Embed Size (px)
DESCRIPTION
CONDUITE À TENIR PRATIQUE DEVANT UNE HYPOPHOSPHORÉMIE. Biblio du 09/04/2013 Mathilde LEMOINE. Fréquence de l’ hypophosphorémie chez les patients hospitalisés. AJM 2005 – Gaasbeek – Hypophosphatemia : an update of its etiology and treatment. - PowerPoint PPT Presentation
Citation preview

CONDUITE À TENIR PRATIQUE DEVANT UNE HYPOPHOSPHORÉMIE
Biblio du 09/04/2013 Mathilde LEMOINE

FRÉQUENCE DE L’HYPOPHOSPHORÉMIE CHEZ LES PATIENTS HOSPITALISÉS
AJM 2005 – Gaasbeek – Hypophosphatemia : an update of its etiology and treatment

RAPPELS DE PHYSIOLOGIE
Phosphore = 1% du poids du corps chez l’adulte
Répartition du phosphore : 85% os (cristaux d’hydroxyapatite) 14% liquide intracellulaire : ATP, acides
nucléiques, 2-3-DPG 1% liquide extracellulaire
Phosphore extracellulaire : 2/3 sous forme organique (non mesurée) 1/3 sous forme inorganique (Pi) : 0,8 à 1,45
mmol/L chez l’adulte ; à 90% sous forme libre ionisée ; minimale le matin à jeun (dosage)

RÔLE DU PHOSPHORE
Minéralisation osseuse Signalisation cellulaire (phosphorylation) Énergie : ATP Transport de l’O2 : 2-3-Diphosphoglycérate
(libération de l’O2 transporté par l’Hb) Synthèse d’ADN Intégrité membranaire Homéostasie acido-basique

MÉTABOLISME DU PHOSPHORE
AJM 2005 – Gaasbeek – Hypophosphatemia : an update of its etiology and treatment

Régulation du P : intestin ↔ os ↔ rein ↔ parathyroïdes
NRN 2010 – Farrow and White – Recent advances in renal phosphate handling

FACTEURS INFLUENÇANT LA PHOSPHATÉMIE

CONDUITE À TENIR DEVANT UNE HYPOPHOSPHATÉMIE
Connaître les facteurs de risque L’évoquer : signes cliniques de
l’hypophosphatémie La confirmer : dosage P sanguin Rechercher des complications :
Examen clinique Rechercher une étiologie : distinguer
aigu/chronique Aiguë : contexte +++ Chronique : Examen clinique / Biologie / Imagerie
Traiter la cause et supplémenter en P

FACTEURS DE RISQUE D’HYPOP AIGUË
Alcoolisme Dénutrition / anorexie mentale Post-opératoire : chirurgie hépatique,
parathyroïdectomie ++ Sepsis

SYMPTOMATOLOGIE
Symptomatique si sévère (P < 0,3mmol/L) et déplétion phosphatée : Symptômes liés à la diminution de l’ATP
(énergie) et du 2-3-DFG (transport O2) SNC : anxiété, paresthésies, convulsions, coma Muscles : myalgies, faiblesse, myopathie
proximale Squelette : douleurs osseuses, ostéomalacie,
rachitisme Insuffisance cardiaque et respiratoire Acidose métabolique, hémolyse, …

RECHERCHER UNE ÉTIOLOGIE
Trois types de cause :
Situations aiguës : Redistribution entre les secteurs intra et
extracellulaires
Situations chroniques : Diminution de l’absorption intestinale Augmentation de pertes rénales
Causes mixtes

EXAMEN CLINIQUE
Complications Étiologie :
Contexte clinique : aigu / chronique Atcd, prise alimentaire / médicamenteuse Examen musculo-squelettique Masse palpable (TIO) Cutané : tâches café au lait

BIOLOGIE : LE MATIN À JEUN
Sang : P, Ca, Créatinine, 1-25-OH-vitD, PTH Urines : P, Ca, Créatinine Phosphaturie :
< 5mmol/24h : origine extra-rénale envisagée > 5mmol/24h : origine rénale envisagée :
calculer TmPi/DFG Excrétion fractionnelle du phosphate :
(Pi(u) x Créat(p)) / (Pi(p) x Créat(u)) < 20% : extra-rénal > 20% : rénal : calculer TmPi/DFG

BIOLOGIE (2)
Détermination du TmPi/DFG : Capacité de réabsorption maximale de P
indépendante des variations de la charge filtrée Normale : 0,77 à 1,45 mmol/L de filtrat
glomérulaire Permet de distinguer les pertes digestives ou
rénales de phosphate en cas d’hypoP chronique Pertes rénales :
HypoP + TmPi/DFG bas ou anormalement normal + phosphaturie conservée > 5mmol/24h

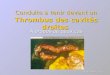
DIAGRAMME DE BIJVOET
Nécessaires : P et Créatinine sanguins et urinaires en mmol/L

BIOLOGIE (3)
Si TmPi/DFG élevé : cause extra-rénale Si TmPi/DFG bas :
Eliminer une hyperparathyroïdie I ou II : mesure Ca sanguin et urinaire, PTH, 25(OH)vitD, calcitriol
Si Ca, PTH et 25(OH)vitD normaux : rechercher des signes de tubulopathie proximale : mesure protéinurie, kaliémie, bicarbonatémie, uricémie
Puis selon orientation clinique

IMAGERIE
Si hypoP chronique : Rx osseuses standards Scintigraphie osseuse au Tc99 Ostéodensitométrie Biopsie osseuse en 2ème intention

HYPOP AIGUË : REDISTRIBUTION INTERNE
Sans déplétion phosphatée : Alcalose respiratoire aiguë (++ sepsis, V°) Iatrogénie : insuline, catécholamines, apports
massifs d’hydrates de carbone Avec déplétion phosphatée :
Correction d’une acidocétose diabétique Syndrome de renutrition (augmentation de la
sécrétion d’insuline) Prolifération cellulaire rapide Mécanismes de réparation osseuse : après
parathyroïdectomie, hungry bone syndrome

PRINCIPALES CAUSES D’HYPOP SÉVÈRE

DIMINUTION DE L’ABSORPTION INTESTINALE
Apports alimentaires faibles Iatrogénie : chélateurs du phosphore, anti-
acides à base d’aluminium ou de magnésium (chélation intestinale du phosphate)
Carence / résistance à la vitamine D Stéatorrhée et diarrhée chronique Vomissements

DIMINUTION DE LA RÉABSORPTION TUBULAIRE
Non liée au FGF-23 : Hyperparathyroïdie I ou II Syndrome de Fanconi Iatrogénie : diurétiques, corticoïdes Déficit/résistance à la vitamine D HHRH (Rachitisme Hypophosphatémique
Héréditaire avec Hypercalciurie) : mutation SLC34A3 codant pour NPT2c

DIMINUTION DE LA RÉABSORPTION TUBULAIRE
Liée au FGF-23 : ADHR : Rachitisme Hypophosphatémique
Autosomique Dominant ARHR: récessif XLH : HypoP Liée à l’X Dysplasie fibreuse du sd de Mc Cune Albright TIO : Tumeurs Inductrices d’Ostéomalacie Transplantation rénale Fer IV

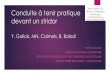
HypoP liée au FGF-23
NRN 2010 – Farrow and White – Recent advances in renal phosphate handling

TRAITEMENT (1)
A initier après les tests biologiques ++ Ttt de la maladie causale ++ Supplémentation si déplétion :
Non nécessaire si HypoP légère (0,6 à 0,8mmol/L)
Per os si HypoP modérée (0,3 à 0,6mmol/L) IV si HypoP sévère (<0,3mmol/L)

TRAITEMENT (2)
Phosphore p.o. : lait (1g/L), NaP, KP 20 à 40 mg/kg/j en 4 prises (Carpenter et al)
Ou 1 à 2g/j pendant 10 jours, apports répartis dans la journée (EMC)
Avantages : plus sûr d’utilisation E.I. : absorption incertaine, troubles digestifs

TRAITEMENT (3)
Phosphore IV: KP : 0,08 à 0,16mmol/kg toutes les 2 à 6 heures (EMC)
Ou 15mmol sur 2h à répéter à 6h, maximum 45mmol/24h (Rosen et al)
Avantages : rapidité E.I. : hypoCa (par diminution de la 1-
25(OH)vitD3), hyperK, hyperP, arythmie, calcifications, IRA
Précautions : scope, surveillance P-Ca/6 heures Contre-indications : hypoCa, IR

TRAITEMENT (4)
JCEM 2012 – Imel and Econs - Approch to the hypophosphatemic patient

TRAITEMENT (5)
Spécificités : Redistribution : supplémentation ssi déplétion P,
hypoP sévère ou symptomatique Pertes rénales : Dipyridamole 300mg/j (Dipyridamole
decreases renal phosphate leak and augments serum phosphorus in patients with low renal phosphate threshold. AmSoc Nephrol 1998)
HypoP liées au FGF-23 : supplémentation en P et Calcitriol
XLH : Cinacalcet (FGF-23 and 1,25 D in children with hypophospatemic rickets: effect of treatment with phosphate, cinacalcet and rocaltrol. J Bone Miner Res. 2007)
TIO : résection complète puis surveillance de la phosphorémie et des PAL

TRAITEMENT (6)
Spécificités (suite) : Sd de Fanconi : supplémentation P-Ca Transplanté :
Augmentation des apports (Hypophosphatemia in kidney transplant recipients: report of acute phosphate nephropathy as a complication of therapy. Am J Kidney Dis. 2011),
Supplémentation P p.o en 2ème intention Cinacalcet (Phosphatemic effect of cinacalcet in kidney transplant recipients with persistent
hyperparathyroidism. Am J Kidney Dis. 2008)

TRAITEMENT PRÉVENTIF
Repérer les patients à risque Refeeding sd :
Surveillance biologique Supplémentation PK IV si alimentation
parentérale (0,5mmol/kg/j de P (EMC ; Stanga et al))

HYPOP ET VIH
Prévalence : 7 à 26% selon les études Causes :
Non spécifiques Spécifiques :
Carence en vitamine D Hyperparathyroïdie II Toxicité tubulaire proximale des ARV (INTI : Fovirs) :
sd de Fanconi ou hypoP isolée

HYPOP ET VIH : PRISE EN CHARGE
Diagnostic :
Ttt : de la cause +/- supplémentation Suivi : Ca, P et vitD : dg, initiation du ttt puis
annuel ; TmPi/DFG ?Bagnis-2009 : Hypophosphatemia : an easy strategy for diagnosis and treatment in HIV patient

CONCLUSION
HypoP aiguë : Contexte souvent évident : ttt de la cause Prévention du syndrome de renutrition Supplémentation si déplétion phosphatée, hypoP
sévère ou symptomatique
HypoP chronique : Distinguer causes rénales ou extra-rénales :
TmPi/DFG Recherche et ttt de la cause Supplémentation p.o. à préférer

BIBLIOGRAPHIE EMC 2008 : Exploration des fonctions tubulaires rénales La lettre d’ICAR en néphrologie 2006 - Hypophosphatémie AJM 2005 – Gaasbeek – Hypophosphatemia : an uptade of its
etiology and treatment IMP 2009 – Bagnis - Hypophosphatemia : an easy strategy for
diagnosis and treatment in HIV patients NRN 2010 – Naderi - Hereditary disorders of renal phosphate
wasting NRN 2010 – Farrow and White – Recent advances in renal phosphate
handling KI 2011 – Harald Jüppner - Phosphate and FGF-23 AJKD 2012 – Feldenfeld - Approch to treatment of hypophosphatemia JCEM 2012 – Imel and Econs - Approch to the hypophosphatemic
patient
- Merci pour votre attention -