Embed Size (px)
Citation preview

Practice Guideline
American College of Chest Surgeons: In patients with a low to moderate pre test probability of malignancy (5% - 60%) and an indeterminate SPN that measures at least 8 to 10 mm in diameter, fluorodeoxyglucose (FDG) positron emission tomography (PET) should be performed to characterize the nodule.
When the pre-test probability of malignancy is moderate to high (>60%), and the nodule is hypermetabolic by FDG PET, surgical diagnosis is preferred when clinically appropriate (6).
Background: The prevalence of non-calcified pulmonary nod-ules in smokers or ex smokers is 23% - 69%, but only 1.4% - 2.7% have malignant nodules. The Fleischner Society has published imaging guide-lines for patients with pulmonary nodules that are smaller than 8 mm (1).
PET/CT is more accurate that CT alone for char-acterizing pulmonary nodules, resulting in fewer equivocal findings, and higher specificity (2). Low to intermediate risk nodules ≥ 8 mm should be evaluated by PET/CT, whereas high-risk nodules should be biopsied or excised.
The sensitivity of PET/CT for lung cancer is >90%, so low to intermediate risk nodules that are meta-bolically inactive can be followed radiographically to ensure stability or resolution. The specificity of PET/CT is approximately 80% because inflamma-tory nodules can be metabolically active (3). PET positive nodules require further investigation.
PET/CT with 18F-fluorodexoyglucose (FDG) has been shown to be cost-effective for character-izing lung nodules ≥ 8 mm when risk-estimates based on clinical versus morphological param-eters are conflicting, or when indeterminate nod-ules are found in high-risk individuals (4).
SNM recommends that 18F-FDG PET/CT should routinely be obtained in the diagnostic work-up of solitary pulmonary nodule (5). Imaging will im-prove health care outcomes, mostly by avoiding futile surgeries in low-risk patients and enabling curative surgeries in high-risk patients.
Value of PET/CTDiagnosis of Pulmonary NodulesCore Message for Referring Physicians
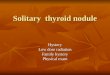
Case Example 2:
84 year-old man with chronic cough and 1.5 cm nodule on chest x-ray. PET /CT showed no FDG uptake. Biopsy was deferred. The nodule had grown to 2 cm 12 months later. Biopsy showed a fungus.
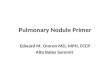
Case Example 1:
47-year-old man with incidental 1.5 cm nodule discovered on chest x-ray. PET/CT showed high FDG uptake. Biopsy showed poorly differentiated lung cancer.

Quantitative criteria have been suggested to improve the accuracy of PET/CT. The standardized uptake value (SUV) is a ratio of the concentration of FDG in the nodule compared to the average concentration in the body. An SUV of 2.5 has been used to differentiate benign from malignant nodules. Many variables, however, affect the measurement of SUV, limiting its accuracy and reproducibility. It has been suggested that an increase or no change in SUV when measured at two time points between 60 to 120 minutes improves accuracy (7). Despite the appeal of a simple numerical measurement, most physicians rely on visual assessment of metabolic activ-ity using a binary decision model of detectable versus no detectable FDG uptake.
References1. MacMahon H, et al. Guidelines for management of small pulmonary nodules detected on CT scans: A statement from the Fleischner Society. Radiology 2005;237:395-400.
2. Pauls S, et al. Performance of integrated FDG-PET/CT for differentiating benign and malignant lung lesions--results from a large prospective clinical trial. Mol Imaging Biol. 2008 Mar-Apr;10(2):121-8.
3. Ung YC, et al. 18Fluorodeoxyglucose positron emission tomography in the diagnosis and staging of lung cancer: a systematic review. J Natl Cancer Inst 2007 Dec 5;99(23):1753-6
4. Gould MK, et al. Cost-effectiveness of alternative management strategies for patients with solitary pulmonary nodules. Ann Intern Med. 2003 May 6;138(9):724-35.
5. Fletcher JW, et al. Recommendations on the use of 18F-FDG PET in oncology. J Nucl Med. 2008 Mar;49(3):480-508.
6. Alberts WM. Chest 2007;132;1-19 Clinical Practice Guidelines (2nd Edition) Executive Summary: ACCP Evidence-Based Diagnosis and Management of Lung Cancer.
7. Alkhawaldeh K, et al. Impact of dual-time-point 18F-FDG PET imaging and partial volume correction in the assessment of solitary pulmonary nodules. Eur j Nucl Med Mol Imaging 2008;35:246-252.
8. CMS Publication 100-03, Medicare National Coverage Determinations Manual, Chapter 1, Part 4, Section 220.6). Available at http://www.cms.hhs.gov/manuals/downloads/ncd103c1_part4.pdf
Reimbursement
CMS Coverage Policy
PET and PET/CT are approved by the Centers for Medicare and Medicaid Services (CMS) for characterization of solitary pulmonary nodules not exceeding 4 cm to determine the likelihood of malignancy. Claims should include evidence of the initial detection of a primary lung nodule, usually by computed tomography (8).