Embed Size (px)
Citation preview

Congenital Aortic Stenosis
Echo Conference
January 7, 2008
Anne B. Riley

Outline
Subvalvular
Valvular
Supravalvular
• Morphology• Epidemiology/
Genetics• Clinical Presentation• Associated
syndromes• Treatment options

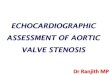
• Caused by an accumulation of fibroelastic tissue
• Thin, crescent shaped membrane just below the aortic valve
• Thick fibromuscular ridge
• Tunnel or tubular: long narrow fibromuscular channel along the LVOT
Subvalvular:Morphology

Imaging
Courtesy: Yale School of Medicine Atlas of Echocardiography
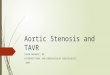
SUBvalvular

SUBvalvularEchocardiogram- PLA

SUBvalvularEchocardiogram- 5 Ch

Epidemiology
• Second most common form of Congenital AS
• More common in males (67-75% of cases)
• Accounts for 8-30% of LVOT obstruction
• Isolated SubAS is felt to be an acquired lesion- not seen in newborns
• Reports published of familial occurrence (? Morphologic abnormalities of LVOT lead to predisposition for cell proliferation)
SUBvalvular

Clinical Presentation
• Lesion often found in children/young adults when evaluating for other cardiac defects
• Presentation in the adult is usually in evaluation of a heart murmur
• Tends to be a progressive lesion • Aortic valve at risk (high velocity jet slams into
aortic valve)• Symptoms depend on degree of obstruction:
fatigue, dyspnea on exertion, chest pain, syncope
• High risk for developing infective endocarditis
SUBvalvular

Clinical Presentation
• Associated with other defects in 60% of cases– Multilevel LVOT obstruction– VSD– Coarctation of the aorta– PDA– Left superior vena cava– Valvular aortic stenosis
SUBvalvular

Shone Syndrome
• Left ventricular inflow and outflow obstruction• Parachute mitral valve (single pap muscle),
supravalvular mitral ring, subaortic stenosis, coarctation
• Treated with surgery often in first year of life• 15-year survival 89%• Deaths secondary to severe mitral valve
disease, need for multiple surgeries
Brown et al. Operative results and outcome in patient with Shone’s anomaly. Ann Thorasic Surgery 2005 April 79(4).
SUBvalvular

Evaluation
• Echocardiography: assess anatomy, measure gradient with continuous wave doppler
• Cardiac cath: further define mechanism and extent of subaortic obstruction (particularly if suspect multiple levels of obstruction)
SUBvalvular

Treatment
• Definitive therapy: Surgical correction• Timing is controversial because of high
recurrence rate (~20%)• Suggested indications in adults
Peak gradient >50 mmHg, mean gradient >30 mmHg
Progressive mod-severe AR, EF <55%, or LVESD 50 mm
Symptomatic from obstruction• Membranectomy +/- myomectomy, Konno-
Rastan procedure (reconstruct LVOT)
SUBvalvular
ACC/AHA 2008 Guidelines for Management of Adults with CHD

Valvular Aortic Stenosis
• Unicuspid, – acommissural – unicommissural
• Bicuspid (most common) • Trileaflet valve
– Miniature– Dysplastic– Fusion of commissures
• Quadricupsid (usually incompetent, rarely stenotic)

Valvular Aortic Stenosis
• 14 year old boy referred for aortic stenosis and regurgitation
• MRI showed …

UnicuspidValvular AS
Diagnosis and Management of Adult Congenital Heart Disease

Case
• 30 year old Guatemalan man with mild shortness of breath on exertion and harsh holosystolic murmur at left sternal border and systolic murmur heard at base
• Echo shows …



Echo showed
• Quadricuspid aortic valve, mild AI, no AS (peak velocity 1.3 m/s)
• Paramembranous VSD
• Large secundum atrial septal defect

Bicuspid Valve Morphology• Right-Left Commissures
– Gives anterior and posterior cusps
– RCA and LMCA both from anterior cusp
– False raphe also on anterior cusp
• Anterior-Posterior Commissures– Gives left and right cusps– RCA from right cusp and
LMCA from left cusp– Often have a false raphe, on
right cusp
Valvular AS
Right-Left Commissures
Courtesy: Yale University School of Medicine Atlas of echocardiography
N
R L

BicuspidValvular AS

Valvular AS

Valvular AS

Epidemiology
• Bicuspid valve accounts for 95% of cases of congenital AS, occurs in 1-2% of general population
• More common in males (3:1)
• Case reports of familial inheritance of bicuspid valves, tends to be autosomal dominant with variable penetrance
Valvular AS

Clinical Presentation
Initially asymptomatic
Valvular AS
Restricted motion
Turbulent flow
Abnormal folding
Scarring, calcification, stenosis, regurgitation
-66% develop aortic stenosis
-Only 15% of patients have a normally functioning valve in the 5th decade

Bicuspids and the Aorta
• Often have abnormalities of the aortic media
• Increased risk for dilatation, dissection (5-9x) and rupture of ascending aorta
• Previously thought to be secondary to “poststenotic turbulence”
• Abnormalities of ascending aorta occur irrespective of degree of stenosis or regurgitation
Valvular AS

Monitoring and Treatment• Dilated aortic root (>4 cm): yearly imaging of aorta (echo,
CT?, MRI?)• Recent data to suggest that ARBs slow the rate of
progression of aortic root dilatation in Marfan’s patients
Brooke et al. Angiotensin II Blockade and Aortic root dilation in Marfan’s Syndrome. NEJM 2008
Valvular AS

Intervention
• Valve replacement surgery indicated for patients with severe stenosis who are symptomatic or are developing LV dysfunction (EF<50%) or LV dilatation
• Consider surgery who have moderate stenosis with moderate AR or dilated ascending aorta
• Repair/replacement of the ascending aorta when 5 cm or expanding at a rate >5 mm/yr
Valvular AS

Supravalvular Aortic Stenosis
• Least common lesion of the LVOT
Courtesy: Yale University School of Medicine Atlas of Echocardiography
Hourglass
vs
Diffuse narrowing

Associated Abnormalities
• Aortic valve leaflets: thickened, redundant, bicuspid
• Coronary artery stenosis
• Coarctation of the aorta or stenoses of carotid, renal, iliac
• Pulmonary artery stenoses
SupraValvular

Classification
• Williams syndrome
• Autosomal dominant form without features of Williams syndrome
• Sporadic
SupraValvular

Williams syndrome
• Affects 1/10,000 individuals• Supravalvular AS (70%)• Mental retardation • Elfin facies• Cocktail personality• Renovascular hypertension • Stellate iris • MRI
Mechanisms and treatment of cardiovascular disease in Williams-Beuren syndrome
SupraValvular

Genetics and Pathology
• Mutation in or deletion of the elastin gene located on chromosome 7q11.23
• Aortic Media is affected:– a reduction of elastic tissue with disorganized
elastin fibers– Decreased elasticity, increased shear stress->
smooth muscle hypertrophy and collagen deposition
SupraValvular

Therapy: Surgery
• Surgical enlargement of sinotubular area and ascending aorta
• Recommended with symptoms (angina, dyspnea, syncope) or mean pressure gradient of >50mmHg, or peak >70 mmHg
• Excision and end-end anastamosis
• Patch enlargement of sinotubular junction

Thank you

Special thanks to
Eli (for suggesting this topic) and
Anne Marie Valente of the BACH program

ReferencesAboulhosn et al. Left Ventricular Outflow Obstruction: Subaortic Stenosis,
Bicuspid Aortic Valve, Supravalvuar Aortic Stenosis, and Coarctation of the Aorta. Circulation 2006:114, 2412-2422.
Brooke et al. Angiotensin II Blockade and Aortic root dilation in Marfan’s Syndrome. NEJM 2008.
Brown et al. Operative results and outcome in patient with Shone’s anomaly. Ann Thorasic Surgery 2005 April 79(4).
Holt et al. Quadricuspid Aortic Valve with Aortic Insufficiency: case report and review of the literature. J Card Surg 2007: 22, 224-239.
Pober et al. Mechanisms and Treatment of Cardiovascular Disease in Williams-Beuren syndrome. J of Clin Investigation: 2008:5, 1606-1615.
ACC/AHA 2008 Guidelines for Management of Adults with Congenital Heart Disease.
Diagnosis and Management of Adult Congenital Heart Disease. Gazoulis. 2003, Elsevier Limited.
The Clinical Recognition of Congenital Heart Disease. Perloff. 1987, WB Saunders.
Yale School of Medicine Atlas of Echocardiography