Embed Size (px)
Citation preview

Corneal Endothelial Deposits in Patients With Cytomegalovirus Retinitis
KEITH A. WALTER, MD., VICKI L. COULTER, MD., DAVID A. PALAY, MD., MICHAEL J. TARAVELLA, MD.,
HANS E. GROSSNIKLAUS, M.D., AND HENRY F. EDELHAUSER, PH.D.
• PURPOSE: We studied six patients with human immunodeficiency virus (HIV) who had cytomegalovirus retinitis and abnormal endothelial de-posits in at least one eye, to characterize their corneal endothelial deposits. • METHODS: The corneas of the six patients were examined by slit-lamp biomicroscopy and specular microscopy with morphometric analysis. The eyes of one patient with endothelial changes were obtained post mortem for histopathologic and ultrastructural examination. • RESULTS: There were multiple diffuse, fine, retractile, stellate-shaped deposits on the corneal endothelium in all affected eyes. The deposits were best seen with retroillumination. Two of six patients examined with specular microscopy showed severe abnormalities, which included marked areas of polymegathism and decreased endothelial cell counts. Examination of one eye obtained post mortem disclosed chains of dendritic macrophages and fibrin adherent to the apical surface of the corneal endothelium. There was no evidence of direct infection of the corneal endothelium by cytomegalovirus.
Accepted for publication Aug. 25, 1995. From the Department of Ophthalmology, Emory University, Atlan
ta, Georgia (Drs. Walter, Palay, Grossniklaus, and Edelhauser); and Department of Ophthalmology, University of Colorado at Denver, Denver, Colorado (Drs. Coulter and Taravella). This study was supported in part by Research to Prevent Blindness, Inc., New York, New York, and National Institutes of Health Departmental Core Grant P30 EY06360, Bethesda, Maryland (Drs. Walter, Palay, Grossniklaus, and Edelhauser).
Reprint requests to David A. Palay, M.D., Department of Ophthalmology, Emory Eye Center, 1327 Clifton Rd. N.E., Atlanta, GA 30322; fax: (404) 778-5128.
• CONCLUSIONS: Deposits on the corneal endothelium in patients with cytomegalovirus retinitis most likely result from an anterior uveitis. A preponderance of macrophages observed by histopathologic examination may be related to the inability of the immunodeficient patient to mount a normal T-cell response.
N 1989, SEVER1N AND ASSOCIATES' DESCRIBED ONE patient with cytomegalovirus retinitis and abnormal deposits on the corneal endothelium. We
identified six patients with cytomegalovirus retinitis and abnormal endothelial deposits. Two eyes, one of which had abnormal endothelial deposits, were obtained for histopathologic examination.
MATERIAL AND METHODS
WE IDENTIFIED SIX HIV-POSITIVE PATIENTS WITH CYTO-
megalovirus retinitis and abnormal endothelial deposits in at least one eye. All patients in this study were examined at Emory University-affiliated hospitals in Atlanta, Georgia, or at the Denver General Eye Clinic, Denver, Colorado, between November 1989 and April 1993. A complete eye examination was performed on all patients. The patients included in this study were nonconsecutive and were included on the basis of their willingness to be in this study and to undergo specular microscopic photography. Informed consent was obtained. Wide-field specular microscopy was performed with the Keeler Konan specular microscope on all patients. Computer-assisted mor-
VOL. 121, No, 4 © AMERICAN JOURNAL OF OPHTHALMOLOGY i996,-i2i:39i-396 3 9 1

phometric analysis2 was used to determine the average endothelial cell counts and the coefficient of variation in two areas of a 400 x enlarged negative of the specular photographs. We calculated the mean cell area and the coefficient of variation in the cell area. Cell density (cells per square millimeter) was calculated by dividing 106 μηι2/ιηπι2 by the mean cell area (in square micrometers).3 The coefficient of variation was calculated by dividing the standard deviation of the cell by the mean cell area. The coefficient of variation is a dimensionless index independent of cell size and provides a quantitative measurement of polymega-thism. Both eyes of one patient with endothelial changes were obtained for postmortem examination. The eyes were fixed in 10% neutral buffered formalin. During gross examination, a portion of the affected cornea was submitted in 2.5% glutaraldehyde for electron microscopic processing. For light microscopy, a central section of each eye was processed in increasing concentrations of alcohol and cleared in xylene; 5^m-thick sections were stained with hema-toxylin and eosin. Representative sections were placed on poly-L-lysine-coated slides and stained with the avidin-biotin complex immunoperoxidase method for lysozyme and cytomegalovirus, with appropriate positive and negative controls. The portion of the cornea in 2.5% glutaraldehyde was postfixed in 0.1 mol/1 of cacodylate buffer and 1% osmium tetroxide. After standard dehydration, the specimen was embedded in epoxy resin, and 1.0-μπι sections were cut and stained with uranyl acetate-lead citrate for transmission electron microscopy.
RESULTS
SIX PATIENTS WITH CYTOMEGALOVIRUS RETINITIS WERE noted to have the characteristic endothelial findings. Three patients had uniocular involvement of the anterior segment, which correlated with their ipsilat-eral cytomegalovirus retinitis. The other three patients had bilateral endothelial deposits and bilateral cytomegalovirus retinitis. There were diffuse, fine, stellate-shaped, linear or reticular deposits, or both, on the corneal endothelium in the involved eye. These keratic precipitates were generally present across the entire corneal endothelium, but in some patients were heavier inferiorly. The deposits were
refractile and were best seen with retroillumination (Fig. 1) or with the relief mode of specular microscopy (Fig. 2). Additionally, some patients had pigmented round deposits spread diffusely across the endothelium that were distinct from the stellate keratic precipitates (Fig. 1). Both types of deposits were noted in the presence or absence of anterior chamber cell and flare. There was no evidence of corneal edema, posterior or anterior synechiae, iris nodules, iris atrophy, or increased intraocular pressure.
The initial diagnosis of cytomegalovirus retinitis was made on the basis of the appearance of yellow-white fluffy retinal infiltrates with or without hemorrhage. All patients were being treated with intravenous ganciclovir at the time of this study.
Specular microscopic analysis was performed on all six pairs of eyes. The average endothelial cell count for healthy individuals between the ages of 30 and 59 years has been reported to be 2,625 to 2,739 cells/ mm2, and the average coefficient of variation, between 0.27 and 0.29.4 An increased coefficient of variation is a quantitative measurement of polymega-thism. Two patients (Patients 3 and 5) had abnormally low endothelial cell counts and increased coefficients of variation (Table).
Figure 2 is a specular micrograph from the left eye of Patient 3. The polymegathism appeared most pronounced in the cells underlying the stellate corneal deposits, which are best seen in relief mode.
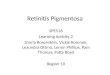
Both eyes from Patient 6 were obtained post mortem and evaluated for the stellate keratic precipitates on the corneal endothelium. The retina of the left eye of this patient had cy tomegalic cells. Results of immunohistochemical stains were positive for cytomegalovirus within infected retinal cells. Light microscopic examination showed attenuated endothelium in the left eye, with macrophages and fibrin in the anterior chamber (Fig. 3). Immunohistochemical stains were positive for lysozyme in macrophages and negative for cytomegalovirus in all retrocorneal cells, including corneal endothelium. Lysozyme-positive macrophages were adherent to the posterior corneal surface (Fig. 4). Transmission electron microscopy showed multiple and single macrophages (Fig. 5) with associated fibrin adherent to the posterior corneal surface in the left eye. These corneal changes and active retinal cytomegalovirus retinitis were not noted in the right eye.
392 AMERICAN JOURNAL OF OPHTHALMOLOGY APRIL 1996

Fig. 1 (Walter and associates). Patient 3. Slit-lamp appearance of eye in which there are diffuse, stellate, refractile, endothelial deposits, which are best seen in retroillumination. Additionally, there are small, round, pigmented, endothelial deposits.
Fig. 2 (Walter and associates). Patient 3, left eye. Specular microscopy showing white keratic precipitates on the endothelial cells. The upper portion of the photograph is the relief mode and shows the stellate-shaped deposits. Endothelial cells under and adjacent to the precipitates show polymegathism (Xl75).
VOL.121, No. 4 CORNEAL ENDOTHELIAL DEPO:
Fig. 3 (Walter and associates). Patient 6, left eye. Rare endothelial cells (arrowhead) are present on the posterior surface of the inferior cornea. Fibrin (asterisk) and vacuolated cells are present in the anterior chamber. There is an absence of lymphocytes. Some vacuolated cells (arrow) are adherent to the posterior corneal surface (hematoxylin and eosin, X160).
Fig. 4 (Walter and associates). Patient 6, left eye. Immunohistochemical staining for lysozyme is positive in vacuolated macrophages adherent to the posterior corneal surface (arrow) but not in the corneal endothelial cells (arrowhead) (peroxidase anti-peroxidase, X160).
DISCUSSION
THE FOLLOWING FEATURES WERE COMMON TO THE patients in this study. There were fine, stellate, retroendothelial deposits across the entire endotheli-um, with more precipitates inferiorly. These deposits were transparent and were best seen with indirect illumination (Fig. 1). Although fewer in number,
393 IN CYTOMECALOVIRUS RETINITIS

TABLE
ENDOTHELIAL SPECULAR MORPHOMETRIC ANALYSIS
PATIENT NO., AGE (YRS), GENDER
EYE WITH CYTOMEGALOVIRUS
RETINITIS
EYE WITH STELLATE KERATIC
PRECIPITATES CELL COUNT
(CELLS/MM2)
COEFFICIENT OF VARIATION
1,43, M
2, 32, M
3, 42, M
4,45, M
5, 43, M
6, 41, M*
R.E. LE. R.E. —
R.E. LE. R.E. —
R.E. LE. —
L.E.
R.E. LE. R.E. Clear LE. R.E. LE. R.E. Clear L.E. R.E. LE. Clear R.E. L.E.
3,162 2,907 2,774 2,660 1,813 1,951 2,796 2,912 1,992 2,156 2,953 2,995
.276
.297
.261
.263
.404
.465
.263
.251
.344
.463
.263
.295
<Bofi èyés of irus patient were examined post mortem.
there were also small, round, pigmented keratic pre-cipitates. A few patients in our study had a mild anterior chamber reaction; however, none of the patients demonstrated corneal edema, posterior or anterior synechiae, or iris atrophy.
It is our impression that keratic precipitates are the result of mild ocular inflammation associated with ocular cytomegalovirus retinitis infection, which was demonstrated in three of our patients who had uniocular involvement of the anterior segment, which correlated with their ipsilateral cytomegalovirus retinitis. Histopathologic examination of one of these six patients disclosed that the right eye was free from corneal and retinal disease, but the left eye showed evidence of cytomegalovirus retinitis and corneal retroendothelial deposits consisting of macrophages and fibrin. None of our patients had clinical evidence of other infectious or inflammatory diseases of the eye.
Other reports have confirmed the association between ocular cytomegalovirus retinitis infection and corneal endothelial deposits. Severin and associates' described a single case of a patient with cytomegalovirus retinitis and an anterior uveitis with a "special form and arrangement of the [keratic] precipitates" in a reticular structure. Severin and associates' described the specular micrographs as having "slight pleomor-
phy" and "small, dark structures and large, bright [reticular] structures in retroendothelial cellular apposition." Brody and associates5 screened 42 eyes of patients with acquired immunodeficiency syndrome (AIDS) and found 31 eyes with cytomegalovirus retinitis. Of those 31 eyes, 25 (81%) had a low-grade iritis with "stellate corneal endothelial deposits" in the eye affected with cytomegalovirus retinitis.
Daicker6 described the histopathologic findings of a patient with cytomegalovirus retinitis and panuveitis. The patient was noted to have lattice-like precipitates on the corneal endothelium during a premortem clinical examination. Postmortem examination disclosed chains of dendritic macrophages adherent to the corneal endothelium, which were similar to those found in the histologie examination of our patient. Daicker noted abnormal endothelial cells with "darker cytoplasm with basophilic nuclear inclusions," which were interpreted as direct infection of the endothelial cells with cytomegalovirus retinitis, although immunohistochemical or electron microscopic examination was not performed. After careful immunohistochemical and electron microscopic examination, we found no evidence of direct infection of the corneal endothelium with cytomegalovirus in the eyes that we examined post mortem.
The reticular pattern of the retrocorneal precipi-
394 AMERICAN JOURNAL OF OPHTHALMOLOGY APRIL 1996

Desc
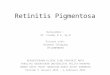
Fig. 5 (Walter and associates). Patient 6, left eye. Transmission electron microscopy shows vacuolated inflammatory cells, with numerous intracytoplasmic inclusions, adherent to the posterior surface of Descemet's membrane (Desc). Some cells are arranged in groups (top), whereas others are single (bottom). Fibrin (fib) is also present (x3,420).
tates may be explained by the presence of macrophages and fibrin seen on histologie examination. Macrophages are capable of extending their pseudopods and engulfing foreign particles. These extended pseudo-pods, along with fibrin, may set up the framework for the stellate appearance seen clinically and with specular microscopy. There were no lymphocytes in
the keratic precipitates in the two eyes examined post mortem, which is of interest because the patient whose eyes were examined post mortem had a low CD4+ T-lymphocyte count, and the keratic precipitates of immunocompetent patients are composed of lymphocytes, macrophages, and neutrophils.7 Therefore, the stellate keratic precipitates we observed may
VOL.121, No . 4 CORNEAL ENDOTHELIAL DEPOSITS IN CYTOMEGALOVIRUS RETINITIS 395

reflect the patient's inability to mount a normal T-lymphocyte-mediated response. However, it also may be possible that ocular infection with cytomegalovirus retinitis elicits a macrophage-prédominant response.
Two of six patients had severe abnormalities on specular microscopy (Fig. 2, Table), which included marked areas of polymegathism and decreased endothelial cell counts. The polymegathism appeared most pronounced in the cells underlying the corneal deposits. We suspect that the endothelial abnormalities are the result of an interaction between the corneal deposits and the endothelial cells. Alternatively, it is possible that a primary endothelial abnormality occurred, which elicited the retrocorneal deposits, although we found no evidence of cytomegalic infection or other primary endothelial abnormality on histopathologic examination. It is possible that the endothelial changes might have developed in the other patients if we had followed them over time.
Several investigators8'11 have published specular photomicrographs of patients with Fuchs' iridocyclitis that are similar in appearance to the specular photomicrographs of our patients. Clinically, our patients' symptoms resembled those of Fuchs' heterochromic uveitis with respect to the presence of stellate keratic precipitates, low-grade anterior chamber reaction, and lack of posterior synechiae. Several articles by Brooks, Grant, and Gillies,9'11 who used standard specular microscopy techniques, as well as relief-mode specular microscopy, noted light, irregular shapes with multiple attenuated processes or a stellate appearance in keratic precipitates associated with Fuchs' iridocyclitis. These stellate structures were thought to be inflammatory debris or macrophages extending their pseudopods. Results of relief-mode specular microscopy in patients with Fuchs' iridocyclitis appear very similar to the findings in our patients. Precise classification of the stellate keratic precipitates seen in Fuchs' heterochromic uveitis is difficult because there have been no detailed histopathologic analyses of the corneal endothelium in these patients.12
In summary, this detailed analysis of corneal endothelial findings in patients with cytomegalovirus retinitis has been documented by slit-lamp biomicro-scopy; specular microscopy; and histologie, immu-nohistochemical, and ultrastructural examinations.
These corneal endothelial deposits appear to be the result of mild ocular inflammation in immunodefi-cient patients. The characteristic keratic precipitates are composed of macrophages and fibrin and are devoid of lymphocytes. This macrophage and fibrin response appeared to account for the clinically atypical appearance of a low-grade uveitis associated with cytomegalovirus retinitis. We found no evidence of direct infection of the corneal endothelium by cytomegalovirus to explain the appearance of the endothelial deposits. When these characteristic endothelial deposits are noted on slit-lamp biomicroscopy, a suspicion should be raised for cytomegalovirus retinitis.
REFERENCES
1. Severin M, Hartmann C, Schädlich HJ, Brunner R, Rasokat H. Endothelprazipitate und Zytomegalieninfektion. Fortschr Ophthalmol 1989;86:227-31.
2. Matsuda M, Suda T, Manabe R. Quantitative analysis of endothelial mosaic pattern changes in anterior keratoconus. Am J Ophthalmol 1984;98:43-9.
3. Waring GO III, Krohn MA, Ford GE, Harris RR, Rosenblatt LS. Four methods of measuring human corneal endothelial cells from specular photomicrographs. Arch Ophthalmol 1980;98:848-55.
4. Yee RW, Matsuda M, Schultz RO, Edelhauser HF. Changes in the normal corneal endothelial cellular pattern as a function of age. Curr Eye Res 1985;4:671-8.
5. Brody JM, Butrus SI, Laby DM, Whitmore PV, Phillips TM. Anterior uveitis in AIDS patients with cytomegaloviral (CMV) retinitis. ARVO Abstracts. Invest Ophthalmol Vis Sci 1991;32(4, suppl):764.
6. Daicker B. Cytomegalovirus panuveitis with infection of corneo-trabecular endothelium in AIDS. Ophthalmologica 1988;197:169-75.
7. Nussenblatt RB, Palestine AG. Examination of ocular structures. In: Nussenblatt RB, Palestine AG, editors. Uveitis, fundamental and clinical practice. Chicago: Year Book Medical Publishers Inc., 1989:63-4.
8. Alanko HI, Vuorre I, Saari KM. Characteristics of corneal endothelial cells in Fuchs' heterochromic cyclitis. Acta Ophthalmol 1986;64:623-31.
9. Brooks AM, Grant G, Gillies WE. Differential specular microscopy in keratopathy and anterior uveitis. Cornea 1988;7:105-11.
10. . Differentiation and assessment of corneal endothelial changes associated with diseases of the anterior segment of the eye. Aust N Z J Ophthalmol 1987;15:65-70.
11. . The use of specular microscopy to investigate unusual findings in the corneal endothelium and its adjacent structures. Aust N Z J Ophthalmol 1988;16:235-43.
12. Jones NP. Fuchs' heterochromic uveitis: an update. Surv Ophthalmol 1993;37:253-72.
396 AMERICAN JOURNAL OF OPHTHALMOLOGY APRIL 1996