Embed Size (px)
Citation preview
Conference Summary, January 5th, 2015
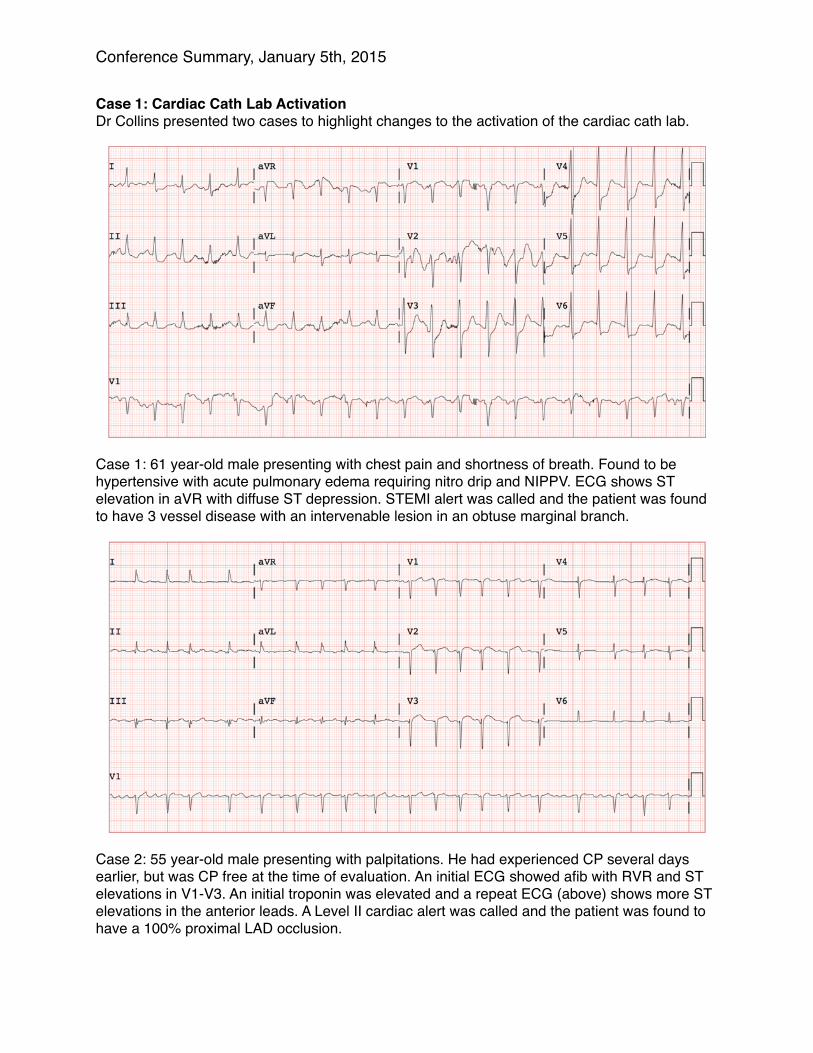
Case 1: Cardiac Cath Lab Activation Dr Collins presented two cases to highlight changes to the activation of the cardiac cath lab.
Case 1: 61 year-old male presenting with chest pain and shortness of breath. Found to be hypertensive with acute pulmonary edema requiring nitro drip and NIPPV. ECG shows ST elevation in aVR with diffuse ST depression. STEMI alert was called and the patient was found to have 3 vessel disease with an intervenable lesion in an obtuse marginal branch.
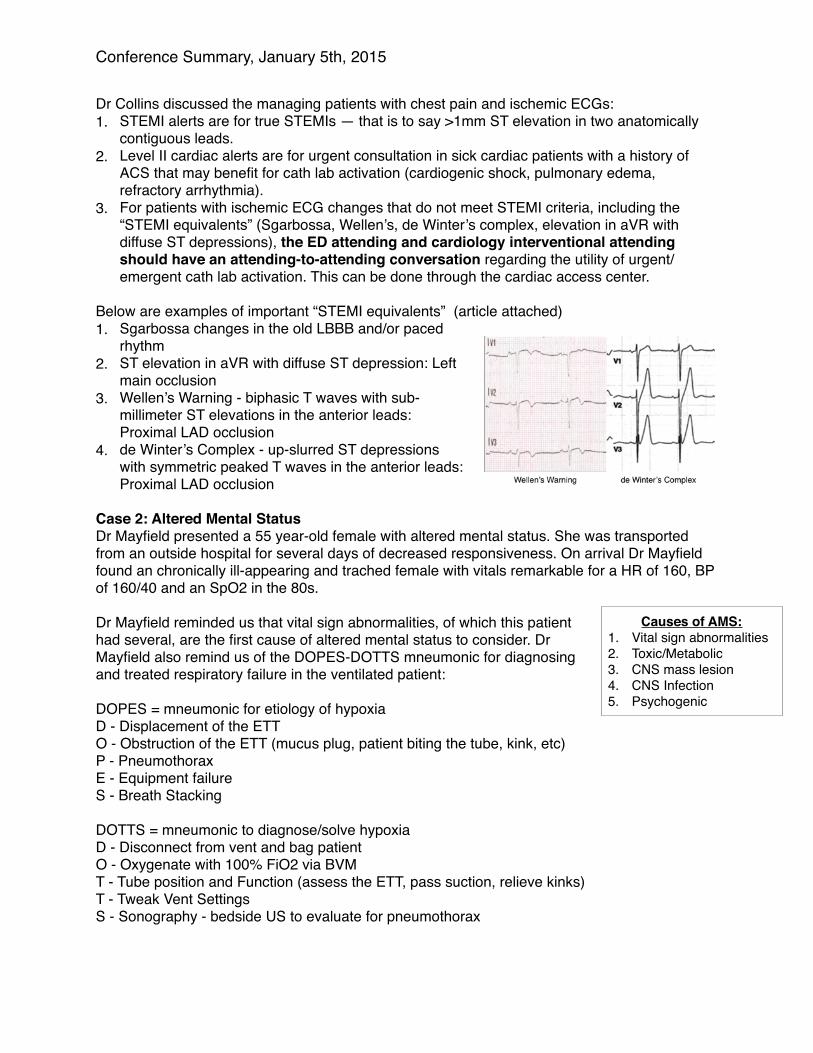
Case 2: 55 year-old male presenting with palpitations. He had experienced CP several days earlier, but was CP free at the time of evaluation. An initial ECG showed afib with RVR and ST elevations in V1-V3. An initial troponin was elevated and a repeat ECG (above) shows more ST elevations in the anterior leads. A Level II cardiac alert was called and the patient was found to have a 100% proximal LAD occlusion.
Conference Summary, January 5th, 2015
Dr Collins discussed the managing patients with chest pain and ischemic ECGs: 1. STEMI alerts are for true STEMIs — that is to say >1mm ST elevation in two anatomically
contiguous leads. 2. Level II cardiac alerts are for urgent consultation in sick cardiac patients with a history of
ACS that may benefit for cath lab activation (cardiogenic shock, pulmonary edema, refractory arrhythmia).
3. For patients with ischemic ECG changes that do not meet STEMI criteria, including the “STEMI equivalents” (Sgarbossa, Wellen’s, de Winter’s complex, elevation in aVR with diffuse ST depressions), the ED attending and cardiology interventional attending should have an attending-to-attending conversation regarding the utility of urgent/emergent cath lab activation. This can be done through the cardiac access center.
Below are examples of important “STEMI equivalents” (article attached)1. Sgarbossa changes in the old LBBB and/or paced
rhythm 2. ST elevation in aVR with diffuse ST depression: Left
main occlusion3. Wellen’s Warning - biphasic T waves with sub-
millimeter ST elevations in the anterior leads: Proximal LAD occlusion
4. de Winter’s Complex - up-slurred ST depressions with symmetric peaked T waves in the anterior leads: Proximal LAD occlusion
Case 2: Altered Mental Status Dr Mayfield presented a 55 year-old female with altered mental status. She was transported from an outside hospital for several days of decreased responsiveness. On arrival Dr Mayfield found an chronically ill-appearing and trached female with vitals remarkable for a HR of 160, BP of 160/40 and an SpO2 in the 80s.
Dr Mayfield reminded us that vital sign abnormalities, of which this patient had several, are the first cause of altered mental status to consider. Dr Mayfield also remind us of the DOPES-DOTTS mneumonic for diagnosing and treated respiratory failure in the ventilated patient: DOPES = mneumonic for etiology of hypoxia D - Displacement of the ETT O - Obstruction of the ETT (mucus plug, patient biting the tube, kink, etc) P - Pneumothorax E - Equipment failure S - Breath Stacking
DOTTS = mneumonic to diagnose/solve hypoxia D - Disconnect from vent and bag patient O - Oxygenate with 100% FiO2 via BVM T - Tube position and Function (assess the ETT, pass suction, relieve kinks) T - Tweak Vent Settings S - Sonography - bedside US to evaluate for pneumothorax
Causes of AMS: 1. Vital sign abnormalities2. Toxic/Metabolic 3. CNS mass lesion 4. CNS Infection 5. Psychogenic
Conference Summary, January 5th, 2015
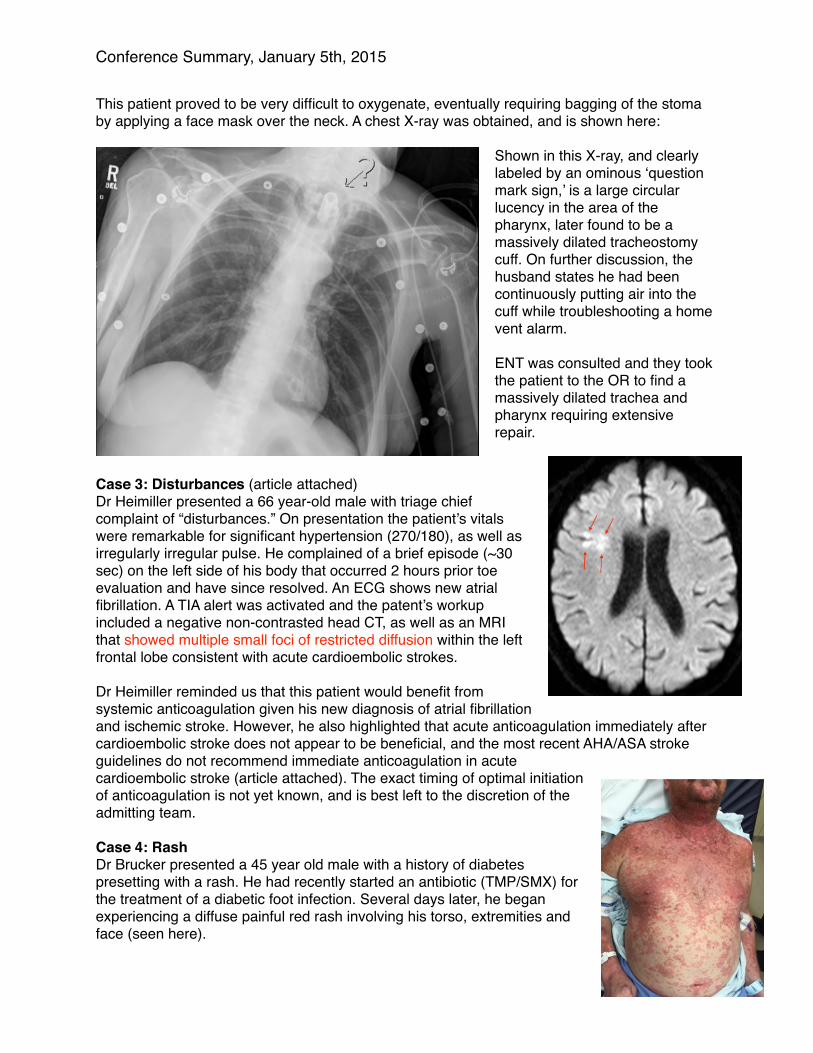
This patient proved to be very difficult to oxygenate, eventually requiring bagging of the stoma by applying a face mask over the neck. A chest X-ray was obtained, and is shown here:
Shown in this X-ray, and clearly labeled by an ominous ‘question mark sign,’ is a large circular lucency in the area of the pharynx, later found to be a massively dilated tracheostomy cuff. On further discussion, the husband states he had been continuously putting air into the cuff while troubleshooting a home vent alarm.
ENT was consulted and they took the patient to the OR to find a massively dilated trachea and pharynx requiring extensive repair.
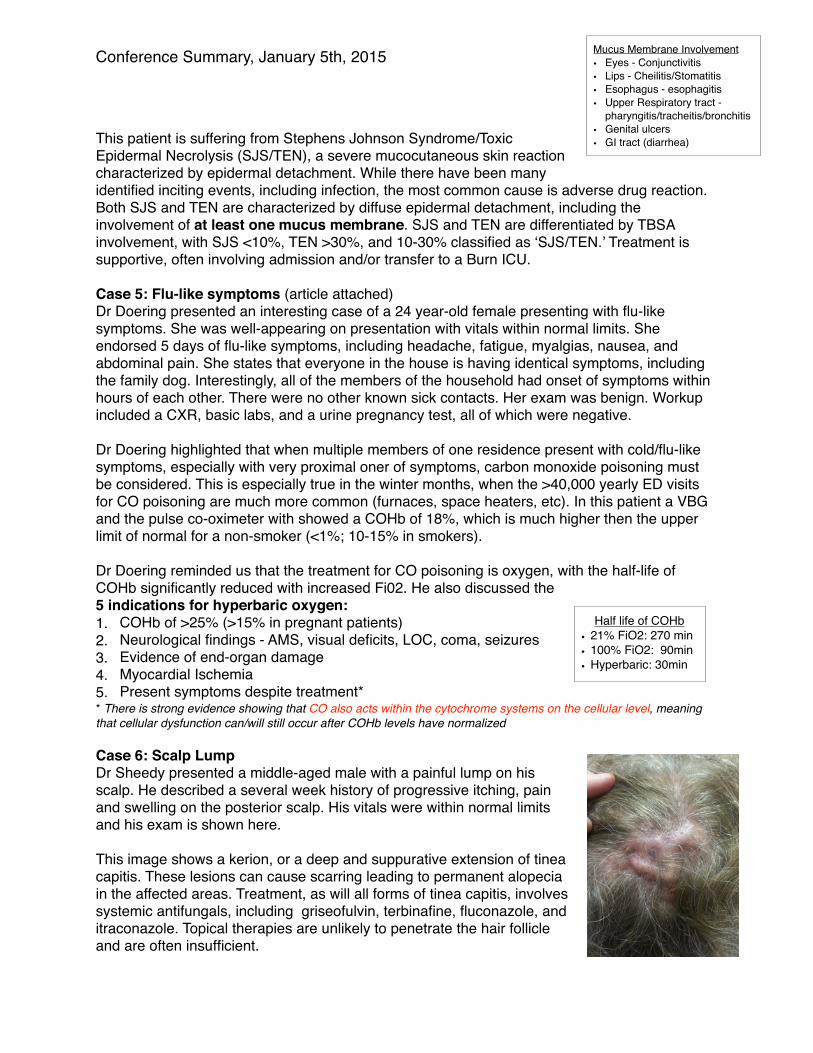
Case 3: Disturbances (article attached)Dr Heimiller presented a 66 year-old male with triage chief complaint of “disturbances.” On presentation the patient’s vitals were remarkable for significant hypertension (270/180), as well as irregularly irregular pulse. He complained of a brief episode (~30 sec) on the left side of his body that occurred 2 hours prior toe evaluation and have since resolved. An ECG shows new atrial fibrillation. A TIA alert was activated and the patent’s workup included a negative non-contrasted head CT, as well as an MRI that showed multiple small foci of restricted diffusion within the left frontal lobe consistent with acute cardioembolic strokes.
Dr Heimiller reminded us that this patient would benefit from systemic anticoagulation given his new diagnosis of atrial fibrillation and ischemic stroke. However, he also highlighted that acute anticoagulation immediately after cardioembolic stroke does not appear to be beneficial, and the most recent AHA/ASA stroke guidelines do not recommend immediate anticoagulation in acute cardioembolic stroke (article attached). The exact timing of optimal initiation of anticoagulation is not yet known, and is best left to the discretion of the admitting team.
Case 4: RashDr Brucker presented a 45 year old male with a history of diabetes presetting with a rash. He had recently started an antibiotic (TMP/SMX) for the treatment of a diabetic foot infection. Several days later, he began experiencing a diffuse painful red rash involving his torso, extremities and face (seen here).
Conference Summary, January 5th, 2015
This patient is suffering from Stephens Johnson Syndrome/Toxic Epidermal Necrolysis (SJS/TEN), a severe mucocutaneous skin reaction characterized by epidermal detachment. While there have been many identified inciting events, including infection, the most common cause is adverse drug reaction. Both SJS and TEN are characterized by diffuse epidermal detachment, including the involvement of at least one mucus membrane. SJS and TEN are differentiated by TBSA involvement, with SJS <10%, TEN >30%, and 10-30% classified as ‘SJS/TEN.’ Treatment is supportive, often involving admission and/or transfer to a Burn ICU.
Case 5: Flu-like symptoms (article attached)Dr Doering presented an interesting case of a 24 year-old female presenting with flu-like symptoms. She was well-appearing on presentation with vitals within normal limits. She endorsed 5 days of flu-like symptoms, including headache, fatigue, myalgias, nausea, and abdominal pain. She states that everyone in the house is having identical symptoms, including the family dog. Interestingly, all of the members of the household had onset of symptoms within hours of each other. There were no other known sick contacts. Her exam was benign. Workup included a CXR, basic labs, and a urine pregnancy test, all of which were negative.
Dr Doering highlighted that when multiple members of one residence present with cold/flu-like symptoms, especially with very proximal oner of symptoms, carbon monoxide poisoning must be considered. This is especially true in the winter months, when the >40,000 yearly ED visits for CO poisoning are much more common (furnaces, space heaters, etc). In this patient a VBG and the pulse co-oximeter with showed a COHb of 18%, which is much higher then the upper limit of normal for a non-smoker (<1%; 10-15% in smokers).
Dr Doering reminded us that the treatment for CO poisoning is oxygen, with the half-life of COHb significantly reduced with increased Fi02. He also discussed the 5 indications for hyperbaric oxygen: 1. COHb of >25% (>15% in pregnant patients) 2. Neurological findings - AMS, visual deficits, LOC, coma, seizures 3. Evidence of end-organ damage 4. Myocardial Ischemia 5. Present symptoms despite treatment** There is strong evidence showing that CO also acts within the cytochrome systems on the cellular level, meaning that cellular dysfunction can/will still occur after COHb levels have normalized
Case 6: Scalp LumpDr Sheedy presented a middle-aged male with a painful lump on his scalp. He described a several week history of progressive itching, pain and swelling on the posterior scalp. His vitals were within normal limits and his exam is shown here.
This image shows a kerion, or a deep and suppurative extension of tinea capitis. These lesions can cause scarring leading to permanent alopecia in the affected areas. Treatment, as will all forms of tinea capitis, involves systemic antifungals, including griseofulvin, terbinafine, fluconazole, and itraconazole. Topical therapies are unlikely to penetrate the hair follicle and are often insufficient.
Half life of COHb• 21% FiO2: 270 min• 100% FiO2: 90min• Hyperbaric: 30min
Mucus Membrane Involvement• Eyes - Conjunctivitis • Lips - Cheilitis/Stomatitis• Esophagus - esophagitis• Upper Respiratory tract -
pharyngitis/tracheitis/bronchitis • Genital ulcers • GI tract (diarrhea)
Conference Summary, January 5th, 2015
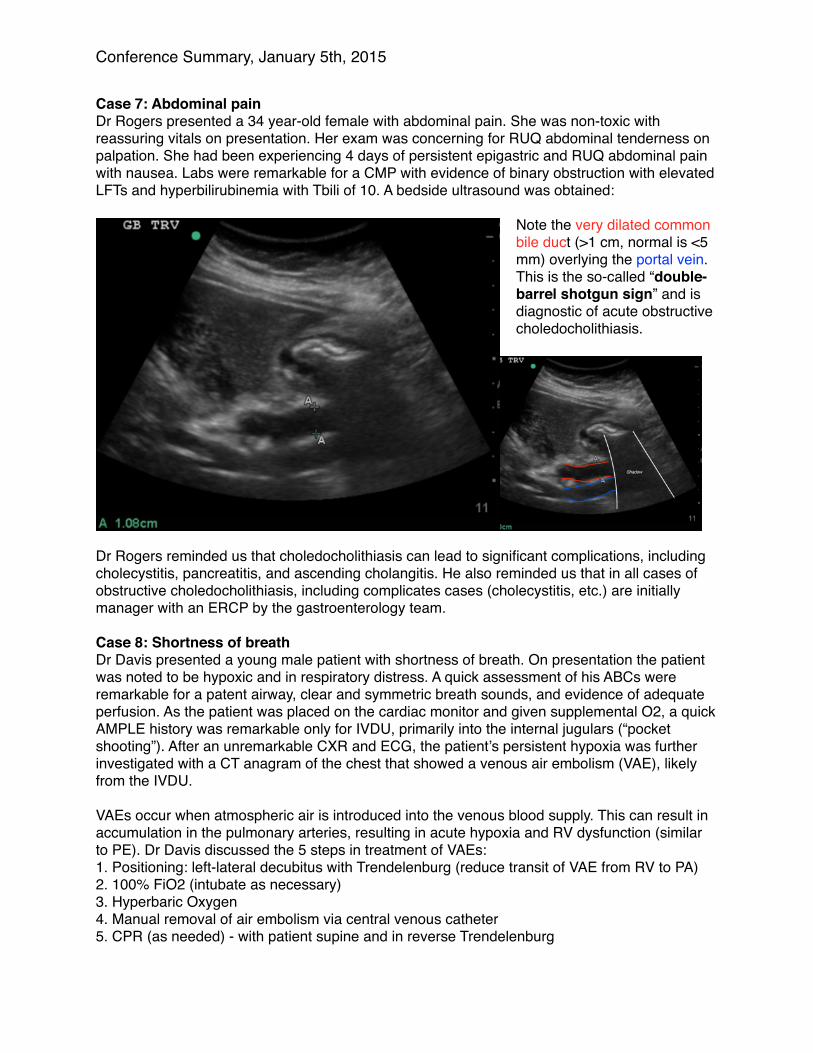
Case 7: Abdominal pain Dr Rogers presented a 34 year-old female with abdominal pain. She was non-toxic with reassuring vitals on presentation. Her exam was concerning for RUQ abdominal tenderness on palpation. She had been experiencing 4 days of persistent epigastric and RUQ abdominal pain with nausea. Labs were remarkable for a CMP with evidence of binary obstruction with elevated LFTs and hyperbilirubinemia with Tbili of 10. A bedside ultrasound was obtained:
Note the very dilated common bile duct (>1 cm, normal is <5 mm) overlying the portal vein. This is the so-called “double-barrel shotgun sign” and is diagnostic of acute obstructive choledocholithiasis.
Dr Rogers reminded us that choledocholithiasis can lead to significant complications, including cholecystitis, pancreatitis, and ascending cholangitis. He also reminded us that in all cases of obstructive choledocholithiasis, including complicates cases (cholecystitis, etc.) are initially manager with an ERCP by the gastroenterology team.
Case 8: Shortness of breath Dr Davis presented a young male patient with shortness of breath. On presentation the patient was noted to be hypoxic and in respiratory distress. A quick assessment of his ABCs were remarkable for a patent airway, clear and symmetric breath sounds, and evidence of adequate perfusion. As the patient was placed on the cardiac monitor and given supplemental O2, a quick AMPLE history was remarkable only for IVDU, primarily into the internal jugulars (“pocket shooting”). After an unremarkable CXR and ECG, the patient’s persistent hypoxia was further investigated with a CT anagram of the chest that showed a venous air embolism (VAE), likely from the IVDU.
VAEs occur when atmospheric air is introduced into the venous blood supply. This can result in accumulation in the pulmonary arteries, resulting in acute hypoxia and RV dysfunction (similar to PE). Dr Davis discussed the 5 steps in treatment of VAEs: 1. Positioning: left-lateral decubitus with Trendelenburg (reduce transit of VAE from RV to PA)2. 100% FiO2 (intubate as necessary) 3. Hyperbaric Oxygen 4. Manual removal of air embolism via central venous catheter5. CPR (as needed) - with patient supine and in reverse Trendelenburg





























