Embed Size (px)
Citation preview
European Heart Journal (1996) 17, 1891-1897
Coronary compliance in patients following orthotopicheart transplantation
An intravascular ultrasound study
S. Kerber*, O. Heinemann-Vechtel*, F. Gunther*, A. Rahmel*, M. Weyandf,M. Dengf, H. H. Scheldt and G. Breithardt*
*Department of Cardiology!'Angiology and Institute for Arteriosclerosis Research, Section 'Coronary HeartDisease', ^Department of Cardiovascular Surgery, Westfdlische Wilhelms-Universitdt Miinster, Germany
Background The aim of this study was to investigatecoronary compliance in patients early and 71-8 weeks afterorthotopic heart transplantation.
Methods Thirty patients (mean age 51-4 years, womenn = 6) underwent coronary angiography early after ortho-topic heart transplantation (mean interval 11-6 ±5-5weeks), by which time 12 recipients had already beentreated for episodes of rejection. A total of 153 differentcoronary segments were investigated using a mechanical30 MHz intravascular ultrasound system. In all segments,the intimal index and the circumferential extension of thevessel wall, which had a three-layered appearance, wereassessed. Systolic-diastolic changes in area, and pressurewith respect to vessel wall area, were used to study normal-ized compliance. All measurements were repeated in asubgroup of 13 patients 71-8 ± 10-7 weeks after transplan-tation.
Results At the first investigation, the mean intimal indexof all estimated cross-sectional areas was 007 ±0-10. Themean circumferential extension of the 'three-layered' cor-onary vessel wall was 74° ± 101°. No correlation could befound between normalized compliance and the intimalindex (r= -0-322, P<0001) or between normalizedcompliance and the circumferential extension of the three-layered vessel wall (r= -0-362, /><0001). Donor age
did not correlate with normalized compliance either(r= - 0-515, P=0004). In 12 patients with proven rejectionperiods before the first investigation, normalized com-pliance was significantly lower (1-76 ± 081 mmHg~ ')than in those without rejection (2-95 ± 1-22 mmHg~ ',/•=0005). Both the intimal index and the circumferentialextension of the three-layered architecture of the vessel wallwere significantly higher in recipients with rejection periods.A comparison of the subgroup of 13 recipients between firstand second investigation showed that the intimal indexincreased slightly from 003 ± 003 to 009 ± 0 1 3 (ns) 71-8weeks after transplantation, but that normalized com-pliance did not differ significantly between the first and thefollow-up investigation.
Conclusions Early after orthotopic heart transplantation,normalized compliance does not correlate with donor ageor the extent of atherosclerotic vessel alterations identifiableby intravascular ultrasound. Early rejection periods areassociated with reduced coronary arterial compliance.Using intravascular ultrasound, this adverse functionaleffect on arterial compliance can be observed together withan increase in the intimal index.(Eur Heart J 1996; 17: 1891-1897)
Key Words: Coronary compliance, intravascular ultra-sound, orthotopic heart transplantation.
Introduction
Intravascular ultrasound is a new imaging modalityfor the cross-sectional depiction of coronary arteries'11.Recent studies have proved that it has the potential
Revision submitted 15 January 1996, and accepted 21 January 1996.
Correspondence: Sebastian Kerber, MD, Medizinische Klinik undPoliklinik, Innere Medizin C, Westfalische Wilhelms-UniversitatMunster, D-48129 Munster, Germany.
to measure cross-sectional areas reliably'2', to analysevessel wall architecture'3'4' and to demonstrate the effectsof interventional procedures'5'. In coronary artery dis-ease, intravascular ultrasound has been regarded as avaluable adjunct to angiography'1'51.
In addition, intravascular ultrasound has thepotential to determine compliance of coronary arterialsegments. Previous studies have suggested that arterialcompliance may be determined by the extent and mor-phology of atherosclerosis'6'7', vessel size and vessel
0195-668X/96/121891+07 S25.00/0 1996 The European Society of Cardiology
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/17/12/1891/532939 by guest on 08 February 2022

1892 S. Kerber et al.
type16-71, the structural basis of the vessel wall'891, topo-graphic factors such as bifurcations'101 and clinicalfactors such as diabetes and age1""131. Intravascularultrasound studies in patients with angiographicallynormal coronary arteries demonstrated an inversecorrelation between the thickness of the intima-mediacomplex and distensibility'141. Studies in patients withcoronary artery disease confirmed that compliancediffers according to the extent and type of atheroscle-rotic lesions. In addition, coronary compliance variesaccording to the localization within the coronarytree'6-71.
Transplant vasculopathy results in specificatherosclerotic lesions within the coronary arteries oforthotopic heart recipients. These vessel alterations aredifferent from 'conventional' coronary artery dis-ease'15181, but until now, there have been no data onwhether or not transplant coronary vasculopathy has animpact on arterial compliance. Thus, the aim of thisprospective in-vivo investigation was to measure cor-onary compliance using intravascular ultrasound earlyand after a follow-up period of more than one year afterorthotopic heart transplantation, and to comparearterial compliance with the extent of coronary vesselalterations and clinical factors.
Methods
Patients
The study population consisted of 30 heart recipients(female n = 6) with a mean age of 51-4 ±11-6 years(range 23 to 69 years). The study protocol was estab-lished at the first routine coronary angiogram earlyafter transplantation and was approved by the EthicalCommittee for the Protection of Human Subjects fromResearch Risk at the Westfalische Wilhelms-UniversitatMiinster. All subjects had given informed written con-sent to this protocol.
Patients were studied at an average of 11-6 ± 5-5weeks (range 3 to 23 weeks) after transplantation. Meandonor age (male n = 21) at time of transplantationwas 290 ±13-2 years (range 10 to 57 years). All patientswere managed with standard immunosuppressiveregimens including prednisone, azathioprine and cyclo-sporin. Patients underwent regular endomyocardialright ventricular biopsies to monitor the possibility ofrejection. A total of 205 biopsies (mean number of 6-8biopsies per recipient until first investigation) were ana-lysed according to the Billingham Classification'19-201.
By the time of the first investigation, 12 recipi-ents had already experienced rejection (defined as rightventricular biopsy showing rejection grade II or worseaccording to the Billingham Classification) for whichthey were specifically treated. A subgroup of 13 recipi-ents (three patients with rejection until the first investi-gation) underwent a second investigation after aninterval of 718 ± 107 weeks after transplantation.
Angiography
Coronary and left ventricular angiography were per-formed via the right femoral artery using the Judkinstechnique in all cases. Vasoactive drugs were withdrawn24 h before the invasive study. After arterial puncture,5000 units of heparin were given intravenously via a 5-Fsheath into the right femoral vein. Left coronary angio-grams were performed via an angioplasty 8-F guidingcatheter using biplane standard angulations. An intra-coronary injection of 0-2 mg nitroglycerin preceded thecoronary angiograms. Subsequently, a guide wire (0014inch) was advanced into the midportion of the leftanterior descending artery (n = 27 patients) or into themidportion of the circumflex artery (n = 3 patients).
Intravascular ultrasound examination
Using this guide wire, a 3- 5-F Sonicath® catheter(Boston Scientific, U.S.A.) which has a 30 MHz single-element piezoelectric crystal transducer at its distal tip,was advanced into the coronary segments using continu-ous biplane fluoroscopic control. The catheter assemblyhouses a flexible drive cable connected to a motor whichrotates a mirror at 900 rpm. The catheter itself has apolyethylene outer shaft with a single distal part that isadvanced over the guide wire (monorail system). Thecatheter was connected to the imaging system Sonos®1000 (Hewlett Packard, U.S.A.). All intravascularimages were stored on VHS videotape for later analysis.
Imaging protocol
The catheter was advanced into the midportion of eitherthe left anterior descending or circumflex artery. Whenthe midportion of one of these vessels was reached withthe transducer, ultrasound settings, including receivergain compensation, compression and rejection wereadjusted to generate images with the largest gray-scalerange for optimized visualization of the vessel-lumeninterface and the intima-media boundary. The catheterwas placed in the most central position possible to depictthe entire lumen-wall interface, and the aortic pressurewas recorded through the guiding catheter to calculatecompliance. It was essential to measure the vessel wallthrough 360°, so that cross-sectional areas with originat-ing side branches were excluded. During withdrawal ofthe transducer to the stem, multiple cross-sectional areasof coronary artery segments were depicted.
Quantitative analysis
Quantitative analysis of intravascular ultrasound imageswas performed off line with the specific computer soft-ware of the Sonos® 1000 (Hewlett Packard, U.S.A.). Allrecordings were analysed blindly by one experiencedobserver. Measurements included the cross-sectional
Eur Heart J, Vol. 17. December 1996
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/17/12/1891/532939 by guest on 08 February 2022
Coronary complications in heart recipients 1893
lumen and plaque areas. The outer boundaries of plaqueareas were determined by following the course of theinternal elastic lamina. The intimal index (intimalindex=plaque area/lumen area) as a parameter ofatherosclerosis was calculated for each cross-sectionalarea. The extension of the three-layered vessel wall,which refers to the intravascular depiction of the hyper-dense intimal layer, the hypodense medial layer and thehyperdense adventitial layer and indicates intimal hyper-plasia of the vessel wall'211, was measured in circumfer-ence. Maximal and minimal luminal areas at the selectedsites were identified by frame-by-frame playback analy-sis. The low intra-observer and inter-observer variabilityin cross-sectional luminal areas has been confirmed byseveral studies'2221. Absolute compliance was deter-mined as change in area/change in pressure (mm2/mmHg x 103). Compliance was normalized to referencevessel area (normalized compliance=change in area/vessel area/change in pressure (mmHg~' x 103)).
Statistical analysis
Data are presented as mean values and standard devia-tion (SD) for continuous variables. Correlation betweencontinuous variables was determined by linear regressionanalysis. A /"-value <005 was considered statisticallysignificant. Mann-Whitney U-Wilcoxon Rank Sum Testwas used to evaluate differences between subgroups inthe study population. Figures 2 and 3 present the medianand first and third quartiles as a box plot.
Results
First investigation 116 ± 5-5 weeks aftertransplantation
A total of 153 different coronary segments with optimalsystolic and diastolic images were analysed. Of thesen=16 (13 patients) were located in the left main stem,n = 69 in the proximal and n=53 in the midportion of theleft anterior descending artery (27 patients); n= 10 cross-sectional areas of the proximal and n = 5 of the mid-portion of the circumflex branch were investigated inthree patients.
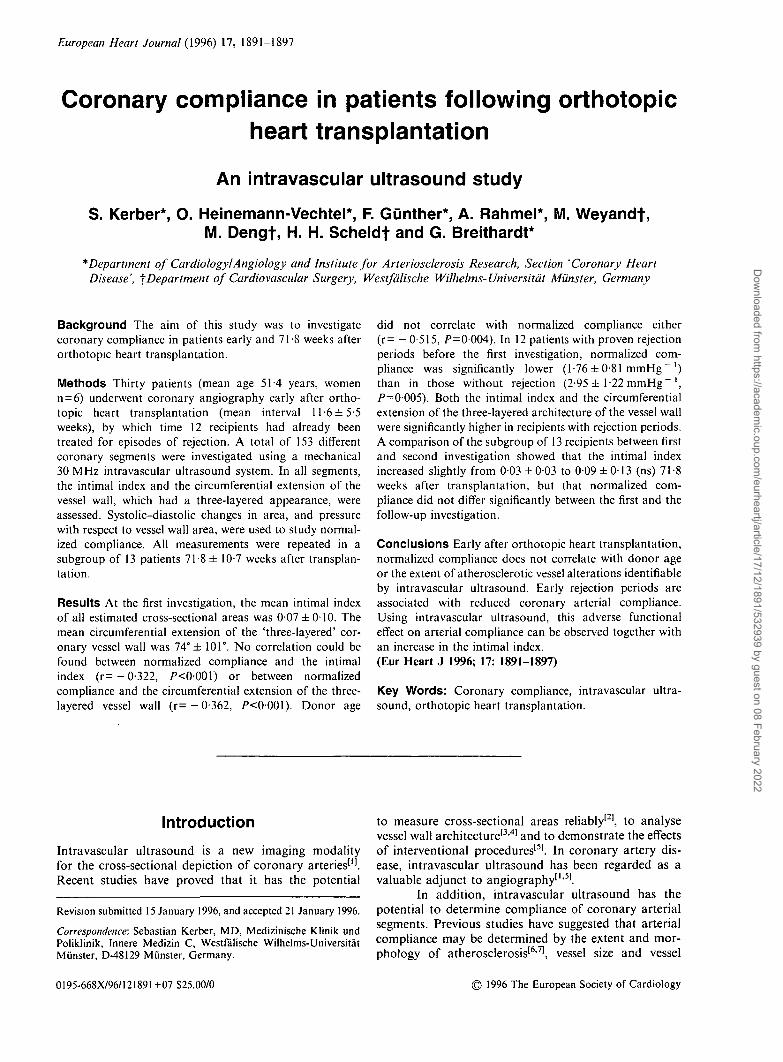
The three-layered appearance of the vessel wallwas not evident in segments in 25 patients. However, in22 cross-sectional areas in eight patients there was a 360°three-layered architecture, but in the remaining 38 cross-sectional areas present in 21 patients the three-layeredappearance was less than 360°. The mean circumferentialextension of the three-layered appearance was 74 ± 101°.Figure 1 is an example of a 30 MHz intravascularultrasound depiction of a proximal cross-sectionalarea in the left anterior descending artery showing aneccentric plaque.
The maximal diastolic luminal cross-sectionalarea was 11 ± 5 mm2, the minimal luminal cross-
Figure 1 30 MHz intravascular ultrasound cross-sectional area of the proximal left anterior descendingartery showing an eccentric plaque (<).
sectional area 10 ± 5 mm2 and mean plaque area1 ± 1 mm2. The intimal index as a parameter of plaqueextension of all evaluated arterial segments was007 ± 0 1 . A significant correlation was found betweendonor age and intimal index (r=0-780, P<0001) andbetween donor age and the extent of the three-layeredappearance of the vessel wall (r = 0-820, P<0001).
The absolute coronary compliance for all seg-ments was 281 ± 21-6 mm2/mmHg, and the normal-ized compliance of these measurements was 2-46 ±1 -59mmHg"1. The normalized compliance within thecircumflex artery was 2-66± 1-72mmHg"1, the corre-sponding value within the left anterior descending arterywas 2-45 ± 1 -47 mmHg " ' and 2-43 ± 1 90 mmHg " 'within the left main stem. Linear regression analysisrevealed no correlation between normalized complianceand intimal index (r= - 0-322, P<0001). There was alsono correlation between the three-layered appearance ofthe vessel wall and normalized compliance (r= — 0-362,/"<0001), and no statistically significant correlationbetween donor age and normalized compliance(r= -0-515, .P=0-004).
Influence of rejection
By the time of the first investigation, 12 recipients hadalready experienced rejection, verified by right ventricu-lar biopsy. All received specific rejection treatmentshown to be effective (demonstrating grade 0 or 1) at theone-week follow-up biopsy. The mean interval betweenheart transplantation and rejection was 5-5 weeks (range2-12).
Regarding vessel wall morphology at the time ofthe first investigation, intimal index and the extent of thethree-layered appearance were significantly higher in thesubgroup with rejection periods; the intimal index was0-11 dt0-11 vs 0 0 5 ± 0 0 8 in recipients without rejection(Fig. 2a). The extension of the three-layered vessel wallwas 107° ± 117° vs 54° ± 88° in recipients without rejec-tion (Fig. 2b). In addition, a significant difference was
Eur Heart J, Vol. 17, December 1996
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/17/12/1891/532939 by guest on 08 February 2022
1894 S. Kerber et al.
0.3
inde
xIn
tim
al p to
0.1
n n
(a)
*25
o27
- 29
118no
12yes
G
300
200
100
(b)
-
—
-
* 25
* 29
j18no
12yes
Rejection
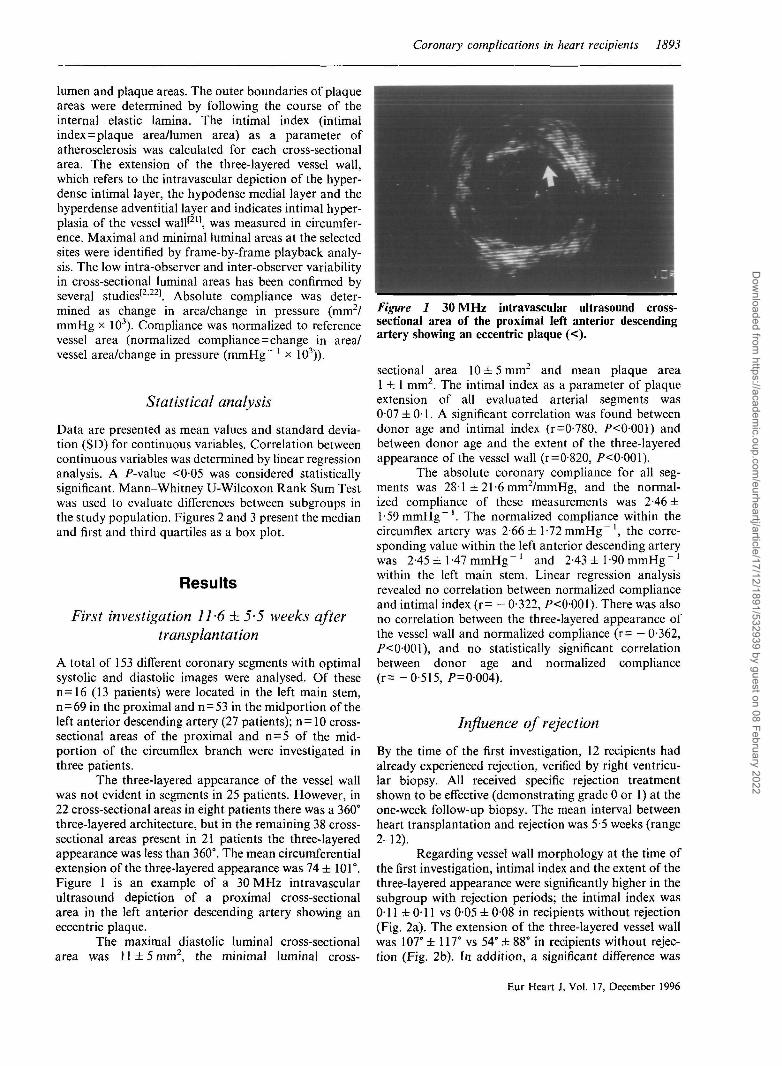
Figure 2 Comparison of atherosclerotic vessel altera-tions in recipients without (left) and with (right) rejectionbefore the first investigation. Panel 2a: Comparison of theintimal index in recipients with and without rejection.Panel 2b: Comparison of circumferential extension ofhyperplasia in recipients with and without rejection.
found in normalized compliance between recipientsexperiencing and those not experiencing rejection: 18recipients with no rejection demonstrated a significantlyhigher normalized compliance (2-95 ± 1-22 mmHg"1)than those without/>=0005) (Fig. 3).
rejection (1-76 ± 081 mmHg"
Repeat study
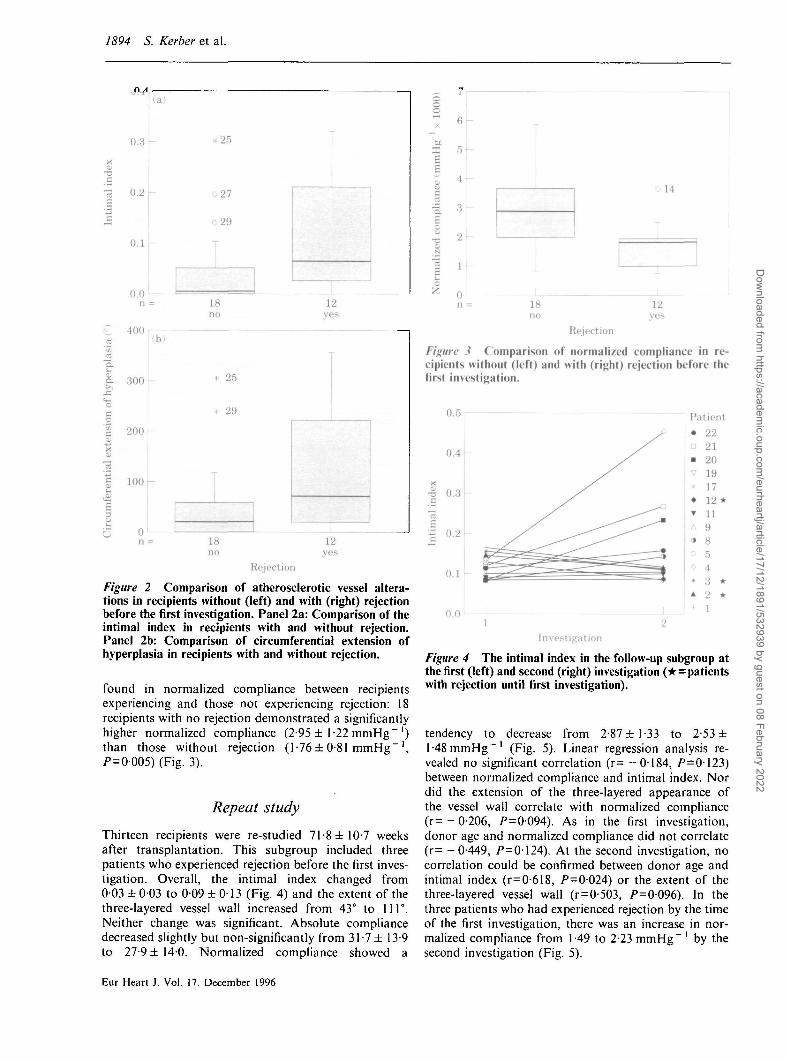
Thirteen recipients were re-studied 71-8 ±107 weeksafter transplantation. This subgroup included threepatients who experienced rejection before the first inves-tigation. Overall, the intimal index changed from003 ± 003 to 0-09 ± 0 1 3 (Fig. 4) and the extent of thethree-layered vessel wall increased from 43° to 111°.Neither change was significant. Absolute compliancedecreased slightly but non-significantly from 31 -7 ± 13-9to 27-9 ± 140. Normalized compliance showed a
r 5
^ 4c
—
£
N
c !
^ n
ol4
T
1 -
1 118no
12ves
Rejection
Figure .? Comparison of normalized compliance in re-cipients without (left) and with (right) rejection before thefirst investigation.
Investigation
Figure 4 The intimal index in the follow-up subgroup atthe first (left) and second (right) investigation (* = patientswith rejection until first investigation).
tendency to decrease from 2-87 ± 1 -33 to 2-53 ±1 -48 mmHg"1 (Fig. 5). Linear regression analysis re-vealed no significant correlation (r= —0184, /)=0123)between normalized compliance and intimal index. Nordid the extension of the three-layered appearance ofthe vessel wall correlate with normalized compliance(r=-0-206, /)=0094). As in the first investigation,donor age and normalized compliance did not correlate(r= -0-449, />=0124). At the second investigation, nocorrelation could be confirmed between donor age andintimal index (r=0-618, P-Q-Q2A) or the extent of thethree-layered vessel wall (r = 0-503, />=0096). In thethree patients who had experienced rejection by the timeof the first investigation, there was an increase in nor-malized compliance from 1-49 to 2-23 mmHg"' by thesecond investigation (Fig. 5).
Eur Heart J, Vol. 17. December 1996
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/17/12/1891/532939 by guest on 08 February 2022
Coronary complications in heart recipients 1895
ooo
ej:I.2
o
Patient
Investigation
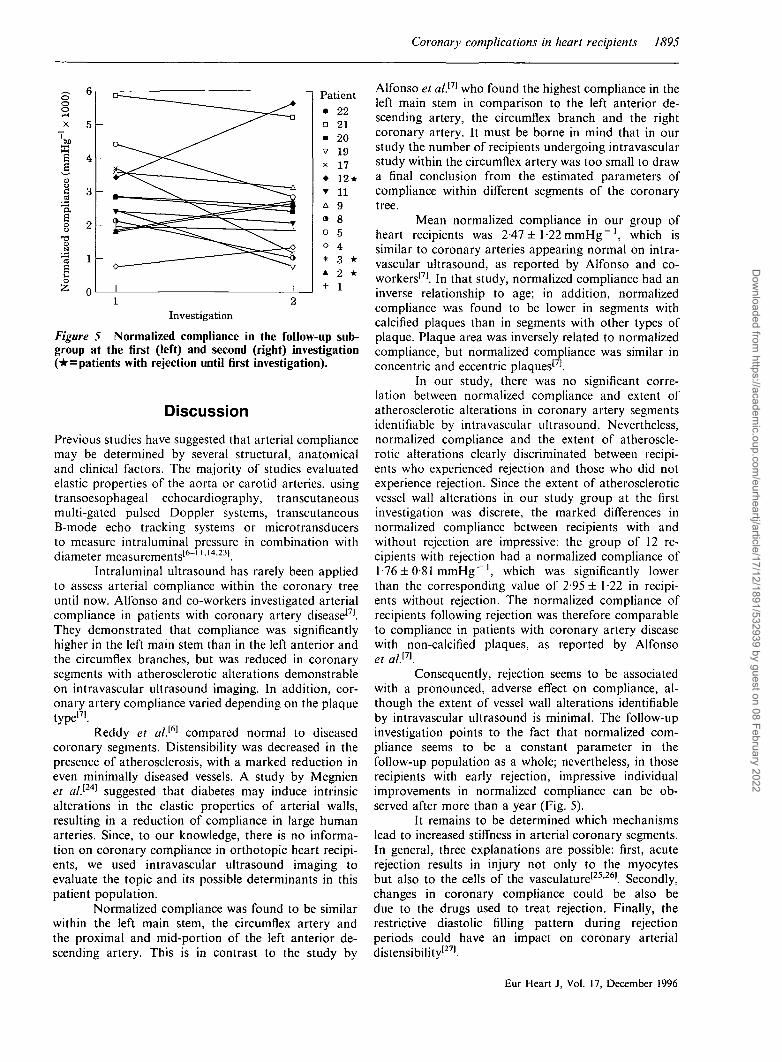
Figure 5 Normalized compliance in the follow-up sub-group at the first (left) and second (right) investigation(* =patients with rejection until first investigation).
DiscussionPrevious studies have suggested that arterial compliancemay be determined by several structural, anatomicaland clinical factors. The majority of studies evaluatedelastic properties of the aorta or carotid arteries, usingtransoesophageal echocardiography, transcutaneousmulti-gated pulsed Doppler systems, transcutaneousB-mode echo tracking systems or microtransducersto measure intraluminal pressure in combination withdiameter measurements'6"1 U 4-2 31.
Intraluminal ultrasound has rarely been appliedto assess arterial compliance within the coronary treeuntil now. Alfonso and co-workers investigated arterialcompliance in patients with coronary artery disease'71.They demonstrated that compliance was significantlyhigher in the left main stem than in the left anterior andthe circumflex branches, but was reduced in coronarysegments with atherosclerotic alterations demonstrableon intravascular ultrasound imaging. In addition, cor-onary artery compliance varied depending on the plaquetype'71.
Reddy et al.[6] compared normal to diseasedcoronary segments. Distensibility was decreased in thepresence of atherosclerosis, with a marked reduction ineven minimally diseased vessels. A study by Megnienet al.[24] suggested that diabetes may induce intrinsicalterations in the elastic properties of arterial walls,resulting in a reduction of compliance in large humanarteries. Since, to our knowledge, there is no informa-tion on coronary compliance in orthotopic heart recipi-ents, we used intravascular ultrasound imaging toevaluate the topic and its possible determinants in thispatient population.
Normalized compliance was found to be similarwithin the left main stem, the circumflex artery andthe proximal and mid-portion of the left anterior de-scending artery. This is in contrast to the study by
Alfonso et a/.'71 who found the highest compliance in theleft main stem in comparison to the left anterior de-scending artery, the circumflex branch and the rightcoronary artery. It must be borne in mind that in ourstudy the number of recipients undergoing intravascularstudy within the circumflex artery was too small to drawa final conclusion from the estimated parameters ofcompliance within different segments of the coronarytree.
Mean normalized compliance in our group ofheart recipients was 2-47 ± 1-22 mmHg" ', which issimilar to coronary arteries appearing normal on intra-vascular ultrasound, as reported by Alfonso and co-workers'71. In that study, normalized compliance had aninverse relationship to age; in addition, normalizedcompliance was found to be lower in segments withcalcified plaques than in segments with other types ofplaque. Plaque area was inversely related to normalizedcompliance, but normalized compliance was similar inconcentric and eccentric plaques'71.
In our study, there was no significant corre-lation between normalized compliance and extent ofatherosclerotic alterations in coronary artery segmentsidentifiable by intravascular ultrasound. Nevertheless,normalized compliance and the extent of atheroscle-rotic alterations clearly discriminated between recipi-ents who experienced rejection and those who did notexperience rejection. Since the extent of atheroscleroticvessel wall alterations in our study group at the firstinvestigation was discrete, the marked differences innormalized compliance between recipients with andwithout rejection are impressive: the group of 12 re-cipients with rejection had a normalized compliance of1-76 ± 0-81 mmHg' 1 , which was significantly lowerthan the corresponding value of 2-95 ± 1-22 in recipi-ents without rejection. The normalized compliance ofrecipients following rejection was therefore comparableto compliance in patients with coronary artery diseasewith non-calcified plaques, as reported by Alfonsoet alP\
Consequently, rejection seems to be associatedwith a pronounced, adverse effect on compliance, al-though the extent of vessel wall alterations identifiableby intravascular ultrasound is minimal. The follow-upinvestigation points to the fact that normalized com-pliance seems to be a constant parameter in thefollow-up population as a whole; nevertheless, in thoserecipients with early rejection, impressive individualimprovements in normalized compliance can be ob-served after more than a year (Fig. 5).
It remains to be determined which mechanismslead to increased stiffness in arterial coronary segments.In general, three explanations are possible: first, acuterejection results in injury not only to the myocytesbut also to the cells of the vasculature'25'26'. Secondly,changes in coronary compliance could be also bedue to the drugs used to treat rejection. Finally, therestrictive diastolic filling pattern during rejectionperiods could have an impact on coronary arterialdistensibilitv'27'.
Eur Heart J, Vol. 17, December 1996
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/17/12/1891/532939 by guest on 08 February 2022

1896 S. Kerber et al.
Limitations
The following methodological limitations should betaken into account.
(1) Intracoronary pressure was not measured within thecoronary arteries. We therefore had to assume that thepressure recorded with the guiding catheter correspondsto the pressure at the imaging site of the intravascularultrasound transducer. Recent studies have demon-strated a difference of less than 10% between intra-aorticand intracoronary pressure'61. No doubt, an on-linemeasurement of the pressure at the tip of the intra-vascular ultrasound catheter would have been a moreprecise assessment.(2) 30 MHz intravascular ultrasound systems do notallow an authentic presentation of discrete atheroscle-rotic vessel wall alterations, as reported by Fitzgeraldand co-workers[211. The application of a 40 MHz systemwould significantly improve the resolution of the depic-tion of vessel wall alterations, especially discriminationbetween the vascular layers.(3) Even though the applied 3-5-F ultrasound catheter isrelatively small with regard to the vessel lumen, thepresence of such a catheter may not only alter the flowpattern but also the elastic properties of the vessel wallat that location.(4) A larger patient cohort is necessary to finally estab-lish our preliminary results and their relationship toclinical and immunological parameters. Too fewpatients had follow-up studies in our analysis. In ad-dition, the number of patients with an intravascularultrasound investigation within the circumflex artery istoo small to draw any general conclusions about thiscoronary segment.(5) A comparative study of both coronary arterial com-pliance and left ventricular diastolic relaxation shouldelucidate whether immunological determinants contrib-ute to a deterioration in compliance as a whole in heartrecipients following rejection periods.
Conclusion
The observation in our study suggests that immuno-logical responses may alter the elastic properties of thecoronary vessel wall. Intravascular ultrasound imagingcan be used to demonstrate atherosclerotic vessel wallalterations and functional alterations such as those ofcompliance. These structural and functional observa-tions may contribute to the interpretation of clinicaland immunological parameters in orthotopic heartrecipients.
References
[1] Liebson PR. Klein LW. Intravascular ultrasound in coronaryatherosclerosis: a new approach to clinical assessment. AmHeart J 1992; 123: 1643-60.
[2] Nissen SE, Gurley JC, Grines CL et al. Intravascular ultra-sound assessment of lumen size and wall morphology innormal subjects and patients with coronary artery disease.Circulation 1991; 84: 1087-99.
[3] Kerber S, Fechtrup C, Budde T, Fahrenkamp A, Bocker W,Breithardt G. Validation of intravascular ultrasound in arte-riosclerotic peripheral vessels. Int J Cardiol 1994; 43: 191-8.
[4] Kerber S, Link TM, Fechtrup C et al. Intravaskularer Ultra-schall bei peripheren verkalkten GefapMasionen: Vergleich zurdirektradiographischen Vergroperung. Z Kardiol 1993: 82:610-17.
[5] Kearney P, Erbel R. Imaging in the catheterization labora-tory. Curr Opin Cardiol 1993; 8: 988-99
[6] Reddy KG, Suneja R, Nair RN, Dhawale P, Hodgson J.Measurement by intracoronary ultrasound of in vivo arterialdistensibility within atherosclerotic lesions Am J Cardiol1993; 72: 1232-7.
[7] Alfonso F, Macaya C, Goicolea J et al. Determinants ofcoronary compliance in patients with coronary artery disease:an intravascular ultrasound study. J Am Coll Cardiol 1994;23: 879-84
[8] Armentano RL, Levenson J, Barra JG et al. Assessment ofelastin and collagen contribution to aortic elasticity in con-scious dogs. Am J Physiol 1991; 260: 1870-7.
[9] Barra JG, Armentano RL, Levenson J, Fischer EIC, PichelRH, Simon A. Assessment of smooth muscle contribution todescending thoracic aortic elastic mechanics in consciousdogs. Circ Res 1993; 73: 1040-50.
[10] Doerr R, Heintz B, Krebbs W. Quantitative assessment of theelastic properties of human arteries by intravascular ultra-sound: pathological arterial stiffening proximal to the aorticbifurcation (Abstr). J Am Coll Cardiol 1992; 19 (Suppl A):300A.
[11] Avolio AP, Deng FD, Li W et al. Effects of aging on arterialdistensibility in populations with high and low prevalence ofhypertension: comparison between urban and rural communi-ties in China. Circulation 1984; 71: 202-10.
[12] Barenbrock M, Spieker C, Laske V et al. Effect of long-termhemodialysis on arterial compliance in end-stage renal failure.Nephron 1993 65: 249-53.
[13] Barenbrock M, Spieker C, Hoeks APG, Zidek W, Rahn K.Effect of Lisinopril and metoprolol on arterial distensibility.Hypertension 1994; 23 (Suppl I): I-161-I-163.
[14] Nakatani S, Yamagishi M, Tamai J et al. Assessment ofcoronary artery distensibility by intravascular ultrasound.Application of simultaneous measurements of luminal areaand pressure. Circulation 1995; 91: 2904-10.
[15] Schroeder JS, Gao S, Hunt SA, Stinson EB. Accelerated graftcoronary artery disease: diagnosis and prevention. J HeartLung Transplant 1992; 84: 2190-2.
[16] Miller LW. Transplant coronary artery disease. J Heart LungTransplant 1992; 11: S1-S4.
[17] Pinto FJ, Chenzbraum A, Botas J et al. Feasibility of serialintracoronary ultrasound imaging for assessment of progres-sion of intimal proliferation in cardiac transplant recipients.Circulation 1994; 90: 2348-55.
[18] Kerber S, Rahmel A, Karbenn U et al. Allograft-Vaskulopathie in der Friihphase nach orthotoper Herztrans-plantation: angiographische, intravaskular-sonographischeund funktionelle In-vivo-Befunde. Z Kardiol 1994; 83: 215-24.
[19] Billingham ME, Cary N, Hammond E. Working formulationfor the standardization of nomenclature in the diagnosis ofheart and lung rejection: heart rejection study group. J HeartTransplant 1990; 9: 587-92.
[20] Billingham ME. Diagnosis of cardiac rejection by endomyo-cardial biopsy. J Heart Transplant 1981; 1: 25-30.
[21] Fitzgerald PJ, Goar FGS, Connolly AJ et al. Intravascularultrasound imaging of coronary arteries. Is three layers thenorm? Circulation 1992; 86: 154-8.
[22] Hausmann D, Lundkvist AJS, Friedrich GJ, Mullen WL,Fitzgerald PJ, Yock PG. Intracoronary ultrasound imaging:intraobserver and interobserver variability of morphometricmeasurements Am Heart J 1994; 128: 674-80.
Eur Heart J. Vol 17. December 1996
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/17/12/1891/532939 by guest on 08 February 2022

Coronary complications in heart recipients 1897
[23] Miigge A, Daniel WG, Niedermeyer J, Hausman D, Nikutta [25] Rose AG, Uys CJ. Pathology of cardiac transplantation. In.P, Lichtlen PR. Usefulness of a new automatic boundary Silver MD, ed. Cardiovascular Pathology. Vol. 2. New York-detection system for assessing stiffness of the descending Churchill Livingstone, 1991: 1649-82.thoracic aorta by transesophageal echocardiography. Am J [26] Ellis B, Madge G, Kolkatkar M, Still W. Clinical and patho-Cardiol 1992; 70: 1629-31. logical findings in human cardiac rejection. Arch Pathol 1971;
[24] Megnien JL, Simon A, Valensi P, Flaud P, Merli I, Levenson 92: 58.J. Comparative effects of diabetes mellitus and hypertension [27] Dawkins KD, Oldershaw PJ, Billingham ME. Changes inon physical properties of human large arteries. J Am Coll diastolic function as a non-invasive marker of cardiac allo-Cardiol 1992; 20: 1562-8. graft rejection. J Heart Transplant 1984; 3: 286-94.
Eur Heart J, Vol. 17, December 1996
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/17/12/1891/532939 by guest on 08 February 2022