Embed Size (px)
Citation preview
Cost barriers reduce confidence in receiving medical carewhen seriously ill
Trust, which according to Mechanic, is ‘the expecta-
tion that individuals and institutions will meet their
responsibilities to us’ (1), has been analysed from
different perspectives. Authors have, for instance,
studied trust in one’s own medical doctor (2),
patient preferences (3) and satisfaction with the
healthcare system (4,5). The question of confidence
in receiving safe and quality medical care when fall-
ing seriously ill, in contrast, has been neglected in
previous comparative research (6). We expect that
this ‘feeling of security’ is influenced by past experi-
ences with the healthcare system, and we therefore
ask in what respect negative experiences influence
confidence in the healthcare system.
The analysis is based on data from the Common-
wealth Fund International Health Policy Survey 2007
(6). Negative experiences are captured by the ques-
tion: ‘During the past 12 months, was there a time
when you had a medical problem but did not visit a
doctor because of cost?’ The lack of confidence in
receiving good medical care in the
future is measured by the question:
‘How confident are you that if you
become seriously ill, you will get
quality and safe medical care?’ In
our analysis, we focused on those
respondents who reported to be ‘not
very’ or ‘not at all confident’. We
conducted pairwise comparisons of
group percentages using the Scheffe
method (7) for the dependent vari-
able (confidence).
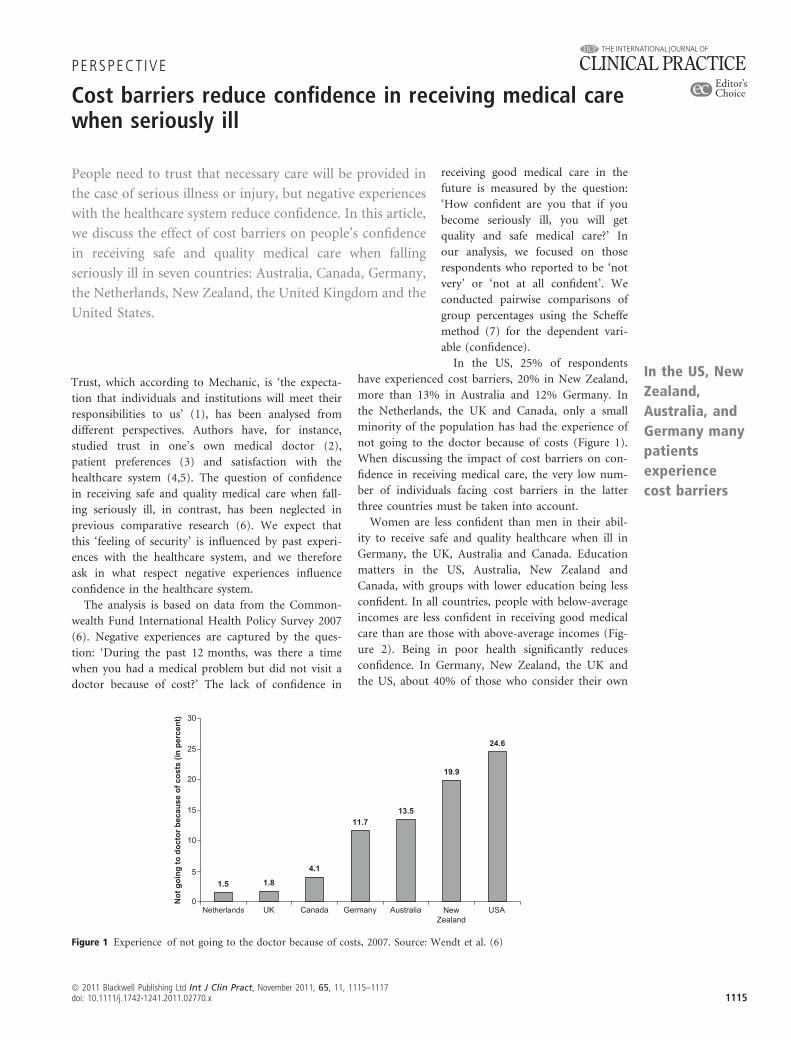
In the US, 25% of respondents
have experienced cost barriers, 20% in New Zealand,
more than 13% in Australia and 12% Germany. In
the Netherlands, the UK and Canada, only a small
minority of the population has had the experience of
not going to the doctor because of costs (Figure 1).
When discussing the impact of cost barriers on con-
fidence in receiving medical care, the very low num-
ber of individuals facing cost barriers in the latter
three countries must be taken into account.
Women are less confident than men in their abil-
ity to receive safe and quality healthcare when ill in
Germany, the UK, Australia and Canada. Education
matters in the US, Australia, New Zealand and
Canada, with groups with lower education being less
confident. In all countries, people with below-average
incomes are less confident in receiving good medical
care than are those with above-average incomes (Fig-
ure 2). Being in poor health significantly reduces
confidence. In Germany, New Zealand, the UK and
the US, about 40% of those who consider their own
People need to trust that necessary care will be provided in
the case of serious illness or injury, but negative experiences
with the healthcare system reduce confidence. In this article,
we discuss the effect of cost barriers on people’s confidence
in receiving safe and quality medical care when falling
seriously ill in seven countries: Australia, Canada, Germany,
the Netherlands, New Zealand, the United Kingdom and the
United States.
1.5 1.8
4.1
11.713.5
19.9
24.6
0
5
10
15
20
25
30
Netherlands UK Canada Germany Australia NewZealand
USA
Not
goi
ng to
doc
tor b
ecau
se o
f cos
ts (i
n pe
rcen
t)
Figure 1 Experience of not going to the doctor because of costs, 2007. Source: Wendt et al. (6)
PERSPECT IVE
ª 2011 Blackwell Publishing Ltd Int J Clin Pract, November 2011, 65, 11, 1115–1117doi: 10.1111/j.1742-1241.2011.02770.x 1115
In the US, New
Zealand,
Australia, and
Germany many
patients
experience
cost barriers
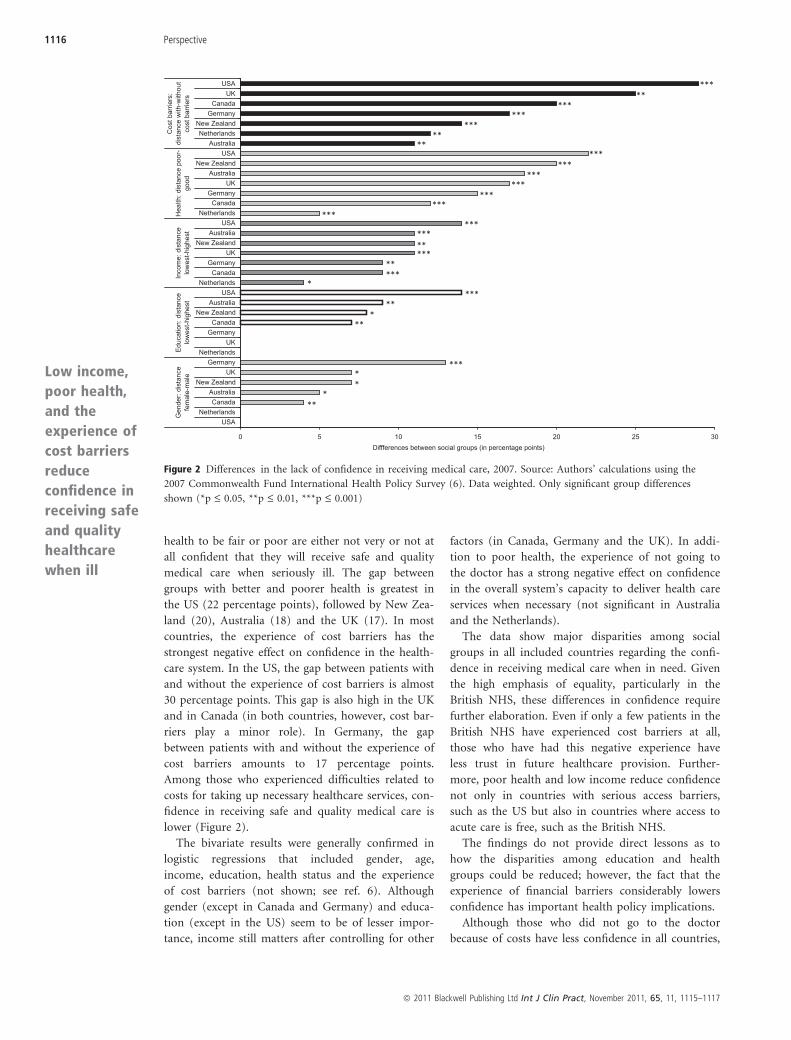
health to be fair or poor are either not very or not at
all confident that they will receive safe and quality
medical care when seriously ill. The gap between
groups with better and poorer health is greatest in
the US (22 percentage points), followed by New Zea-
land (20), Australia (18) and the UK (17). In most
countries, the experience of cost barriers has the
strongest negative effect on confidence in the health-
care system. In the US, the gap between patients with
and without the experience of cost barriers is almost
30 percentage points. This gap is also high in the UK
and in Canada (in both countries, however, cost bar-
riers play a minor role). In Germany, the gap
between patients with and without the experience of
cost barriers amounts to 17 percentage points.
Among those who experienced difficulties related to
costs for taking up necessary healthcare services, con-
fidence in receiving safe and quality medical care is
lower (Figure 2).
The bivariate results were generally confirmed in
logistic regressions that included gender, age,
income, education, health status and the experience
of cost barriers (not shown; see ref. 6). Although
gender (except in Canada and Germany) and educa-
tion (except in the US) seem to be of lesser impor-
tance, income still matters after controlling for other
factors (in Canada, Germany and the UK). In addi-
tion to poor health, the experience of not going to
the doctor has a strong negative effect on confidence
in the overall system’s capacity to deliver health care
services when necessary (not significant in Australia
and the Netherlands).
The data show major disparities among social
groups in all included countries regarding the confi-
dence in receiving medical care when in need. Given
the high emphasis of equality, particularly in the
British NHS, these differences in confidence require
further elaboration. Even if only a few patients in the
British NHS have experienced cost barriers at all,
those who have had this negative experience have
less trust in future healthcare provision. Further-
more, poor health and low income reduce confidence
not only in countries with serious access barriers,
such as the US but also in countries where access to
acute care is free, such as the British NHS.
The findings do not provide direct lessons as to
how the disparities among education and health
groups could be reduced; however, the fact that the
experience of financial barriers considerably lowers
confidence has important health policy implications.
Although those who did not go to the doctor
because of costs have less confidence in all countries,
035202510150
USANetherlands
CanadaAustralia
New ZealandUK
GermanyNetherlands
UKGermany
CanadaNew Zealand
AustraliaUSA
NetherlandsCanada
GermanyUK
New ZealandAustralia
USANetherlands
CanadaGermany
UKAustralia
New ZealandUSA
AustraliaNetherlands
New ZealandGermany
CanadaUK
USA
Gen
der:
dist
ance
fem
ale-
mal
eE
duca
tion:
dis
tanc
elo
wes
t-hig
hest
Inco
me:
dis
tanc
elo
wes
t-hig
hest
Hea
lth: d
ista
nce
poor
-go
od
Cos
t bar
riers
:di
stan
ce w
ith-w
ithou
tco
st b
arrie
rs
Diffferences between social groups (in percentage points)
*****
******
*****
*****
***
******
**********
******
******
***
***
***
*****
****
**
Figure 2 Differences in the lack of confidence in receiving medical care, 2007. Source: Authors’ calculations using the
2007 Commonwealth Fund International Health Policy Survey (6). Data weighted. Only significant group differences
shown (*p £ 0.05, **p £ 0.01, ***p £ 0.001)
Low income,
poor health,
and the
experience of
cost barriers
reduce
confidence in
receiving safe
and quality
healthcare
when ill
1116 Perspective
ª 2011 Blackwell Publishing Ltd Int J Clin Pract, November 2011, 65, 11, 1115–1117

we could show that not only in the UK but also in
the Netherlands only a few people have experienced
cost barriers. This phenomenon could be partly
related to the fact that visits to a doctor are free and
that other private out-of-pocket payments have also
been particularly low for many years in both coun-
tries while remaining at a high level in the US, Aus-
tralia and New Zealand. The type of co-payment, as
well as the time of the introduction of co-payments,
also plays a role in establishing cost barriers. In Ger-
many, for instance, a payment of ten Euros per quar-
ter for a doctor’s visit was introduced in 2004. This
fee seems to have a stronger impact on patients’
decision to not see a doctor, as patients can be sure
that these costs will apply as soon as they visit a doc-
tor (in contrast, for instance, to co-payments for
pharmaceuticals).
The trend towards increased cost-sharing for
patients in healthcare systems therefore has more
unintended consequences than previously realised.
Beside the risk of an increased burden on low-
income groups and those with a lower health status,
experienced cost barriers also affect trust in the
healthcare system. As trust is not only important for
the legitimacy of the healthcare system but also for
treatment outcomes, we suggest that policy makers
consider the negative impact on trust when dealing
with cost-sharing instruments. Guaranteeing access
to necessary healthcare services for those who fall
seriously ill can be considered the single most impor-
tant task of healthcare systems in modern societies,
and patients therefore need ‘markers of certainty’
(8), which indicate that this promise will be fulfilled.
Being able to go to a doctor with a minor symptom
seems to represent such a ‘marker of certainty’, indi-
cating that quality healthcare will be provided when
facing a serious disease.
Disclosures
None.
Acknowledgements
The research reported here has received financial
support from the Harkness Program of Health Policy
& Practice of the Commonwealth Fund and the
Bosch Foundation.
C. Wendt,1 M. Mischke,1 M. Pfeifer,1 N. Reibling2
1Department of Sociology, University of Siegen,Siegen, Germany
2MZES, University of Mannheim, Mannheim, GermanyEmail: [email protected]
References1 Mechanic D. The functions and limitations of trust
in the provision of medical care. JHPPL 1998; 23:
661–86.
2 Calnan MW, Sanford E. Public trust in health care:
the System or the Doctor? Qual Saf Health Care
2004; 13: 92–7.
3 Cheraghi-Sohi S, Bower P, Mead N, McDonald R,
Whalley D, Roland M. What are the key attributes of
primary care for patients? Building a conceptual ‘map’
of patient preferences. Health Expect 2006; 9: 275–84.
4 Wendt C, Kohl J, Mischke M, Pfeifer M. How do
Europeans perceive their healthcare system? Euro Soc
Rev 2010; 26: 177–92.
5 Blendon RJ, Hunt K, Benson JM, Fleischfresser C,
Buhr T. Understanding the American Public’s Health
Priorities: a 2006 perspective. Health Aff 2006; 25:
w508–15.
6 Wendt C, Mischke M, Pfeifer M, Reibling N. Confi-
dence in receiving medical care when seriously Ill: a
seven-country comparison of the impact of cost bar-
riers. Health Expect 2011. doi: 10.1111/j.1369-7625.
2011.00677.x. http://onlinelibrary.wiley.com/doi/10.1111/
j.1369-7625.2011.00677.x/abstract (accessed 24 August
2011).
7 UCLA Academic Technology Services. https://www.
ats.ucla.edu/stat/Stata/faq/pairwise.htm (accessed 10
October 2009).
8 Eisenstadt SN. Multiple Modernities. New Brunswick
and London: Transaction Publishers, 2002.
Perspective 1117
ª 2011 Blackwell Publishing Ltd Int J Clin Pract, November 2011, 65, 11, 1115–1117