Embed Size (px)
Citation preview

Thorax (1958), 13, 116.
CONGENITAL OESOPHAGEAL ATRESIA AND TRACHEO-OESOPHAGEAL FISTULA*A REVIEW OF 36 PATIENTS
BY
K. D. ROBERTSFrom the Children's Hospital, Birmingham
" Atresia of the oesophagus, with or withouttracheo-oesophageal fistula, has been a bafflingproblem for the surgeon. If there is any surgeonwho has attempted to save the lives of patientssuffering from these malformations who has nothad many disappointments and numerous trials andtribulations, I have not heard of him."-W. E.LADD (1944).In this paper the clinical features, complications
of operation, and results of treatment are con-sidered in a personal series of 36 babies sufferingfrom congenital abnormalities of the oesophagus.The patients were treated in the Children'sHospital, Birmingham, during the period June,1953, to June, 1957. During this time, 44 suchbabies were admitted and, as an indication of therelative occurrence of these abnormalities, it maybe stated that the average annual admissions forcongenital hypertrophic pyloric stenosis were 85.The classification of oesophageal abnormalities
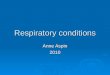
used is that described by Gross in 1953 (Fig. 1).Thirty-three babies belonged to Group C and oneeach to Groups A, D, and E.
In 1955, Roberts, Carre, and Inglis noted thatGroup C could be divided into two subgroups(Fig. 2), namely, Group C(i) in which the fistulaenters the bifurcation of the trachea or thebronchus and there is a considerable length ofatresia; these cases are unfavourable for primaryanastomosis (18 patients); Group C(ii) in whichthe fistula enters the trachea high up and theupper oesophageal segment overlaps the fistulaor the gap between the segments is not great (14patients).
In one baby in the series, there were two fistulaebetween the lower oesophagus and the trachea, onebeing at the thoracic inlet and the other at thebifurcation of the trachea. No similar case hasbeen described in the literature and this one hasprovisionally been classified in both categories asC(i)-(ii).
* Based on a paper read before the Society of Thoracic Surgeonsof Great Britain and Ireland on November 22. 1957.
A feature of the condition which has been neg-lected is the association of atresia with maternalhydramnios. It has long been believed thatatresias of the alimentary tract may cause hydram-nios, as the foetus is unable to swallow and absorbamniotic fluid, and the incidence is particularlymarked in the case of oesophageal atresia(Ballantyne, 1904; Scheurer, 1928; Brigham,1929; Meyer, 1929). In the present series of 36babies, 35 had oesophageal atresia and hydramnioshad been present in 13; the incidence may well behigher than this, as details of the pregnancy havenot always been available.
CLINICAL SYMPTOMS AND SIGNSThe essential feature of total oesophageal
obstruction in the newborn is the inability of thebaby to swallow its saliva, so that a characteristicfine frothy mucus is continually produced in themouth, unlike the rather coarse bubbles which arefrequently found for a time after birth (Belseyand Donnison, 1950). The froth may be bile-stained owing to regurgitation of alimentary con-tents through a tracheo-oesophageal fistula into thetrachea. Lecutier (1955) has given an interestingaccount of " paradoxical haematemesis " in a babywith a Group C abnormality, and one of the babiesin the present series was said to have " vomited"blood shortly after delivery.
Signs of respiratory obstruction with stridor maybe due to a fold of mucous membrane in thetrachea at the site of the fistula (Franklin andGraham, 1953). Stridor was noted before opera-tion in only one baby in the series and recurredafter operation, but no tracheal fold was found atpost-mortem examination to account for it. Iffeeds are attempted, " spill-over" from theobstructed oesophagus into the larynx causescough and cyanosis. Where oesophageal atresia issuspected no feeds should be given until fullinvestigation of the oesophagus has shown that
on July 29, 2020 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.13.2.116 on 1 June 1958. Dow
nloaded from

GROUP A GROUP B GROUP C
GROUP D GROUP E GROUP FFia. 1
Flo. 1.-The varieties of oesophageal abnormality. (Modified afterGross.)
FIG. 2.-The subdivisions of Group C.
GROUP C (i)FiO. 2
on July 29, 2020 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.13.2.116 on 1 June 1958. Dow
nloaded from

K. D. ROBERTS
this can be done. Owing to the inevitable aspira-tion of some oral secretions most infants have a" wet" chest on admission, while atelectasis(usually of the right upper lobe) will be indicatedby diminished air entry.
Occasionally, air may be forced into thestomach when the infant cries so that the abdomenis distended and tympanitic.The clinical features vary according to the type
of abnormality and are summarized in Table I.
TABLE ICLINICAL FEATURES IN VARIOUS TYPES OF
OESOPHAGEAL ABNORMALITY
Clinical Group Group Group Group Group GroupFeature A B C D E F
Excess oral Always Perhaps Always Perhaps No Perhapsmucus
Cough and ,, Always ., Always Perhapscyanosiswithfeeds
"Wet " Usually May be Usually May bebronchial severe severetree
Abdominal Never Never Fre- Fre- Fre- Nodisten- quent quent quentsion
In Groups B and D, if the fistula from theupper oesophagus is large the infant is likely tohave a severe aspiration pneumonia on admission.If the communication between the oesophagus andtrachea is small in Group E cases there may beonly slight difficulty with feeds, cough andcyanosis only occurring in certain positions, andthe condition may not be incompatible with sur-vival. Thus two reported patients were aged 6years (Imperatori, 1939) and 4 years (Haight, 1948)at the time of operation.Of the present cases, 31 of Group C showed
excessive oral mucus as did also the babies inGroup A and Group D. The infant's bronchialtree in the last case was not excessively " wet," asthe fistula between the upper oesophagus and thetrachea was only small and was, in fact, not recog-nized before or during operation but at post-mortem examination. The only patient in GroupE had no oral frothy mucus, but in this patient thefistula was large enough to cause coughing andcyanosis at each of three attempted feeds.When oesophageal atresia is suspected, an
attempt should always be made to demonstratethis by introducing an oesophageal catheter whichcan be passed no further than 10 to 12 cm. fromthe alveolar margin. This was done in 26 ofGroup C cases and showed obstruction to bepresent; it was also a positive finding in bothcases of Groups A and D. It is important to usea rigid enough tube, as this may otherwise coil up
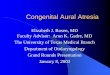
FIG. 3.-Group C abnormality: note the opacity ot the right upperlobe and the distended stomach.
in the upper oesophageal pouch and appear tohave reached the stomach; this happened in twobabies and tube feeds were given, resulting in over-spill into the larynx; passing a larger tube con-firmed the presence of oesophageal obstruction.
RADIOLOGICAL INVESTIGATIONRadiological examination of a baby suspected
of having an oesophageal abnormality shouldbegin with fluoroscopy in antero-posterior andlateral views in order to evaluate the state of thelungs and note the appearance of the stomach andsmall bowel. It is not possible to distinguishradiologically between atelectasis and aspirationpneumonia in these babies and it may only be pos-sible to state that there is an abnormal increase indensity (Fig. 3) in one or more lobes (Holt, Haight,and Hodges, 1946).Where gas is seen in the stomach and intestines
a fistula between the lower oesophagus and tracheamust be present, but the absence of air does notexclude the presence of a small fistula in the
118
on July 29, 2020 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.13.2.116 on 1 June 1958. Dow
nloaded from

CONGENITAL OESOPHAGEAL ATRESIA
(a) (b)Fio. 4.-(a) Oesophageal atresia, with tracheo-oesophageal fistula and duodenal atresia. (b) The stomach and first part of the duodenum
are distended with air, but there is no gas in the small or large intestine.
present cases the fistula was always large enoughto transmit air to the gastro-intestinal tract. Aduodenal atresia may be revealed by gaseous dis-tension of the stomach and duodenum and no gasshadows in the remainder of the intestine (Fig. 4).A " pencil-like " airway may be seen extending
from the region of the trachea to the stomach,indicating the lower oesophageal segment. In thelateral view, the dilated, hypertrophied upperoesophageal pouch may produce a characteristicanterior displacement and narrowing of thetrachea (Selander, 1941). Screening may alsoreveal other developmental defects such as con-genital cardiac abnormalities.
After fluoroscopic examinations a contrastmedium should be introduced into the upperoesophagus; barium sulphate suspension must notbe used owing to its irritant effect should anyenter the bronchial tree. Iodized oil (" lipiodol ")should be put in through an oesophageal catheter(Roberts and others, 1955), and the tech-nique described by Astley (1956) is satisfactory.This consists of introducing a soft rubber catheterinto the oesophagus under radiological control,
the catheter having first been filled with iodizedoil. When the catheter is just in the oesophagus afew drops of oil are injected; these outline therounded termination of the oesophageal pouch atthe level of the second to fourth thoracic vertebrae(Fig. 5). This blind pouch shows up-and-downexcursion with respiratory movement. Too muchoil increases the risk of spill-over into the larynxand trachea, and is a serious error of technique.Radiographs are taken and the catheter is with-drawn after aspirating all the oil from the oeso-phageal pouch. In Groups B, D, and E oil maypass directly into the bronchial tree if the fistulais large enough. An important indication of thepresence of the fistula to the upper oesophagus inGroups B and D is the absence of the typical dila-tation of the upper oesophageal pouch seen inGroup C. This was not appreciated in the onlybaby in Group D in the series, and the presence ofthe upper fistula was not diagnosed radiologicallyor found at operation, being only discovered atnecropsy; the upper fistula was small and did notappear to transmit iodized oil to the trachea atfluoroscopy, but oil spilled over into the larynx,
119
on July 29, 2020 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.13.2.116 on 1 June 1958. Dow
nloaded from

K. D. ROBERTS
Fio. 5.-(a) Antero-posterior view ofoesophageal atresia and tracheo-oesophageal fistula, Group C; note the typical dilatation of theupper oesophageal segnent and the gas in the stomach. (b) Lateralview of Group C abnormality; again note the distended oeso-phageal pouch and gas in the intestines. `(
an error of technique (Fig. 6). A similar case was
reported by Krediet (1955), in which the upperfistula did not fill with iodized oil and was not dis-covered until after death. Krediet felt that therewere no routine means by which this rare abnor-mality could be diagnosed where radiologicalexamination provided no clue.A Group E abnormality may be difficult to
demonstrate. Astley (1956) recommended thatthe infant should be examined in a variety ofpostures, particularly prone and with varyingdegrees of obliquity. Ferguson (1951) has statedthat even if preliminary examination with iodizedoil has excluded oesophageal atresia, bariumsulphate should be avoided, and has pointed outthat recurring or persistent pneumonitis may be
due to a small tracheo-oesophageal fistula.Ferguson suggested passing two thin latex rubberballoons into the oesophagus and inflating themto occlude the lumen, one balloon being in thelower oesophagus, the other in the upper. Acatheter is let down to the segment of oesophagusbetween the balloons and air is injected to dis-tend it. A small amount of iodized oil is injectedand the increased oesophageal pressure forces theoil into the trachea (Fig. 7).
In the only Group E abnormality treated at theChildren's Hospital barium sulphate suspensionhad been given at another hospital; this revealedthe fistula, and fortunately the contamination ofthe bronchial tree did not have serious effects(Fig. 8).
120
on July 29, 2020 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.13.2.116 on 1 June 1958. Dow
nloaded from

FiG. 4.-Anterior view bronchogram of the right upper chest showing woolly opactowards the axilla. ( x 1.)
;ht lateral view of the same bronchogram showing that the woolly shadows inof line shadows. ( x 1.)
-Al
on July 29, 2020 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.13.2.116 on 1 June 1958. Dow
nloaded from

K. D. ROBERTS
OTHER ABNORMALITIES
Congenital abnormalities are often multiple,and other defects were present in seven of the 36babies. These are summarized in Table II.
TABLE IIDEFECTS IN ADDITION TO OESOPHAGEAL ABNORMALITY
Case No. Other Defects
16 Persistent ductus arteriosus20 Incomplete rotation of the gut; agenesis of right kidney;
pelvic left kidney22 Absent thumbs; absent left radius28 Right arching aorta29 Imperforate anus; rectovesical fistula; agenesis of right
kidney30 Ventricular septal defect33 Mongolism; suprabiliary duodenal atresia; Meckel's
diverticulum; incomplete rotation of the gut
TREATMENT
It is not the purpose of this paper to discussdetails of operative treatment and management.Whenever possible, a primary oesophageal ana-
stomosis was carried out, but where tension was
too great or other factors contraindicated an
anastomosis, the first stage of a staged procedurewas done, that is, closure of the fistula, left cer-
vical oesophagostomy, and Stamm gastrostomy.The mortality in the 36 patients is given in TableIII.On considering the type of operation performed
initially in the 33 Group C babies, it is apparentthat one may anticipate a high survival fromprimary anastomosis in patients of Group C(ii) in
MORTALITY INTABLE III
36 CASES OF OESOPHAGEAL ABNORM-ALITY
Total Primary First Second
Group No. of Anasto- Stage Stage DiedPatients mosisStg
C 33 25 - - 108 -3
3
D 1 1 IE I I --0
TABLE IVMORTALITY AFTER VARIOUS PROCEDURES INDIFFERENT TYPES OF GROUP C ABNORMALITY (33 CASES)
Operation Group No. of Cases Deaths
Primary anastomosis .. C(i) 11 7C(ii) 13+(1)* 3
C(i)-(ii) 0
:, C(i) 7 3
C(ii) (I)* 0
* This baby first had a primary anastomosis, but later a first-stageoperation had to be done owing to severe stricture formation andrecurrence of tracheo-oesophageal fistula.
-ontradistinction to those in Group C(i) where.nastomosis is technically more difficult (TableVT).
Five babies underwent a second-stage recon-st iction operation, two attempts being made inor of them. The survival in these babies is shownin [able V.
TABLE VMORTALITY IN FIVE BABIES UNDERGOING RECON-
STRUCTIVE PROCEDURES
Case Operation Result
26 Oesophago-gastrostomy .. Lived*27 Lived31 (1) Colon replacement
(2) Oesophago-gastrostomy .. Diedt32 Colon replacement .. Died33 ,, , I I
* Died at 34 years of age as a result of a road accident.t At the first reconstructive procedure the interposed colon became
black due to traction on the vascular pedicle and was therefore excised.
COMPLICATIONSPre-operative evidence of aspiration of mucus
into the bronchial tree was proved radiologicallyin 16 patients, the commonest site being the rightupper lobe. In the babies surviving operation theaffected lobe eventually re-expanded. New areasof lung opacity developing usually indicatedfurther spill into the bronchial tree due to inco-ordination of swallowing, stricture formation, orrecurrence of the tracheo-oesophageal fistula.Other threats to survival were a variety of con-ditions causing intrapleural tension.
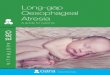
POST-OPERATIVE OESOPHAGEAL STRICTURE.Some narrowing of the oesophageal anastomosis iscommon after a primary anastomosis for atresia.Significant stenosis leads to difficulties in feedingand, more important, to the overspill of oralsecretions into the bronchial tree. Strictures maybe divided into two groups: early, developingwithin six weeks of the anastomosis, and late,occurring more than six months after operationor persisting from the early stage (Figs. 9 and 10).
In nine babies early strictures were found andin three late, one of these babies also having hadan early stricture but apparently being well for17 months after discharge from operation (TableVI). An early stricture is caused by necrosis dueto tension at the suture line. Thus any attempt toexcise an early stricture and re-anastomose theoesophagus is likely to fail, as the oesophagus hasnot had time to grow and adequate length will notbe available. A plastic operation was performedin one baby, but it continued to aspirate mucusinto the bronchial tree and died. Re-anastomosiswas done for a stricture and a recurrence of a
122
on July 29, 2020 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.13.2.116 on 1 June 1958. Dow
nloaded from

CONGENITAL OESOPHAGEAL ATRESIA 123
........ y,Fio. 9,-(a) Severe stricture at the site of' anastomosis 10 days post-operatively; oral feeds were supplemented by gastrostomy feeds.(b) The same patient aged 2j years.
Fio. IO.-Oesophageal stricture 20 months after primary anastomosis.
__1 ~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~.
FIG. Q(a)
l X7X:.........................:.:.:. 10
FIG.g(b>~~ ~ ~ ~ ~ ~ ~ ~ ~~~~FG 1!0
FIG. q (b)
on July 29, 2020 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.13.2.116 on 1 June 1958. Dow
nloaded from

K. D. ROBERTS
TABLE VIEFFECT OF OESOPHAGEAL STRICTURE AND ITS
TREATMENT ON SURVIVAL
Strpctureo Treatment Result
Early Prolonged gastros- Survivedtomy feeds
None needed dur- Survived but strictureing first admis- persisted. See belowsion
Prolonged gastros- Survived; later hadtomy feeds recurrence of tra-
Early + recurrenceof tracheo-oeso-phageal fistula
Early
Late,,9
9,9
(l) Gastrostomy(2) Plastic opera-
tionRe-anastomosisand closure offistula
(1) Dilatations(2) Conversion to
first-stageoperation
Prolonged gastros-tomy feeds
Dilatations,,1
.,$
cheo-oesophagealfistula
Died; lung abscessdue to penetrationof stomach, dia-sphragm, and leftlower lobe by gas-trostomy tube
Died
Survived
tracheo-oesophageal fistula in one baby; a trache-ostomy was necessary as further overspill ofmucus was not prevented and eventually theanastomosis broke down to cause a right pyo-
pneumothorax from which the baby died.Oesophageal dilatation in the acute stage is alsounlikely to succeed and failed in the only baby inwhich it was attempted.From the experience of the above nine patients,
the management of an early stricture has beendeveloped. If overspill of mucus is not excessive,and a naso-gastric polythene tube can be passedthrough the stricture, this provides a satisfactorymethod of giving feeds, while the tube acts as an
indwelling bougie; when an iodized oil swallowwith the tube in situ shows an adequate lumenoral feeds can be resumed, supplemented at firstby tube feeds. A difficulty with a naso-gastrictube may be atonicity of the upper dilated oeso-
phageal segment so that saliva cannot be swal-lowed past the tube through the stricture andspills over; a gastrostomy is then necessaryfor feeding. An unusual cause of death in one
patient was perforation of the stomach, diaphragm,and left lower lobe by the gastrostomy tube, ulti-mately causing a lung abscess. When the stricturefails to respond to conservative measures (in threeof the eight cases in the present series) a procedurelikely to prevent death from aspiration pneumonia
is a thoracotomy to divide the oesophagus, thelower segment being closed and the upper endexteriorized as a cervical oesophagostomy: agastrostomy is done for feeding.
Late strictures have occurred in three patientsand have responded to oesophageal dilatation.The difficulties with the late cases are nutritional,as the infant is unable to swallow solid foods.Mucus overspill is not a feature, and correctiveoperations do not seem to be necessary.RECURRENCE OF THE TRACHEO-OESOPHAGEAL
FISTULA.-As with oesophageal stricture, twogroups of recurrent fistula have been found (TableVII). Early fistulae are those developing within
TABLE VIIEFFECT OF RECURRENCE OF TRACHEO-OESOPHAGEAL
FISTULA AND ITS TREATMENT ON SURVIVAL
Ca Type of Recurrence ofNo. Tracheo-esophageal Treatment SurvivalNo.Fistula
23 Early Operative closure Died31 ,, Conversion to first- Survived
stage operation3 Late Operative closure10 .,
six weeks of the primary operation, and late recur-rences are those found after three months fromoperation.Two early recurrences were diagnosed. In one
the addition of a severe oesophageal strictureinfluenced the attempt to excise the stricture,close the fistula, and re-anastomose the oeso-phagus, but leakage from the anastomosis causedthe baby's death. The other early recurrence wasassociated with a stricture, but, in the light of theprevious case, at re-operation the oesophagus wasdivided, the lower end closed and the upper endexteriorized. The fistula closed and a feedinggastrostomy was done; the baby survived butdied after a reconstruction operation.Three late recurrences were found. In one baby
it was successfully closed at the age of 7 months(Fig. 1 1). The other two were successfullyoperated on at the ages of 1 year and 7months respectively, and in both there had beenan early oesophageal stricture.The coexistence of a severe oesophageal stric-
ture with recurrence of a tracheo-oesophagealfistula in the two early cases, and the fact that intwo of the late recurrences an early stricture hadbeen present, suggests to us that the cause ofrecurrence is necrosis at the oesophageal sutureline. Certainly in one early recurrence at opera-tion the oesophagus communicated with the
CCaseNo.
4
9
10
1121
22
23
31
36
679
124
on July 29, 2020 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.13.2.116 on 1 June 1958. Dow
nloaded from

FIG. 1 I.-(a) Recurrence of tracheo-oesophageal fistula three monthspost-operatively. (b) Recurrence of tracheo-oesophageal fistulaseven months post-operatively; note the " lipiodol" lying out-side the oesophagus. (c) Normal oesophagus following opera-tive closure of the fistula.
§o(
|i#E.._~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~....w.... ~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~.....~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~...;f .q-e a~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~j. ...
151>
:~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~......:..::S . ~~~~~~~~~~~~~~~(b)...
.;..i;......
(c)
on July 29, 2020 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.13.2.116 on 1 June 1958. Dow
nloaded from

K. D. ROBERTS
trachea via a small peri-oesophageal abscess, andin the other there was recent acute mediastinitis.However, it is possible that in one of the late casesthe fistula may have recurred owing to a portionof fistula being left attached to the trachea at theprimary anastomosis as the appearance at thesecond operation suggested; infection in a" tracheal diverticulum" might lead to abscessformation in the mediastinum (comparable to abronchial stump abscess) and the abscess couldlater rupture into the oesophagus.From the above cases the management of a
recurrent fistula can be described. First, an earlyfistula, being associated with recent infection,should not be treated by early operative closure,as this is likely to break down. Whenever possiblethe baby should be tided over with naso-gastrictube or gastrostomy feeds until the acute media-stinal infection has subsided. Should operation benecessary, for example, if a coexistent strictureleads to considerable mucus overspill into thebronchial tree, then the correct procedure appearsto be an exteriorization as described for earlystricture.The second point is that a recurrent fistula is
unlikely to close spontaneously. Such manceuvresas cauterization of the fistula with silver nitratethrough a bronchoscope (attempted in one baby)are of doubtful value, as sufficient cauterizationto destroy the fistula would also cause breakdownand mediastinal abscess. In one baby the fistulaapparently closed after a gastrostomy, but at alater examination it was still open and operativeclosure was necessary.Cough with feeds, perhaps associated with
cyanosis, may be due to oesophageal stricture ora recurrence of tracheo-oesophageal fistula. Thelatter may be difficult to demonstrate radio-logically, although the persistence of a radio-logical picture of bilateral pneumonitis, or of arecurrent pneumonitis, is suggestive. Since thefistula takes an oblique course upwards from theoesophagus to the trachea, radiological screeningin a variety of positions (particularly prone) afteran iodized oil swallow is necessary. Ferguson'smethod (1951) may be used. Should repeatedexaminations with iodized oil be negative, but theclinical picture and radiological evidence of pneu-monitis still point to the presence of a fistula,bronchoscopy may be helpful, as mucus or fooddebris may be seen to extrude from the fistula.INCREASED INTRAPLEURAL TENSION. - Tension
effects after primary anastomosis may be due toleakage of air from the trachea, or a breakdownof the oesophageal anastomosis. A tracheal leak
occurred in one baby; during dissection of theupper oesophageal segment a small perforationwas made in the trachea. Although this wassutured, and no apparent air leak was demon-strable, this was probably due to close appositionof the endotracheal tube. On removing this atthe end of the operation and inflating the lungsthrough a face-mask a tension pneumothoraxdeveloped, causing cardiac arrest; although thetension was relieved and the heart restarted, deathoccurred later from cerebral damage. In additionto this experience, a tension pneumothoraxoccurred in another baby, the leak being presumedto occur through the sutured tracheal end of thefistula, but its presence was recognized in time andan intercostal tube inserted; this baby survived.
Oesophageal leakage occurred in two babiesafter primary anastomosis. In one the conditionwas treated by intercostal tube drainage andgastrostomy feeds until the oesophagus healed andthe baby survived. The other baby had an opera-tive closure of a perforation below the anastomosis(possibly through an avascular area of oeso-phagus), this being necessary as the intercostaltube repeatedly obstructed with debris so that ten-sion recurred, but the baby died from atelectasisdue to inhaled mucus. In a third baby there wasa leakage from the anastomosis after reoperationfor an oesophageal stricture and recurrence of afistula, and this baby died from a mediastinalabscess and suppurative pneumonitis, although thelung had re-expanded after drainage.The acute mediastinal infection which occurs
when an oesophageal leak develops is best treatedby ensuring lung expansion by underwater-sealedintercostal drainage, and maintaining nutrition bygastrostomy feeds. It sometimes happens thatmost of a gastrostomy feed is regurgitated into thepleura through the oesophageal perforation, pre-sumably because (for some reason unknown) thecardia becomes incompetent. This occurred in thebaby described above and responded to withhold-ing gastrostomy feeds for a week, hydration beingmaintained parenterally. Should the cardia notbecome competent at the end of this time, so thatall the gastrostomy feed drains via the pleuraltube, a feeding jejunostomy may be necessary.
After reconstructive procedures, distension ofthe intrathoracically placed viscus (stomach orcolon) may seriously embarrass respiration. Inone baby, distension of the stomach in the leftpleural cavity produced the clinical and radio-logical appearance of a tension pneumothorax(Fig. 12). It proved impossible to pass a tubeinto the stomach as it was held up at the anasto-
126
on July 29, 2020 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.13.2.116 on 1 June 1958. Dow
nloaded from

CONGENITAL OESOPHAGEAL ATRESlA
FIG. 12.-Gaseous distension of the stomach following cervicaloesophago-gastrostomy. The left lung is collapsed and themediastinum displaced to the right, causing right upper lobecollapse.
mosis, and the stomach could not be aspiratedwith a needle, so thoracotomy and transpleuralgastrostomy were done; the baby survived. In
I
FIG. 13.-Severe distension of the intrathoracic colon. The left lungis totally collapsed.
another oesophago-gastrostomy a pyloro-myotomywas done to prevent post-operative pyloro-spasmand the stomach drained by a transpleural gastro-stomy and tension did not occur. A sufficientlylarge oesophageal tube to evacuate the stomachcannot be left down in a small infant, as thiswould obstruct the anastomosis leading to salivaspilling over.When a colon graft is used to restore continuity,
difficulty may arise from a closed loop obstructingthe graft. This is due to three factors: first, tostomal oedema at the oesophago-colic and gastro-colic anastomoses; secondly, to pressure on thegraft at the thoracic inlet and oesophageal hiatus;and thirdly, because the graft is largely de-nervated. In one baby the graft was widely dis-tended, eventually perforating (Fig. 13); the heartstopped, and, although the heart beat was restoredby massage, intrapleural tension was relieved, andthe graft sutured and drained transpleurally, cere-bral damage resulted in the baby's death.
In future cases it is now advised that oesophago-colic anastomosis be delayed, the upper end of thegraft being drained on the neck until all danger ofobstruction is past.
DISCUSSION OF RESULTSHumphreys, Hogg, and Ferrer (1956) listed the
factors they considered to influence survival asfollows: (1) The size and degree of prematurityof the infants ; (2) the association with othersevere malformations; (3) the awareness ofdoctors and nurses caring for newborn infants ofthe possibility of the condition and their alertnessin recognizing it; (4) the promptness with whichbabies are referred for surgery; (5) the care inpre- and post-operative management; (6) thetechnical aspects of the operation itself.They considered that, although the first two of
these are uncontrollable, the others leave room forimprovement. Shaw (1956), in discussing theirpaper, pointed out that delay in surgical treatmentneed not necessarily result in death, and thenquoted the case of a baby aged 28 days who hadbeen maintained on parenteral fluids and then sur-vived a primary oesophageal anastomosis.
Since it is reasonable to suppose that the pre-sumed high mortality for infants of low birthweight is from lung complications due to a feeblecough reflex, the deaths occurring within twoweeks of operation (nine) have been plotted withthe survivors for corresponding birth weights inthe form of stick graphs (Fig. 14). There does notappear to be any great difference in two weeks'
127
on July 29, 2020 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.13.2.116 on 1 June 1958. Dow
nloaded from

K. D. ROBERTS
10 Q4iV ot
0
z
Under 4-5 5-6 6-7 7-8 Over4 lb. lb. Ib. lb. lb. 8 lb.
Birth weightFIG. 14.-Histogram of the mortality and survival rate within the
first two post-operative weeks at various birth weights.
survival between any groups. These nine deathsare then plotted with the survivors for two weeksagainst the age of the baby on admission, sincemany presume that delay in admission for surgeryincreases the mortality due to established aspira-tion pneumonitis (Fig. 15). Again there seems tobe no indication that moderate delay is unfavour-able, the longest period before admission beingfive days. The nine early post-operative deathshave been analysed in Table VIII.
Six of the early deaths are attributable to spill-over of oral secretions into the bronchial tree. Inone a large persistent ductus arteriosus may havebeen a contributory factor. One death caused bya tension pneumothorax was due to a technicalerror and should not have occurred. The cause
15
10
0-_ '
z
f'QAEea.ve upton2 weeks
after opertion
nII
Under 12-24 25-48 49-72 Over12 hr. hr. hr. hr. 72 hr.
Age on admission
FIG. 15.-The mortality and survival rate within the first two post-operative weeks at various ages of admission to hospital.
TABLE VIIICAUSE OF DEATH WITHIN TWO WEEKS OF OPERATION
Case No. Cause of Death
16 Atelectasis: ? persistent ductus arteriosus17 Atelectasis19 ,.20 Tension pneumothorax: anoxia of the cardio-
respiratory contre24 Bronchopneumonia25 Atelectasis28 ? Anoxia of cardio-respiratory centre34 Probable leakage from thoracic duct35 Bronchopneumonia
of death was confirmed by post-mortem examina-tion in all save one patient. In this baby goodrespiratory movements were not resumed afteroperation; rib recession had been present beforeoperation, and death clinically appeared to bedue to a gradual cardio-respiratory failure fromanoxia, although intolerance to the anaestheticagents cannot be excluded.Out of 18 deaths in hospital, permission for
post-mortem examination was obtained in 16. Thecause of death in these patients is summarized inTable IX. One other child died at the age of31 years from multiple injuries following a roadaccident, but has been counted as a survival ofoperation; no post-mortem findings are availablefor this child.
TABLE IXCAUSE OF DEATH IN 18 PATIENTS'AFTER OPERATION
CNaose Operation Necropsy Cause of Death
16 Primary Yes Atelectasis; ? persistent ductusanastomosis arteriosus contributing
17 Atelectasis18 Unknown191, Atelectasis; small tentorial tear
with intracranial haemor-rhage
20 Tension pneumothorax; anoxiaof cardio-respiratory centre
21 Empyema; lung abscess22 Atelectasis23 Pericarditis; mediastinal ab-
scess; fibro-purulent pleurisy24 Bilateral confluent broncho-
pneumonia25 Atelectasis28 First stage No Anoxia of cardio-respiratoryI centre
29 Yes Mediastinal abscess30 Ventricular septal defect31 Second stage Peripheral circulatory failure
due to inadequate bloodreplacement
32 Rupture of colic graft; anoxiaof cardio-respiratory centre
33 No Post-operative respiratory ob-struction; ? inhaled mucus.Anoxia of cardio-respiratorycentre
34 First stage Yes Peripheral circulatory failuredue to thoracic duct leakage
35 Primary Bronchopneumonia; unsuspec-anastomosis ted fistula between upper
oesophagus and trachea
128
on July 29, 2020 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.13.2.116 on 1 June 1958. Dow
nloaded from

CONGENITAL OESOPHAGEAL ATRESIA
Thus, of 18 deaths, seven were due to aspirationof mucus and oral secretions into the bronchialtree (atelectasis, bronchopneumonia), a contribu-tory factor in one case being intracranial haemor-rhage from a tentorial tear. Four infants diedowing to cerebral damage, anoxia of the cardio-respiratory centre being due to cardiac arrest intwo as a result of tension effects (tension pneumo-thorax in one; rupture of a colon graft in one);one patient failed to breathe properly followingoperation, and in one the heart stopped a shorttime after operation.
Sepsis was responsible for death in threebabies; one constituted an error of managementas a gastrostomy tube had perforated the fundusof the stomach, passed across the diaphragm andinto the left lower lobe, causing a lung abscess.Peripheral circulatory failure was due to inade-quate blood transfusion in one baby. In anotherrecurrent bilateral pleural effusions were probablydue to a thoracic duct injury, but the characteristicchylous fluid was not obtained on aspiration asthe baby was being maintained on parenteralfluids, and no fat had been given into the ali-mentary tract.One baby's death was unexplained; in view of
the possibility of mediastinal leakage from theoesophageal anastomosis, gastrostomy feeds werebeing given, and death occurred suddenly onehour after a feed; at post-mortem examination nocause of death was found, and the oesophagealanastomosis had healed.
CONCLUSIONSWhenever possible, primary oesophageal anas-
tomosis should be done for oesophageal atresia,and in those cases most suitable for anastomosis(Group C(ii)) a high survival rate may be ex-pected. Where tension is too great to allow a safeanastomosis, a staged procedure should be done.Further improvement in the prevention and treat-ment of atelectasis in the infants is required todecrease the immediate post-operative mortality.Early recurrence of a tracheo-oesophageal fistula,or early stricture formation, are best treated con-servatively. When the prevention of aspiration ofmucus into the bronchial tree demands furthersurgery the cervical oesophagus should beexteriorized, the lower oesophagus closed, andfeeding gastrostomy should be done.
Reconstruction by oesophago-gastrostomy givesa good chance of survival to two babies out ofthree in the series, the one death being due toinadequate blood replacement after operation.When colon oesophagoplasty is done, specialcare is necessary in post-operative management.The three colon grafts in the series have been un-successful. One failed owing to death of thegraft at the time of operation because there wastraction on the pedicle, and this was the baby thatfailed to survive oesophago-gastric anastomosislater. One baby died shortly after operation,probably from respiratory obstruction due to in-haled mucus, and in the other a "closed-loop"obstruction of the graft was recognized andtreated too late. In future cases it will be advis-able to delay oesophago-colic anastomosis until alldanger of obstruction of the graft is past.
It is with great pleasure that I record my indebted-ness to Mr. A. L. d'Abreu, by whose permission thesepatients were treated, and whose encouragement wasa constant stimulus. I am extremely grateful to thephysicians of the Children's Hospital, Birmingham,for referring these babies to me, and especially toProfessor J. M. Smellie, to whose ward most of themwere admitted. The radiological investigations con-ducted by Dr. Roy Astley have been an essentialfeature of the work. A debt of gratitude which can-not be placed too highly is owed to successive residentmedical officers and the nursing staff at the Children'sHospital, Birmingham, for their devoted care of theseinfants. Mr. J. G. Williamson has been responsiblefor the excellence of the illustrations. To MissMargaret Wilkie I am especially grateful for typingthe manuscript.
REFERENCESAstley, R. (1956). Radiology of the Alimentary Tract in Infancy.
Arnold, London.Ballantyne, J. W. (1904). Manual of Antenatal Pathology and
Tfvrriene. Green. Edinburgh.Belsey, R. H. R.. and Donnison, C. P. (1950). Brit. med. J., 2, 324.Brigham, R. 0. (1929). Amer. Med. (Philad.), 35, 297.Ferguson, C. F. (1951). Laryngoscope, 61, 718.Franklin, R. H., and Graham, A. J. P. (1953). Thorax, 8, 102.Haight, C. (1948). J. thorac. Surg., 17, 600.Holt, J. F., Haight, C., and Hodges, F. J. (1946). Radiology, 47, 457.Humphreys, G. H., Hogg, B. M., and Ferrer, J. (1956). J. thorac.
Surg., 32, 332.Imperatori, C. J. (1939). Arch. Otolaryngol., 30, 352.Krediet, H. (1955). Arch. chir. neerl., 7, 265.Ladd, W. E. (1944). New Engl. J. Med., 230, 625.Lecutier, E. R. (1955). Brit. med. J., 1, 647.Meyer, H. (1929). Zbl. Gynak., 53, 1562.Roberts, K. D., Carr6, I. J., and Inglis, J. McN. (1955). Thorax,
10,45.Scheurer, D. (1928). Schweiz. med. Wschr., 9, 1097.Selander, E. (1941). Acta radiol. (Stockh.), 22, 802.Shaw, R. R. (1956). J. thorac. Surg., 32, 343.
129
K
on July 29, 2020 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.13.2.116 on 1 June 1958. Dow
nloaded from












![Congenital multiple colonic atresias with intestinal ... · Congenital intestinal atresia develops in 1 in 1500 to 20, 000 births [1, 2]. Colonic atresia, which accounts for 1.8–15%](https://img.pdfslide.net/doc/110x75/611666aecc6a8a6a642d622a/congenital-multiple-colonic-atresias-with-intestinal-congenital-intestinal-atresia.jpg)