Embed Size (px)
Citation preview
Connecting CareOur story so far…
Andy Kinnear June 2015
• What is Connecting Care?• Connecting Care – Why?
– Local drivers– National drivers
• Who the partners are• What we have delivered so far
– What are the benefits? • What can Connecting Care offer & what’s coming next• How our Governance framework works• How Connecting Care fits with the national strategy• Kinnear’s 5 key messages!!
introduction to Connecting Care
Connecting Care is the Bristol, North Somerset and South Gloucestershire [BNSSG] programme, dedicated to using technology to support -• Better information sharing between local
health and social care organisations• Joining up information to ensure care is
focused around the individual and their needs• Improving better, safer and more joined-up
care• Supporting increased efficiency in the delivery
of health and social care services• Ensuring that the people who are providing
care have the information they need, when they need it
what is Connecting Care?
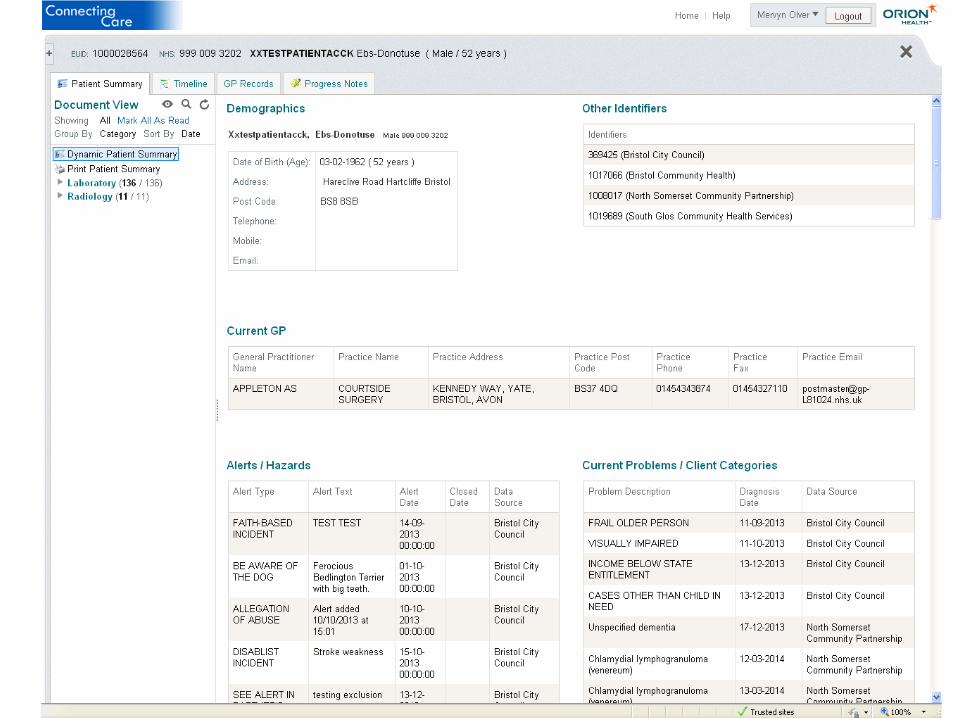
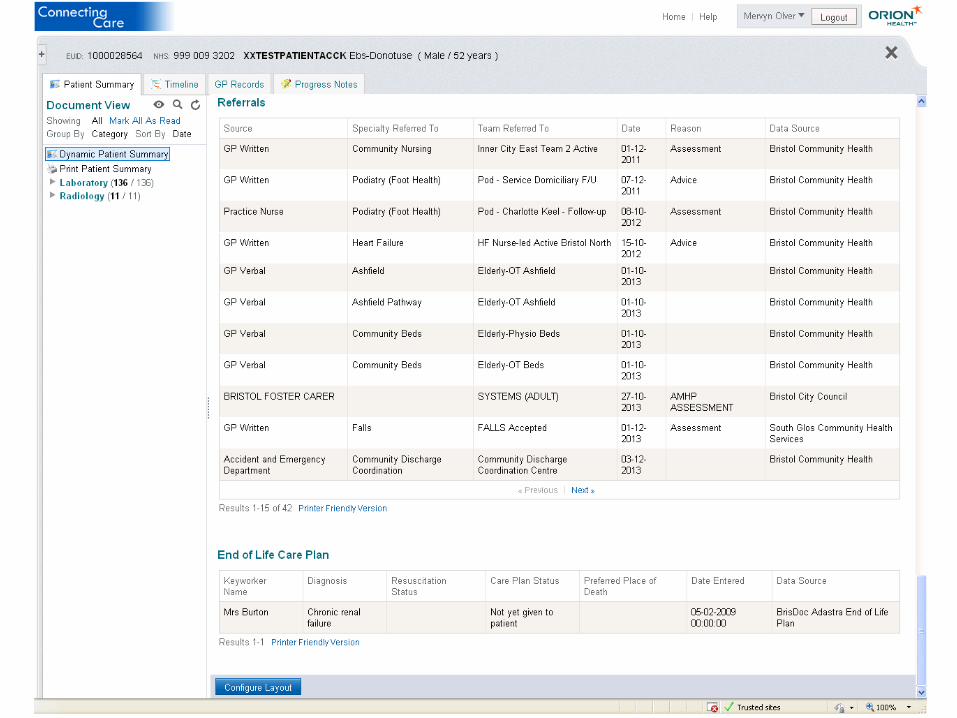
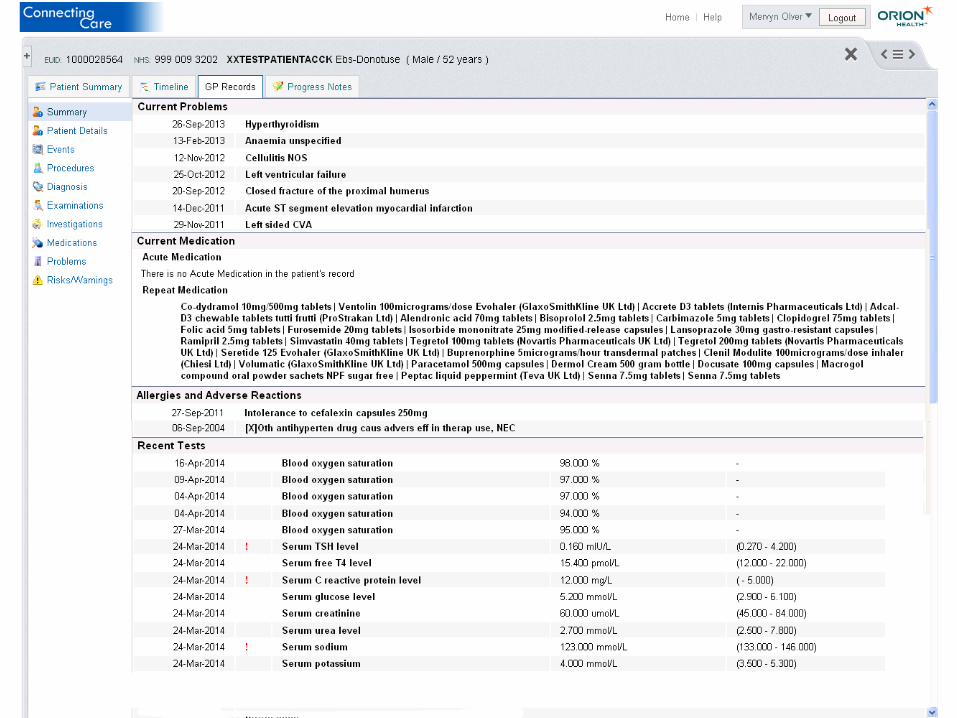
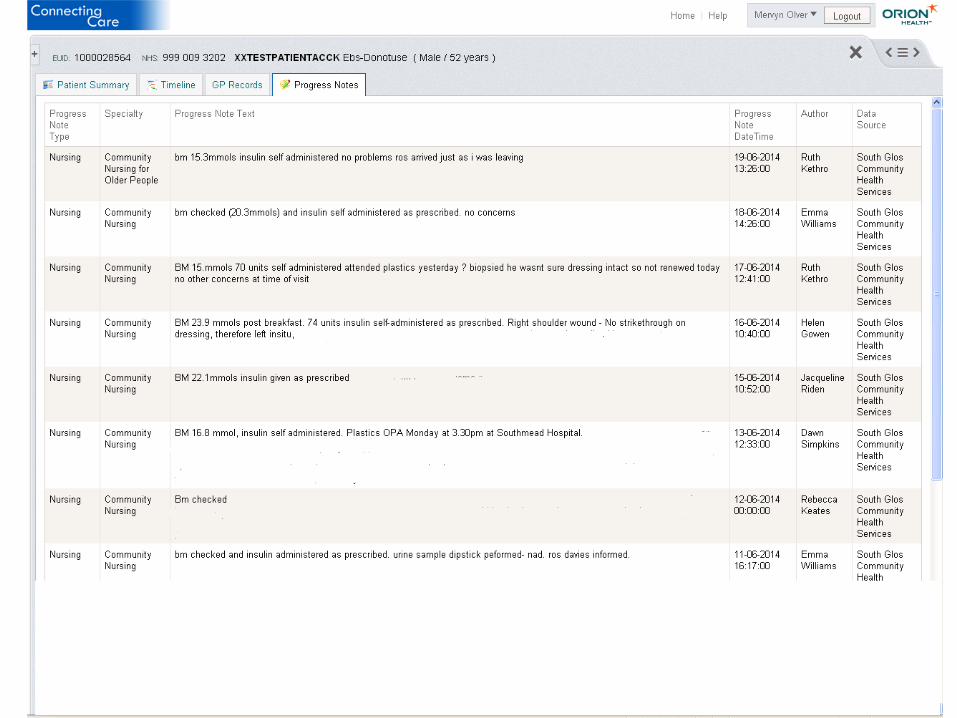
Our first focus has been the delivery of a shared ‘view only’ electronic patient record (a ‘portal’ sharing our IDCR)
local need
“Adequate and timely information must be shared between services whenever there is a transfer of care between individuals or services.”
“Services in all settings including health and social care need to improve their communication and handover ”
“The information I have is limited and frequently is missing important elements…”
“Better information would support better safeguarding”
“I don’t have access to some important information electronically…”
“If I had better information then it would help me evaluate risks when deciding whether to admit a patient…” “There are delays in getting
hold of information that I need…and I spend a lot of time chasing it up…”
*Summarised from feedback from local clinicians & practitioners during workshop events
NOT having access to accurate, timely, shared information
is a ‘blocker’ to providing high-
quality, effective, efficient care…
“There needs to be better communication between ‘in-hours’ and out of hours services.”
national drivers
Royal College of Physicians’ “We must
revolutionise the way we use information. We
must create pathways in which information
moves with patients across the system in real-
time”
Victoria Climbié (The Laming Report):
“...systems were crude and information failed to
be passed...information systems that depend on
the random passing of slips of paper have no
place in modern services”
Caldicott 2:“For the purposes of direct care,
relevant personal confidential data should be
shared among the registered and regulated health
and social care professionals who have a
legitimate relationship with the individual.”
Caldicott 2: “people also expect professionals
to share information with other members of the
care team, who need to co-operate to provide a
seamless, integrated service. …”
DoH Winterbourne View Final Report:
“All local authorities and their local safeguarding partners should
ensure they have...information-sharing processes in place across
health and social care to identify and deal with safeguarding...this
requires a multi-agency approach including all partners”

strategic alignment
5 year forward view: “Most countries have been slow to recognise and capitalise on the opportunities presented by the information revolution……the NHS has oscillated between two opposite approaches to information technology adoption.....the result has been
systems that don’t talk to each other and a failure to harness the shared benefits that come from interoperable systems…..In future we intend to take a different approach”

Connecting Care partnership
project approach
• 2011 Vision• 2012 Procurement • 2013 Staged approach
– First stage (pilot) started in March 2013. Key deliverables:
• A working system for 500 users• Evaluation of benefits • Stage one themed on urgent & unplanned care
• 2014 A business case for the second stage .Second stage started Dec 2014 (next 5-7 years)
FYFV PUBLISHED• 2015 = GROWTH
Stage two will extend the breadth & depth (10,000 more users, more information sharing)
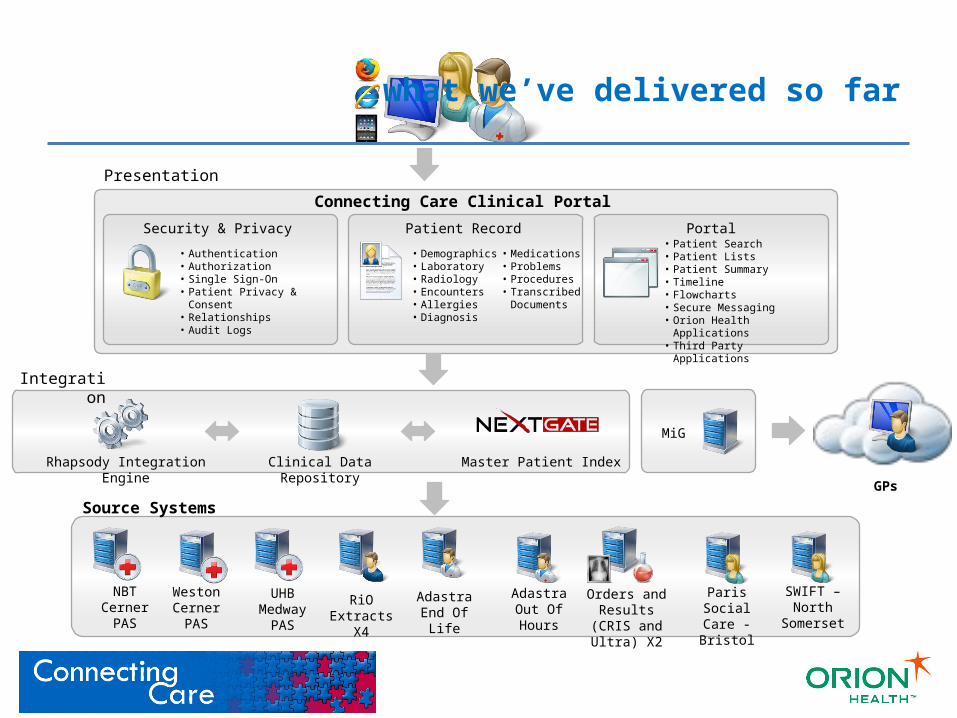
• Demographics• Laboratory• Radiology• Encounters• Allergies• Diagnosis
Clinical Data RepositoryRhapsody Integration Engine
Orders and Results (CRIS and Ultra) X2
GPs
RiO Extracts
X4
• Authentication• Authorization• Single Sign-On• Patient Privacy & Consent• Relationships• Audit Logs
• Patient Search• Patient Lists• Patient Summary• Timeline• Flowcharts• Secure Messaging• Orion Health Applications• Third Party Applications
Presentation
Integration
Source Systems
Security & Privacy Patient Record
• Medications• Problems • Procedures• Transcribed
Documents
Portal
Connecting Care Clinical Portal
Master Patient Index
MiG
NBT Cerner
PAS
Weston Cerner
PAS
Adastra End Of
Life
SWIFT – North
Somerset
UHB Medway
PAS
Adastra Out Of Hours
Paris Social Care - Bristol
what we’ve delivered so far
benefits approach
The backdrop - the scope & theme of the
pilot
The hypothesis & a framework for assessing
benefits
A detailed methodology
and plan
Capture and review
Analyse and reflect
The backdrop: scope and theme of the pilot
• Theme of ‘urgent and unplanned care’
• 500 licences, shared across all partner organisations teams
The hypothesis and framework used
• ‘Better sharing of information and better integrated information should have a positive effect on the quality, efficiency and cost of providing care’
• Framework based on MSP
A detailed methodology and plan
• Benefits realisation plan
• Based on Quality, Innovation, Productivity and Prevention (QUIPP) themes
The main benefits for me (as a clinician or social care professional) are:
• Confidence in my decision making is improved
• The quality of my consultation (or assessment) is improved
• I do not make unnecessary referrals or carry out duplicate assessments
• It saves me time (which can be used to provide care, or for other duties)
• I am more informed before a visit/appointment, which means I can provide more timely/more appropriate care
• I have better relationships with colleagues
• My input into a patient/service user’s care can be seen by others, so the recognition of my profession is increased
Connecting Care - benefits
The main benefits for my patients/service users are:
• They don’t have to keep telling their story (e.g. remembering / explaining medications
• They receive safer, more appropriate care
• They have a better experience of the services offered, potentially with fewer duplications or delays
• They might not have to be admitted to hospital
Connecting Care - benefits
Connecting Care - benefits
Out of hours care
• Saves appointments and visits• Saves admissions• Safer prescribing• Improved quality of consultation
Pharmacy • Safer prescribing – provides access to allergy and GP prescribing information
• Saves time – Reduces the amount of time calling GP practices • Safer communication – reduces errors
Hospitals / A&E
• Safer care – patient background, context and medications• Saves time – reduces time trying to find out information• Reduces risks – where patients unable to inform clinicians about
relevant information / fax errors etc
Connecting Care - benefits
Community care
• Saves time in triage and assessment • Saves time – reduces the amount of calls to GPs • Saves unnecessary home visits • Supporting risk management and safeguarding
Social care • Supporting referral management• Saves time in triage and assessment• Informs assessments & care planning • Saves installation and equipment costs• Supports risk management and safeguarding
General practice
• Reduces burden on practice administrators • Supports risk management and safeguarding• Increased confidence in better care being provided outside of the
practice• Immediate access to GP records (new registrations)
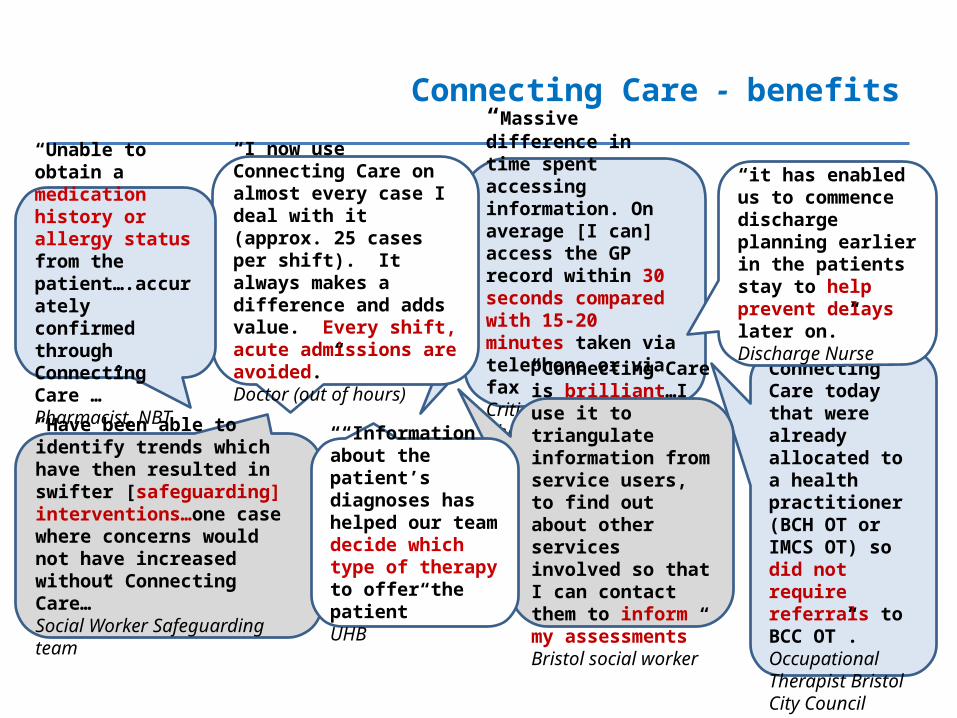
Connecting Care - benefits
“Massive difference in time spent accessing information. On average [I can] access the GP record within 30 seconds compared with 15-20 minutes taken via telephone or via fax” Critical Care Pharmacist Manager UHB “3 cases identified
on Connecting Care today that were already allocated to a health practitioner (BCH OT or IMCS OT) so did not require referrals to BCC OT”. Occupational Therapist Bristol City Council
“I now use Connecting Care on almost every case I deal with it (approx. 25 cases per shift). It always makes a difference and adds value. Every shift, acute admissions are avoided.” Doctor (out of hours)
“Have been able to identify trends which have then resulted in swifter [safeguarding] interventions…one case where concerns would not have increased without Connecting Care…”Social Worker Safeguarding team
“Connecting Care is brilliant…I use it to triangulate information from service users, to find out about other services involved so that I can contact them to inform my assessments” Bristol social worker
“it has enabled us to commence discharge planning earlier in the patients stay to help prevent delays later on.”Discharge Nurse
“Unable to obtain a medication history or allergy status from the patient….accurately confirmed through Connecting Care …” Pharmacist, NBT
““Information about the patient’s diagnoses has helped our team decide which type of therapy to offer the patient” UHB
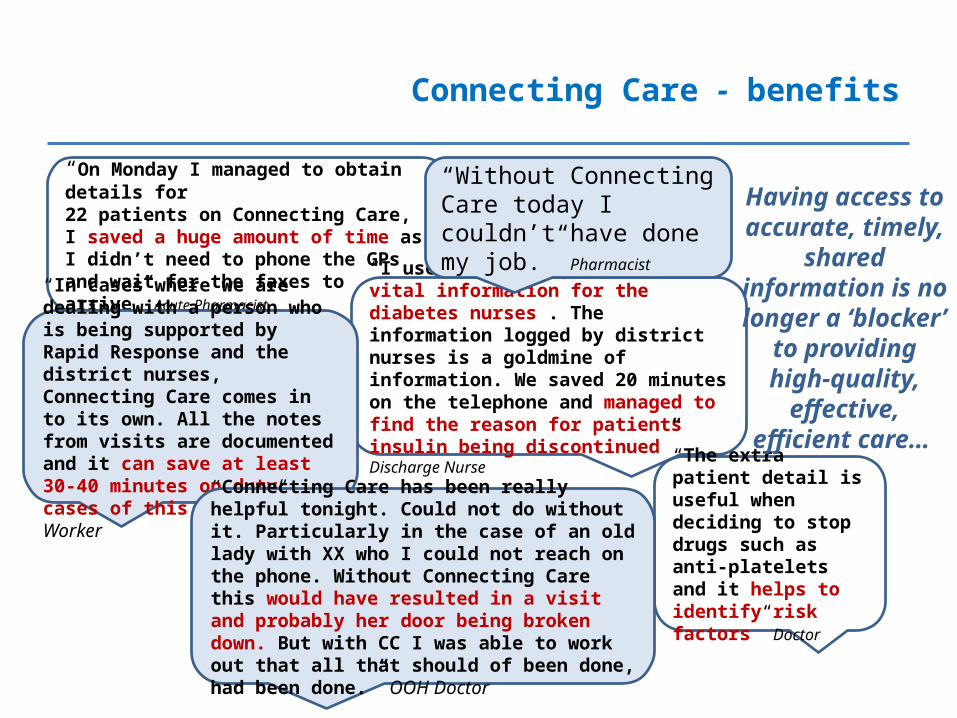
Connecting Care - benefits
“On Monday I managed to obtain details for 22 patients on Connecting Care, I saved a huge amount of time as I didn’t need to phone the GPs and wait for the faxes to arrive” Acute Pharmacist
“I used Connecting Care to find vital information for the diabetes nurses . The information logged by district nurses is a goldmine of information. We saved 20 minutes on the telephone and managed to find the reason for patients insulin being discontinued” Discharge Nurse
“In cases where we are dealing with a person who is being supported by Rapid Response and the district nurses, Connecting Care comes in to its own. All the notes from visits are documented and it can save at least 30-40 minutes on duty cases of this nature” Social Worker “The extra patient detail
is useful when deciding to stop drugs such as anti-platelets and it helps to identify risk factors” Doctor
Having access to accurate, timely,
shared information is no longer a
‘blocker’ to providing high-
quality, effective, efficient care…
“Without Connecting Care today I couldn’t have done my job.” Pharmacist
“Connecting Care has been really helpful tonight. Could not do without it. Particularly in the case of an old lady with XX who I could not reach on the phone. Without Connecting Care this would have resulted in a visit and probably her door being broken down. But with CC I was able to work out that all that should of been done, had been done.” OOH Doctor
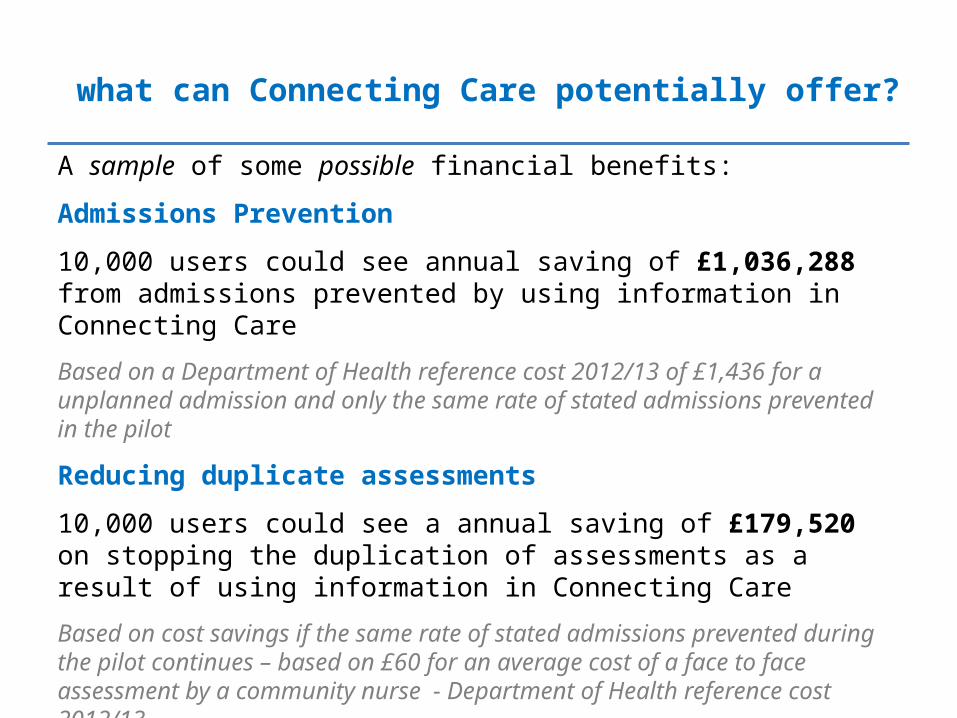
A sample of some possible financial benefits:
Admissions Prevention
10,000 users could see annual saving of £1,036,288 from admissions prevented by using information in Connecting Care
Based on a Department of Health reference cost 2012/13 of £1,436 for a unplanned admission and only the same rate of stated admissions prevented in the pilot
Reducing duplicate assessments
10,000 users could see a annual saving of £179,520 on stopping the duplication of assessments as a result of using information in Connecting Care
Based on cost savings if the same rate of stated admissions prevented during the pilot continues – based on £60 for an average cost of a face to face assessment by a community nurse - Department of Health reference cost 2012/13
what can Connecting Care potentially offer?
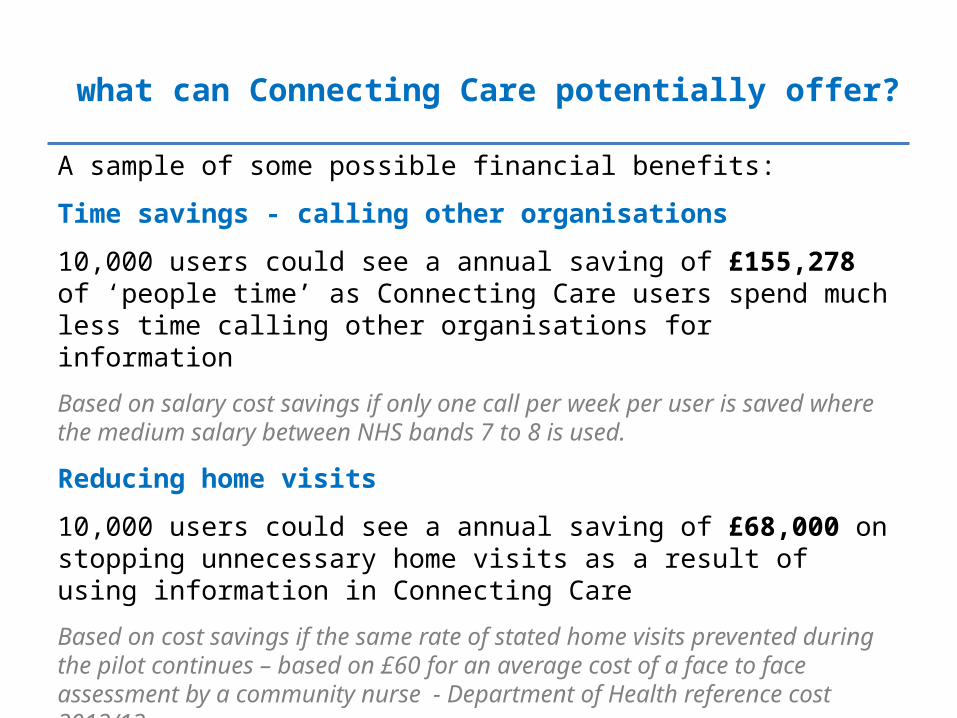
A sample of some possible financial benefits:
Time savings - calling other organisations
10,000 users could see a annual saving of £155,278 of ‘people time’ as Connecting Care users spend much less time calling other organisations for information
Based on salary cost savings if only one call per week per user is saved where the medium salary between NHS bands 7 to 8 is used.
Reducing home visits
10,000 users could see a annual saving of £68,000 on stopping unnecessary home visits as a result of using information in Connecting Care
Based on cost savings if the same rate of stated home visits prevented during the pilot continues – based on £60 for an average cost of a face to face assessment by a community nurse - Department of Health reference cost 2012/13
what can Connecting Care potentially offer?
what’s next?
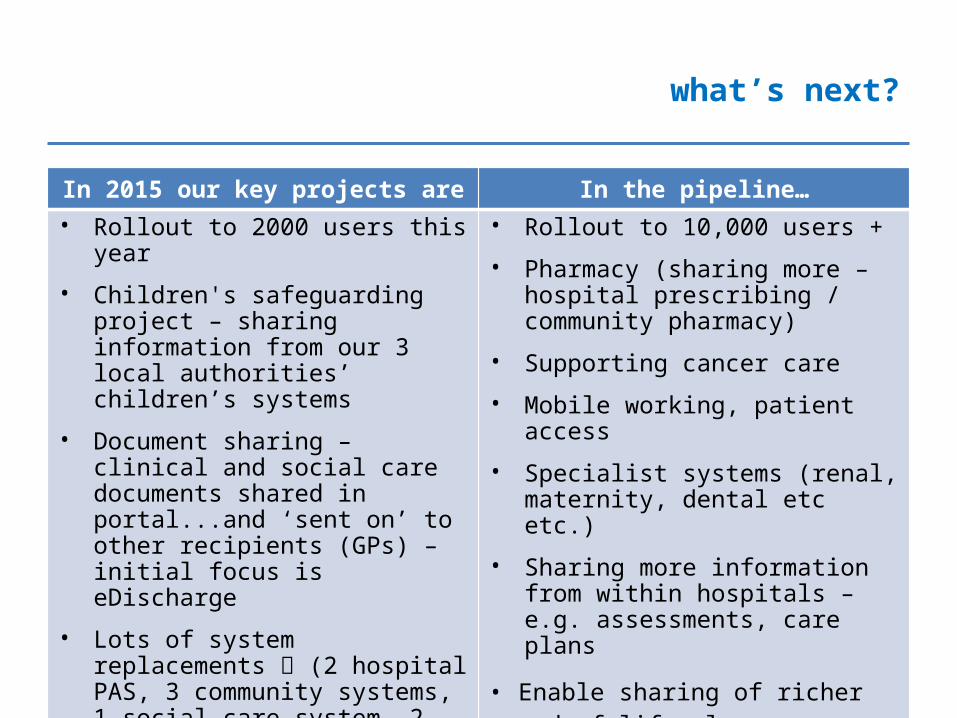
In 2015 our key projects are In the pipeline…
• Rollout to 2000 users this year• Children's safeguarding project –
sharing information from our 3 local authorities’ children’s systems
• Document sharing – clinical and social care documents shared in portal...and ‘sent on’ to other recipients (GPs) – initial focus is eDischarge
• Lots of system replacements (2 hospital PAS, 3 community systems, 1 social care system, 2 pathology systems)
• New infrastructure, new data centre with UHB hosting, re-write lots of our ‘core config’ to support improved performance
• Rollout to 10,000 users + • Pharmacy (sharing more – hospital
prescribing / community pharmacy)• Supporting cancer care• Mobile working, patient access • Specialist systems (renal, maternity,
dental etc etc.)• Sharing more information from within
hospitals – e.g. assessments, care plans
• Enable sharing of richer end of life plans
• Better support for some workflow / pathways
• And lots and lots more!!
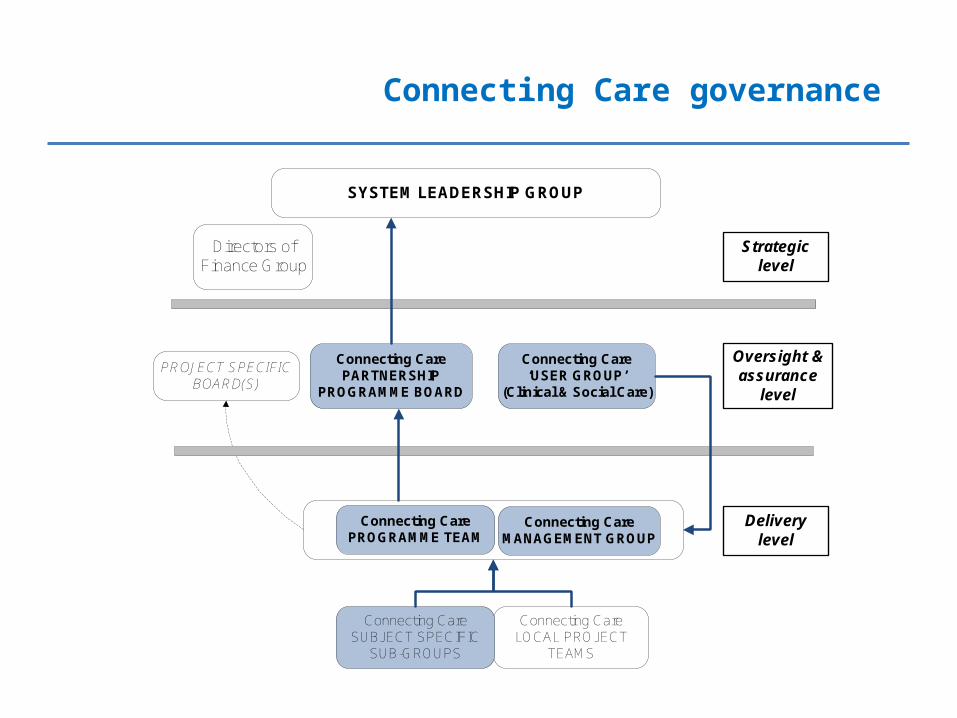
Connecting Care governance
SYSTEM LEADERSHIP GROUP
Connecting Care MANAGEMENT GROUP
Connecting Care PARTNERSHIP
PROGRAMME BOARD
Connecting Care ‘USER GROUP’
(Clinical & Social Care)
PROJECT SPECIFIC BOARD(S)
Connecting Care PROGRAMME TEAM
Connecting Care LOCAL PROJECT
TEAMS
Directors of Finance Group
Strategic level
Oversight & assurance
level
Delivery level
Connecting Care SUBJECT SPECIFIC
SUB-GROUPS
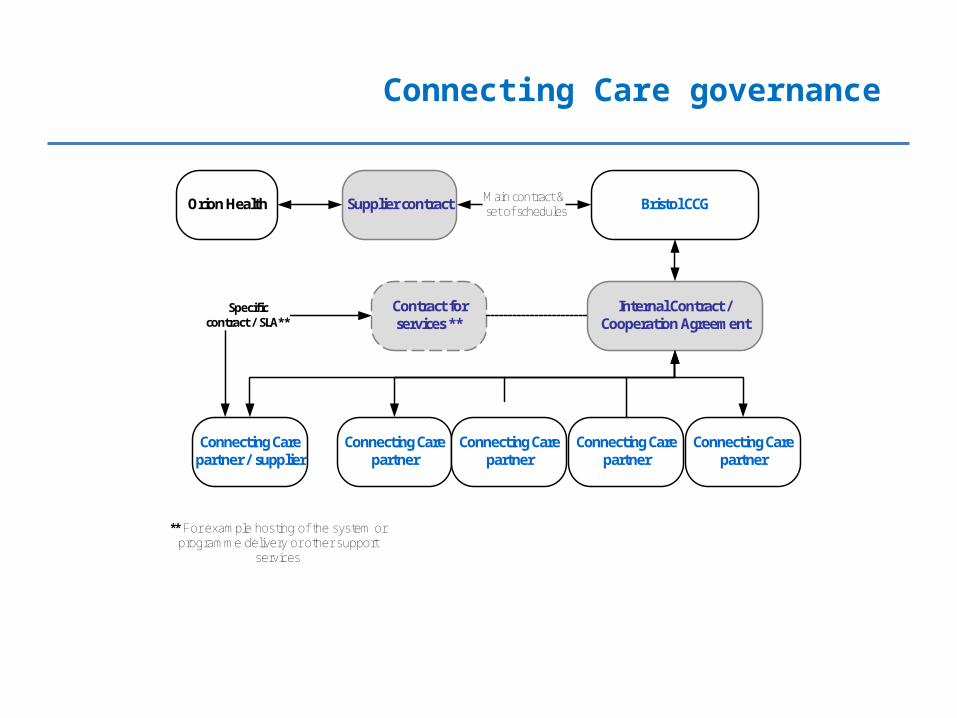
Connecting Care governance
Bristol CCG
Connecting Care partner
Internal Contract / Cooperation Agreement
Orion Health Main contract & set of schedules
Connecting Care partner
Connecting Care partner
Connecting Care partner
Contract for services **
Supplier contract
Connecting Care partner / supplier
Specific contract / SLA**
** For example hosting of the system or programme delivery or other support
services
How does it fit with national strategy?
Connecting Care

strategic alignment
5 year forward view: “Most countries have been slow to recognise and capitalise on the opportunities presented by the information revolution……the NHS has oscillated between two opposite approaches to information technology adoption.....the result has been
systems that don’t talk to each other and a failure to harness the shared benefits that come from interoperable systems…..In future we intend to take a different approach”
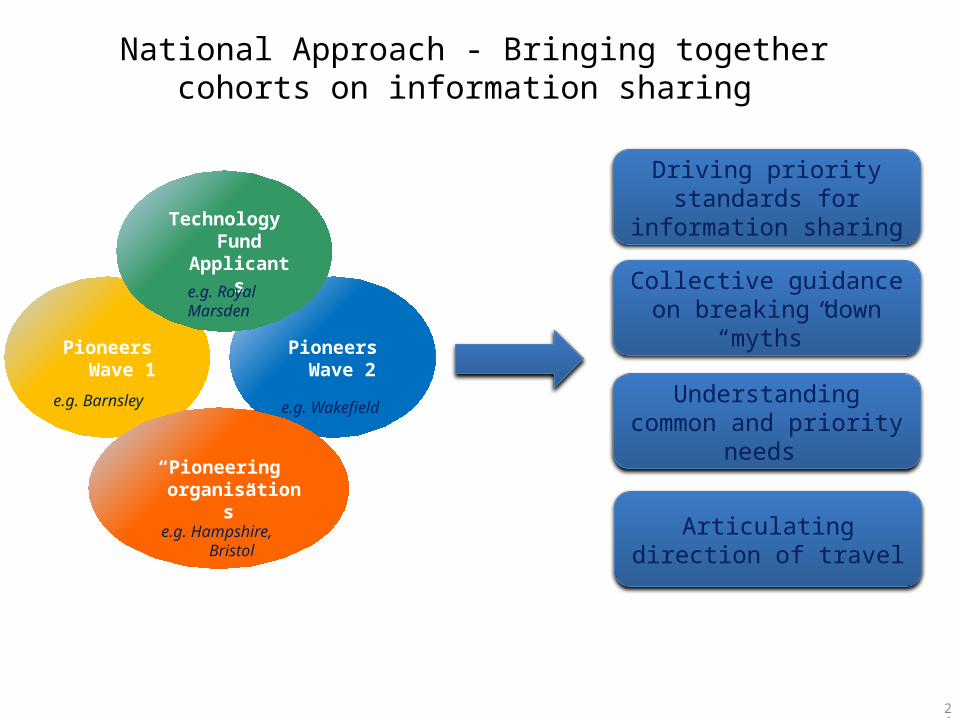
National Approach - Bringing together cohorts on information sharing
Pioneers Wave 1
Pioneers Wave 2
Technology Fund Applicants
“Pioneering organisations”
e.g. Hampshire,
Bristol
e.g. Royal Marsden
e.g. Wakefielde.g. Barnsley
Driving priority standards for information sharing
Collective guidance on breaking down “myths”
Understanding common and priority needs
Articulating direction of travel
24
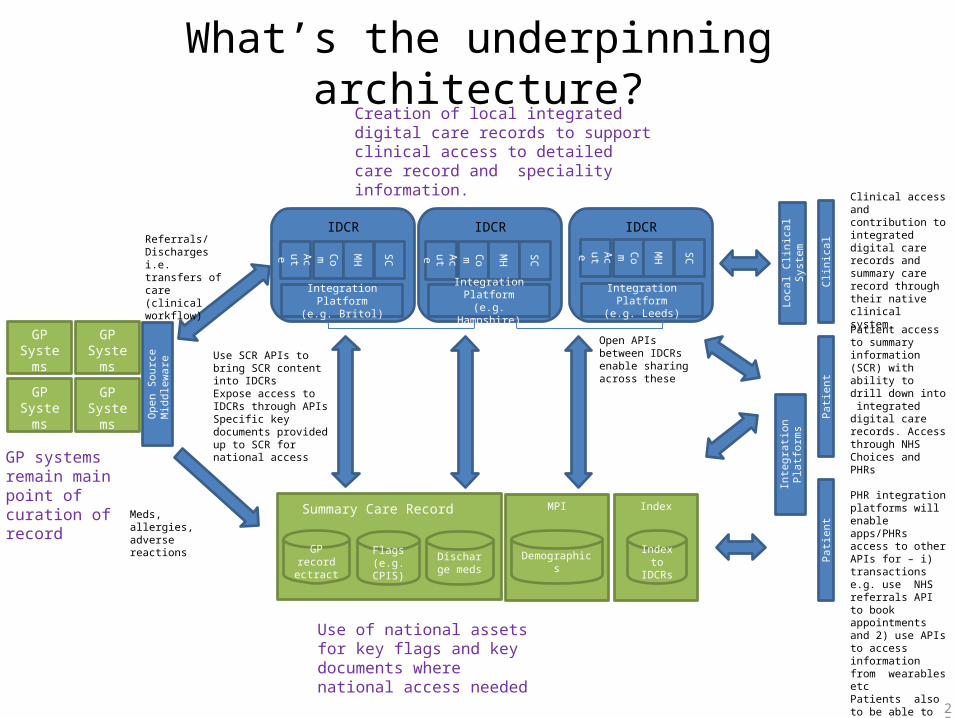
What’s the underpinning architecture?
Creation of local integrated digital care records to support clinical access to detailed care record and speciality information.
Use of national assets for key flags and key documents where national access needed
IDCRIDCRIDCR
Clin
icalAcu
te Com MH
SC
GP Systems
GP systems remain main point of curation of record
Acute Com M
H
SC
Acute Com M
H
SC
Integration Platform(e.g. Britol)
GP Systems
GP Systems
GP Systems
Referrals/Discharges i.e. transfers of care(clinical workflow)
GP record ectract
Flags (e.g. CPIS)
Discharge meds
Summary Care RecordMeds, allergies, adverse reactions
MPI
Demographics
Integration Platform(e.g. Hampshire)
Integration Platform(e.g. Leeds) Lo
cal C
linic
al S
yste
m
Patie
nt
Inte
grati
on P
latfo
rms
Use SCR APIs to bring SCR content into IDCRsExpose access to IDCRs through APIs Specific key documents provided up to SCR for national access
Clinical access and contribution to integrated digital care records and summary care record through their native clinical system.
Index
Index to IDCRs
Patie
nt
Patient access to summary information (SCR) with ability to drill down into integrated digital care records. Access through NHS Choices and PHRs
PHR integration platforms will enable apps/PHRs access to other APIs for – i) transactions e.g. use NHS referrals API to book appointments and 2) use APIs to access information from wearables etc Patients also to be able to contribute to PHRs
Open APIs between IDCRs enable sharing across these
Ope
n So
urce
M
iddl
ewar
e
25
KINNEAR’S - 5 reasons we have been successful…..
1. Line of business systems that ‘share’
• You cannot share paper data easily• Good electronic ‘line of business’ systems that share
data are critical
2. Integration Partner • Integration is tricky. Find a software partner who ‘gets it’
3. Money…locally owned money!
• Invest locally….seek national money too, but make your local organisations put skin in the game
4. People….local talented people
• Hire really talented project people….we did, we do, we always will
5. SPIRIT • Overrides everything else• Stamp on ‘organisationally centric’ thinking at every
single opportunity. • Command the morale high ground that the
patients/citizens best interest occupies
• What is Connecting Care?• Why have Connecting Care?
– Strategic alignment - UHB– National drivers
• Who are the partners?• What have we delivered so far? • What are the benefits? Tangible results so far• What can Connecting Care offer & what’s coming next?• Governance Framework
Thank you for your time!
summing up
what does it look like?



















![Milestones and the CCC handout - Kinnear [Read-Only]](https://img.pdfslide.net/doc/110x75/61a24c67a4e32f2697749798/milestones-and-the-ccc-handout-kinnear-read-only.jpg)









