Embed Size (px)
Citation preview

Constipation and catharsisW. Grant Thompson,* md
Constipation is endemic in the Westernworld. Stool consistence and associatedsymptoms are more important thanstool frequency. The patient's attitudetowards his bowel habit is alsoimportant. Exclusion of "organic"disease, reassurance and discussionof normal variations of bowel habit are
necessary first steps in treatment.Adequate bulk in the stool must beensured, either through diet or
bulking agents, and bowel retrainingattempted. Laxatives should bereserved for episodes of constipationfollowing enforced bedrest, or as a
preparation for diagnostic procedures.Long-term use should be avoided.
La constipation est endemique dans lemonde occidental. La consistance desselles et les symptdmes associessont plus importants que la frequencede la defecation. L'attitude dupatient a I'egard de ses habitudesde defecation est aussi importante.Apres avoir elimine la possibilited'une cause organique, lespremieres etapes necessaires au
traitement consistent a rassurer lepatient et a discuter avec lui desvariations normales des habitudes dedefecation. On doit assurer un volumede selles adequat, par le regimealimentaire ou a I'aide d'agentsmucilagineux, et une reeducation deshabitudes de defecation doit etretentee. Les laxatifs doivent etrereserves aux episodes de constipationtels ceux qui suivent les periodesd'alitement forcees, ou a la preparationpour les tests de diagnostic. Leurutilisation en traitement prolongedoit etre evitee.
?Associate professor of medicine, Universityof Ottawa; gastroenterologist, Ottawa CivicHospitalReprint requests to: Dr. W.G. Thompson,lst link, Ottawa Civic Hospital, Ottawa, ONKIY 4E9
Of the beliefs handed down to us byour forefathers, the concept of regu-larity is among the most enduring.Since antiquity an empty colon hasbeen equated with purity; and whatgenerations of mothers have cherished,let no man put asunder. Nevertheless,there is a logical approach to "con-stipated" patients, and physiciansshould be firm in their convictions,which, in turn, should be based on
science, not fantasy.The definition of constipation is elu-
sive. The world's record for rectal con¬tinence is held by a man who resistedthe temptations of the toilet for 368days.1 He is said to have become weakafter delivering 36 / of feces on June21, 1901, but "there was much rejoic-ing in the family". Statistically the"normal population" has from threebowel movements per week to three a
day.2 The 1% of individuals who failoutside that range are unusual but notnecessarily abnormal. It is probable thatthe actual frequency of motions is notrelevant, although it may be of greatconcern to the patient. More importantare the consistence of the stool andassociated symptoms.
Pathophysiologic considerations
There are two modes of colonicmotor activity.3 The first is propulsivecontractions or mass movements, longrecognized by radiologists. These peri¬staltic rushes are more frequent in diar¬rhea than in constipation. The othermode is segmental or nonpropulsive ac¬
tivity, which appears to have a mixingand braking function. Such activitytends to be decreased in diarrhea andincreased in some patients with con¬
stipation. Segmentation that succeeds inisolating part of the colon from theremainder may generate very high pres¬sures and result in proximal dilatationor diverticula formation.
In the spastic type of irritable colonsyndrome the stool is hard, scybalousand often associated with lower abdom¬inal pain.4 These symptoms relate toexcessive segmental contraction of thelower colon and rectum, and the in¬dividual subsequently has a feeling ofincomplete evacuation. Constipationmay alternate with periods of diarrhea.Hemorrhoids and fissures may com-
plicate the passage of stony stools. Lesscommonly, obstipation may result froman atonic, lax colon, in which pro¬gressive peristaltic activity is decreased,a condition characterized by Sir ArthurHurst as dyschezia.5 This may occur
spontaneously but is also seen follow¬ing chronic abuse of laxatives.
Constipation may result from a widevariety of local and systemic condi¬tions. Perianal disorders such as fis¬sures or localized proctitis may lead toconscious or subconscious defence ofthe area by the withholding of stool.Cancer of the colon, diverticular dis¬ease and volvulus are causes of a re¬cent change in bowel habit and mustbe rigorously excluded. In hypothyroid-ism or dehydration, appropriate re¬
placement therapy may be curative.Many drugs, including codeine, some
antihypertensive agents, iron, aluminumand calcium compounds, are constipat-ing. Inactivity, such as that followingsurgery, or travel, especially withchange in time zones, may induce thisdistressing nuisance, and it is a frequentconsequence of pregnancy and of oldage. Endogenous depression often pro¬duces constipation, which may im¬prove with antidepressant therapy.Parents reward their children for asuccessful bowel action and imbue inmany the idea that daily movementsare essential for cleanliness or purity.Psychoanalysts have attributed repres-sion of defecation to anal eroticism. Ifthe patient is an unmarried girl it issaid that marriage may effect a cure.®
CMA JOURNAL/MAY 22, 1976/VOL. 114 927

I know of no controlled trials to sub-stantiate this.
Constipation, like the irritable colon,diverticular disease and appendicitis, isa disease of Western civilization, ap¬parently attributable to our low-fibre,refined diet.7 It has been demonstratedthat the daily stool weight in Englishsubjects is one third that of Africansliving under native conditions on an
unrefined diet.8 The transit time of thebulky African stool is less than halfthat of the British. It would appear thatour colons have not had time to adaptto the fibre-free, low-bulk stool that hasresulted from the refined diet adoptedover the past century. Thus, partiallyfilled colons can generate very high seg¬mental pressures, accounting for thepain and constipation of the spasticcolon. Peristaltic activity is disorderedand the patient may have an increasedtransit time. In individuals who are
given 20 g of unprocessed bran daily,the stool bulk is significantly increasedby water entrapped in the interstices ofthe dietary residue.9 Such treatmentspeeds up transit in those in whom itwas slow and, paradoxically, slows tran¬sit in those in whom it was rapid. Inother words, increased dietary bulknormalizes colon motility.9,10 Coarsebran is more effective than fine becauseof the former's greater water-holdingcapacity.11The individual with constipation may
complain of foul breath, furred tongue,anorexia, flatulence, headache, irritabil-ity, insomnia, and so on. These were
once considered manifestations of auto-intoxication.12 Proponents of this con¬
cept held that poisons were elaboratedin the gut as a result of constipation.In one experiment, however, fivehealthy men were required to eat nor¬
mally but refrain from defecation for90 hours.13 Each man complained ofthe above symptoms and experiencedimmediate relief when the situation was
reversed by an enema. Such promptrelief seems to militate against toxemia,and the symptoms are now believed tobe due to distension and mechanicalirritation of the rectum. In fact, masses
of cotton wool packed into the rectumproduce identical effects.1213 Many in¬dividuals whose colons may be emptymay incorrectly blame such common
symptoms on constipation, and on thisbasis indulge in excessive purgation.
There is no doubt that constipationis distressful. Empires have trembled atthe prospect of doing without purga-tives. In an exercise of pharmacologicwarfare Britain placed an embargo on
the export of purgatives to Napoleon-controlled Europe.14 This strategy was
expounded by one Sydney Smith:
What a sublime thought that no purge
can now be taken between the Weserand the Garonne; that the bustling pestleis still, the canorous mortar mute, andthe bowels of men locked up for fourteendegrees of latitude .... Without castor oilthey might for some months, to be sure,have carried on a lingering war; but whatcan they do without bark [cascara]?14
InvestigationOrganic disease must be excluded.
This demands careful history-takingand physical examination and, at least,sigmoidoscopy.15 Most patients shouldhave a barium enema examination andan estimation of hemoglobin concen¬tration. Recent onset of constipationdemands rigorous exclusion of localand systemic disease, particularly car¬
cinoma of the colon, hypothyroidismand depression. The patient's drug his¬tory should be carefully reviewed toensure that there is not a pharmaco¬logic cause for his symptoms.
Treatment
General measures
It is believed by many that exercisepromotes a normal bowel habit. Con-versely, enforced confinement to bed,such as after a coronary occlusion or a
fractured hip, is frequently associatedwith constipation, especially if the pa¬tient must grapple with pulleys andbedpans. Adequate fluid must also beensured. The chronically constipatedcolon may be retrained. This is bestachieved by using natural reflexes toadvantage. It is recognized that theresting colon may be spurred into ac¬tion by a meal, particularly breakfast.Many individuals insist that theirbowels function only following theircustomary morning coffee or cigarette,although whether this effect is pharma¬cologic, physiologic or psychologic isuncertain. The regular post-breakfast re¬
tirement with a good book to the relax-ing solitude of the bathroom may havea salutary effect. It is said that a lowtoilet seat results in a squatting posi¬tion, which is more favourable for def¬ecation. Certainly a draughty outhousein January is no place to commence theexercise. To initiate the habit in thoseaccustomed to taking laxatives it maybe necessary to use an enema for thefirst while. A glycerine suppository,while inactive pharmacologically, mayset in motion the defecation reflex. Pa¬tient attention to such details, alongwith the use of bulking agents as de¬scribed below, may restore even themost recalcitrant colon to normalcy.
Bulking agentsDietary fibre is described as "unavail-
able carbohydrate" and includes cel¬
lulose, hemicellulose and lignin.16 Inaddition to its hydrophilic bulking prop¬erties fibre may have a cathartic effectdue to the volatile fatty acids releasedby bacterial metabolism. Since there ismuch evidence that deficiency of fibreor bulk is an important factor in con¬
stipation, it seems reasonable to in¬crease the intake of fibre by constipatedpatients.17 As Cleave7 forcefully states,this means less refined sugar and flour,and more natural fruits and whole-wheat products. Bran has long beenrecognized as an effective laxativeand this has had scientific confirma-tjon 9,10,18,19 MiUer's bran> 6 tQ 1Q tea.spoonfuls (12 to 20 g) per day, is a
cheap and effective laxative.9'10'16,18Coarse bran has been shown to havea greater water-holding capacity thanbran made finer by milling;11 this ac¬counts for the greater effectiveness ofthe former in improving transit time.The resourceful patient may improvepalatability of this material by addingit to cereals, sauces, meat loaves andother foods. Liberal use of whole-wheatbread, breakfast cereals and fresh fruitsand vegetables may assist in providingextra bulk.
Since bran in therapeutic quantitiesis inconvenient, many physicians nowprescribe bulking agents. The most sa¬
tisfactory of these is psyllium hydro¬philic mucilloid (Metamucil, Hydrocil).This is useful for preventing constipa¬tion and other manifestations of theirritable colon syndrome, as an adjunctto the therapy of perianal disease, andin the prevention, not the treatment, ofacute diverticulitis. It is superior tomethylcellulose for this purpose.20 Theappeal of the use of bulking agents istheir almost complete lack of side ef¬fects, although impaction is a potentialhazard if they are given to patients withunderlying obstructing lesions.21 Meta¬mucil contains dextrose as a dispersingagent and is best taken in juice, 1 to 3teaspoonfuls three times a day withmeals. Some patients have transientbloating with the commencement oftherapy, but the dose may be adjustedto achieve a stool that is formed .neither loose and watery, nor stony andfragmented. For patients who are fussythere is an expensive flavoured prepa¬ration.To understand better how psyllium
exerts its effect, one can perform thefollowing simple experiment. In a med¬icine glass place 5 ml of the psylliumpowder. Add water to make up a totalof 30 ml. Stir and allow to stand fora few minutes. You will notice that asoft gel forms in the glass. In the colonthis gelling action may soften a hard,marble-like stool or firm a watery one.The added bulk promotes normal peri¬stalsis.
928 CMA JOURNAL/MAY 22, 1976/VOL. 114

Anticholinergics
Anticholinergic drugs have a greateraction on the segmenting or brakingcontractions of the colon than on peri¬stalsis.22 Thus, they may be of use intreating colonic spasm when it mani-fests itself as abdominal pain.23 Anti¬cholinergics achieve an effect on thecolon only in doses that cause sideeffects such as tachycardia and drymouth. Further, they may aggravatecolonic stasis and lead to drying ofthe stool.24 Dicyclomine hydrochloride(Bentylol) is said to have a specificeffect on smooth muscle with less effecton secretion.25 If this were true it wouldbe the best antispasmodic to use. Other¬wise, synthetic agents offer no practicaladvantages over atropine, are expensiveand are poorly absorbed from the gut.It is therefore a sad comment thatatropine preparations to be taken orallyare not available in Canada. Antichol¬inergics have very little applicability inconstipation and should be tried onlyin cases in which abdominal pain pre¬sumably due to colonic segmentalspasm is not controlled by bulkingagents. Patients who have postprandialpain due to an exaggerated "gastro-colic" reflex may occasionally benefitfrom the administration of an effectivedose before meals.
Stool softenersStool softeners are used to lubricate
the stool and are often recommendedby surgeons for perianal disease. Thereare many reasons why mineral oil (li¬quid paraffin) should not be used. As¬piration (lipoid) pneumonia has beenreported in the elderly26'27 and in in¬fants.28 Mineral oil is a solvent for thefat-soluble vitamins A, D, E and K,and thus may interfere with their ab¬sorption.29'30 If used in patients withenteric fistulas it may interfere withhealing.31 Further, if used excessivelyit may actually cause incontinence, andoil leaking through the anal sphinctermay cause pruritis ani.32 Mineral oil haseven been blamed for gastrointestinalcancer. For these reasons mineral oilshould be banished from the marketplace.
Dioctyl sodium sulfosuccinate (DSS)is an anionic detergent, which, by low-ering surface tension, is thought to fa-cilitate penetration of the fecal mass
by water and fat.32 Like mineral oil itproduces its laxative effect by softeningthe stool, apparently through inhibitionof water absorption.34 This substanceshould be reserved for those situationsin which a stool softener is required fora short period that is, acute perianaldisease. DSS may facilitate the absorp¬tion of other normally unabsorbed laxa¬
tives and should not be used in drugcombinations.35
Chemical stimulants
Chemical stimulant laxatives can beused in relative safety provided they arenot abused. The diphenylmethane laxa¬tive phenolphthalein, originally intendedas a wine colouring, is present in manypatent medicines. Some of the dye isabsorbed and appears in the urine,which, if alkaline, may become pinkor red.36 It may undergo enterohepaticcirculation. The absorbed drug is be¬lieved to act directly on the muscle ofthe distal colon to stimulate peristalsis.37It acts within 6 to 8 hours after inges¬tion and is not inhibited by atropine.The usual dose is 200 mg. Even in 200times the usual dose it is remarkablynontoxic, although hypersensitivity re¬actions have been reported.38 Long-termuse and abuse, on the other hand, mayhave devastating effects (see below).Oxyphenisatin, a relative of phenolph¬thalein, has been associated with the de¬velopment of chronic active hepati¬tis.35'39"11 The responsible preparationcontained DSS, which may have facili-tated the absorption of oxyphenisatinand its transport to the liver.35 Bisa-codyl (Dulcolax) is the most useful ofthis series of drugs and can be giveneither as a suppository or by mouth.The enteric-coated tablet has no actionon the small bowel. If, however, thetablets are taken orally with an alkali,the coating may dissolve, allowing thedrug to act on the small bowel, causingunpleasant gastrointestinal symptoms.Bisacodyl does not work for 6 hoursor more following oral administration.It is therefore ideally given the nightbefore the desired morning evacuation.The suppository will have more promptaction, reflexly stimulating the wholecolon.42 The stimulant effect of thediphenylmethane cathartics is inhibitedby local anesthesia.43The anthracene glycosides include
senna and cascara and are more potentthan phenolphthalein.44 The mechanismof the catharsis effected by these orallyadministered drugs is due to direct ac¬tion on the submucosal nerve plexus inthe colon; the effect is blocked by priorapplication of local anesthetic.45 Sennais the active principle of liquorice pow¬der. The intact glycoside is ineffectivein the colon.45'46 When administeredorally it is apparently hydrolyzed bycolonic bacteria to release aglycones,which cause peristalsis of the trans¬verse and descending colon and de¬crease sigmoid segmentation,47 a pro¬cess that requires 6 to 8 hours. Agly¬cones are ineffective when adminis¬tered orally.45 Long-term use leads to a
peculiar pigmentation of the rectal mu¬
cosa called melanosis coli.48
Abuse of diphenylmethane and an¬thracene cathartics has been associatedwith a number of serious complications.Long-term use results in dependence ofthe bowel on these drugs for "success¬ful" function. In mice and in one wom¬an subjected to long-term administra¬tion of senna, damaged myentericneurons were demonstrated in thecolon.48 Thus, the patient may becomephysiologically and psychologically de¬pendent on continued purgation. A fre¬quent result is, paradoxically, diar¬rhea.49-52 For reasons best known tothemselves such patients may concealtheir laxative habit from the haplessphysician who is dutifully investigatingtheir copious diarrhea. A radiograph ofthe colon may show loss of haustrationsand smooth, tapering contractionsknown as pseudostrictures.49 In onesuch patient finger clubbing developed,which delayed recognition of purgativeabuse.53 The clubbing disappeared whenthe senna was withdrawn, only to re-
appear when purgative abuse was re-sumed. In these misguided patients thediagnosis of laxative abuse may onlybe confirmed by "locker search" orexamination of the urine for phen¬olphthalein or anthraquinone deriva¬tives.50'51'53 A further clue to laxativeabuse may be an associated hypokale¬mia,51'54'55 which may resemble hyper-aldosteronism.56 Malabsorption andprotein-losing enteropathy have alsobeen described.50-52
Saline cathartics
The saline cathartics consist of a
variety of magnesium and sodium salts.Their effect depends in part upon theirionization, osmotic effect and low ab-sorbability. There is also good evidencethat magnesium and sulfate ions in thegut cause secretion of cholecystokinin.57This hormone in turn stimulates intes¬tinal and colonic motility. Magnesiumsulfate (Epsom salt) is a commonlyused saline cathartic. It has a bitter,unpleasant taste but causes a semifluidevacuation in less than 3 hours whengiven in a dose of 5 to 15 g.43 It istherefore useful to rid the gut of bloodin patients with hepatic coma, of drugsin poisoning situations and of wormsafter administration of a vermifuge.Milk of magnesia (magnesium hydro¬xide), more often used as an antacid,is also a saline cathartic but has a
relatively mild action. Magnesium-con-taining salts should be given with cau¬tion to patients with impaired renalfunction. Sodium-based compoundsmay be taken orally, but the mostcommonly used sodium-containing sa¬line cathartic, sodium phosphate-bi-phosphate compound (Fleet), is avail¬able as an enema. This hyperosmolarsolution is available in small plastic
CMA JOURNAL/MAY 22, 1976/VOL. 114 929

containers. It is sometimes described asa "disposable enema", although one isunlikely to encounter an enema thatanyone would wish to keep. This prep-aration is most useful in fecal or bari-um impaction and in preparing therectum for sigmoidoscopy. A hyper-tonic or any other type of enema maycause mucosal irritation, which inter-feres with interpretation of sigmoido-scopic findings.58 Therefore, it is betterto attempt the examination first andat least get a look at the mucosa. Onecan administer an enema subsequentlyif necessary.
Miscellaneous
Castor oil, a triglyceride expressedfrom the seeds of a tropical Africanplant, has been used as a catharticfor 3500 years. It is hydrolyzed in thesmall intestine by pancreatic enzymesto release glycerol and ricinoleic acid ;43the latter produces hypermotility of thesmall and large bowel. Castor oil pro-duces abdominal cramping and loosebowel motions within 2 hours and ifused in excess may induce electrolyteimbalance. Because of this violent ac-tion it is unsuitable for routine use andshould be reserved for situations inwhich total colonic cleanout is neces-sary, such as for a barium enema orcolonoscopy.
Lactulose is a synthetic disaccharidenot digested by small intestinal or pan-creatic enzymes. In the colon it is meta-bolized by the microflora, with resul-tant acidification of the stool and re-
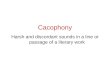
Table I-Types of laxatives available andtime lags in their action
Type Time lag
Bulking agents BranPsyllium DaysMethylcellulose J
Stool softeners Mineral oil*Dioctyl sodium D
sulfosuccinate ays
Chemical Diphenylmethanestimulants Phenolphthalein .6 hours
Oxyphenisatin* rBisacodyl J
Anthracene gly-cosides 6 hoursSennaCascara
Saline cathartics Magnesium sulfateMagnesium 3 hourshydroxideSodium sulfate
Miscellaneous Castor oil - 2 hoursLactuloseCalomel *Croton oil*Podophyllum*Caroid and Bile Salts*
*Obsolete
lease of gas. It is effective in treatingconstipation and changes the nature ofthe colon flora.59 The main indicationis portal-systemic encephalopathy be-cause it decreases the availability ofammonia and other amines from thegastrointestinal tract to the brain.00 Thedrug is too costly for routine purgationand with long-term use there is riskof superinfection.61
There are other traditional laxativesthat are now considered obsolete. Theseinclude mercury-containing compoundssuch as calomel, and mucosal irritantssuch as croton oil. The latter has beenused to alter the political views of pri-soners and would seem to have limitedappeal in a democracy.62 Podophyllum,a resin used to remove warts, is nolonger considered a practical cathartic.Oral bile salts have a direct stimulatingeffect on the colon and, in addition,inhibit the absorption of salt andwater.63 The resultant catharsis explainsthe durability of that ancient prepara-tion still on druggists' shelves, Caroidand Bile Salts. Because of the adverseeffects of bile salts in the stomach andthe existence of many other effectiveagents, this preparation can no longerbe considered useful.64
Conclusion
Constipation, like beauty, "often liesin the eyes of the beholder". It is asobering thought that many patientspurge themselves because they thinkthey are constipated.TM In one study, 14of 20 patients using laxatives habituallyfor constipation were able to maintaina satisfactory bowel habit during a2-week period on a placebo.65 Thus,the physician must first determine thatthe patient is indeed constipated. Laxa-tives should be reserved for episodes ofconstipation such as may occur afterbarium radiography or enforced bed-rest. The types of laxatives availableand the time lags in their action aresummarized in Table I.
In a lecture delivered nearly 40 yearsago Witts66 urged his colleagues to re-frain from ritual purgation of their pa-tients. He pointed out that purging "anyunfortunate patient who is robustenough to stand the strain" pre- andpostoperatively is a practice "rooted inarchaic and primitive beliefs, ratherthan physiology and pathology." Seri-ously ill patients in a state of precarioushydration can ill afford further gastro-intestinal loss of fluid. In spite of in-junctions by clinical pharmacologistsagainst their long-term use, over 700laxative preparations are available overthe counter in the United States,17 andthese are dispensed literally by theton.67 Like King Lear in the storm, thephysician must stand firm on his scien-
tific convictions and defy this costlyand harmful tide.
I thank Miss Diane Moore for typing themanuscript.
References
1. GEIB D, JONES JD: Unprecedented case ofconstipation. JAMA 38: 1305, 1902
2. CONNELL AM, HILTON C, IRVINE G, et al:Variation of bowel habit in two populationsamples. Br Med 1 2: 1095, 1965
3. Misntwicz JJ: Colonic motility. Gut 16: 311,1975
4. THOMPSON WG: The irritable colon. CanMed Assoc 1 111: 1236, 1974
5. Hustsr AF: Constipation and Allied IntestinalDisorders, London, Oxford U Pr, 1919
6. TRUELOVE SC, REYNELL PC: Diseases of theDigestive System, 2nd ed, Oxford, Blackwell,1972, p 389
7. CLEAVE TL: The Saccharine Disease, Bristol,Wright, 1974
8. BUluurr DP, WALKER ARP, PAINTER NS:Effect of dietary fibre on stools and transittime and its role in the causation of disease.Lancet 2: 1408, 1972
9. HEATON KW, PAYLER D, POMARE EW, et al:The relationship between intestinal transittime and stool weight, and the effects ofbran (abstr). Gastroenterology 66: 843, 1974
10. LYFORD C, FIsHER J, Buass B, et al: Con-trolled clinical trial of bran in irritablebowel syndrome (abstr). Gun Res 23: 247,1975
11. KIRWAN WO, SMITH AN, MCCONNELL AA,et al: Action of different bran preparationson colonic function. Br Med 1 4: 187, 1975
12. ALVAREZ WC: Intestinal autointoxication. Phy-stol Rev 4: 352, 1924
13. DONALDSON AN: Relation of constipation tointestinal intoxication. JAMA 78: 884, 1922
14. SMITH 5: cited in In England Now. Lancet 2:1079, 1973
15. THOMPSON WG: Sigmoidoscopy. Can MedAssoc / 110: 683, 1974
16. CUMMINGS JH: Progress report: dietary fibre.Gut 14: 69, 1973
17. Laxatives and dietary fiber. Med Lett DrugsTher 15: 98, 1973
18. PAINTER NS: Aetiology of diverticular disease.Br Med 1 2: 156, 1971
19. COWGILL OR, ANDERSON WE: Laxative ef-fects of wheat bran and "washed bran lflhealthy men. JAMA 98: 1866, 1932
20. CAss U, WOLF LP: A clinical evaluation ofcertain bulk and irritant laxatives. Gastro-enterology 20: 149, 1952
21. SOUTER WA: Bolus obstruction of gut afteruse of hydrophilic colloid laxatives. Br Med I1:166, 1965
22. PAINTER NS, TRuU.OvE SC, ANDRAN GM, etal: Effect of morphine, prostigmine, pethidineand Pro-Banthine on the human colon indiverticulosis studied by intra-luminal pressurerecorders and cineradiology. Gut 6: 57, 1965
23. Ivav KJ: Are anticholinergics of use in theirritable colon syndrome? Gastroenterology68: 1300, 1975
24. INGELFINOER FJ: The treatment of chronicconstipation. Ann NY Acad Sci 58: 503, 1954
25. GOODMAN LS, OILMAN A: The Pharmaco-logical Basis of Therapeutics, 4th ed, NewYork, Macmillan, 1970, p 540
26. ZURROW HB, SERGAY H: Lipoid pneumoniain a geriatric patient. I Am Geriatr Assoc14: 240, 1966
27. FREIMAN DO, ENGELBERO H, MEJUtIT WH:Oil aspiration (lipoid) pneumonia in adults: astudy of 47 patients. Arch Intern Med 66:11, 1940
28. EL5TON CW: Pneumonia due to liquid paraf-fin: a chemical analysis. Arch Dis Child 41:428, 1966
29. Effect of mineral oil on the absorption ofcarotine and vitamin A in man (E). NutrRev 6: 170, 1948
30. JAVERT CT, MACRI C: Prothrombin concentra-tion and mineral oil. Am J Obstet Gynecol42: 409, 1941
31. DONALD I: Practical Obstetrical Problems, 3rded, London, Lloyd Lake, 1964, p 743
32. JoNas A, GODDING EW: Management ofConstipation, Oxford, Blackwell, 1972, chap2, part 2, p 38
33. Bovo JT, DOLL R: Gastro-intestinal cancerand the use of liquid paraffin. Br I Cancer8: 231, 1954
930 CMA JOURNAL/MAY 22, 1976/VOL. 114

34. SAUNDERS DR. SILLERY I, RACHMILEWFVL D:Effect of dioctyl sodium sulfosuccinate (DSS)on structure and function of human and ratintestine (abstr). Gastroenterology 68: 979,1975
35. NA.ss K: Oxyphenisatin and jaundice. JAMA212: 1961, 1970
36. FANTus B, DYNIEwIcz JM: Phenolphthaleinstudies. Elimination of phenolphthalein.JAMA 110: 1656, 1938
37. BLIcK P, BERARDI JB, WOZASEK 0: The modeof the laxative action of phenolphthalein. AmJ Dig Dis 9: 292, 1942
38. AsItAMOwITz EW: Phenolphthalein today: acritical review. Am J Dig Dis 17: 79, 1950
39. REYNOLDs TD, LAPIN AC, PamIts RL, et al:Puzzling jaundice: probable relationship tolaxative ingestion. JAMA 211: 86, 1970
40. MAcHARDY G, BALART LA: Jaundice andoxyphenisatin. Ibid, p 83
41. PEARsON AJG, GRAINGER JM, SCHAUER DJ,et al: Jaundice due to oxyphenisatin. Lancet1: 994, 1971
42. KocK NG, KEWENTER J, SUNDIN T: Studieson the defecation reflex in man. Scand IGastroenterol 7: 689, 1972
43. GOoDMAN LS, GILMAN A: PharmacologicalBasis of Therapeutics, op cit, p 1020
44. HusAcHER MH, DOERNBERO S: Laxatives.II. Relationship between structure and po-tency. J Pharm Sci 53: 1067, 1964
45. HARDCASTLE JD, WILKINS JL: The action ofsennosides and related compounds on humancolon and rectum. Gut 11: 1038, 1970
46. SMITH B: Effect of irritant purgatives on themyenteric plexus in man and the mouse. Gut9: 139, 1968
47. WALLER 5: Comparative effects of codeineand senna on the motor activity of the leftcolon (abstr). Gut 16: 407, 1975
48. BocKus HL, WILLARD JH, BANK J: Melanosiscoli: the etiological significance of the an-thracine laxatives. A report of 41 cases.JAMA 111: 1, 1933
49. RAWSON MD: Cathartic colon. Lancet 1:1121, 1966
50. FRENCH JM, GADDIE R, SMITH N: Diarrhoeadue to phenolphthalein. Lancet 1: 551, 1956
51. CUMMINO5 JH, SLADEN GE, JAMES OFW,et al: Laxative-induced diarrhoea: a continu-ing clinical problem. Br Med 1 1: 537, 1974
52. HEIZER WD, WARSHAW AL, WALDMANN TA,et al: Protein-losing gastroenteropathy andmalabsorption associated with factitious diar-rhea. Ann Intern Med 68: 839, 1968
53. SILK DDA, Glasovi JA, MURRAY CRH: Re-versible finger clubbing in a case of purgativeabuse. Gastroenterology 68: 790, 1975
54. SCHWARTZ WB, RELMAN AS: Metabolic andrenal studies in chronic potassium depletionresulting from overuse of laxatives. J ClinInvest 32: 258, 1953
55. HOUGHTON BJ, Pa.tRS MA: Chronic potassiumdepletion due to purgation with cascara. BrMed / 1: 1328, 1958
56. FLEISCHER N, BROWN H, GRAHAM DY, et al:Chronic laxative induced hyperaldosteronismand hypokalemia simulating Bartter's syn-drome. Ann Intern Med 70: 791, 1969
57. HARVEY RF, READ AE: Saline purgatives actby releasing cholecystokinin. Lancet 2: 185,1973
58. DEVROEDE G, LaitIcHa M, SANcHEZ G, et al:Effects of hypertonic enemas on the rectalmucosa (abstr). Ann R Coil Phys Surg Can8: 27, 1975
59. WESSELIUS-DE CASPARIS A, BRAADBAART 5,BERGH-BOHLKEN GE, et al: Treatment ofchronic constipation with lactulose syrup:results of a double blind study. Gut 9: 87,1968
60. ELKINOTON SG: Lactulose. Gut 11: 1043,1970
61. Dusos RJ, SAVAGE DC, SCHAEDLER RW: Theindigenous flora of the gastrointestinal tract.Dis Colon Rectum 10: 23, 1967
62. GADDUM JH: Pharmacology, 4th ed, London,Oxford U Pr, 1953, p 251
63. MEKJIAN HS, PHILLIPS SF, HOFFMAN AF:Colonic secretion of water and electrolytesinduced by bile acids: perfusion studies inman. J Clin Invest 50: 1569, 1971
64. HEATON KW: The importance of keeping bilesalts in their place. Gut 10: 857, 1969
65. GREINER T, BROSS I, GOLD H: A method forevaluation of laxative habits in human sub-jects. I Chronic Dis 6: 244, 1957
66. Wsrrs U: Ritual purgation in modern medi-cine. Lancet 1: 427, 1937
67. TRAvELL I: Pharmacology of stimulant laxa-tives. Ann NY Acad Sd 58: 416, 1954
BactriinRoche
Rx summaryIndicatIonsThe following types of infections when caused bysusceptible pathogens:* Genitourinary tract infections: acute, recurrent,and chronic cystitis, pyelonephritis, urethritis(including uncomplicated gonococcal urethritis),prostatis, vaginitis, cervicitis, salpingitis
* Upper and lower respiratory tract infections(particularly chronic bronchitis and includingacute and chronic otitis media)
* Gastrointestinal tract infectionsIt is not indicated in infections due to Pseudomonas,Mycoplasma, or viruses.ContraindicationsEvidence of marked liver damage; blood dyscrasias;known hypersensitivity to trimethoprim or sulfona-mides; or marked renal impairment where repeatedserum assays cannot be carried out.Infants during the first few weeks of life (especiallypremature infants).For the time being, during pregnancy.Adverse reactionsMost frequent: nausea; vomiting; gastric intolerance;and rash.Less frequent: diarrhea; constipation; flatulence;anorexia; pyrosis; gastritis; gastroenteritis; urticaria;headache; and liver changes (abnormal elevationsin alkaline phosphatase and serum transaminase).Occasionally reported: glossitis; oliguria; hema-tuna; tremor; vertigo; alopecia; and elevated BUN,NPN, and serum creatinine.Hematological changes, occurring particularly inthe elderly, are mostly transient and reversible(primarily, neutropenia and thrombocytopenia; lessfrequently, leukopenia, aplastic or hemolytic anemia,agranulocytosis, and bone marrow depression).PrecautionsAs with other sulfonamide preparations, benefitshould be critically appraised against risk inpatients with liver damage, renal damage, urinaryobstruction, blood dyscrasias, allergies,or bronchial asthma.The possibility of superinfection with a non-sensitiveorganism should be borne in mind.Dosage and administrationChildren under 12 years of age:Young children - according to weightUnder 2 years - 2.5 ml suspension, twice daily2 to 5 years -2.5 to 5 ml suspension or ito 2pediatric tablets, twice daily6 to 12 years -5 to 10 ml suspension or 2 to 4pediatric tablets or 1 adult tablet, twice dailyAdults and children over 12 years of age:Standard dosage -2 adult tablets, twice dailyMinimum dosage and long-term treatment -1 adult tablet, twice dailyMaximum dosage (overwhelming infections)-3 adult tablets, twice dailyUncomplicated gonorrhea -2 adult tablets, 4 timesdaily for 2 daysFor acute urinary tract infections, 2 tablets twicedaily should be given until the urine becomessterile.When the patient has a history of chronic reinfection,1 tablet twice daily can be given as prophylaxis.SuppiySuspension (aniseed-flavoured), each teaspoonful(5 ml) containing 40 mg trimethoprim plus 200 mgsulfamethoxazole. Bottles of 100 and 400 ml.Pediatric tablets, containing 20 mg trimetho-prim plus 100 mg sulfamethoxazole. Bottles of 100and 500.Adult tablets, containing 80 mg trimethoprimplus 400 mg sulfamethoxazole. Bottles of 100 and500.
Product monograph available on request.
*Trade Mark of Hoffmann-La Roche Limited
@Reg. Trade Mark
Q Hoffmann-La Roche LimitedVaudreull, Quebec
DaImane.Roche(fi urazepam)
Rx summary:Indications Useful in all types of insomniacharacterized by difficulty in falling asleep,frequent nocturnal awakenings and/or earlymorning awakening. Dalmane' can be admin-istered effectively for short-term and intermittentuse in patients with recurring insomnia andpoor sleeping habits; however, the safety andefficacy of long-term use has not beenestablished.Contraindications Known hypersensitivity to thedrug and, because of lack of sufficient clinicalexperience, in children under fifteen years of age.Warnings Safety in women who are or maybecome pregnant has not been establishedhence as with all medication, Dalmane shouldbe given only when the potential benefits havebeen weighed against possible hazard to motherand child.Precautions Use in fhe Elderly: In elderly anddebilitated patients, it is recommended that thedosage initially be limited to 15 mg to precludethe development of oversedation, dizzinessand/or ataxia reported in some patients.Use in Emotional Disorders: The usual precau-tions are indicated for severely depressedpatients or those in whom there is any evidenceof latent depression, particularly the recognitionthat suicidal tendencies may be present andprotective measures may be necessary.Potenfiafion of Drug Effects: Since Dalmanehas a central nervous system depressant effect,patients should be advised against the simul-taneous ingestion of alcohol and other centralnervous system depressant drugs duringDalmane' therapy.Physical and Psychological Dependence: Aswith any hypnotic, caution must be exercised inadministering to individuals known to beaddiction-prone or those whose history suggeststhey may increase the dosage on their owninitiative.General: All patients should be cautionedagainst engaging in activities requiring precisionand complete mental alertness such as inoperating machinery or driving a motor vehicleshortly after ingesting the drug. ShouldDalmane' be used repeatedly, periodic bloodcounts and liver and kidney function testsshould be performed. The usual precautionsshould be observed in patients with impairedrenal or hepatic function. Patients' reactions willbe modified to a varying extent depending ondosage and individual susceptibility.Adverse Effects Dizziness, drowsiness,lightheadedness and ataxia may occur. Theseadverse effects are particularly common in elderlyand debilitated patients. (See Precautions).Severe sedation, lethargy, disorientation, prob-ably indicative of drug intolerance or overdose,have been reported.Dosage Dosage should be individualized formaximal beneficial effects. The usual adultdosage is 3D mg before retiring. In elderly and/ordebilitated patients, it is recommended thattherapy be initiated with 15 mg until individualresponses are determined. Moderate to severeinsomnia may require 15 or 30 mg.Supply Dalmane' 15, capsules (orange andivory) 15 mg, 100 and 500.Dalmane 3D, capsules (red and ivory) 30 mg,100 and 500.Complete prescribing information availableon request.@Reg. Trade Mark
Hoffmann-La Roche Limited\E1III.E1I.,f Vaudreull, Quebec
CMA JOURNAL/MAY 22, 1976/VOL. 114 931