Embed Size (px)
Citation preview

Correspondence
Ljubljana classification of epithelialhyperplastic laryngeal lesions
Sir: We have recently presented a detailed description ofthe criteria that can be used for the grading of laryngealepithelial hyperplastic lesions in the Ljubljana classifi-cation.1 In his Commentary, published in the same issueof Histopathology, Helliwell has usefully discussed thehistopathological guidelines given by the Ljubljanaclassification.2 We agree with Helliwell’s stipulationthat further evaluation of this system in histopatho-logical practice is required. His analysis has, however,indicated a need for us to clarify the basis of thedistinction that the new classification proposes between‘atypical’ (risky) hyperplasia and carcinoma in situ.
The object of a classification of laryngeal intraepithe-lial lesions is to give the pathologist the means ofrecording for any particular lesion the most accurateassessment possible of the biopsy findings. Helliwell is atvariance with the criteria that we have presented forcarcinoma in situ as part of the Ljubljana classification.In summary, these are that ‘the epithelium shows thefeatures of carcinoma without invasion’. We agree withHelliwell that there is a great deal of variation of thedegree of atypia seen in invasive carcinoma, but do notaccept that this is an argument against the specificationof some intraepithelial lesions as carcinoma. Surface anddeeper regions of invasive laryngeal carcinoma mayshow cellular abnormalities ranging from those of mildbasal cell hyperplasia through moderate atypia to thoseof severe nuclear change. In those invasive tumourswith lesser degrees of atypical change the diagnosis ofinvasive squamous carcinoma may be based only on thepresence of infiltration. In contrast, carcinoma cannotbe diagnosed in a purely intraepithelial lesion showingthese milder features only. As Helliwell himself pointsout, even the use of molecular markers or DNAcytometry would, at present, be of little use for anaccurate specification that the final change to carcin-oma has been reached. The criteria that we suggested inour article for the Ljubljana grade of carcinoma in situare those of the extreme situation in which thecarcinomatous nature of the cells cannot be in doubt.We have found this to be very unusual in laryngealhyperplastic lesions, and would classify the majority ofsuch lesions with severe atypia by the lesser designationin the new classification of atypical (‘risky’) hyperplasia.In the few cases in which the grade of carcinoma in situcan be confidently allocated, the patient would benefitby receiving more radical treatment at once. Moreover,in such cases the search for possible foci of invasive
carcinoma which Helliwell mentions would be inten-sified. Thus, by separating out cases of undoubtedintraepithelial carcinoma, the Ljubljana classificationoffers a further improvement in the accuracy ofassessment of epithelial hyperplastic lesions of thelarynx additional to that provided by the distinction ofabnormal from atypical (‘risky’) hyperplasia.
L Michaels
Department of Histopathology,Royal Free and University College,
Medical School,University College London,
London, UK
On behalf of H Hellquist (Bergen, Norway), A Cardesa(Barcelona, Spain) N Gale (Ljubljana, Slovenia) andV Kambic (Ljubljana, Slovenia).
1. Hellquist H, Cardesa A, Gale N, Kambic V, Michaels L. Criteria forgrading in the Ljubljana classification of epithelial hyperplasticlaryngeal lesions. A study by members of the Working Group onEpithelial Hyperplastic Lesions of the European Society ofPathology. Histopathology 1999; 34; 226–223.
2. Helliwell TR. ‘Risky’ epithelium of the larynx—a practicaldiagnosis? Histopathology 1999; 34; 262–265.
Pseudotuberculous pyelonephritis: a rareentity and a diagnostic pitfall
Sir: Recent correspondence described an unusual formof chronic pyelonephritis with nephrolithiasis mimick-ing tuberculosis.1 We describe the features of two morecases of this rare form of chronic pyelonephritis. Thepotential diagnostic pitfall with this apparently infec-tious condition is highlighted by its occurrence in twopatients in the same hospital at the same time.
The first patient was a 30-year-old woman admittedfor bilateral native nephrectomy and cadaveric renaltransplant. Bilateral nephrolithiasis had been diagnosedin infancy and renal transplantation had first beenperformed at the age of 12 years. Graft failure occurred13 years later and continual ambulatory peritonealdialysis (CAPD) was commenced. Repeat cadaverictransplantation was performed 2 years later but wascomplicated by vascular thrombosis 4 days postopera-tively and the transplanted kidney was removed.Histological examination showed infarction and CAPDwas recommenced. Since the second transplant thepatient had two episodes of peritonitis, the most recent of
Histopathology 1999, 35, 181–191
q 1999 Blackwell Science Limited.

which occurred 10 weeks prior to admission for surgery.Escherichia coli was cultured. Sinus tract formation hadcomplicated previous nephrolithotomy. This tract haddischarged pus approximately 2 months prior to thisadmission. Pseudomonas was cultured at this time. Thetract was dry in the weeks prior to admission. Repeatedcultures for Mycobacterium tuberculosis were negative.Bilateral native nephrectomy was successfully per-formed and the patient had an uneventful postoperativerecovery.
The second patient was a 50-year-old womanadmitted for surgical exploration of her left kidney andpossible left nephrectomy. She first presented 18 monthsearlier with a 10-day history of left flank pain. She hadno previous history of pyelonephritis. Investigationsshowed a pyuria with a mixed growth. An intravenousurogram (IVU) showed bilateral duplex collectingsystems and multiple perirenal opacities of calcificdensity, with scarring and dilatation of the upper polecalyces. A CT scan of the left kidney showed a perirenalabscess, which was then drained at surgery. A stone wasalso removed from the left kidney at this time. Culture ofthe abscess contents grew no organisms. The patientpresented again with further left flank pain. Repeat IVUshowed no evidence of hydronephrosis but persistentrenal and extrarenal calculi. Extracorporeal shockwavelithotripsy (ESWL) was performed twice but her flankpain persisted. Exploration of her left kidney found ascarred kidney with cortical loss, particularly in thelower pole. A left nephrectomy was performed. Herpostoperative recovery was uncomplicated.
In the first case, the right and left nephrectomyspecimens measured 120 × 70 × 60 mm and 115 ×70 × 30 mm and weighed 287.5 g and 107 g, respec-tively. There was bilateral calyceal dilatation with corticalthinning, and calculi were present in the pelvicalycealsystems of both kidneys. Histologically, the right and leftkidneys showed similar features. There was focalsquamous metaplasia of the pelvic urothelium. Noremaining normal renal parenchyma was identified.There was extensive and severe chronic pyelonephritiswith histological changes of end stage kidneys. Withinboth kidneys there were poorly formed granulomas withcentral necrosis surrounded by histiocytes (Figure 1).There were giant cells, some of which containedcalcified material.
In the second case the nephrectomy specimenmeasured 100 × 50 × 25 mm and weighed 165 g. Theexternal surface of the kidney was nodular andscarred. Cutting revealed dilatation of the renal pelvis,which was surrounded by necrotic material. Histo-logical examination confirmed the presence of exten-sive peripelvic necrosis, which was surrounded by
histiocytes, giant cells and loosely formed granulomaswith some surrounding lymphocytes. Immediately adja-cent to the area of necrosis was evidence of chronicpyelonephritis with thick walled vessels, sclerosedglomeruli, hyaline casts within the tubules and chronicinflammation within the interstitial tissue. The renalparenchyma distant from this area was unremarkable.
Special stains for microorganisms, including fungalstains and ZN stain for mycobacteria, were negative inboth cases. There was no evidence of Michaelis–Guttmanbodies.
Despite relatively dissimilar histories, the two patientsdescribed above had remarkably similar renal histolo-gical findings. The predominant features in each casewere those of nephrolithiasis, chronic pyelonephritisand necrotizing granulomatous inflammation. Thesetwo patients had surgery performed within 2 days of oneanother in the same hospital. The first patient describedhad a bilateral native nephrectomy and the second aunilateral nephrectomy. All three kidneys showedsimilar histological findings with granulomatousinflammation suggestive of tuberculous infection.Their proximity in time further increased the degree ofsuspicion of an infective aetiology. However, in neithercase were there clinical features or microbiologicalevidence to support such a diagnosis. A number ofalternative diagnoses—considered and subsequentlyrejected in each case—included xanthogranulomatouspyelonephritis (no xanthoma cells), malakoplakia (noMichaelis–Guttman bodies) and renal sarcoidosis(rarely causes necrotizing granulomas) as well asother infectious agents particularly fungi (negativespecial stains). Thus following exclusion of otherpossible diagnoses, the diagnosis of pseudotuberculouspyelonephritis associated with nephrolithiasis was madein each case. This is an unusual entity.
182 Correspondence
q 1999 Blackwell Science Ltd, Histopathology, 35, 181–191.
Figure 1. The edge of a granuloma showing necrosis (arrowhead)rimmed by histiocytes (H & E × 400).

The aetiology of this form of granulomatous pyelone-phritis is, as yet, unknown. It has been suggested that itspathogenesis is related to the presence of calciumoxalate crystals, which may be dispersed by lithotripsy(ESWL).1 In the cases described above, calcification wasnoted within granulomas in the kidneys and this featurehas been emphasized by several authors previously.1,2
Lithotripsy had been performed on two occasions in thesecond case. The first patient had not had lithotripsy atany time. Other suggested aetiological factors includeurinary tract infection and hydronephrosis.2 There is adefinite history of the former in the second casedescribed and it does seem quite feasible that the firstpatient may have had clinically silent episodes ofurinary tract infection at some stage. Evidence ofhydronephrosis was seen at gross examination of thenephrectomy specimens in each case. Thus, while theexact cause of the granulomatous inflammation inthese two cases remains unclear, it does seem reason-able to associate it with the presence of nephrolithiasis,taken in conjunction with the cases described by otherspreviously.1–4
While the diagnosis of granulomatous pyelonephritis(or ‘pseudotuberculous pyelonephritis’) associated withnephrolithiasis may appear little more than a curiosity,it is worth considering the possible value in itsrecognition. It avoids the necessity of treating a patient,who is often immunosuppressed and on numerousother medications, with antituberculous therapy, whichhas its own potential side-effects. Of course one mustalso be aware of the danger of mistaking a true case ofrenal tuberculous infection for this pseudotuberculousentity. The diagnostic difficulty involved is illustrated bythe cases described above, which occurred in twopatients in the same hospital at the same time andfurther highlights the need for clinicopathologicalcorrelation in such instances.
C MuldoonD Hickey1
D Murphy1
E Kay
Departments of Histopathology and 1Urology,Beaumont Hospital,
Dublin, Ireland
1. Bouzourene H, Bouzourene N, Francke M. An unusual granulo-matous form of chronic pyelonephritis mimicking tuberculosis.Histopathology 1998; 32; 481–482.
2. Hoorens A, Van der Niepen P, Keuppens F, Vanden Houte K, KloppelG. Pseudotuberculous pyelonephritis associated with nephrolithia-sis. Am. J. Surg. Pathol. 1992; 16; 522–525.
3. Valerdis Cassola S, Parra Muntaner L, Garcia Alonso J. Pseudo-tuberculous pyelonephritis. Archivos Espanoles de Urologica 1994;47; 172–174.
4. Mohammed SH, Vyas H. Chronic granulomatous disease with renalstones. Pediatr. Radiol. 1992; 22; 596–597.
Mammary fibroadenoma in a male-to-femaletranssexual
Sir: Idiopathic male fibroadenoma is considered anextremely rare event and only very few cases ofiatrogenic male fibroadenoma are to be found in theliterature.1–3 As Holleb et al.4 did not observe any caseof malignant phyllodes tumours in their series of 198male breast cancers, they even concluded that thereis no true fibroadenoma of the male breast. Afterreviewing several cases of alleged fibroadenoma of themale breast in retrospect, it was concluded that manyof the reported lesions were poorly documented orappeared to have been nodular foci of gynaecomastia.1
Nielsen5 reported an unusual 160 mm fibroadenoma-toid tumour that arose in one breast of a 69-year-oldman with bilateral gynaecomastia. Breast enlargementand the appearance of the unilateral tumour beganafter spironolactone was added to his digoxin andfurosemide medications, suggesting that the latter drugcontributed to the induction of the mammary lesion.Gynaecomastia has been associated with digitalis andspironolactone interferes with the production of testos-terone and its conversion to the potent metabolite 5a-dihydrotestosterone.6 Four additional cases of malefibroadenomas have been reported by the ArmedForces Institute of Pathology.2 Gynaecomastia withlobular differentiation was present microscopically ineach case. One of the four patients had been treatedwith oestrogens whereas another had been treated withmethyldopa and chlordiazepoxide. The genetic differ-ences in oestrogen sensitivity to dopaminergic regula-tion of prolactin secretion has been reported and is likelyto play a role in the latter case.7 Possible causes offibroadenoma formation in the other two patientsremain unkown and together with the case reportedby Uchida et al.8 these may well be the only cases of malefibroadenoma not induced by drugs. We describe whatappears to be the first case of fibroadenoma in the breastof a hormonally treated male-to-female transsexual.
At age 22, the patient underwent orchidectomy,vaginoplasty, and augmentation mammoplasty else-where. Since then she had been prescribed cyproteroneacetate 1 × 50 mg/day and ethinyl oestradiol 2 × 50 mg/day.6 Nineteen years later, at age 41, she presented witha 15 × 15 mm mass in the medial upper quadrant of theright breast (Figure 1). A firm but smooth tumour was
Correspondence 183
q 1999 Blackwell Science Ltd, Histopathology, 35, 181–191.

resected. Four-micrometre thick haematoxylin andeosin stained slides showed the tumour to consist of afibroadenoma of the pericanalicular type (Figure 2).
Most male-to-female transsexuals seek demasculiniza-tion and feminization through hormonal and surgicaltreatment. For this, they are chemically and, subse-quently, surgically castrated and exposed to life-longoestrogen administration.6,9 The slight increase ofplasma oestrogen-to-androgen ratio observed in idio-pathic prepubertal or senile gynaecomastia usually willnot induce acinar and lobular formation in the malebreast,10,11 but full acini and lobular formation willoccur in transsexuals in whom progestagenic antiandro-gens are combined with feminizing oestrogen therapy.12
Cyproterone acetate is such a progestagenic with astrong androgen receptor-blocking effect. In our patient,
it was continued even after orchidectomy to reduceunfavourable hair growth. Ethinyloestradiol is a potentoestrogenic chemical modification of 17b-oestradiol,the latter being the main oestrogen of the body. Thecombination of ethinyloestradiol and cyproterone acetateresults in maximal suppression of serum testosteronelevels and blocking of the androgen receptor.6 As a result,the histology of the male breast becomes indistiguishablefrom the natural histology of the genetically femalebreast.13 Fibroadenoma is a common finding in thegenetic female and, hence, it may be expected to occur inthe feminized mammary tissue of hormonally treatedmale-to-female transsexuals. This case proves that itdoes.
R C J KanhaiJ J Hage
E Bloemena1
P J van Diest1
R B Karim
Departments of Plastic Surgery and 1Pathology,Academisch Ziekenhuis Vrije Universiteit,
Amsterdam, The Netherlands
1. Rosen PP. Benign proliferative lesions of the male breast. In: RosenPP, ed. Rosen’s Breast Pathology. Philadelphia: Lippincott-Raven,1997; 609–617.
2. Ansah-Boateng Y, Tavassoli FA. Fibroadenoma and cystosarcomaphyllodes of the male breast. Mod. Pathol. 1992; 5; 114–116.
3. Bartoli C, Zurrida SM, Clemente C. Phyllodes tumor in a malepatient with bilateral gynaecomastia induced by oestrogentherapy for prostatic carcinoma. Eur. J. Surg. Oncol. 1991; 17;215–217.
4. Holleb AI, Freeman HP, Farrow HJ. Cancer of male breast, part II.N. Y. State J. Med. 1968; 68; 656–663.
5. Nielsen BB. Fibroadenomatoid hyperplasia of the male breast. Am.J. Surg. Pathol. 1990; 14; 774–777.
6. Asscheman H, Gooren LJG. Hormone treatment in transsexuals.J. Psychol. Human Sexual. 1992; 5; 39–54.
7. Asscheman H, Gooren LJG, Assies J, Smits JPH, de Slegte R.Prolactin levels and pituitary enlargement in hormone-treatedmale-to-female transsexuals. Clin. Endocrinol. 1988; 28; 538–588.
8. Uchida T, Ishii M, Motomiya Y. Fibroadenoma associated withgynaecomastia in an adult man—case report. Scand. J. Plast.Reconstr. Hand Surg. 1993; 27; 327–329.
9. van Kesteren PJM, Asscheman H, Megens JAJ, Gooren LJG.Mortality and morbidity in transsexual subjects treated withcross-sex hormones. Clin. Endocrinol. 1997; 47; 337–342.
10. Nuttall FQ. Gynecomastia as a physical finding in normal men.J. Clin. Endocrinol. Metab. 1979; 48; 338–340.
11. Ribeiro GG, Phillips HV, Skinner LG. Serum oestradiol-17b,testosterone, luteinizing hormone, and follicle-stimulating hor-mone in males with breast cancer. Br. J. Cancer 1980; 41; 474–477.
12. Kanhai RCJ, Hage JJ, van Diest PJ, Bloemena E, Mulder JW. Short-term and long-term histologic effects of castration and estrogen
184 Correspondence
q 1999 Blackwell Science Ltd, Histopathology, 35, 181–191.
Figure 1. Preoperative mammography of the patient’s right breast. A15 × 15 mm mass was noted in the medial upper quadrant (arrows).This firm but smooth tumour was surgically removed.
Figure 2. Microscopic appearance of fibroadenoma. The tumour issurrounded by a thin fibrous capsule and consists of tubules com-posed of low columnar cells and stroma composed of loose connec-tive tissue. Normal breast tissue (top) shows small lobules (H & Estain; original magnification × 40).

treatment on breast tissue of 14 male-to-female transsexuals incomparison with chemically castrated males. Am. J. Surg. Pathol.submitted for publication.
13. McCarty KS Jr, Tucker JA. Breast. In: Sternberg SS, eds. Histologyfor Pathologists. New York, NY: Raven Press, 1992; 893–902.
Congenital lipoid adrenal hyperplasia
Sir: Congenital lipoid adrenal hyperplasia (lipoid CAH) isthe most severe and rare form of congenital adrenalhyperplasia.1 We present the clinical and histopatho-logical findings of a neonate with this disorder.
The patient was the first child of consanguinousparents. At 17 days of age, she was referred to ourhospital because of vomiting, weakness and oliguria forfive days. On physical examination she was tachypnoeic,severely dehydrated and had normal female externalgenitalia without hyperpigmentation. The laboratorydata were: serum Na, 135 meq/l; K, 12.7 meq/l; Cl,91 meq/l; Ca, 9.9 mg/dl; P, 15.4 mg/dl; blood ureanitrogen, 119 mg/dl; creatinine, 4.6 mg/dl and glucose,42 mg/dl. She was hospitalized with the initial diagnosesof renal failure and septicaemia. Abdominal ultrasono-graphy was normal. She died on the first day ofhospitalization. The parents refused a complete autopsyand only incisional post-mortem samples of kidney, liver,spleen and adrenal were examined.
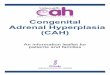
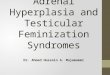
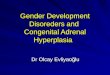
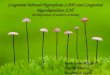
The main pathology was in the adrenal tissue. It wasyellowish-white in colour, firm and lobular. Microscopicexamination revealed a lobulated hyperplastic adrenalcortex with loss of normal architecture. The adreno-cortical cells were enlarged and vacuolated. Cholesterolclefts and multinucleated giant cells were present insome areas (Figure 1). Frozen sections stained with oilred-O showed diffuse accumulation of lipid in these cells
and numerous aggregates of birefringent crystals wereseen under polarized light (Figure 2). Macroscopic andmicroscopic examination of the other organs wereunremarkable.
The conversion of cholesterol to pregnenolone is the firststep in steroid synthesis and is catalysed by cytochromep450 side-chain cleavage enzyme (p450scc) and by itselectron transfer proteins NADPH-adrenodoxin reduc-tase (AR) and adrenoxin (AD).1 Initially a defect in thisenzyme formerly termed 20,22-desmolase was thoughtto be the cause of lipoid CAH.2 However, defects inp450scc, AD and AR were simultaneously eliminated bymolecular studies.3 Recently, the gene for steroidogenicacute regulatory protein (StAR), which functions as alabile protein factor mediating cholesterol transportwithin mitochondria, was cloned, and detection ofdifferent mutations in this gene from various ethnicgroups implies these as the cause of lipoid CAH in themost if not all cases of this syndrome.4 Lipoid CAH ischaracterized by the absence or very low levels of allsteroids in blood or urine, high concentrations of ACTHand high levels of plasma renin activity.1,3 Affectedpatients are phenotypically females regardless of karyo-type. Because of failure to produce androgen in utero,males present usually with normal female externalgenitalia and with abdominal, inguinal or labialtestes.2,3 Ambiguous genitalia have also been reportedin affected males.5 Females with this disorder showed noambiguity of either external genitalia or the gonaducts.2
Severity of clinical findings and age of clinicallyapparent adrenocortical deficiency are varied consider-ably. Patients usually present within the first 2 weeks oflife with adrenocortical insufficiency, including poorfeeding, lethargy, dehydration and hyponatraemichyperkalaemic acidosis, that is generally fatal if nottreated in early infancy.2,5 Patients can survive with
Correspondence 185
q 1999 Blackwell Science Ltd, Histopathology, 35, 181–191.
Figure 1. Cholesterol clefts and vacuolated cells in the adrenalcortex (H & E × 33).
Figure 2. Aggregates of birefringent crystals in adrenal illuminatedby polarized light (frozen section × 33).

appropriate mineralocorticoid and glucocorticoid repla-cement theraphy.2 There is an autosomal recessiveinheritance.6 The prenatal diagnosis of lipoid CAH ispossible and can be done by using ultrasonography ofthe fetal external genitalia combined with hormonaldeterminations in amniotic fluid.1 There are not manycases of lipoid CAH with post-mortem findings.2,6 Ourpatient had a clinical picture of acute renal failure. Asthe diagnosis of lipoid CAH was made after post-morteminvestigation, phenotypic and hormonal studies couldnot be performed. Therefore, we wish to emphasize thatlipoid CAH must be considered in neonates with acuterenal failure.
S GogusZ AkcorenS T Kinik
G Tekinalp1
Paediatric Pathology Unit and 1Neonatology Unit,Hacettepe University Children’s Hospital,
Ankara, Turkey
1. Saenger P. New developments in congenital lipoid adrenalhyperplasia and steroidogenic acute regulatory protein. Pediatr.Clin. N. Am. 1997; 44; 397–421.
2. Hauffa BP, Miller WL, Grumbach MM, Conte FA, Kaplan SL.Congenital adrenal hyperplasia due to deficient cholesterol side-chain cleavage activity (20,22-desmolase) in a patient treated for18 years. Clin. Endocrinol. 1985; 23; 481–493.
3. Lin D, Gitelman SE, Saenger P, Miller WL. Normal genes for thecholesterol side chain cleavage enzyme, P450scc, in congenitallipoid adrenal hyperplasia. J. Clin. Invest. 1991; 88; 1955–1962.
4. Bose HS, Sugawara T, Strauss JF III, Miller WL. The pathophysiol-ogy and genetics of congenital lipoid adrenal hyperplasia. N. Engl. J.Med. 1996; 335; 1870–1878.
5. Camacho AM, Kowarski A, Migeon CJ, Brough J. Congenitaladrenal hyperplasia due to a deficiency of one of the enzymesinvolved in the biosynthesis of pregnenolone. J. Clin. Endocrinol.1968; 28; 153–161.
6. Frydman M, Kauschansky A, Zamir R, Bonne-Tamir B. Familiallipoid adrenal hyperplasia: genetic marker data and an approach toprenatal diagnoses. Am. J. Med. Gen. 1986; 25; 319–325.
Large B-cell lymphoma of the mandiblecomprising filiform and signet-ring cells
Sir: We present here a large B-cell non-Hodgkin’slymphoma.1–3 This is a rare lymphoma since it occursin an extranodal site (mandible). It also exhibits morpho-logical and immunohistochemical features of a filiformlarge cell lymphoma4 with signet-ring appearance.5
A 44-year-old woman was referred to the OralDiagnosis Branch, University of Sao Paulo School ofDentistry. She presented a symptomatic expansive
growth of the left mandible. Local lymphadenopathywas absent. Intraorally there was a hard expansiveswelling of the mandible covered by normal mucosa.The panoramic radiograph showed a diffuse radiolucentlesion involving the mandible from the left mandiblebody to the canine of the opposite side.
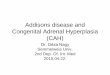
Histological sections revealed a neoplasm composedof compact cellular aggregates (Figure 1a). The tumourcells were characterized by a large nucleus with evenlydispersed chromatin and a single large nucleolus. Rare
186 Correspondence
q 1999 Blackwell Science Ltd, Histopathology, 35, 181–191.
Figure 1. Histopathological and immunohistochemical findings ofthe tumour. Sheet of transformed lymphocytes exhibiting largenuclei with one or more prominent nucleoli (a, H & E, × 100).Signet-ring cells (a, SR) are present. These cells show intracyto-plasmic large vacuoles and peripherally displaced nuclei. Mitoticcell is observed (a, arrow). CD45 RB labels the cell boundaries(b, arrowheads, × 100).

mitotic figures were found. The cells had a moderateamount of pale to eosinophilic cytoplasm. In some cells,nuclei were eccentric with vacuoles in the cytoplasmthat frequently displayed a signet-ring appearance(Figure 1a, SR). There was no evidence of folliculargrowth pattern.
The search for lymphoid markers included: CD45 RB(Dako Co., Glostrup, Denmark), CD20 B-cell marker(Dako), CD45 RO T-cell marker (Dako), CD30 (Dako),and immunoglobulins such as kappa (Biogenex, SanRamon, CA), lambda (Biogenex), IgM (Biogenex) andIgG (Biogenex). Positive reactions in the neoplastic cellswere observed only to CD45 RB (Figure 1b), CD20 andIgG.
The tumour was characterized ultrastructurally bylarge cells with abundant filiform cytoplasmic projec-tions. Except for these processes, neoplastic cellsresembled large transformed lymphocytes. Nuclearcontour was usually ovoid or slightly folded. Thesenoncleaved nuclei revealed a predominant euchromatinpattern with marginated heterochromatin, and one ormore small to large nucleoli. There was abundantcytoplasm containing mitochondria, free ribosomes andpolyribosomes. The majority of neoplastic cells exhibitedelaborated cytoplasmic processes, which were relativelybroad and intertwining (Figure 2).
The most prominent finding was the presence of cellscontaining large vacuoles limited by a single membrane.The vacuoles were electron-lucent, and only a fewvesicular profiles were present at the periphery, inproximity to the limiting membrane. Some neoplasticlymphocytes exhibited single or multiple vacuoles. Cellscontaining a large single vacuole sometimes assumed asignet-ring appearance.
The presence of cells with a signet-ring appearancemay suggest a diagnosis other than lymphoma. Signet-ring cells are seen in a variety of tumours includingadenocarcinomas, malignant melanoma and liposarc-oma. To analyse these diagnostic possibilities we per-formed an initial immunohistochemical investigation ofthe tumour using antibodies against vimentin (Biogenex),cytokeratin (AE1/AE3, Biogenex), and S100 protein(Dako), which resulted in negative reactions.
Three types of signet-ring cell lymphomas, withdistinctive light microscopic, ultrastructural and immu-nohistochemical features, have been described.6 Ourcase fits into the second type where the vacuoles in thecells were clear, PAS-negative, did not stain with theperoxidase-conjugated antiserum, but presented posi-tive reaction to IgG antibody at the periphery of thevacuoles.
There is no agreement in the literature about themechanisms of generation of the signet-ring cell
Correspondence 187
q 1999 Blackwell Science Ltd, Histopathology, 35, 181–191.
Figure 2. Electron micrograph showing large lymphoid cells withrelatively broad interlacing peripheral processes (a, × 10 000). Close-up view of the boxed area shows filiform processes (b, arrows,× 35 000).

morphology in the lymphomas. For some authors theorganelle responsible for the Russell body signet-ringlymphoma appearance is the rER, while for others ismultivesicular bodies. In our case, multivesicular bodieswere not found. In fact, some cells showed dilated ERcisternae that sometimes present fusion sites originatingvacuoles of several sizes. These findings suggest thatthe signet-ring appearance would be the result of ERenlargement, with following formation of vacuoles,which passively aggregate. We believe that a search forspecific ER markers in the limiting membranes ofcytoplasmic vacuoles would be of importance to testthis hypothesis.
M M M Jaeger*J N Santos*R G Jaeger
N N SugayaV C Araujo
Department of Oral Pathology,School of Dentistry,
University of Sao Paulo,Brazil
*Authors contributed equally to this work.
1. Berard CW, Dorfman RF, eds. Malignant Lymphoma. Baltimore:Williams & Wilkins, 1987.
2. Harris NL, Jaffe ES, Stein H et al. A revised European–Americanclassification of lymphoid neoplasms: a proposal from the Interna-tional Lymphoma Study Group. Blood 1994; 84; 1361–1392.
3. Erlandson RA, ed. Diagnostic Transmission Electron Microscopy ofTumors. New York: Raven Press, 1994.
4. Azar HA, Espinoza CG, Richman AV, Saba SR, Wang T-Y.‘Undifferentiated’ large cell malignancies: an ultrastructural andimmunocytochemical study. Human Pathol. 1982; 13; 323–333.
5. Kim H, Dorfman RF, Rappaport H. Signet ring cell lymphoma: arare morphologic and functional expression of nodular (follicular)lymphoma. Am. J. Surg. Pathol. 1978; 2; 119–132.
6. Navas-Palacios JJ, Valdes MD, Lahuerta-Palacios JJ. Signet-ring celllymphoma: ultrastructural and immunohistochemical features ofthree varieties. Cancer 1983; 52; 1613–1623.
Amyloid tumour (amyloidoma) of the leg:histology, immunohistochemistry andelectron microscopy
Sir: Amyloidomas occur very rarely in soft tissues1 andmay present diagnostic difficulties. We report a detailedmorphological and phenotypical analysis of a case ofamyloidoma in a 66-year-old female patient who wasadmitted to the Surgery Department of S. Paolo Hospitalwith a 20 mm subcutaneous tumour-like lesion of theleft leg of one year’s duration. The mass was hypoecho-genic, with indistinct boundaries and a well-distributedvascularization suggesting a malignant neoplasm. The
past medical history was significant for diabetes mellitustreated with insulin subcutaneous administration andsystemic hypertension controlled by medication. Therewas no history of chronic infections or connective tissuesdisorders and no correlation was established betweeninsulin site injection and amyloidoma, nor were previousspecific injuries on the site of the lesion known.
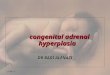
The surgically resected mass measured 50 × 30 ×10 mm. Its cut surface was lobulated, firm and grey-yellow. Histological examination revealed multiplenodules composed of eosinophilic amorphous materialand scattered lymphocytes, plasma cells and multi-nucleated giant cells. Since this histological appearancesuggested amyloid deposits, both haematoxylin andeosin and Congo red stained sections were evaluatedtogether. The sections were examined with and withoutpretreatment with 5% potassium permanganate atroom temperature in order to distinguish immuno-globulin (Ig) derived amyloid (AL),2,3 which retainsbirefringence after oxidation, from AA amyloid which is
188 Correspondence
q 1999 Blackwell Science Ltd, Histopathology, 35, 181–191.
Figure 1. a,b, Congo red stained section showing deposition of amor-phous material; with strong birefringence (a) under polarized lightand strongly reactive (b) to anti-AA antibody (Dako Amyloid Amc1, 1:400, ABC method).

sensitive to permanganate treatment. On the basis ofhistochemical and immunohistochemical reactions thenodules proved to be composed of AA amyloid. Withthe Congo red stain the nodules showed apple-greenbirefringence under polarized light (Figure 1a) withloss of Congo red positivity after treatment with 5%potassium permanganate. With the avidin–biotin–peroxidase complex (ABC) the nodules were decorated(Figure 1b) by anti-AA antibodies (Dako Amyloid A, clonemc1 at dilution of 1 : 400) but were negative with anti-k(Dako A192, 1:16000), anti-l (Dako A 194, 1:2000) andwith islet amyloid polypeptide (Peninsula Laboratories,IHC 7321, 1:4000). Electron microscopy revealed depositscomposed of haphazardously arranged, non branchingfilaments 7.5–10 nm in diameter (Figure 2) which weredecorated with anti-AA antibody (1:100) using theimmunogold staining (IGS) method (Figure 2 inset). Thesample included scattered cellular elements consisting offibroblast-like cells, macrophages with filopodia anddistinct phagolysosomes and multinucleated giant cells.
Amyloidoma or amyloid tumour is a rare lesionoccurring as a localized mass, in absence of systemicamyloidosis. It has been observed in many localizations(buttock, breast, larynx, mediastinum, retroperito-neum, etc.) but rarely in soft tissues.1,4 Whereas mostamyloidomas are composed of AL amyloid derived fromimmunoglobulin light chain, in the present case theamyloidoma was composed of AA amyloid derivedfrom proteolytic cleavage of serum amyloid A protein(SAA). Typically AA amyloid is thought to result fromactivation of the monocyte-macrophage system byinflammatory stimuli with subsequent release of cyto-kines and deposition of amyloid material.
The association of amyloidoma with diabetes mellitusis also uncommon. In the series of 14 cases reported byKrishnan et al. only one case was associated withdiabetes mellitus; it was phenotypically AA amyloid asin our case and it was not islet amyloid polypeptide(IAPP) amylin derived as reported in the literature.3 Ourpatient did not suffer from plasma cell dyscrasia, asascertained by urine and serological studies and therewas no evidence of systemic amyloidosis.
Finally, to our knowledge, this is the first case ofamyloidoma in which the amyloid phenotype wasconfirmed by immunoelectronmicroscopy.
S RomagnoliP Braidotti
F Di Nuovo1
G Coggi
II Department of Pathology,University of Milan School of Medicine and
1Department of Anatomic Pathology,‘G. Salvini Hospital’,
Garbagnate Milanese,Milan, Italy
1. Krishnan J, Chu WS, Elrod J, Frizzera G. Tumoral presentation ofamyloidosis (amyloidomas) in soft tissues. Am. J. Clin. Pathol. 1993;100; 135–144.
2. Stone MJ. Amyloidosis: a final common pathway for proteindeposition in tissues. Blood 1990; 75; 531–545.
3. Tan SY, Pepys MB. Amyloidosis. Histopathology 1994; 25; 403–414.4. Shinoda T, Komatsu M, Aizawa T et al. Intestinal pseudoobstruction
due to dialysis amyloidosis. Clin. Nephrol. 1989; 32; 284–289.
Chondrolipoma of the breast presenting ascalcifications in a routine mammogram
Sir: Cartilaginous differentiation in breast neoplasms israre, and is associated with malignant neoplasms moreoften than benign ones. We recently observed a case of
Correspondence 189
q 1999 Blackwell Science Ltd, Histopathology, 35, 181–191.
Figure 2. Typical amyloid filaments: haphazardously arranged non-branching filaments, 7.5–10 nm in diameter (× 32 800), immuno-reactive (inset) to anti-AA antibody (Dako Amyloid A clone mc1,1:100, IGS).

chondrolipoma of the breast, in which the cartilage wascalcified focally, a feature not previously reported in theliterature.
A 72-year-old Hispanic woman with bilateral breastpain and a maternal history of breast carcinoma,underwent a routine mammogram which showed asubtle increase in the number of calcifications incomparison to the mammograms done two years earlier(Figure 1), with no abnormal density of the parenchyma.Stereotactic core biopsies showed islands of focallycalcified mature hyaline cartilage with fat (Figure 2).The cartilage showed a normal density of chondro-cytes which lacked atypia, multinucleation and mitoticactivity.
Cartilage is rarely seen in the breast, and is associatedprincipally with malignancies, such as sarcoma and‘metaplastic’ carcinoma.1 Benign breast tumours con-taining cartilage are exceedingly rare. Although therehave been descriptions of this entity in the non-Englishliterature dating back to the 19th century, chondrolip-oma of the breast first appeared in the English-languageliterature in 1977 in a case report by Kaplan and
Walts.2 Since then, there have been a number of articleson the subject3,4
Chondrolipomas may occur at any age, althoughmost patients are postmenopausal. They may present asa palpable mass mimicking a fibroadenoma, or as anincidental mammographic finding. Pathological find-ings are of a well circumscribed mass composed of fatand mature hyaline cartilage. Treatment consists ofsimple excision. Our patient declined further treatmentafter the diagnosis was made.
The terminology and pathogenesis of these lesions iscontentious. The question of whether these lesions areneoplasms, hamartomas or choristomas is unsettled. Ahamartoma is defined as an overgrowth of maturetissues normally present in the affected organ. There-fore, the use of this term is imprecise, as there is nocartilage in the normal breast; neither can the termchoristoma be used. Choristomas are ectopic rests ofnormal tissue; chondrolipoma does not represent a‘normal’ structure. Finally, neoplasm, signifying autono-mous ‘new growth’, is the most accurate term for theselesions, since chondrolipomas are composed of benigncartilage and fat.
Chondrolipomas lack an epithelial component andtherefore fall into the category of benign mammarynonepithelial neoplasms. In 1948, Stout5 proposedthe term mesenchymoma to designate benign tumourscomposed of a mixture of two or more nonepithelialelements other than fibrous tissue. Benign mesenchy-momas have been described in children, the mostcommon anatomic location being the retroperitoneum.The term has been abandoned due to its lack ofspecificity.
Other benign breast neoplasms that may containcartilage, include myofibroblastomas and pleomorphic
190 Correspondence
q 1999 Blackwell Science Ltd, Histopathology, 35, 181–191.
Figure 1. a, Mammogram showing a cluster of calcifications.b, Second mammogram, performed 2 years later, showing subtleincrease in the number of calcifications.
Figure 2. Chondrolipoma consisting of islands of mature hyaline car-tilage embedded in adipose tissue. Note the dark areas correspondingto calcifications (breast core biopsy, low magnification).

adenomas. Myofibroblastoma is a benign neoplasmcomposed of myofibroblasts arranged in a fascicular orstoriform pattern in a collagenous stroma occasionallycontaining cartilage and bone. Pleomorphic adenomaof the breast, however, belongs to the category of mixedtumours. Its histological features are similar to pleo-morphic adenomas of the salivary gland. Occasionally,cartilage and bone are found in the myxoid stroma ofthese neoplasms. Adenofibrolipomas or hamartomas ofthe breast may contain cartilage; however, by definition,the presence of extramammary tissue excludes thediagnosis of hamartoma. Arrigoni et al.6 defined breasthamartomas as benign, well circumscribed lesionscomposed of disorganized normal mammary tissuecomponents. They may be mistaken for fibroadenomasor normal breast tissue by the pathologist, particularly ifthe lesion is incompletely excised or only core biopsiesare available for histological examination. Therefore,the diagnosis of mammary hamartoma relies on acombination of clinical, radiological and pathologicalfeatures. Whether these lesions are hyperplastic orneoplastic remains uncertain.
This case expands the pathological differentialdiagnosis of mammographic calcifications.
M T PerezJ B Alexis
Arkadi M. Rywlin MDDepartment of Pathology and Laboratory Medicine,
Mount Sinai Medical Center,Miami and the University of Miami School of Medicine,
Florida, USA
1. Norris HJ, Taylor HB. Sarcomas and related mesenchymal tumorsof the breast. Cancer 1968; 22; 22–28.
2. Kaplan L, Walts AE. Benign chondrolipomatous tumor of thehuman female breast. Arch. Pathol. Lab. Med. 1977; 101; 149–151.
3. Peison B, Benisch B, Tonzola A. Case report. Benign chondrolipomafemale breast. N. J. Med. 1994; 91; 401–402.
4. Marsh WL, Lucas JG, Olsen J. Chondrolipoma of the breast. Arch.Pathol. Lab. Med. 1989; 113; 369–371.
5. Stout AP. Mesenchymoma, the mixed tumor of mesenchymalderivatives. Ann. Surg. 1948; 127; 278.
6. Arrigoni MG, Dockerty MB, Judd ES. The identification andtreatment of mammary hamartoma. Surg. Gynaecol. Obstet.1971; 133; 577–582.
Correspondence 191
q 1999 Blackwell Science Ltd, Histopathology, 35, 181–191.