Embed Size (px)
Citation preview
Australian Journal of Ophthalmology 1983; 11: 209-213
CONGENITAL ANTERIOR SEGMENT EPITHELIALISATION (CASE)
LAWRENCE W. HlRST FRACO The Wiirner Ophlhalrnoiogicai lnshfufe The Johns Hopkins Medical insfitufions, Baitirnore. Maryland
Abstract Posterior polymorphous endothelial dystrophy and iridocorneal endothelial syndrome share common specular microscopic findings, clinical course, and some histopatholog/cal features Despite differences in inherited trait and severity of disease a common pathogenetic mechanism for the two diseases is suggested This consists of congenital epithelia6ation of the posterior corneal surface during embryogenesis with migration of these cells around the anterior segment uninhibited by surrounding normal endothebum
Key words iridocorneal endothelial syndrome, posterior polymorphous endothelial dystrophy specular microscopy. corneal endothelium, epifhelialisation, ultrastructural pathology. hypothesis
INTRODUCTION The clinical course and histopathology of three disparate anterior segment conditions-the iridocorneal endothelial (ICE) syndrome,’ posterior polymorphous endothelial dystrophy, and epithelial ingrowth’-may lead to a very similar end result including corneal opacification, extensive peripheral anterior synechiae, iris distortion, and glaucoma. In all three conditions the end result may be loss of vision or loss of the eye.
Examination of the corneal endothelial surface in the first two diseases by specular microscopy in an early stage of the disease, for which histopathology has not previously been a~ailable,~.’ has permitted some clinicospecular microscopic/pathologic correlations to be drawn.
The implications of these correlations in the two naturally-occurring diseases, ICE syndrome and posterior polymorphous endothelial dystrophy, will be addressed.
MATERIALS AND METHODS The ICE Syndrome Thirty patients with the clinical diagnosis of either Chandler’s syndrome, essential iris atrophy, or iris nevus syndrome were examined clinically by slit-lamp examination, gonioscopy, intraocular pressure measurement, and clinical specular microscopy. A minimum of 36 frames of either small-field6 and/or wide-field specular microscopy’ weJe taken of each eye.
Histopathological examination of the cornea and, in some cases, iris was obtained in six of these patients. These specimens were examined by light microscopy, transmission electron microscopy, and scanning electron microscopy.
The cornea of one of these patients was submitted also for keratin staining.
Posterior Polymorphous Endothelial Dystrophy Thirty-six patients with a clinical diagnosis of posterior polymorphous endothelial dystrophy were examined by slit-lamp examination,
Reprint requesfs: Dr Lawrence W. Hirst, Johns Hopkins Hospital, Wilmer Institute, Baltimore, Maryland 21205, USA.
CONGENITAL ANTERIOR SEGMENT EPITHELIALISATION (CASE) 209
gonioscopy, intraocular pressure measurement, and clinical specular microscopy. A minimum of 36 frames of either wide-field or small-field specular microscopy were taken of each eye where corneal clarity permitted.
Corneal specimens were obtained from six of these patients for ultrastructural examination.
Manual digitisation was performed using a Hewlett Packard 9845 computer and interfaced digitiser ‘on the endothelial cells of selected micrographs of the opposite eyes of patients with the ICE syndrome and of both eyes of patients with posterior polymorphous endothelial dystrophy.
RESULTS The ICE Syndrome Of the 30 patients there were 21 with Chandler’s syndrome,’ with essential iris atrophy, and two with iris nevus syndrome. The average age was 43 years with a range of 20 to 7 2 . The female to male ratio was two to one. Glaucoma surgery and/or medication were required in three- quarters of the patients, and penetrating keratoplasty in two. Vision and fields were lost in half these patients in their affected eye at the time of presentation.
Clinical specular microscopy confirmed a consistent pattern of abnormal endothelial cells in the involved eye which consisted of grossly pleomorphic, bizarre c e k 4 These cells contained large central or eccentric “blackout” areas, frequently associated with a reversal of the cell outlines, that is, bright outlines of cell boundaries with dark interiors. In one patient only was any area of apparently normal endothelium seen. Digitisation of these cells was not possible because of their poor definition.
Digitisation of cell outlines and calculation of distribution of cell areas from specular micrographs of the uninvolved eye revealed a consistently increased spread of cell areas in comparison with patients of the same age. There appeared to be a definite tendency of the cells to become somewhat smaller with advancing age in the uninvolved eyes of these patients, in contrast to the generally accepted increase in cell size in the normal population.
210
Histopathological examination of one case revealed definite epithelial-like characteristics of the cells lining the posterior surface of the cornea and the anterior surface of the iris specimen including desmosomal formation, intracyto- plasmic filament formation (8nm diameter), microvillus projection,* and some basement membrane production. In addition, the specimen of the iris suggested polarisation of the cell organelles and some overlapping and multi- layering of the cells on the back of the posterior surface of the cornea. Staining for keratin in this case was positive in the cells lining the back surface of the cornea.
Ultrastructural examination of a further six specimens revealed epithelial-like characteristics, including intracytoplasmic filament formation, desmosome formation, microvillus projections and basement membrane formation, in four specimens.
Posterior Polymorphous Endothelial Dystrophy The clinical examination of 36 patients with posterior polymorphous endothelial dystrophy revealed typical vesicular or band-shaped lesions in 25 cases, and a geographic or geographic/ vesicular mixture of morphology in a further 13. The average age was 26 years (range 6 months to 7 6 years), and the male to female ratio was one to one. Three of these patients came to transplantation because of their disease and a further three had significant disease requiring medication or surgery. Visual loss or field loss occurred in a further three patients.
Clinical specular microscopy revealed two cell populations on the posterior surface of the cornea. First , the general background endothelium in most patients had a grossly pleomorphic appearance. Digitisation and calculation of the distribution of cell areas in 10 of these cases revealed cell areas increased twofold compared with a normal age-matched population. In two patients (both with the geographic type variant) the density of the background endothelial cell population was significantly increased with the cells being half the size of a normal age-match control. Second, the localised areas of vesicular, band-shaped, or
AUSTRALIAN JOURNAL OF OPHTHALMOLOGY
geographic type abnormalities on specular microscopy revealed bizarre, large cells with intracellular blackout areas and reversal of cell contrast. These were sharply demarcated from the surrounding background endothelium and corresponded to the slit-lamp location of the vesicular, band-shaped, or geographic abnormalities. Digitisation of these cells was not possible because of their lack of definition.
Histopathological examination of four of these cases confirmed the well-recognised appearance of more than one layer of the posterior surface of the cornea. These cells had a number of characteristics of corneal epithelium.
The clinical specular microscopic appearance of the cells lining the entire cornea in the involved eyes in the ICE syndrome appeared morpho- logically identical to the cells within the localised abnormalities on the posterior surface of the corneas with posterior polymorphous endothelial dystrophy.
DISCUSSION As the ICE syndrome is a sporadic disease,’ clinical identification of patients with this disease occurs either at an asymptomatic stage during routine examination, usually in the teens or later, or as a result of early glaucoma or corneal problems secondary to the disease itself. The youngest patient in ou r series was 15 years old. Despite controversy about the possible sequence of events with primary iridocorneal adhesions and secondary endothelial changes, it .is generally now accepted that the endothelial changes precede angle and iris involvement. This is supported by the uniform involvement of the entire corneal surface seen by specular microscopy in early stages prior to significant peripheral anterior synechiae (PAS) formation. The requirement for glaucoma medication or glaucoma surgery early in the disease as a result of secondary angle closure by broad anterior synechiae suggests migration of cells around the angle from the posterior corneal surface early in the disease. Most corneal specimens obtained for pathological examination had been obtained at a later stage after treatment of glaucoma and
subsequent failure of the corneal pump mechanism and corneal oedema. In these cases the cells on the posterior corneal surface are frequently scanty and difficult to characterise. In those cases which a well-preserved layer has been examined histopathologically there appears to be evidence for epithelial-like characteristics* of these cells on the posterior surface of the cornea.
Evidence from examination by specular microscopy of the opposite eye confirms some abnormalities of the endothelial layer of these eyes as well. Despite the absence of abnormal cell types the endothelial layer appears to become more pleomorphic with advancing age and also somewhat more cellular. The ICE syndrome may well be a bilateral disease with a superimposed factor giving rise to the gross asymmetry of involvement
Posterior polymorphous endothelial dystrophy has been less well recognized as leading to migration of cells on to the angle and anterior iris surface and causing secondary glaucoma.’ Although this occurs relatively uncommonly with posterior polymorphous endothelial dystrophy, the histological appearance of such cases has been well demonstrated as consisting of a similar pattern of cells to that seen in the ICE ~ y n d r o m e . ~ More commonly, the cornea is examined histopathologically after penetrating keratoplasty for corneal decompensation alone without secondary angle involvement. L o These cases also demonst ra te epit helial-like characteristics of some of the cells lining the posterior surface of the cornea.’’
Specular microscopy demonstrates a “normal” endothelium albeit extremely pleomorphic and reduced in cell density in cases of vesicular or band-shaped type posterior polymorphous endothelial dystrophy. These areas of endothelium surround areas of bizarre cells which are similar to those covering the entire surface of the affected eyes in the ICE syndrome.
In the geographic variant of posterior polymorphous endothelial dystrophy, larger areas of abnormal bizarre cells are found sharply demarcated from the surrounding endothelium, which in many cases appears distinctly abnormal
CONGENI I A L AN I EKlOK StGMLNT EPI I HELIAI ISATION (CASL) 21 1
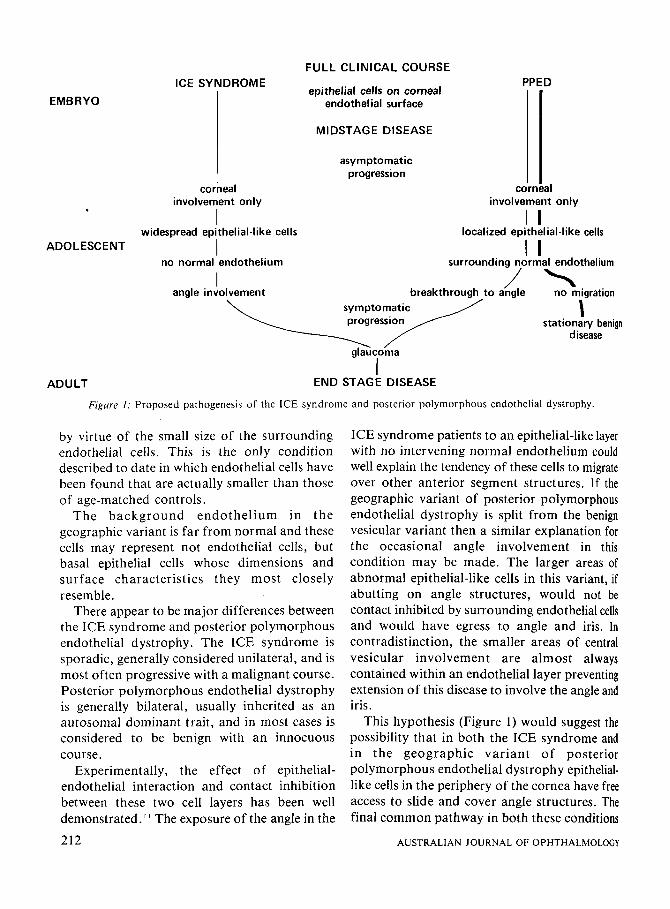
FULL CLINICAL COURSE
epithelial cells on corneal endothelial surface I
ICE SYNDROME EMBRYO
PPED
I I I I MI DSTAG E DISEASE
corneal involvement only
widespread epithelial-like cells I I ADOLESCENT
asymptomatic progression I I
corneal involvement only
localized epithelial-like cells I I I I
no normal endothelium
angle involvement
surrounding normal endothelium
I symptomatic I
stationary benign disease
I A D U L T END STAGE DISEASE
Figure I: Proposed pathogenesis of the ICE syndrome and posterior polymorphous endothelial dystrophy.
by virtue of the small size of the surrounding endothelial cells. This is the only condition described to date in which endothelial cells have been found that are actually smaller than those of age-matched controls.
The background endothelium in the geographic variant is far from normal and these cells may represent not endothelial cells, but basal epithelial cells whose dimensions and surface characteristics they most closely resemble.
There appear to be major differences between the ICE syndrome and posterior polymorphous endothelial dystrophy. The ICE syndrome is sporadic, generally considered unilateral, and is most often progressive with a malignant course. Posterior polymorphous endothelial dystrophy is generally bilateral, usually inherited as an autosomal dominant trait, and in most cases is considered to be benign with an innocuous course.
Experimentally, the effect of epithelial- endothelial interaction and contact inhibition between these two cell layers has been well demonstrated." The exposure of the angle in the
ICE syndrome patients to an epithelial-like layer with no intervening normal endothelium could well explain the tendency of these cells to migrate over other anterior segment structures. If the geographic variant of posterior polymorphous endothelial dystrophy is split from the benign vesicular variant then a similar explanation for the occasional angle involvement in this condition may be made. The larger areas of abnormal epithelial-like cells in this variant, if abutting on angle structures, would not be contact inhibited by surrounding endothelial cells and would have egress to angle and iris. In contradistinction, the smaller areas of central vesicular involvement are almost always contained within an endothelial layer preventing extension of this disease to involve the angle and iris.
This hypothesis (Figure 1) would suggest the possibility that in both the ICE syndrome and in the geographic variant of posterior polymorphous endothelial dystrophy epithelial- like cells in the periphery of the cornea have free access to slide and cover angle structures. The final common pathway in both these conditions
212 AUSTRALIAN JOURNAL OF OPHTHALMOLOGY
of broad PAS, iris distortion, and glaucoma resemble closely the end stage of epithelial downgrowth following surgery with a patho- genesis that in the latter disease has been well documented histopathologically.
What remains to be explained is the major difference of an apparent inherited trait in posterior polymorphous endothelial dystrophy and a sporadic occurrence in the ICE syndrome. The absence of history of postnatal trauma, infection, or other common factors in the involved eyes of the ICE patients makes the likelihood of postnatal metaplasia or change in a pre-existing normal endothelial layer unlikely. The slow changes observed once these patients have been identified suggests that, at least in some of the younger patients, the condition has been present a number of years, and probably since birth. The abnormalities of the endothelial cells in the contralateral eyes would also suggest a prenatal abnormality during the invasion of mesenchyme into the optic cup at two months’ gestation. The asymmetry of ocular involvement remains to be explained.
There is no suggestion that posterior polymorphous endothelial dystrophy and the ICE syndrome are one and the same condition or even that they occupy different ends of a spectrum. However, they both appear to be congenital anomalies with bilaterality in one case inherited as an autosomal dominant trait and in another, unilaterality precipitated by an unknown factor. The pathogenic mechanism of this disease can then be readily understood with the progression of time as an invasion of anterior structures by epithelial-like cells which are not contact-inhibited by surrounding normal endothelium.
The clinical significance of this concept relates to the possible replacement of abnormal epithelial-like cells on the posterior corneal surface at an early stage of both diseases to minimise anterior segment spread of these abnormal cells and to inhibit their spread centrally on the cornea by an intact transplanted endothelial layer. The future also offers the potential that medical, radiation, or laser treatment t o residual epithelial-like cells may
prevent the devastating end result of angle involvement.
The acronym Congenital Anterior Segment Epithelialisation or CASE syndrome describes the essential features of the common pathogenic mechanism in these two conditions.
The future requires confirmation of the epithelial-like characteristics of the cells in the ICE syndrome, as has been convincingly displayed already for posterior polymorphous endothelial dystrophy. A continued search is required to identify the factor that determines the asymmetry of involvement in the ICE syndrome. Finally, a reason for metaplasia or abnormal location of epithelial cells on the posterior corneal surface needs to be found.
ACKNOWLEDGEMENTS This study was supported in part by NEI grant EY 02476, EM Core Grant EY 01765, and Computer Core Grant 2P30 EY 01765.
References 1. Shields MB. Progressive essential iris atrophy, Chandler’s
syndrome, and the iris nevus (Cogan-Reese) syndrome. A spectrum of diseases. Surv Ophthalmol 1979; 24: 3.
3 Cibis GW, Krachmer JA. Phelps CD, Weingeist TA. The -.
3 .
4.
5.
6.
7.
8.
9.
10.
11.
clinical spectrum of posterior polymorphois dystrophy. Arch Ophthalmol 1977; 95: 1529. Maumenee AE, Paton D, Morse P H , Butner R. Review of 40 histologically proven cases of epithelial downgrowth following cataract extraction and suggested surgical management. Am J Ophthalmol 1970; 69: 598. Hirst LW, Quigley HA, Stark WJ, Shields MB. Specular microscopy of iridocorneal endothelial syndrome. Am J Ophthalmol 1980; 89: 11 . Hirst LW, Quigley HA, Waring GO, Stark WJ. Specular microscopy of posterior polymorphous endothelial dystrophy. lnvest Ophthalmol Vis Sci 1981; suppl 20. Laing RA, Sandstrom MM, Leibowitz HM. In vivo photomicrography of the corneal endothelium. Arch Ophthalmol 1975; 93: 143. Koester CJ , Roberts CW, Donn A, Hoefle FB. Wide field specular microscopy. Clinical and research applications. Ophthalmology (Rochester) 1980; 87: 849. Hirst LW, Green WR, Luckenbach M, de la Cruz Z, Stark WJ. Epithelial characteristics of the endothelium in Chandler’s syndrome. Invest Ophthalmol Vis Sci (in press). Boruchoff SA, Kuwabara T. Electron microscopy of posterior polymorphous degeneration. Am J Ophthalmol 1971; 72: 879. Rodrigues MM, Sun TT, Krachmer J , Newsome D. EDithekalization of the corneal endothelium in Dosterior pblymorphous dystrophy. Invest Ophthalmoi Vis Sci 1980; 19: 832. Cameron JD, Flaxman BA, Yanoff M: In vitro studies of corneal wound healing: epithelial-endothelial interac- tions. Invest Ophthalmol Vis Sci 1974; 13: 555.
CONGENITAL ANTERIOR SEGMENT EPITHEL.IALISATION (CASE) 213

![Eye anomalies and neurological manifestations in patients with … · 2009. 10. 21. · hypoplasia, congenital cataracts, or anterior segment anomalies [21,22]. There has been no](https://img.pdfslide.net/doc/110x75/602f7fdf0aa91b372a24c40b/eye-anomalies-and-neurological-manifestations-in-patients-with-2009-10-21-hypoplasia.jpg)