Embed Size (px)
Citation preview

RESEARCH ARTICLE Open Access
Compassion fatigue and compassionsatisfaction among palliative care healthproviders: a scoping reviewManal Hassan Baqeas* , Jenny Davis and Beverley Copnell
Abstract
Background: Palliative care can be demanding and stressful for providers. There is increasing recognition in theliterature of the impact of caregiving in palliative care settings, including compassion fatigue and compassionsatisfaction. However, to date this literature has not been systematically reviewed. The purpose of this scopingreview was to map the literature on compassion fatigue and compassion satisfaction among palliative care healthproviders caring for adult patients.
Methods: Scoping review method guided by Joanna Briggs Institute guidelines was conducted using fourelectronic databases to identify the relevant studies published with no time limit. Following the title and abstractreview, two reviewers independently screened full-text articles, and extracted study data. A narrative approach tosynthesizing the literature was used.
Results: Twenty studies were included in the review. Five themes emerged from synthesis: conceptualisation ofcompassion fatigue and compassion satisfaction; measurement of compassion fatigue and compassion satisfaction;consequences of compassion fatigue or compassion satisfaction and providing care for patients with life-threateningconditions; predictors or associated factors of compassion fatigue and compassion satisfaction among palliative care healthproviders; and strategies or interventions to support palliative care health providers and reduce compassion fatigue.
Conclusions: Limited studies examined the effectiveness of specific interventions to improve compassion satisfaction andreduce compassion fatigue among palliative care health providers. Further investigation of the impacts of compassionfatigue and compassion satisfaction on palliative care health providers and their work is also needed.
Keywords: Compassion fatigue, Compassion satisfaction, Palliative care, Palliative care health providers, Scoping review
BackgroundPalliative care aims to support people with life-threateningconditions and improve their quality of life [1]. Palliativecare health providers (PCHP) comprise medical, nursing,and allied health care professionals who work in palliativecare settings and who have specific knowledge, skills, andexpertise in providing care for people living with a life lim-iting illness and their families. PCHP can provide direct
care in various settings such as dedicated hospital wards,hospices, and community, and through consultancy to pa-tients in other areas [2].Prolonged contact with these patients predisposes
PCHP to emotional and psychological distress such ascompassion fatigue. There are various definitions ofcompassion fatigue documented in the literature. In gen-eral, compassion fatigue is a term used to describe theexhaustion that results from prolonged exposure tocompassion stress among those who work in a caringprofession [3]. Compassion fatigue is also described as
© The Author(s). 2021 Open Access This article is licensed under a Creative Commons Attribution 4.0 International License,which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you giveappropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate ifchanges were made. The images or other third party material in this article are included in the article's Creative Commonslicence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commonslicence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtainpermission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to thedata made available in this article, unless otherwise stated in a credit line to the data.
* Correspondence: [email protected] of Nursing and Midwifery, La Trobe University, Bundoora, VIC 3086,Australia
Baqeas et al. BMC Palliative Care (2021) 20:88 https://doi.org/10.1186/s12904-021-00784-5

the diminished ability to feel compassion or empathizewhen providing care. In contrast, compassion satisfac-tion is related to the pleasure derived from alleviation ofpatient suffering and positive work experience [4]. Thereis no consensus in the literature on the dimensions orcomponents of compassion fatigue. However, there is ageneral agreement that compassion fatigue is related toboth burnout (BO) and secondary traumatic stress(STS). While STS is very closely related to compassionfatigue, the nature of the relationship is defined differ-ently and both terms used interchangeably by some au-thors [4]. The concept of compassion satisfaction isrelated to positive work experience, whereas compassionfatigue is associated with physical and emotional exhaus-tion, caused by constant, progressive, and cumulativenegative experiences associated with various clinical set-tings [3, 5, 6]. Compassion fatigue has negative impactson job satisfaction and patient outcomes [7–9]. This em-phasizes the significance of investigating compassion fa-tigue in PCHP.To date, compassion fatigue has been widely studied
in health care providers in a range of settings, as synthe-sized in a recent meta-narrative review [10]. However, toour knowledge, no such synthesis has been undertakenof literature pertaining specifically to PCHP. This gap inthe literature makes it difficult to identify and implementinterventions to support these workers. Therefore, theaim of this scoping review is to synthesize findings fromextant research about compassion fatigue and compas-sion satisfaction among PCHP.
MethodsThe scoping review, as a method, is suitable when thestudy topic is abstract, broad, emerging, or multi-dimensional [11]. Scoping reviews are used to answer abroad question such as “what is known about the studyconcepts?” [11]. It was, therefore, deemed suitable to ad-dress the aim of the current study. It answers the re-search question through a narrative synthesis of theliterature. In addition, it is used to summarize thecurrent knowledge about a topic and identify knowledgegaps regardless of the quality of reviewed studies andtheir design [11].The current scoping review was conducted based on
the guidelines published by the Joanna Briggs Institute(JBI) [12]. These guidelines were developed based on theprevious work by Arksey and O’Malley [13] and Levac,Colquhoun, and O’Brien [14]. In addition, the literaturereview followed the PRISMA-ScR checklist to provideclear details of the search protocol and enhance meth-odological transparency [11]. As per the Joanna BriggsInstitute guidelines, the following five stages werefollowed: 1. Identifying the research question 2. Identify-ing relevant studies 3. Selection of relevant studies 4.
Charting the data 5. Collating, summarizing and report-ing the results [12]. There is a sixth (optional) step thatincludes consultation with key stakeholders. This stepwas omitted, however, and only evidence published inpeer-reviewed literature was included.
Stage 1. Identifying the research questionThis review aims to identify what is known about com-passion fatigue and compassion satisfaction amongPCHP. To address the study aim, the review was con-ducted to answer the following question: “what researchhas been undertaken on compassion fatigue and com-passion satisfaction among palliative care healthproviders?”
Stage 2. Identifying relevant publicationsThe review was conducted by a team of researchers in-cluding the primary researcher, content experts, andmethodological experts. A search of four electronic data-bases: MEDLINE (OVID), CINAHL, PsycInfo, andEMBASE was conducted in August 2019. To ensure acomprehensive search, the search terms “compassion fa-tigue”, “compassion satisfaction”, and “palliative carehealth providers” were initially kept broad and then ex-ploded to cover MeSH terms. In addition, keywords in-cluded in the title and abstract of retrieved papers, andthe keywords used to describe the articles were identi-fied. These keywords were searched across the databases.Finally, the reference lists of the selected articles werehand searched to identify additional studies. The terms“compassion fatigue”, “compassion satisfaction”, and“palliative care health providers” were combined withthe following terms: “burnout, professional”, “stress dis-orders, post-traumatic”, “fatigue, compassion”, “second-ary trauma”, “secondary traumatic stress”, “secondarytraumatization”, “trauma, vicarious”, “traumas, second-ary”, “traumatic stress, secondary”, “burnout, career’,“burnout, occupational”, “burnout, professional”, “sec-ondary post-traumatic stress”, “hospice professionals”,“hospice, palliative care nursing”, “palliative care”, “pal-liative medicine”, “terminal care”, “palliative supportivecare”, and “palliative treatment”. The Boolean operators‘AND’ and ‘OR’ were used to combine various terms andconcepts. All identified sources were stored in the End-Note reference program. Irrelevant records and dupli-cates were excluded from the literature search. The finalscreening of title/abstract and then full text was man-aged in Covidence.Inclusion criteria were: 1. all research designs (e.g.,
quantitative, qualitative, mixed methods, and systematicreviews); 2. addressing compassion fatigue and compas-sion satisfaction from the perspectives of PCHP caringfor adult patients in any practice setting; 3. published inEnglish with no date limits applied. Exclusion criteria
Baqeas et al. BMC Palliative Care (2021) 20:88 Page 2 of 13

were: 1. grey literature (e.g., book chapters, theses, re-ports, and conference abstracts); 2. Non-research publi-cations (eg editorials; discussion papers; opinion pieces);3. targeting volunteers working in palliative care settings;4. investigating BO without STS or Compassion Fatigue;5. focusing on PCHP working with pediatric patients aswe consider pediatric palliative care has distinct differ-ences from adult palliative care and can be considered aspeciality in its own right [15].
Stage 3. Publication selectionAfter removal of duplicates, article titles and abstractswere screened by two researchers independently. Dis-agreements were discussed and resolved by consensusamong the research team. After full text screening, stud-ies meeting all inclusion criteria were included in thefinal review.
Stage 4. Charting the dataA data extraction table was used to extract the data fromthe included studies. Extracted data included country,year of publication, names of authors, study purpose, re-search design, study sample, and main study findings.The data extraction was conducted by one researcherand reviewed by the research team. Any disagreementsin data extraction were resolved by consensus. Refer-ences were managed utilising EndNote (version X9) andincluded studies were imported to Covidence during thefinal screening. In line with the PRISMA-ScR standards[11], no formal quality appraisal was undertaken as itwas not intended to exclude any paper based on qualityassessment.
Stage 5 data synthesisNarrative synthesis was employed due to the heterogen-eity of the studies. The characteristics of the reviewedstudies (i.e design, sample, settings, main variables, andpublication year) were collated and summarized. Studieswere summarized in a Table and a content analysis wasperformed based on the tabulated data. Then, contentswere translated into main themes. Lastly, the findingswere interpreted and compared with studies from othersettings.
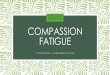
ResultsOverall, the initial search yielded 1822 records. After re-moving duplicates, 1085 records were screened for po-tential relevance by title and abstract. Of these, 921records were found to be irrelevant and 164 full-text ar-ticles were screened. Finally, 144 articles were excludedand 20 articles were included in the final review (Fig. 1).Studies were conducted in different countries worldwide,the majority in a Western setting. Countries representedwere: United States (n = 9), Spain (n = 3), Israel (n = 3),
with one study from each of Australia, Canada, NewZealand, and India. The majority of the studies werepublished within the last 5 years (n = 15). More than halfof the studies were correlational (n = 10), four studieswere qualitative, one a quantitative descriptive study,one a pre-post study with control group, one pre-postwith no control group, two studies examined the psy-chometric properties of the Professional Quality of Life(ProQOL) scale, one paper was a systematic review.Study populations included PCHP from several disci-plines (n = 14), only nurses (n = 3), or only physicians(n = 2).The samples in the included studies were recruited from
various settings that provide palliative care (Table 1). Onestudy was conducted in inpatient hospices and hospitals[20]. One study was conducted in inpatient hospices [21],one in outpatient hospices [1], and one in hospice settingswithout specifying whether inpatient or outpatient [22].One study was conducted in outpatient palliative care set-ting [24]. Eight studies included participants from both in-patient and outpatient settings including hospices [16, 18,19, 23, 28–30, 33]. However, the combination betweeninpatient and outpatient settings in these eight studieswas unclear and not described in detail. Six studiesincluded participants from settings that provide in-patient and outpatient services without stating specif-ically if all participants were recruited from inpatient,outpatient, or both [17, 25–27, 31, 32].
Themes extracted from the included studiesFive main themes were identified in the synthesis of theincluded studies: 1. conceptualisation of compassion fa-tigue and compassion satisfaction; 2. measurement ofcompassion fatigue and satisfaction; 3. consequences ofcompassion fatigue or satisfaction and of providing carefor patients with life-threatening conditions; 4. predic-tors or associated factors of compassion fatigue and sat-isfaction among PCHP; 5. strategies or interventions tosupport PCHP and reduce compassion fatigue. Thesethemes are described further in the following sections.The summary of the included studies is shown inTable 1.
Theme 1- conceptualisation of compassion fatigueOverall, the reviewed studies did not discuss the concep-tualisation of compassion fatigue in depth. Their defin-ition was mainly embedded in that used by themeasurement tool and thus reflects changes in the con-cept over time. Compassion satisfaction was defined bysome studies as a positive consequence of providing carefor acutely ill or traumatised patients (e.g., a sense of ac-complishment and reward) [1, 18, 19, 22, 25, 30, 31].Some studies treated compassion fatigue as a singlediscrete entity with no constitutive components [1, 21].
Baqeas et al. BMC Palliative Care (2021) 20:88 Page 3 of 13

On the other hand, some studies treated compassion fa-tigue as being synonymous with STS, and these termswere used interchangeably [20, 31, 32]. The remainingstudies conceptualized compassion fatigue as having twodiscrete components (STS and BO), each of which wasmeasured separately [16, 18, 19, 22, 23, 25, 27–30]. Thequalitative studies did not specify a clear definition ofcompassion fatigue [17, 24, 26, 33].
Theme 2: measurement of compassion fatigue andsatisfactionThe measurement tools used to assess compassion fa-tigue and compassion satisfaction among PCHP in-cluded the 30-item professional quality of life scale(ProQOL) scale, the 20-item compassion fatigue scale(CFS), and the 13-item Compassion Fatigue Short-Scale.The various versions of the ProQOL reflect the changes
in conceptualisation described in the previous section.The ProQOL-V includes two domains of compassionfatigue (composed of BO and STS) and compassionsatisfaction. The ProQOL-IV measures three domains:compassion satisfaction, BO, and compassion fatigue/secondary trauma. The ProQOL-III measures threedomains: compassion satisfaction, BO, and compas-sion fatigue. The 20-item compassion fatigue scale(CFS) is a subscale of the 66-item Compassion Satis-faction/Fatigue Self-Test for Helpers which measurescompassion satisfaction, compassion fatigue, and BO.The 13-item Compassion Fatigue Short-Scale mea-sures compassion fatigue in two dimensions (second-ary trauma and job BO).The most commonly used measure of compassion fa-
tigue and compassion satisfaction among PCHP was theProQOL scale (III, IV, and V versions), which was used
Fig. 1 Flow diagram of search strategy
Baqeas et al. BMC Palliative Care (2021) 20:88 Page 4 of 13

Table
1SummaryTableof
Includ
edStud
ies
Autho
rs,Y
ear,an
dCou
ntry
Settings
Design
Sample
Research
Aim
sOutco
mes
Alkem
aet
al.[1],U
SAOutpatient
palliative
care
settings:hom
eho
spicesettings.
Quantitative(Cross
sectionalsurvey)
n=37
Hospice
Profession
als
includ
ing
17Registered
Nurse
5Hom
eHealth
Aide
4SocialWorker
2Vo
lunteerCoo
rdinator
3Bereavem
entProfession
al2Chaplain
1Adm
inistrativeAssistant
2Med
icalDirector
2Other.
Exam
inetherelatio
nships
amon
gself-care,com
passion
fatig
ue,com
passionsatisfac-
tion,andBO
amon
gho
spice
care
workers.
Self-care
strategies
were
associated
with
decreased
levelsof
compassionfatig
ueandBO
andhigh
erlevelsof
compassionsatisfaction.
Barnett,Ru
iz[16],U
SABo
thinpatient
and
outpatient
palliative
care
settings
Inpatient
–ho
spices,
hospitals,nursing
homes,other
long
-term
care
facilities,
Outpatient
–ho
me
healthcare.
Quantitative(Cross
sectionalsurvey)
90ho
spicenu
rses.
Tostud
ytheroleof
self-
esteem
inmed
iatin
gtherela-
tionshipbe
tweencompassion
fatig
ueandpsycho
logicald
is-
tressam
ongho
spicenu
rses.
Psycho
logicald
istresscan
decrease
self-esteem
,and
thereb
yincrease
theriskof
compassionfatig
ue.
Bessen
etal.[17],USA
Med
icalcentre
–un
ableto
determ
ine
ifinclud
esbo
thinpatient
and
outpatient
settings.
Qualitative(sem
i-structured
interviews)
13ph
ysicians.
Tode
scrib
ecompassionate
care
provisionby
physicians
durin
gen
d-of-life
care.
Therewerevariablewaysfor
deliveringcompassionate
care.
Physicians
need
training
inen
d-of-life
care
toovercome
somebarriersof
providing
care
onorganizatio
naland
in-
dividu
allevel.
Frey
etal.[18],New
Zealand
Inpatient
–ho
spital,
hospice,reside
ntial
aged
care,
Outpatient
–ho
spital,
commun
ityho
spice,
districtnu
rsing,
gene
ralp
ractice,
othe
rcommun
ityservices.
Quantitative(Cross
sectionalsurvey)
256registered
nurses.
ToinvestigateBO
and
compassionfatig
ueandtheir
associated
factorsam
ong
nurses
inNew
Zealand.
BOne
gativelyassociated
with
psycho
logicalempo
wermen
t&commitm
ent&challeng
ecompo
nentsof
psycho
logical
hardiness.STSne
gatively
associated
with
palliativecare
education.
Com
passionsatisfaction
positivelyassociated
with
palliativecare
education,
psycho
logicalempo
wermen
t,&bo
thcommitm
ent&
challeng
ecompo
nentsof
psycho
logicalh
ardine
ss.
Galiana
etal.[19],Braziland
Spain.
Inpatient
and
outpatient
palliative
care
settings
includ
ingho
spice
(Hom
e-based
Psycho
metrics
Brazil/
(n=161)
Spain/
(n=385)
PCHPinclud
ingdo
ctors,
nurses,p
sycholog
ists,nursing
assistants,socialw
orkersand
Toassess
thereliabilityand
validity
oftheSpanishandthe
Portug
uese
versions
ofthe
ProQ
OLscale.
Both
SpanishandPo
rtug
uese
versions
oftheProQ
OLshow
good
psycho
metric
prop
erties.
Baqeas et al. BMC Palliative Care (2021) 20:88 Page 5 of 13

Table
1SummaryTableof
Includ
edStud
ies(Con
tinued)
Autho
rs,Y
ear,an
dCou
ntry
Settings
Design
Sample
Research
Aim
sOutco
mes
palliativecare
Social-health
center
unitpalliativecare
Hospitalsup
port
team
Hospice
Oncolog
yun
itIntensivetreatm
ent
unit
Pediatricsun
itof
palliativecare
Others)
othe
r.(Individu
alproviders
numbe
rno
tspecified
)
Heeteret
al.[20],USA
Inpatient
hospiceand
hospitalp
alliative
care
settings
(Pre-Post)on
egrou
p36
Hospice
andPC
HP
includ
ingnu
rses,m
anagers
from
therespectiveho
me
hospiceandpalliativecare
units,p
hysicians,clerical,aides,
socialworkers,and
othe
rs.
(Individu
alprovidersnu
mbe
rno
tspecified
)
Exam
inetheeffectsof
6-week
techno
logy-assistedmed
itatio
nprog
ram
onem
otionalaware-
ness,com
passionfatig
ue,and
BO
The6-weektechno
logy-
assisted
med
itatio
ntechno
logy
successfullyredu
cedcompas-
sion
fatig
ue/BOandincreased
emotionalawaren
essam
ong
thestud
yparticipants.
Hillet
al.[10]
Vario
ussettings
System
aticReview
547PC
HPacross
9stud
ies
Toexploretheeffectiven
essof
interven
tions
used
toen
hance
psycho
logicalw
ellbeing
ofpalliativecare
staff.
Few
interven
tions
werehe
lpful
tosupp
ortpalliativecare
staff
andim
provetheirwell-b
eing
.
Hilliard
[21],U
SAInpatient
palliative
care
settings:hospice
Twogrou
pspre-po
st-
testgrou
pn=17
nurses,socialw
orkers,
andchaplains(Individu
alprovidersnu
mbe
rno
tspecified
)
Toexam
inetheeffectiven
ess
ofmusictherapyto
redu
cecompassionfatig
ueand
improveteam
buildingof
hospiceworkers.
Musictherapywas
effectiveto
improveteam
buildingbu
tno
tredu
cecompassion
fatig
ue.
Hotchkiss
[22],U
SAHospice
settings
from
VITA
S®Health
care
Quantitative(Cross
sectionalsurvey)
324Hospice
care
profession
als
includ
ing
68Registered
nurse
60Chaplain
48Socialworker
40Hom
ehe
alth
aid
28Licensed
vocatio
naln
urse
20Adm
inistrative
16Managem
ent
14Nurse
practitione
rs8Ph
ysician
4Musictherapists
18Other
Exam
inetherelatio
nship
betw
eencompassion
satisfaction,BO
,STS,and
mindful
self-care
Participantshadhigh
levelsof
self-care
andcompassionsatis-
factionandlow
levelsof
STS
andBO
.Self-carestrategies
canim
provecompassion
satisfaction.
Kaur
etal.[23],India
Inpatient
and
Outpatient
palliative
care
settings
includ
ingho
spice
(hospitaland
hospice
Quantitative(Cross
sectionalsurvey)
65PC
HPinclud
ingdo
ctor,
nurse,coun
selor,psycho
logist,
socialworker,ph
armacist,or
physiotherapist.(Individu
alnu
mbe
rno
tspecified
).
Toexploretheprofession
alqu
ality
oflifeam
ongPC
HP.
Theauthorsconclude
dthat
implem
entin
gspecific
interven
tions
couldbe
helpful
toredu
ceSTSandBO
and
enhancecompassion
Baqeas et al. BMC Palliative Care (2021) 20:88 Page 6 of 13

Table
1SummaryTableof
Includ
edStud
ies(Con
tinued)
Autho
rs,Y
ear,an
dCou
ntry
Settings
Design
Sample
Research
Aim
sOutco
mes
atcancer
palliative
care
centers)
satisfactionam
ongPC
HP.
Melvin[24],U
SAOutpatient
palliative
care
settings:hom
ehe
alth
agen
cy
Qualitative(sem
i-structured
interviews)
6palliativecare
nurses
Assessprevalen
ceof
compassionfatig
ue,its
conseq
uences,and
metho
dsof
coping
with
itam
ong
palliativecare
nurses.
Com
passionfatig
uehad
negativeph
ysicaland
emotionalh
ealth
impactson
palliativecare
nurses.
Mon
tross-Thom
aset
al.[25],
USA
Can
notde
term
ine
theparticipantswere
recruitedon
line
throug
ha
mem
bershiplist
serveof
theNational
Hospice
andPalliative
CareOrganization
(NHPC
O).All
participantswere
hospicestaffor
volunteerswho
were
emailedade
scrip
tion
ofthestud
yanda
Survey
Mon
keylink
Quantitative(Cross
sectionalsurvey)
390ho
spicestaffand
volunteers(Individu
alprovidersno
tspecified
)
Toinvestigatetheroleof
practicingritualsto
improve
profession
alqu
ality
oflife
amon
gho
spicecare
providers
Hospice
care
providerswho
practiceritualswerefoun
dto
have
better
profession
alqu
ality
oflife.
MotaVargas
etal.[26],
Spain
Can
notde
term
ine
(purpo
sefulsam
ple)
Qualitative(sem
i-structured
individu
alinterviews)
10PC
HPinclud
enu
rses,
doctorsandpsycho
logists.
Individu
alprovidersnu
mbe
rno
tspecified
).
Tode
scrib
eexpe
riences
ofpalliativecare
workersover
time
PCHPwerefoun
dto
gothroug
hvario
usph
ases
durin
gtheirprofession
allife.
O’Mahon
yet
al.[27],USA
Can
notde
term
ine
Participantswere
recruitedfro
ma
grou
pof
70profession
als
participatingin
acontinuing
education
prog
ram
onpalliative
med
icinein
Midwest
Acade
micMed
ical
Cen
ter
Quantitative(Cross
sectionalsurvey)
66PC
HPinclud
ingph
ysicians,
nurses,chaplains,social
workers,and
other.(Individu
alprovidersnu
mbe
rno
tspecified
)
Exam
inetherelatio
nship
betw
eenpe
rson
ality
traitsand
compassionfatig
uein
PCHP.
Neuroticism
was
associated
with
STSandBO
.Agreeablene
sswas
associated
with
compassionsatisfaction.
Expe
riencein
palliativecare
was
associated
with
lower
levelsof
BOandincreased
levelsof
compassion
satisfaction.
Samson,Shvartzm
an[28],
Israel
Both
inpatient
and
outpatient
palliative
care
settings
(hospital-b
ased
and/
orho
me-basedpallia-
tivecare
units)
Quantitative(Cross
sectionalsurvey)
144PC
HPinclud
ing
47Ph
ysicians
97Nurses
Toiden
tifytheassociation
betw
eenSTSand
peritraum
aticdissociatio
nam
ongpalliativeworkers.
STSwas
foun
dto
besign
ificantlycorrelated
with
clinicallevelsof
peritraum
atic
dissociatio
nam
ongpalliative
workers.
Samson,Shvartzm
an[29],
Israel
Both
inpatient
and
outpatient
palliative
care
settings
(end
-of-
Quantitative(Cross
sectionalsurvey)
241participantsproviding
palliativecare
andprim
ary
care
includ
ing
Toassess
therelatio
nship
betw
eenexpo
sure
tode
ath
anddyingandprofession
al
Therewas
asign
ificant
relatio
nshipbe
tweenexpo
sure
tode
athanddyingand
Baqeas et al. BMC Palliative Care (2021) 20:88 Page 7 of 13

Table
1SummaryTableof
Includ
edStud
ies(Con
tinued)
Autho
rs,Y
ear,an
dCou
ntry
Settings
Design
Sample
Research
Aim
sOutco
mes
lifecommun
ity-and
hospital-b
ased
pallia-
tivecare
units)
84Ph
ysician
157Nurse
quality
oflifein
PCHP
profession
alqu
ality
oflife
amon
gthestud
yparticipants.
Samsonet
al.[30],Israel
Both
inpatient
and
outpatient
palliative
care
settings
includ
ingho
spice
(hom
e-andho
spital-
basedho
spiceun
itsandof
prim
aryhe
alth
care
providers,work-
ingin
Clalit
Health
CareServices
and
Maccabi
Health
Care
Services
(the
twolar-
gesthe
alth
care
or-
ganizatio
nsin
Israel)
Quantitative
(psychom
etric
prop
erties)
1100
health
care
providers
Toassess
thereliabilityand
validity
oftheHeb
rew
version
ofthe30-item
ProQ
olscale
TheHeb
rew
versionof
the
compassionsatisfaction
subscalewas
foun
dto
show
good
psycho
metric
prop
erties
Sansóet
al.[31],Spain
Can
notde
term
ine
settings:m
embe
re-
maillistof
theSpan-
ishSocietyof
Pallia-
tiveCare
Quantitative(Cross
sectionalsurvey)
387PC
HPinclud
edo
ctors,
nurses,p
sycholog
ists,nursing
assistants,socialw
orkers.
(Individu
alprovidersnu
mbe
rno
tspecified
)
Toassess
therelatio
nships
amon
gSelf-Care,Awaren
ess,
profession
alqu
ality
oflife,and
Cop
ingwith
Death
amon
gPC
HP.
Therewas
asign
ificant
relatio
nshipam
ongthestud
yvariables
consistent
with
the
awaren
ess-basedmod
elof
self-care.
Slocum
-Gorietal.[32],
Canada
Can
notde
term
ine:
TheCanadian
Hospice
Palliative
CareAssociatio
n(CHPC
A)provided
theirmem
bership
mail-o
utforcontact-
ingmanagersand
administratorsof
HPC
organizatio
ns.
Quantitative(Cross
sectionalsurvey)
630PC
HPinclud
ingclinical,
administrative,alliedhe
alth
workersandvolunteers.
(Individu
alprovidersnu
mbe
rno
tspecified
)
Exam
inetherelatio
nships
amon
gcompassionfatig
ue,
compassionsatisfaction,and
BOam
ongpalliativecare
workers
Com
passionsatisfactionwas
negativelyassociated
with
BOandcompassionfatig
ue.BO
andcompassionfatig
uewere
positivelyassociated
.Com
passionsatisfaction,BO
,andcompassionfatig
uedifferedsign
ificantlyaccording
tosomecharacteristicsof
the
sample.
Zambranoet
al.[33],
Australia.
Inpatient
and
outpatient
palliative
care
settings
includ
ingho
spice
(inpatient
unit/
hospice,a
consultatio
nliaison
into
tertiary
and
othe
rho
spitalsin
the
region
anda
commun
ityou
treach
prog
ram)
Qualitative(one
-on-
oneinterview)
7palliativemed
icineph
ysician
specialists
Toassess
expe
riences
ofpalliativemed
icinespecialists
who
providecare
fordying
patients,as
wellastheim
pact
ofprovidingcare
forthese
patients
Thestud
yparticipantswereat
high
riskforcompassion
fatig
ue.H
owever,the
yused
somecoping
strategies
that
redu
cedtheirstress.
Baqeas et al. BMC Palliative Care (2021) 20:88 Page 8 of 13

in 11 studies [1, 18, 20, 22, 23, 25, 27–29, 31, 32]. Thisscale measures compassion satisfaction, STS, and BO.The items of each subscale are rated on a five-pointLikert-type scale. The scale has demonstrated excellentpsychometric properties with Cronbach’s alpha of 0.80or more for its subscales [4].The Compassion Fatigue Scale (CFS) was used in only
one study [21] which was a pre-post study. This tool isdistinguished from the other tools by focusing more onthe helper and working environment. In addition, theCompassion Fatigue Short-Scale was used in one study[16]. This tool measures only compassion fatigue. Boththe 20-item CFS and the 13-item CFS were reported tohave adequate reliability and validity [16, 21]. Therefore,all of the three tools have been utilised internationallywith various populations. Apart from the psychometricproperties of these three measurement tools, authors didnot report any other evidence about their efficacy. Inaddition, they did not provide a rationale for their choiceof these tools in their studies.Four studies reported the levels of compassion fatigue
and compassion satisfaction among PCHP. All four usedthe professional quality of life scale (ProQOL) scale. Inthe study of Frey et al., [18] about half (48.4%) of pallia-tive care nurses had moderate to high levels of compas-sion satisfaction. However, about a quarter of theparticipants had high BO scores (26.8%) and more thanhalf (51.6%) had moderate STS [18]. O’Mahony et al.[27] found that palliative medicine physicians had overallhigh levels of compassion satisfaction and low levels ofBO and STS. Alkema, Linton, and Davies [1] found thatthe mean scores of compassion satisfaction, BO, andcompassion fatigue among hospice professionals were inthe average range. Finally, Kaur, Sharma, and Chaturvedireported that, among palliative care providers, 49.2% hadan average level of compassion satisfaction, 53.8% hadan average level of BO, while 95.4% scored above 75thpercentile on STS [23].
Theme 3: consequences of compassion fatigueTwo studies, both qualitative, reported consequences ofcompassion fatigue among their findings. A study con-ducted by Melvin reported that providing palliative careand working with dying patients could contribute tocompassion fatigue among PCHP [24]. The author alsosuggests that providing palliative care and working withdying patients could contribute to physical and emo-tional consequences. PCHP reported feeling responsiblefor patient care even after going home and leaving theworkplace [24]. In addition to compassion fatigue, work-ing with dying patients likely affects many dimensionsconcerning mental health including feelings of guilt, sad-ness, crying, thinking of death, remembering personalexperiences with death, isolation, and grief [33].
Theme 4: predictors or associated factors of compassionfatigue and satisfactionEleven articles provided data about the correlates of highlevels of compassion fatigue and poor compassion satis-faction among PCHP. In general, studies included PCHPfrom several disciplines. However, two studies had onlynurse samples and one study had both physician andnurse samples. The synthesis of these studies is includedbelow.In general, demographic, personal, and organisational
factors were associated with compassion fatigue andcompassion satisfaction among PCHP. Demographic fac-tors were found to be associated with compassion fa-tigue in some studies. Slocum-Gori et al. [32] found thatemployment status was associated with compassion fa-tigue as part-time workers had lower scores than thosewho worked full time. Additionally, they found thatgreater experience in palliative care was associated withlower levels of BO. O’Mahony et al. [27] supported theseresults and found that duration of experience in pallia-tive care was associated with higher levels of compassionsatisfaction.Personal factors were found to be associated with
compassion fatigue in several studies. For example, hav-ing a neuroticism personality trait was associated withincreased levels of STS and BO among PCHP, while hav-ing an agreeableness personality trait was associated withincreased levels of compassion satisfaction [27]. Inaddition, psychological hardiness (e.g., commitment andchallenge) were associated with lower BO and greatercompassion satisfaction [18]. Furthermore, practicingsome personal rituals on specific occasions was associ-ated with lower BO and more compassion satisfactionamong hospice staff [25]. Also, the ability to cope withdeath was associated with lower levels of compassion fa-tigue and BO and higher compassion satisfaction amongPCHP [31]. Greater exposure to death was also signifi-cantly correlated with STS among physicians and nursesemployed in a palliative care unit [29]. In addition, highlevels of dissociation (detachment) were associated withhigher levels of STS [28]. Psychological distress was alsoassociated with increased compassion fatigue [16]. Fur-ther, using self-care strategies was associated with lowerlevels of compassion fatigue and BO and higher levels ofcompassion satisfaction [1]. Further, mindful self-carewas associated with more compassion satisfaction andless risk of BO among health care workers in the pallia-tive care setting [22].Frey et al. found that organizational factors such as
work-related empowerment could decrease BO levels[18]. Furthermore, the authors found that STS was nega-tively associated with previous palliative care education[18]. Kaur et al. concluded that receiving training in pal-liative care was associated with lower levels of BO and
Baqeas et al. BMC Palliative Care (2021) 20:88 Page 9 of 13

STS [23]. Kaur et al. found that professional orientationwas associated with compassion satisfaction, with nursesscoring lower levels than other health professionals [23].Slocum-Gori et al. [32] found that compassion fatiguewas negatively correlated with compassion satisfactionand positively correlated with BO.
Theme 5: strategies or interventions to support PCHP orreduce compassion fatigueIn one systematic review, Hill et al. identified multipleinterventions reported to improve wellbeing of PCHP;however, most were found to be ineffective in reducingcompassion fatigue [34]. Examples of these interventionsinclude cognitive training, education, relaxation, andsupport [34]. Two of the included studies evaluated in-terventions to reduce compassion fatigue among PCHP.The first study by Heeter, Lehto, Allbritton, Day andWiseman examined the effectiveness of a 6-week medi-tation program delivered via smartphone apps to reducecompassion fatigue among 36 PCHP [20]. The singlegroup pre and post-test study design reported a signifi-cant reduction in compassion fatigue after the interven-tion [20]. Another study conducted by Hilliard [21]investigated the effectiveness of a music therapy inter-vention to reduce compassion fatigue in a sample of 17hospice workers. Participants were randomly assigned toan ecological music therapy group and a didactic musictherapy group. A pre-and post-test was performed tomeasure compassion fatigue levels. The results indicatedno significant differences in compassion fatigue betweenpre-and post-test scores of compassion fatigue in eithergroup [21].Four qualitative studies reported strategies to support
PCHP from the perspectives of the study participants[17, 24, 26, 33]. These studies did not actually measurethe effectiveness of these strategies. However, the re-searchers interviewed PCHP and asked them to liststrategies they believed helped to protect them fromcompassion fatigue. Palliative care nurses in the study byMelvin described adopting various strategies includingsetting professional boundaries, seeking support fromcolleagues and supervisors, reflection, physical exercise,and social activities out of work [24]. In the study ofMota Vargas et al. researchers interviewed PCHP andasked them to identify the self-care strategies they used[26]. Participants reported that reflecting on their experi-ence of providing palliative care, understanding themethods used to enhance self-control, and acknowledg-ing one’s limits and accepting the fact that many thingscannot be changed and learning to live with them werethe most commonly used strategies. Other self-carestrategies included attending training in palliative care,improving their communication skills, and developingpersonal hobbies [26]. Zambrano, Chur-Hansen, and
Crawford reported that PCHP highlighted supportivemeasures such as finding spiritual meaning, receivingsupport, and using both problem-focused and emotion-focused coping strategies [33]. Bessen, Jain, Brooks et al.reported that physicians described sharing experienceswith their colleagues or using individual-based strategies(e.g., improving self-awareness) to prevent compassionfatigue [17].
DiscussionThis scoping review mapped available evidence on com-passion fatigue and compassion satisfaction amongPCHP in various palliative care settings. The currentscoping review included all relevant studies regardless ofthe publication year but the majority that met inclusioncriteria were published within the last 5 years (n = 16).This suggests that interest in compassion fatigue andcompassion satisfaction in the field of palliative care isincreasing.Themes that emerged in this review were also reported
by previous reviews focusing on other health profes-sionals in non-palliative care settings. In a meta-narrative review related to compassion fatigue in healthliterature, the main themes that emerged were related topredictors/risk factors of compassion fatigue, its conse-quences, conceptualization, and measurement [10]. An-other review related to compassion fatigue in cancercare providers included themes related to compassionfatigue prevalence, measurement, and management [35].These reviews reported various predictors/risk factorsand consequences of compassion fatigue that are, tosome extent, similar to these reported in the currentstudy.Findings in our review suggest a general agreement
that compassion satisfaction reflects a sense of accom-plishment and reward of providing care for patients [1,18, 19, 22, 25, 30, 31]. However, there was no consensuson the definition of compassion fatigue in palliative caresettings. While some studies treated compassion fatigueas a single discrete entity, or synonymous with STS [20,31, 32], it was considered a multi-dimensional conceptby others [16, 18, 19, 22, 23, 25, 27–30]. The multi-dimensionality of compassion fatigue is further compli-cated because it is informed by different theories that in-form the definition of compassion fatigue [10, 36]. Thisrenders the development of a unified meaning of com-passion fatigue difficult. This also resulted in the vari-ability of the domains or subscales of the measures usedto assess compassion fatigue. Most of the included stud-ies used the ProQOL scale which assessed BO and STSas components of compassion fatigue rather than report-ing an overall score for compassion fatigue.Compassion is a central concept for PCHP who pro-
vide care for people with life limiting conditions. The
Baqeas et al. BMC Palliative Care (2021) 20:88 Page 10 of 13

more empathic a palliative care provider becomes, themore likely compassion fatigue will occur. Therefore, itis important to educate PCHP to modify empatheticability in response to prolonged work with patientsneeding palliative care. The human nervous system playsan important role in regulating the empathetic responseof the individual. Recent literature has shown that em-pathy is influenced by nervous system stimulation and itmay lead to empathic distress [37].The literature review revealed various organizational
factors (e.g., work-related empowerment, receiving train-ing in palliative care, and being recognized as a palliativecare nurse) and demographic factors (e.g., employmentstatus as part-time workers or full time and experiencein palliative care) associated with compassion fatigueand compassion satisfaction across PCHP. Further, itwas noted that some personal factors associated withcompassion fatigue and compassion satisfaction werenonmodifiable (e.g., neuroticism personality trait andpsychological hardiness). Additional factors includedpersonal variables such as practicing some personal rit-uals, the ability to cope with death and self-care, levelsof dissociation, using self-care strategies and mindfulself-care. Therefore, it can be concluded that compas-sion fatigue and compassion satisfaction are predicted bymany factors, some of which may not be modifiable.The majority of studies included participants from
multiple work settings (hospital, hospice and community)and none compared findings across settings or attemptedto differentiate between them. Given that work in the vari-ous settings can vary considerably, the incidence and ex-perience of compassion fatigue may also vary. Futureresearch should explore the impact of work setting oncompassion fatigue and compassion satisfaction.Receiving palliative care training or education was
found to help reduce the likelihood of developing symp-toms of compassion fatigue [18, 23, 38]. None of thesestudies explored the content of education programs toidentify which aspects induced this effect. Studies in non-palliative care settings have investigated training programsspecifically focused on reducing or preventing compassionfatigue. For example, in a Pre- Post- test study conductedto examine the effect of Mindful Self-Compassion (MSC)training on compassion fatigue and resilience amongnurses working in various settings, there was a significantreduction in the scores of secondary trauma and BO afterthe intervention [39]. Another study reported a significantreduction in participants’ compassion fatigue and BO andimprovement in compassion satisfaction after CompassionFatigue Specialist Training for mental health professionals[40]. It would seem likely given the nature of palliativecare work that specialist education programs would in-clude a focus on similar self-care activities; an examinationof the curricula of these programs would be useful in
explicating this content. We recommend that PCHPundergo specific education/training in this area, whetherthrough formal programs or continuing professionaldevelopment.A number of interventions have been shown to reduce
compassion fatigue and improve compassion satisfactionacross a wide range of populations [39, 40]. However,few intervention studies were conducted specific to thefield of palliative care. Only two of the included studiesin this review involved interventions and measured theireffectiveness to mitigate compassion fatigue and improvecompassion satisfaction among PCHP. Only one of thetested interventions (The 6-week technology-assistedmeditation) was found to be effective in reducing com-passion fatigue. Despite this, many descriptive or correl-ational studies pointed to such interventions. Otherstudies investigated strategies to support PCHP usingself-report data with correlational or qualitative ap-proaches rather than actually implementing these strat-egies or measuring their effectiveness [17, 24, 26, 33].Therefore, most of the knowledge regarding the inter-ventions used to mitigate compassion fatigue and im-prove compassion satisfaction among PCHP is informedby low level evidence. Furthermore, while there is someoverlap between palliative care and other health carespecialties, there are also aspects that are unique to pal-liative care. Therefore, it cannot be assumed that re-search undertaken in other specialty areas can beapplied to PCHP, and we recommend interventions betested in this population.
Strengths and limitationsThe strengths of this review include conducting a com-prehensive search with no limits on publication dates. Inaddition, studies that used concepts related to compas-sion fatigue but did not examine the concept directly(e.g., empathy, moral distress) were excluded from theliterature search to make the search methodology morerigorous. Nevertheless, the review has some limitations.First, some relevant studies may have been missed des-pite using a rigorous search strategy. This could occurdue to the complexity of compassion fatigue terms andinconsistencies in its conceptualisation across differentstudies. Second, only publications written in Englishwere included which limits generalisability and mayintroduce language bias. The limited number of studiesexamining compassion fatigue in palliative care settingsmay warrant conducting a broad search in all languages.Grey literature was excluded, which may introduce pub-lication bias.The results of this review highlight a gap in the litera-
ture examining impacts of compassion fatigue and com-passion satisfaction on PCHP. This gap in the literaturedemonstrates the need for further research on the
Baqeas et al. BMC Palliative Care (2021) 20:88 Page 11 of 13

impacts of compassion fatigue and compassion satisfac-tion on PCHP. Therefore, as nurses make up a signifi-cant proportion of the palliative care health providerworkforce, we recommend exploring the impact ofcompassion fatigue and compassion satisfaction onproductivity among palliative care nurses. Targeting ahomogeneous sample of nurses is also recommendedsince the included studies predominantly involvedheterogenous samples of PCHP rather than specificallynurses. Research is also required to understand whetherand how the experience of compassion fatigue and com-passion satisfaction may vary across different work envi-ronments. In addition, there is a need to conductinterventional studies to identify the most effective strat-egies, including education or training, to reduce compas-sion fatigue among PCHP.
ConclusionThis review sought to identify current evidence aboutcompassion fatigue and compassion satisfaction amongPCHP. Most of the studies investigating the impacts ofcompassion fatigue and compassion satisfaction onPCHP were descriptive in nature. This indicates a gap inthe literature that needs more investigation. Only onestudy identified an effective intervention to reduce com-passion fatigue in PCHP. Most of the reviewed studieswere correlational or exploratory in nature which affectsthe quality and strength of the retrieved evidence. Oneimportant aspect to be considered is the impact of com-passion fatigue and compassion satisfaction on the prod-uctivity of PCHP and their ability to provide safe andcompassionate care. This is an important topic especiallyamong palliative care nurses since they are the largestgroup of PCHP and they spend a long time caring forpeople with life-threatening conditions and relatedtrauma. The current work suggests a need to fill variousgaps in knowledge and provides a clear direction for fu-ture research.
AbbreviationsPCHP: Palliative care health providers; BO: Burnout; STS: Secondary traumaticstress; ProQOL: Professional quality of life; CFS: Compassion fatigue scale
AcknowledgementsWe would like to thank Ms. Elizabeth Lawrence for her contributions todeveloping the search strategy for this manuscript.
Authors’ contributionsMB and BC conceived the study. MB developed the search strategy,conducted the initial literature search, and contributed to the writing of themanuscript. BC and MB extracted and screened articles. BC and JD providedsubstantive expertise, oversaw all stages of the review, provided expertise tothe review and analysis process, and critically revised the manuscript. Allauthors approved the final version of the manuscript.
FundingMB was supported by a scholarship from the Ministry of Higher EducationSaudi Arabia. The funding body had no involvement in the design or
conduct of the study, nor in the writing of the manuscript. No other fundingwas received.
Availability of data and materialsData used in this manuscript consist of published articles which cannot beshared by the authors for copyright reasons but are available throughsubscription to the relevant journals/databases.
Declarations
Ethics approval and consent to participateNot applicable; no original data.
Consent for publicationNot applicable; no details, images, or videos relating to individual personsincluded.
Competing interestsThe author(s) declare no potential conflicts of interest with respect to themanuscript, authorship, and/or publication of this article.
Received: 8 August 2020 Accepted: 1 June 2021
References1. Alkema K, Linton JM, Davies R. A study of the relationship between self-
care, compassion satisfaction, compassion fatigue, and burnout amonghospice professionals. J Soc Work End-of-Life Palliat Care. 2008;4(2):101–19.
2. Consortium GRPC. Specialist palliative care for complex care and referral tospecialist palliative care - Grampians Region Palliative Care Consortium.Grampians Region Palliative Care Consortium. [cited 13 December 2020].Available from: https://grampianspalliativecare.com.au/health-care-professionals/specialist-palliative-care-for-complex-care/
3. Sorenson C, Bolick B, Wright K, Hamilton R. Understanding compassionfatigue in healthcare providers: a review of current literature. J NursScholarsh. 2016;48(5):456–65.
4. Stamm B. The concise ProQOL manual. 2nd ed. Pocatello: Beth HundallStamm; 2020. [cited 14 January 2021]. Available from: https://proqol.org/uploads/ProQOLManual.pdf
5. Coetzee SK, Klopper HC. Compassion fatigue within nursing practice: aconcept analysis. Nurs Health Sci. 2010;12(2):235–43.
6. Nolte AG, Downing C, Temane A, Hastings-Tolsma M. Compassion fatiguein nurses: a metasynthesis. J Clin Nurs. 2017;26(23–24):4364–78.
7. Drury V, Craigie M, Francis K, et al. Compassion satisfaction, compassionfatigue, anxiety, depression and stress in registered nurses in Australia:phase 2 results. J Nurs Manag. 2014;22(4):519–31.
8. Harris C, Griffin MTQ. Nursing on empty: compassion fatigue signs,symptoms, and system interventions. J Christ Nurs. 2015;32(2):80–7.
9. Hegney DG, Craigie M, Hemsworth D, et al. Compassion satisfaction,compassion fatigue, anxiety, depression and stress in registered nurses inAustralia: study 1 results. J Nurs Manag. 2014;22(4):506–18.
10. Sinclair S, Raffin-Bouchal S, Venturato L, et al. Compassion fatigue: a meta-narrative review of the healthcare literature. Int J Nurs Stud. 2017;69:9–24.
11. Tricco AC, Lillie E, Zarin W, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018;169(7):467–73.
12. Khalil H, Peters M, Godfrey CM, et al. An evidence-based approach toscoping reviews. Worldviews Evid Based Nurs. 2016;13(2):118–23.
13. Levac D, Colquhoun H, O'Brien KK. Scoping studies: advancing themethodology. Implement Sci. 2010;5(69):1–9.
14. Arksey H, O'Malley L. Scoping studies: towards a methodological framework.Int J Soc Res Methodol. 2005;8(1):19–32.
15. Mellor C, Hain R. Paediatric palliative care: not so different from adultpalliative care? Br J Hosp Med (2005). 2010;71(1):36–9.
16. Barnett MD, Ruiz IA. Psychological distress and compassion fatigue amonghospice nurses: the mediating role of self-esteem and negative affect. JPalliat Med. 2018;21(10):1504–6.
17. Bessen S, Jain RH, Brooks WB, Mishra M. “Sharing in hopes and worries”-aqualitative analysis of the delivery of compassionate care in palliative careand oncology at end of life. Int J Qual Stud Health Well-Being. 2019;14(1):1622355.
Baqeas et al. BMC Palliative Care (2021) 20:88 Page 12 of 13

18. Frey R, Robinson J, Wong C, Gott M. Burnout, compassion fatigue andpsychological capital: findings from a survey of nurses delivering palliativecare. Appl Nurs Res. 2018;43:1–9.
19. Galiana L, Arena F, Oliver A, et al. Compassion satisfaction, compassionfatigue, and burnout in Spain and Brazil: ProQOL validation and Cross-cultural diagnosis. J Pain Symptom Manag. 2017;53(3):598–604.
20. Heeter C, Lehto R, Allbritton M, et al. Effects of a technology-assistedmeditation program on healthcare providers’, interoceptive awareness,compassion fatigue, and burnout. J Hospice Palliat Nurs. 2017;19(4):314–22.
21. Hilliard RE. The effect of music therapy sessions on compassion fatigue andteam building of professional hospice caregivers. Arts Psychother. 2006;33(5):395–401.
22. Hotchkiss JT. Mindful self-care and secondary traumatic stress mediate arelationship between compassion satisfaction and burnout risk amonghospice care professionals. Am J Hosp Palliat Care. 2018;35(8):1099–108.
23. Kaur A, Sharma MP, Chaturvedi SK. Professional quality of life amongprofessional care providers at Cancer palliative care centers in Bengaluru,India. Indian J Palliat Care. 2018;24(2):167–72.
24. Melvin CS. Professional compassion fatigue: what is the true cost of nursescaring for the dying? Int J Palliat Nurs. 2012;18(12):606–11.
25. Montross-Thomas LP, Scheiber C, Meier EA, et al. Personally meaningfulrituals: a way to increase compassion and decrease burnout among hospicestaff and volunteers. J Palliat Med. 2016;19(10):1043–50.
26. Mota Vargas R, Mahtani-Chugani V, Solano Pallero M, et al. Thetransformation process for palliative care professionals: the metamorphosis,a qualitative research study. Palliat Med. 2016;30(2):161–70.
27. O'Mahony S, Ziadni M, Hoerger M, et al. Compassion fatigue amongpalliative care clinicians: findings on personality factors and years of service.Am J Hosp Palliat Care. 2018;35(2):343–7.
28. Samson T, Shvartzman P. Secondary traumatization and proneness todissociation among palliative care workers: a Cross-sectional study. J PainSymptom Manag. 2018;56(2):245–51.
29. Samson T, Shvartzman P. Association between level of exposure to deathand dying and professional quality of life among palliative care workers.Palliat Support Care. 2018;16(4):442–51.
30. Samson T, Lecovich E, Shvartzman P. Psychometric characteristics of theHebrew version of the professional quality-of-life scale. J Pain SymptomManag. 2016;52(4):575–81.
31. Sansó N, Galiana L, Oliver A, et al. Palliative care Professionals’ inner life:exploring the relationships among awareness, self-care, and compassionsatisfaction and fatigue, burnout, and coping with death. J Pain SymptomManag. 2015;50(2):200–7.
32. Slocum-Gori S, Hemsworth D, Chan WY, et al. Understanding compassionsatisfaction, compassion fatigue and burnout: a survey of the hospicepalliative care workforce. Palliat Med. 2013;27(2):172–8.
33. Zambrano SC, Chur-Hansen A, Crawford GB. The experiences, copingmechanisms, and impact of death and dying on palliative medicinespecialists. Palliat Support Care. 2014;12(4):309–16.
34. Hill RC, Dempster M, Donnelly M, et al. Improving the wellbeing of staffwho work in palliative care settings: a systematic review of psychosocialinterventions. Palliat Med. 2016;30(9):825–33.
35. Najjar N, Davis LW, Beck-Coon K, et al. Compassion fatigue: a review of theresearch to date and relevance to cancer-care providers. J Health Psychol.2009;14(2):267–77.
36. Cross LA. Compassion fatigue in palliative care nursing: a concept analysis. JHosp Palliat Nurs. 2019;21(1):21–8.
37. Brito-Pons G, Librada-Flores S. Compassion in palliative care: a review. CurrOpin Support Palliat Care. 2018;12(4):472–9.
38. Flarity K, Gentry JE, Mesnikoff N. The effectiveness of an educationalprogram on preventing and treating compassion fatigue in emergencynurses. Adv Emerg Nurs J. 2013;35(3):247–58.
39. Delaney MC. Caring for the caregivers: Evaluation of the effect of an eight-week pilot mindful self-compassion (MSC) training program on nurses’compassion fatigue and resilience. PloS One. 2018;13(11):e0207261.
40. Gentry JE, Baggerly J, Baranowsky A. Training-as-treatment: effectiveness ofthe certified compassion fatigue specialist training. Int J Emerg MentalHealth. 2004;6(3):147–55.
Publisher’s NoteSpringer Nature remains neutral with regard to jurisdictional claims inpublished maps and institutional affiliations.
Baqeas et al. BMC Palliative Care (2021) 20:88 Page 13 of 13