Embed Size (px)
Citation preview

American Journal of Medical Genetics 29:263-268 (1988)
Congenital Scalp Skull Defects With Distal Limb Anomalies (Adams-Oliver Syndrome-McKusick 10030): Further Suggestion of Autosomal Recessive Inheritance
C.P. Koiffmann, A. Wajntal, B.J. Huyke, and R.M. Castro
Genetic Counseling Unit, Department of Biology, Institute of Biosciences (C.P. K., A. W.) and Dermatological Clinic Division of Hospital das Clinicas, Faculty of Medicine (B. J.H., R.M.C.) University of Siio Paulo, SBo Paulo, S. P., Brazil
We describe a man with manifestations of the Adams-Oliver syndrome: congenital scalp defect with hypoplastic fingers and toes. The patient has normal first-cousin parents: among seven sibs, three sisters and two brothers are normal; two brothers born with the same scalp lesion died as a consequence of bleeding from this abnormal area. There is no evidence of other affected relatives. The family of our patient is suggestive of autosomal recessive inheritance of this disorder with phenotypic manifestations identical to those present in the autosomal dominant form. Dermatoglyphic findings are discussed.
Key words: congenital scalp bleeding, hypoplastic fingers and toes, congenital scalp lesion with fhger and toe anomalies, tortuous scalp veins
INTRODUCTION
Adams-Oliver syndrome is a rare syndrome of congenital scalp and skull defects with distal limb anomalies [Adams and Oliver, 19451.
Apparent autosomal dominant inheritance and variable expressivity has been reported in at least six families [Adams and Oliver, 1945; Scribanu and Temtamy 1975; Burton et al., 1976; McMurray et al., 1977; Bonafede and Beighton, 1979; Hidalgo et al., 19831. One other report is suggestive of autosomal recessive inheritance [Kahn and Olmedo, 19501. Sporadic cases have been reported [Farmer and Maxmen, 1960; Fryns et al., 1977, review in Toriello et al., 19881.
Received for publication September 9, 1986; revision received September 15, 1987.
Address reprint requests to C.P. Koiffmann, Unidade de Aconselhamento Genitico, Departamento de Biologia, Instituto de Biocibncias, Universidade de SBo Paulo, Caka Postal 1 1.461, CEP 05.499, SBo Paulo, S.P., Brad.
0 1988 Alan R. Liss, Inc.

264 Koiffmann et al.
V
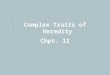
Fig. 1. Pedigree.
We have studied one patient with scaIp/skull defects and distal limb anomalies, whose two younger brothers bled to death from a congenital scalp lesion. His normal parents are consanguineous and no other relatives are affected.
CLINICAL REPORT
The propositus (A.B.P.), a 19-year-old mulatto man, was born in Minas Gerais, Brazil, to healthy, young and consanguineous parents. He was the product of his mother’s fifth pregnancy. Birth weight and length were not recorded; the propositus stated that he had bled neonatally from a vertex scalp lesion which healed spontaneously. The family pedigree is shown in Figure 1. Among his seven sibs, three sisters and two brothers are normal; two brothers, born with the same scalp defect, died before age two months of bleeding from this abnormal area. There is no evidence of further scalp or limb defects in other relatives.
The propositus was referred because of alopecia on the vertex of the scalp and chronic headache.
At the time of examination, he was 162 cm tall and had an arm-span of 162 cm, the OFC was 55 cm. There was a hairless discoid lesion (8 x 6.5 cm) on the vertex which was hypochromic, cicatricial, smooth, lustrous, hard, nonretractile and with atrophic and nodular areas (Fig. 2). The second to fifth fingers and toes were hypoplastic, the right limbs being more severely affected than the left. The affected fingers were short with narrow tips and hypoplastic but present nails; there was a single flexion crease on each finger on the right and on the second digit on the left. There was partial syndactyly of the second, third and fourth toes on the left and between the second and third toes on the right. Hypoplastic nails were present on all toes. Besides moderate bilateral gynecomastia, the patient was otherwise normal. The parents were not available for examination.
Complementary Tests Head and limb radiographs show normal cranium with normal sella turcica and
hypophalangism on fingers (Fig. 3) and toes (Fig. 4). Intense hypoplasia of median and distal phalanges can be seen on fingers R4, R5 and L3. A line of osseous sclerosis can be seen on the remaining fingers suggesting that clefting did not develop between the second

Autosomal Recessive Adams-Oliver Syndrome 265
Fig. 2. Propositus. Scalp lesion with cicatricial alopecia.
and third phalanges. Proximal phalanges with more or less rudimentary second phalanges are present on all 10 toes and vestiges of third phalanges on toes R2-4. Histopathological examination of a scalp fragment showed restored epidermis, thickened dermis showing an excess of collagen and absence of anexe; elastic fibers were conserved. The histological aspect was that of cicatricial alopecia.
Dermatoglyphics Digits: left hand, L" (4), A, L" (2), LR (2), A'; right hand, L" (8), absence of digital
patterns on the remaining fingers. Normal palmar flexion creases. Main line formula left hand: 9.7.5".5'.13-t, t"-LR/L"; right hand; 9.9.5".5'13-t, t"-A"/W.A".M.L.M. (Fig. 5 ) .
DISCUSSION
In the family described by Adams and Oliver [ 19451, eight persons were affected in three generations; the anomalies varied in their appearance and degree. The authors suggested that the syndrome was an autosomal dominant trait with complete penetrance and variable expression. Later, Kahn and Olmedo [ 19501 reported one patient with the same association and cutis marmorata; the patient's sister had only scalp anomalies. Farmer and Maxmen [ 19601 described one patient who also had prominent, tortuous scalp veins. Scribanu and Temtamy [I9751 studied a family in which the propositus had skull and scalp defects and terminal transverse defects of the lower limbs; he also had cutis marmorata and prominent and tortuous scalp veins; the hands were normal. His mother was clinically normal, with the toes on the right shorter than those on the left, and his maternal aunt was said to have similar defects on the lower limbs, and one of her children had cutis marmorata and prominent scalp veins; this family is suggestive of autosomal dominant inheritance with variable expressivity. Burton et al. [ 19761 reported a family that provides additional evidence for autosomal dominant inheritance of this disorder; the expression of the trait was extremely variable in this family but the affected relatives had

266 Koiffmann et al.
Fig. 3. showing hypoplastic phalanges on fingers.
A. Hypplasia of fingers and nails of propositus. B. Diagrammatic representation of radiographs
hypoplastic toes and normal hands. McMurray et al. [1977] described two affected children and an affected father; the father had only the scalp lesion but the children had scalp/skull defects and absent distal phalanges of the feet, except for the great toes. Hands were normal, and autosomal dominant inheritance was suggested. Finally, Bonafede and Beighton [1979] described nine persons in four generations of a kindred in which congenital scalp defects were associated with abnormalities of hands and feet; the difficulties of genetic counseling were pointed out because the clinical expression in each of

Autosomal Recessive Adams-Oliver Syndrome 267
Fig. 4. showing hypoplastic phalanges.
A. Hypoplastic toeS and nails. Note syndactyly. B. Diagrammatic representation of radiographs of feet
the kindreds already described was variable. Since then one more family, studied by Hidalgo et al. [ 19831, pointed to autosomal dominant inheritance with incomplete penetrance and variable expressivity, as the patient with scalp/skull defect and short fingers and toes had a paternal great aunt with skull defect and short distal phalanges and parents were referred as normal.
Our patient has Adams-Oliver syndrome with congenital scalp/skull and limb anomalies. However, autosomal dominant inheritance is unlikely as parents and other relatives seem to be normal. Furthermore, the fact that the parents of our patient are first cousins and the presence of two affected sibs points towards autosomal recessive inheritance, as suggested by Kahn and Olmedo [ 19501, although autosomal dominant inheritance cannot be ruled out. Genetic heterogeneity and variability of clinical expres-

268 Koiffmann et al.
Fig. 5. especially on the right.
Hand prints of propsitus. Note absence of digital patterns and single flexion creases on some fingers,
sion makes genetic counseling difficult. However, ultrasound examination around the 16th week of pregnancy may detect the limb anomalies. Physicians should be prepared to treat promptly the scalp lesion that might be present.
ACKNOWLEDGMENTS
This work was supported by the Conselho Nacional de Desenvolvimento Cientifico e Tecnol6gico (CNPq), Brasil. The photographic service was done by Mr. Romildo Fabricio and Ana Flora C. Billerbeck. We thank Dr. John Opitz for the stimulating attention in examining our data.
REFERENCES
Adam FH, Oliver CP (1945): Hereditary deformities in man due to arrested development. J Hered 36:3-8. Bonafede RP, Beighton P (1979): Autosoma1 dominant inheritance of scalp defects with ectrodactyly. Am J Med
Burton BK, Hauser L, Nadler HL (1976): Congenital scalp defects with distal limb anomalies. J Med Genet
Farmer AW, Maxmen MD (1960): Congenital absence of skin. Plast Reconstr Surg 25291-297. Fryns JP, Corbeel L, Van den Berghe H (1977): Congenital scalp defect with distal limb reduction anomalies.
Eur J Pediatr 126:289-295. Hidalgo JE, Greer DM, Johnston DW (1983): Congential scalp defect with distal limb anomalies: Brachydactyly
and hypoplastic toes. Plast Reconstr Surg 72:708-711. Kahn EA, Olmedo L (1950): Congenital defect of the scalp with a note on the closure of large scalp defects in
general. Plast Reconstr Surg 6:435440. McMurray BR, Martin LW, Dignan PStJ, Fogelson MH (1977): Hereditary aplasia cutis congenita and
associated defects: Clin Pediatr 166 1 MI 4. Scribanu N, Temtamy SA (1975): The syndrome of aplasia cutis congenita with terminal transverse defects of
limbs. J Pediatr 87:79-82. Toriello HV, Graff RG, Florentine MF, Lacina S, Moore WD (1988): Scalp and limb defects with cutis
marmorata telangiectatica congenita: Adams-Oliver syndrome? Am J Med Genet 29:269-276.
Edited by John M. Opitz and James F. Reynolds
Genet 3:35-41.
13:466468.