Embed Size (px)
Citation preview

Case report
Congenital mitral
associated with a
Ghislaine Gilbert, M.D.* Nicholas Aerichid6, M.D.
Lkonard Lapointe, M.D. Paul Da&, M.D.
Montreal, Canada
insufficiency
ventricular septal defect
C ongenital mitral valve defects are rare. Of the cases reported in the
literature, mitral insufficiency is the most frequent and is usually associated with other cardiac ma1formations.i In such cases, the medical manifestations are the same as those with the acquired lesion; however, the onset of symptoms is much earlier and there is no history of rheumatic fever.2 Since the association of mitral insufficiency and ventricular septal defect seems to be very unusual, we present the clinical and pathologic findings in one case.
Case report
R.A., a Z-year-old boy, was admitted to the Insti- tute of Cardiology for complete cardiac investi- gation in February, 1961. His past history revealed that his early growth and development had been essentially normal until the age of 3 months. At that time, he was hospitalized because of marked dyspnea after an episode of acute bronchitis. A heart murmur was detected. He was rehospitalized at the ages of 7, 9, 11, and 20 months for episodes of pulmonary infection with heart failure. Subse- quent to each of these episodes, he became more symptomatic, so that at the time of his admission at the Institute, he was experiencing not only dys- pnea on exertion, but paroxysmal noctural dyspnea, marked cough, and epistaxis.
On physical examination, the child weighed 28 pounds. The heart rate was 100 per minute and regular. The second pulmonic sound was accentu- ated and palpable. A loud systolic murmur was
heard along the lower left border and was accompa- nied by a thrill. There was an apical systolic murmur with a thrill transmitted to the axilla and the back, as well as a short diastolic rumble at the apex. Blood pressure in the arms was 90/70 mm. Hg, and loo/75 mm. Hg in the legs. There were a few &es at both lung bases. The liver was slightly enlarged. There was no cyanosis, clubbing, or peripheral edema. The pulses were normal.
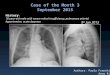
The electrocardiogrant (Fig. 1) revealed left atria1 dilatation, and biventricular hypertrophy. Roent- genographic examination (Fig. 2) showed marked cardiac enlargement with a cardiothoracic ratio of 11.5/17.5. The pulmonary conus was convex, and there was accentuation of the pulmonary vascular markings. On oblique view and after barium swallow. we noticed a marked left atria1 dilatation.
Fig. 1. Electrocardiogram taken on Feb. 22, 1961.
From the Montreal Institute of Cardiology, Montreal, Canada.
Received for publication Oct. 1. 1963. *Address: Institut de Cardiologie de Montreal, 5415 Boul. de l’Assomption, Montreal 36, Quebec, Canada.
107

108 Gilbeyt, Aerichide’, Lapointe, and David
Fig. 2. Chest x-ray films taken on June 22, 1961. oblique view.
Left: Anteroposterior view. Right: Right anterior
Fig. 3. Left atrium. The arrow shows the mitral cleft.
Laboratory studies, including hemoglobin, hema- tocrit, sedimentation rate, white blood count, and urinalysis, were normal.
Cardiac catheterizetion was performed (Table I). Right ventricular and pulmonary pressures were found to be at systemic levels. There was a left-to- right shunt at the ventricular level. The capillary pressure could not be measured.
The diagnosis of ventricular septal defect with left-to-right shunt and systemic pulmonary pres- sure was thus established. However, because of the left atria1 enlargement of a degree not usually seen with ventricular septal defect alone, we thought that there was an associated mitral stenosis con- tributing to the apical diastolic murmur.
The child was discharged. However, the clinical condition became progressively worse, and he was
readmitted for surgery in June, 1962. The physical examination was essentially unchanged. He had lost 1 pound (he weighed 27 pounds), and the liver was palpable 2 fingerbreadths below the right costal margin.
Surgicaljindings. On June 27, 1962, an operation for correction of the congenital cardiac lesions was undertaken with cardiopulmonary bypass and mocl- erate hypothermia. A marked left atria1 enlarge- ment was noted with an intra-atria1 systolic pres- sure of 30 cm. The investigation of the mitral valve with the index finger did not reveal any stenosis. The ventricular septal defect was closed by a pros- thesis. The immediate postoperative course was uneventful, but the child died suddenly 24 hours after operation. The cause of death appeared to be a cerebral vascular accident.
Pathological @dings. At autopsy, there was a marked cardiomegaly, predominantly of the left chnmhers. Roth atria were dilated, the left one being
Fig. 4. View of the left cavities. 1, Mitral cleft. 2, Ventricular septal defect.

Volume 68 Nfrmber 1 Congen,ital mitral insuficiency and ventricular septal defect 109
Table I. Cardiac catheterization data obtained on Feb. 18, 1961, in Patient R.A., 2 years old
Location
Systolic
Pressure (mm. Hg)
I Diastolic Mean
Oxygen saturation
(%)
Superior vena cava 66 Right atrium 10 0 54 Right ventricle-inflow 95 5 74 Right ventricle-outflow 90 5 68 Main pulmonary artery 90 40 60 72 Right pulmonary artery 100 45 74 Left pulmonary artery 9.5 35 70 69
almost aneurysmal. The endocardium of the latter was white and thick. On the anterior wall, there was a rough and reddish area, suggestive of a “jet l&ion,” covered by an adherent clot. The interatrial septum was intact. The mitral opening had a circumference of 9 cm. On the anterior leaflet of the mitral valve, a cleft of 2 cm. was present, causing a major mitral insufficiency (Fig. 3). Both leaflets were thick, and on their free edges were small fibrous nodules at the origin of the chordae. The tricuspid orifice had a circumference of 5 cm., and the leaflets were also thick. The right ventricular cavity was smaller then the left one, with the thickness of the walls, respectively, 0.6 and 1.2 cm. There was a 1.5cm. defect (Fig. 4) in the membranous portion of the ventricular septum. It was located posteriorly and closed surgically by a prosthesis. The pulmonary infundibulum was slightly hypertrophied, but not narrowed. The pulmonary arterial and aortic di- ameters were 2.5 and 1.2 cm., respectively. Both pulmonary and aortic valves were normal. The coronary ostia were normally located. There was no anomalous pulmonary venous drainage, and the vena cava was normally located. Injection of water into the right carotid artery showed complete ob- struction of the intracerebral segment, although the left carotid artery was normally patent. Both lungs were slightly congested. The brain weighed 1,360 grams. There was a slight compression of the cerebellar tonsils. The circumvolutions were flattened. Thus, the major autopsy findings were: a large, posterior ventricular septal defect and a mitral insufficiency caused by a mitral cleft. The cause of death appeared to be a cerebral thrombosis which was probably due to embolization.
Discussion
The interesting feature of this case was the similarity of the clinical picture to that presented by a large ventricular septal defect alone. However, the severity of the symptoms and the early onset of dyspnea made us suspect that the septal defect was not the sole malformation. The symptoms, an apical diastolic rumble, and the x-ray evidence of a large left atrium
were compatible with an associated con- genital mitral stenosis. The hemodynamic findings confirmed the ventricular septal defect and showed a high pulmonary pressure, but it was not possible to register the wedge pressure. However, at operation, the left systolic atria1 pressure was 30 mm. Hg.
The pulmonary congestion with episodes of acute pulmonary edema was secondary to the high pressure in the left atrium. When the mitral lesion is congenital, the signs of pulmonary congestion occur very early. Both mitral stenosis and mitral in- sufficiency may result in enlargement of the left atrium, but it is more marked in the case of regurgitation. If associated with ventricular septal defect, the enlargement is earlier and more rapid because of the in- creased flow by the shunt at the ventricular level.
Cases of congenital mitral insufficiency have been reported as the result of dilata- tion of the annulus ring, fibrous deforma- tion of the leaflet, and anomalous insertion and shortening of the chordae tendineae.3 However, most frequently, congenital mi- tral insufficiency is due to a cleft in the anterior mitral leaflet. This lesion rarely occurs alone, but rather in conjunction with another congenital lesion, such as atria1 septal defect of the ostium primum type.4 Likewise, it is always seen as an integral part of a common atrioventricular canal. It is rarely associated with an atria1 septal defect of the ostium secundum type or with a ventricular septal defect. Such a combined malformation may be a part of the spectrum of an endocardial cushion defect. On the basis of our experience and

110 Gilbert, Aerichidk, Lapointe, and David
the cases reviewed in the literature, we preferred to report our findings as a rare combination of two anomalies. The surgical correction of the lesion depends upon the morphology of the anonlaly.5 A mitral cleft can be repaired by suture of the edges.
Despite the rarity of associated con- genital mitral insufficiency and ventricular septal defect, we think that the lesion could have been suspected clinically on the basis of the apical systolic murmur and thrill which were well transmitted to the axilla and the back, along with the tremendous enlargement of the left atrium. In the majority of the cases described in the literature, there was also a diastolic rumble.
Summary
We have reported the case of a 2-year- old boy with congenital mitral insufficiency and ventricular septal defect. Symptoms began in early infancy with severe, pro- gressive dyspnea on exertion, episodes of pulmonary congestion, and bronchitis. The child underwent operation, with correction
Am. Heart J. July. 1964
of the ventricular septal defect, but, un- fortunately, he died 1 day postoperatively of a cerebral vascular accident.
The rarity of this congenital syndrome is the main reason for our presenting a description of it. A correct diagnosis seems to be feasible.
\%‘e wish to thank Mr. Jean Gauthier, medical photographer of the Montreal Institute of Cardi- ology, for the illustrations.
1.
2.
3.
4.
5.
REFERENCES
Gould, S. E.: Pathology of the heart, Spring- field, Ill., 1960, Charles C Thomas Publisher. Taussig, H. B.: Congenital malformations of the heart, Cambridge, Mass., 1960, Harvard University Press. Edwards, J. E., and Burchell, H. B.: Pathologic anatomy bf mitral insufficiency, Proc. Staff Meet. Mayo Clin. 33:497, 1958. Prior, J. T.: Congenital anomalies of the mitral valve, two cases associated with long survival, AM. HEART J. 46:649, 1953. Starkey, G. N. B.: Surgical experiences in the treatment of congenital mitral stenosis and mitral insufficiency, J. Thoracic Surg. 38:336, 1959.

![[1996] Quantitative Evaluation of the Severity of Mitral Insufficiency in Dogs by the Color Doppler Method](https://img.pdfslide.net/doc/110x75/577c77da1a28abe0548dc0d6/1996-quantitative-evaluation-of-the-severity-of-mitral-insufficiency-in-dogs.jpg)