Embed Size (px)
Citation preview
Surg Today (2000) 30:268–271
Congenital Hepatoportal Arteriovenous Fistula: Report of a Case
Sandeep Agarwala1, Hemonta Dutta1, Veereshwar Bhatnagar1, Manpreet Gulathi2, Sashi Paul2,and DilipKumar Mitra1
Departments of 1 Paediatric Surgery and 2 Radiodiagnosis, All India Institute of Medical Sciences, New Delhi 110029, India
case of an infant with HPAVF, who was successfullytreated by percutaneous transcatheter embolization ofthe right feeding hepatic artery, and present a review ofthe relevant literature.
Case Report
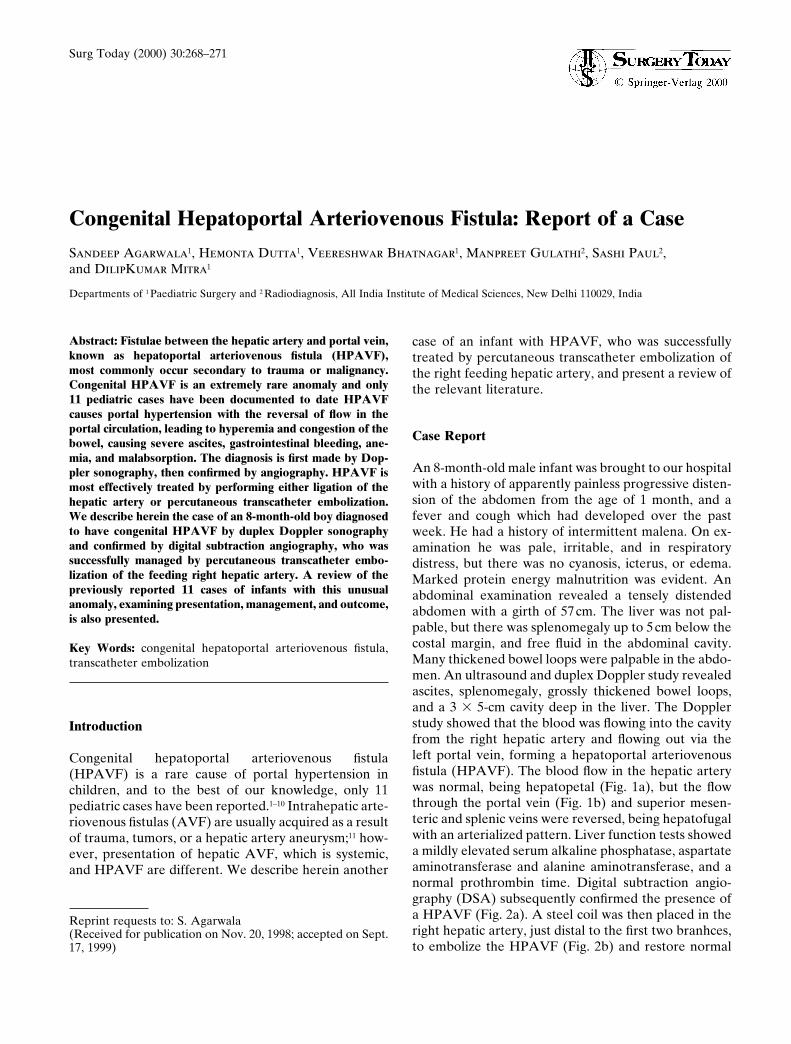
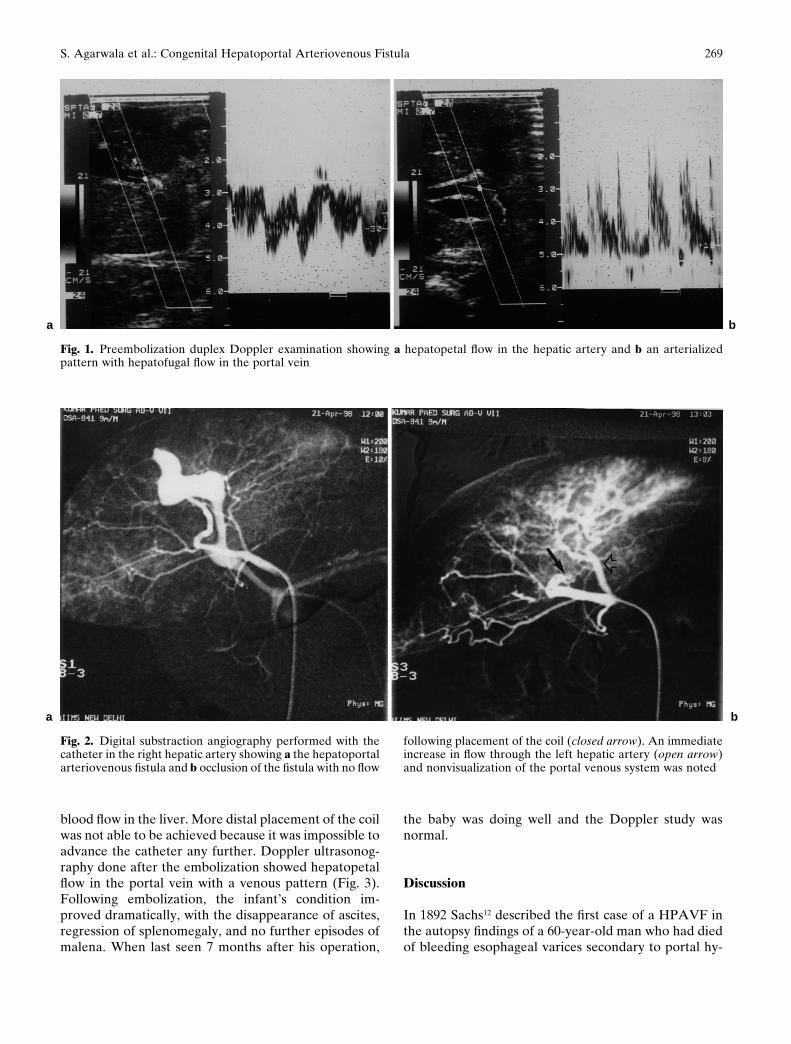
An 8-month-old male infant was brought to our hospitalwith a history of apparently painless progressive disten-sion of the abdomen from the age of 1 month, and afever and cough which had developed over the pastweek. He had a history of intermittent malena. On ex-amination he was pale, irritable, and in respiratorydistress, but there was no cyanosis, icterus, or edema.Marked protein energy malnutrition was evident. Anabdominal examination revealed a tensely distendedabdomen with a girth of 57cm. The liver was not pal-pable, but there was splenomegaly up to 5cm below thecostal margin, and free fluid in the abdominal cavity.Many thickened bowel loops were palpable in the abdo-men. An ultrasound and duplex Doppler study revealedascites, splenomegaly, grossly thickened bowel loops,and a 3 3 5-cm cavity deep in the liver. The Dopplerstudy showed that the blood was flowing into the cavityfrom the right hepatic artery and flowing out via theleft portal vein, forming a hepatoportal arteriovenousfistula (HPAVF). The blood flow in the hepatic arterywas normal, being hepatopetal (Fig. 1a), but the flowthrough the portal vein (Fig. 1b) and superior mesen-teric and splenic veins were reversed, being hepatofugalwith an arterialized pattern. Liver function tests showeda mildly elevated serum alkaline phosphatase, aspartateaminotransferase and alanine aminotransferase, and anormal prothrombin time. Digital subtraction angio-graphy (DSA) subsequently confirmed the presence ofa HPAVF (Fig. 2a). A steel coil was then placed in theright hepatic artery, just distal to the first two branhces,to embolize the HPAVF (Fig. 2b) and restore normal
Abstract: Fistulae between the hepatic artery and portal vein,known as hepatoportal arteriovenous fistula (HPAVF),most commonly occur secondary to trauma or malignancy.Congenital HPAVF is an extremely rare anomaly and only11 pediatric cases have been documented to date HPAVFcauses portal hypertension with the reversal of flow in theportal circulation, leading to hyperemia and congestion of thebowel, causing severe ascites, gastrointestinal bleeding, ane-mia, and malabsorption. The diagnosis is first made by Dop-pler sonography, then confirmed by angiography. HPAVF ismost effectively treated by performing either ligation of thehepatic artery or percutaneous transcatheter embolization.We describe herein the case of an 8-month-old boy diagnosedto have congenital HPAVF by duplex Doppler sonographyand confirmed by digital subtraction angiography, who wassuccessfully managed by percutaneous transcatheter embo-lization of the feeding right hepatic artery. A review of thepreviously reported 11 cases of infants with this unusualanomaly, examining presentation, management, and outcome,is also presented.
Key Words: congenital hepatoportal arteriovenous fistula,transcatheter embolization
Introduction
Congenital hepatoportal arteriovenous fistula(HPAVF) is a rare cause of portal hypertension inchildren, and to the best of our knowledge, only 11pediatric cases have been reported.1–10 Intrahepatic arte-riovenous fistulas (AVF) are usually acquired as a resultof trauma, tumors, or a hepatic artery aneurysm;11 how-ever, presentation of hepatic AVF, which is systemic,and HPAVF are different. We describe herein another
Reprint requests to: S. Agarwala(Received for publication on Nov. 20, 1998; accepted on Sept.17, 1999)
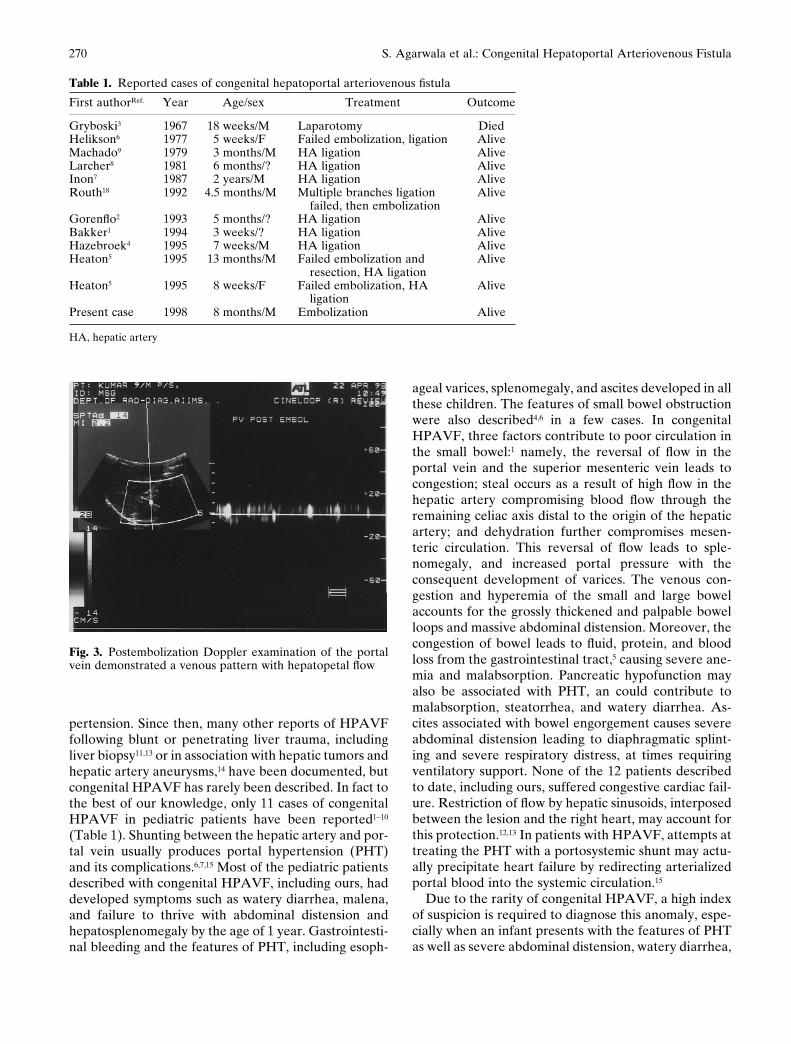
blood flow in the liver. More distal placement of the coilwas not able to be achieved because it was impossible toadvance the catheter any further. Doppler ultrasonog-raphy done after the embolization showed hepatopetalflow in the portal vein with a venous pattern (Fig. 3).Following embolization, the infant’s condition im-proved dramatically, with the disappearance of ascites,regression of splenomegaly, and no further episodes ofmalena. When last seen 7 months after his operation,
the baby was doing well and the Doppler study wasnormal.
Discussion
In 1892 Sachs12 described the first case of a HPAVF inthe autopsy findings of a 60-year-old man who had diedof bleeding esophageal varices secondary to portal hy-
Fig. 1. Preembolization duplex Doppler examination showing a hepatopetal flow in the hepatic artery and b an arterializedpattern with hepatofugal flow in the portal vein
a b
Fig. 2. Digital substraction angiography performed with thecatheter in the right hepatic artery showing a the hepatoportalarteriovenous fistula and b occlusion of the fistula with no flow
following placement of the coil (closed arrow). An immediateincrease in flow through the left hepatic artery (open arrow)and nonvisualization of the portal venous system was noted
a b
269S. Agarwala et al.: Congenital Hepatoportal Arteriovenous Fistula
pertension. Since then, many other reports of HPAVFfollowing blunt or penetrating liver trauma, includingliver biopsy11,13 or in association with hepatic tumors andhepatic artery aneurysms,14 have been documented, butcongenital HPAVF has rarely been described. In fact tothe best of our knowledge, only 11 cases of congenitalHPAVF in pediatric patients have been reported1–10
(Table 1). Shunting between the hepatic artery and por-tal vein usually produces portal hypertension (PHT)and its complications.6,7,15 Most of the pediatric patientsdescribed with congenital HPAVF, including ours, haddeveloped symptoms such as watery diarrhea, malena,and failure to thrive with abdominal distension andhepatosplenomegaly by the age of 1 year. Gastrointesti-nal bleeding and the features of PHT, including esoph-
ageal varices, splenomegaly, and ascites developed in allthese children. The features of small bowel obstructionwere also described4,6 in a few cases. In congenitalHPAVF, three factors contribute to poor circulation inthe small bowel:1 namely, the reversal of flow in theportal vein and the superior mesenteric vein leads tocongestion; steal occurs as a result of high flow in thehepatic artery compromising blood flow through theremaining celiac axis distal to the origin of the hepaticartery; and dehydration further compromises mesen-teric circulation. This reversal of flow leads to sple-nomegaly, and increased portal pressure with theconsequent development of varices. The venous con-gestion and hyperemia of the small and large bowelaccounts for the grossly thickened and palpable bowelloops and massive abdominal distension. Moreover, thecongestion of bowel leads to fluid, protein, and bloodloss from the gastrointestinal tract,5 causing severe ane-mia and malabsorption. Pancreatic hypofunction mayalso be associated with PHT, an could contribute tomalabsorption, steatorrhea, and watery diarrhea. As-cites associated with bowel engorgement causes severeabdominal distension leading to diaphragmatic splint-ing and severe respiratory distress, at times requiringventilatory support. None of the 12 patients describedto date, including ours, suffered congestive cardiac fail-ure. Restriction of flow by hepatic sinusoids, interposedbetween the lesion and the right heart, may account forthis protection.12,13 In patients with HPAVF, attempts attreating the PHT with a portosystemic shunt may actu-ally precipitate heart failure by redirecting arterializedportal blood into the systemic circulation.15
Due to the rarity of congenital HPAVF, a high indexof suspicion is required to diagnose this anomaly, espe-cially when an infant presents with the features of PHTas well as severe abdominal distension, watery diarrhea,
Fig. 3. Postembolization Doppler examination of the portalvein demonstrated a venous pattern with hepatopetal flow
Table 1. Reported cases of congenital hepatoportal arteriovenous fistula
First authorRef. Year Age/sex Treatment Outcome
Gryboski3 1967 18 weeks/M Laparotomy DiedHelikson6 1977 5 weeks/F Failed embolization, ligation AliveMachado9 1979 3 months/M HA ligation AliveLarcher8 1981 6 months/? HA ligation AliveInon7 1987 2 years/M HA ligation AliveRouth18 1992 4.5 months/M Multiple branches ligation Alive
failed, then embolizationGorenflo2 1993 5 months/? HA ligation AliveBakker1 1994 3 weeks/? HA ligation AliveHazebroek4 1995 7 weeks/M HA ligation AliveHeaton5 1995 13 months/M Failed embolization and Alive
resection, HA ligationHeaton5 1995 8 weeks/F Failed embolization, HA Alive
ligationPresent case 1998 8 months/M Embolization Alive
HA, hepatic artery
270 S. Agarwala et al.: Congenital Hepatoportal Arteriovenous Fistula

and malnutrition. Careful sonographic examinationduring the PHT workup may indicate the presence ofHPAVF, and this can be confirmed by duplex Dopplersonography or color-coded sonography which are themodalities of choice to evaluate flow direction and pat-terns of hepatic shunts and the portal vein.1 Arteriogra-phy plays an important role in defining the anomalousblood supply and predicting the embolization or hepaticartery ligation.1,16
Various methods of treatment of congenital HPAVFhave been attempted, but due to its rarity, none havebeen able to be evaluated properly. Surgical resection,hepatic artery embolization, and hepatic artery ligationhave all been said to be important tools in the manage-ment of this condition. Ligation of the hepatic arteryproved successful in most of the reported cases,1,2,4,6–9,17
while hepatic artery embolization using a variety ofmaterials is also possible. The first cases of successfulpercutaneous transcatheter embolization for congenitalHPAVF, achieved with a coil, was reported by Routhet al.18 in 1992. We successfully treated congenitalHPAVF in our patient by occluding the feeding vesselwith transcatheter placement of a coil and establishingnormal hepatopetal blood flow through the portal vein.
References
1. Bakker J, Robben SG, Hazebroek FW, Meradji M (1994) Con-genital arterioportal fistula of the liver with reversal of flow in thesuperior mesenteric vein. Pediatr Radiol 24:198–199
2. Gorenflo M, Waldschmidt J, Bein G, Flocken W, Vogel M (1993)Arterioportal fistula in infancy. J Pediatr Gastroenterol Nutr16:87–89
3. Gryboski JD, Clemett A (1967) Congenital hepatic artery aneu-rysm with superior mesenteric artery insufficiency: a steal syn-drome. Pediatrics 39:344–347
4. Hazebroek FWJ, Tibboel D, Robben SGF, Bergmeyer JHLH,Molenaar JC (1995) Hepatic artery ligation for hepatic vasculartumors with arteriovenous and arterioporto-venous shunts in thenewborn: successful management of two cases and review ofliterature. J Pediatr Surg 30:1127–1130
5. Heaton ND, Davenport M, Karani J, Mowat AP, Howard ER(1995) Congenital hepatoportal arteriovenous fistula. Surgery117:170–174
6. Helikson MA, Shapiro DL, Seashore JH (1977) Hepatoportalarteriovenous fistula and portal hypertension in an infant. Pediat-rics 60:921–924
7. Inon AE, D’Agostina D (1987) Portal hypertension secondary tocongenital arterioportal fistula. J Pediatr Gastroenterol Nutr6:471–473
8. Larcher VF, Howard ER, Mowat AP (1981) Hepatic heman-giomata: diagnosis and management. Arch Dis Child 56:7–14
9. Machado MCC, de Cunha JEM, Bachella T, Lima SS, ToporovskiJ (1979) Fistula arterio-venosa intrahepatica congenita acom-panhada de hipertensao portal e sangramento digestivo. RevHosp Clin Fac Med Sao Paulo 37:285–288
10. Mays ET, Conti S, Fallahzadeh H, Rosenblatt M (1979) Hepaticartery ligation. Surgery 86:536–541
11. Vanway CW, Crane JM, Riddell JH, Foster JH (1971) Arterio-venous fistula in portal circulation. Surgery 70:876–890
12. Sachs R (1892) Zur casuistik der gefasserkrankungen. Dtsch MedWochenschr 18:443–447
13. Foley WJ, Turcotte JG, Hoskins PA, Brant RL, Ause RG (1971)Intrahepatic arteriovenous fistula between the hepatic artery andthe portal vein. Ann Surg 174:849–855
14. Foster JH, Sandbolm P (1961) Portal hypertension secondary to ahepato-portal aretriovenous fistula. Ann Surg 154:300–304
15. Ramchandani P, Goldenberg NJ, Sonlen RL, White RI Jr (1983)Isobutyl 2-cyanoacrylate embolization of a hepatoportal fistula.Am J Roentgenol 140:137–140
16. Luks FI, Yazbeck S, Brandt ML, Bensoussan AL, Brochu P,Blanchard H (1991) Benign liver tumors in children: a 25 yearsexperience. J Pediatr Surg 26:1326–1330
17. Howard ER, Heaton ND (1991) Hemangiomas. In: Howard ER(ed) Surgery of liver disease in children. Butterworth Heinemann,Oxford, pp 115–125
18. Routh WD, Keller FS, Caine WS, Royal SA (1992) Transcatheterembolization of a high flow congenital intrahepatic arterial-portalvenous malformation in an infant. J Pediatr Surg 27:511–514
271S. Agarwala et al.: Congenital Hepatoportal Arteriovenous Fistula





























