Embed Size (px)
Citation preview

Context Matters in Pediatric Obesity: Commentary on InnovativeTreatment and Prevention Programs for Pediatric Overweightand Obesity
Barbara H. Fiese,1,2 PHD, and The STRONG Kids Team1Family Resiliency Center and 2Department of Human and Community Development, University of Illinois
at Urbana-Champaign
All correspondence concerning this article should be addressed to Barbara H. Fiese, PHD, University of
Illinois at Urbana-Champaign, 904 West Nevada, Doris Kelley Christopher Hall, MC-081, Urbana, IL
61801, USA. E-mail: [email protected]
Received July 16, 2013; revisions received July 27, 2013; accepted August 8, 2013
This commentary reviews the 9 articles in the Special Issue on Innovative Treatment and Prevention
Programs for Pediatric Overweight and Obesity. Taking a socio-ecological perspective, contextual factors such
as characteristics of the child, family, community, and culture are offered as ways to improve treatment and
prevention programs. Using a more tailored approach that takes into account individual differences in family
communication patterns and problem solving is warranted. Pediatric psychologists are urged to consider the
role of prevention and targeted efforts during early childhood to reduce the prevalence of childhood obesity.
Key words family function obesity; prevention/control; weight management.
The Journal of Pediatric Psychology has long been a leader in
publishing innovative approaches to treating and under-
standing complex health conditions in childhood and ad-
olescence. There is perhaps a no more complicated and
daunting condition than childhood obesity in its resistance
to amelioration. Without exception, each article begins
with dire statistics drawn from nationally representative
datasets indicating that in 2009–2010, 16.9% of children
and adolescents between 2 and 19 years of age were con-
sidered obese (Ogden, Carroll, Kit, & Flegal, 2012). The
editors of this special issue are to be commended for col-
lecting an excellent set of articles that represent the state of
the science in treating overweight and obesity in childhood
and adolescence. For some readers of this issue, there may
be disappointing news in that many of the innovative and
intensive treatments described had little appreciative effect
above and beyond less intensive and standard forms of
intervention. For example, Berkowitz and colleagues
(2013) compared the relative effectiveness of an in-
person 17 session family-based group life style manage-
ment program with a self-directed family-based life style
management program and found that both were (modestly)
effective in weight loss for adolescents. Similarly, Davis and
colleagues report that an intensive family-based telemedi-
cine intervention was equally effective in reducing BMI as a
pediatrician-delivered program (Davis, Sampilo, Gallagher,
Landrum, & Malaone, 2013). Motivational Interviewing
(MI) techniques were also compared using enhanced
approaches supporting more autonomy within the family
(Saelens, Lozano, & Scholz, 2013) and self-efficacy in
youth (Walpole, Dettmer, Morrongiello, McCrindle, &
Hamilton, 2013). Both of these studies found little differ-
ences in BMI change between the enhanced approach or in
comparison to a control group. A skeptic may conclude
that family-based interventions add little value to obesity
treatment for children and youth. This conclusion would
be in contrast to the large literature base suggesting that
family-based interventions are effective in weight manage-
ment for children (Whitlock, O’Connor, Williams, Beil, &
Lutz, 2010). What appears to be missing from the discus-
sion in the carefully controlled randomized controlled trials
(RCTs) is the context in which the family-based interven-
tions are delivered and the daily experiences of the families
receiving treatment.
Journal of Pediatric Psychology 38(9) pp. 1037–1043, 2013
doi:10.1093/jpepsy/jst069
Advance Access publication September 6, 2013
Journal of Pediatric Psychology vol. 38 no. 9 � The Author 2013. Published by Oxford University Press on behalf of the Society of Pediatric Psychology.All rights reserved. For permissions, please e-mail: [email protected]
at Old D
ominion U
niversity on June 30, 2014http://jpepsy.oxfordjournals.org/
Dow
nloaded from
The authors of these articles are not discouraged by
their findings but rather offer discussions about universal
elements of interventions as well as new directions in the
treatment of pediatric obesity. The program described by
Berkowitz and colleagues (2013) illustrates the important
role that primary care providers can play in supporting
weight loss with their patients. Similarly, Davis and col-
leagues (2013) found that treatment by physicians was
just as effective as a more comprehensive telemedicine
approach. Both the Berkowitz and Davis studies illustrate
the role that unobserved factors such as the relationship
between provider and patient may play in effecting change.
For adolescents who may have established a relationship
with their primary care provider over many years, imple-
menting a lifestyle change may be as effective as imple-
menting change when establishing new relationships—
albeit with added support. Walpole and colleagues
(2013) directly address how the client/therapist relation-
ship may be more similar than different across treatment
conditions.
In addition to characteristics of therapist and/or pro-
vider that may account similarities across treatment and
comparison groups, it is also important to consider char-
acteristics of the family. Saelens and colleagues (2013)
incorporated a self-directed approach as did Berkowitz
and colleagues (2013). The effectiveness of self-directed
approaches may be better understood by readiness to
change and a better understanding of family characteristics
that make it more or less likely that the family will be
receptive to the intervention. The remaining articles
address some of these issues. First, it is important to
consider what is meant by family context.
Family Context of Pediatric Obesity
In a previous special issue of the Journal of Pediatric
Psychology dedicated to overweight in childhood, Black
and Young-Hyman (2007) conclude ‘‘the articles in this
Special Issue highlight the psychological, family, health,
and social challenges associated with weight-related
issues among children, illustrating the importance of incor-
porating contextual factors into an understanding of child
overweight.’’ (p. 2). Several socio-ecological models have
been put forth to elucidate the complexities in the causes
of childhood obesity (Birch & Anzman, 2010; Fiese &
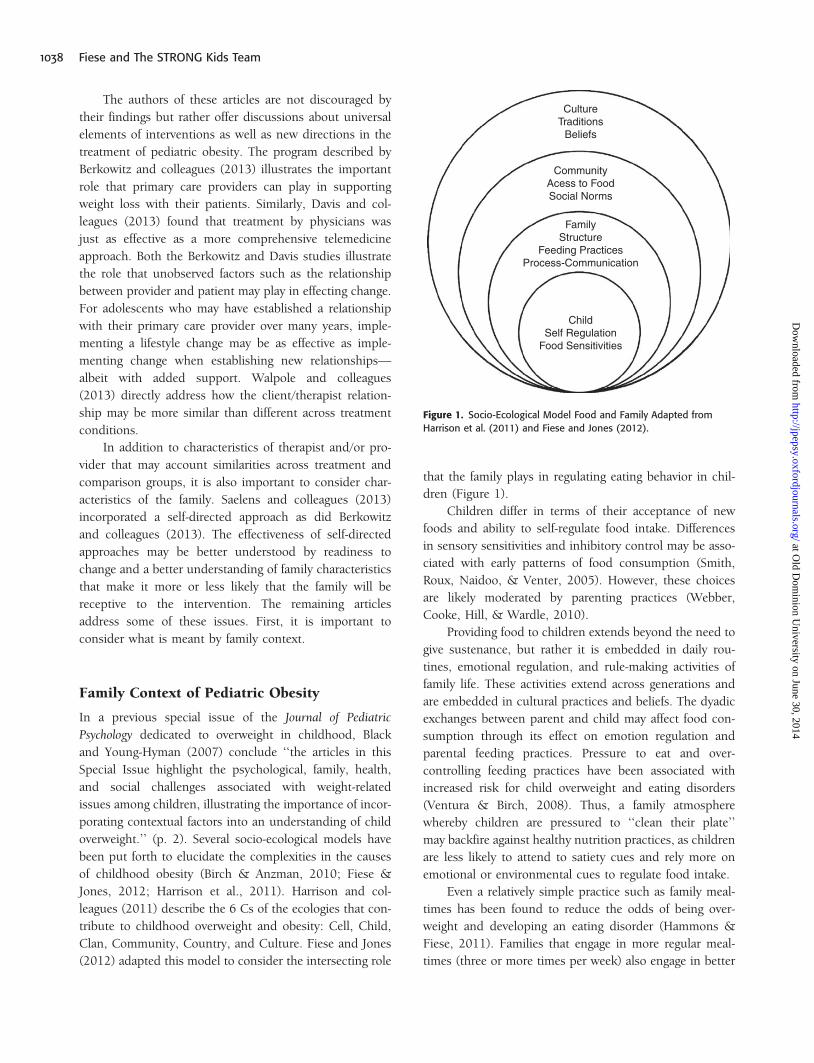
Jones, 2012; Harrison et al., 2011). Harrison and col-
leagues (2011) describe the 6 Cs of the ecologies that con-
tribute to childhood overweight and obesity: Cell, Child,
Clan, Community, Country, and Culture. Fiese and Jones
(2012) adapted this model to consider the intersecting role
that the family plays in regulating eating behavior in chil-
dren (Figure 1).
Children differ in terms of their acceptance of new
foods and ability to self-regulate food intake. Differences
in sensory sensitivities and inhibitory control may be asso-
ciated with early patterns of food consumption (Smith,
Roux, Naidoo, & Venter, 2005). However, these choices
are likely moderated by parenting practices (Webber,
Cooke, Hill, & Wardle, 2010).
Providing food to children extends beyond the need to
give sustenance, but rather it is embedded in daily rou-
tines, emotional regulation, and rule-making activities of
family life. These activities extend across generations and
are embedded in cultural practices and beliefs. The dyadic
exchanges between parent and child may affect food con-
sumption through its effect on emotion regulation and
parental feeding practices. Pressure to eat and over-
controlling feeding practices have been associated with
increased risk for child overweight and eating disorders
(Ventura & Birch, 2008). Thus, a family atmosphere
whereby children are pressured to ‘‘clean their plate’’
may backfire against healthy nutrition practices, as children
are less likely to attend to satiety cues and rely more on
emotional or environmental cues to regulate food intake.
Even a relatively simple practice such as family meal-
times has been found to reduce the odds of being over-
weight and developing an eating disorder (Hammons &
Fiese, 2011). Families that engage in more regular meal-
times (three or more times per week) also engage in better
CultureTraditions
Beliefs
CommunityAcess to FoodSocial Norms
FamilyStructure
Feeding PracticesProcess-Communication
ChildSelf Regulation
Food Sensitivities
Figure 1. Socio-Ecological Model Food and Family Adapted from
Harrison et al. (2011) and Fiese and Jones (2012).
1038 Fiese and The STRONG Kids Team
at Old D
ominion U
niversity on June 30, 2014http://jpepsy.oxfordjournals.org/
Dow
nloaded from

nutritional practices, serving more fruits and vegetables
than those who share meals less regularly (Hammons &
Fiese, 2011). However, it may not be sheer frequency of
shared meals that account for better health outcomes, as
the types of communication, including positive response to
affect and expressed genuine concern about the child’s
daily activities, are also associated with reduced risk for
overweight and obesity (Fiese, Hammons, & Grigsby-
Toussaint, 2012).
Societal factors also affect mealtime practices, such as
exposure to media. Several studies have documented the
effects of food advertising on the consumption of high fat
foods and sugar sweetened beverages (Harrison, Liechty, &
The STRONG Kids Program, 2012; Institute of Medicine,
2013). The ever presence of cell phones and other forms of
mobile media at the table also present challenges in terms
of distractions and preventing positive forms of communi-
cation known to promote healthy outcomes (Fiese, Winter,
& Botti, 2011).
Families differ in terms of access to healthy foods.
Low-income families and families living in rural communi-
ties have more difficulty accessing fresh fruits and vegeta-
bles and often have to rely on corner stores or convenience
stores to procure food (Larson, Story, & Nelson, 2009).
In addition to limited access to healthy foods, African
American and Hispanic families in low-income neighbor-
hoods often find it difficult to access culturally relevant
foods common to their traditional diets (Grigsby-
Toussaint, Zenk, Odoms-Young, Ruggiero, & Moise,
2010).
Relevant to this discussion and the studies reported in
this special issue, is whether these contextual variables
reported in descriptive studies have been taken into con-
sideration and if so, how can it inform future prevention
and treatment efforts?
Characteristics of the Child
Loss of Control (LOC) eating, body image, eating disor-
ders, and body dissatisfaction were considered in two of
the reports (Cassidy et al., 2013; Wilksch & Wade, 2013).
These are important characteristics to consider in an ado-
lescent age-group and as comorbidities of obesity. As
pointed out by Cassidy and colleagues, body image is
integrally embedded in cultural values. If interventions
address body image as part of weight reduction then cul-
tural considerations must surely be taken into account.
Surprisingly, outside of LOC little attention is paid to
other self-regulatory features such as inhibition and emo-
tional regulation more broadly speaking. Future research
may want to consider individual differences in self-
regulation that may influence responsiveness to treatment
and the likelihood that individuals will stay engaged in
treatment.
Family Structure and Process
Although the majority of the reports in this special issue
refer to family-based interventions, none of the studies
report on family structure. Given the rapid changes in
family demographics, it is important to know whether
the child or adolescent is being raised by a single parent,
may reside in multiple households in a given week, and
may be receiving different messages about eating and phys-
ical activity norms from multiple family members. Only the
Cassidy report identified parent as the mother, grand-
mother, or father. There is increasing evidence that marital
status is related to child health outcomes, with children
living in households with cohabitating adults faring less
well (Bzostek & Beck, 2011). The mechanism of this
effect may be due to economic resources as well as the
ability of adults to adequately monitor children’s health-
related behaviors including sleep, TV viewing, and eating.
Future obesity trials should include an assessment of
family structure as well as adults responsible for feeding
and arranging physical activity opportunities for the child
or adolescent.
A promising approach taken by St. George and col-
leagues (2013) incorporates both a focus on family process
variables and attention to variability within families. Project
SHINE implemented a family communication and moni-
toring intervention to reduce sedentary behavior in adoles-
cents. The family communication intervention was
successful in decreasing sedentary behavior and further,
those families that demonstrated the most positive com-
munication had adolescents that improved the most in
decreasing sedentary behavior. The results of this study
are important from a conceptual and analytical perspective.
Conceptually, the study incorporated a key feature of
family functioning, positive communication, known to be
associated with positive health outcomes (Alderfer et al.,
2008). Families can communicate in a variety of ways—
either directly—‘‘It is time for our family walk.’’ Or
indirectly—‘‘Get your lazy body off the couch.’’ Future
research may incorporate more nuanced and comprehen-
sive approaches to family functioning including the
McMaster model that assesses problem solving, communi-
cation, roles, affective responsiveness, affective involve-
ment, behavior control, and general functioning (Epstein,
Ryan, Bishop, Miller, & Keitner, 2003) and has been
Context Matters in Pediatric Obesity 1039
at Old D
ominion U
niversity on June 30, 2014http://jpepsy.oxfordjournals.org/
Dow
nloaded from

applied to the study of chronic health conditions in chil-
dren including obesity (Herzer et al., 2010). Theory-driven
approaches to family communication and functioning are
warranted for future research in this promising area.
The SHINE project also points toward innovative strat-
egies in analyzing family response to treatment. In consid-
ering the interaction between treatment condition and
communication scores, the authors were able to demon-
strate that those families with high scores on communica-
tion had the most significant decrease in sedentary
behavior. It is important to understand within-group dif-
ferences, particularly as it comes to families, in planning
for future intervention efforts. Tailored approaches that
target families most receptive to change and most likely
to benefit from interventions may explain some of the
modest effects seen in previous RCTs. Clearly not all fam-
ilies are created equal. More sophisticated understanding
of these differences in communication and problem solving
strategies may improve the effectiveness of future clinical
trials.
Community as a Resource
Ecological models require that the community be system-
atically integrated with family and institutional resources.
Programs such as 5-2-1-0 as described by Rogers and
colleagues (2013) have become increasingly popular
across the United States, yet are infrequently evaluated.
This innovative approach to evaluation is to be com-
mended for its comprehensiveness and involvement of
multiple stakeholders. There are several take home mes-
sages from this report for pediatric psychologists. First, it
is important to consider the value of simple messages that
can be repeated in multiple settings. Be assured, these are
not simplistic messages, but ones that take much care and
thought to develop as described by the authors. These
messages can be reinforced by health care providers and
practicing psychologists as lessons for healthy living not
only for those seeking treatment for obesity and over-
weight. Indeed, the interventions described by Berkowitz
and colleagues (2013) and Davis and colleagues (2013) are
examples where a community-based intervention could be
paired with primary care-based interventions for a more
comprehensive approach. Second, this is the only report
that addresses young children and child care settings.
Recent estimates suggest that 27% of 2- to 5-year-old chil-
dren are overweight and 12% are obese (Ogden et al.,
2012). Pediatric psychologists can play an important role
in preventing childhood obesity by working closely with
childcare providers and directors in offering educational
sessions on healthy eating and physical activity. Programs
such as the 5-2-1-0 provide clear and easy to follow steps
that can be implemented in early care and education
settings. Third, this community-based effort illustrates
how public campaigns can have an influence on policies
at child care centers, schools, and the workplace. Active
involvement by pediatric psychologists in these efforts
can only strengthen the research to practice to policy
connections.
Cultural Context
The Cassidy (Cassidy et al., 2013) and Olvera (Olvera,
Leung, Kellam, & Liu, 2013) reports directly address
cultural context of obesity interventions. Cassidy and col-
leagues highlight the need to consider how body image
ideals may differ across cultures. Starting at an early age,
parents tend to underestimate their child’s weight with
parents of overweight children more likely to consider
them to be of healthy weight (Hager et al., 2012). When
cultural norms are considered, values for robust and full-
figured physiques are often in contrast to media images of
the ‘‘thin ideal.’’ The Cassidy report points to an important
topic to discuss, particularly for adolescent girls who often
struggle with body image as part of a normative process.
The Olvera report on the BOUNCE program illustrates
the importance of considering the context of the daily lives
of African American and Hispanic youth. Summer time is a
vulnerable period for many low-income youth with few
available resources. Planning physical activity programs as
part of summer programs has the potential to affect a
significant number of youth. It is impressive that these
researchers were able to affect change in percent body fat
after only a 30-day intervention. Future efforts may pair
physical activity programs with the Summer Food Service
Program sponsored by the United States Department of
Agriculture (http://www.fns.usda.gov/summer-food-serv
ice-program-sfsp) to increase the likelihood that the pro-
gram is sustainable over time.
Conclusion
The articles in this special issue represent some of the best
science in the treatment of pediatric overweight and obe-
sity. Carefully constructed and implemented RCTs are the
gold standard for clinically based treatment programs. The
investigators of these programs are to be commended for
their innovation in adapting new paradigms and consider-
ing how treatment of childhood obesity can be improved.
However, these trials do not come without costs. Strict
1040 Fiese and The STRONG Kids Team
at Old D
ominion U
niversity on June 30, 2014http://jpepsy.oxfordjournals.org/
Dow
nloaded from

inclusionary and exclusionary criteria, time commitment
for lengthy sessions, travel time to facilities, and coordina-
tion of family schedules often make it difficult to reach
children and youth in need. Alternative approaches pre-
sented in this special issue such as telemedicine and self-
directed programs are promising but require further work.
To increase the effectiveness of existing programs
and inform new programs, greater attention to the socio-
ecological context of childhood obesity is warranted.
Variation in child self-regulation, family structure, family
routines, cultural traditions, and community resources
may influence the likelihood that any given treatment
will have an effect. As we move more toward models of
personalized medicine, pediatric psychology can take a
leadership role in recognizing the contextual factors that
are the causes and consequences of childhood obesity.
This will result in a sharper and more refined approach
to practice and policy.
A glaring omission, with the exception of the commu-
nity-based effort (Rogers et al., 2013), was attention to
early childhood and preventative efforts. The Institute of
Medicine (2011) has called for increased attention for the
prevention of childhood obesity starting at birth. There are
clear and actionable steps that pediatric psychologists can
take working with parents, pediatricians, health care pro-
viders, and hospitals to prevent childhood obesity. Simple
steps include the promotion of breast feeding, responsive
feeding practices during early childhood, reducing screen
time to <2 hr per day, practicing good sleep hygiene, and
being physically active as a family. It is incumbent on
pediatric psychologists to be strong advocates for families
to prevent childhood obesity and promote healthy habits
from an early age.
Childhood obesity is complex condition. The last
special issue dedicated to childhood overweight did not
yet recognize obesity as a classification in childhood
(Black & Young-Hyman, 2007). In many ways we have
come a long way in better understanding just how multi-
faceted this condition is. Although the simple story is more
calories in than expended, the persistent difficulty in turn-
ing the tide clearly suggests that context matters. The next
generation of researchers will be challenged to integrate
solid clinical science with an understanding of the intrica-
cies of contemporary family life. Hopefully this can be done
before the health of a significant number of children is
further compromised.
Acknowledgments
The STRONG Kids Team includes Kristen Harrison,
Kelly Bost, Brent McBride, Sharon Donovan, Diana
Grigsby-Toussaint, Juhee Kim, Janet Liechty, Angela
Wiley, Margarita Teran-Garcia, and Barbara Fiese.
Funding
Preparation of this manuscript was supported, in part, by
USDA National Institute of Food and Agriculture, Hatch
Project number 793 328, and the Christopher Family
Foundation Food and Family Program.
Conflict of interest: None declared.
References
Alderfer, M. A., Fiese, B. H., Gold, J. I., Cutuli, J. J.,
Holmbeck, G. N., Goldbeck, L., . . . Patterson, J.
(2008). Evidence-based assessment in pediatric
psychology: Family measures. Journal of Pediatric
Psychology, 33, 1046–1061. doi:jsm083 [pii]
10.1093/jpepsy/jsm083
Berkowitz, R. I., Rukstalis, M. R., Bishop-Gilyard, C. T.,
Moore, R. H., Gehrman, C. A., Xanthopoulos, M. S.,
. . . Wadden, T. A. (2013). Treatment of adoles-
cent obesity comparing self-guided and group
lifestyle modification programs: A potential
model for primary care. Journal of Pediatric
Psychology, 38, 978–986.
Birch, L. L., & Anzman, S. L. (2010). Learning to eat in
an obesogenic environment: A developmental
systems perspective on childhood obesity. Child
Development Perspectives, 4, 138–143.
Black, M. M., & Young-Hyman, D. (2007). Introduction
to the special issue: Pediatric overweight. Journal of
Pediatric Psychology, 32, 1–5.
Bzostek, S. H., & Beck, A. N. (2011). Family instability
and young children’s health. Social Science &
Medicine, 73, 282–292. doi:10.1016/j.socscimed.
2011.04.014
Cassidy, O., Sbrocco, T., Vannucci, A., Nelson, B.,
Jackson-Bowen, D., Heimdal, J., . . . Tanofsky, M. B.
(2013). Adapting interpersonal psychotherapy for
the prevention of excessive weight gain in
rural African American girls. Journal of Pediatric
Psychology, 38, 965–977.
Davis, A. M., Sampilo, M., Gallagher, K. S., Landrum, Y.,
& Malaone, B. (2013). Treating rural pediatric
obesity through telemedicine: Outcomes from a
small randomized controlled trial. Journal of Pediatric
Psychology, 38, 932–943.
Epstein, N. B., Ryan, C. E., Bishop, D. S., Miller, I. W.,
& Keitner, G. I. (2003). The McMaster Model: A
Context Matters in Pediatric Obesity 1041
at Old D
ominion U
niversity on June 30, 2014http://jpepsy.oxfordjournals.org/
Dow
nloaded from
view of healthy family functioning. In F. Walsh
(Ed.), Normal family processes (3rd ed., pp. 581607).
New York, NY: Guilford.
Fiese, B. H., Hammons, A., & Grigsby-Toussaint, D. S.
(2012). Family mealtimes: A contextual approach to
understanding childhood obesity. Economics and
Human Biology, 10, 365–374.
Fiese, B. H., & Jones, B. L. (2012). Food and family:
A socio-ecological perspective for child development.
Advances in Child Development and Behavior, 42,
307–337.
Fiese, B. H., Winter, M. A., & Botti, J. C. (2011). The
ABC’s of family mealtimes: Observational lessons
for promoting healthy outcomes for children
with persistent asthma. Child Development, 82,
133–145.
Grigsby-Toussaint, D., Zenk, S. N., Odoms-Young, A. M.,
Ruggiero, L., & Moise, I. (2010). Availability of
commonly consumed and culturally specific fruits
and vegetables in African-American and Latino
neighborhoods. Journal of the American Dietetic
Association, 110, 746–752.
Hager, E. R., Candelaria, M., Latta, L. W., Hurley, K. M.,
Wang, Y., Caulfield, L. E., & Black, M. M. (2012).
Maternal perceptions of toddler body size: Accuracy
and satisfaction differ by toddler weight status.
Archives Pediatric and Adolescent Medicine, 1666,
417–422.
Hammons, A., & Fiese, B. H. (2011). Is frequency of
shared family meals related to the nutritional health
of children and adolescents? A meta-analysis.
Pediatrics, 127, e1565–e1574. doi:10.1542/peds.
2010-1440
Harrison, K., Bost, K. K., McBride, B. A.,
Donovan, S. M., Grigsby-Toussaint, D. S., Kim, J.,
. . . Jacobsohn, G. C. (2011). Toward a
developmental conceptualization of contributors
to overweight and obesity in childhood: The
Six-C’s model. Child Development Perspectives, 5,
50–58.
Harrison, K., Liechty, J. M., & The STRONG Kids
Program. (2012). US Preschoolers’ media exposure
and dietary habits: The primacy of television and the
limits of parental mediation. Journal of Children
and Media, 6, 18–36. doi:10.1080/17482798.2011.
633402
Herzer, M., Godiwala, N., Hommel, K. A., Driscoll, K.,
Mitchell, M., Crosby, L. E., . . . Modi, A. (2010).
Family functioning in the context of pediatric
chronic conditions. Journal of Behavioral and
Developmental Pediatrics, 31, 26–34.
Institute of Medicine. (2011). Early childhood obesity
prevention policies. Washington, DC: The National
Academies Press.
Institute of Medicine. (2013). Challenges and opportunities
for change in food marketing to children and youth:
Workshop summary. Washington, DC: The National
Academies Press.
Larson, N. I., Story, M., & Nelson, M. C. (2009).
Neighborhood environments: Disparities in access to
healthy foods in the U.S. American Journal of
Preventive Medicine, 36, 74–81.
Ogden, C. L., Carroll, M. D., Kit, B. K., & Flegal, K. M.
(2012). Prevalence of obesity and trends in body mass
index among US children and adolescents, 1999–2010.
JAMA, 307, 483–490. doi:10.1001/jama.2012.40
Olvera, N., Leung, P., Kellam, S.F., & Liu, J. (2013). Body
fat and fitness improvements in Hispanic and African
American girls. Journal of Pediatric Psychology, 38,
987–996.
Rogers, V. W., Hart, P. H., Motyka, E., Rines, E.,
Vine, J., & Deatrick, D. A. (2013). Impact of Let’s
Go! 5-2-1-0: A community-based, multisetting
childhood obesity prevention program. Journal of
Pediatric Psychology, 38, 1010–1020.
Saelens, B. E., Lozano, P., & Scholz, K. (2013). A ran-
domized clinical trial comparing delivery of behav-
ioral pediatric obesity treatment using standardized
and enhanced motivational approaches. Journal of
Pediatric Psychology, 38, 954–964.
Smith, A. M., Roux, S., Naidoo, N. T., & Venter, D. J. L.
(2005). Food choices of tactile defensive children.
Nutrition, 21, 14–19.
St. George, S. M., Wilson, D. K., Schneider, E., &
Alia, K. (2013). Project SHINE: Effects of parent-
adolescent communication on sedentary behavior in
African American adolescents. Journal of Pediatric
Psychology, 38, 997–1009.
Ventura, A. K., & Birch, L. L. (2008). Does parenting
affect children’s eating and weight status?
International Journal of Behavioral Nutrition and
Physical Activity, 5, 15.
Walpole, B., Dettmer, E., Morrongiello, B. A.,
McCrindle, B. W., & Hamilton, J. (2013).
Motivational interviewing to enhance self-efficacy and
promote weight-loss in overweight and obese adoles-
cents: A randomized controlled trial. Journal of
Pediatric Psychology, 38, 944–953.
Webber, L., Cooke, L., Hill, C. S., & Wardle, J. (2010).
Associations between children’s appetitive traits and
maternal feeding practices. Journal American Dietetic
Association, 110, 1718–1722.
1042 Fiese and The STRONG Kids Team
at Old D
ominion U
niversity on June 30, 2014http://jpepsy.oxfordjournals.org/
Dow
nloaded from

Whitlock, E. P., O’Connor, E. A., Williams, S. B.,
Beil, T. L., & Lutz, K. W. (2010). Effectiveness of
weight management interventions in children: A
targeted systematic review for the USPSTF. Pediatrics,
125, e393–e418.
Wilksch, S. M., & Wade, T. D. (2013). Life Smart: A
pilot study of a school-based program to reduce the
risk of both eating disorders and obesity in young
adolescent girls and boys. Journal of Pediatric
Psychology, 38, 1021–1029.
Context Matters in Pediatric Obesity 1043
at Old D
ominion U
niversity on June 30, 2014http://jpepsy.oxfordjournals.org/
Dow
nloaded from