Embed Size (px)
Citation preview
Complex Coding Decisions
Using ICD-10-PCS, Part 4
Lynn Kuehn, MS, RHIA, CCS-P, FAHIMAKuehn Consulting, LLC
Waukesha, WI 53186
(262) 574-1064
Learning Objectives
• At the conclusion of this program, you will be
able to:
– Describe the system design for ICD-10-PCS
– Compare and contrast the root operation groups
– Differentiate between similar root operations using
critical thinking skills
– Identify the root operations assigned for 10
common PCS cases
– Determine the remaining characters in each code
for 10 common PCS cases
2
PCS Files
Download the PCS files from:
http://www.cms.gov/Medicare/Coding/ICD
10/2015-ICD-10-PCS-and-GEMs.html
– 2015 Code Tables and Index
– 2015 Official ICD-10-PCS Coding
Guidelines
– 2015 ICD-10-PCS Reference Manual
• Use electronic version – too big to print
3
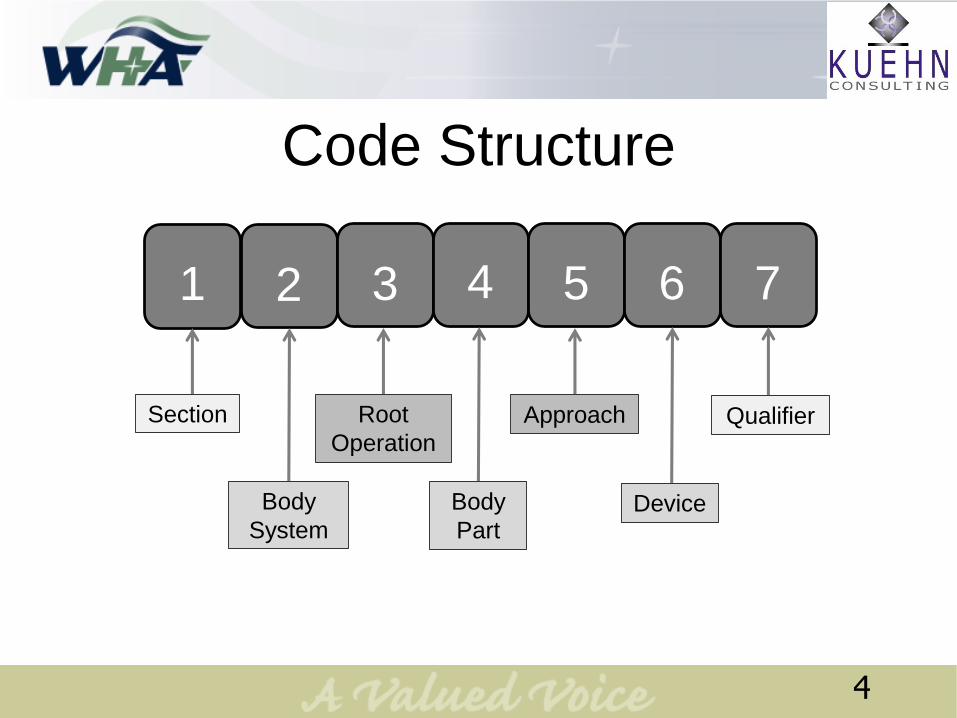
Code Structure
2 3 4 5 6 71
Section
Body
System
Root
Operation
Body
Part
Approach
Device
Qualifier
4
ICD-10-PCS Index
• Provides the first three or four
characters of the code
• Refers the coder to the correct code
table
• The code tables must always be used to
obtain the complete code
5
ICD-10-PCS Tables
Each table contains four columns and a
varying numbers of rows
Column: Specifies the allowable values for
characters 4 through 7
Row: Specifies the valid combinations of
values
6
Root OperationsAlteration
Bypass
Change
Control
Creation
Destruction
Detachment
Dilation
Division
Drainage
Release
Removal
Repair
Replacement
Reposition
Resection
Restriction
Revision
Supplement
Transfer
Transplantation
Excision
Extirpation
Extraction
Fragmentation
Fusion
Insertion
Inspection
Map
Occlusion
Reattachment
7
Nine Root Operation Groups
Root operations that take out some or all of
a body part
Root operations that take out solids, fluids, or gases from a body
part
Root operations that involve cutting or separation only
Root operation that put in, put back, or move some or all of a body
part
8
Nine Root Operation Groups
Root operations that always
involve a device
Root operations that involve examination
only
Root operations that define other repairs
Root operations that define other objectives
Root operations that alter the
diameter or route of a tubular body
part
9
What is the intent of the
procedure?
10

Take Out Group
11

• To determine whether
it’s Excision or
Resection, always
start in the Index
under the heading
Resection.
• All body parts can be
Excised.
12
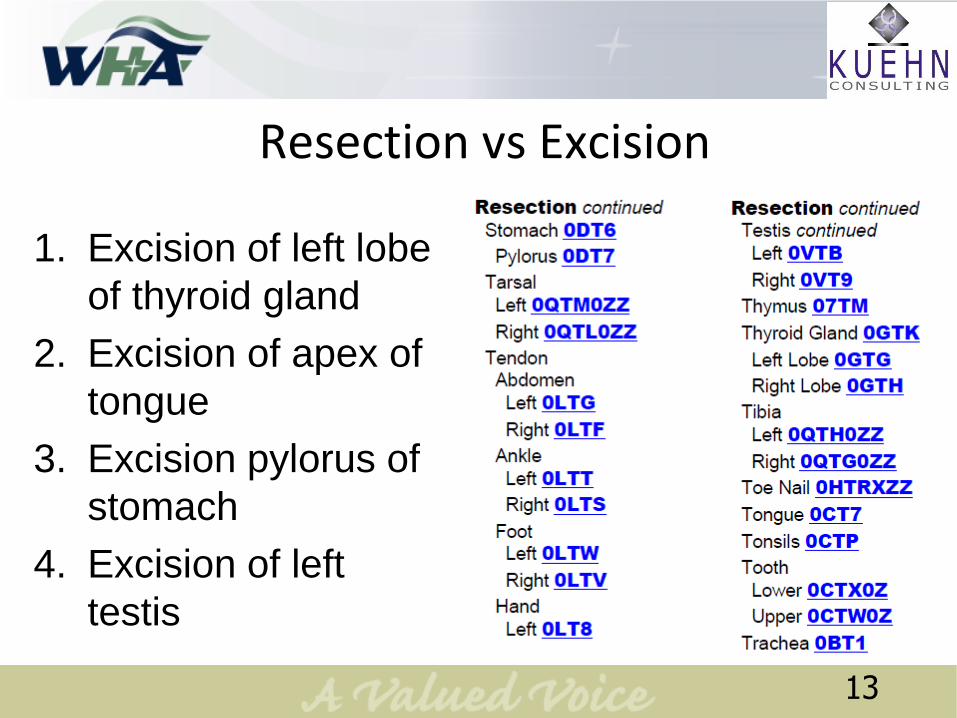
Resection vs Excision
1. Excision of left lobe
of thyroid gland
2. Excision of apex of
tongue
3. Excision pylorus of
stomach
4. Excision of left
testis
13
Answers
1. Excision of left lobe of thyroid gland
– Resection
2. Excision of apex of tongue
– Excision
3. Excision pylorus of stomach
– Resection
4. Excision of left testis
– Resection
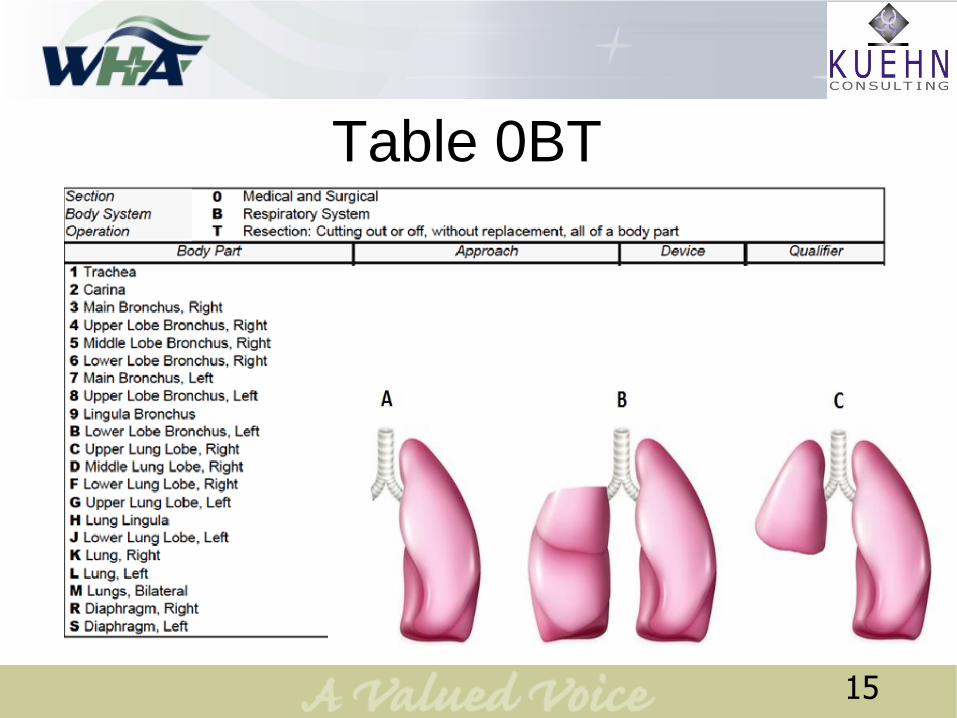
Table 0BT
15
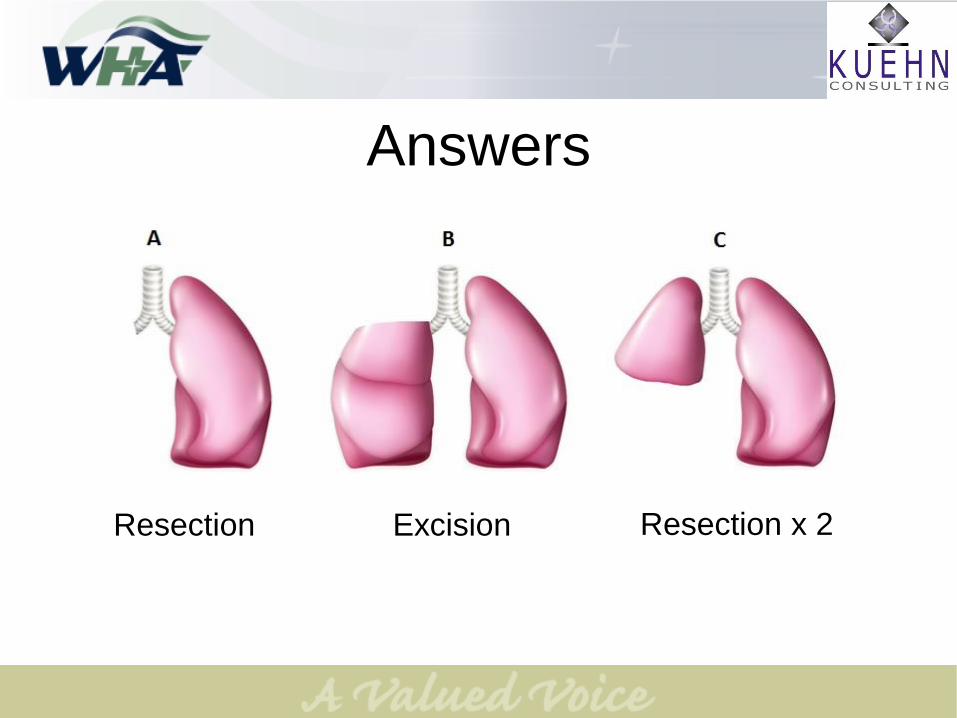
Answers
Resection Excision Resection x 2
Case #1
He presents with a right upper lobe pulmonary nodule. The
patient was taken to the OR and an incision was made over
the sixth rib. The lung was explored and only the single lung
nodule was found.
The wedge resection was performed using a tissue stapler,
removing the lesion and a 2 cm margin. The specimen was
sent for frozen section. The findings returned as metastatic
colon cancer, with clear margins in the specimen. The ribs
were approximated and the chest wall was closed in layers.
The subcutaneous tissue and skin were approximated.
17
Decision to be made?
18
Case #1 – Poll Question
Which root operation is it?
1. Excision
2. Resection
3. Extraction
19

Case #1
Which root operation?
Excision
Which body part value
will we pick?
Right upper lobe of the
lung
20
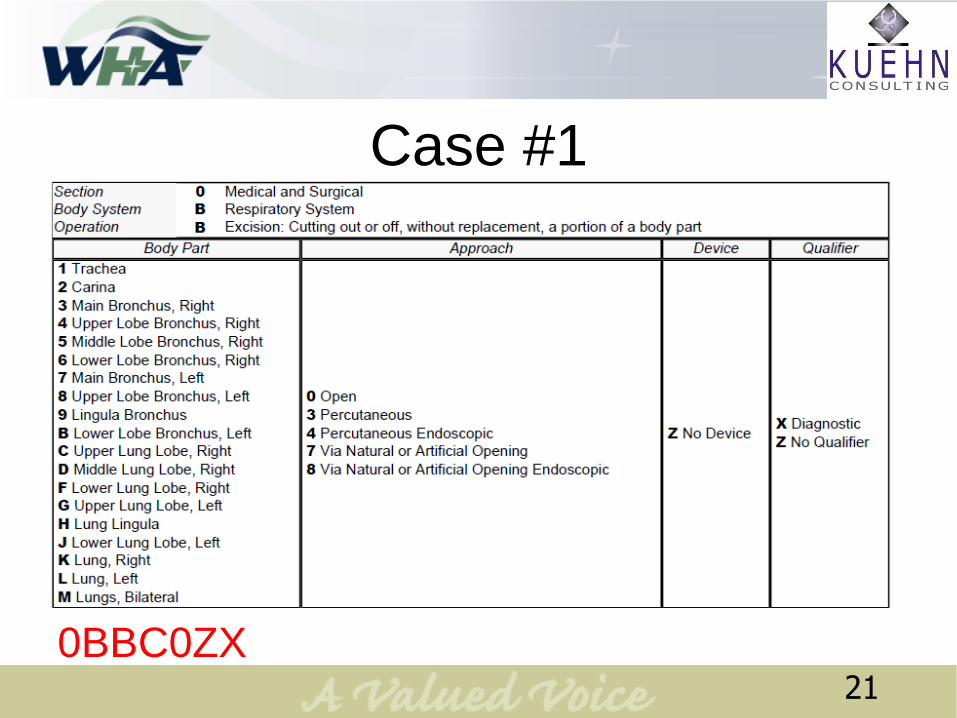
Case #1
0BBC0ZX21

Gunk Group
22
• Excision and
Extraction removes
body parts
• Extirpation removes
foreign objects from
a body part
23
Case #2
PREOPERATIVE DIAGNOSIS: Abnormal EKG suggestive of anterior
ischemia.
POSTOPERATIVE DIAGNOSIS: 1.Coronary artery disease
2. Thrombus in proximal diagonal branch with severe stenosis
PROCEDURES:
1. Left heart catheterization with pressure readings
2. Left ventricular angiography, right and left coronary
angiography using Isovue-370
3. Diagonal branch mechanical thrombectomy, angioplasty and
stenting with a 2.5 x 12 mm long Promus Element DES stent
4. Angio-seal deployment for hemostasis
24
Case #2
• Root operations to assign?
– Extirpation
– Dilation
– Measurement
– Fluoroscopy
25
Case #2
26
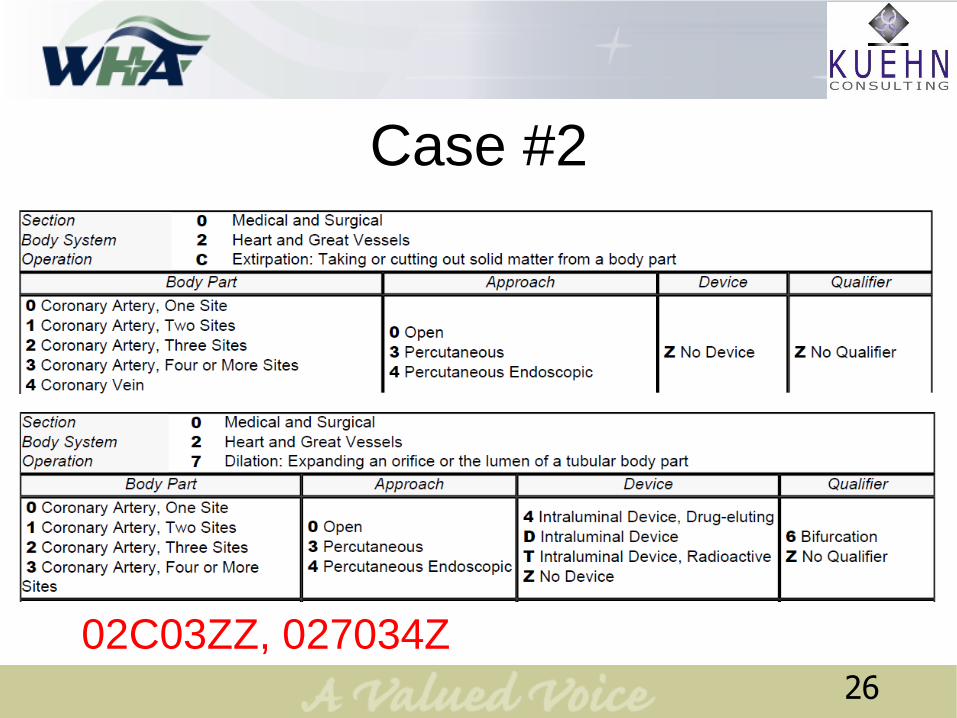
02C03ZZ, 027034Z

Case #2
4A023N7, B2151ZZ , B2111ZZ27
Case #2
02C03ZZ Thrombectomy (Extirpation)
027034Z PTCA (Dilation) with Drug-
eluting stent
4A023N7 Left heart catheterization
B2151ZZ Left ventriculogram with low
osmolar contrast
B2111ZZ Coronary angiogram (multiple)
with low osmolar contrast28
Cutting Group
29
Fasciotomy is a
surgical procedure
where the fascia is
cut to relieve tension
or pressure and
restore circulation to
an area of tissue or
muscle.
30
Case #3
PREOPERATIVE DIAGNOSIS: Left lower extremity with ischemic leg.
POSTOPERATIVE DIAGNOSIS: Ischemic leg with diseased left common femoral
artery.
OPERATION: 4-Compartment left lower extremity fasciotomy
PROCEDURE AS FOLLOWS: The patient was taken to the operating room, placed on
the operating room table in the supine position. After an adequate level of general
endotracheal anesthesia was obtained, his left lower extremity was prepped and draped
in the usual sterile fashion with Chloraprep. Intravenous antibiotics were provided. Four
compartment fasciotomies were performed through medial and lateral incisions
exposing the musculature of both the lateral, anterior, and both the deep and superficial
posterior compartments and these were viable. Due to lack of additional significant
swelling, the skin was closed utilizing staples. Patient was awakened, extubated, and
transferred to recovery room in stable condition. He has a palpable left dorsalis pedis
pulse that is 1+, mildly diminished. He tolerated the procedure well.
31
Case #3 – Poll Question
Which root operation is it?
1. Division
2. Release
3. Excision
32
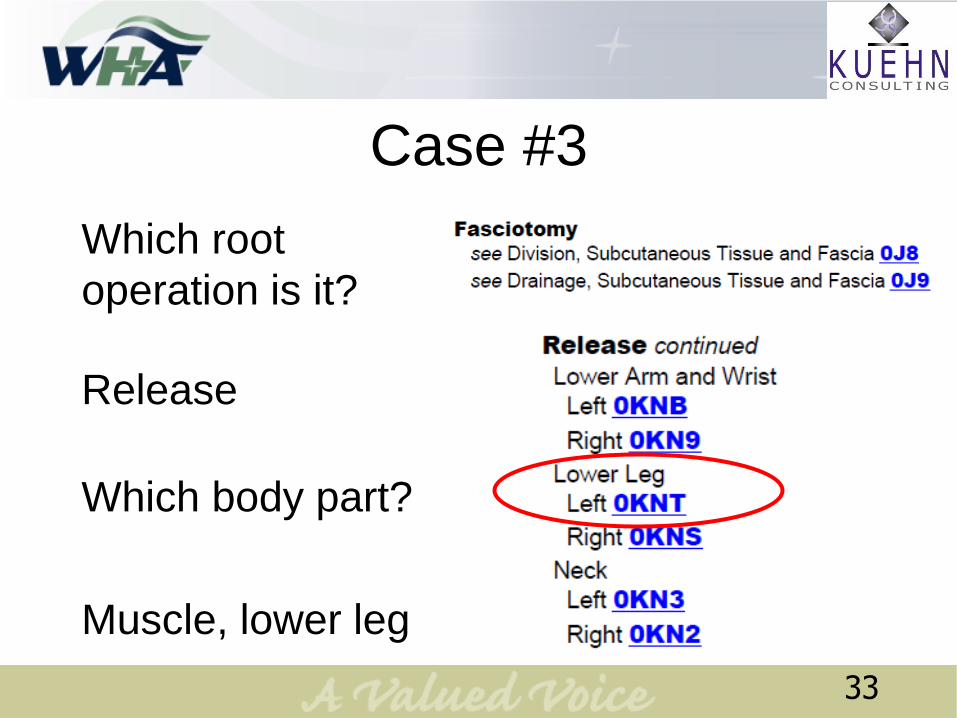
Case #3
Which root
operation is it?
Release
Which body part?
Muscle, lower leg
33

Release
0KNT0ZZ x4
34

Repair Group
35

• Repair tables
always say “No
Device” in the
Device character.
• Why?
36
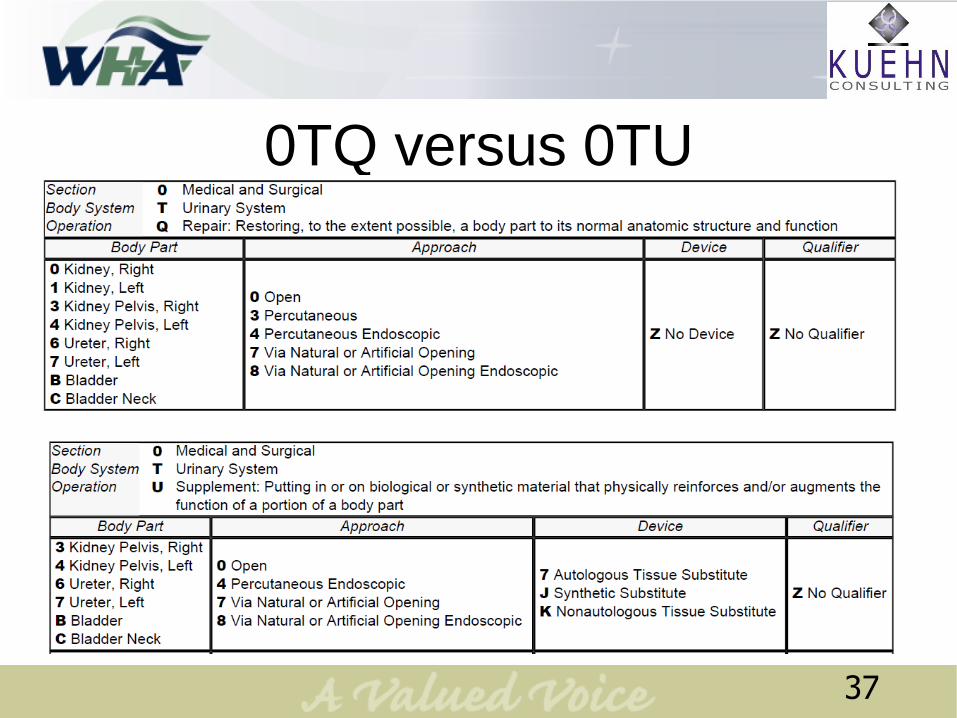
0TQ versus 0TU
37
Device Group
38
• The Device Group
root operation must
always involve a
device.
• Removal and
revision are only
coded for devices.
39
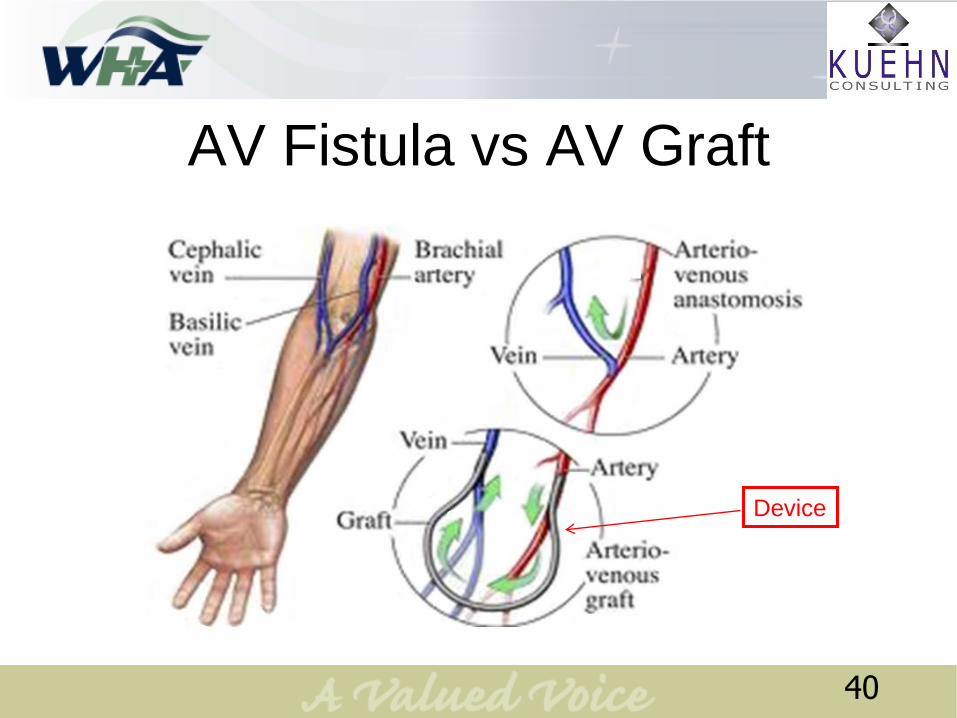
AV Fistula vs AV Graft
Device
40
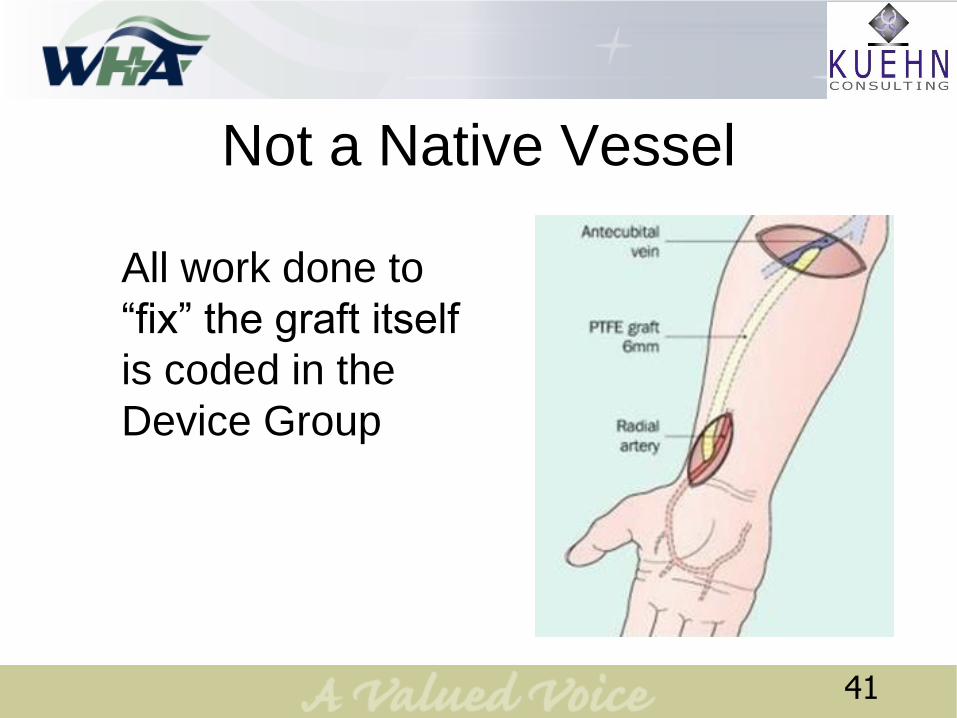
Not a Native Vessel
All work done to
“fix” the graft itself
is coded in the
Device Group
41
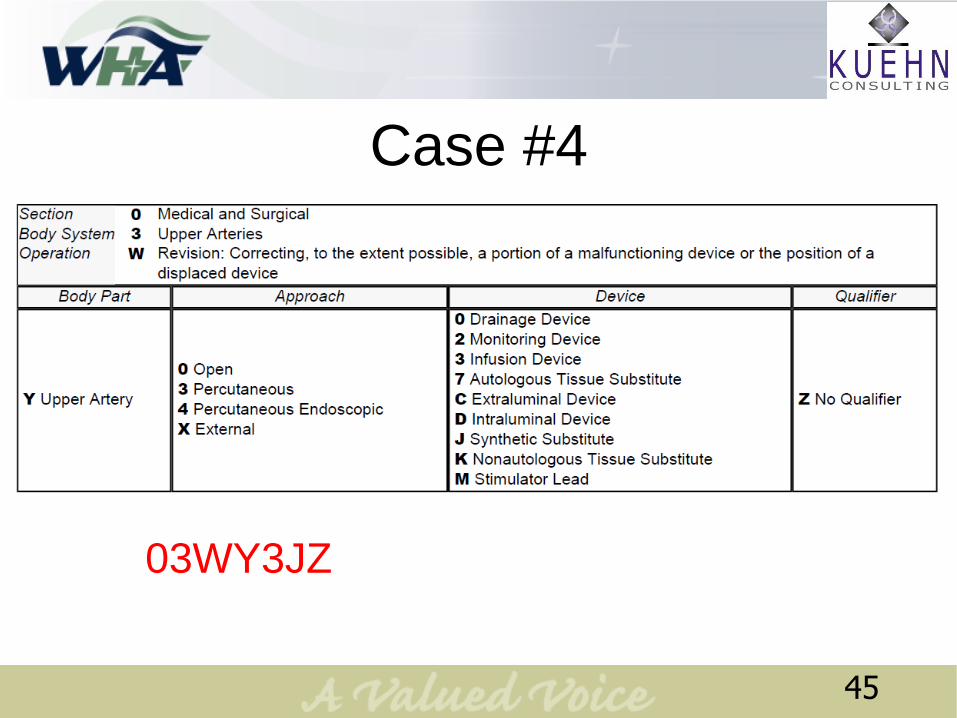
Case #4
DIAGNOSIS: Thrombosed right arm arteriovenous Gortex graft.
PROCEDURE: Balloon catheter thrombectomy of right lower arm
arteriovenous graft and angioJet thrombectomy of right lower arm
arteriovenous graft.
DESCRIPTION OF OPERATION: A Glidewire and then a 6-
French sheath was inserted into the graft and then a 5 mm x 2 cm
balloon catheter was passed over the Glidewire into the graft and a
thrombectomy was performed. Thrombectomy was not complete.
At this point, an AngioJet thrombectomy catheter was advanced
over the Glidewire and two passes of the AngioJet was performed.
Satisfied with the thrombectomy results, the sheaths were removed
and pressure held over the puncture site. The patient tolerated the
procedure well.
42
Case #4
Which root operation is it?
1. Extirpation
2. Extraction
3. Revision
43
Case #4
44
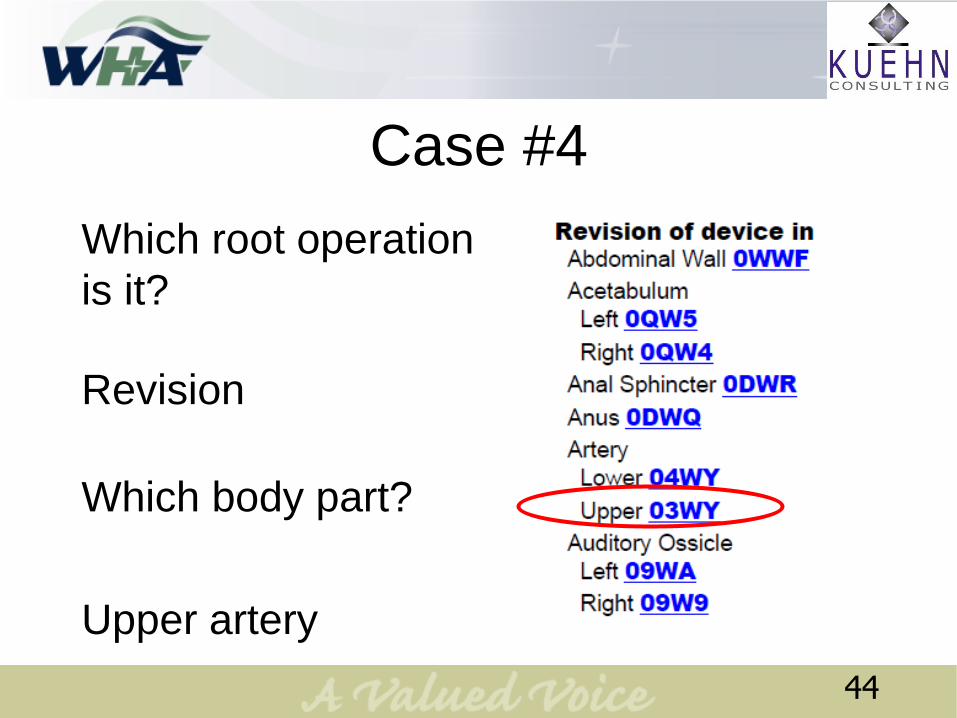
Which root operation
is it?
Revision
Which body part?
Upper artery
Case #4
45
03WY3JZ
• Supplement is the
partner root
operation to Repair.
• Supplement is
repair of a body part
using a device.
46
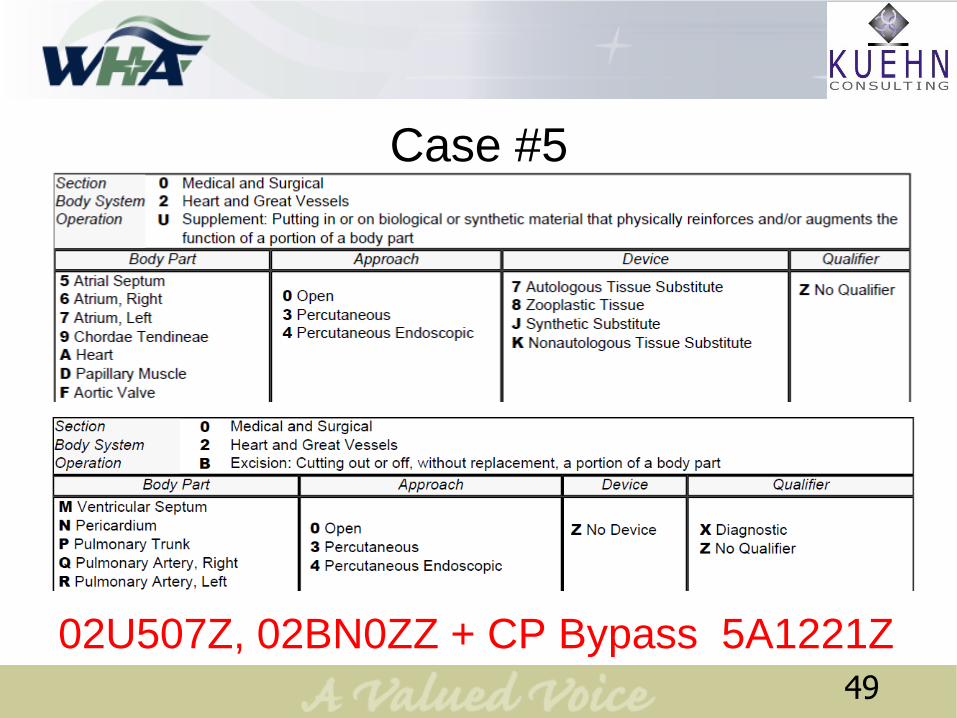
Case #5
Pre-operative Diagnosis: Atrial septal defect
Post-operative Diagnosis: Atrial septal defect
Procedure: ASD repair with pericardial patch
Summary: The patient’s chest is opened via midline
sternotomy. A portion of pericardium is harvested and
prepared for patching. The patient is placed on CP
Bypass and the heart is opened. The defected is
repaired by sewing the patch over the hole. CP Bypass
is concluded. The pericardium, sternum and chest wall
are closed.
47
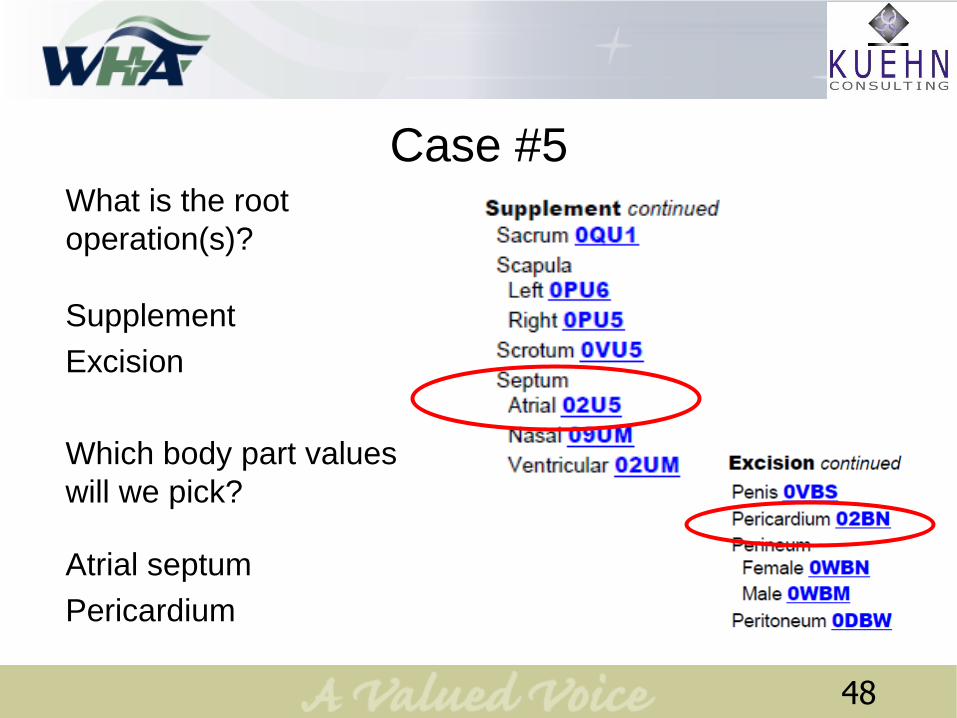
Case #5What is the root
operation(s)?
Supplement
Excision
Which body part values
will we pick?
Atrial septum
Pericardium
48
Case #5
02U507Z, 02BN0ZZ + CP Bypass 5A1221Z
49
Tubular Group
50
If the body part is a
tube, start here first.
51
Case #6DIAGNOSIS: A 7 cm infrarenal abdominal aortic aneurysm.
OPERATION: Abdominal aortic aneurysm repair using a 22 mm Hemashield Dacron tube
graft.
DESCRIPTION OF PROCEDURE: After adequate general endotracheal anesthesia, the
abdomen was entered and the infrarenal abdominal aortic aneurysm was identified.
The neck of the aneurysm was encircled with an umbilical tape. Both common iliac
arteries were isolated with umbilical tapes as well. IV hperarin sulfate 5000 units
administered. After clamping, the aneurysm was opened and the neck of the aneurysm
was cut into a T fashion. A 22 mm Hemashield Dacron tube graft was brought into the
field and cut to the desired length and shape. The proximal anastomosis was then
performed using 3-0 Prolene in a running fashion. Hemostasis was obtained.
The distal anastomosis was next performed in a similar fashion. The distal neck was cut
into a T fashion and the graft was cut to the desired length and shape. The anastomosis
was performed using 3-0 Prolene in a running fashion. There were strong femoral pulses
at the end of the procedure. The heparin was then reversed. The aneurysm sac was
closed over the graft using 0 Vicryl in a running fashion. The incision was closed in layers.
52
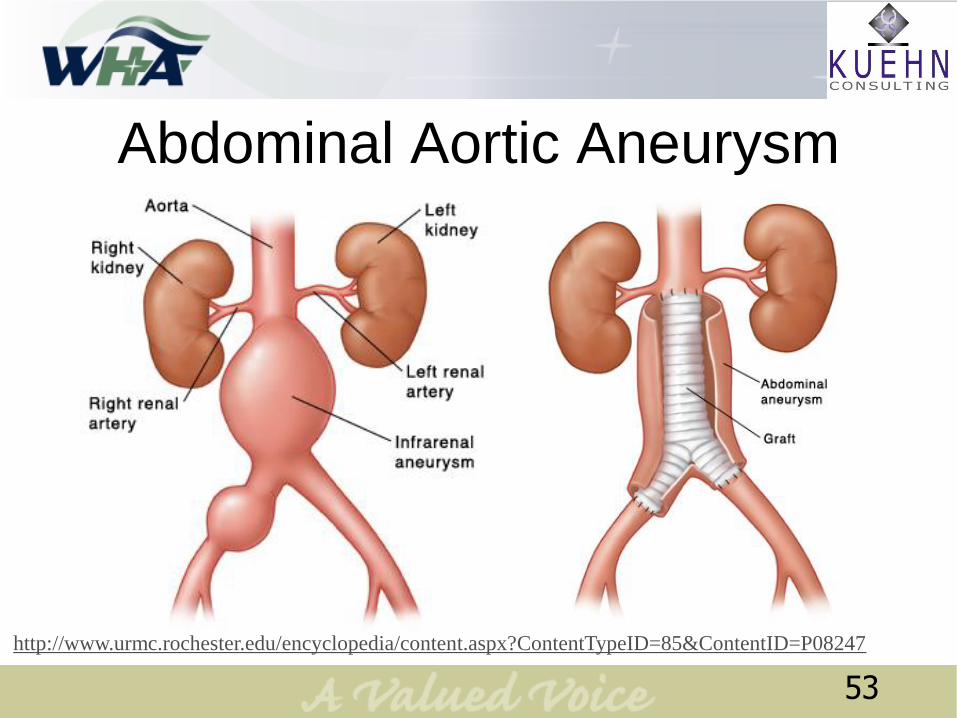
Abdominal Aortic Aneurysm
http://www.urmc.rochester.edu/encyclopedia/content.aspx?ContentTypeID=85&ContentID=P08247
53
Case #6 – Poll Question
What root operation is it?
1. Occlusion
2. Restriction
3. Supplement
54
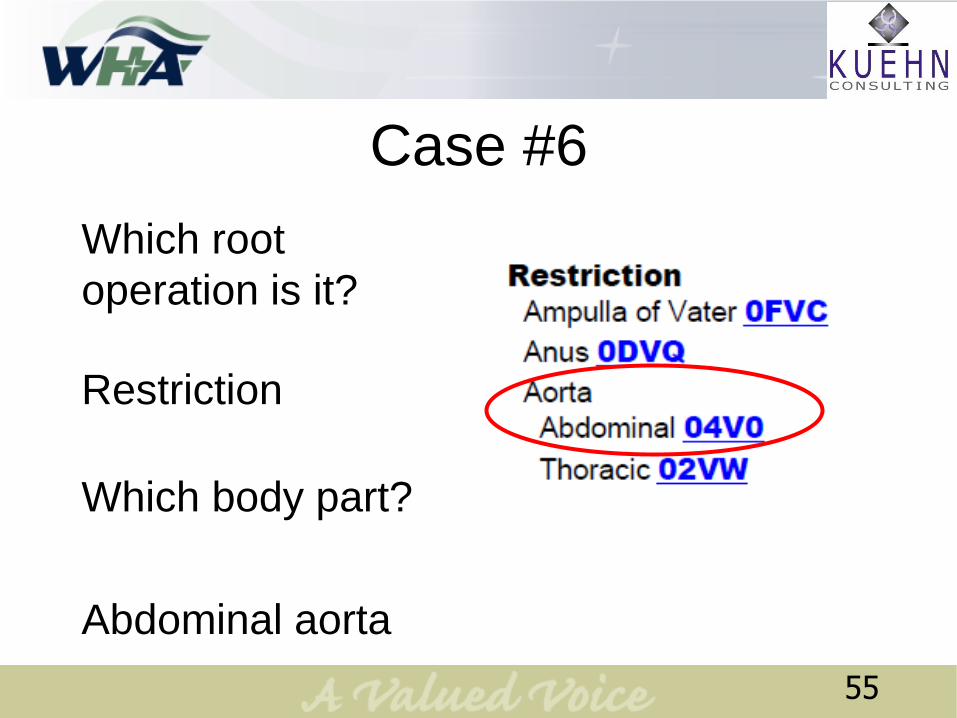
Case #6
55
Which root
operation is it?
Restriction
Which body part?
Abdominal aorta
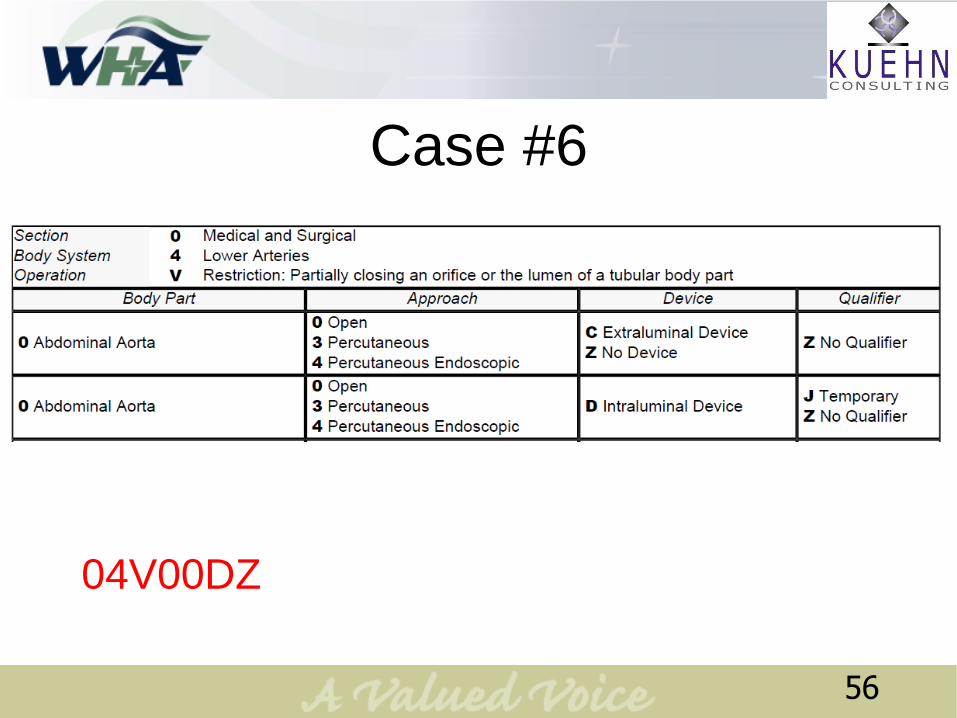
Case #6
04V00DZ
56
To be used as, and
coded as a device,
the tissue must
become completely
separated from the
body.
57

Case #7
Procedure: CABG
Description of Procedure: The chest was opened through a median sternotomy
incision. The pericardium was opened. Cardiopulmonary bypass was initiated. The
greater saphenous vein was harvested via incision from the left lower extremity. The
patient was cooled and cross-clamped. The cold blood cardioplegia solution was
administered. Individual segments of saphenous vein were sewn to the obtuse
marginal, to the posterolateral branch of the circumflex artery, and to the distal right
coronary artery respectively. Each of these anastomoses were carried out with
running sutures of 7-0 Prolene.
At the termination of this, warm blood cardioplegia was administered and the aortic
cross-clamp was then released. A partial occluding clamp was placed on the aorta.
Three buttons of aortic tissue were excised and used as three proximal
anastomoses for the saphenous grafts which were carried out with running sutures
of 6-0 Prolene. With the patient fully re-warmed, the heart resumed a good
contractility and resumed a normal sinus rhythm. The patient was weaned from
cardiopulmonary bypass. The chest was closed in layers in the usual fashion and
dry sterile dressing was applied.
58
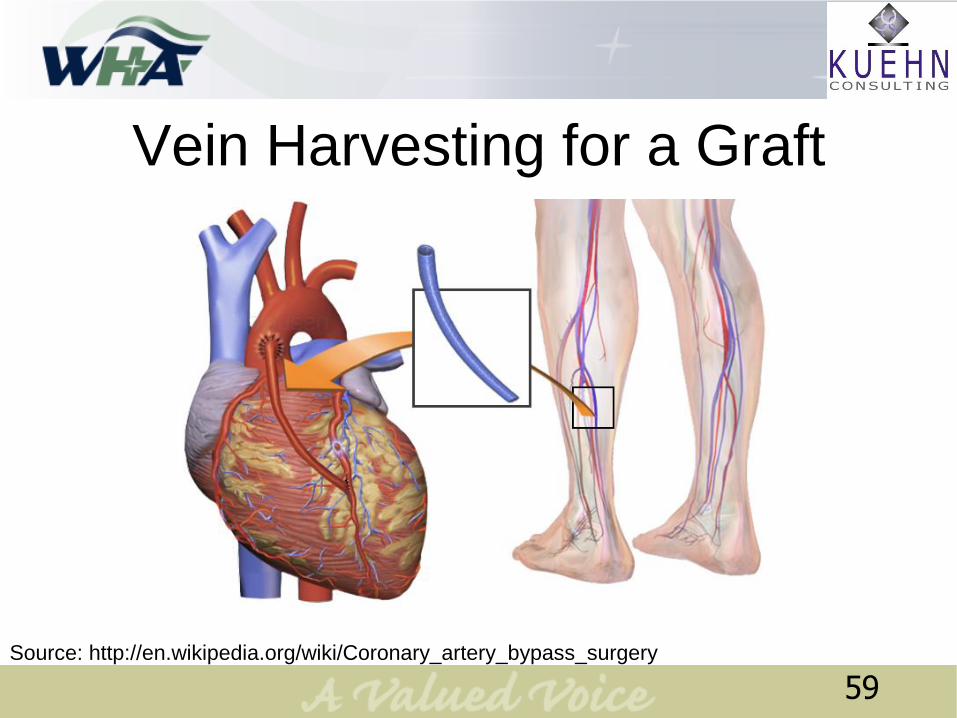
Vein Harvesting for a Graft
Source: http://en.wikipedia.org/wiki/Coronary_artery_bypass_surgery
59
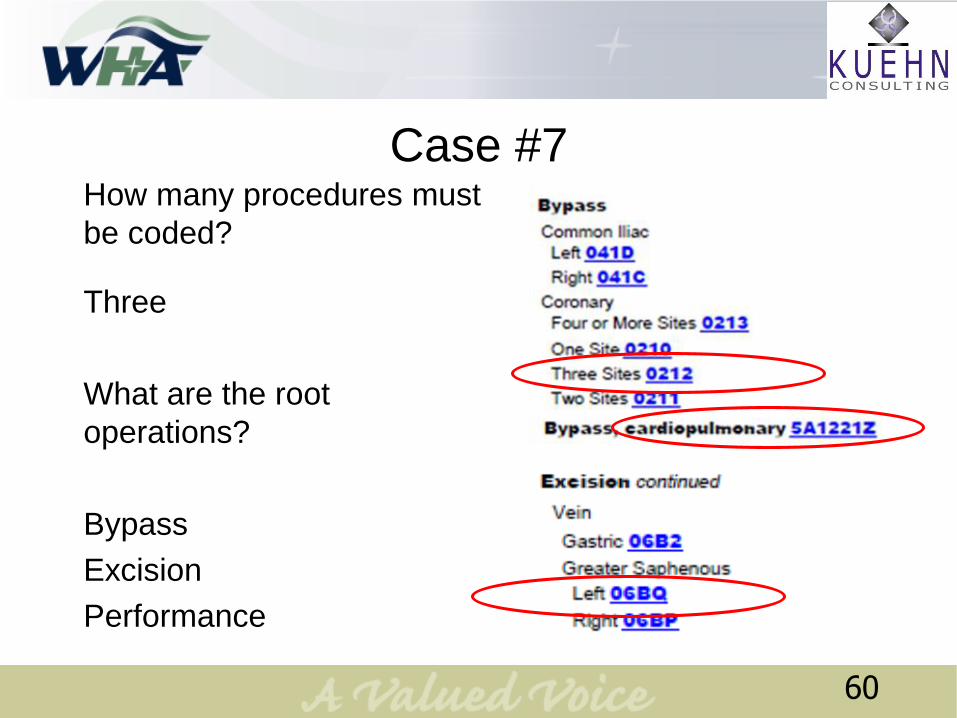
Case #7How many procedures must
be coded?
Three
What are the root
operations?
Bypass
Excision
Performance
60
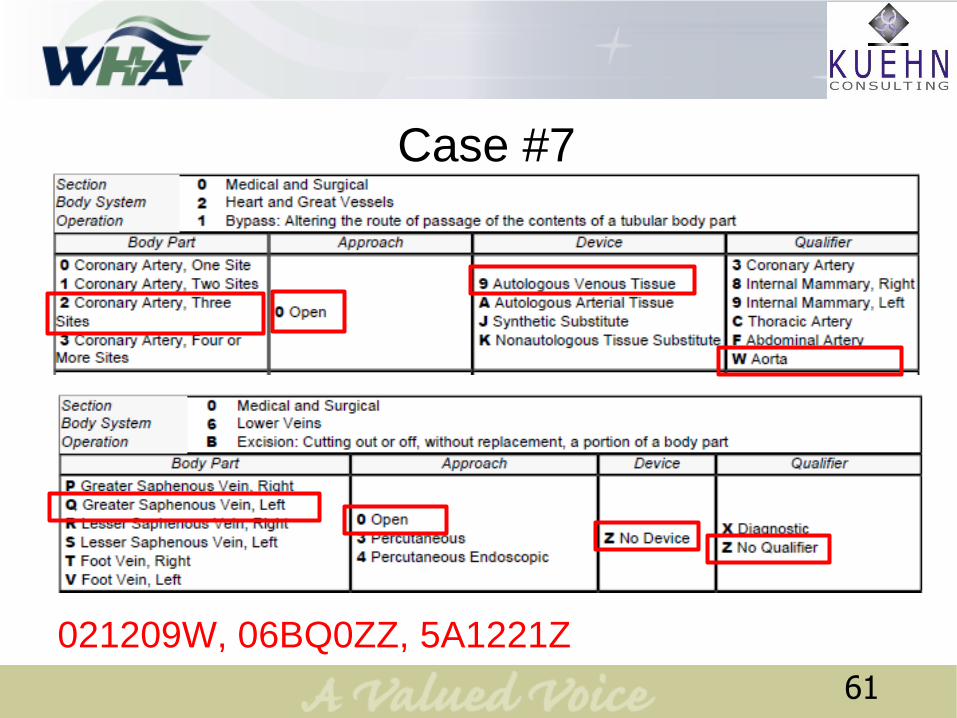
Case #7
021209W, 06BQ0ZZ, 5A1221Z
61
Moving Group
62
• Reposition only
involves body parts,
not devices.
• Reattachment is
coded when a body
part has become
separated from the
body (not by the
surgeon).
63
Case #8Procedure: Left Triceps Brachii Distal Tendon Repair
With the patient under general anesthesia, a straight posterior midline incision was
performed with the patient in the lateral decubitus position and the arm over a tibial
post. Dissection was performed through skin and subcutaneous tissues, identifying
the triceps tendon. The edges of the ruptured triceps tendon were debrided, and a
#5 Ethibond suture was inserted through the tendon using a Bunnell stitch
technique. Next, needles were drilled through the olecranon in a crossed pattern.
To improve fixation, 2 to 3 suture anchors were drilled into the olecranon for
augmentation of the reattachment; the sutures of the bone anchors were passed
through the tendon in a horizontal mattress pattern. The Ethibond suture was
inserted into the holes of the Keith needles and advanced through the olecranon by
advancing the needles. With the elbow in extension, the tendon was reattached to
the olecranon; the Ethibond sutures were tied first, followed by the bone anchor
sutures. Stability of the reattachment was evaluated intraoperatively by moving the
elbow through its total range of motion. The wound was irrigated and closed in
layers.
64
Case #8
65
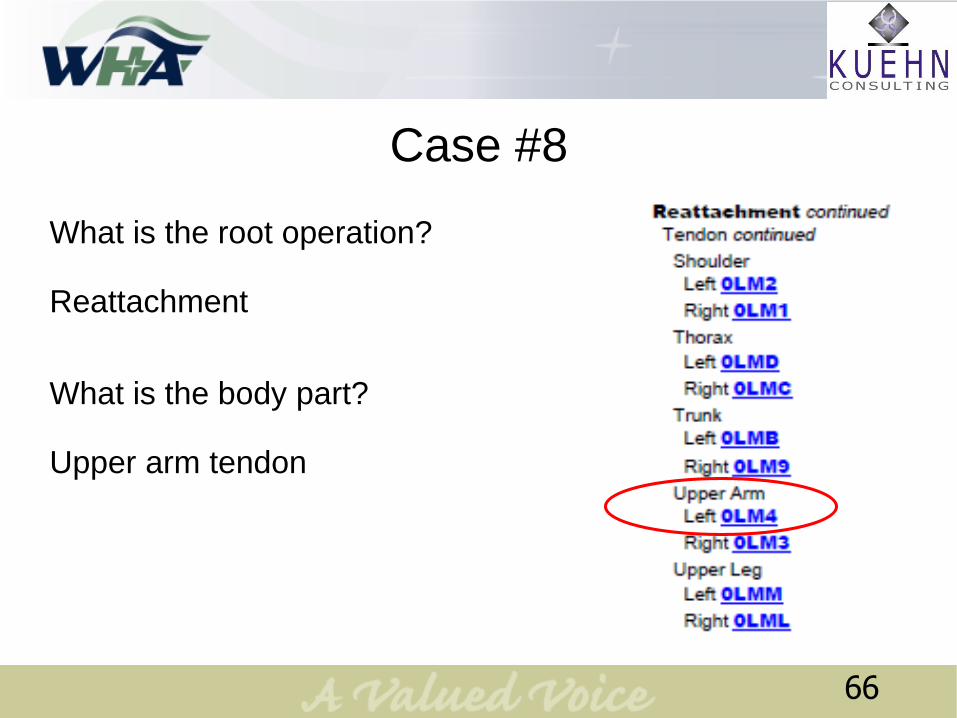
Case #8
What is the root operation?
Reattachment
What is the body part?
Upper arm tendon
66
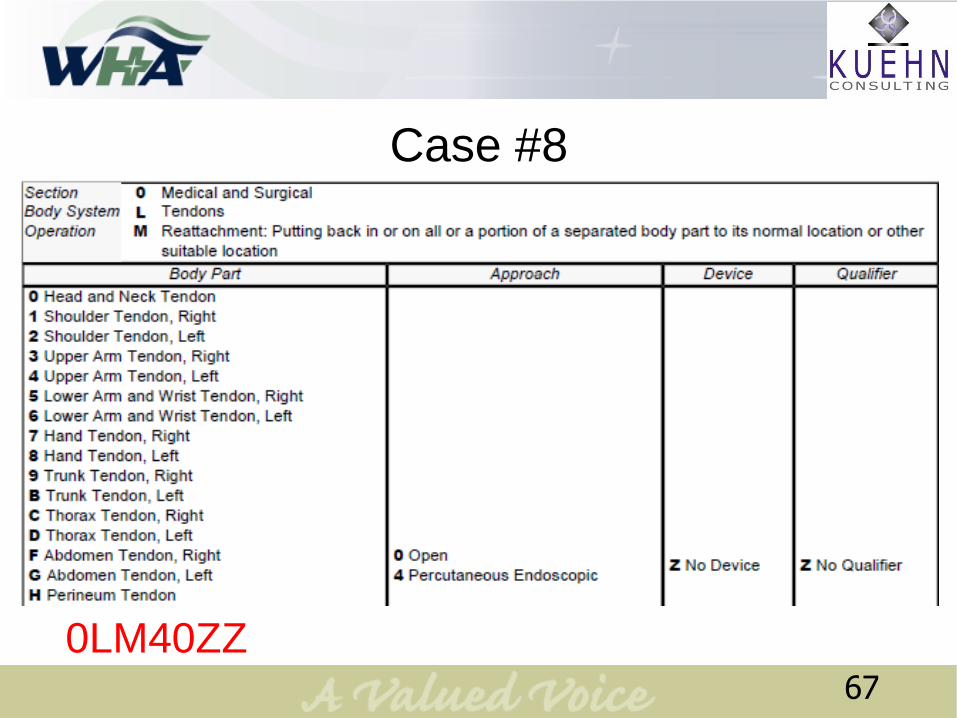
Case #8
0LM40ZZ67
Case #9
Preoperative Diagnosis: Pacemaker malfunction
Postoperative Diagnosis: Same
Anesthesia: Local
Operation Performed: Repositioning of pacemaker electrode
Procedure: The patient was positioned on the fluoroscopy table and the
right chest was prepared and draped. Local anesthesia was obtained with
1% lidocaine with epinephrine. The pocket was opened and the right
ventricular lead was identified and disconnected from the generator. The
lead was gently advanced under fluoroscopy until it was properly situated
in the ventricle. It was sutured in place using 2-0 silk and reconnected to
the generator. Hemostasis was achieved. The wound was closed using 3-0
Vicryl for subcutaneous tissue and 3-0 nylon for skin. Dry dressings were
applied, and the patient was returned to the recovery room in satisfactory
condition.
68
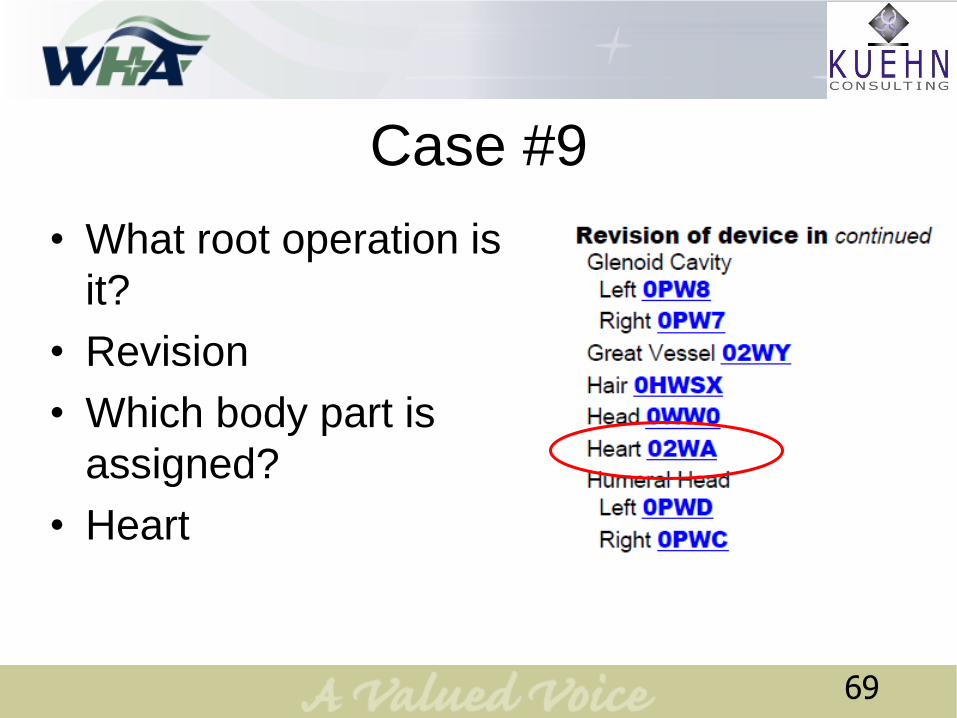
Case #9
• What root operation is
it?
• Revision
• Which body part is
assigned?
• Heart
69
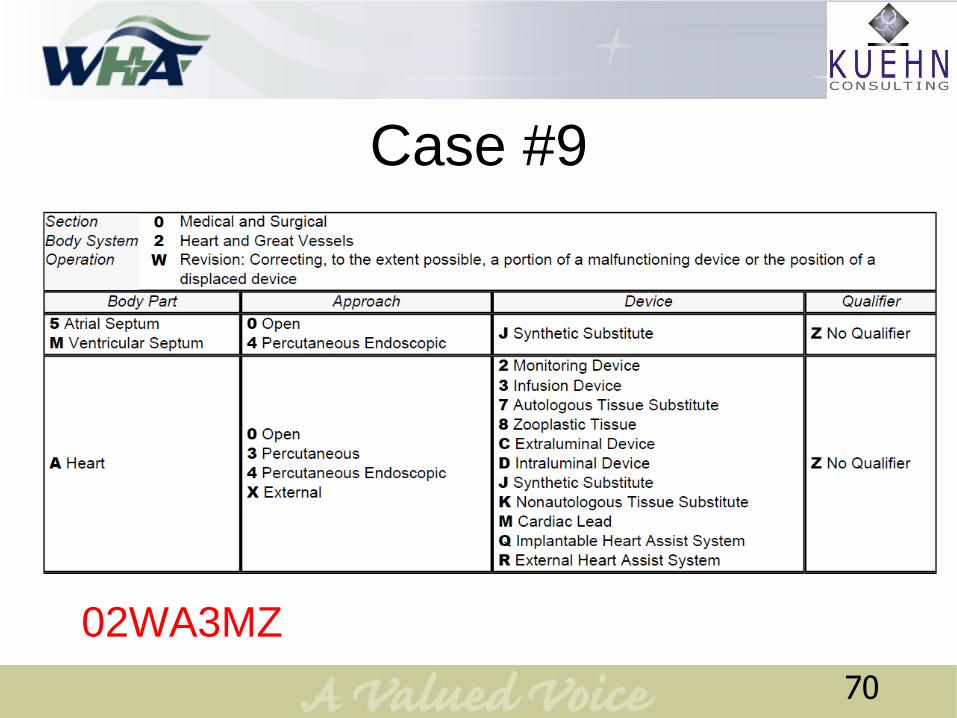
Case #9
02WA3MZ
70
Case #10 – Poll Question
The patient has a perforated duodenal ulcer.
The surgeon explores the abdomen and
performs a Graham omentoplasty by sewing a
flap of omentum over the ulcer.
1. Transfer
2. Supplement
3. Repair
71
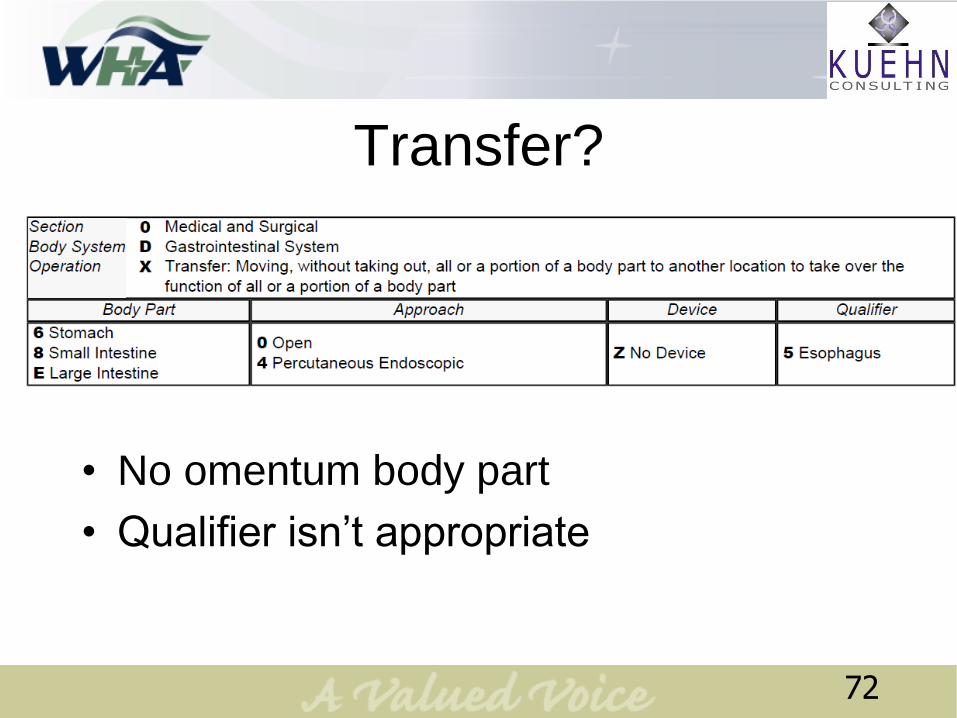
Transfer?
72
• No omentum body part
• Qualifier isn’t appropriate
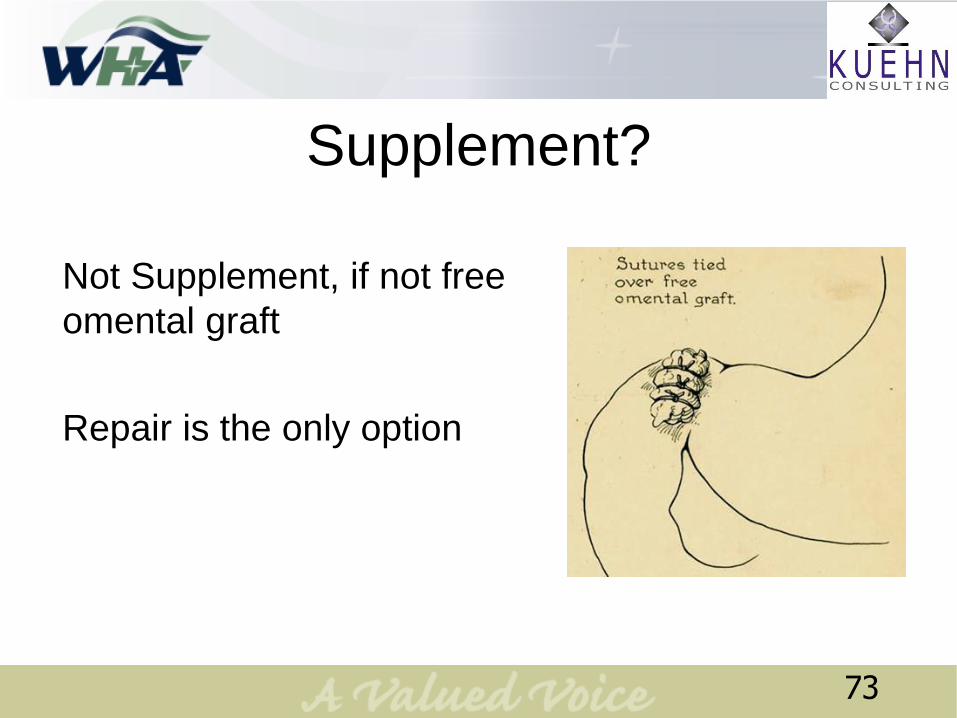
Supplement?
Not Supplement, if not free
omental graft
Repair is the only option
73

Case #10
0DQ90ZZ74
Summary
• You’ve learned:
– Determining the group and the root
operation is based on the intent
– To tell the difference between root
operations that seem similar and why
– To assign root operations and codes to 10
complex ICD-10-PCS
• Next Step: Use these skills to code!
75
Questions?
76
Thank you!
Contact Information:
Lynn Kuehn, MS, RHIA, CCS-P, FAHIMA
President
Kuehn Consulting, LLC
Waukesha, WI
O: 262-574-1064
F: 262-574-0828
www.KuehnConsulting.com
Contact Information:
Jennifer Frank,
Vice President Education
Wisconsin Hospital Association
O: 608-274-1820
F: 608-274-8554
http://www.wha.org
77