Embed Size (px)
Citation preview

This article was downloaded by: [University of Chicago Library]On: 05 October 2014, At: 22:52Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registered office: MortimerHouse, 37-41 Mortimer Street, London W1T 3JH, UK
Aging & Mental HealthPublication details, including instructions for authors and subscription information:http://www.tandfonline.com/loi/camh20
Correspondence of perceptions about centenarians’mental healthMaurice MacDonald a , Peter Martin a , Jennifer Margrett a & Leonard W. Poon ba Human Development and Family Studies , Iowa State University , 1321 Palmer Building,Ames, IA 50011-4380, USAb University of Georgia , Institute of Gerontology , Athens, GA 30602Published online: 02 Nov 2009.
To cite this article: Maurice MacDonald , Peter Martin , Jennifer Margrett & Leonard W. Poon (2009) Correspondence ofperceptions about centenarians’ mental health, Aging & Mental Health, 13:6, 827-837, DOI: 10.1080/13607860902918249
To link to this article: http://dx.doi.org/10.1080/13607860902918249
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all the information (the “Content”) containedin the publications on our platform. However, Taylor & Francis, our agents, and our licensors make norepresentations or warranties whatsoever as to the accuracy, completeness, or suitability for any purpose ofthe Content. Any opinions and views expressed in this publication are the opinions and views of the authors,and are not the views of or endorsed by Taylor & Francis. The accuracy of the Content should not be reliedupon and should be independently verified with primary sources of information. Taylor and Francis shallnot be liable for any losses, actions, claims, proceedings, demands, costs, expenses, damages, and otherliabilities whatsoever or howsoever caused arising directly or indirectly in connection with, in relation to orarising out of the use of the Content.
This article may be used for research, teaching, and private study purposes. Any substantial or systematicreproduction, redistribution, reselling, loan, sub-licensing, systematic supply, or distribution in anyform to anyone is expressly forbidden. Terms & Conditions of access and use can be found at http://www.tandfonline.com/page/terms-and-conditions

Aging & Mental HealthVol. 13, No. 6, November 2009, 827–837
Correspondence of perceptions about centenarians’ mental health
Maurice MacDonalda*, Peter Martina, Jennifer Margretta and Leonard W. Poonby
aHuman Development and Family Studies, Iowa State University, 1321 Palmer Building, Ames,IA 50011-4380, USA; bUniversity of Georgia, Institute of Gerontology, Athens, GA 30602
(Received 28 August 2008; final version received 19 March 2009)
Objectives: The goals of this study were to uncover the criteria by which centenarians, proxy/caregivers, andinterviewers rated centenarians’ mental health. Often proxy and interviewer reports are obtained in studies of theoldest-old and become a primary source of information.Methods: Data were from a population-based sample of mentally competent US centenarians in northernGeorgia. The dependent variables were based on alternative reports for the centenarians’ mental or emotionalhealth. Regression analysis was used to predict each source’s rating of mental health separately with the same setof variables. These variables included information obtained from the centenarians and proxies about their distalexperiences, demographics, and proximal resources including Mini-Mental Status Examination (MMSE), health,personality, socioeconomic resources, and coping behaviors.Results: Examination of mean-level differences between sources revealed similarity across mental health ratings.For centenarians and proxies, perceived economic status was a very important predictor of mental health.For centenarians and interviewers, personality (neuroticism and extraversion) was an important commonpredictor. The interviewer and proxy mental health ratings were strongly associated with MMSE, but that wasnot the case for centenarians.Conclusion: Mean-level findings and the comparative regression results provide corroborating evidence thatcentenarians’ self-reports of mental health are similar based on average ratings and presence of commonassociations with other raters (i.e., perceived economic status and personality). Implications of differences acrossrater pairs are discussed as guidance about the comparative value of substitution of proxies as informants foraddressing specific influences on mental health.
Keywords: extreme old age; mental health assessment; quality of life/well-being
Introduction
With increased longevity and the expansion of the
oldest-old population, attention to understanding the
consequences of surviving to extreme age has grown
substantially (Poon & Perls, 2007). Understanding the
correlates of psychological well-being among the
oldest-old is important because that may lead to
prescriptions for enhancing life quality in extreme age
and also suggest important factors associated with
longevity. Still, concerns have been expressed about
whether centenarians and oldest-old adults are fully
reliable in their mental health assessments as compared
to younger-old. For example, Pinquart and Sorenson
(2000) suggested that those among the very old who
suffer less from incapacitating losses may have espe-
cially high subjective well-being because they compare
themselves to those who have experienced more losses.
Thus, more investigation is needed to assess self-
reported mental health among oldest-old adults and
to refine understanding of the factors contributing to
their positive mental health. The main objectives of this
study were to: (a) investigate mean-level differences
in mental health ratings as assessed by centenarians
themselves and two other raters, and (b) examine the
relation of each sources’ rating with proximal and
distal resources in order to determine the factors
influencing each rater.Gerontologists have long relied on proxy reporters
to obtain data about the oldest-old, but there has not
been much attention paid to the comparative value of
that kind of alternative reporting. Except for measur-
ing constructs that are about others’ perspectives on
study participants, the use of proxy informants is
dictated by necessity if the oldest-old person is unable
to self-report, or to reduce respondent burden by
obtaining proxy reports about aspects the proxies are
presumed to know well enough. That is, proxy reports
are desirable for increasing analysis sample size
and for efficiency in data collection. Additionally for
situations where multiple indicators are needed or
appropriate to reduce measurement error with latent
factor analysis techniques, proxy reports can provide
valuable supplementary information.Prior studies suggest that informant perceptions
may vary, but that each may add a potentially valuable
perspective on the characteristics of the oldest-old, and
together reports from varied sources provide a unique
opportunity to compare and contrast ratings of mental
*Corresponding author. Email: [email protected] the Georgia Centenarian Study. Additional authors include S.M. Jazwinski, R.C. Green, M. Gearing, W.R. Markesbery,J.L. Woodard, M.A. Johnson, J.S. Tenover, I.C. Siegler, W.L. Rodgers, D.B. Hausman, C. Rott, A. Davey, and J. Arnold.
ISSN 1360–7863 print/ISSN 1364–6915 online
� 2009 Taylor & Francis
DOI: 10.1080/13607860902918249
http://www.informaworld.com
Dow
nloa
ded
by [
Uni
vers
ity o
f C
hica
go L
ibra
ry]
at 2
2:52
05
Oct
ober
201
4

health and the relationship of those ratings to a varietyof relevant domains. Under certain circumstances,proxy data are reliable as a source of information. Forexample, elder-proxy concordance is typically high forsuch items as activities of daily living (ADL), medicalhistory, and instrumental activities of daily living(Schatzberg, Sudha, & Mutran, 1998). Data frompersonality research suggests that even though thereare mean differences in some personality trait ratings,these differences are only in degree and not insubstance (Martin, 2007). Collectively considered,results from these studies indicate that the use ofproxies to collect data across selected domains isimportant (Walsh, Wu, Mitchell, & Berkmann, 2003).However others have suggested that proxy scorescannot simply be used as substitutes (Kane et al.,2005), but should be viewed as additional importantinformation. Additionally some results have ledinvestigators to be concerned about the accuracy ofproxy informants. Kolanowski, Hoffman, and Hofer(2007) reported that the concordance of self report andinformant assessment of emotional well-being amongnursing home residents was quite low. Lum, Lin,and Kane (2005) noted that the agreement on ADLassessments based on nursing home residents andfamily or staff report differed as well.
Given the difficulty of interviewing extremelyold individuals who have more physical and mentalimpairments than any other adult age group, our studymay suggest whether proxy reporters are neededto obtain reliable reports about their mental health.The centenarian, the proxy, and the interviewer wereall considered subjects for analysis, so our strategy wasto obtain multivariate estimates of the effects ofthe same set of predictors within separate analysissamples for each of the three types of mental healthreports. Similar results for different reporters wouldcorroborate the importance of specific variables forcentenarians’ mental health. Differences between thecentenarians’ versus others’ results would suggestcaution for firm conclusions about the reliability ofcentenarians’ own mental health reports, but may alsoestablish what areas of centenarians’ lives seem moresalient to the proxy/caregiver and the study interviewerfrom their perspectives. As a practical matter, theremay be a concern that if proxies (who are oftencaregivers) have very different views of what consti-tutes healthy mental status than centenarians, theremay be a disconnect about priorities for maintainingor enhancing resources for a mentally healthy lifestyleamong exceptional survivors.
Conceptual framework and literature review
Our analysis comparing correlates of alternativereports of mental health is also intended to providenew evidence about factors that enhance or hindercentenarians’ psychological well-being. Because cente-narians are rare survivors and have not been studied
extensively, it is important to consider evidence aboutthem in the broader context of what has been learnedfrom research with samples of other old-age groups.Additionally, centenarian studies have used a varietyof psychological well-being measures so that it wasnecessary to consider measures other than mentalhealth per se to guide the analysis, thereby includingmorale, life-satisfaction, happiness, etc.
The theoretical basis for the analyses reportedhere is the model of proximal and distal resourceinfluences in developmental adaptation to aging(Martin & Martin, 2002). That model guided prioritiesfor the Georgia Centenarian Study, which provides thedata for our analyses. In essence, the developmentaladaptation model suggests that distal and proximalexperiences, as well as personal and social resources,determine to what extent old and very old adultsmaintain relatively high levels of physical and mentalfunctioning. Additionally, a survey of the recentliterature concerning what contributes to mentalhealth and other aspects of psychological well-beingfor the oldest-old guided choices about predictorvariables available from the study. For the empiricalliterature search of this study, we considered researchon the mental health, morale, happiness and overalllife satisfaction of oldest-old adults. In that sense wehave pursued the line of research begun by GerdaFillenbaum, which focused on self and interviewerratings of mental health as part of the Older AmericansResources and Services (OARS) multidimensionalfunctional assessment of older adults (Fillenbaum,1988). The OARS mental health ratings are designedto help the informants make a summary assessment.For the interviewer these judgments are to be basedon the overall impression of the participant frominformation contained in the survey questionnaire andfrom all other sources (Fillbenbaum, 1988, p. 73).
Mental health
For the purposes of this study, mental health refersto the emotional aspects of mental well-being. Therehave been only a few studies of mental health amongthe oldest-old (MacDonald, 2007). Selim et al. (2005)emphasized psychological resilience as the criticalfactor for US centenarian veterans’ mental healthadvantage based on the OARS question. Martin (2002)found that both economic resources and socialresources were positively related to mental health(OARS rating by the interviewer) in the first phaseof the Georgia Centenarian Study. An additionalinsight Martin obtained was that adverse cumulativelife event experiences of Georgia centenarians reducedboth social and economic resources, and adverseevents also had a direct, negative effect on mentalhealth. Landau and Litwin (2001) also analyzed theinfluence of background variables, physical capacity,and perceptions of social network supportivenesson mental health among Israelis aged 75 and olderusing the Zung Depression Scale (Zung & Zung, 1986).
828 M. MacDonald et al.
Dow
nloa
ded
by [
Uni
vers
ity o
f C
hica
go L
ibra
ry]
at 2
2:52
05
Oct
ober
201
4

They found that locus of control and networksupportiveness were positive influences and educationwas positively related to locus of control. Availablecentenarian studies have also begun to elucidate thelinkages among a variety of influences that havedirect as well as indirect effects on mental health,particularly for research focused on the personalitydomain. Although Adkins, Martin, and Poon (1996)found that extraversion was positively related tomorale of Georgia centenarians, Martin (2002) rejectedthe hypothesis that extraversion mediated the influ-ence of negative event history on the interviewer’sOARS mental health rating for them.
Life satisfaction
This construct refers to overall well-being, or feelingsabout life as a whole, and thus may involve summaryassessments across sub-domains such as for subjectivephysical health, perceived economic status, emotionalhealth or mental health, etc. Hence although evidenceabout the correlates of life satisfaction may be useful tosuggest influences on mental health, it is also the casethat life satisfaction is a much broader construct.However the paucity of research on the mental healthof the oldest-old and centenarians in particularrequires that we consider studies of life satisfactionbecause they are potentially relevant. The authorsof the cross-sectional studies of elderly populationsthat characterize oldest-old adults as remarkably well-off psychologically relative to younger groups havesummarized their conclusions about three importantdomains, which are: health-related behaviors, psycho-logical resilience, and social resources. Berg, Hassing,McClearn, and Johannson (2006) conducted one ofthe few analyses designed to examine the relativeimpact on life satisfaction of psychosocial and healthvariables among 315 Swedish participants aged 80–98years, and concluded that social network quality, self-rated overall health, sense of being in control of one’slife and depressive symptoms were significant factors(in that order of importance) but that the specificinfluences were different for men than women. Ozaki,Uchiyama, Tagaya, Oshida, and Ogihara (2007)reported that the most well-off (‘autonomous’)Japanese centenarians had better nutritional habits,had never smoked, rarely or never drank alcohol, andexercised regularly. Hilleras, Jorm, Herlitz, andWinblad (1999) also documented that among Swedes90 years or older, those with high life satisfaction spentmore time in physical activity during a day. Similarly,Yi and Vaupel (2002, p. 733) attributed Chinese old-old individuals’ ability to maintain life satisfaction to‘being more positive in self-feeling of life’. For Italiancentenarians, there was a stronger relationship betweensatisfaction with social and family relations and lifesatisfaction than for octogenarian and nonagenarianItalians (Dello Buono, Urciuoli, & de Leo, 1998).From their meta-analysis, Pinquart and Sorenson(2000) concluded that social networks were more
important influences on subjective well-being for theoldest-old, as was personal competence. In their mostcomprehensive analysis based on the Berlin AgingStudy, Smith, Fleeson, Geiselmann, Settersten, andKunzmann (1999) conducted a path analysis foroverall well-being, which linked sociodemographiccharacteristics, objective life conditions (includinghealth status, income, and social participation) tosub-domains of subjective well-being as causal influ-ences. Apart from subjective health, satisfaction withsocial participation and social relationships (together)had the strongest effects on overall well-being.
To summarize, the literature for oldest old adultsand for centenarians in particular characterizes them asresilient with respect to mental health and life satis-faction despite their health disadvantages relative tothe young-old. Based on multivariate studies reviewedhere, the sources of mental resiliency at extreme ageinclude health habits, personality, locus of control, andsocial resources (social network support and inter-personal relationships). With the exception of onestudy of centenarians’ mental health that relied on aninterviewers’ report (Martin, 2002), research to datehas been based on self-assessment of mental health andwell-being and there have been no comparisons withmental health assessments by proxies or interviewers.Although Pinquart and Sorenson (2000) suggested thatdownward comparisons may help to explain psycho-logical resilience in extreme age, research to datehas not tested whether self-assessments are reliablein comparison with other informants’ assessments.We have no guidance from prior research on mentalhealth or life satisfaction that compares alternativeraters and so formulated only some general hypothesesfor this exploratory study.
Hypotheses
Based on our review of prior research, there were twomain hypotheses:
(1) Proxy and interviewer informants will ratemental health of centenarians lower than thecentenarians’ self-assessments.
(2) Among domains of influence, physical health,personality, and social support were expected tobe stronger predictors of mental health ratingsthan distal experiences (i.e., events that occurredmore than 20 years ago) or other types ofresources (e.g., income, or community supportservices).
Methods
Data and samples
The recruitment of participants in a 44-county areaof Northern Georgia from lists of nursing facilities andpersonal care homes and for registered voters withdate-of-birth information resulted in an 83% response
Aging & Mental Health 829
Dow
nloa
ded
by [
Uni
vers
ity o
f C
hica
go L
ibra
ry]
at 2
2:52
05
Oct
ober
201
4

rate for a population-based sample of 239 community-
dwelling and institutionalized centenarians and near-
centenarians. Because our study was not intendedto make comparisons to other birth cohorts, the issue
of selection into our sample due to mortality has notyet been analyzed; yet we must still exercise caution
with respect to interpretation of the influence of theparticipants’ characteristics on mental health because
they are a very special group of extreme survivors witha high mortality rate once they reach centenarian
status. Based on the survival analysis using the first
two phases of the Georgia Centenarian Study for acommunity-dwelling sample Poon et al. (2000) found
that gender, race, and functional health were signifi-cantly related to mortality within 18 months for their
participants ranging in age from 99 to 110 years.On the other hand, compared to most other studies of
centenarians, our sampling frame for this study isnot restricted to community-dwelling centenarians and
thus represents the entire population of survivorsbetter on that account. In order to participate in
the interview section about resources and subjective
well-being, centenarians needed to score 17 or higheron the Mini-Mental Status Examination (MMSE:
Folstein, Folstein, & McHugh, 1975). The reason forthis relatively low MMSE cutoff score is that lower
education levels for this cohort and the inclusion ofdifferent ethnic groups may yield lower MMSE scores
than would be expected in more highly educated ormajority populations (Tombaugh & McIntyre, 1992).
In very old populations, vision impairment may also
account for lower MMSE scores (Holtsberg, Poon,Noble, & Martin, 1995). Although the relatively low
MMSE cutoff may include cases with mild cognitiveimpairment, that may permit a stronger test of inter-
rater reliability because proxy and interviewer ratingsshould deviate more from mildly impaired centenar-
ians’ ratings. After that restriction, the sample included137 centenarians and near centenarians (mean age of
99.7 years, age range from 98 to 108). The averageMMSE score was 23.58 (SD¼ 3.94).
Although 71.8% of centenarians reported that their
overall physical health was good or excellent, 44.9%lived in either a skilled nursing facility (23.5%) or
in assisted living residences (20.4%) while the remain-
ing 56.2% lived in their private home or apartment.Most of the participants were women (78.8%).
By ethnicity, 83.2% were White and the other 16.8%of the participants were African-American. Only 3.6%
were married; 6.6% were divorced, and 84.7% werewidowed.
Proxy informants were nominated by the centen-
arians to obtain a close family member first and thenother relatives, or if no relatives were available another
knowledgeable person (e.g. neighbors, nurses, etc.);61.1% of proxies were adult children, 13.9% nephews
and nieces, 9.9% granddaughters, and the other 15.1%of informants included spouses (2.2% of all proxies)
siblings, or friends. Of the proxies, the majority
were women. From the target sample of 239 proxy
informants, 230 (96%) filled out a questionnaire andmailed the questionnaire back to the interviewer.
Beyond inability to locate the selected proxy, we
suspect that the burden of cooperating with themultiple demands of our larger program project that
included physical testing and other contacts with theproxy may explain why some did not respond.
The single interviewer for the centenarians was
a trained social worker, and the interviewer completed
a rating form to provide additional informationabout the centenarian based on the interview. Hence
the interviewer was informed about everything that thecentenarian reported in the interview, including aspects
of the centenarians’ history as well as their perfor-
mance on the MMSE (which was part of the OARSprotocol).
Although some proxies were present during the
centenarians’ interview, most of them were not.Additionally, proxies were numerous, and varied in
the extent to which they had recently or ever known
about aspects of the centenarians’ histories andcharacteristics. With respect to our method of compar-
ing alternate sources’ reports of mental health andassociations with other variables, it is important to note
that while some participants may not be able to give
accurate reports of their own mental health, unrelia-bility between raters may be caused as well by
interviewers and proxies providing inaccurate assess-ments of centenarians’ mental health. Also, to obtain
information about economic resources we relied on
proxy reports whereas our other predictor variablesare based on centenarians’ self-reports.
Because collecting comprehensive information
from centenarians is very expensive and thus necessi-tates relatively small samples even before considering
missing data on specific variables, it seemed best to
maximize the number of cases for separate analyses foreach of the different mental health raters. In addition
to case number differences that result from the use ofthe proxy reporter (not all proxies were interviewed),
the centenarians and the proxies varied with respect
to missing values on variables included in theanalysis. To avoid restricting the entire analysis to
the smaller subset of cases available for each reporter
type with no missing data for any of the predictorvariables, the number of cases differs across the
regressions we obtained. In preliminary regressionsshown in Table 1, we used subsets of predictors
representing construct domains (e.g., economic
resources) so that the number of cases involved atthat step depended on the rater type as well as the
extent of list-wise deletion for missing data in eachsubset of predictors. In the final regressions for
Table 2, the respective sample sizes for each rater
type were: interviewer (n¼ 101); proxy, (n¼ 91); andcentenarian (n¼ 95).
830 M. MacDonald et al.
Dow
nloa
ded
by [
Uni
vers
ity o
f C
hica
go L
ibra
ry]
at 2
2:52
05
Oct
ober
201
4

Dependent variables
Our measures for the mental health dependent variableare based on the OARS protocol (Fillenbaum, 1988) toobtain reports from centenarians and the proxy/caregiver as well as from the interviewer. Thecentenarians were asked ‘How would you rate yourmental or emotional health at the present time—excellent, good, fair, or poor?’ The proxy reporter wasasked: ‘How would you rate his/her mental oremotional health or ability to think at the presenttime compared to the average person living indepen-dently—excellent, good, fair, or poor?’ There was onestudy interviewer and for each centenarian this inter-viewer filled out the rating form provided by theOARS to rate mental health. Specific instructionsincluded: ‘Rate the current mental functioning of the
person being evaluated along a six point scale. Markthe ONE answer which best describes the person’spresent functioning’. The interviewer had six categoriesto choose from: outstanding mental health, goodmental health, mildly mentally impaired, moderatelymentally impaired, severely mentally impaired, andcompletely mentally impaired. Each of the anchorpoints included specific definitions (e.g. for outstand-ing mental health: intellectually alert and clearly
enjoying life, manages routine and major problems inhis/her life with ease and is free from any psychiatricsymptoms). Thus the instructions to the interviewerand question for the proxy informant did not specifythat they were expected to separate the cognitivehealth aspect of mental health from the emotionalaspect, whereas the question for the centenarianreferred to mental or emotional health without refer-ence to mental impairment or ability. Of course inretrospect it would have been better for the purposesof this particular study to define ‘mental health’ for all
the raters to be primarily about emotional or psycho-logical well-being.
Upon examining the distribution of responses forthe three raters, it was quite apparent that convertingthe interviewer responses to a four-point scale wouldbe feasible for comparisons. The interviewer categoriesfor mildly or moderately mentally impaired correspondwell to the ‘fair’ response category in the centenarianand proxy scale. After also converting ‘severely andcompletely’ mentally impaired to correspond to ‘poor’,we obtained a four-point scale with four as high for theinterviewer’s rating. Hence for all sources, the mental
Table 1. Standardized regression coefficients for mentalhealth ratings by domain.
DomainSelf(�)
Interviewer(�)
Proxy(�)
Demographics n¼ 135 n¼ 133 n¼ 119Age 0.08 �0.02 0.01Female �0.17* 0.03 �0.05Nursing home residence �0.21* �0.48** �0.25**African-American 0.04 �0.04 �0.05Adjusted R2 0.04 0.20 0.06
Distal resources n¼ 125 n¼ 125 n¼ 111Engaged lifestyle �0.05 0.23* 0.13Distal events 0.09 0.23* 0.28*Education 0.11 �0.12 0.03Occupation 0.22* 0.06 0.05Adjusted R2 0.09 0.09 0.12
Health n¼ 132 n¼ 129 n¼ 114ADL 0.24* 0.02 0.12Subjective health 0.23* 0.19* 0.12MMSE 0.10 0.49*** 0.43***Adjusted R2 0.17 0.29 0.27
Personality n¼ 88 n¼ 88 n¼ 85Competence 0.05 0.06 0.01Extraversion 0.13 0.17 0.11Ideas 0.20y 0.07 0.18y
Neuroticism �0.27* �0.29** �0.01Trust 0.12 0.09 0.28*Adjusted R2 0.14 0.13 0.13
Social and economic n¼ 95 n¼ 95 n¼ 91Social provisions 0.19* 0.14 0.17y
Perceived economic status 0.42* 0.21* 0.36***Adjusted R2 0.20 0.05 0.17
Other economic resources n¼ 81 n¼ 81 n¼ 81Income 0.16 0.15 0.13Care services �0.21y �0.35* �0.27*Community services 0.15 0.03 0.01Health cost help �0.04 �0.02 0.15Adjusted R2 0.08 0.13 0.08
Stress and coping n¼ 127 n¼ 125 n¼ 111Proximal events �0.03 �0.03 0.01Religious coping �0.02 0.29* 0.18y
Support coping 0.05 �0.07 0.01
Adjusted R2 0.02 0.06 0.03
Note. *p50.05; **p50.01; ***p50.001; yp50.10.
Table 2. Standardized (Beta) coefficients for mental healthratings by centenarian, interviewer, and proxy/caregiver.
Centenarian Interviewer Proxy
n¼ 95 n¼ 101 n¼ 91Domain and predictors
DemographicsNursing home residence �0.28**
Distal resourcesEngaged lifestyle 0.05Distal events 0.22*
HealthADL 0.20*Subjective health 0.14 0.13 0.05Mental status 0.32** 0.36***
Personality
Extraversion 0.18y 0.20*Neuroticism �0.19* �0.20*
Social and economic
Social provisions 0.08 �0.04 0.11Perceived economic status 0.26** 0.29**
Stress and coping
Religious coping �0.11 0.13 0.07Adjusted R2 0.30 0.49 0.35
Note. *p50.05; **p50.01; ***p50.001; yp50.10.
Aging & Mental Health 831
Dow
nloa
ded
by [
Uni
vers
ity o
f C
hica
go L
ibra
ry]
at 2
2:52
05
Oct
ober
201
4

health ratings were coded from one to four with fouras the highest category.
Predictors
Table 1 contains the entire list of independentvariables, which are grouped by domains for demo-graphics and distal variables, and also for the proximalresource domains of health, personality, social andeconomic resources (social interactions and perceivedeconomic status), other economic resources (e.g.,income or assistance received from others), andaspects of stress and coping. As designated in thenext two segments, the information for the majorityof the predictor variables was obtained from thecentenarian interviews. However because there wassubstantially greater missing data in centenarians’reporting of economic variables (such as their annualincome in particular) compared to proxy informantsreports on those same variables, we relied on proxyinterviews to create predictors representing economicresources. Many proxies may know the financialsituation of the centenarians better than centenariansthemselves.
Variables from centenarian interviews
The demographic variables include exact age, gen-der (female¼ 1, male¼ 0), residence (residence in anursing home¼ 1, otherwise 0) and ethnicity (African-American¼ 1, otherwise 0; all of the non-whiteparticipants identified themselves as African-American). Past engaged lifestyle activities weredefined by answers about a series of cognitive engage-ment tasks (Hultsch, Hertzog, Small, & Dixon, 1999)to construct a scale based on eight dichotomousquestions about activities such as continued education,learning a foreign language, volunteer working,preparing income tax, taking a major vacation, orgiving a public talk (�¼ 0.54). Higher scores for theengaged lifestyle scale indicated greater engagement.Distal (and proximal) events were selected from a lifeevents lists for occurrences such as death of a parent,marriage, divorce, deaths of close family members,births or loss of children, job events, and majorfinancial losses. Proximal events were defined asoccurring two or fewer years ago, and distal eventshad happened more than 20 years ago. Both eventsvariables count the number of events reported so thatthe variables involved indicate a greater number ofevents as the highest values. Education was coded ineight categories for a continuous variable coded from 1to 8 to represent the range of education from 0–4 yearsto postgraduate education. Occupation was codedfrom 0 to 10 as a continuous variable correspondingto ten categories respectively from ‘homemaker’ toe.g. ‘unskilled’, ‘clerical, sales, technical’ and so on upto ‘professional’ coded as 10. This occupational codingis admittedly crude but sufficient for our purpose,which was simply to distinguish between more skilled
and less skilled occupations. For health, participantsresponded to the Duke Older Adults Resources andServices (OARS) questions about overall subjectivehealth, and activities of daily living (Fillenbaum, 1988)from which a scale for functional health was con-structed (�¼ 0.85). The participants’ Mini-MentalStatus Exam score (MMSE) measured their cognitiveability (Folstein et al., 1975). Psychological resourceswere assessed through self-reports administered forthe NEO-PI R (Costa & McCrae, 1994), for a subsetof personality traits chosen based on experience withthe first Georgia study: Extraversion (�¼ 0.61),Neuroticism (�¼ 0.85), Ideas (�¼ 0.54), Competence(�¼ 0.70), and Trust (�¼ 0.73). To measure socialresources, the centenarians’ responses on 12 items werecombined (�¼ 0.68) for the Social Provisions Scale(Cutrona & Russell, 1987). Examples of social provi-sion items are: ‘There are people I can depend on tohelp me, if I really need it’; and ‘There is no one I cantrust to turn to for guidance’. Perceived economicstatus was measured on a three-item scale (�¼ 0.74)from the OARS questions pertaining to income ade-quacy (Fillenbaum, 1988). Selected items concerningreligious, and seeking support coping (�¼ 0.62) werebased on the Coping Response Indices Scale (Moos,Cronkite, Billing, & Finney, 1985).
Economic resource variables reported by the proxy
The variables in this domain were obtained from theproxy interview and were based primarily on OARSresource questions (Fillenbaum, 1988). Including theseitems permits a test of whether economic resourceshave effects on mental health separate from that forthe centenarians’ perceptions about resource adequacy.The income variable was obtained as a responsefor selection among thirteen annual income brackets,coded from 1 to 13 to represent rank-order by income.The Care Services variable is the sum of the numberof types of care received by the centenarian (rangingfrom zero to five, �¼ 0.81) and could include personalcare, nursing care, checking on the centenarians’ well-being, home chores, and meal preparation. A questionsequence adapted from the Asset and Health Dynamicssurvey (Soldo, Hurd, & Rodgers, 1997) determinedwhether the centenarians had received any specialservices such as from a social worker, an adult daycenter, outpatient rehabilitation, transportation, ormeals assistance. The proxy responses were codedto indicate whether any of those services had beenreceived (Community Services). A binary variable alsoindicates that the proxy reported the centenarian hadreceived help to pay for health costs that were notcovered by insurance, Medicare, or Medicaid (HealthCost Help).
Analysis
The analysis involved three steps. First, we obtainedthe means of the mental health reports for all three
832 M. MacDonald et al.
Dow
nloa
ded
by [
Uni
vers
ity o
f C
hica
go L
ibra
ry]
at 2
2:52
05
Oct
ober
201
4

raters and tested for differences in those averages tounderstand how the different raters may have assessedthe overall level of mental health for the centenarians.Second, restricted lists of independent variableswithin domains (e.g., distal resource variables) wereused to predict mental health with multiple regressionto learn which variables within domains had statisti-cally significant relationships with each mental healthrating. Third, for each mental health dependentvariable (i.e., for each type of rater), the significantpredictors from the within-domain regression resultswere considered as candidates for the final multipleregression specifications. Initially we planned toinclude all variables that were significant in thepreliminary regressions as final predictors. Howeverbased on related analysis of perceived economic statusand its relationship to caregiving services and physicalhealth we decided to exclude caregiving servicesfrom the final regressions to avoid multicollinearitywith ADL. Additionally based on another study inprogress we included extraversion as a predictor thatwe had found to be associated with mental healthin an analysis of the effects of caregiving services.Comparisons of the final regression results across theanalysis samples for mental health (centenarian,interviewer, and proxy reports) provided the basis fordiscussion of the different perspectives.
Results
Paired t-tests on the differences between means forthe respective pairs clearly rejected the hypothesisof any mean differences ( p40.05). The means of themental health ratings for the largest number of casesbefore any reductions for missing data were 1.92for the centenarians (N¼ 117), 1.94 for the proxyreporters (N¼ 117), and 1.98 for the interviewerratings (N¼ 131). In other words, with respect tothe average level of the mental health score forcentenarians, all rater sources were in agreement.Hence we can reject our first hypothesis, whichwas that proxy and interviewer informants wouldrate mental health lower than the centenarians’themselves.
Table 1 exhibits the standardized regression coeffi-cients for the mental health predictors within thedomains of interest for our three mental healthraters, and provides the adjusted R-squared measureof explanatory power for each domain. For all ratertypes, every domain included at least one variablethat had a significant ( p50.05) relationship to mentalhealth. There are obvious differences among theresults for the domains across raters. For example,the regressions for the health domain have the greatestexplanatory power for the interviewer and proxy(R2¼ 0.29 and 0.27, respectively) but for centenarians
the social and economic domain possessed greatestexplanatory power (R2
¼ 0.20). In absolute value the
largest effect size for the significant predictors varied
across raters. For centenarians and proxies, perceived
economic status was the most important predictor,whereas for interviewers it was nursing home residence.
Still, there were many similar results. Nursing home
residence had a substantial negative effect for all ratertypes, and for all raters the centenarians’ perceived
economic status had a positive effect. Furthermore,
there were common predictors across mental healthraters for every domain. Specifically there was cross-
rater pair corroboration of significance ( p50.05) or
a statistical trend ( p50.10) for distal events, nursinghome residence, MMSE, subjective health, personality
(neuroticism, and ideas), perceived economic status,the number of types of instrumental care received, and
religious coping.To account for the correlation of significant
predictor variables across domains for each rater typeand discover which ones are the most important
predictors for each of the alternative mental health
reports, the final step of the analysis was to include allof the significant predictors in a single regression
(except omitting care services based on concern formulticollinearity with ADL, and retaining extra-
version). Table 2 contains those final regressions.
Considering all raters, the domains represented withat least one significant predictor include demographics,
distal resources, health, personality, and social and
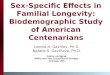
economic resources.Figure 1 depicts the significant effects for mental
health within regressions for each reporter type.
As the figure shows, there is one variable that issignificant but not corroborated by another reporter
for each analysis sample. Those are: functional health
(ADL) for centenarians; distal events for proxy/caregivers; and nursing home residence for inter-
viewers. For the centenarian and proxy rater pairs
perceived economic status is a highly significantpredictor of mental health. However for the proxies
personality and functional health were not significant
but those variables were significant predictors amongcentenarians. The interviewer results do corroborate
that neuroticism, and extraversion influenced percep-tions of centenarians’ mental health. The centenarian’s
MMSE score was a highly significant predictor of
mental health from the perspective of both the proxyand the interviewer, but the centenarians’ reports
of their mental health were not significantly related
to their MMSE. That pattern of results may haveoccurred because the OARS question about mental
health for the interviewer included reference to mental
impairment, and the question for the proxy includeda reference to the participant’s ability to think, but the
centenarians were asked simply to rate their mental or
emotional health. On the whole, there is agreementamong results for either the proxy or the interviewer
with the centenarians’ results that extraversion,neuroticism, and perceived economic status were
associated with mental health.
Aging & Mental Health 833
Dow
nloa
ded
by [
Uni
vers
ity o
f C
hica
go L
ibra
ry]
at 2
2:52
05
Oct
ober
201
4

With respect to our second hypothesis concerningthe relative importance of mental health predictorsbased on the literature review (such that physicalhealth, personality, and social support would be thebest predictors), we reject the hypothesis that socialsupport is important. Instead, perceived economicstatus was an additional important predictor forthe mental health as reported by the centenarian andthe proxy. We confirmed our expectation that healthis important, as functional capacity and nursinghome residence were significantly associated respec-tively with self-rated and interviewer-rated mentalhealth. Personality (extraversion positively, neuroticismnegatively) was an important predictor for centenariansand interviewers, but not for proxies. The finding thatMMSE as a measure of cognitive resources was a verystrong predictor for the proxy and interviewer ratingsalso provides evidence to reject our second hypothesis,and thus adds substantially to what we know aboutmental health from the perspective of informants otherthan study participants.
Discussion
For centenarians who participated in the most recentphase of the Georgia Centenarian Study we obtainedcomparisons from mental health reports about thecentenarian from proxy/caregivers, and from theinterviewer. Contrary to the conjecture of Pinquartand Sorenson (2000) that very old individuals whoremain relatively healthy are influenced by their goodfortune relative to peers who have not, we found nodifferences in the mean for ratings of mental health asassessed by the centenarians, proxies, or the inter-viewer. Substantively, this adds to the existing evidencethat centenarians as a group report mental health thatis ‘fair’, despite their advanced age and likely reducedcircumstances. Thus in the current sample centenariansdid not appear to overstate their mental health.An alternative hypothesis we cannot address is thatthe proxies’ involvement with ‘their’ centenarian andthe interviewer’s exposure to centenarians as a specialgroup has caused them to construct a perspective thatis biased upward via some sort of halo effect concern-ing the participant’s mental health. Still, with respect tothe single interviewer, systematic bias seems particu-larly unlikely as her experience interviewing all ofthe participants should have provided the basis fordistinguishing among them for the OARS mentalhealth rating task.
Our finding that there were no differences in meanratings from the alternative sources encouraged usto examine differences and similarities in potentialinfluences related to how the various raters arriveat the same overall conclusion. For that purposewe compared regressions that predicted mental healthseparately for each type of rater with commonvariables that indicated centenarians’ distal andproximal resources.
As a general hypothesis about the relative impor-tance of predictors for mental health, we expectedto find that physical health, personality, and socialsupport are critical for maintaining an overall senseof mental well-being. Although prior research withcommunity-dwelling centenarians for Phase 1 of theGeorgia Centenarian Study had also identified thosevariables as important positive influences on mentalhealth (Adkins et al., 1996; Martin, 2002), we failed toconfirm the importance of social support in the presentstudy, which includes residents of nursing homes.Additionally, Martin (2002) measured social supportby the interviewers’ rating of social resources overall,while here social support was measured using theSocial Provisions Scale (Cutrona & Russell, 1987) asreported by centenarians. Further research is recom-mended to identify what specific aspects of socialsupport are most important for centenarians’ mentalhealth.
For personality, our finding that Extraversion wasrelated to centenarians’ self-assessment ( p50.05) aswell as to the interviewer’s rating of mental healthconfirms the importance of that variable as found for
Centenarians
Proxy/caregiver
Interviewer
Neuroticism
Extraversion
Perceived economic status
Mental health (self rating)
ADL
Distal events
MMSE
Perceived economic status
Mental health (proxy rating)
Nursing home residence
MMSE
Neuroticism
Extraversion
Mental health (interviewer rating)
0.20*
−0.19*
0.18†
0.26**
0.22*
0.26***
0.29**
−0.28**
0.32**
−0.20*
0.20*
Figure 1. Estimated effects of resource domain variables onmental health.Note: *p50.05; **p50.01; ***p50.001; yp50.10.
834 M. MacDonald et al.
Dow
nloa
ded
by [
Uni
vers
ity o
f C
hica
go L
ibra
ry]
at 2
2:52
05
Oct
ober
201
4

morale by Adkins et al. (1996). Additionally, neuroti-cism had a negative effect on mental health (except forthe proxy reporter). Other aspects of personality suchas locus of control (Landau & Litwin, 2001) have alsobeen found to predict mental health among oldest oldadults. Hence, the current study once again emphasizesthat personality may be a critical factor for resiliency invery late life.
For mental health among community-dwellingcentenarians in Georgia, (Martin, 2002), it has beenestablished that perceived resource adequacy is posi-tively related to well-being. The current study hasconfirmed the positive effect of perceived economicresources on centenarians’ mental health assessmentwith the same effect for proxy reports on mentalhealth. However the centenarians’ report of resourceadequacy was not a significant predictor in our modelfor interviewer mental health ratings. Instead, nursinghome residence may have captured that effect, as it wasa significant negative influence on interviewers’ mentalhealth rating and presumably basic resource needs aremet by nursing homes. Hence, analyzing the relation-ship of services and resources to perceived economicstatus in future research could clarify the role of basicresources such as income and caregiving support asbackground factors that may also have direct effectson mental health in addition to their role as influenceson perceived economic status.
Compared to earlier studies, the theoretical frame-work we adopted recommended more attention todistal influences such as an engaged life style, orcumulative experience with important life events.Additionally, the focus on adaptation behaviorsin the developmental adaptation model (Martin &Martin, 2002) led us to include proximal events too aspotential stressors and to consider specific copingresponses via religion or seeking support as a copingmechanism. Distal events were found to be a signifi-cant and positive predictor in the sample for the proxymental health raters, and in the preliminary regressionsfor the interviewer rating. From the distal domainpreliminary analysis, we also found that engagedlifestyle (interviewer) and occupation (centenarian)had positive mental health effects. This tentativesupport for the importance of distal variables suggeststhat more careful disaggregation of event types anda focus on specific experiences could yield betterinformation about how centenarians’ individualhistories contribute to their longevity. Whetherproximal events or coping deserves further attentionseems doubtful because the only significant resultin that domain was restricted to religious coping inthe preliminary analysis for the interviewer ratings.Perhaps the role of religious and other forms of copingis more important for global measures such as overalllife-satisfaction, or constructs concerning meaningin life.
Our interpretation of the results across differentsources and for rater pair comparisons may be mis-leading to the extent that the interviewer’s reports of
centenarians’ mental health were affected by theirknowledge of the centenarians’ self-reports. Relatedto this point, the proxy would not have known aboutthe centenarians’ self-report, which would provideanother source of bias for comparing the averagereports of mental health levels across rater pairs aswell as affecting comparisons about predictors forproxies compared to centenarians and the interviewer.
Implications for future research and practice
Our most distinctive finding may be that MMSE isan important predictor of mental well-being fromthe perspective of persons other than the centenarian.Evidently our study’s proxy/caregivers and inter-viewers consider cognitive ability to be an importantand readily observable aspect of mental health.However from the Georgia centenarians’ own perspec-tive the critical health domain variable for mentalwell-being is functional capacity. An important nextstep could be to identify those centenarians for whichcognition was likely impaired.
Another strong implication of this study is thatgerontologists need to recognize that their findingsrelated to associations between mental health andother variables may be strongly influenced by whoprovided the mental health data. For example, a studyfocusing on activities of daily living and mental healthmay be more likely to find a significant associationwith self-reports than if proxies are used. That is,although we found that there is high inter-raterreliability among self, proxy, and interviewer mentalhealth reports and thus want to encourage the useof multiple informants, there is still the need to beaware that the type of report influences whether ornot we find significant associations with other keyvariables.
Taking the comparative regression results here as aguide, it may help to be explicit about when to useproxies and when not. Using proxy reports on mentalhealth may partially measure MMSE and thus notbe as effective as centenarians’ self-reports unless itis possible to identify better which centenarians arenot cognitively impaired and focus on them entirely.Conversely, if resources do not permit testing formental ability, proxy ratings of mental health mayprovide a useful measure that captures those infor-mants’ knowledge of the participants’ mental abilityand emotional health together. Caregiver/proxyreports of mental health were not related to personalitytraits reported by the centenarian in our study whereaswe did find associations between those traits andself-reported mental health so that self-reports wouldbe recommended for personality research. (Howeverwe have not analyzed how proxy reports of person-ality characteristics are related to proxy mentalhealth reports, and that strategy could be fruitful.)Centenarians’ perceived economic status was stronglyrelated to both centenarians’ own mental health and
Aging & Mental Health 835
Dow
nloa
ded
by [
Uni
vers
ity o
f C
hica
go L
ibra
ry]
at 2
2:52
05
Oct
ober
201
4

the proxy reports, indicating that studies concernedwith economic resource issues may want to concentrateon proxies as informants about resource adequacy aswell as using them to supply data about income andcaregiving services. In fact our results relied on proxiesfor income and care service reports, which may haveattuned the proxies to the resource adequacy aspectsof their centenarians’ well-being.
A recommendation for mental health professionalsand caregivers concerned with maintaining psycholog-ical well-being among the oldest-old is to be aware thatcaregivers have a strong tendency to equate cognitiveability with mental health. However self-reportedmental health ratings from centenarians in our studyare correlated instead with their functional health andeconomic resources. Fortunately, even though elderlyindividuals’ cognition tends to decline there are waysto maintain cognitive ability, overcome functionalhealth limitations, and remain vigilant about andrespond to their unmet economic needs.
Study limitations
To test the sensitivity of our results and conclusionsthat were based on the largest number of casesavailable for each mental health reporter separatelywe also obtained regressions using the same predictorsfor the smaller analysis samples for the two rater pairtypes involving centenarians. (e.g. the smallest listwisedeletion n¼ 74 for centenarians-interviewers, and 71for centenarians-proxies). Despite the reductionsin the number of cases, the substantive results fromthe smaller paired samples were very similar to theresults reported in Table 2 and summarized inFigure 1. However there was one exception. Theeffect of neuroticism for the centenarians’ self-reportin the interviewer–centenarian paired analysis samplebecame non-significant. Hence although our sensitivityanalysis generally supported our strategy of relyingon the largest analysis samples separately, the results ofthat analysis do suggest caution with respect to ourconclusion that both the interviewer and the centenar-ian mental health reports are negatively associatedwith neuroticism. Throughout our study we havealso relied primarily on the centenarians’ self-reportsfor most of the predictor variables, and thus we havenot analyzed the correspondence between regressionresults based on proxy reports for defining predictorvariables and their mental health rating to thecentenarians’ results when using centenarians reportson the predictors as well as their mental health.Such comparison could provide an additional basisfor considering correspondence among correlates ofmental health. With respect to omitted variables, ourresults may not capture systematic differences amongcentenarians on personality traits such as self-efficacyand locus of control that may moderate their senseof mental well-being. However we have establishedthat there are important commonalities amongmental health raters, which is encouraging to develop
a measurement model with our three mental healthreports as indicators of a latent mental health factor,and in that context we can contrast the predictiveability of proxy and centenarians’ reports of centenar-ians’ characteristics.
Acknowledgements
The Georgia Centenarian Study (Leonard W. Poon, PI) isfunded by 1P01-AG17553 from the National Institute onAging, a collaboration among The University of Georgia,Tulane University Health Sciences Center, BostonUniversity, University of Kentucky, Emory University,Duke University, Wayne State University, Iowa StateUniversity and University of Michigan. Authors acknowl-edge the valuable recruitment and data acquisition effortfrom M. Burgess, K. Grier, E. Jackson, E. McCarthy,K. Shaw, L. Strong and S. Reynolds, data acquisition teammanager; S. Anderson, E. Cassidy, M. Janke, and T. Savla,data management; M. Poon for project fiscal management.
References
Adkins, G., Martin, P., & Poon, L.W. (1996). Personalitytraits and states as predictors of subjective well-being in
centenarians/octogenarians and sexagenarians. Psychology
and Aging, 11, 408–416.Berg, A.I., Hassing, L.B., McClearn, G.E., & Johannson, B.
(2006). What matters for life satisfaction in the oldest-old?
Aging & Mental Health, 10, 257–264.Costa, P.T., & McCrae, R.R. (1994). Stability and
change in personality from adolescence through adulthood.In C.F. Halverson, G.A. Kohnstamm, &R.P.Martin (Eds.),
The developing structure of temperament and personality
from infancy to adulthood (pp. 139–164). Hillsdale, NJ:
Erlbaum.Cutrona, C.E., & Russell, D. (1987). The provisions of social
relationships and adaptation to stress. In W.H. Jones, &
D. Perlman (Eds.), Advances in personal relationships(Vol. 1, pp. 37–67). Greenwich, CT: JAI Press.
Dello Buono, M., Urciuoli, O., & de Leo, D. (1998). Qualityof life and longevity. A study of centenarians. Age and
Ageing, 27, 207–216.Fillenbaum, G.G. (1988). Multidimensional functional assess-
ment of older adults: The Duke Older Americans Resources
and Services Procedures. Hillsdale: Lawrence Erlbaum
Associates.Folstein, M.F., Folstein, S.E., & McHugh, P.R. (1975).
Mini-mental state: A practical method for grading thecognitive state of patients for the clinician. Journal of
Psychiatric Research, 12, 189–198.Hilleras, P.K., Jorm, A.F., Herlitz, A., & Winblad, B. (1999).
Activity patterns in very old people a survey of cognitively
intact subjects aged 90 years or older. Age and Ageing, 28,
147–152.Holtsberg, P.A., Poon, L.W., Noble, C.A., & Martin, P.
(1995). Mini-mental state exam status of communitydwelling, cognitively intact centenarians. International
Psychogeriatrics, 7, 417–427.
Hultsch, D., Hertzog, C., Small, B., & Dixon, R. (1999). Useit or lose it: Engaged lifestyle as a buffer of cognitive
decline in aging? Psychology and Aging, 14, 245–263.Kane, R.L., Kane, R.A., Bershadsky, B., Degenholtz, H.,
Kling, K., Totten, A., et al. (2005). Proxy sources of
836 M. MacDonald et al.
Dow
nloa
ded
by [
Uni
vers
ity o
f C
hica
go L
ibra
ry]
at 2
2:52
05
Oct
ober
201
4

information on nursing home residents’ quality of life.Journal of Gerontology: Social Sciences, 60B, S318–S325.
Kolanowski, A., Hoffman, L., & Hofer, S.M. (2007).Concordance of self-report and informant assessment ofemotional well-being in nursing home residents withdementia. Journal of Gerontology: Psychological Sciences,
62B, P20–P27.Landau, R., & Litwin, H. (2001). Subjective well-beingamong the old-old: The role of health, personality, and
social support. International Journal of Aging and HumanDevelopment, 54, 265–280.
Lum, T.Y., Lin, W.C., & Kane, R.L. (2005). Use of proxy
respondents and accuracy of minimum data set assess-ments of activities of daily living. Journal of Gerontology:Medical Sciences, 60A, 654–659.
MacDonald, M. (2007). Social support for centenarians’
health, psychological well-being and longevity.In L.W. Poon, & T.T. Perls (Eds.), Annual review ofgerontology and geriatrics: Vol. 27. Biopsychosocial
approaches to longevity (pp. 107–127). New York: Springer.Martin, P. (2002). Individual and social resources predictingwell-being and functioning in later years: Conceptual
models, research, and practice. Ageing International,27(2), 3–29.
Martin, P. (2007). Personality and coping among centenar-
ians. In L.W. Poon, & T.T. Perls (Eds.), Annual review ofgerontology and geriatrics, Vol. 27: Biopsychosocialapproaches to longevity (pp. 89–106). New York: Springer.
Martin, P., & Martin, M. (2002). Proximal and distal
influences on development: The model of developmentaladaptation. Developmental Review, 22, 78–96.
Moos, R.H., Cronkite, R.C., Billings, A.G., & Finney, J.W.
(1985). Health and daily living form manual. Stanford:Stanford University Medical Center.
Ozaki, A., Uchiyama, M., Tagaya, H., Oshida, T., &
Ogihara, R. (2007). The Japanese centenarian study.Journal of the American Geriatrics Society, 55, 95–191.
Pinquart, M., & Sorenson, S. (2000). Influences of socio-
economic status, social network, and competence onsubjective well-being in later life: A meta-analysis.Psychology and Aging, 15, 187–207.
Poon, L.W., Johnson, M.A., Davey, A., Dawson, D.V.,Siegler, I.C., & Martin, P. (2000). Psycho-social predictors
of survival among centenarians. In P. Martin, C. Rott,B. Hagberg, & K. Morgan (Eds.), Centenarian: Autonomyversus dependence in the oldest-old (pp. 77–90). New York:Springer Publishing.
Poon, L.W., & Perls, Thomas T. (2007). Annual review ofgerontology and geriatrics: Vol. 27. Biopsychosocialapproaches to longevity. New York: Springer.
Schatzberg, K.L., Sudha, S., & Mutran, E.J. (1998).Elder-proxy agreement concerning the functional sta-tus and medical history of the older person: The
impact of caregiver burden and depressive symptomatol-ogy. Journal of the American Geriatrics Society, 46,1103–1111.
Selim, A.J., Fincke, G., Berlowitz, D.R., Miller, D.R.,
Qian, S.X., Lee, A., et al. (2005). Comprehensive healthstatus assessment of centenarians: Results from the 1999large Health Survey of Veteran Enrollees. Journal of
Gerontology, 60A, 515–519.Smith, J., Fleeson, W., Geiselmann, B., Settersten Jr, R., &Kunzmann, U. (1999). Sources of well-being in very old
age. In P.B. Baltes, & K.U. Mayer (Eds.), The Berlin agingstudy: Aging from 70 to 100 (pp. 450–471). New York:Cambridge University Press.
Soldo, B.J, Hurd, M.D., & Rodgers, W.L (1997). Asset andhealth dynamics among the oldest old: An overview of theAHEAD study. Journal of Gerontology: PsychologicalSciences, 52, 1–20.
Tombaugh, T.N., & McIntyre, N.J. (1992). The Mini-mentalstatus examination: A comprehensive review. Journal ofthe American Geriatrics Society, 40, 922–935.
Walsh, E.G., Wu, B., Mitchell, J.B., & Berkmann, L.F.(2003). Cognitive function and acute care utilization.Journal of Gerontology: Social Sciences, 58B, S38–S49.
Yi, Z., & Vaupel, J.W. (2002). Functional capacity andself-evaluation of health and life of oldest old in China.Journal of Social Issues, 58, 733–748.
Zung, W.K., & Zung, E.M. (1986). Use of the Zungself-rating depression scale in the elderly. ClinicalGerontologist, 5(1–2), 137–147.
Aging & Mental Health 837
Dow
nloa
ded
by [
Uni
vers
ity o
f C
hica
go L
ibra
ry]
at 2
2:52
05
Oct
ober
201
4





















![[Global HR Forum 2011] An Age of Centenarians? Lifelong Learning Policies and Ageing](https://img.pdfslide.net/doc/110x75/5590df251a28ab32578b470d/global-hr-forum-2011-an-age-of-centenarians-lifelong-learning-policies-and-ageing.jpg)