Embed Size (px)
Citation preview

J A C C : C A R D I O V A S C U L A R I M A G I N G VO L . 1 2 , N O . 1 , 2 0 1 9
ª 2 0 1 9 B Y T H E AM E R I C A N C O L L E G E O F C A R D I O L O G Y F O UN DA T I O N
P U B L I S H E D B Y E L S E V I E R
ORIGINAL RESEARCH
Comprehensive EchocardiographicAssessment of Normal TranscatheterValve Function
Rebecca T. Hahn, MD,a Jonathon Leipsic, MD,b Pamela S. Douglas, MD,c Wael A. Jaber, MD,d Neil J. Weissman, MD,ePhilippe Pibarot, DVM, PHD,f Philipp Blanke, MD,b Jae K. Oh, MDg
ABSTRACT
ISS
Fro
Co
an
Re
Ins
PA
Me
We
wh
for
Co
the
Ed
Sci
Ma
OBJECTIVES This study aims to establish parameters for identifying normal function for each of the 3 iterations of
balloon-expandable valves and 2 iterations of self-expanding valves.
BACKGROUND Expected transthoracic echocardiographic Doppler-derived hemodynamic data for transcatheter aortic
valves inform pre-implant decision-making and post-implanted monitoring of longitudinal valve function.
METHODS We collected the echocardiography core Lab measured mean gradients and effective orifice area (EOA) from
discharge or 30-day echocardiograms from randomized trials; the PARTNER (Placement of Aortic Transcatheter Valves)
trials for the balloon-expandable valves and the Medtronic CoreValve US Pivotal trial and Medtronic CoreValve Evolut R
United States IDE Clinical Study for the self-expanding valves.
RESULTS For all SAPIEN (Edwards Lifesciences, Irvine, California) valve sizes, mean EOA is 1.70 � 0.49 cm2 with a
mean gradient of 9.36 � 4.13 mm Hg. For all SAPIEN XT valve sizes, mean EOA is 1.67 � 0.46 cm2 with a mean gradient
of 9.52 � 3.64 mm Hg. For all SAPIEN 3 valve sizes, the mean EOA is 1.66 � 0.38 cm2 with a mean gradient of 11.18 �4.35 mm Hg. For all CoreValve valve sizes, the mean EOA is 1.88 � 0.56 cm2 with a mean gradient of 8.85 � 4.14
mm Hg. For all Evolut R valve sizes, the mean EOA is 2.01 � 0.65 cm2 with a mean gradient of 7.52 � 3.19 mm Hg. The
SAPIEN 3 post-implant EOA was progressively larger for each quintile of baseline annular area by computed tomog-
raphy (p < 0.001). Similarly, for the Evolut R valve, post-implantation EOA was significantly larger for each quintile of
baseline annular perimeter (p < 0.001).
CONCLUSIONS Tables of expected mean transcatheter aortic valve hemodynamics by valve type and size are essential
in evaluating the function of these transcatheter prosthetic valves. Tables of expected EOA by the native annular anatomy
may be useful for pre-implantation decision making. Criteria for defining structural valve dysfunction are proposed.
(J Am Coll Cardiol Img 2019;12:25–34) © 2019 by the American College of Cardiology Foundation.
N 1936-878X/$36.00 https://doi.org/10.1016/j.jcmg.2018.04.010
m the aColumbia University Medical Center/New York-Presbyterian Hospital, New York, New York; bUniversity of British
lumbia and St. Paul’s Hospital, Vancouver, Canada; cDivision of Cardiovascular Medicine, Duke University Medical Center,
d Duke Clinical Research Institute, Durham, North Carolina; dCleveland Clinic Foundation, Cleveland, Ohio; eMedstar Health
search Institute, Washington, DC; fInstitut Universitaire de Cardiologie et de Pneumologie de Québec/Québec Heart & Lung
titute, Department of Medicine, Laval University, Québec, Canada; and the gMayo Clinic, Rochester, Minnesota. The
RTNER 1 and PARTNER 2 Trials were sponsored by Edwards Lifesciences. The Medtronic CoreValve US Pivotal trial and
dtronic CoreValve Evolut R United States IDE Clinical Study were sponsored by Medtronic. Drs. Pibarot, Hahn, and
issman are the Directors of the Echocardiography Core Labs for the P2S3 Trials (sponsored by Edwards Lifesciences) for
ich they receive no direct compensation. Drs. Blanke and Leipsic are the Co-Directors of the CT Core lab for the P2S3 Trial
which they receive no direct compensation. Dr. Jaber is the Director of the Echocardiography Core Lab for PARTNER II,
horts A and B (sponsored by Edwards Lifesciences) for which he receives no direct compensation. Dr. Oh is the Director of
Echocardiography Core Lab for CoreValve/Evolut R; and a consultant for Medtronic. Dr. Leipsic is a consultant for
wards. Dr. Douglas has received a grant from Edwards Lifesciences. Dr. Weissman has received grants from Boston
entific, Edwards, Medtronic, Abbott, and LivaNova. Dr. Blanke is a consultant with Edwards Lifesciences.
nuscript received March 30, 2018; revised manuscript received April 9, 2018, accepted April 10, 2018.

ABBR EV I A T I ON S
AND ACRONYMS
2D = 2-dimensional
AS = aortic stenosis
CT = computed tomography
DVI = Doppler velocity index
ECL = echo cardiography core
lab
EOA = effective orifice area
EOAi = effective orifice area
indexed to body surface area
LVOT = left ventricular
outflow tract
TAVR = transcatheter aortic
valve replacement
THV = transcatheter
heart valve
VTI = velocity time integral
Hahn et al. J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 1 , 2 0 1 9
Hemodynamic Function TAVR J A N U A R Y 2 0 1 9 : 2 5 – 3 4
26
A s the indications for transcatheteraortic valve replacement (TAVR)continue to broaden, with low-risk
studies as well as moderate aortic stenosis(AS) studies underway (1), the number oftranscatheter heart valve (THV) implanta-tions continue to grow. Current AmericanHeart Association/American College of Cardi-ology guidelines (2) indicate that TAVR is aClass I intervention for severe, symptomaticAS in inoperable or high-risk patients, andClass IIa intervention for those of intermedi-ate surgical risk. In the recent report of theSociety of Thoracic Surgeons (STS)/AmericanCollege of Cardiology Transcatheter ValveTherapy Registry (3), 54,782 patients had aTAVR between 2012 and 2015. There was aprogressive reduction in the STS predictedrisk of mortality (PROM) from 7% to 6%,
and TAVR PROM (transcatheter valve therapyPROM) from 4% to 3% (both p < 0.0001) from 2012to 2015. TAVR continues to change the algorithm fortreatment of severe, symptomatic aortic stenosiswith the first Appropriate Use Criteria report for thetreatment of patients with AS developed to informdecision-making, improve the quality of patientcare, and assist education initiatives (4).
SEE PAGE 35
With recent reports of THV thrombus and leafletthickening (5,6), questions about THV hemodynamicshave been raised for both surgical (7,8) and trans-catheter valves (9). The Valve-in-Valve InternationalData Registry (8) reported a time-to-intervention forbioprosthetic valve failure of only 9 years (inter-quartile range: 6 to 12 years). Assessment of longitu-dinal hemodynamics from the PARTNER (Placementof Aortic Transcatheter) trial (9) has shown that at amedian follow-up of 3.1 years (maximum of 5 years);there were no significant hemodynamic changes seenin this TAVR population. Longer follow-up will beneeded to address long-term durability questions.
Longitudinal echocardiographic follow-up remainsan essential tool for assessing valve deterioration. Anumber of societal guidelines for the echocardio-graphic assessment of prosthetic valve function havebeen published (10,11). Important measurementsinclude the peak and mean transvalvular gradients,effective orifice area (EOA) by the continuity equation,and Doppler velocity index (DVI). Recent clinical trialdata and registries have reported “normal” values forboth early iterations of the balloon-expandable andself-expanding valves based on implanted valve size(12,13). Similar to common practice with surgical
prostheses, a complete assessment of prosthetic valvefunction requires an understanding of the constructand appearance of each THV and the normal functionof each type and size of implanted valve. Unlike thesurgical valves, the transcatheter valves expand to fillthe annular space. Thus pre-procedural computed to-mography (CT), which has been integral to the sizing ofthese valves, may also allow clinicians to estimate theexpected valve area before implantation. Normativedata of commercially available THVs by valve type andsize are herein reported, along with normal referencevalues for each valve type by pre-procedural CTmeasured native annular measurements, based oncomplete data from echocardiographic core labassessed hemodynamics from early randomized trialsand registries (12,14,15).
METHODS
Mean gradients and EOA were measured by theechocardiography core lab (ECL) (for PARTNER 1[including the continued access registry]: Duke Clin-ical Research Institute, Durham, North Carolina; ForPARTNER 2A and 2B [including nested registries]: C5Research, Cleveland Clinic, Cleveland, Ohio; forPARTNER 2 S3: Quebec Heart & Lung Institute,Quebec, Canada; Cardiovascular Research Founda-tion, New York, New York; and Medstar HealthResearch Institute, Washington, DC) on the dischargeor 30-day studies in the PARTNER database: for theSAPIEN (Edwards Lifesciences, Irvine, California)valve (n ¼ 2,509) this included patients receivingTAVR in PARTNER I and PARTNER I continued accessregistries; for the SAPIEN XT valve (Edwards Life-sciences, Irvine, California) (n ¼ 596) this includedpatients randomized to SAPIEN XT in the PARTNERIIA or IIB trial (including the alternative access and29-mm valve nested registries); for the SAPIEN 3valve (n ¼ 1,657) this included patients in the PART-NER II – SAPIEN 3 registry. Salient differences in theSAPIEN family of valves are listed in Table 1.
ECL (Mayo Clinic, Rochester, Minnesota) assessedforward flow hemodynamics at 30 days with theCoreValve (Medtronic, Minneapolis, Minnesota) bio-prostheses were obtained from the TAVR cohorts inthe CoreValve US Pivotal Extreme Risk (n ¼ 489) andHigh Risk (n ¼ 391) trials (16,17). Hemodynamic dataat 30 days with the Evolut R (Medtronic) valveincluded 301 implanted patients from the MedtronicCoreValve Evolut R United States IDE Clinical Study(18,19). Valve descriptions are included in Table 1.
MULTIDETECTOR CT MEASUREMENTS. Pre-implan-tation CT images for a subset of the balloon-expandable valves (primarily the intermediate-risk

TABLE 1 Types of Transcatheter Aortic Valves and Their Respective Design Features
Valve Features
Balloon-expandablevalve iterations
SAPIEN valve � Trileaflet bioprosthesis made of bovine pericardium that is mounted on a balloon-expandable stainless steel stent.� The stent frame has an inner polyethylene terephthalate (PET) fabric skirt placed on the ventricular side covering
half of the frame, limiting stent expansion and decreasing paravalvular insufficiency.� Available in 2 sizes: 23 and 26 mm, allowing for the treatment of patients with aortic annuli
ranging from 18 to 24 mm.
SAPIEN XT � Cobalt chromium, balloon-expandable stent with an integrated trileaflet bovine tissue valve and an inner fabricskirt on the ventricular side.
� Changes in the stent material and design, as well as the ability to mount the valve on the deployment ballooninside the abdominal aorta, allows for a smaller delivery system.
� Available in 3 valve sizes: 23, 26, and 29 mm, allowing for the treatment of patients with aortic annuli ranging from18 to 27 mm.
SAPIEN 3 � Cobalt chromium, balloon-expandable stent with wide strut angles providing a low delivery profile and anenhanced frame geometry for greater radial strength.
� The inflow portion of the valve has a PET fabric cuff in addition to an internal skirt to minimize paravalvular leak. Ithas a smaller crimped profile and a longer stent frame compared to the first- and second-generationSAPIEN valves.
� Available in 4 sizes: 20, 23, 26, and 29 mm, allowing for the treatment of patients with aortic annuli ranging from16 to 28 mm.
Self-expanding valveiterations
CoreValve � A porcine pericardial supra-annular valve within a self-expanding Nitinol frame.� Available in 4 sizes: 23, 26, 29, and 31 mm, allowing for the treatment of patients with aortic annuli ranging from
18 to 29 mm. All sizes delivered via an 18-F catheter delivery system.
Evolut R � A porcine pericardial supra-annular valve within a self-expanding Nitinol frame.� Available in 4 sizes: 23, 26, 29, and 34 mm, allowing for the treatment of patients with aortic annuli ranging from
18 (17 mm for failed surgical valves) to 30 mm.� The 23-, 26-, and 29-mm valves are delivered via a 14-F equivalent catheter delivery system. The 34-mm valve is
delivered with a 16-F equivalent delivery system.� The valve can be partially or fully recaptured before final valve placement.
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 1 , 2 0 1 9 Hahn et al.J A N U A R Y 2 0 1 9 : 2 5 – 3 4 Hemodynamic Function TAVR
27
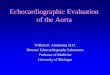
group) were analyzed using standard methodology(20). Left ventricular outflow tract (LVOT) measure-ments were obtained by convention immediatelybelow the annular plane (Figure 1A). All CT examina-tions were reviewed and interpreted in a central corelaboratory (St Paul’s Hospital, Cardiac CT Laboratory,Vancouver, University of British Columbia). When CTwas not adequate, 3-dimensional (3D) transesophagealechocardiography annular area was measured (21).EOA by quintiles of annular area are reported.
For the CoreValve and Evolut R THVs, the aorticannular perimeter was measured from 3D recon-struction of CT images at each site.
ECHOCARDIOGRAPHIC MEASUREMENTS FOR
BALLOON-EXPANDABLE VALVES. Peak and meangradients across the aortic valve were performedusing continuous wave Doppler. Measurements ofneo-LVOT diameter were performed from 2 locations(Figure 1B): 1) the outer-to-outer border of the stentedvalve (blue arrow); and 2) in-stent measurement at themid-stent level (red arrow). Pulsed-wave Doppler wasperformed at 2 locations: 1) sample volume just apicalto THV stent (Figure 1C); and 2) Sample volume withinTHV stent on left ventricular side of aortic valve leaf-lets (Figure 1D). Calculation of left ventricular strokevolume was performed by pairing the LVOT diametermeasurement with the appropriate pulsed-wave
spectral Doppler measurement of the velocity timeintegral (VTI), preferentially using the outer-to-outerstent diameter/pre-stent VTI. The in-stent measure-ments were only used if the outer-to-outer measure-ments could not be accurately assessed, typically inthe setting of a low valve implantation. Once the leftventricular stroke volume was calculated, the EOAwas calculated by dividing the stroke volume bytransaortic continuous wave Doppler VTI.
ECHOCARDIOGRAPHIC MEASUREMENTS FOR SELF-
EXPANDING VALVES. The neo-LVOT diameter wasmeasured from the outer-to-outer border of thestented valve at its ventricular tip consistent with themethodology used for prosthetic surgical valves(Figure 2) (10). When the outer-to-outer border mea-surement of the prosthesis was difficult due to diffi-cult image quality, the prosthesis tip was insertedinto the left ventricular cavity, or there was systolicanterior motion of the mitral valve, stroke volumemeasured by 2D disc method (22) was used for thecalculation of EOA as long as there was no more thantrivial degree of mitral regurgitation. Pulsed-waveDoppler was performed by placing the sample vol-ume just apical to the THV stent. Peak instantaneousand mean gradients across the aortic prosthesis weremeasured by continuous wave Doppler, most fromapical window, but occasionally from the right

FIGURE 1 Multislice Computed Tomography and Echocardiographic Measurements
A
Min. Ø: 22.3 mmMax. Ø: 28.0 mmAvg. Ø: 25.1 mmArea: 504.2 mm2
Perimeter: 80.5 mm
LC
NC
RC
LV
1
2
Ao
LA
Annular Area = 504.2 mm2
Annular perimeter = 80.5 mm
B C
D
(A) MSCT measurements of the annulus were performed immediately below the hinge points of the coronary cusps. (B) The calculation of EOA required calculation of
left ventricular stroke volume using the outer-to-outer diameter of the stented valve (blue arrow 1) paired with the pulsed wave Doppler placed just apical to the
stented valve (C). If the outer-to-outer diameter of the valve could not be measured accurately, the in-stent measurement (B, red arrow 2) would then be paired with
the pulsed wave Doppler placed within the stented valve (D). Ao ¼ aorta; EOA ¼ effective orifice area; LA ¼ left atrium; LV ¼ left ventricle; MSCT ¼ multislice
computed tomography.
Hahn et al. J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 1 , 2 0 1 9
Hemodynamic Function TAVR J A N U A R Y 2 0 1 9 : 2 5 – 3 4
28
parasternal location. The DVI was calculated as theratio of the LVOT VTI to the aortic valve VTI.
STATISTICS. Balloon-expandable valve. For the SA-PIEN family of valves, 3 generations of valves from thePARTNER database, SAPIEN, SAPIEN XT, and SAPIEN3, are included. Salient differences among the valvesin the SAPIEN family are listed in Table 1. SAPIEN pa-tients are from PARTNER 1 and its continued accessregistries. SAPIEN XT patients are from PARTNER 2Aand PARTNER 2B with its nested registries. SAPIEN S3patients are from PARTNER 2 S3 registries. The mainvariables for comparison are aortic valve meangradient (mm Hg), EOA (cm2), and DVI. Mean gradientand EOA were measured by ECL during each trialfollow-up period. DVI (LVOT TVI / aortic valve VTI) isderived from LVOT pulsed-wave VTI and aortic valvecontinuous-wave VTI, both of which were alsomeasured by echo core labs. The measurements at 30-days or discharge are selected for analysis. The maininclusion criteria are TAVR as actual treatment andhaving non-missing values for mean gradient, EOA,DVI, and valve size. Patients undergoing valve-in-valve TAVR are excluded. There are a total of 5,283subjects eligible for analysis with 2,342 in the SAPIENgroup, 1,471 in the SAPIEN XT group, and 1,470 in theSAPIEN 3 group. The echo variables are reported bymean � SD for each valve type and for each valve size
within the same valve type (Table 2). The differencesamong valve sizes within each SAPIEN type arecompared by Student’s t-test or analysis of variance F-test. All analysis is performed using SAS version 9.4(SAS Institute, Inc., Cary, North Carolina).
Self-expanding valve. The aortic valve mean gradient,EOA, and the LVOT VTI and aortic valve VTI (used tocalculate the DVI) at 30 days were included. All mea-surements were centrally assessed by the ECL duringeach trial. The patient cohort comprises patients whowere successfully implanted with 1 THV in the nativeaortic valve, and who have non-missing data for themean gradient, EOA, DVI, and valve size. The echovariables are reported by mean � SD and also for eachvalve size within the same valve type (Table 2). Thedifferences among valve sizes were compared by theanalysis of variance F-test. For the comparisonsamong quintiles of perimeter-derived annulus diam-eter, a trend test was performed using a generalizedlinear model with quintiles as an independent ordinalvariable. All analyses were performed using SASversion 9.4.
RESULTS
Table 2 shows the mean gradients, EOA, and DVI foreach balloon-expandable valve iteration by valve size

FIGURE 2 Measurement of Self-Expanding Valve Area
A
LV
LA
Ao
B
C
(A) A zoomed systolic still frame image of the LVOT with the outer-to-outer stent diameter measurement (yellow arrow). (B) A pulsed-wave
Doppler recording of LVOT velocity (sample volume apical to transcatheter valve in systole) which is paired with a continuous wave Doppler
velocity recording from the stented aortic prosthesis (C). LVOT ¼ left ventricle outflow tract; other abbreviations as in Figure 1.
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 1 , 2 0 1 9 Hahn et al.J A N U A R Y 2 0 1 9 : 2 5 – 3 4 Hemodynamic Function TAVR
29
implanted. For the balloon-expandable valves, thereare significant differences in mean gradient and EOAbetween valve sizes for each iteration (p < 0.001). Forthe SAPIEN XT and SAPIEN 3 valves, the DVIremained significantly different between valve sizes
TABLE 2 Mean Gradient and EOA for Balloon-Expandable SAPIEN Va
Valve Iteration 20 23
SAPIEN
EOA, cm2 NA 1.56 � 0.43 (1,212) 1.84
Mean gradient, mm Hg NA 9.92 � 4.27 (1,212) 8.76
DVI NA 0.53 � 0.13 (1,212) 0.53
SAPIEN XT
EOA, cm2 NA 1.41 � 0.30 (545) 1.74
Mean gradient, mm Hg NA 10.41 � 3.74 (545) 9.2
DVI NA 0.52 � 0.10 (545) 0.5
SAPIEN 3
EOA, cm2 1.22 � 0.22 (47) 1.45 � 0.26 (471) 1.74
Mean gradient, mm Hg 16.23 � 5.01 (47) 12.79 � 4.65 (471) 10.5
DVI 0.42 � 0.07 (47) 0.43 � 0.08 (471) 0.4
Values are mean � SD (n). This table shows the mean gradients and EOA for each balloowere significantly different for each valve size for a given valve type (range p < 0.03 t
DVI ¼ Doppler velocity index; EOA ¼ effective orifice area; NA ¼ not available.
(p < 0.01). For the SAPIEN 3 valve, multislice CT or 3Dannular area was measured and the patient cohortdivided into quintiles. Table 3 shows the mean EOA �SD for each quintile of annular area. When indexed tobody size, there remained significant differences in
lves
Prosthetic Valve Size, mm
26 29 All Sizes p Value
� 0.52 (1,130) NA 1.70 � 0.49 (2,342) <0.001
� 3.89 (1,130) NA 9.36 � 4.13 (2,342) <0.001
� 0.13 (1,130) NA 0.53 � 0.13 (2,342) 0.64
� 0.42 (675) 2.06 � 0.52 (251) 1.67 � 0.46 (1471) <0.001
4 � 3.57 (675) 8.36 � 3.14 (251) 9.52 � 3.64 (1,471) <0.001
4 � 0.11 (675) 0.53 � 0.11 (251) 0.53 � 0.11 (1,471) 0.004
� 0.35 (626) 1.89 � 0.37 (326) 1.66 � 0.38 (1,470) <0.001
9 � 3.88 (626) 9.28 � 3.16 (326) 11.18 � 4.35 (1,470) <0.001
3 � 0.09 (626) 0.40 � 0.09 (326) 0.43 � 0.09 (1,470) <0.001
n-expandable valve iteration by valve size implanted. All mean valve areas and EOAso p < 0.0001).

TABLE 3 Normal Reference Values for the SAPIEN 3 Valve by Pre-Procedural Native Annular Area by Quintiles of 3D Annular Areas for the
Enrolled Patients
248 to 384 mm2
(n ¼ 189)385 to 439 mm2
(n ¼ 191)440 to 488 mm2
(n ¼ 192)489 to 537 mm2
(n ¼ 191)538 to 678 mm2
(n ¼ 188) p Values for Trend
EOA, cm2 1.41 � 0.27 1.58 � 0.33 1.73 � 0.36 1.79 � 0.35 1.91 � 0.42 <0.0001
EOAi, cm2/m2 0.80 � 0.16 0.86 � 0.19 0.92 � 0.21 0.90 � 0.20 0.93 � 0.21 <0.0001
Mean gradient, mm Hg 13.96 � 5.28 11.94 � 4.82 10.93 � 5.04 10.56 � 4.16 9.17 � 3.35 <0.0001
DVI 0.43 � 0.10 0.44 � 0.10 0.42 � 0.09 0.43 � 0.09 0.42 � 0.09 0.13
Values are mean � SD.
3D ¼ 3-dimensional; EOAi ¼ effective orifice area indexed to body surface area; other abbreviations as in Table 1.
Hahn et al. J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 1 , 2 0 1 9
Hemodynamic Function TAVR J A N U A R Y 2 0 1 9 : 2 5 – 3 4
30
effective orifice area indexed to body surface area(EOAi) between the smallest quintile and allother groups. Importantly, the DVI was not signifi-cantly different between quintiles of annular area(p ¼ 0.13).
Table 4 shows the 30-day mean gradients, EOA,and DVI for the CoreValve and Evolut R bioprosthesesby valve size implanted. There are significant differ-ences in mean gradient and EOA among valve sizesfor each iteration (p # 0.001). For the Evolut R valve,the DVI was not significantly different between valvesizes. Table 5 shows the EOA, EOAi, mean gradient,and DVI by quintiles of perimeter-derived annulardiameter. For the Evolut R valve, the DVI was notsignificantly different between quintiles of annulardiameter (p ¼ 0.07).
DISCUSSION
This manuscript is the first to compile the mean post-TAVR valve areas and mean gradients for the currentiterations of the balloon-expandable and self-expanding valves both by valve size and type, andalso by baseline annular dimensions. These referencetables are essential tools for: 1) comparing the imme-diate and longitudinal function of an implanted valve
TABLE 4 Mean Gradient and EOA for CoreValve and Evolut R by Valv
Valve Iteration 23 26
CoreValve
EOA, cm2 1.12 � 0.36 (19) 1.74 � 0.49 (289) 1.
Mean gradient, mm Hg 14.43 � 5.72 (22) 8.27 � 3.82 (307) 8
DVI 0.44 � 0.09 (20) 0.59 � 0.15 (300) 0
Evolut R
EOA, cm2 1.09 � 0.26 (3) 1.69 � 0.40 (71) 1
Mean gradient, mm Hg 14.97 � 7.15 (3) 7.53 � 2.65 (77) 7
DVI 0.42 � 0.04 (3) 0.61 � 0.13 (75) 0
Values are mean � SD (n). p values are from analysis of variance F-test.
Abbreviations as in Table 1.
of known size to normative core lab-assessed data; 2)assessing the immediate and longitudinal function ofan implanted valve of unknown size but known nativeannular anatomy; and 3) predicting the expected valvearea by native annular anatomy before valve implan-tation. Importantly, the methodology used by the ECLfor measuring the EOA for each valve type has beendescribed and important differences in the balloon-expandable and self-expanding valves are noted.
To assess THV longitudinal function, comparingthe patient to their own immediate post-implantationhemodynamics is highly recommended (10,11). TheValve Academic Research Consortium 2 update (23)suggests that an increase in the mean gradient >10mm Hg, a decrease in the EOA >0.3 to 0.4 cm2, or areduction in the DVI >0.1 to 0.13 probably indicates achange in valve function and should trigger acomprehensive hemodynamic evaluation. A recentanalysis of the longitudinal function of the SAPIENvalve suggested that detection of valve dysfunctioncould be broken down into early dysfunction andmore extreme valve dysfunction, the latter beingassociated with poor outcomes (9). Given the pro-gressive nature of valve dysfunction, this makesintuitive sense and a recent review by Rodriguez-Gabella et al. (24) proposes using 2 sets of criteria
e Size in Native Aortic Stenosis at 30 Days
Prosthetic Valve Size, mm
29 31 All Sizes p Value
97 � 0.53 (446) 2.15 � 0.72 (81) 1.88 � 0.56 (835) <0.001
.85 � 4.17 (478) 9.55 � 3.44 (83) 8.85 � 4.14 (890) <0.001
.54 � 0.12 (463) 0.49 � 0.12 (83) 0.55 � 0.13 (866) <0.001
.97 � 0.54 (129) 2.60 � 0.75 (52) 2.01 � 0.65 (255) <0.001
.85 � 3.08 (141) 6.30 � 3.23 (57) 7.52 � 3.19 (278) <0.001
.59 � 0.14 (135) 0.58 � 0.15 (55) 0.59 � 0.14 (268) 0.09

TABLE 5 Normal Reference Values for the CoreValve and Evolut R Valves by Native Annular Diameter Quintiles at 30 Days
Quintiles #22.8 mm >22.8 to 24.5 mm >24.5 to 25.9 mm >25.9 to 27.6 mm >27.6 to 41.5 mmp Valuefor Trend
CoreValve
EOA, cm2 1.71 � 0.55 (166) 1.80 � 0.53 (141) 1.92 � 0.48 (167) 1.94 � 0.52 (165) 2.06 � 0.66 (160) <0.001
EOAi, cm2/m2 1.03 � 0.33 (166) 1.02 � 0.30 (141) 1.04 � 0.29 (167) 1.01 � 0.30 (165) 1.07 � 0.36 (160) 0.34
Mean gradient,mm Hg
9.01 � 4.06 (180) 8.96 � 4.71 (151) 8.75 � 3.99 (179) 9.16 � 4.50 (170) 8.75 � 3.61 (171) 0.75
DVI 0.59 � 0.15 (172) 0.55 � 0.13 (145) 0.54 � 0.11 (173) 0.53 � 0.12 (167) 0.55 � 0.14 (170) 0.001
#22.3 mm >22.3 to #23.2 mm >23.2 to #24.7 mm >24.7 to #26.2 mm >26.2 to #30.2 mmp Valuefor Trend
Evolut R
EOA, cm2 1.66 � 0.42 (53) 1.82 � 0.43 (38) 1.98 � 0.56 (62) 1.98 � 0.59 (49) 2.56 � 0.77 (53) <0.001
EOAi, cm2/m2 0.99 � 0.27 (53) 1.09 � 0.26 (38) 1.10 � 0.32 (62) 1.06 � 0.34 (49) 1.29 � 0.37 (53) <0.001
Mean gradient,mm Hg
7.94 � 3.10 (58) 6.91 � 2.58 (43) 7.66 � 2.94 (63) 8.53 � 3.49 (56) 6.40 � 3.34 (57) 0.21
DVI 0.61 � 0.11 (57) 0.61 � 0.14 (41) 0.61 � 0.15 (63) 0.56 � 0.14 (51) 0.58 � 0.15 (55) 0.07
Values are mean � SD (n). Trend test p value from generalized linear modeling with quintiles as independent ordinal variable.
Abbreviations as in Tables 1 and 3.
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 1 , 2 0 1 9 Hahn et al.J A N U A R Y 2 0 1 9 : 2 5 – 3 4 Hemodynamic Function TAVR
31
for detecting early valve dysfunction and clinicallyrelevant valve dysfunction. However, the PARTNERtrial found the absolute change in EOA of $0.35 cm2
occurred in 45% to 49% of transcatheter and surgicalvalve replacement patients during the median follow-up of 3 years (9). This finding may reflect inherentdifficulties with measurement of the LVOT diameterafter prosthetic valve replacement and thus may notbe a reliable measure of longitudinal function.Indeed, Douglas et al. (9) found that poor outcomeswere associated with absolute mean gradients >40mm Hg, DVI #0.25 (guidelines definitions of “severe”native valve stenosis), and a mean gradient changeof $20 mm Hg. Given the differences in both EOA and
TABLE 6 Proposed Definitions of Structural Valve Dysfunction
Possible (Subclinical) Structural Valve Dysfunction
� Hemodynamic changea. Possible stenosis: an increase in mean transvalvular
gradient of >10 mm Hg with concomitant decrease inEOA >25% and/or DVI >20% of baseline echocardiographicassessment performed 1 to 3 months post-intervention.
b. Change in regurgitation: new onset of $ mild intraprostheticregurgitation or increase by $1 grade of pre-existentintraprosthetic regurgitation compared with baselineechocardiographic assessment performed 1 to 3 monthspost-intervention, with the resulting regurgitationgrade < moderate.
� Changes in morphology (prolapse, thickening,calcification, pannus) and/or mobility (excessive, reduced)of the bioprosthetic valve leaflets when compared withthe baseline assessment obtained in the echocardiographyperformed at 1 to 3 months post-intervention.
*A number of guidelines criteria for severe aortic stenosis have been published: 1) severepeak velocity$4.0 m/s, mean gradient$40 mmHg, and DVI<0.25; 2) severe aortic sten>4.0 m/s, mean transvalvular gradient >35 mm Hg, DVI <0.25; 3) severe aortic stevelocity $4.0 m/s, mean transvalvular gradient $35 mm Hg, DVI <0.25. Modified from
AR ¼ aortic regurgitation; EACVI ¼ European Association of Cardiovascular Imaging; o
DVI for the various valve iterations and types, it maybe more useful to use a percent change rather thanabsolute change to indicate functional deterioration.In fact, the European Association of CardiovascularImaging (EACVI) guidelines suggest using an increaseof >10 mm Hg and a reduction of EOA >25% to indi-cate probable stenosis (11). Because each iteration andvalve type has an EOA SD of w25% to 30% of the meanand a DVI SD of w20% to 25% of the mean, this al-gorithm would have some justification. Thus, wewould propose using mean gradient and percentchanges in EOA and DVI to assess longitudinal func-tion realizing that structural valve deterioration is aprogressive disease requiring separate criteria for
Clinically Relevant Structural Valve Dysfunction
� Hemodynamic changea. Probable stenosis: an increase in mean transvalvular
gradient >20 mm Hg with concomitant decrease inEOA >50% and/or DVI >40% of baseline echocardiographicassessment performed 1 to 3 months post-intervention.
b. Severe prosthetic valve aortic stenosis accordingto current guidelines.*
c. Change in regurgitation: new occurrence or increase of$1 grade of intraprosthetic AR leading to $ moderate AR
� Severe changes in morphology (flail/avulsed, thickening,calcification, pannus) and/or mobility (excessive, reduced) ofthe bioprosthetic valve leaflets when compared with thebaseline assessment obtained in the echocardiographyperformed at 1 to 3 months post-intervention.
aortic stenosis according to current ACC/AHA guidelines (2) including EOA <1.0 cm2,osis according to ASE prosthetic guidelines (10) including EOA<0.8 cm2, peak velocitynosis according to EACVI prosthetic guidelines (11) including EOA <0.8 cm2, peakRodriguez-Gabella, et al. (24).
ther abbreviations as in Table 1.

Hahn et al. J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 1 , 2 0 1 9
Hemodynamic Function TAVR J A N U A R Y 2 0 1 9 : 2 5 – 3 4
32
detection of early and late dysfunction. Table 6 ismodified from Rodriguez-Gabella et al. (24) usingthese proposed criteria.
Methods for accurate calculation of valve area afterTAVR have been described for the balloon-expandable valve (25,26). Because of flow accelera-tion within the stented valve (27), pulsed-waveDoppler of the LVOT is performed with the pulsedDoppler sample volume just apical to the proximaledge of the stent. The LVOT diameter, thus, shouldalso be measured just apical to the proximal edge ofthe stent (and thus measuring the outer-to-outerstent diameter). This diameter measurement hasbeen shown to correlate best with measurements ofmean gradient (26). If the LVOT diameter cannot beaccurately measured, the DVI is calculated and maybe a useful measurement for long-term follow-up ofvalve function. Recent reports of the PARTNER trialsuggest that the DVI in the normal balloon-expandable valve should be >0.45 (12). The currentstudy shows that the expected DVI for the SAPIEN 3valve is 0.43 � 0.09 and that of the self-expandingvalve 0.59 � 0.14. If the stent protrudes into theLVOT cavity (failing to make contact with surround-ing tissue), particularly if flow is seen around theoutside of the inflow stent, then stroke volumemeasurements using this region of the THV may beinaccurate. The inner-to-inner stent diameter atthe level of the prosthetic leaflet hinge points maythen be used, along with the pulsed-wave Dopplerat this same level. Stroke volume may also be ob-tained from 2D or 3D measurements of ventricularvolumes, unless there is significant mitral regurgita-tion. (22)
Initial studies of the self-expanding valvemeasured the LVOT diameter just below the hingepoints of the visible prosthetic leaflets, measuring theinner-to-inner stent (28). However, recent trials haveused the outer-to-outer edge of the ventricular edgeof the THV (15). Validation of this method comparedto previously described methods for calculating theEOA of the self-expanding THV is lacking. However,the average stroke volume measured by the outer-to-outer method was within 3 to 5 ml of the stroke vol-ume measured by the 2D volumetric method (15).Hence, the ECL methods used for the self-expandingvalve are similar methods to the ones described forthe balloon-expandable valve: the LVOT diameterwith normal THV position (and stent apposition toadjacent tissue) should be measured from the outer-to-outer stent borders and just apical to the loweststent edge. When the lower stent frame protrudesinto the LV cavity, there was systolic anterior motionof the mitral valve, or imaging quality was too poor to
measure; the stroke volume from 2D ventricular vol-ume determination was used as long as there was nomore than trivial degree of mitral regurgitation.Because recent studies have suggested that thenitinol frame of the CoreValve Classic (first genera-tion) may continue to expand over time (15), re-measurement of the outer-to-outer stent diametermust be performed for this valve at baseline andduring each follow-up study; however, the changewas quite small (from 2.03 cm at discharge to 2.09 cmat 1 year) (9).
This study is the first to report valve area byquintiles of annular dimensions. Unlike a surgicalvalve with a fixed size and sewing ring, the trans-catheter valves are sized by the native annular area(29,30) with the expectation of expanding the valveto fit securely into the annulus. Pre-procedural de-cisions about valve size are, however, not entirelydependent on annular dimensions but also includeconsiderations of coronary height, aortic size, anddegree/pattern of calcification. In the border zonesbetween valve sizes, a smaller or larger valve maybe chosen based on these other anatomic assess-ments. Both 23- and 26-mm balloon-expandablevalves could result in the same EOA if the annulardimensions were the same. Since the EOA of anormally functioning transcatheter valve with agiven size may vary depending on patient’s annulusarea and degree of oversizing, another measure ofTHV function may be the expected EOA expressedaccording to aortic annulus area (11).
Having information about the expected EOA forany given annular area may be particularly helpful inpre-procedural decision-making. TAVR has beenshown to have less prosthesis-patient mismatch(PPM) than surgical aortic valve replacement (AVR)(31). Poor outcomes associated with PPM for surgicalAVR has been well-described (12,31,32) but recentreports of poor outcomes with PPM after balloon-expandable and self-expanding TAVR (31,33) suggestthat avoiding PPM may an important variable in pre-procedural planning. Although valve choice is amultifactorial heart team decision, as the indicationsfor TAVR have moved toward the lower risk groups ofpatients in whom surgical AVR may also be an option,tables of expected valve areas based on annular di-mensions or valve size may be a useful tool in theheart team decision-making process.STUDY LIMITATIONS. These results represent ECLassessed measurements of hemodynamics, EOA,and annular measurements, and may not be repre-sentative of site-measured values. The hemody-namics of the small number of patients receivingthe 23-mm CoreValve (n ¼ 19) and Evolut R (n ¼ 3)

PERSPECTIVES
COMPETENCY IN PATIENT CARE AND PROCEDURAL
SKILLS: Tables of normal reference values for mean gradients
and EOA for valve type and size provide actual hemodynamic
data that may be useful for assessing initial and longitudinal THV
function. We have described not only the methods for perform-
ing the calculation of EOA for the balloon-expandable and self-
expanding transcatheter aortic valves, but also compiled the ECL
measured mean gradients, EOA, and DVI for each valve size.
Because transcatheter valve expansion is dependent on native
aortic annular anatomy, tables listing the expected EOA for each
valve type are also reported by the native annular area or
perimeter.
TRANSLATIONAL OUTLOOK: Based on the expected mean
and SD of transcatheter EOA and DVI, the assessment of longi-
tudinal function using mean gradients and percent changes in
EOA or DVI has been proposed. Additional studies using these
criteria to determine longitudinal transcatheter valve durability
should be performed. In addition, studies are required to deter-
mine if outcomes can be predicted using these suggested criteria.
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 1 , 2 0 1 9 Hahn et al.J A N U A R Y 2 0 1 9 : 2 5 – 3 4 Hemodynamic Function TAVR
33
will require confirmation. Between-iteration com-parisons are limited by: 1) differences in both CoreLabs and patient cohorts; and 2) differences innominal sizes for each labeled valve size. However,we believe the purpose of this paper is not tocompare prior iterations or valve types, but ratherto present tables of expected normal values thathave been measured by ECL. Quintiles for the self-expanding valve are not likely to reflect the distri-bution of annular sizes for patients encountered inclinical practice because not all valve sizes wereavailable through the duration of the trials. Impor-tantly, these tables should not be used to assess thefunction of transcatheter valves placed into failingbiological valves, which were not included in thisanalysis. Finally, this is a report of the commerciallyavailable valves that will be commonly encounteredin clinical practice. Tables of expected hemody-namic variable for newer generations of valvesshould be developed.
CONCLUSIONS
Tables of normal reference values for mean gradientsand EOAs for valve type and size provide actual he-modynamic data that may be useful for assessinginitial and longitudinal THV function. The estimationof expected post-TAVR valve area by annular mea-surement may be important for pre-procedural plan-ning, particularly when assessing a patient forprosthesis-patient mismatch and deciding betweensurgical and transcatheter options.
ACKNOWLEDGMENTS The authors thank YangboLiu, MS (Cardiovascular Research Foundation) and
Jane Moore, MS (Medtronic), for assistance with datacoordination and statistical analysis.
ADDRESS FOR CORRESPONDENCE: Dr. Rebecca T.Hahn, Columbia University Medical Center, NewYork-Presbyterian Hospital, 177 Fort WashingtonAvenue, New York, New York 10032. E-mail: [email protected].
RE F E RENCE S
1. Capodanno D, Leon MB. Upcoming TAVI trials:rationale, design and impact on clinical practice.EuroIntervention 2016;12:Y51–5.
2. Nishimura RA, Otto CM, Bonow RO, et al. 2017AHA/ACC Focused update of the 2014 AHA/ACCguideline for the management of patients withvalvular heart disease: a report of the AmericanCollege of Cardiology/American Heart Associationtask force on clinical practice guidelines. J Am CollCardiol 2017;70:252–89.
3. Grover FL, Vemulapalli S, Carroll JD, et al. 2016Annual report of The Society of Thoracic Sur-geons/American College of Cardiology Trans-catheter Valve Therapy Registry. J Am Coll Cardiol2017;69:1215–30.
4. BonowRO,BrownAS,GillamLD, etal. ACC/AATS/AHA/ASE/EACTS/HVS/SCA/SCAI/SCCT/SCMR/STS2017 appropriate use criteria for the treatment of
patients with severe aortic stenosis: a report ofthe American College of Cardiology AppropriateUse Criteria Task Force, American Association forThoracic Surgery, American Heart Association,American Society of Echocardiography, EuropeanAssociation for Cardio-Thoracic Surgery, HeartValve Society, Society of CardiovascularAnesthesiologists, Society for CardiovascularAngiography and Interventions, Society ofCardiovascular Computed Tomography, Societyfor Cardiovascular Magnetic Resonance, and So-ciety of Thoracic Surgeons. J AmColl Cardiol 2017;70:2566–98.
5. Makkar RR, Fontana G, Jilaihawi H, et al.Possible subclinical leaflet thrombosis in bio-prosthetic aortic valves. N Engl J Med 2015;373:2015–24.
6. Chakravarty T, Søndergaard L, Friedman J, et al.Subclinical leaflet thrombosis in surgical and
transcatheter bioprosthetic aortic valves: anobservational study. Lancet 2017;389:2383–92.
7. Dvir D, Webb J, Brecker S, et al. Transcatheteraortic valve replacement for degenerative bio-prosthetic surgical valves: results from the globalvalve-in-valve registry. Circulation 2012;126:2335–44.
8. Dvir D, Webb JG, Bleiziffer S, et al. Trans-catheter aortic valve implantation in failed bio-prosthetic surgical valves. JAMA 2014;312:162–70.
9. Douglas PS, Leon MB, Mack MJ, et al. Longi-tudinal hemodynamics of transcatheter and sur-gical aortic valves in the PARTNER trial. JAMACardiol 2017;2:1197–206.
10. Zoghbi WA, Chambers JB, Dumesnil JG, et al.Recommendations for evaluation of prostheticvalves with echocardiography and Doppler ultra-sound: a report from the American Society of

Hahn et al. J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 1 , 2 0 1 9
Hemodynamic Function TAVR J A N U A R Y 2 0 1 9 : 2 5 – 3 4
34
Echocardiography’s Guidelines and StandardsCommittee and the Task Force on ProstheticValves, developed in conjunction with the Amer-ican College of Cardiology Cardiovascular ImagingCommittee, Cardiac Imaging Committee of theAmerican Heart Association, the European Asso-ciation of Echocardiography, a registered branchof the European Society of Cardiology, the Japa-nese Society of Echocardiography and the Cana-dian Society of Echocardiography, endorsed by theAmerican College of Cardiology Foundation,American Heart Association, European Associationof Echocardiography, a registered branch of theEuropean Society of Cardiology, the JapaneseSociety of Echocardiography, and Canadian Soci-ety of Echocardiography. J Am Soc Echocardiogr2009;22:975–1014; quiz 1082–4.
11. Lancellotti P, Pibarot P, Chambers J, et al.Recommendations for the imaging assessment ofprosthetic heart valves: a report from the Euro-pean Association of Cardiovascular Imagingendorsed by the Chinese Society of Echocardiog-raphy, the Inter-American Society of Echocardi-ography, and the Brazilian Department ofCardiovascular Imaging. Eur Heart J CardiovascImaging 2016;17:589–90.
12. Hahn RT, Pibarot P, Stewart WJ, et al. Com-parison of transcatheter and surgical aortic valvereplacement in severe aortic stenosis: a longitu-dinal study of echocardiography parameters incohort A of the PARTNER trial (Placement ofAortic Transcatheter Valves). J Am Coll Cardiol2013;61:2514–21.
13. Nombela-Franco L, Ruel M, Radhakrishnan S,et al. Comparison of hemodynamic performance ofself-expandable CoreValve versus balloon-expandable Edwards SAPIEN aortic valves inser-ted by catheter for aortic stenosis. Am J Cardiol2013;111:1026–33.
14. Douglas PS, Hahn RT, Pibarot P, et al. He-modynamic outcomes of transcatheter aorticvalve replacement and medical management insevere, inoperable aortic stenosis: a longitudinalechocardiographic study of cohort B of thePARTNER trial. J Am Soc Echocardiogr 2015;28:210–7.e1–9.
15. Oh JK, Little SH, Abdelmoneim SS, et al.Regression of paravalvular aortic regurgitation andremodeling of self-expanding transcatheter aorticvalve: an observation from the CoreValve U.S.Pivotal trial. J Am Coll Cardiol Img 2015;8:1364–75.
16. Popma JJ, Adams DH, Reardon MJ, et al.Transcatheter aortic valve replacement using aself-expanding bioprosthesis in patients with
severe aortic stenosis at extreme risk for surgery.J Am Coll Cardiol 2014;63:1972–81.
17. Adams DH, Popma JJ, Reardon MJ, et al.Transcatheter aortic-valve replacement with aself-expanding prosthesis. N Engl J Med 2014;370:1790–8.
18. Popma JJ, Reardon MJ, Khabbaz K, et al. Earlyclinical outcomes after transcatheter aortic valvereplacement using a novel self-expanding bio-prosthesis in patients with severe aortic stenosiswho are suboptimal for surgery: results of theEvolut R U.S. study. J Am Coll Cardiol Intv 2017;10:268–75.
19. Bajwa T, O’Hair DP, Williams M, et al. TCT-357Transcatheter aortic valve replacement with a 34-mm repositionable self-expanding bioprosthesis.J Am Coll Cardiol 2017;70:B147.
20. Achenbach S, Delgado V, Hausleiter J,Schoenhagen P, Min JK, Leipsic JA. SCCT expertconsensus document on computed tomographyimaging before transcatheter aortic valve implan-tation (TAVI)/transcatheter aortic valve replace-ment (TAVR). J Cardiovasc Comput Tomogr 2012;6:366–80.
21. Hahn R, Khalique O, Williams M, et al. Pre-dicting paravalvular regurgitation followingtranscatheter valve replacement: utility of a novelmethod for three-dimensional echocardiographicmeasurements of the aortic annulus. J Am SocEchocardiogr 2013;26:1044–52.
22. Lang RM, Badano LP, Mor-Avi V, et al. Rec-ommendations for cardiac chamber quantificationby echocardiography in adults: an update from theAmerican Society of Echocardiography and theEuropean Association of Cardiovascular Imaging.J Am Soc Echocardiogr 2015;28:1–39.e14.
23. Kappetein AP, Head SJ, Genereux P, et al.Updated standardized endpoint definitions fortranscatheter aortic valve implantation: theValve Academic Research Consortium-2consensus document. J Am Coll Cardiol 2012;60:1438–54.
24. Rodriguez-Gabella T, Voisine P, Puri R,Pibarot P, Rodés-Cabau J. Aortic bioprostheticvalve durability: incidence, mechanisms, pre-dictors, and management of surgical and trans-catheter valve degeneration. J Am Coll Cardiol2017;70:1013–28.
25. Shames S, Koczo A, Hahn R, Jin Z, Picard MH,Gillam LD. Flow characteristics of the SAPIENaortic valve: the importance of recognizing in-stent flow acceleration for the echocardiographicassessment of valve function. J Am Soc Echo-cardiogr 2012;25:603–9.
26. Clavel MA, Rodes-Cabau J, Dumont E, et al.Validation and characterization of transcatheteraortic valve effective orifice area measured byDoppler echocardiography. J Am Coll Cardiol Img2011;4:1053–62.
27. Shames S, Koczo A, Hahn R, Gillam LD.In-stent flow acceleration in the SAPIEN trans-catheter aortic valve: impact on the echocardio-graphic assessment of valve function (P3–28).J Am Soc Echocardiogr 2011;24:B63.
28. Jilaihawi H, Chin D, Spyt T, et al. Pros-thesis-patient mismatch after transcatheteraortic valve implantation with the Medtronic-Corevalve bioprosthesis. Eur Heart J 2010;31:857–64.
29. Willson AB, Webb JG, Labounty TM, et al.3-dimensional aortic annular assessment by mul-tidetector computed tomography predicts mod-erate or severe paravalvular regurgitation aftertranscatheter aortic valve replacement: a multi-center retrospective analysis. J Am Coll Cardiol2012;59:1287–94.
30. Hahn RT, Khalique O, Williams MR, et al.Predicting paravalvular regurgitation followingtranscatheter valve replacement: utility of anovel method for three-dimensional echocar-diographic measurements of the aorticannulus. J Am Soc Echocardiogr 2013;26:1043–52.
31. Pibarot P, Weissman NJ, Stewart WJ, et al.Incidence and sequelae of prosthesis-patientmismatch in transcatheter versus surgicalvalve replacement in high-risk patients withsevere aortic stenosis: a PARTNER trialcohort-A analysis. J Am Coll Cardiol 2014;64:1323–34.
32. Head SJ, Mokhles MM, Osnabrugge RL, et al.The impact of prosthesis-patient mismatch onlong-term survival after aortic valve replacement:a systematic review and meta-analysis of 34observational studies comprising 27 186 patientswith 133 141 patient-years. Eur Heart J 2012;33:1518–29.
33. Zorn GL, 3rd, Little SH, Tadros P, et al. Pros-thesis-patient mismatch in high-risk patients withsevere aortic stenosis: a randomized trial of a self-expanding prosthesis. J Thorac Cardiovasc Surg2016;151:1014–23.e1–3.
KEY WORDS echocardiography, effectiveorifice area, hemodynamics, transcatheteraortic valve replacement