878-8750(15)01210-3/sref1http://refhub.elsevier.com/S1878-8750(15)01210-3/sref2http://refhub.elsevier.com/S1878-8750(15)01210-3/sref2http://refhub.elsevier.com/S1878-8750(15)01210-3/sref2http://refhub.elsevier.com/S1878-8750(15)01210-3/sref2http://refhub.elsevier.com/S1878-8750(15)01210-3/sref3http://refhub.elsevier.com/S1878-8750(15)01210-3/sref3http://refhub.elsevier.com/S1878-8750(15)01210-3/sref3http://refhub.elsevier.com/S1878-8750(15)01210-3/sref3http://refhub.elsevier.com/S1878-8750(15)01210-3/sref3http://refhub.elsevier.com/S1878-8750(15)01210-3/sref3http://refhub.elsevier.com/S1878-8750(15)01210-3/sref4http://refhub.elsevier.com/S1878-8750(15)01210-3/sref4http://refhub.elsevier.com/S1878-8750(15)01210-3/sref4http://refhub.elsevier.com/S1878-8750(15)01210-3/sref4http://refhub.elsevier.com/S1878-8750(15)01210-3/sref4http://refhub.elsevier.com/S1878-8750(15)01210-3/sref5http://refhub.elsevier.com/S1878-8750(15)01210-3/sref5http://refhub.elsevier.com/S1878-8750(15)01210-3/sref5http://refhub.elsevier.com/S1878-8750(15)01210-3/sref5http://refhub.elsevier.com/S1878-8750(15)01210-3/sref5http://refhub.elsevier.com/S1878-8750(15)01210-3/sref6http://refhub.elsevier.com/S1878-8750(15)01210-3/sref6http://refhub.elsevier.com/S1878-8750(15)01210-3/sref7http://refhub.elsevier.com/S1878-8750(15)01210-3/sref7http://refhub.elsevier.com/S1878-8750(15)01210-3/sref7http://refhub.elsevier.com/S1878-8750(15)01210-3/sref7http://www.WORLDNEUROSURGERY.org
-
ORIGINAL ARTICLE
SANG-SOAK AHN ET AL. PELD VERSUS OLM FOR YOUNG ADULTS
clinical study with a 5-year follow-up.
Neurosurgery.2011;68:1568-1575; discussion 1575.
8. Perez-Cruet MJ, Foley KT, Isaacs RE, Rice-Wyllie L,
Wellington R, Smith MM, et al. Micro-endoscopic lumbar discectomy:
technical note.Neurosurgery. 2002;51:S129-136.
9. Wenger M, Mariani L, Kalbarczyk A, Groger U.Long-term outcome
of 104 patients after lumbarsequestrectomy according to Williams.
Neurosur-gery. 2001;49:329-334; discussion 334e325.
10. Hirabayashi S, Kumano K, Ogawa Y, Aota Y,Maehiro S.
Microdiscectomy and second opera-tion for lumbar disc herniation.
Spine (Phila Pa1976). 1993;18:2206-2211.
11. Choi I, Ahn JO, So WS, Lee SJ, Choi IJ, Kim H.Exiting root
injury in transforaminal endoscopicdiscectomy: preoperative image
considerations forsafety. Eur Spine J. 2013;22:2481-2487.
12. Gempt J, Jonek M, Ringel F, Preuss A, Wolf P,Ryang Y.
Long-term follow-up of standardmicrodiscectomy versus minimal
access surgeryfor lumbar disc herniations. Acta Neurochir
(Wien).2013;155:2333-2338.
13. Kim MJ, Lee SH, Jung ES, Son BG, Choi ES,Shin JH, et al.
Targeted percutaneous trans-foraminal endoscopic diskectomy in 295
patients:comparison with results of microscopic dis-kectomy. Surg
Neurol. 2007;68:623-631.
14. Lee DY, Shim CS, Ahn Y, Choi YG, Kim HJ,Lee SH. Comparison
of percutaneous endoscopiclumbar discectomy and open lumbar
micro-discectomy for recurrent disc herniation. J KoreanNeurosurg
Soc. 2009;46:515-521.
15. Lee SH, Chung SE, Ahn Y, Kim TH, Park JY,Shin SW.
Comparative radiologic evaluation ofpercutaneous endoscopic lumbar
discectomy and
258 www.SCIENCEDIRECT.com
open microdiscectomy: a matched cohort analysis.Mt Sinai J Med.
2006;73:795-801.
16. Peng CW, Yeo W, Tan SB. Percutaneous endo-scopic discectomy:
clinical results and how it af-fects the quality of life. J Spinal
Disord Tech. 2010;23:425-430.
17. Rasouli MR, Rahimi-Movaghar V, Shokraneh F,Moradi-Lakeh M,
Chou R. Minimally invasivediscectomy versus microdiscectomy/open
dis-cectomy for symptomatic lumbar disc herniation.Cochrane
Database Syst Rev. 2014;9:CD010328.
18. Ruetten S, Komp M, Merk H, Godolias G. Full-endoscopic
interlaminar and transforaminal lum-bar discectomy versus
conventional microsurgicaltechnique: a prospective, randomized,
controlledstudy. Spine (Phila Pa 1976). 2008;33:931-939.
19. Mayer HM, Brock M. Percutaneous endoscopicdiscectomy:
surgical technique and preliminaryresults compared to microsurgical
discectomy.J Neurosurg. 1993;78:216-225.
20. Hermansen E, Moen G, Barstad J, Birketvedt R,Indrekvam K.
Laminarthrectomy as a surgicalapproach for decompressing the spinal
canal:assessment of preoperative versus postoperativedural sac
cross-sectional areal (DSCSA). Eur SpineJ. 2013;22:1913-1919.
21. Lohman CM, Tallroth K, Kettunen JA,Lindgren KA. Comparison
of radiologic signs andclinical symptoms of spinal stenosis. Spine
(PhilaPa 1976). 2006;31:1834-1840.
22. Sirvanci M, Bhatia M, Ganiyusufoglu KA,Duran C, Tezer M,
Ozturk C, et al. Degenerativelumbar spinal stenosis: correlation
with OswestryDisability Index and MR imaging. Eur Spine
J.2008;17:679-685.
WORLD NEUROSURGERY, http://
23. Pan L, Zhang P, Yin Q. Comparison of tissuedamages caused by
endoscopic lumbar dis-cectomy and traditional lumbar discectomy:
arandomised controlled trial. Int J Surg. 2014;12:534-537.
24. Sairyo K, Matsuura T, Higashino K, Sakai T,Takata Y, Goda Y,
et al. Surgery related compli-cations in percutaneous endoscopic
lumbar dis-cectomy under local anesthesia. J Med Invest.
2014;61:264-269.
25. Kang SH, Park SW. Symptomatic post-discectomypseudocyst
after endoscopic lumbar discectomy.J Korean Neurosurg Soc.
2011;49:31-36.
26. Carragee EJ, Han MY, Suen PW, Kim D. Clinicaloutcomes after
lumbar discectomy for sciatica: theeffects of fragment type and
anular competence.J Bone Joint Surg Am. 2003;85-A:102-108.
27. Yorimitsu E, Chiba K, Toyama Y, Hirabayashi K.Long-term
outcomes of standard discectomy forlumbar disc herniation: a
follow-up study of morethan 10 years. Spine (Phila Pa 1976).
2001;26:652-657.
Conflict of interest statement: The authors declare that
thearticle content was composed in the absence of anycommercial or
financial relationships that could be construedas a potential
conflict of interest.
Received 2 July 2015; accepted 15 September 2015
Citation: World Neurosurg. (2016)
86:250-258.http://dx.doi.org/10.1016/j.wneu.2015.09.047
Journal homepage: www.WORLDNEUROSURGERY.org
Available online: www.sciencedirect.com
1878-8750/$ - see front matter ª 2016 Elsevier Inc.All rights
reserved.
dx.doi.org/10.1016/j.wneu.2015.09.047
http://refhub.elsevier.com/S1878-8750(15)01210-3/sref7http://refhub.elsevier.com/S1878-8750(15)01210-3/sref7http://refhub.elsevier.com/S1878-8750(15)01210-3/sref8http://refhub.elsevier.com/S1878-8750(15)01210-3/sref8http://refhub.elsevier.com/S1878-8750(15)01210-3/sref8http://refhub.elsevier.com/S1878-8750(15)01210-3/sref8http://refhub.elsevier.com/S1878-8750(15)01210-3/sref9http://refhub.elsevier.com/S1878-8750(15)01210-3/sref9http://refhub.elsevier.com/S1878-8750(15)01210-3/sref9http://refhub.elsevier.com/S1878-8750(15)01210-3/sref9http://refhub.elsevier.com/S1878-8750(15)01210-3/sref9http://refhub.elsevier.com/S1878-8750(15)01210-3/sref10http://refhub.elsevier.com/S1878-8750(15)01210-3/sref10http://refhub.elsevier.com/S1878-8750(15)01210-3/sref10http://refhub.elsevier.com/S1878-8750(15)01210-3/sref10http://refhub.elsevier.com/S1878-8750(15)01210-3/sref11http://refhub.elsevier.com/S1878-8750(15)01210-3/sref11http://refhub.elsevier.com/S1878-8750(15)01210-3/sref11http://refhub.elsevier.com/S1878-8750(15)01210-3/sref11http://refhub.elsevier.com/S1878-8750(15)01210-3/sref12http://refhub.elsevier.com/S1878-8750(15)01210-3/sref12http://refhub.elsevier.com/S1878-8750(15)01210-3/sref12http://refhub.elsevier.com/S1878-8750(15)01210-3/sref12http://refhub.elsevier.com/S1878-8750(15)01210-3/sref12http://refhub.elsevier.com/S1878-8750(15)01210-3/sref13http://refhub.elsevier.com/S1878-8750(15)01210-3/sref13http://refhub.elsevier.com/S1878-8750(15)01210-3/sref13http://refhub.elsevier.com/S1878-8750(15)01210-3/sref13http://refhub.elsevier.com/S1878-8750(15)01210-3/sref13http://refhub.elsevier.com/S1878-8750(15)01210-3/sref14http://refhub.elsevier.com/S1878-8750(15)01210-3/sref14http://refhub.elsevier.com/S1878-8750(15)01210-3/sref14http://refhub.elsevier.com/S1878-8750(15)01210-3/sref14http://refhub.elsevier.com/S1878-8750(15)01210-3/sref14http://refhub.elsevier.com/S1878-8750(15)01210-3/sref15http://refhub.elsevier.com/S1878-8750(15)01210-3/sref15http://refhub.elsevier.com/S1878-8750(15)01210-3/sref15http://refhub.elsevier.com/S1878-8750(15)01210-3/sref15http://refhub.elsevier.com/S1878-8750(15)01210-3/sref15http://refhub.elsevier.com/S1878-8750(15)01210-3/sref16http://refhub.elsevier.com/S1878-8750(15)01210-3/sref16http://refhub.elsevier.com/S1878-8750(15)01210-3/sref16http://refhub.elsevier.com/S1878-8750(15)01210-3/sref16http://refhub.elsevier.com/S1878-8750(15)01210-3/sref17http://refhub.elsevier.com/S1878-8750(15)01210-3/sref17http://refhub.elsevier.com/S1878-8750(15)01210-3/sref17http://refhub.elsevier.com/S1878-8750(15)01210-3/sref17http://refhub.elsevier.com/S1878-8750(15)01210-3/sref17http://refhub.elsevier.com/S1878-8750(15)01210-3/sref18http://refhub.elsevier.com/S1878-8750(15)01210-3/sref18http://refhub.elsevier.com/S1878-8750(15)01210-3/sref18http://refhub.elsevier.com/S1878-8750(15)01210-3/sref18http://refhub.elsevier.com/S1878-8750(15)01210-3/sref18http://refhub.elsevier.com/S1878-8750(15)01210-3/sref19http://refhub.elsevier.com/S1878-8750(15)01210-3/sref19http://refhub.elsevier.com/S1878-8750(15)01210-3/sref19http://refhub.elsevier.com/S1878-8750(15)01210-3/sref19http://refhub.elsevier.com/S1878-8750(15)01210-3/sref20http://refhub.elsevier.com/S1878-8750(15)01210-3/sref20http://refhub.elsevier.com/S1878-8750(15)01210-3/sref20http://refhub.elsevier.com/S1878-8750(15)01210-3/sref20http://refhub.elsevier.com/S1878-8750(15)01210-3/sref20http://refhub.elsevier.com/S1878-8750(15)01210-3/sref20http://refhub.elsevier.com/S1878-8750(15)01210-3/sref21http://refhub.elsevier.com/S1878-8750(15)01210-3/sref21http://refhub.elsevier.com/S1878-8750(15)01210-3/sref21http://refhub.elsevier.com/S1878-8750(15)01210-3/sref21http://refhub.elsevier.com/S1878-8750(15)01210-3/sref22http://refhub.elsevier.com/S1878-8750(15)01210-3/sref22http://refhub.elsevier.com/S1878-8750(15)01210-3/sref22http://refhub.elsevier.com/S1878-8750(15)01210-3/sref22http://refhub.elsevier.com/S1878-8750(15)01210-3/sref22http://refhub.elsevier.com/S1878-8750(15)01210-3/sref23http://refhub.elsevier.com/S1878-8750(15)01210-3/sref23http://refhub.elsevier.com/S1878-8750(15)01210-3/sref23http://refhub.elsevier.com/S1878-8750(15)01210-3/sref23http://refhub.elsevier.com/S1878-8750(15)01210-3/sref23http://refhub.elsevier.com/S1878-8750(15)01210-3/sref24http://refhub.elsevier.com/S1878-8750(15)01210-3/sref24http://refhub.elsevier.com/S1878-8750(15)01210-3/sref24http://refhub.elsevier.com/S1878-8750(15)01210-3/sref24http://refhub.elsevier.com/S1878-8750(15)01210-3/sref24http://refhub.elsevier.com/S1878-8750(15)01210-3/sref25http://refhub.elsevier.com/S1878-8750(15)01210-3/sref25http://refhub.elsevier.com/S1878-8750(15)01210-3/sref25http://refhub.elsevier.com/S1878-8750(15)01210-3/sref26http://refhub.elsevier.com/S1878-8750(15)01210-3/sref26http://refhub.elsevier.com/S1878-8750(15)01210-3/sref26http://refhub.elsevier.com/S1878-8750(15)01210-3/sref26http://refhub.elsevier.com/S1878-8750(15)01210-3/sref27http://refhub.elsevier.com/S1878-8750(15)01210-3/sref27http://refhub.elsevier.com/S1878-8750(15)01210-3/sref27http://refhub.elsevier.com/S1878-8750(15)01210-3/sref27http://refhub.elsevier.com/S1878-8750(15)01210-3/sref27http://dx.doi.org/10.1016/j.wneu.2015.09.047http://www.WORLDNEUROSURGERY.orgwww.sciencedirect.com/science/journal/18788750www.sciencedirect.com/science/journal/18788750http://dx.doi.org/10.1016/j.wneu.2015.09.047
-
本文献由“学霸图书馆-文献云下载”收集自网络,仅供学习交流使用。
学霸图书馆(www.xuebalib.com)是一个“整合众多图书馆数据库资源,
提供一站式文献检索和下载服务”的24 小时在线不限IP
图书馆。
图书馆致力于便利、促进学习与科研,提供最强文献下载服务。
图书馆导航:
图书馆首页 文献云下载 图书馆入口 外文数据库大全 疑难文献辅助工具
http://www.xuebalib.com/cloud/http://www.xuebalib.com/http://www.xuebalib.com/cloud/http://www.xuebalib.com/http://www.xuebalib.com/vip.htmlhttp://www.xuebalib.com/db.phphttp://www.xuebalib.com/zixun/2014-08-15/44.htmlhttp://www.xuebalib.com/
Comparison of Outcomes of Percutaneous Endoscopic Lumbar
Discectomy and Open Lumbar Microdiscectomy for Young Adults: A Ret
...IntroductionMaterials and MethodsStudy DesignClinical
AssessmentRadiologic AssessmentSurgical ProcedureStatistics
ResultsDemographicsClinical OutcomesRadiologic
OutcomesPerioperative OutcomesComplicationsOperation Failures and
Recurrences
DiscussionComparison of Clinical OutcomesComparison of
Radiologic OutcomesComparison of Perioperative OutcomesComparison
of ComplicationsComparison of Hospital Stay and Return to
WorkComparison of Operation Failures and RecurrencesLimitations
ConclusionReferences