Embed Size (px)
Citation preview
2 REPORT OF A TASK GROUP OF COMMITTEE 4
the occurrence of accidents cannot be entirely excluded and emergency response planning for any site with such an installation, facility or source should be regarded as an essential secondary level of protection needed to mitigate the consequences of any radiological emergency.
2. CONCEPTS, QUANTITIES AND BASIC PRINCIPLES FOR INTERVENTION
2.1. The Basic Quantities
(5) The basic concepts and quantities for radiation protection purposes are presented in ICRP Publicution 60 and are summarised here. In accidental situations, there is a possibility for both deterministic and stochastic health effects, therefore the necessary quantities for both cases are summarised briefly.
(6) The quantity for use in relation to deterministic effects is the absorbed dose, the energy absorbed per unit mass. Absorbed dose is used in radiation protection to mean the average dose over a tissue, organ, or over the whole body. The special name for the unit of absorbed dose, Jkg-‘, is the gray (Gy). Deterministic effects are not likely to occur at absorbed doses less than 0.5 Gy.
(7) Equivalent dose, effective dose and committed effective dose are the dosimetric quantities to be used to assess risks of stochastic effects. The equivalent dose in a tissue or organ is formed by weighting the absorbed dose in that tissue by the radiation weighting factors. The effective dose is formed by weighting the equivalent dose by the tissue weighting factor and summing over the tissues. The committed effective dose is the time integral of the effective dose rate following an intake of a radionuclide. The name for the special unit for both equivalent and effective dose is the sievert (Sv). Effective dose is not a good measure of risk of stochastic effects when doses approach or exceed the thresholds for deterministic effects.
(8) For the purpose of consideration of justification and optimisation, another quantity is useful in some cases, namely the collective effective dose. This is the sum of all individual values of effective dose in a group of individuals, often estimated as the product of the mean effective dose in a group and the number of individuals in that group.
2.2. Special Concepts for Intervention
(9) In the event of an accident, doses to the population at risk should first be estimated for each exposure pathway without taking into account possible protective actions. These are called projected doses (PD).
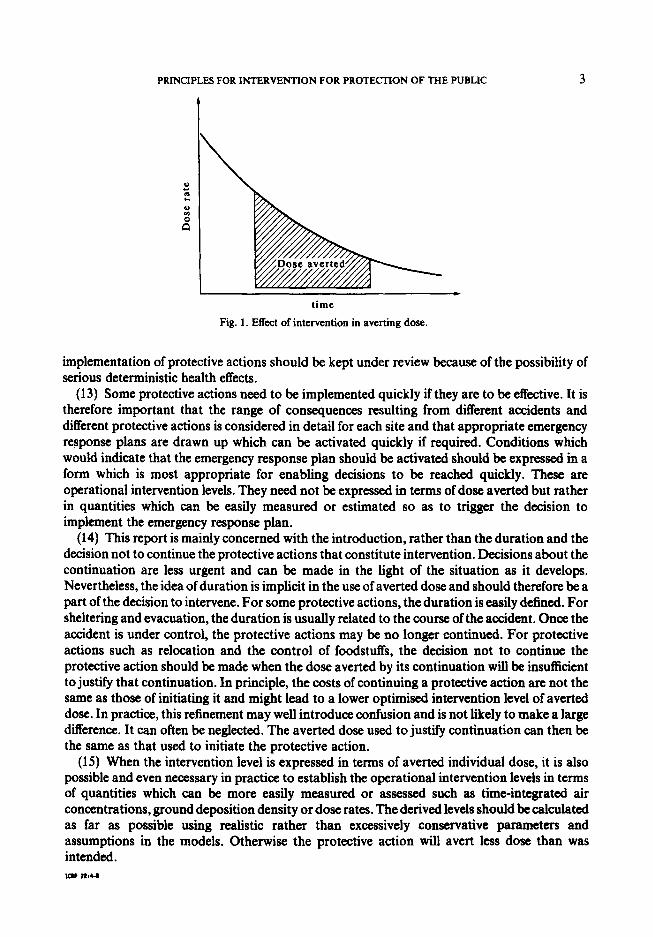
(10) The key concept for an intervention is the averted dose (AD) for each pathway, which is the dose saved by implementing a protective action. This is illustrated in Fig. 1. It may be expressed in any of the relevant dosimetric quantities. The duration of the exposure is an important consideration since protraction of the dose influences the threshold dose at which deterministic effects appear.
(11) If the interventions are fully effective, the averted dose is numerically equal to the projected dose, but these are conceptually different quantities (uide in@z). However, it may be appropriate to express the intervention level in terms of a projected dose for that pathway rather than an averted dose.
(12) Intervention may not be fully effective, either because dose has already been received, or because the intervention itself may only partly reduce the total projected dose. The remaining dose from each pathway (projected dose minus averted dose) is called residual dose (RD). Each intervention is judged on its merits. However, the sum of residual doses from all pathways after
PRINCIPLES FOR INTERVENTION FOR PROTECTION OF THE PUBLIC 3
time
Fig. 1. Effect of intervention in averting dose.
implementation of protective actions should be kept under review because of the possibility of serious deterministic health effects.
(13) Some protective actions need to be implemented quickly if they are to be effective. It is therefore important that the range of consequences resulting from different accidents and different protective actions is considered in detail for each site and that appropriate emergency response plans are drawn up which can be activated quickly if required. Conditions which would indicate that the emergency response plan should be activated should be expressed in a form which is most appropriate for enabling decisions to be reached quickly. These are operational intervention levels. They need not be expressed in terms of dose averted but rather in quantities which can be easily measured or estimated so as to trigger the decision to implement the emergency response plan.
(14) This report is mainly concerned with the introduction, rather than the duration and the decision not to continue the protective actions that constitute intervention. Decisions about the continuation are less urgent and can be made in the light of the situation as it develops. Nevertheless, the idea of duration is implicit in the use of averted dose and should therefore be a part of the decision to intervene. For some protective actions, the duration is easily defined. For sheltering and evacuation, the duration is usually related to the course of the accident. Once the accident is under control, the protective actions may be no longer continued. For protective actions such as relocation and the control of foodstuffs, the decision not to continue the protective action should be made when the dose- averted by its continuation will be insufficient to justify that continuation. In principle, the costs of continuing a protective action are not the same as those of initiating it and might lead to a lower optimised intervention level of averted dose. In practice, this refinement may well introduce confusion and is not likely to make a large difference. It can often be neglected. The averted dose used to justify continuation can then be the same as that used to initiate the protective action.
(15) When the intervention level is expressed in terms of averted individual dose, it is also possible and even necessary in practice to establish the operational intervention levels in terms of quantities which can be more easily measured or assessed such as time-integrated air concentrations, ground deposition density or dose rates. The derived levels should be calculated as far as possible using realistic rather than excessively conservative parameters and assumptions in the models. Otherwise the protective action will avert less dose than was intended.
4 REPORT OF A TASK GROUP OF COMMiTTEE 4
(16) Results of the optimisation process will lead to intervention levels which can be expressed directly in terms of quantities other than averted dose. These other quantities should be directly measurable, such as activity concentrations for food or exposure rates for ground contamination and generally can be related to the averted dose.
(17) Care should be taken that the magnitude of the dose averted is sufficient to justify the implementation of any protective action, irrespective of the implementation strategy.
(18) To establish a common basis for the level of protection sought after different types of accidents and under differing local conditions it is important that guidance is given at a general level. This will take the form of intervention levels of averted dose above which it is likely that intervention is almost always justified (generically justified intervention levels) or in the form of generically optimised intervention levels in any relevant quantities which correspond to the averted dose.
23. Justification
(19) The introduction of any particular protective action entails some risk to the individuals affected and some harm to society in terms of financial costs and of social and economic disruption. Therefore, before introducing a protective action, it should be shown that it can produce a positive net benefit. In other words, implementation of a given protective action will be justified if its benefits, which include radiation detriment averted, are greater than its associated detriments, in terms of non-radiological risks associated with it, its financial cost and other, less quantifiable consequences such as social disruption. Public anxiety, which can be either relieved or increased by a protective action, is another factor to be considered. Each protective action which has been implemented should be subject to periodic review to ensure that its continuation in its present form is justified. For emergency situations where the projected dose from a specific pathway or combination of pathways may approach thresholds for serious deterministic health effects, protective actions are almost always justified a priori.
2.4. Optimisation
(20) For any situation where intervention is considered, some protective actions might be justified while others are not justified. Of those protective actions which are justified, it is necessary to establish the level at which the best protection will be provided. In other words the radiation detriment averted by each protective action should be balanced against the cost and other detriments of the action in such a way that the net benefit achieved by the protective action is maximised (i.e. optimisation of protection). As the radiological situation changes, protective actions should be reviewed periodically for both justification of their continuation and for their contribution to optimisation of protection.
25. Intervention
(21) For any situation where intervention is considered, some protective actions will be justified and optimised. In the case of intervention for radiation accidents, it is not possible to use the dose limits or source-related constraints. The guidance for decision-makers is in terms of intervention levels for the specific countermeasures for defined accident consequences. The levels are established in quantitative terms by the processes of justification and optimisation. For practical application, derived intervention levels will be expressed in quantities directly
PRINCIPLES FOR INTERVENTION FOR PROTECTION OF THE PUBLIC 5
measurable, i.e., exposure rate, activity concentrations in air or water, food, etc. These derived intervention levels must be directly related to the intervention levels.
3. APPLICATION OF THE PRINCIPLES FOR PROTECTIVE ACTIONS
(22) The first concern in the event of a radiological emergency is to keep,the exposure to individuals from all pathways below the thresholds for serious deterministic health effects. In addition to preventing serious deterministic effects, the unacceptability of a high risk of stochastic health effects to individuals may be a significant factor in the decision making process. In this case, the justification of the protective action from the individual’s point of view may become the dominant factor. In fact when deciding on the implementation of protective actions, the decision maker should first determine whether the protective action is justified from the view point of those individuals who are the most at risk. After that consideration should be given to justification of the action from the viewpoint of society, since the costs and benefits will probably not be evenly distributed amongst the same people. The societal considerations may extend the protective action to cover an even larger group of affected people, or they may set limits to the practical or financial feasibility of the action (e.g. evacuation of a large city). In case the proposed protective action is not justified from the viewpoint of the individual, decision makers may still seek to reduce the collective dose and hence the detriment from the emergency and care should be taken not to do more harm than good in the process.
(23) Any protective action interferes to some extent with normal living conditions and may itself involve some risk. The benefits include: averted individual dose, averted collective dose, reassurance and accompanying reduction of stress and anxiety, recovery of land for economic use; the disadvantages include: individual physical risk, collective physical risk, dose and other risks to workers implementing the protective action (see Annex A), doses incurred by the population as a result of the protection action, e.g. during evacuation, financial cost, individual inconvenience, social disruption and anxiety.
(24) The guidance given in ZCRP Publication 60, paragraphs 220-222, is as follows: “The first step in deciding on the intervention likely to be needed in the event of an accident is to define the type of all the likely protective actions and to consider the costs and disadvantages as well as the expected reductions in individual and collective doses as functions of the scale and duration of each. For individual doses, both the average dose and the distribution of doses within the population will have to be taken into consideration. A substantial amount of preliminary work on economic and environmental models and on accident forecasting is needed for these assessments.
(25) “Because the initial introduction of protective actions on any scale, however small, involves significant costs, it may well be that small-scale, short-duration, intervention is costly without being effective. As the scale and duration are increased, the effectiveness initially increases without a marked increase in costs. Eventually, further increases will fail to achieve increased benefits comparable with their costs and the net benefit again begins to fall. There is then a range of values of the possible intervention level of individual dose averted, within which there is an optimum level. If the net benefit at that optimum is positive, intervention of the defined type, scale and duration will be justified. The initial planning for emergencies should include the choice of intervention levels of dose averted, or a range of such intervention levels, that are likely to lead to intervention that is justified and reasonably well optimised.
(26) ‘The benefit of a particular protective action within a programme of intervention should be judged on the basis of the reduction in dose achieved or expected by that specific protective