Embed Size (px)
Citation preview

Review ArticleFam Proc 32:235-248, 1993
Conceptualizing Social Support in Families of Children with SpecialHealth Needs
GLORIA L. KRAHN, Ph.D.a
aRequest for reprints should be sent to Dr. Krahn at the Child Development and Rehabilitation Center, Oregon Health SciencesUniversity, P.O. Box 574, Portland OR 97207-0574.
The concept of social support is used increasingly to understand families and their functioning. Whileconceptualization of the support process is regrettably absent for much research on families, earlier models developedfor examining social support of individuals can enlighten research on families. The history of the social support conceptis presented along with an overview of current typologies of social support and models of how it impacts physical andmental health. Research on the social support of families with children with special needs is reviewed relative to theseissues. Greater recognition of a comprehensive model of support is advocated. Recommendations are made forlongitudinal research on temporal patterns of utilization and satisfaction with support, and for consideration of culturalcontexts in interpreting social supports.
Researchers and clinicians are increasingly using the concept of social support to understand families and how theyfunction. Too frequently, however, research design and measurement reflect only a partial consideration or generalunderstanding of the concept of support itself. Although social support is often regarded as a generic concept to refer to thesupportive aspects of a social environment, closer examination of the extant literature reflects diversity in itsconceptualization, measurement, and associated outcomes. Researchers and theoreticians have developed models of howsocial support mediates its influence for individual adults, but have examined the social support of families lesssystematically and with less reliance on conceptual models. With a few exceptions (for example, Dunst & Trivette, 1990;Kazak & Wilcox, 1984), family researchers fail to incorporate into their designs the models and findings regarding socialsupport of individual adults that could enlighten and direct their efforts with families.
The measurement of social support of families may be approached in several ways. The most popular is relying onindividual informants whose roles are defined vis à vis the family (for example, mother, father). Another approach is tocombine information across informants, such as averaging across reporters, or developing other indices that combineinformation across respondents. In all cases, the familial role defines their perspective for reporting.
Because of the hypothesized relationship between stress and support, the role and functioning of social support infamilies can be examined most clearly by considering families under significant stress. Families whose children havespecial developmental or health care needs provide valuable illustrations of normal families in abnormal situations. Thesefamilies are not more likely than the general population of families to experience familial dysfunction or alterations in theirsocial support systems prior to the diagnosis of the child's illness. Similarly, they are not immune to other crises impactingtheir family functioning. They represent members of "the family next door" who suddenly and inexplicably must deal withhigh levels of stress stemming from the characteristics of their child's illness or disability.
Families of children with special needs are known to experience excessive caretaking demands as well as extraordinaryemotional stresses (Mullins, 1987; Singer & Irvin, 1989). Parents of a child with special needs often need to engage inphysically demanding care activities, constantly monitor the child's health status, and maintain multiple health, therapy, andeducational appointments. Emotionally, parents must learn to live with the child's condition and revise their earlier dreamsand expectations, concurrently assessing and sometimes challenging professional recommendations and available services.By examining the nature, measurement, and operational functioning of social support for these families, researchers canunderstand the role of social support of families more generally. Findings can also inform service providers and policymakers about needed support services for families of children with special health needs.
This article is intended to provide researchers and practitioners with a framework for conceptualizing social support offamilies and to promote greater clarification and specificity in its use in research with families. It does so by discussingmodels of social support as developed for individuals, and uses this framework to consider research findings about socialsupport of families with children with special needs.
Historical Interest in Social SupportThe paradigm shift in the social sciences that began in the 1950s reflected a change in perspective from an emphasis on
individuals and categories to an appreciation of structures, systems, and the relations among system components. Etiology
______________________________________________________________________________________________________________
1

of and solutions to problems were no longer seen to reside within the individual but, rather, within the larger environmentalcontext. The theory of ecological systems and processes, as reflected by the writings of Bronfenbrenner (1979), is amanifestation of this new perspective. This paradigm shift contributed to the burgeoning attention paid to the socialenvironment generally and to social support specifically, which has been witnessed in the past several decades (Wellman,1981). The work of epidemiologist John Cassel in the 1970s was seminal in applying this ecological perspective tounderstanding the role of the psychosocial environment for personal well-being. Noting the absence of etiologicalspecificity across many illnesses, Cassel (1976) concluded that psychosocial processes contribute to increased or decreasedvulnerability to diseases and disorder (see Gottlieb, 1981; Turner, 1983). This perspective of social etiology of physicalillness soon was extended to mental illness as well. Historical development of the stressor-illness model has been reviewedelsewhere (Carveth & Gottlieb, 1979; Cohen & Syme, 1985; Lin, Dean, & Ensel, 1981).
Notably, much of this early work focused on the ecological context of the individual adult; it is only in the past 15 yearsor so that substantial research has examined the ecological context of the family. Concurrent with this perspective shift ofviewing the family as the unit of study, a concomitant shift occurred in service delivery systems. For example, earlyintervention services for infants and toddlers, as specified in the legislation of PL 99-457 and, more recently, PL 101-476,specifically regards the family as the service recipient.
The resources and support of the family are critical components of the ecological context of the family. Social support isa concept of considerable explanatory power, but one that has generally been plagued with vague and differing definitionsof what is included within its definition and how it should be measured. As Bruhn and Phillips (1984) state: "Perhaps theconcept of social support continues to be ambiguous because we have been involved in quantifying the phenomenon beforeit has been defined satisfactorily" (p. 163). At the least, a general theory of social support that can be extended to familiesrequires a clear definition that includes a careful delineation of kinds of support.
DEFINING SOCIAL SUPPORTIn a general sense, social support refers to the supportive assistance from important others that addresses perceived
needs. Too frequently, greater precision in definition is lacking. Perhaps the greatest single source of confusion in the socialsupport research is the often implicit assumption that social support is a singular, monolithic construct. This leads to thepresumption that different measures of support are interchangeable. As examples, while Thoits (1986) defines socialsupport as "functions performed for a distressed individual by significant others" (p. 417), that is, as services, Dunst,Trivette, Gordon, and Pletcher (1989) describe it as "the re-sourcespotentially useful information andmaterialsprovided to individuals or family units for aid and assistance" (p. 124), that is, as tangible goods andinformation; and Hirsch (1980, p. 160) describes a support system as "the set of presently significant others who are eithermembers of one's social network (i.e. family or friends) or affiliated non-mental health professionals (e.g., physician,clergy)," that is, as relationships.
Researchers and theoreticians alike have advocated for the separate measurement of distinct components of support andwarned that when single indices of support include several components, the resulting data may be theoreticallyindecipherable (Barrera, 1986, 1988; Cohen & Syme, 1985; House & Kahn, 1985). Toward that end, greater precision inthe definition of social support requires an understanding of different components of social support, including theircomplementarities and contrasts.
Components of Social SupportNumerous frameworks for categorizing social support have been proposed. Perhaps the most comprehensive framework
is that of Turner (1983) who outlines different components for examining social support. These components includealternatives for the person who makes the assessment (respondent versus investigator), the nature of reality assessed(perceived versus enacted), the metric used (intensity, frequency, or durability), the content or kind of support (love, status,information, aid), the status of utilization (utilized versus accessible), the social role of contacts (for example, spouse,friend, co-worker), and the focus of the problem (general versus focused problem). While this framework is valuable forportraying virtually all of the categories reflected in other frameworks, its inclusiveness (a possible 576 cells in the model!)makes it cumbersome. The vast array of possibilities for measuring social support can be overwhelming. One parsimoniousand popular approach to differentiating among potential measures is to distinguish between structural characteristics of thesupport network and functional aspects of support (for example, Cohen & Syme, 1985; House & Kahn, 1985; Mitchell& Trickett, 1980), which are both frequently included under the general rubric of social support but reflect very differentcharacteristics and often operate orthogonally to each other.
Structural Characteristics of SupportStructural measures have their origins in social network analysis and reflect the degree to which an individual or family
______________________________________________________________________________________________________________
2

is embedded in a social context. The existence and interconnectedness of social relationships are used to describe thenetwork. Mitchell and Trickett (1980) provide a historical and conceptual review of the social network approach.
There are a number of structural dimensions to assess embeddedness and they are presented here to inform readers whomay not be familiar with them. Size of the network describes the number of persons who are regarded as supportive. This istypically obtained by eliciting a list of names of supportive persons in categories of relationships such as family, friends,and professionals. Density of the network refers to the extent to which members of the network have relationships witheach other independent of the respondent. It provides an index of concentration or dispersion of the network ofrelationships. A measure unique to family researchers is the index of spousal density, which refers to the degree to whichrelationships are shared by the marital partners. Multiplexity is a measure of the number of kinds of aid (for example,material, emotional, informational, physical assistance) that characterize specific relationships. Symmetry or reciprocityindicates the degree to which relationships are balanced in help-giving and help-receiving, including the direction of flow insupportive exchanges within a network of relationships. Researchers have used reciprocity to refer to both a specificlinkage and the total network.
Proxy measures are frequently used in structural assessment. Summary characteristics like marital status or proximity ofextended family have been used as abbreviated measures of the social network. While such measures may provide a quickand crude measure of social embeddedness, they are based on assumptions about quality and availability of support thatmay not be accurate. For example, being married does not guarantee that one has a partner who is positive, available, orsupportive; likewise, being single does not preclude the presence of a highly supportive relationship. Although attractivefor their convenience, these proxy measures are not sufficiently discriminating to enhance understanding of social supportnetworks.
Size and DensityResearch findings about structural characteristics of social support networks have generally focused on network size and
density. In the general population of families, networks differ between families with and without children (Hammer,Gutwirth, & Phillips, 1982). Total network size was found to be fairly similar for parents and nonparents, but parents sawpersons in their networks less frequently than did nonparents. Working mothers reported larger networks than nonworkingmothers, and nonworking mothers in the lowest social class were observed to have smaller absolute networks of support.These results portray the relative social isolation of nonworking mothers, particularly those with restricted financial andeducational resources.
In the special-needs population of families, Kazak and her colleagues have studied the social networks of several groupsof families with children with different diagnoses. Their measures look at network size in terms of family, friendship,professional, and total network. Compared with families of children with no diagnosis, families of children with spina bifida(mean age = 7 years) reported smaller support networks, especially in terms of mothers' total and friendship networks; andtheir networks were more dense (Kazak & Wilcox, 1984). Families with young children (mean age = 3 years) withphenylketonuria (PKU) showed no differences in network size or density relative to comparison families, although PKUfamilies did have larger professional networks. When each group was dichotomized on distress level, the more distressedmothers had smaller and more dense networks; more distressed fathers reported a smaller group of friends but not moredense networks (Kazak, Reber, & Carter, 1988). Families of older children (mean age = 21 years) who wereinstitutionalized and mentally retarded (IMR) did not have smaller total networks; instead, mothers' total networks weremore dense and mothers' networks of professionals were larger and more well-developed (Kazak, 1988).
One interpretation of these findings is that these conditions represent different levels of stress on families: spina bifidaplacing both physical and emotional demands on parents, PKU requiring constant dietary monitoring and management butfewer other physical demands, and IMR older children continuing to place emotional demands but fewer physical stresseson families. The social network findings for both size and density reflect these presumptions of different levels of stress.Differences are seen in network density for spina bifida and IMR families relative to nondisabled comparison families, butare not seen for PKU families. Total network size differs for spina bifida families but not for PKU or IMR, althoughnetwork size continues to be associated with level of distress in the PKU family study. Increased levels of stress stemmingfrom the child's condition appear to lead to increased network density and decreased total network size. Additionally, thefindings from the PKU families (Kazak et al., 1988) remind us that parenting a child with special needs is not ahomogeneous experience, with some families reporting more distress than others.
Additional findings are available based on the same social support instrument but used with a different population. Truteand Hauch (1988a,b) examined a Canadian sample of families that were assessed through self-report and by professionaljudgment to be adapting positively to their young children (mean age = 3 years) with various developmental disabilities.Using a modification of the Kazak measure and comparing their results with the Kazak & Wilcox (1984) comparisonsample, they found that both mothers' and fathers' networks were relatively small (mean size = 7.5 persons versuscomparison sample mean = 11.2) and more similar to their spina bifida sample (mean = 8.3). No independent comparisongroup was reported. Network density was high for the total and family network, but not for friendship relationships, in
______________________________________________________________________________________________________________
3

which positively adapting families appeared to maintain a "loosely knit constellation of friendship ties" (1988b, p. 11).These findings suggest that structural characteristics of the support network are affected even in families that are adaptingwell to their child's disability. This interpretation could be further supported if comparison data were available for theCanadian study. Alternatively, these findings may reflect cultural differences between the southeastern U.S. families andmidwestern Canadian families.
ReciprocityWhile these results demonstrate the discriminability of network size and density, less research has been conducted on the
structural characteristic of reciprocity. Maintaining reciprocity in relationships has been presumed important (Dunst, et al.,1989; Shumaker & Brownell, 1984), but it may be more complex than initially considered. The norm of reciprocitypresumes that persons who by their circumstances are forced to accept assistance without being able to reciprocate areplaced in an uncomfortable position that will lead them to take alternative actions. Kazak and Wilcox (1984) found mothersof children with spina bifida to have nonreciprocal relationships with their families but not with their friends. In a modelcooperative program designed to develop reciprocal relationships among participating families, Dunst et al. (1989)encountered significant difficulties around the principle of reciprocity. Specifically, they describe a number of families ofchildren with disabilities that willingly received assistance without reciprocating, and another group of families withadequate resources that contributed to others, but resisted accepting contributions from families that were seemingly lessadvantaged. These findings suggest that a static interpretation of reciprocity may not be the norm across all kinds ofrelationships and situations. At a national level, contemporary advocacy groups maintain that access to services is a rightand not a privilege. This stance further challenges the necessity of presumed reciprocity in professional components of thesocial network.
Functional Characteristics of SupportWhile structural characteristics quantify the relationships of the support network, functional characteristics describe their
nature. Two key functional characteristics relate to availability and content of support.
Availability of SupportMany writers (for example, Barrera, 1986, 1988; Cobb, 1979; Cohen, Mermelstein, Kamarck, & Hoberman, 1985) have
emphasized the distinction between perceiving that support is available if needed (perceived support) and actually gainingaccess to support (enacted support). This distinction between perceived and enacted/ administered support is critical whenexamining the mechanism of how social support works. The ameliorative effect of support is often regarded as cognitivelymediated, with a person's appraisal of how stressful a situation is being reduced by the perception that help is available. Asa result, many social support instruments measure the perceived availability of support (for example, Cohen, Mermelstein,et al., 1985; Sarason, Sarason, & Pierce, 1990). A recent review of studies confirmed the primary importance ofindividuals' perceptions that support is available (Sarason et al., 1990). Of note is the suggestion that mandated help maynot always be viewed as helpful by the recipient. Affleck, Tennen, Rowe, et al. (1989) found that a hospital-to-hometransition program intended to be supportive to mothers of high-risk infants showed positive effects only for mothers ratingthemselves as needing support. Unrequested assistance may actually erode one's sense of competence.
Content of SupportMost writers have recognized the content of support to be multidimensional (see Cohen, Mermelstein, et al., 1985; Moos
& Mitchell, 1982; Wellman, 1981). While they have given the categories various labels, they have generally madedistinctions among: a) instrumental support (also referred to as tangible support, material aid and services, physicalassistance, doing things, giving and lending things); b) emotional support (appraisal, someone to talk with about problems,help with personal problems, self-esteem); c) informational support (cognitive guidance and advice, informational help); d)belonging (social companionship, people one can do things with); and e) social regulation (appraisal support, informationthat helps evaluate personal performance). Family researchers may customize these categories to include areas of specificconcern to families, such as childcare and respite.
Little research is available that has addressed the relative helpfulness to families of these different categories of content.However, Cohen (1988) and Dunst and Trivette (1990), among others, have emphasized that "support" is supportive only ifit matches in kind an indicated need for assistance. For instance, informational support may be valued less when the feltneed is for material assistance.
Sources of SupportResearch findings suggest that the relative importance of different support categories varies with characteristics of the
support provider and recipient. Carveth and Gottlieb (1979) examined stress in mothers of newborns as it related to three
______________________________________________________________________________________________________________
4

indices of social support: amount of contact, problem-centered feedback, and relationship importance. Different kinds ofsupport were identified to be needed from different members of the network. Maternal stress was significantly related torate of contact with husband and physician, and to relationship importance and problem-centered feedback with mother andmother-in-law.1
Dunst, Trivette, and Cross (1986a), in their research review of roles and social networks of mothers with handicappedand nonhandicapped children, repeatedly found that families of children with disabilities reported less available socialsupport from both friends and families. These same authors also found that the important sources of support vary dependingon the marital status of mothers. Intimate support from a husband or partner was most beneficial in promoting mothers'general life satisfaction (Crnic, Greenberg, Ragozin, et al., 1983) and proximal behavior with high-risk infants (Feiring,Fox, Jaskir, & Lewis, 1987), while extra-family support was more important as a mediator of life satisfaction for single thanmarried mothers (Brim, 1974).
Factors Influencing Support
Personality and Family VariablesVarious factors are known to influence the availability and utilization of social support of individual adults, including
personal resources, gender, network orientation, life stressors, and geographical location, among others (Heller & Swindle,1983; Holahan & Moos, 1981; Moos & Mitchell, 1982; Shinn, Lehmann, & Wong, 1984). Personality variables affect notonly the degree to which persons use support networks, but also their interpersonal attractiveness in developing andmaintaining intimate relationships (Hobfoll & Lerman, 1989). Many of these factors likely also influence families'inclinations to access support. Geographically or culturally isolated families may perceive themselves as having lesssupport available. Characteristics not only of the individual parents but also of the marital couple (for example, maritaldiscord) and of the family (for example, child disruptiveness) may influence the family's attractiveness to other families formaintaining long-term relationships, as well as the family's inclination toward relationships.
Changes Over Time in Needed SupportDevelopmental changes occurring over an individual's or family's life-span are accompanied by changes in the quantity
and nature of support needed (see Bruhn, & Phillips, 1984). Hirsch (1985) provides a framework for examining socialsupport over the life-span and in relation to role transitions, with different kinds of support predicted to be important atdifferent times. Research findings have supported this. Schulman (1975) found that social support varied as a function ofboth age and life stage. Persons named as supportive varied with life cycle. For example, family members were less likelyto be listed as supportive by single respondents, and more so by married, widowed, separated, or divorced respondents.Support was more stable (provided by the same persons) as the respondent grew older.
Changes in the nature of needed support are evident in families of children with disabilities. In a short-term, longitudinalstudy of support to families with a chronically ill young child, Long, Katz, and Pokorni (1989) demonstrated that families'needs for emotional support and caregiving information were initially high and then diminished over the baby's first 18months. Motor concerns remained consistent and educational concerns increased in salience for parents. Regardingsupportive services, findings from a cross-sectional survey of parents of mentally retarded children of varying ages (Suelzle& Keenan, 1981) suggested that use of support services declined over the life-span of the child, with parents of olderchildren using services less and being more isolated. Perhaps related to changing needs of families is one study's findingthat satisfaction with support appeared to vary with the age of the child: mothers of preschool-aged children with handicapsreported less satisfaction with supportive services while mothers of handicapped adolescents reported more (Dunst,Trivette, & Cross, 1986b). Thus, services available to families may be better matched to the needs of older children, or,with increased experience with the service delivery systems, families have fewer expectations of them and consequentlyreport higher satisfaction.
Valence of "Supportive" ContactsSocial contacts can be regarded to have a valence, as positive, neutral, or negative. Not all social contacts or
relationships are positively supportive (Bruhn & Phillips, 1984). Social contacts can be negative rather than helpful, andsocial relationships can be resource-depleting rather than enriching. Extended families can request financial or emotionalsupport, for example, rather than provide it. Sandler and Barrera (1984) acknowledge this in their assessment of"conflicted" relationships, while Wellman (1981) describes the involuntary nature of some ties, particularly those withrelatives. The valence of supportiveness is often included only indirectly in measures of perceived support or supportsatisfaction, and not assessed at all when only the structural characteristics of the social network are measured.
Research provides little information about how relationship valences impact social support for families with a child withspecial needs. However, anecdotal accounts suggest this to be an area warranting further study. The emotional struggle that
______________________________________________________________________________________________________________
5

extended family members also experience in accepting the child's condition may compromise their ability to provide socialsupport to the immediate family. Parents who themselves are in great need of support sometimes report finding themselvesproviding support to those extended family members from whom they would like to receive support.
MODELS OF HOW SOCIAL SUPPORT WORKSAlternative models of how support relates to stress, distress, and health have been proposed and examined (see Barrera,
1988; Sarason et al., 1990). Two of the most popular models posit that support works primarily in the presence of highstress to buffer against negative consequences (stress-buffering model), or that support directly enhances health and generalwell-being regardless of level of stress (direct-effects model). Research on these models has been reviewed extensively(Cohen & Syme, 1985;, Cohen & Wills, 1985; Lin et al., 1981). Familiarity with these alternative models of how supportmediates the influence of stress is of value to family researchers and practitioners. That knowledge can inform modeldevelopment and predictions of research, and can help in the development of programs of support delivery systems forfamilies. These models also provide a framework for reviewing research results that can at times seem very disparate andcontradictory.
Stress-Buffering ModelEarly conceptualizations asserted that social support is mobilized to aid the individual during stressful episodes, with
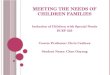
support ameliorating the otherwise negative effects of stress (Caplan, 1974; Cobb, 1976; Dean & Lin, 1977). Figure 1illustrates the relationships among stress, support, and distress, as predicted by the stress-buffering model. According tothis model, the benefits of social support would be evident only under conditions of relatively high stress, with nodifferences noted during conditions of low stress. Enacted support is viewed as reducing the stress experience by institutinghelpful or health-promoting actions, while perceived support reduces the appraised threat of a stressor. Links to physicalhealth could be mediated through the neuroendocrine or immune system functioning.
Figure 1.Stress-buffering model of predicted relationship among stress, support, and distress.
Despite a wealth of studies of the stress-buffering effect, researchers have generated only mixed support for this model(see reviews of Cohen & Wills, 1985; Thoits, 1982, 1985, 1986; Wilcox, 1981). Not only has increased mobilization ofsupport during times of stress not always been clearly demonstrated (for example, Gore, 1985), but the converse,deterioration of the support system under conditions of stress, has been described (Dunst et al., 1989; Shinn et al., 1984;Wortman & Lehman, 1985). A difficulty associated with this model is the need for appropriate research design and analysis
______________________________________________________________________________________________________________
6

to identify the statistical interaction that demonstrates a buffering effect.Cohen (1988) describes three methods of analysis to examine for stress buffering effects: a) dichotomous groups and
testing for different patterns of relationships; b) hierarchical multiple regression with the interaction term representing theproduct of stress and social support; and c) multiple regressions between stress and symptoms with network variables.Cohen and Wills (1985) conclude that stress-buffering is most evident when studies are methodologically adequate todetect the significant interaction between stress and support, measure perceived availability of functional support, andmeasure emotional and informational support. Barrera (1988) reaches similar conclusions and additionally proposes thatstress-buffering may function in a curvilinear fashion, making analyses based on assumptions of linear relations insensitiveto existing relations.
Direct-Effects ModelIn its simplest form, this model posits that social support is beneficial regardless of the degree of stress an individual or
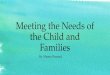
family is experiencing; higher levels of support are directly related to lower levels of distress or physical symptomatology(see Figure 2). Such a model would be consistent with the view of Antonovsky (1979; 1987) who asserts that living is acontinuously stressful process, and that life situations of low stress levels are more imaginary than real. Posited mediationallinks of perception of threat, immune system functioning, and impact on health-promoting behavior are similar to those ofthe buffering model.
Figure 2.Direct-effects model of predicted relationship among stress, support, and distress.
Research support for this model has been mixed. While clear and inverse relationships between support andsymptomatology have been identified in some studies, others have failed to obtain such findings. The direct-effects modelhas pertained most frequently when embeddedness has been assessed, particularly embeddedness assessed with multipleitems rather than simple proxy measures (see reviews by Cohen & Syme, 1985; Cohen & Wills, 1985). Being an integraland well-linked member of a social community appears to predict to decreased distress and symptomatology. Even theseconclusions may be limited, however, to dichotomies between persons who are socially isolated and those who havereached or exceeded a minimal threshold level of embeddedness (Cohen & Wills, 1985).
Distinctions Among Models
______________________________________________________________________________________________________________
7

Despite Cobb's (1979) earlier assertion that it is not worth worrying about the distinction between main effects andinteraction effects, the relative prevalence of these two models has continued to be considered (see Barrera, 1986; Cohen& Wills, 1985). General findings indicate that, when structural characteristics of social embeddedness are measured, adirect-effects model is more likely to be supported. Alternatively, when the measure relates to perceived support,particularly emotional and informational support, a buffering interaction is more likely to be identified.
The few identified studies that examined model effects in families provide ambiguous findings. Frydman (1981)examined the effect of support on two groups of families: those with a child with cystic fibrosis, and those with a child withleukemia. Different results were observed for each. For the cystic fibrosis families, a stress-buffering interaction effect wasnoted for neighborhood contacts, while, for the leukemia families, no buffering was noted but a strong main effect was seen.Brandt (1984), in a study of social support and negative life events for mothers of young, developmentally disabledchildren, also observed a direct relationship between negative life events and satisfaction with support. Future research isneeded to measure stress, support, and distress over repeated time intervals, as in longitudinal studies, in order to delineatethe mechanisms of different kinds of support in different populations. Such research would need to be attentive to absolutelevels of stress in families to make interaction detection possible. If these families never experience times of low stress, theinteraction effect necessary to demonstrate a stress-buffering model cannot be observed.
SUMMARY AND FUTURE DIRECTIONSIndividuals and families live, love, and survive within social contexts, and these contexts influence their physical,
emotional, and social well-being. Social support is a dimension popularly used in the past several decades to conceptualizethese influences. Research in social support has moved from an awareness of its importance for physical and mental healthoutcomes to a recognition of different components and increased specificity in the measurement of its components. Inchorus with many other writers, this author advocates discarding a global concept of social support in favor of examiningthe structure and functioning of the social support network as it relates to enacted support, perceived adequacy orsatisfaction with support, content and sources of support, and characteristics that predispose one to accessing support.Researchers and practitioners alike need to be mindful of these distinctions among components of support, and not assumeinterchangeability among them.
Research findings with families have suggested that size of the support network is related to parental distress and topresence of a child illness or disability. Smaller and more dense networks were associated with more distress. Changeshave been observed over time in the nature and the amount of support sought by families with a child with special needs.While source of support for family varies depending on whether mother is married or not, marital status itself is not a goodsingle index of support availability or administration.
Research and intervention designs for families with special-needs children must be based on an understanding of howdifferent kinds and sources of support, and perceptions of support adequacy, relate to family needs and resources, and,ultimately, how these variables relate to family role division and family functioning. Trivette, Dunst, Deal, et al. (1989)have recently developed a measure of family functioning from an adaptive coping perspective that examines strengths offamilies.
Future research on the social support of families needs to be conducted in at least two important areas. The first is theassessment of the social support process over time. The need for longitudinal and prospective studies of patterns of supportneeded and used has frequently been cited by others (for example, Heller & Swindle, 1983; Turner, 1983). This approachholds promise for gathering data that will be useful in planning for family support services over the life-span. Families mayvary over time in patterns of support-seeking, showing alternating periods of support-seeking and relative self-sufficiency.This issue is particularly relevant for families of children with chronic illness and disabilities, whose need for support andability to access support will vary in accordance with the developmental stages of their child and the characteristics of theirchild's disorder or illness. Such information would enable service providers to plan for the actual needs of families as theyconduct their daily lives.
The second important but largely unreported area is that of cultural differences in support-utilization patterns. Culturaldiversity relating to values of family, individual rights, and illness or disability, may result in different patterns ofsupport-seeking. One example is childcare for children with special needs. Nihira and Mink (1991) found that inAsian-American families extended family members were much more likely to provide childcare for children withdisabilities than was observed in Euro-American families. Similarly, anecdotal reports suggest cultural differences in thelikelihood that families will access public agency services.
Direct implications for policy and intervention can be identified from research findings. Many states and service agenciesare developing and implementing family support programs for families that are highly stressed or have high careresponsibilities. Optimally, such programs would be developed from an understanding of research findings about the natureand functioning of informal and formal support systems and sources of support. As a specific example, if the noted decreasein friendships (informal support) for highly stressed families with a child with chronic illness or disability (see Kazak
______________________________________________________________________________________________________________
8

& Wilcox, 1984; Kazak et al., 1988) occurs because families are too stressed to cope with maintaining their pre-existingsupport networks, is it counterproductive to recommend expanding network size through support groups or special interestgroups (formal support)? Should intervention efforts, instead, be focused on relieving the burden of care through respitecare, transportation, or home-based services? Careful assessments of the social supports available and those used can serveas the beginning for the development of such an understanding. And such an understanding will only come about throughcareful attention to the manner in which support is conceptualized and measured.
REFERENCES
1. Affleck, G., Tennen, H., Rowe, J., Roscher, B. and Walker, L., Effects of formal support on mothers' adaptation tothe hospital-to-home transition of high-risk infants: The benefits and costs of helping. Child Development, 60,488-501, 1989.
2. Antonovsky, A., (1979). Health, stress and coping. San Francisco: Jossey-Bass. 3. Antonovsky, A., (1987). Unraveling the mystery of health: How people manage stress and stay well. San
Francisco: Jossey-Bass. 4. Barrera, M., Jr., Distinctions between social support concepts, measures, and models. American Journal of
Community Psychology, 14, 413-445, 1986. 5. Barrera, M., Jr., (1988). Models of social support and life stress (pp. 211-236). In L.H. Cohen (ed.), Life events
and psychological functioning. Beverly Hills CA: Sage Publications. 6. Brandt, P. S., (1984). Social support and negative life events of mothers with developmentally delayed children
(pp. 205-223). In K.E. Barnard, P.A. Brandt, B.S. Raff & P. Carroll (eds.), Social support and families ofvulnerable infants. March of Dimes Birth Defects Foundation, Birth Defects: Original Article Series, Vol. 20, No.5.
7. Brim, J. A., Social network correlates of avowed happiness. Journal of Nervous and Mental Disease, 158,432-439, 1974.
8. Bronfenbrenner, U., (1979). The ecology of human development: Experiments by nature and design. Cambridge:Harvard University Press.
9. Bruhn, J. G. and Phillips, B. U., Measuring social support: A synthesis of current approaches. Journal ofBehavioral Medicine, 7, 151-169, 1984.
10. Caplan, G., (1974). Support systems and community mental health. New York: Behavioral Publications. 11. Carveth, W. B. and Gottlieb, B. H., The measurement of social support and its relation to stress. Canadian
Journal of Behavioural Science, 11, 179-188, 1979. 12. Casse, J., The contribution of the social environment to host resistance. American Journal of Epidemiology, 104,
107-123, 1976. 13. Cobb, S., Social support as a moderator of life stress. Psychosomatic Medicine, 38, 300-314, 1976. 14. Cobb, S., (1979). Social support and health through the life course (pp. 93-106). In M.W. Riley (ed.), Aging from
birth to death. Boulder CO: Westview Press. 15. Cohen, S., Psychosocial models of the role of social support in the etiology of physical disease. Health
Psychology, 7, 269-297, 1988. 16. Cohen, S., Mermelstein, R., Kamarck, T. and Hoberman, H. M., (1985). Measuring the functional components of
social support (pp. 73-94). In I.G. Sarason & B.R. Sarason (eds.), Social support: Theory, research andapplications. Boston: Martinus Nijhoff Publishers.
17. Cohen, S. and Syme, S. L. (Eds.), (1985). Social support and health. Orlando FL: Academic Press. 18. Cohen, S. and Wills, T. A., Stress, social support, and the buffer hypothesis. Psychological Bulletin, 98, 310-357,
1985. 19. Crnic, K. A., Greenberg, M. T., Ragozin, A. S., Robinson, N. M. and Basham, R. B., Effects of stress and social
support on mothers and premature and full-term infants. Child Development, 54, 209-217, 1983. 20. Dean, A. and Lin, N., The stress-buffering role of social support: Problems and prospects for systematic
investigation. Journal of Nervous and Mental Disease, 165, 403-417, 1977. 21. Dunst, C. J. and Trivette, C. M., (1990). Assessment of social support in early intervention programs (pp.
326-349). In S.J. Meisels & J.P. Shonkoff (eds.), Handbook of early childhood intervention. Cambridge:Cambridge University Press.
22. Dunst, C. J., Trivette, C. M. and Cross, A. H., (1986a). Roles and support networks of mothers of handicappedchildren (pp. 167-192). In R.R. Fewell & P.F. Vadasy (eds.), Families of handicapped children. Austin TX:PRO-ED.
23. Dunst, C. J., Trivette, C. M. and Cross, A. H., Mediating influences of social support family and child outcomes.
______________________________________________________________________________________________________________
9

American Journal of Mental Deficienc Personal, 90, 403-417, 1986b. 24. Dunst, C. J., Trivette, C. M., Gordon, N. J. and Pletcher, L. L., (1989). Building and mobilizing informal family
support networks (pp. 121-141). In G.H.S. Singer & L.K. Irvin (eds.), Support for caregiving families: Enablingpositive adaptation to disability. Baltimore MD: Paul H. Brookes.
25. Feiring, C., Fox, N. A., Jaskir, J. and Lewis, M., The relation between social support, infant risk status andmother-infant interaction. Developmental Psychology, 23, 400-405, 1987.
26. Frydman, M. I., Social support, life events and psychiatric symptoms: A study of direct, conditional and interactioneffects. Social Psychiatry, 16, 69-78, 1981.
27. Gore, S., (1985). Social support and styles of coping with stress (pp. 263-278). In S. Cohen & S.L. Syme (eds.),Social support and health. Orlando FL: Academic Press.
28. Gottlieb, B. H., (1981). Preventive interventions involving social networks and social support (pp. 201-232). InB.H. Gottlieb (ed.), Social networks and social support. Beverly Hills CA: Sage Publications.
29. Hammer, M., Gutwirth, L. and Phillips, S., Parenthood and social networks: A preliminary view. Social Scienceand Medicine, 16, 2091-2100, 1982.
30. Heller, K. and Swindle, R. W., (1983). Social networks, perceived social support, and coping with stress (pp.87-103). In R.D. Felner, L.A. Jason, J.N. Moritsugu, & S.S. Farber (eds.), Preventive psychology: Theory,research and practice. New York: Pergamon Press.
31. Hirsch, B. J., Natural support systems and coping with major life changes. American Journal of CommunityPsychology, 8, 159-172, 1980.
32. Hirsch, B. J., (1985). Social networks and the ecology of human development: Theory, research, and application(pp. 117-136). In I.G. Sarason & B.R. Sarason (eds.), Social support: Theory, research and applications.Boston: Martinus Nijhoff Publishers.
33. Hobfoll, S. E. and Lerman, M., Predicting receipt of social support: A longitudinal study of parents' reactions totheir child's illness. Health Psychology, Health Psychology, 8, 61-77, 1989.
34. Holahan, C. J. and Moos, R. H., Social support and psychological distress: A longitudinal analysis. Journal ofAbnormal Psychology, 90, 365-370, 1981.
35. House, J. S. and Kahn, R. L., (1985). Measures and concepts of social support (pp. 83-108). In S. Cohen & S.L.Syme (eds.), Social support and health. Orlando FL: Academic Press.
36. Kazak, A. E., Stress and social networks in families with older institutionalized retarded children. Journal ofSocial and Clinical Psychology, 6, 448-461, 1988.
37. Kazak, A. E., Reber, M. and Carter, A., (1988). Structural and qualitative aspects of social networks in familieswith young chronically ill children. Journal of Pediatric Psychology, 13, 171-182, 1988.
38. Kazak, A. E. and Wilcox, B., The structure and function of social networks in families with a handicapped child.American Journal of Community Psychology, 12, 645-661, 1984.
39. Lin, N., Dean, A. and Ensel, W. M., Social support scales: A methodological note. Schizophrenia Bulletin, 7,73-89, 1981.
40. Long, T., Katz, K. and Pokorni, J., Developmental intervention with the chronically ill infant. Infants and YoungChildren, 1, 78-88, 1989.
41. Mitchell, R. E. and Trickett, E. J., Task force report: Social networks as mediators of social support: An analysisof the effects and determinants of social networks. Community Mental Health Journal, 16, 27-44, 1980.
42. Moos, R. H. and Mitchell, R. E., (1982). Social network resources and adaptation: A conceptual framework (pp.213-232). In T.A. Wills (ed.), Basic processes in helping relationships. New York: Academic Press.
43. Mullins, J. B., Authentic voices from parents of exceptional children. Family Relations, 36, 30-33, 1987. 44. Nihira, K. and Mink, I. T., (1991). Home environment of developmentally delayed children: A comparison
between Euro-American and Asian-American families. Paper presented at the Society for Research in ChildDevelopment, Seattle WA, April, 1991.
45. Sandler, I. N. and Barrera, M., Jr., Toward a multimethod approach to assessing the effects of social support.American Journal of Community Psychology, 12, 37-52, 1984.
46. Sarason, B. R., Sarason, I. G. and Pierce, G. R., (1990). Traditional views of social support and their impact onassessment (pp.9-25). In B.R. Sarason, I.G. Sarason, & G.R. Pierce (eds.), Social support: An interactional view.New York: John Wiley & Sons.
47. Schulman, N., Life cycle variations in patterns of close relationships. Journal of Marriage and the Family, 37,813-821, 1975.
48. Shinn, M., Lehmann, S. and Wong, N. W., Social interaction and social support. Journal of Social Issues, 40,55-76, 1984.
49. Shumaker, S. A. and Brownnell, A., Toward a theory of social support: Closing the conceptual gaps. Journal ofSocial Issues, 40, 11-36, 1984.
______________________________________________________________________________________________________________
10

50. Singer, G. H.S. and Irvin, L. K., (1989). Family caregiving, stress, and support (pp. 9-25). In G.H.S. Singer& L.K. Irvin (eds.), Support for caregiving families. Baltimore MD: Paul H. Brookes.
51. Suelzle, M. and Keenan, V., Changes in family support networks over the life cycle of mentally retarded persons.American Journal of Mental Deficiency, 86, 267-274, 1981.
52. Thoits, P. A., Conceptual, methodological, and theoretical problems in studying social support as a buffer againstlife stress. Journal of Health and Social Behavior, 23, 145-159, 1982.
53. Thoits, P. A., (1985). Social support and psychological well-being: Theoretical possibilities (pp. 51-72). In G.Sarason & B.R. Sarason (eds.), Social support: Theory, research and application. Boston: Martinus Nijhoff.
54. Thoits, P. A., Social support as coping assistance. Journal of Consulting and Clinical Psychology, 54, 416-423,1986.
55. Trivette, C. M., Dunst, C. J., Deal, A. G., Hamer, A. W. and Propst, S., (1989). Assessing family strengths andfamily functioning style. Unpublished manuscript, Center for Family Studies, Morganton NC.
56. Trute, B. and Hauch, C., Building on family strength: A study of families with positive adjustment to the birth of adevelopmentally disabled child. Journal of Marital and Family Therapy, 14, 185-193, 1988a.
57. Trute, B. and Hauch, C., Social network attributes of families with positive adaptation to the birth of adevelopmentally disabled child. Canadian Journal of Community Mental Health, 7, 5-16, 1988b.
58. Turner, R. J., (1983). Direct, indirect, and moderating effects of social support on psychological distress andassociated conditions (pp. 105-155). In H.B. Kaplan (ed.), Psychosocial stress. New York: Academic Press.
59. Wellman, B., (1981). Applying network analysis to the study of support (pp. 171-200). In B.H. Gottlieb (ed.),Social networks and social support. Beverly Hills CA: Sage Publications.
60. Wilcox, B. L., Social support, life stress, and psychological adjustment: A test of the buffering hypothesis.American Journal of Community Psychology, 9, 371-386, 1981.
61. Wortman, C. B. and Lehman, D. R., (1985). Reactions to victims of life crisis: Support attempts that fail (pp.463-489). In I.G. Sarason & B.R. Sarason (eds.), Social support: Theory, research and applications. Boston:Martinus Nijhoff Publishers.
Manuscript received March 30, 1992; Revisions submitted September 25, 1992; Accepted January 22, 1993.
1This study yielded a direct, positive association between stress and social support. The authors interpret these findings toindicate that at the time of heightened stress, social support will increase, but that, over the course of a stressful life event, aninverse correlation between support and health outcomes would still be predicted.
______________________________________________________________________________________________________________
11