Embed Size (px)
DESCRIPTION
cpr
Citation preview

1.0 BACKGROUND
ACTIGRAPHY HAS BEEN USED TO STUDY SLEEP/WAKE PAT-TERNS FOR OVER 20 YEARS. The advantage of actigraphy over tra-ditional polysomnography (PSG) is that actigraphy can convenientlyrecord continuously for 24-hours a day for days, weeks or even longer.In 1995, Sadeh et al.,1 under the auspices of the American Sleep Disor-ders Association (now called the American Academy of Sleep Medicine,AASM), reviewed the current knowledge about the role of actigraphy inthe evaluation of sleep disorders. They concluded that actigraphy doesprovide useful information and that it may be a “cost-effective methodfor assessing specific sleep disorders...[but that] methodological issueshave not been systematically addressed in clinical research and prac-tice.” Based on that task force’s report, the AASM Standards of PracticeCommittee concluded that actigraphy was not indicated for routine diag-nosis or for assessment of severity or management of sleep disorders,but might be a useful adjunct for diagnosing insomnia, circadian rhythmdisorders or excessive sleepiness.2 Since that time, actigraph technologyhas improved, and many more studies have been conducted. Severalreview papers have concluded that wrist actigraphy can usefully approx-imate sleep versus wake state during 24 hours and have noted that actig-raphy has been used for monitoring insomnia, circadian sleep/wake dis-turbances, and periodic limb movement disorder.3,4 This paper beginswhere the 1995 paper left off. Under the auspices of the AASM, a newtask force was established to review the current state of the art of thistechnology.
Actigraphs are devices generally placed on the wrist (although theycan also be placed on the ankle or trunk) to record movement. Collecteddata are downloaded to a computer for display and analysis of activi-ty/inactivity that in turn can be further analyzed to estimate wake/sleep.The latter technology is based on the observation that there is less move-ment during sleep and more movement during wake. As described inAncoli-Israel,5 the first actigraphs were developed in the early 1970’s.6-8
Kripke and colleagues were some of the first investigators to publishreliability data on the use of wrist actigraphy for the assessment ofsleep.9-11 Over the years, additional types of actigraphs were developedleading to the digital types used today.
Actigraphs today have movement detectors (e.g., accelerometers) andsufficient memory to record for up to several weeks. Movement is sam-pled several times per second and stored for later analysis. Computerprograms are used to derive levels of activity/inactivity, rhythm param-eters (such as amplitude or acrophase) and sleep/wake parameters (suchas total sleep time, percent of time spent asleep, total wake time, percentof time spent awake and number of awakenings).
2.0 OBJECTIVES
This paper reviews four major areas in which actigraphy is used forthe measurement of sleep or rhythms. The first area of review covers themore recent papers on the technology and validity of actigraphy. Sadehet al. concluded that the validation studies for normal subjects showedgreater than 90% agreement and were very promising.1 Actigraphs andcomputer programs using different algorithms to process the data havebeen commercially available for quite some time. Actigraphs differ inhow they detect and record movements and they use different method-ologies for computing activity levels. The output of the analysis pro-grams has been compared to the results of PSG and sleep diaries. Thissection reviews the results and evaluates the conclusions of these typesof studies.
The second area of review is of those studies examining actigraphy inpopulations with sleep disorders. Actigraphy is being used more often instudies of sleep disorders, either as an alternative to PSG, as an additionto partial unattended monitoring devices or for follow-up. This is espe-cially common in patients with complaints of insomnia.
In addition to gaining information about sleep, data collected overlong periods can be used to determine activity circadian rhythm cycles.Actigraphy is particularly useful for recording rhythms, as it is very dif-ficult to record PSG for 24-hours and almost impossible to record formore than 24-hours. The use of actigraphy in studies of circadianrhythms comprises the third area of review.
The fourth area of review is those studies in which actigraphy wasused as a treatment outcome measure or to examine the relationshipbetween sleep/activity patterns and demographic or clinical variables.Since actigraphy is easier to use, less invasive and substantially lessexpensive than PSG, actigraphy is often used in lieu of PSG in both clin-ical trials where it is necessary to determine the effect of a treatment onsleep and in studies requiring multiple measurements.
3.0 METHODS
As with the first review in 1995, the Standards of Practice Committeeof the American Academy of Sleep Medicine commissioned this updat-ed review. A Medline literature search was conducted from the year 1995to April 2002. Key words for the Medline search included actigraphy,actigraph, actigraphic recording, actimeter, actometer, wrist actigraph,actigraph recording, wrist activity, rest activity, activity, and sleep-wakeactivity, each paired with sleep, sleep disorders and sleep disorders-cir-cadian. Articles published prior to the original American Academy of
Actigraphy Review Paper—Ancoli-Israel et alSLEEP, Vol. 26, No. 3, 2003 342
The Role of Actigraphy in the Study of Sleep and Circadian Rhythms
AMERICAN ACADEMY OF SLEEP MEDICINE REVIEW PAPER
Sonia Ancoli-Israel PhD,1 Roger Cole PhD,2 Cathy Alessi MD,3 Mark Chambers PhD,4 William Moorcroft PhD,5 Charles P. Pollak MD6
1Department of Psychiatry, University of California, San Diego and Veterans Affairs San Diego Healthcare System, 2Synchrony Applied Health Sci-ences, Del Mar, CA, 92014, 3Geriatric Research, Education and Clinical Center; VA Greater Los Angeles Healthcare System and UCLA School ofMedicine, Multicampus Program in Geriatric Medicine and Gerontology, 4Private Practice, Las Vegas, Nevada, 5Colorado State University andNorthern Colorado Sleep Consultants, LLC, 6Department of Neurology, The Ohio State University
Citation: Ancoli-Israel S, Cole R, Alessi C et al. The role of actigraphy in the study of sleep and circadian rhythms. American Academy of Sleep MedicineReview Paper. SLEEP 2003;26(3):342-92.
Disclosure StatementSupported by: NIA AG08415, NCI CA85264, the Department of Veterans AffairsVISN-22 Mental Illness Research, Education and Clinical Center (MIRECC),the Research Service of the Veterans Affairs San Diego Healthcare System [toSAI]; NIA AG13885, VA HSRD IIR 01-053-1, the Department of Veterans AffairsGeriatric Research, Education and Clinical Center (GRECC) at the VA GreaterLos Angeles Healthcare System [to CA].
Address correspondence to: Sonia Ancoli-Israel, Ph.D., Department of Psychia-try, VASDHS, 3350 La Jolla Village Drive, San Diego, Ca 92161,USA. Tele-phone: 858 642-3828; Fax: 858 552-7536; email: [email protected]
Sleep Medicine’s (AASM) Practice Parameters for the Use of Actigra-phy in the Clinical Assessment of Sleep Disorders1 in 1995 were notincluded in the current update, and only articles written in English wereincluded.
A total of 171 articles were identified as potentially relevant based onthese Medline searches. All of these were obtained in full length andexamined. Upon review of these articles, approximately 30 additionalreferences were discovered by perling (i.e., checking the reference sec-tions for articles otherwise missed). These were references located in
publications not typically found through Medline. In an attempt toinclude all articles matching the stated criteria, task force members alsoadded any articles they discovered through their personal review of theliterature. All new articles published up to the point of the final draft ofthis manuscript (July 2002) were reviewed.
Only papers where actigraphs were used to measure some aspect ofsleep/wake activity or circadian rhythms were included. Papers that onlymeasured activity (without any reference to sleep) or that made mea-surements only in the daytime were excluded. Only papers published inEnglish, in peer-reviewed journals, were included. Case studies andreview articles were included in the narrative, but not in the evidencetables. No conference abstracts, even if published, were included. Paperswere categorized into four sections: Technology, Sleep Disorders, Circa-dian Rhythms, and Other Clinical Research.
Within each category, task force members were assigned to read eachpaper, summarize the relevant points for the evidence tables and rate thestudy according to the evidence levels shown in Table 1. Abbreviationsused in the evidence tables are described in Appendix A.
4.0 TECHNOLOGY
The technology section (see Table 2) includes studies that comparedfunctional differences between actigraphic devices, data acquisitionstrategies, and software programs. The question asked was, “How welldid the devices and the computer programs that process data, assessstates of sleep/wake and related phenomena?”
4.1 Data Acquisition
Mechanically, the first generation actigraphs were threshold-motiondetectors, which were nonlinear and failed to be sensitive enough todetect small movements.12 They also tended to saturate with modest lev-els of movement. Some of the newer actigraphs detect motion with lin-ear accelerometers in a single axis or multiple axes.12 Most single axisacceleration devices in use today use .25 to 2-3Hz bandpass filteringbefore data are stored, essentially eliminating very slow movements ofless than .25 Hz and movements faster than 2-3 Hz. This is consistentwith the early recommendations of Redmond and Hegge who noted thatvoluntary human movement rarely exceeds 3-4 Hz, and that involuntarymovements such as tremor and shivering exceed 5Hz.13 However, vanSomeren et al. suggested using 0.5-11Hz bandpass filters that wouldreduce gravitational artifacts while picking up some of the faster move-ments that occur in younger subjects.14
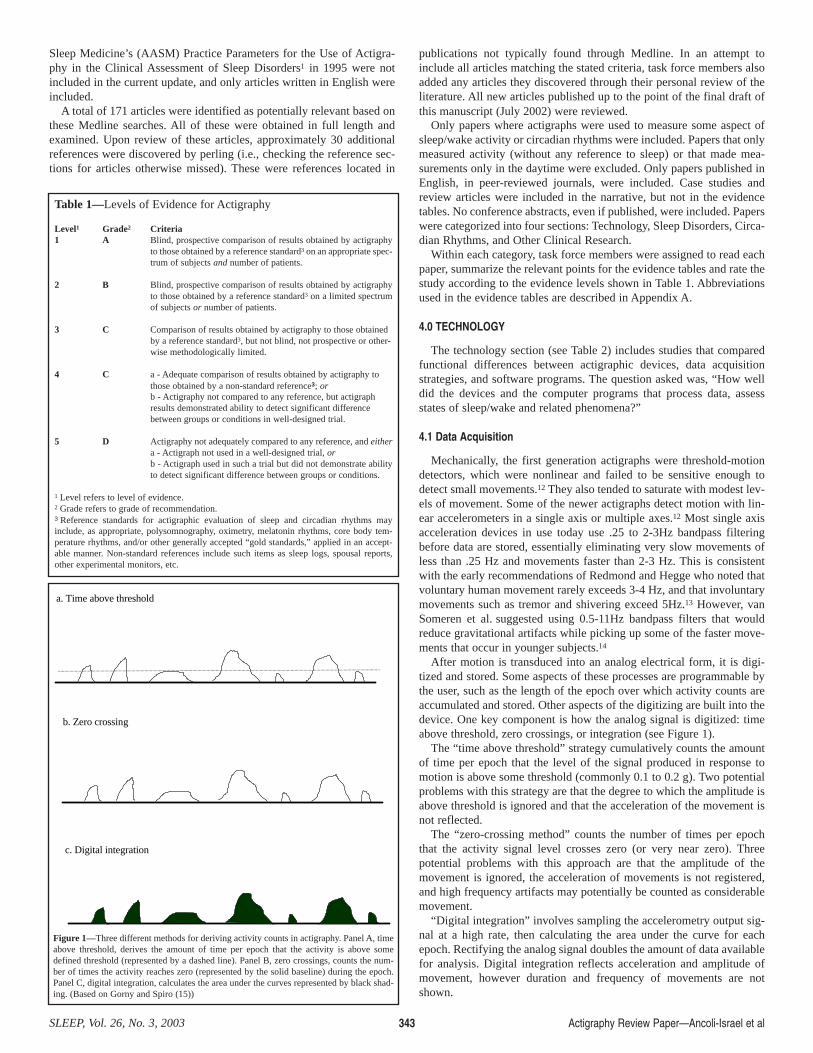
After motion is transduced into an analog electrical form, it is digi-tized and stored. Some aspects of these processes are programmable bythe user, such as the length of the epoch over which activity counts areaccumulated and stored. Other aspects of the digitizing are built into thedevice. One key component is how the analog signal is digitized: timeabove threshold, zero crossings, or integration (see Figure 1).
The “time above threshold” strategy cumulatively counts the amountof time per epoch that the level of the signal produced in response tomotion is above some threshold (commonly 0.1 to 0.2 g). Two potentialproblems with this strategy are that the degree to which the amplitude isabove threshold is ignored and that the acceleration of the movement isnot reflected.
The “zero-crossing method” counts the number of times per epochthat the activity signal level crosses zero (or very near zero). Threepotential problems with this approach are that the amplitude of themovement is ignored, the acceleration of movements is not registered,and high frequency artifacts may potentially be counted as considerablemovement.
“Digital integration” involves sampling the accelerometry output sig-nal at a high rate, then calculating the area under the curve for eachepoch. Rectifying the analog signal doubles the amount of data availablefor analysis. Digital integration reflects acceleration and amplitude ofmovement, however duration and frequency of movements are notshown.
Actigraphy Review Paper—Ancoli-Israel et alSLEEP, Vol. 26, No. 3, 2003 343
Table 1—Levels of Evidence for Actigraphy
Level1 Grade2 Criteria 1 A Blind, prospective comparison of results obtained by actigraphy
to those obtained by a reference standard3 on an appropriate spec-trum of subjects and number of patients.
2 B Blind, prospective comparison of results obtained by actigraphyto those obtained by a reference standard3 on a limited spectrumof subjects or number of patients.
3 C Comparison of results obtained by actigraphy to those obtained by a reference standard3, but not blind, not prospective or other-wise methodologically limited.
4 C a - Adequate comparison of results obtained by actigraphy to those obtained by a non-standard reference3; orb - Actigraphy not compared to any reference, but actigraph results demonstrated ability to detect significant difference between groups or conditions in well-designed trial.
5 D Actigraphy not adequately compared to any reference, and eithera - Actigraph not used in a well-designed trial, orb - Actigraph used in such a trial but did not demonstrate abilityto detect significant difference between groups or conditions.
1 Level refers to level of evidence. 2 Grade refers to grade of recommendation.3 Reference standards for actigraphic evaluation of sleep and circadian rhythms mayinclude, as appropriate, polysomnography, oximetry, melatonin rhythms, core body tem-perature rhythms, and/or other generally accepted “gold standards,” applied in an accept-able manner. Non-standard references include such items as sleep logs, spousal reports,other experimental monitors, etc.
a. Time above threshold
b. Zero crossing
c. Digital integration
Figure 1—Three different methods for deriving activity counts in actigraphy. Panel A, timeabove threshold, derives the amount of time per epoch that the activity is above somedefined threshold (represented by a dashed line). Panel B, zero crossings, counts the num-ber of times the activity reaches zero (represented by the solid baseline) during the epoch.Panel C, digital integration, calculates the area under the curves represented by black shad-ing. (Based on Gorny and Spiro (15))

In direct comparisons of these three methods of deriving activitycounts, using the same movement input, digital integration was found tobe better for identifying movement amplitude than time above thresholdand both digital integration and time above threshold were better thanzero crossing.15 Some devices simultaneously utilize more than onemethod of acquiring data thus increasing the benefits and reducing thedeficits of utilizing only one method.
Many investigators have begun to report actigraphy data simply asactivity counts. However, different devices, different data collectionstrategies,12 and different scoring algorithms produce very differentcounts for the same activity.15 These differences have made direct com-parisons between laboratories and clinics difficult and contentious.Although relative changes in activity can be meaningful, more directcomparisons following computer processing of the data (such assleep/wake scoring) are more meaningful.
4.2 Data Processing
Actigraphy data today are generally processed by computers, after thedata are downloaded from the actigraphs, rather than by hand or eye.While most programs are designed to work with a specific device, someare intended to work with data produced by several, if not all, devices.Different programs often use different algorithms. However, there are nopublished articles comparing the different algorithms. Rather, publishedarticles present information about the accuracy and/or usefulness of theoutputs of specific computer programs. Before choosing an actigraph touse, two questions need to be asked and answered satisfactorily aboutsuch programs and the device(s) they work with:1. Is the output reliable, that is, how well does the same input result in
the same output?2. Is the output valid, that is, how well does the output actually measure
what it is purported to measure?There are only a few published reports of direct studies of reliability
between actigraphs and PSG. In general, when tested, actigraphy deviceshave been found to be reliable. Jean-Louis et al. compared new and oldinstruments of the same make and model in healthy adults and found nodifferences when the devices were worn on the same wrist (evidencelevel 3C).16 In a second study when healthy adults wore two actigraphs,one on each wrist or two on the same wrist, correlations of activitycounts were 0.80 to 0.96; when these data were converted to sleep/wakescores the agreement rates between pairs of devices ranged from 93% to99% (evidence level 1A).17 The correlations between devices for datacollected just at night were between 0.60 and 0.96 and the sleep/wakescoring agreements again were between 93% and 99%.17 Pollak and col-leagues had their subjects wear actigraphs from two different manufac-turers and found that there were differences between them (evidencelevel 3C).18
There are many published reports on the validity of actigraphs formeasuring sleep/wake. Many of these are reviewed in other sections ofthis report. When comparing actigraphic to other biological variables,their similarity needs to be taken into account. If the actigraphic andother variables are judged to have equal standing, a measure of correla-tion is appropriate, but if one of the variables is invested with definitiveimportance (“gold standard”), different measures are needed to quantifyhow close actigraphy approaches the gold standard. For studies of sleep,PSG is considered definitive. Most tests of actigraph validity, therefore,involve comparing actigraphy with PSG. Comparison by correlation pro-vides information about the relative, but not the absolute performance ofactigraphy. For example, a high correlation on total sleep time wouldmean that individuals who sleep longer by PSG criteria also sleep longerby actigraph criteria, and vice versa, but this could be true even if actig-raphy systematically over-estimated total sleep time. Therefore, it is pos-sible for the correlation between actigraph and PSG sleep results to behigh, even when the epoch-by-epoch agreement is relatively low. Corre-lations provide an incomplete picture, especially if most of the datacome from the sleep period.19
An alternate approach is Tryon’s method of calculating and reporting
sensitivity, specificity, and overall accuracy or agreement (true sleepepochs + true wake epochs/all epochs) separately.20 Sensitivity for sleepis the proportion of PSG sleep epochs also identified as sleep by actig-raphy. Specificity for sleep is the proportion of non-sleep (wake) epochscorrectly identified by actigraphy. Sensitivity and specificity for wake-fulness are similarly defined. Agreement is the proportion of PSGepochs correctly identified by actigraphy. Sensitivity, specificity andagreement therefore assess actigraphic recorders using an establishedstandard. Data collected using this scheme have shown that actigraphy ismore likely to detect sleep (sensitivity) but less reliable at detectingwake (specificity) (evidence level 1A and 3C).19,21
More recently, Pollak and colleagues have suggested different ways tocompute the performance of an actigraph’s ability to detect sleep andwake.21 They use “predicted value for sleep” (PVS) which is the pro-portion of actigraphic sleep epochs that are also classified as sleep byPSG, and use “predicted value for wakefulness” (PVW) which is the pro-portion of actigraphic wake epochs that are also classified as wakeful-ness by PSG. PVS answers the question, “What percentage of the epochsthat the actigraph scores as sleep are true (PSG) sleep?” This is not thesame as sensitivity for sleep, which answers the question, “What per-centage of true (PSG) sleep epochs are detected by the actigraph?” Pol-lak and colleagues also report agreement rates but correctly point outthat this measure is actually not very useful because it confounds PVSwith PVW. For example, a high PVS but a poor PVW during the sleepperiod would yield a high agreement rate since most of the epochs wouldbe sleep. This high agreement rate gives a false sense of validity sincemuch of wake after sleep onset (WASO) could be mis-scored by actig-raphy because of the low PVW. In fact, it has generally been shown thatactigraphy is better at detecting sleep (high PVS) than at detecting wake(PVW) during the sleep period (evidence level 1A and 3C).19,21 Resultsof future studies are likely to result in more useful measures if predictivevalues are reported in addition to sensitivity, specificity and agreement.It is worth noting that all of these measures vary with the proportion ofrecorded PSG epochs that represent sleep (base rate of sleep). During thesleep period, even malfunctioning recorders that are not being worn orare insensitive to movement will appear to accurately identify sleep ifthe low activity counts recorded by them are interpreted by scoring algo-rithms as “sleep”.
4.3 Comparisons to PSG
As PSGs are still considered the gold standard, most studies havecompared actigraphy to PSG. A technical difficulty in doing these com-parisons is accurately time-locking the epochs of the actigraph withthose of the PSG.21 If they gradually drift apart, over time different seg-ments of sleep or wake may be compared with each other, rendering theresults meaningless. A related problem is how to compare the often-used1-minute epoch of actigraphy with the standard 30-second epoch of PSG.
In these comparisons, low threshold actigraph algorithms (e.g., defin-ing wake as occurring even when a small number of activity countsaccumulated during the epoch) yielded the best accuracy rate and PVS,however, as sleep efficiency diminished, accuracy rate diminished (evi-dence level 1A).19 Actigraph PVW was best with high threshold algo-rithms (e.g., defining wake as occurring when a large number of activi-ty counts, such as 100, accumulated during the epoch) compared to lowthreshold algorithms but at a cost of lower accuracy and PVS.19 Onecomputer program, Actigraph Data Analysis Software (ADAS), whichconverts raw actigraph data into information about sleep/wake, has beenshown to be valid when compared to PSG (evidence level 2B),22 evenwhen raw data were derived from different devices and in patients withinsomnia (evidence level 3C).16
Other studies have also shown that actigraphy was highly correlatedwith PSG for differentiating sleep from wake (evidence level 2B and 3Crespectively),22,23 with reported correlations for total sleep time (TST)being 0.97.22 Comparisons showed 91%-93% overall agreement inadults (age 20-30 years) (evidence level 2B),24 and 91.4%-96.5%
Actigraphy Review Paper—Ancoli-Israel et alSLEEP, Vol. 26, No. 3, 2003 344

minute-by-minute agreement rates in adolescents (age 10-16 years) andadults (age 20-30 years) (evidence level 1A).17 In healthy adults, actig-raphy was valid for assessing sleep durations and sleep/wake activity,but less reliable for more specific measures such as sleep offset or sleepefficiency (evidence level 3C).25 There was also no first night effect inhealthy adults (evidence level 3C).16 In nursing home populations,Ancoli-Israel et al. reported correlations between actigraphy and PSGfor TST of 0.81 - 0.91 and for percent sleep of 0.61 - 0.78 (evidence level3C).26
There are discrepant reports about the validity of actigraphy for othersleep variables. One study of four adults found good correlations forsleep onset latencies, wake time after sleep onset, sleep efficiency, andtotal sleep time (evidence level 3C),27 while two other studies of healthyadults found poorer relationships for sleep onset latency and wake timeafter sleep onset with quiet wake being frequently misidentified as sleep(evidence level 2B and 3C respectively).22,23 Early actigraph validationresearch found that the correlation between actigraphy and PSG forsleep onset latency was only 0.53 when sleep onset was defined as thefirst minute of actigraph-estimated sleep, but jumped to 0.94 when sleeponset was defined as the beginning of the first period containing 20 min-utes of actigraph-identified sleep with no more than one minute of wakeintervening.28 However, subsequent research has continued to use thefirst-minute definition. This may account for some of the observed errorin actigraphic scoring not only of sleep onset latency, but also of vari-ables that depend upon it, such as sleep efficiency and wake time aftersleep onset. A study of healthy adults on a shiftwork schedule found poorrelationships with sleep efficiency and less reliability for determiningsleep offset compared to PSG (evidence level 3C).25 Yet others foundthat actigraphy overestimated sleep efficiency and total sleep time inpatients with sleep disorders (evidence level 1A).19 To summarize, whencompared to PSG, actigraphy was found to be valid and reliable fordetecting sleep in normal, healthy adult populations but less reliable fordetecting sleep as sleep became more disturbed (evidence level 2B).22
4.4 Comparisons to Observations, Sleep Logs, and Diaries
Actigraphy has also been compared to both direct observations ofsleep and to sleep logs and diaries. In a study of the effects of circadianrhythms entrainment (entrained vs. free-running) on sleep by Lockley etal., sleep logs and actigraphy yielded similar data for sleep timing, sleepduration, sleep onset and sleep offset but not for sleep latency, numberand duration of night awakenings or number of naps (evidence level1A).29 Nurses’ observations of sleep in psychiatric patients were similarto actigraph data but sleep logs kept by patients in the morning were notfound to be satisfactory (evidence level 4C-a).30 Observations of nursinghome residents by research staff yielded a PVS of 87% and PVW of 90%when compared to actigraphy (evidence level 3C).26
Monk et al. compared both actigraphs and sleep diaries to PSG duringspace flight (evidence level 3C).31 Predicted values of actigraphy wereclearly superior to those of diaries for sleep onset and offset, sleep dura-tion, and sleep efficiency. The authors concluded that in general, actig-raphy is a simple, efficient means of evaluating sleep in situations, suchas space, when PSG is too cumbersome for routine use.31 Dijk et al. mea-sured wrist activity continuously in five astronauts during 10 to 16 daysof space flight, and performed sleep PSG on four of those days (evidencelevel 3C).32 They found that actigraphically estimated sleep duration wassignificantly longer on PSG-recording nights than non-PSG nights. Theyconcluded that astronauts probably adhered more closely to their sched-uled bedtime when their work duties included PSG sleep recording.
Actigraphy appears to be useful in other populations where PSGmight be difficult to obtain, such as in nursing home patients as men-tioned above,26 or in infants and young children. In general, Sadeh con-cluded that with infants, actigraphy should be paired with parental sleeplogs for screening infant sleep problems, although actigraphy appearedto be a more consistent measure than parents’ sleep logs of the child’ssleep/wake (evidence levels 4C-a).33,34 The agreement rates between the
logs and actigraphy declined over time apparently because the parentsincreasingly tended to omit items from the logs. Thus, for determining ifa child’s night awakenings decline during treatment, actigraphy appearsto be more accurate (evidence level 4C-a).35
In a study of children and adolescents, Sadeh found that a minimumof seven nights of actigraphy were needed to get five nights of usefuldata for sleep onset and number of minutes of wake (evidence level 4C-a).33 In another study of children and teenagers, Acebo et al. reportedgood agreement between observations and actigraphy for sleep onset,number of minutes awake, and sleep efficiency (evidence level 4C-a).36
Acebo et al. also found that, in children, more than seven nights of datacollection were needed to get useful data for sleep efficiency, sleep peri-od and number of minutes of sleep.36
4.5 Comparisons to MSLT
In a study of the effects of diphenhydramine vs. placebo on daytimesleepiness, Roehrs et al. showed that MSLT was more sensitive thanactigraphy to sleep loss (evidence level 2B).37 Yet, their data showed thatactigraphy during the day reflected prior sleep loss with more epochs ofinactivity, suggesting more daytime sleep. Since actigraphy is notrestricted to use in a laboratory as is the MSLT, the authors concludedthat actigraphy during the day may yield a more accurate index of theeffects of sleepiness.
4.6 Comparisons to EMG
Since the actigraph records movements, placement on the foot can beused to record movements that are most typical of periodic limb move-ment disorder (PLMD). In a study of PLMD, Kazenwadel et al. foundactigraphy recorded on the foot to be comparable to surface EMG ante-rior tibialis measurements during PSG (evidence level 1A).38 The corre-lations between leg kicks determined by activity counts and tibialisEMG measurements remained high both on and off medication. Theauthors concluded that measurement of PLMD by actigraphy was possi-ble if 0.5-second epochs were used. However, considerable manualadjustment and editing of computerized data were necessary to avoidunderestimating the number of leg kicks. These results were in dis-agreement with those of Sforza et al., who also compared actigraphyrecorded from the foot to PSG-recorded anterior tibialis EMG (evidencelevel 5D-b).39 However, the Sforza et al. study had a very small samplesize for a validity study, and only two out of 35 patients had PLMD. (Foradditional discussion on the use of actigraphy in PLMS see also section5.5, Restless Legs Syndrome/Periodic Limb Movement Disorder)
4.7 Actigraph Placement
Two studies found no difference between data collected from acti-graphs placed on different locations (e.g., dominant wrist, non dominantwrist, ankle, or trunk) (evidence level 3C and 1A respectively).16,17 How-ever, in a series of two studies by Middelkoop et al., other results werefound. In one study, wrist placement was shown to detect more move-ments than ankle placement which in turn detected more movementsthan trunk placement in the first study (evidence level 4C-a).40 In a sec-ond study of healthy adults, wrist placement was again superior to bothankle and trunk placement, however, dominant wrist placement was bet-ter than all other placements at detecting wake (evidence level 4C-b}.41
Violani et al. found that the right wrist recorded more activity than theleft wrist both early and late in the sleep period but no differences werefound between ankle placements (evidence level 4C-a).42 Middelkoopand colleagues concluded that more studies which compare differentplacements of actigraphy concomitant with PSG recordings were need-ed.41
4.8 Artifacts in Actigraphic Recordings
There are some potential artifact problems when using actigraphy for
Actigraphy Review Paper—Ancoli-Israel et alSLEEP, Vol. 26, No. 3, 2003 345

sleep/wake determinations. For example, artifacts can come from non-compliance (not wearing the recorder), from breathing movements, frompostural blocking of arm movements, or from externally imposed move-ment from riding in vehicles.21 Many investigators routinely have vol-unteers who wear actigraphs keep concomitant logs of sleep times andactigraph removal, and use these data to help with artifact rejection.43,44
4.9 Summary
Recent research has refined the ability of actigraphs to studysleep/wake. Although there are still some technical differences in themechanical aspects of how actigraphs accumulate data on movements,how these data are processed, and the nature of the algorithms used toprocess these data, both the actigraphs themselves and the algorithmsthat process the data from actigraphs have improved since the last task-force report published in 1995.1 For example, a method using dichoto-mous indices of activity has been developed to compare activity in-bedto out-of-bed that, among other things, might be useful for studying cir-cadian phase shifts.45 However, no head-to-head comparisons have beenmade between actigraphs and no conclusions can be drawn about whichmethod is more valid vs. PSG.
Actigraphy is useful in populations where PSG would be difficult torecord, such as in demented patients,26 and in astronauts in space.31
There does not seem to be a first night effect with non-sleep disorderedpatients (evidence level 3C),16 which is of particular benefit when onlyone night of recording is possible. If more nights are needed, the acti-graph also has the advantage of being easy to record for multiple nights.There may be advantages of using combined data from actigraphy and asubjective questionnaire with sleep-disordered patients, especially ifthey are excessively somnolent (evidence level 1A).19 For studies ofrhythms or for studies where time of lights out is important, an actigraphthat also records light exposure would be beneficial.5,46
Yet, regardless of the technology, research studies must demonstratethat actigraphy serves the needs of sleep/wake researchers and clini-cians. Given the expanded use of actigraphy, the time has arrived forstandards to be established, similar to those developed for polysomnog-raphy in 1968 by Rechtshaffen and Kales.47 Such standards mightinclude device standards (e.g., digital integration is best) and/or countsdefined with standardized units of measurements (e.g., g-force units) sodata from different machines and algorithms could be compared andcomparisons could be made to other acceleration measures. In addition,bench-test minimal standards for computer programs used with actigra-phy need to be developed.
Ultimately, field tests are needed to determine what actigraphy iscapable of doing and how well it can do it. Data showing that actigraphyis reliable and valid are necessary as are data demonstrating the best pro-cedures for getting the best measurements for sleep/wake evaluations(e.g., best location on the body to place the device, how to analyze rawdata) and evaluating potential problems. Published reports using actigra-phy must contain complete reporting of sensitivity, specificity, scoringalgorithm, and filters, as well as reliability, validity, ruggedness, and arti-fact rejection for the device and computer program used.18 On the otherhand, technical standards may not be as important as simply demon-strating validity and reliability for determination of sleep/wake status ofall actigraphic measurements with any given apparatus and scoring algo-rithm.
5.0 ACTIGRAPHIC ASSESSMENT OF CLINICAL SLEEP DISORDERS
One possible application of actigraphy in sleep medicine has been thediagnosis and assessment of clinical sleep disorders (see Table 3). Com-pared to traditional polysomnography, the actigraph is relatively unob-trusive and can record for multiple days and nights. This may be usefulin the assessment of insomnia patients, whose sleep has been shown tobe quite variable from night to night.48 Moreover, actigraphy makeshome recording more accessible, permitting the evaluation of patients intheir natural sleeping environment and eliminating laboratory effects
that may alter a patient’s typical sleep patterns.The convenience of using actigraphy to evaluate disordered sleep,
however, must be weighed against its reliability and validity as com-pared to the traditional gold standard for sleep assessment, polysomnog-raphy. In addition, a determination of actigraphy’s potential usefulnessmust take into consideration how it compares to alternative methods thatmay be equally or less expensive, such as self-report. Although it mightbe expected that the objective and unbiased nature of data produced bythe actigraph would necessarily be more accurate than those yielded bysubjective assessment techniques such as sleep logs, this assumptionmust be confirmed empirically.
5.1 Insomnia
Chambers, in an analysis of previously published data,49 found thatwhen total sleep time estimates from actigraphs and sleep logs werecompared to polysomnography for a group of insomnia patients, therewas no significant difference in the mean absolute error for the two tech-niques (evidence level 4C-b).50 Moreover, sleep log estimates of totalsleep time had a significantly higher correlation with PSG than did thosefrom actigraphy, suggesting that for insomnia patients as a group, sleeplog error, at least with respect to the estimation of total sleep time, ismore systematic and predictable for sleep logs than for actigraphy. How-ever, this same analysis did reveal a substantial within-subjects, or night-to-night correlation (r = 0.81) between actigraph and PSG total sleeptime. Such a finding indicates that those factors contributing to actigrapherror for a given patient (e.g., periodic leg movements, minimal activityduring extended periods of nocturnal wakefulness) tend to be consistentfrom night to night. Therefore, at least for insomnia patients, actigraphymay be useful in the assessment of sleep variability or in the measure-ment of treatment effects.
A number of recent studies have employed actigraphy in the evalua-tion of sleep of the patient with insomnia; however, few of these studieshave validated the actigraphy findings with PSG data. Guilleminault andcolleagues in a study of non-drug treatments for insomnia, evaluatedpotential subjects using a sleep questionnaire, one week of sleep diaries,and four days of actigraph monitoring (evidence level 4C-b).51 Thesesubjects also underwent one night of laboratory polysomnography, butsimultaneous recording with an actigraph was not performed, so directvalidation of the actigraphy with PSG findings was not possible. How-ever, baseline data from this study did show that actigraphy consistentlyproduced higher estimates of total sleep time and the number of awak-enings and lower estimates of sleep onset latency than those yielded bysleep logs. The differences between actigraph and sleep log data wereattenuated somewhat in the post-treatment recordings, with greater treat-ment-related improvement seen in sleep log variables than in actigraphvariables.
Wilson et al., in a study of insomnia patients with musculoskeletalpain, found a similar discrepancy between the sleep estimates reportedon sleep logs and those determined by the actigraph, with a much largerdisagreement in the number of awakenings during the night (evidencelevel 5D-b).52 These researchers found relatively low correlations amongpatients (r = 0.34 to 0.42) between the two measures for estimates oftotal sleep time and number of awakenings, and no significant correla-tion for sleep efficiency. Consistent with the analysis of Chambers (evi-dence level 4C-b),50 the highest correlation found in this study was fornight-to-night actigraphic estimates of total sleep time. However, acti-graph sleep variables consistently failed to produce significant correla-tions with clinical assessment measures such as pain severity estimatesor scores on the Pittsburgh Sleep Quality Index. Two other studies alsofailed to find correlations between actigraph sleep variables and globalsubjective reports of well-being, sleep behaviors, and health-relatedsymptoms (evidence level for both 5D-b).53,54
Wicklow and Espie examined the relationship between cognitiveintrusions prior to sleep onset and sleep-related variables as measured byactigraphy and sleep logs (evidence level 4C-a).55 Their findings indi-cated that the presence of certain categories of intrusive thoughts was
Actigraphy Review Paper—Ancoli-Israel et alSLEEP, Vol. 26, No. 3, 2003 346

associated with longer sleep-onset latencies, but only as measured byactigraphy, not sleep logs. These researchers also found that actigraphicTST was greater and sleep latency was less than that indicated by sleeplogs. However, there were significant correlations (r = .419 for sleeplatency, r = .526 for TST, both p < .001) between the two methods forthese variables.
5.2 Insomnia Secondary to Circadian Rhythm Disturbance
Other researchers have utilized actigraphy to assess insomnia com-plaints secondary to a circadian rhythm disturbance. Kerkhof and vanVianen divided a group of chronic insomniacs into early- and late-sleepphase groups, based on oral body temperature data, and found greaternocturnal motor activity, as measured by actigraph, in the early phasegroup (evidence level 4C-b).56 This finding was consistent with the sub-jective assessments of these subjects, who reported spending more timeawake during the night than the late phase group. Several studies haveused actigraphy to assist in the diagnosis of delayed sleep phase syn-drome (DSPS) and to assess effects of DSPS treatments.44,45,57-61 DSPSis characterized by a consistent pattern of late sleep onset and offset,often making diagnosis by PSG impractical. Although sleep logs areoften used to diagnose DSPS, actigraphy can potentially offer objectiveevidence about rest-activity patterns that either corroborates logs or callsthem into question. Dagan et al. used 4-7 days of actigraphy at home inconjunction with a comprehensive clinical assessment to diagnosedozens of subjects with DSPS, but they offered no independent evidenceof the validity of this method (evidence level 5D-a).57 Similarly, Quintoet al. reported that actigraphy “confirmed” sleep logs in a case ofDSPS.59 Minors et al. reported that there were significant differences inwrist activity patterns that distinguished people with DSPS from normalsleepers (evidence level 4C-b).45 Nagtegaal et al., in two separate stud-ies, provided evidence that wrist activity patterns in DSPS were consis-tent with a “gold-standard” biological marker of circadian rhythm dis-turbance. In the first study (a case report), they found that the late timeof day of low activity corresponded with a late period of high melatoninsecretion in a case of DSPS.60 In the second study (a randomized, place-bo-controlled trial), they found that actigraphy detected a 38-minuteadvance in sleep-onset time with melatonin treatment, parallelingadvances in dim-light melatonin onset. Sleep log variables, however,failed to detect this phase shift (evidence level 1A).61 Cole et al. also pro-vided objective evidence that actigraphy can detect circadian rhythmdisturbance in DSPS (evidence level 2B).44 They reported that the circa-dian phase of melatonin secretion was significantly delayed, comparedto normal, historical controls, in 45 DSPS volunteers whose delayedsleep was identified both by actigraphy and sleep logs. Additional infor-mation on the use of actigraphy in circadian rhythms can be found insection 6.0.
5.3 Disturbed Sleep in Children
Actigraphy has also been used to assess disturbed sleep in children.Franck et al. compared sleep, recorded by actigraph, of HIV-infectedchildren to that of normal controls and confirmed that sleep-related com-plaints, as reported by parents, were greater in the patient group (evi-dence level 4C-b).62 Actigraph estimates of sleep efficiency, WASO, andnumber of awakenings were significantly different between the twogroups, while differences in TST and SOL failed to reach significance.Within the patient group, the only significant correlation between acti-graph data and subjective reports was for night waking. Another studyexamined autistic children with and without parent-reported sleep prob-lems and found an earlier sleep offset time for the sleep problem groupbut no other significant differences in actigraphically measured sleepvariables (evidence level 5D-b).63 Sadeh et al. using actigraphy, report-ed that newborns slept twice as much during night time hours than dur-ing the day and that later gestational age was correlated with anincreased percentage of quiet sleep time (evidence level 4C-b).64 In acase report, Etzioni et al., using wrist actigraphy, found that 3mg of
melatonin administered in the evening for two weeks restored sleep con-tinuity in a child with a germ cell tumor involving the pineal region.65
Some studies have used actigraphy to examine developmental differ-ences in sleep patterns. Sadeh et al. recorded the sleep of school-agechildren for 4 to 5 nights and found that older subjects had delayedsleep-onset times, shorter sleep periods, and shorter sleep times thanyounger subjects (evidence level 4C-b).66 They also found that increasedreported daytime sleepiness was associated with greater age and shortersleep periods, as measured by the actigraphy. Aronen et al. demonstrat-ed that actigraphically measured TST was negatively correlated withteacher-reported behavioral symptoms in young children (evidence level4C-b).67 Kramer et al., although not specifically studying children, didshow apparent developmental differences in sleep between young andelderly adult subjects (evidence level 4C-b).68 They found the elderlysubjects, whose average age was 65 years, to have less variability fortime in bed, advanced sleep phase, and more nocturnal awakenings thanthe younger subjects (mean age = 20.6 years).
5.4 Sleep-Related Breathing Disorders
Several study protocols have attempted to detect the presence ofobstructive sleep apnea from actigraphic data. This work has generallyrelied on the fact that compared to normal sleepers, apnea patients havemore fragmented sleep and that this fragmentation is manifested in bodymovements that can be detected by the actigraph. Middelkoop et al.found that the average duration of periods with no movement (i.e., noactivity), as measured by the actigraph, differed significantly amongthree subject groups of varying apnea severity (evidence level 4C-b).69
No other actigraph or sleep log variable correlated significantly with theapnea index. However, the proportion of variance accounted for by thisvariable was small (11%), and the sensitivity of this measure to detectsubjects with an apnea index greater than 5 was 5% while the specifici-ty was 100%.
Drinnan et al. attempted to determine whether the specific placementof the actigraph might affect its accuracy in the identification of arousalsassociated with sleep-disordered breathing (evidence level 5D-b).70
Their data revealed that a left tibia placement resulted in the most favor-able relationship between actigraph-measured movement and EEGarousals, with placement on the right tibia, left ankle, and left wrist far-ing somewhat worse. Still, none of the placements yielded statisticallysignificant correlations with EEG arousals, and none were adequate inpredicting the degree of sleep disordered breathing present. As with theMiddelkoop et al. study (evidence level 4C-b),69 however, the relativelylow severity of sleep apnea among patients in this study (mean apnea-hypopnea index or AHI = 18.9) may have limited the power of the tech-nique to differentiate between groups.
Kushida et al. compared PSG, actigraphy and subjective reports in astudy of 100 sleep clinic patients, the majority of whom had a diagnosisof obstructive sleep apnea syndrome or upper airway resistance syn-drome (evidence level 2B).19 Consistent with previous studies, theyfound that the actigraph was considerably better at detecting sleep thandetecting wakefulness, with a sensitivity of 98% for sleep detection anda specificity of 48% for wake detection using a high-threshold algo-rithm. This algorithm compared PSG and actigraphic data in 30-secondepochs, modifying the activity counts during the epoch by the level ofactivity in the surrounding 2-minute time period. When compared toPSG, the actigraph was much more prone to overestimate total sleep timeand sleep efficiency than was subjective patient report. However, theactigraph’s estimates of number of nocturnal awakenings did not differsignificantly from PSG data while self-report did, suggesting actigraphywas more accurate than the patient’s subjective reports.
Elbaz et al. reported on an inventive use of actigraphy in the diagno-sis of sleep-disordered breathing that combines the actigraph with whatthey termed “simplified polysomnography,” consisting of airflow, tho-racic and abdominal movements, and pulse oximetry (evidence level3C).71 They reasoned that the addition of actigraphy could improve theestimation of the RDI from that of simplified polysomnography alone by
Actigraphy Review Paper—Ancoli-Israel et alSLEEP, Vol. 26, No. 3, 2003 347

supplying a more precise value for TST than the traditionally used TIB.However, the actual increase in correlation with RDI estimates from tra-ditional polysomnography was somewhat modest, from r = .94 for sim-plified polysomnography alone to r = .976 for simplified polysomnogra-phy plus actigraphy. The authors did find that specificity and negativepredictive value were substantially improved with use of the actigraph,but only for severe OSAS (RDI > 30).
5.5 Restless Legs Syndrome/Periodic Limb Movement Disorder
One of the more natural applications of actigraphy has been in theidentification and assessment of periodic leg movement disorder(PLMD). Sforza et al. conducted a study of 35 patients with varyingdiagnoses to determine if actigraphy could reliably detect leg move-ments during sleep (evidence level 5D-b).39 Subjects were simultane-ously recorded using PSG and actigraphy placed on the upper part of theright foot. PSG-recorded EMG tibialis activity was visually scored andclassified in 8 levels based on duration and amplitude. Actigraphic datawere collected in 5-second epochs and compared directly to EMG activ-ity of similar-length epochs. The results of this analysis revealed thatalthough there was a high correlation between the two collection meth-ods, actigraphy substantially underestimated the number of movementsyielded by the EMG. However, this failure may be attributable to the lowsensitivity of the actigraph used, which is only able to detect accelera-tions greater than 0.1 g. In contrast, Pollak used actigraphs that were sen-sitive to 0.033 and 0.024 g, respectively (evidence level 4C).18 ForSforza, agreement was greater for the activity events with greater dura-tion and amplitude. Because of the actigraph’s failure to detect manyevents of lesser duration or amplitude, this study’s authors concludedthat the device “cannot be regarded as a good method to estimate motoractivity during sleep” (p. 158). However, other authors did note that theactigraph had adequate night-to-night reliability and suggested that itmight be useful in the assessment of treatment effects in patients withPLMD or restless legs syndrome (RLS) (evidence level 4 C-b and 5 D-b, respectively).50,52
Two recent studies have employed actigraphy in the evaluation oftreatment efficacy for RLS.72,73 Trenkwalder et al. in a placebo-con-trolled crossover design, studied the effects of L-dopa therapy for idio-pathic and uremic restless legs syndrome, using both PSG and actigra-phy at baseline and at the end of each treatment period (evidence level1A).72 Their data revealed that treatment resulted in a significant reduc-tion of leg movements, measured by both PSG and actigraph, for bothpatient types. Both PSG and actigraphic data also showed that thisimprovement was limited to the first 4 hours of recording time. Parallelto these objective indices, subjective measures such as sleep diaries andquality of life ratings showed similar improvement in response to treat-ment. Furthermore, because actigraphy was continued for two addition-al nights after the PSG study, the authors were able to confirm the sta-bility of this treatment effect.
Collado-Seidel et al. conducted a similar study of L-dopa and slow-release L-dopa efficacy, but without the use of polysomnography (evi-dence level 4C-b).73 Like Trenkwalder et al.,72 these researchers foundsignificant treatment-related effects for most actigraphic variables,including movements per hour and number of movement episodes. Onlythe change in the time without movements in the first half of the nightfailed to reach significance. Subjective improvements were also seenwith patients reporting increases in sleep quality and overall well-beingand decreases in number of awakenings, time awake, and reports of day-time fatigue.
5.6 Other Sleep Disorders
Various case reports have employed actigraphy in the assessment ofother sleep disorders, including fatal familial insomnia,74 non-24-hoursleep-wake syndrome,75,76 REM sleep behavior disorder,77 and posttrau-matic delayed sleep phase syndrome.59 In each of these reports, the acti-graph provided data relevant to the patients’ sleep/wake patterns, in
many cases over a substantial period of time. However, these case stud-ies did not compare the actigraphy data to PSG, nor did they indicatewhether the actigraph alone was sufficient to diagnose the conditions.
5.7 Summary
Recent literature suggested that actigraphy might have some value inthe assessment of sleep disorders. For insomnia, actigraphy may be mostvaluable in assessing treatment effects or night-to-night variations insubjects’ sleep. It has been demonstrated that actigraphy has the abilityto detect sleep phase alterations associated with circadian rhythm distur-bances. Additionally, actigraphy is capable of distinguishing moderate tosevere sleep apnea patients from normal controls, due to its greater sen-sitivity, compared to sleep logs, in detecting brief arousals from sleep.For patients with restless legs and periodic leg movements, the diagnos-tic value of actigraphy is limited by its tendency to underestimate the fre-quency of leg movements during sleep. However, it does show somepromise in the assessment of treatment-related improvement.
Later-generation scoring algorithms have demonstrated greater accu-racy than earlier versions in the detection of sleep and wake, improvingthe actigraph’s ability to detect sleep latency, nocturnal awakenings, andtotal sleep time, variables important in evaluating an insomnia com-plaint. The actigraph appears to have a particular advantage over alter-native assessment methods such as sleep logs in the measurement ofawakenings during the night, as many of these awakenings appear to goundetected by patients and subjects completing sleep diaries. The abili-ty of actigraphy for detecting activity also holds some promise in theidentification of other disorders characterized by frequent movementssuch as obstructive sleep apnea and periodic limb movement disorder.Perhaps of greatest importance is the actigraph’s ability to measurenight-to-night changes in sleep patterns within a given individual, afunction that has great value for assessing treatment effects and otherfactors that affect the consistency of a patient’s sleep. This, combinedwith its relative economy in assessing sleep-wake patterns over extend-ed periods of time, suggests a potentially important role for the actigraphin longitudinal research and clinical studies in which long-term changesin sleep patterns are of particular interest.
The actigraph’s limitations, however, continue to restrict its value as astand-alone diagnostic device. Recent research has reasserted the find-ings from previous studies that the accuracy of the actigraph to detectsleep and wakefulness declines as sleep efficiency is decreased, a prob-lem particularly relevant to insomnia and other sleep disorders. Thereare indications that for the simple estimation of total sleep time, insom-nia patients’ subjective estimates outperform the actigraph (evidencelevel 4 C-b).50 Moreover, although the actigraph may be able to distin-guish patients with a particular sleep disorder (e.g., obstructive sleepapnea, periodic limb movement disorder) from normal controls, there isvirtually no evidence to date that the actigraph can distinguish betweendifferent sleep disorders. Until such evidence becomes available, theactigraph’s function in the assessment and diagnosis of clinical sleep dis-orders is likely to be restricted to the role of an adjunct to clinical histo-ry, sleep diary data, and PSG findings or to examine treatment effectsand follow-up.
6.0 CIRCADIAN RHYTHMS
Activity is a standard marker of circadian rhythms in studies of non-human mammals. This section examines the use of wrist activity in themeasurement of circadian rhythms in humans. In the studies reviewedhere, wrist actigraphy was used in a number of different ways relevantto human rhythms. Methodologies included characterizing spontaneousrhythms in adults, children, infants and the elderly, exploring the rela-tionships between activity rhythms and the light-dark cycle, helping toidentify sleep or rhythm disturbances induced by change of schedule,measuring improvement in disturbed rhythms after experimental inter-vention, helping to diagnose circadian rhythm sleep disorders, charac-terizing rhythm abnormalities that accompany dementia or psychiatric
Actigraphy Review Paper—Ancoli-Israel et alSLEEP, Vol. 26, No. 3, 2003 348
disturbance, and investigating the role of motor activity in cardiovascu-lar rhythms.
6.1 Actigraphy for the Study of Circadian Rhythms
Several studies have demonstrated that human wrist activity oftenshows a robust circadian pattern. Pollak et al. showed that the circadianperiod of the actigraph-defined sleep/wake rhythm accurately predictedthe period of the PSG-defined sleep/wake rhythm, measured simultane-ously (evidence level 3C).21
Actigraphs have measured circadian rhythms under circumstanceswhere it would not be practical to record with polysomnography. Forexample, Binkley measured wrist activity in one woman continuouslyfor an entire year.78 She found well-defined, entrained circadian rest-activity cycles, changes in sleep length synchronized with the menstrualcycle, and annual phase changes she attributed to daylight saving time.Wirz-Justice and colleagues presented several case reports in which acti-graphs were worn daily by demented or psychiatric patients for extend-ed periods of up to 1.5 years.79-84 The long-duration recordings allowedthe authors to produce plots that graphically revealed striking changes incircadian rhythms over time. These included severe, apparently medica-tion-induced disruption of the rest activity cycle, the gradual consolida-tion of the cycle upon change of medication, circadian effects ofimposed therapeutic rest/activity schedules, and the gradual decline ofcircadian organization over time. Siegmund et al. measured seven-daywrist activity rhythms in inhabitants of Papua New Guinea, living in atraditional culture without electric lights (evidence level 4C).85 Theyfound that rest-activity rhythms were synchronized with the light-darkcycle, and that time of arising was more consistent than bedtime. Acti-graphic recordings in infants showed that circadian activity rhythmsarose from ultradian antecedents. Periods of inactivity presumablyencompassing sleep were shorter (9-12 hours/day) than typically foundin European society. In another actigraphic study of infants, “sleep” dif-ferences were not explained by differences in temperament (evidencelevel 5D-b).86 Dijk et al. measuring wrist activity during 10 to 16 daysof space flight, visually identified imposed advances in the sleep-wakeschedule, and noted that time of arising was more regular than bedtime(evidence level 3C).32
In the studies cited above, and many others,87-91 circadian rhythmresults were computed from actigraphic sleep/wake predictions. Usual-ly, the phase marker was sleep onset time or sleep offset time. Similarly,Binkley marked circadian phase with visually identified “activity onset”and “activity offset,” defined by threshold criteria similar to those usedin some sleep/wake prediction algorithms (evidence level 4C-b).92
Another way actigraphic sleep/wake predictions (or similar “activitylevel” scores) have been used to yield circadian results is by showingthat actigraph-identified sleep is disturbed when people attempt to sleepout of phase with their endogenous rhythm, as in shift work,93-96 jet
lag,92,97 illness,91 or experimental manipulations of the sleep/wakecycle,87,98 or by showing98 that sleep is improved by treatment that nor-malizes rhythms.93,99-101 For example, both Dawson et al.93 and Yoon etal.102 found that actigraphic indicators of sleep improved during the dayfollowing simulated night shift work in volunteers treated with brightlight or melatonin, but not in those treated with placebo (evidence levels4C-b). Actigraphy was also used to infer when shiftworking nurses sleptand, along with shifts of the melatonin rhythm, demonstrated that a sub-group of nurses was able to successfully adapt to rapid changes in work-shift (evidence levels 4C-b).94,95
Although three shift work studies reported negative results,103-105
enough well-designed, well-controlled studies showed significant dis-turbance of actigraph-defined sleep after shift work or other circadiandisturbance to make a convincing case that actigraphy can be useful fordetecting such disturbances (evidence levels 3C to 4C-b).87,91-95,97,98,106
6.2 Actigraphy Algorithms for Computing Circadian Rhythms
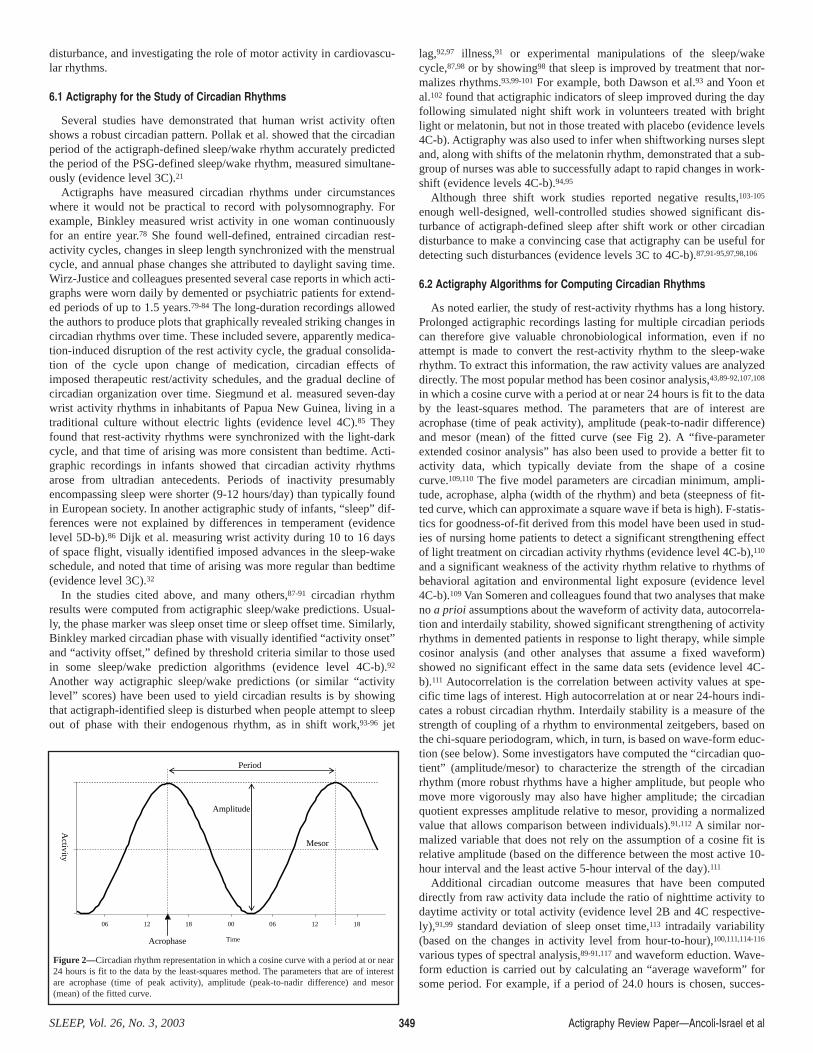
As noted earlier, the study of rest-activity rhythms has a long history.Prolonged actigraphic recordings lasting for multiple circadian periodscan therefore give valuable chronobiological information, even if noattempt is made to convert the rest-activity rhythm to the sleep-wakerhythm. To extract this information, the raw activity values are analyzeddirectly. The most popular method has been cosinor analysis,43,89-92,107,108
in which a cosine curve with a period at or near 24 hours is fit to the databy the least-squares method. The parameters that are of interest areacrophase (time of peak activity), amplitude (peak-to-nadir difference)and mesor (mean) of the fitted curve (see Fig 2). A “five-parameterextended cosinor analysis” has also been used to provide a better fit toactivity data, which typically deviate from the shape of a cosinecurve.109,110 The five model parameters are circadian minimum, ampli-tude, acrophase, alpha (width of the rhythm) and beta (steepness of fit-ted curve, which can approximate a square wave if beta is high). F-statis-tics for goodness-of-fit derived from this model have been used in stud-ies of nursing home patients to detect a significant strengthening effectof light treatment on circadian activity rhythms (evidence level 4C-b),110
and a significant weakness of the activity rhythm relative to rhythms ofbehavioral agitation and environmental light exposure (evidence level4C-b).109 Van Someren and colleagues found that two analyses that makeno a prioi assumptions about the waveform of activity data, autocorrela-tion and interdaily stability, showed significant strengthening of activityrhythms in demented patients in response to light therapy, while simplecosinor analysis (and other analyses that assume a fixed waveform)showed no significant effect in the same data sets (evidence level 4C-b).111 Autocorrelation is the correlation between activity values at spe-cific time lags of interest. High autocorrelation at or near 24-hours indi-cates a robust circadian rhythm. Interdaily stability is a measure of thestrength of coupling of a rhythm to environmental zeitgebers, based onthe chi-square periodogram, which, in turn, is based on wave-form educ-tion (see below). Some investigators have computed the “circadian quo-tient” (amplitude/mesor) to characterize the strength of the circadianrhythm (more robust rhythms have a higher amplitude, but people whomove more vigorously may also have higher amplitude; the circadianquotient expresses amplitude relative to mesor, providing a normalizedvalue that allows comparison between individuals).91,112 A similar nor-malized variable that does not rely on the assumption of a cosine fit isrelative amplitude (based on the difference between the most active 10-hour interval and the least active 5-hour interval of the day).111
Additional circadian outcome measures that have been computeddirectly from raw activity data include the ratio of nighttime activity todaytime activity or total activity (evidence level 2B and 4C respective-ly),91,99 standard deviation of sleep onset time,113 intradaily variability(based on the changes in activity level from hour-to-hour),100,111,114-116
various types of spectral analysis,89-91,117 and waveform eduction. Wave-form eduction is carried out by calculating an “average waveform” forsome period. For example, if a period of 24.0 hours is chosen, succes-
Actigraphy Review Paper—Ancoli-Israel et alSLEEP, Vol. 26, No. 3, 2003 349
Amplitude
Mesor
06 12 18 00 06 12 18
Time
Period
Acrophase
Activity
Figure 2—Circadian rhythm representation in which a cosine curve with a period at or near24 hours is fit to the data by the least-squares method. The parameters that are of interestare acrophase (time of peak activity), amplitude (peak-to-nadir difference) and mesor(mean) of the fitted curve.

sive activity levels at similar times of the 24.0-hour day are averaged.Sleep-wake consolidation is the extent to which continuous bouts ofsleep and wakefulness are clustered into periods that are circadian (lastfor several hours). Waveform eduction can be quantified by a measure-ment related to the lengths of the “stair treads and risers” in cumulativeplots of sleep vs. wakefulness.21
6.3 Actigraphy versus Other Methodologies for Determining CircadianRhythms
Several studies compared circadian outcomes derived from wristactigraphy to those derived from other measurement methods consideredreference standards. Pollak’s finding that actigraphic sleep/wake predic-tions have the same circadian period as PSG sleep/wake scores suggest-ed that actigraphy could provide valid measurements of entrainedsleep/wake rhythms (evidence level 3C).21 Youngstedt et al. providedgood evidence that the phases of actigraph-identified bedtime, wake-uptime, mid-sleep time and acrophase were all significantly correlated withthe acrophase of urinary 6-sulphatoxymelatonin secretion in entrainedyoung and elderly adults living at home (evidence level 1A).43 Cole etal. found similar home results in volunteers with delayed sleep phasesyndrome (DSPS) (evidence level 2B).44 Middleton et al. found that thephase and period of actigraph-derived sleep onset time, wake-up timeand fitted cosine were generally consistent with those of both 6-sulpha-toxymelatonin and “demasked” core body temperature in men undergo-ing experimental manipulations in constant dim light (both evidence lev-els 2B).89,90 However, these studies also showed that activity rhythmswere less stable than melatonin or temperature rhythms, and could bereadily masked by voluntary behavior. Carskadon et al., studying ado-lescents, found correlations ranging from .39 to .82 between actigraph-identified sleep onset time at home and salivary dim light melatoninonset time (evidence level 2B to 3C).118,119 However, in one study thecorrelation dropped to a non-significant level under an imposed light-dark cycle,118 and in the other it was not significant on weekends.119
Heikkilä et al. found that in children suffering a severe medical disorder,the circadian rhythm of wrist activity could be grossly disturbed despitenormal rhythms of melatonin, temperature and cortisol (evidence level5D).120 Guilleminault et al. found that consolidated wakefulness, visual-ly scored from wrist activity, only developed in infants after they estab-lished a circadian rectal temperature rhythm (evidence level 3C).121 Bla-grove et al. provided very strong evidence that actigraph-identified sleepwas influenced directly by the central circadian pacemaker (presumablythe suprachiasmatic nuclei, or SCN of the hypothalamus) (evidence level3C).87 They measured wrist activity during a forced desynchrony proto-col in which volunteers lived on a 27-hour day (9 hours in bed, 18 hoursup and active), so the pacemaker free-ran at a period closer to 24 hours,and sleep was attempted at various circadian phases. Despite theimposed rest-activity rhythm, actigraph-identified total sleep time waslower when sleep was attempted at an unfavorable phase of the circadi-an cycle. This strongly suggested that the influence of the circadianclock on actigraph-identified sleep could not be entirely masked by asocially-dictated rest/activity schedule. On the other hand, the maskingeffect of the imposed schedules was substantial, and this was likely to betrue of actigraph studies in general. Because of their susceptibility tomasking, wrist activity rhythms alone cannot be used as pure markers ofSCN circadian output, even though they contain an SCN signal. Actig-raphy has been used to “demask” the circadian temperature rhythm, byremoving the effects of activity and inactivity (evidence level 5D-b).98
Another line of evidence that actigraphy can accurately characterizethe circadian sleep/wake rhythm is that the rhythm of actigraph-inferredsleep/wake generally agrees with that of sleep/wake reported on sleeplogs (evidence level 3C).29 This raises the question of whether sleep logsare just as good as actigraphs for circadian measurements. Two studiessuggest a possible advantage of actigraphy, that is, that it may identifynaps that volunteers do not report on their sleep logs (both evidence level4C-a).88,103 However, actigraphy may also identify naps when none exist.
6.4 Actigraphy and Circadian Rhythm Sleep Disorders
There is good evidence that actigraphy can detect circadian phasedelays in people with DSPS, corresponding to delays in melatoninrhythms (level 1A to 2B) e.g., (44,60,61). This evidence is summarizedabove in the section 5.2. Insomnia Secondary to Circadian Rhythm Dis-turbance. There are also case reports in which actigraphy identified sys-tematic delays of the rest-activity cycle in non-24-hour sleep-wake syn-drome.75,76
6.5 Actigraphy and Circadian Rhythms in Aging and Dementia
Actigraphy has been used to explore circadian rhythms in aging anddementia. Three studies found that the overall activity level declinedwith age (evidence level 4C-b to 5D-a),108,122,123 as did the amplitude ofthe circadian rest-activity cycle (evidence levels 4C-b).116,124 Fragmenta-tion (hour-to-hour variability) of the rest-activity rhythm was found inhealthy elderly101,116 and could be reduced in elderly men by aerobictraining (evidence levels 4C-b).101
Mishima found increased overall activity and nighttime activity inAlzheimer’s disease (evidence level 4C-b).125 Friedman et al. showedthat actigraphic measures of circadian activity (including amplitude,acrophase and mesor) did not correlate significantly with behavioral dis-turbance in patients with Alzheimer’s disease (AD) (evidence level 4C-b).126 Martin et al. found little evidence of sundowning (increased agita-tion around sunset) (evidence level 4C-b).109 Actigraphic rest-activityrhythms in demented patients were stabilized by increased illuminationif vision was intact (evidence level 4C).100
6.6 Actigraphy and Cardiovascular Rhythms
Another group of studies used sleep and wake activity to help distin-guish “dippers” (people whose blood pressure decreases normally atnight) from “non-dippers” (blood pressure that remains the same or risesduring sleep). Although sleep wake activity was not necessarily corre-lated with blood pressure or heart rate (evidence level 5D-b),127 twostudies found that dippers have lower nocturnal activity than nondippers(both at evidence level 4C).128,129 Daytime activity levels were also cor-related with the nocturnal dip in BP (evidence level 4C).129 By usingactigraphy to define sleep and wake periods, a calcium-channel blockerwas found to have therapeutic effects in hypertensives that differedaccording to the time of day it was administered (evidence level 4C-b).130 A third study found that defining “night” as the actigraph-identi-fied sleep period yielded very different blood pressure results than diddefining “night” by fixed clock time criteria (evidence level 5D-a).131
6.7 Actigraphy and Circadian Rhythms in Psychiatry
Actigraphy has also been used to examine circadian rhythms in psy-chiatry. Wirz-Justice and colleagues found severe disturbance of rest-activity rhythms in one bipolar individual82 and several schizophrenicindividuals recorded for extended periods (evidence level 5D-a).79,81,83
Similarly, Martin et al. found that both rest-activity rhythms and acti-graph-identified sleep were often seriously disturbed in 28 olderschizophrenics (evidence level 4C-b).132 The magnitude of disturbancewas associated with the degree of neuropsychological impairment. Neu-roleptic-induced akathisia was associated with increased motor activityin schizophrenic patients, at least at certain times of the day (evidencelevel 4C-a).133 Two studies reported that specific depressive syndromeswere characterized by distinctive circadian activity rhythms.107,134 Glodet al. found blunted circadian amplitude but normal phase of wrist activ-ity in children with Seasonal Affective Disorder, compared to healthycontrols (evidence level 4C-b).107 Lemke et al. found that depressedadult inpatients displayed significantly greater motor activity in themorning than the evening (evidence level 4C-b).134
These studies, taken together, provide preliminary evidence that actig-raphy may prove useful for characterizing and monitoring the circadian
Actigraphy Review Paper—Ancoli-Israel et alSLEEP, Vol. 26, No. 3, 2003 350

rhythm disturbances that often accompany psychiatric disorders.
6.8 Summary
In summary, actigraphy has been used successfully in a variety ofhuman circadian studies. Wrist activity appears to be a valid marker ofentrained PSG sleep phase, and a strong correlate of entrained endoge-nous circadian phase. Under non-entrained conditions, wrist activityrhythms may become dissociated from the endogenous rhythm of theSCN pacemaker; however, actigraphy still appears to be useful for iden-tifying disturbed sleep caused by disruption of circadian rhythms, andimproved sleep caused by treatments that improve rhythms. There is evi-dence that the circadian phase of wrist activity covaries with the phaseof melatonin secretion in DSPS, supporting the use of actigraphy inhelping to diagnose this condition. Actigraphy may also be useful in cir-cadian characterization of non-sleep disorders, such as schizophreniaand hypertension. A variety of methods for analyzing circadian aspectsof activity data show promise. It would be useful to formally comparethese to arrive at standard methodology.
7.0 OTHER CLINICAL RESEARCH
Actigraphy has been used as a measure of sleep/wake activity or cir-cadian rhythms in a broad range of clinical studies. These studies varyconsiderably with respect to the specific actigraphy variables of interest,the methodology used and the types of individuals studied. Unfortunate-ly, many of these studies do not report adequate detailed information onthe technical aspects of the actigraphy devices used, and few studiesattempt validity testing on the use of actigraphy in the particular popu-lation or setting studied.
7.1 Actigraphy in Sleep Intervention Trials and Comparative Studies ofSleep/Activity
Much of the work using actigraphy as a measure of sleep disorders isreviewed earlier in this paper (see section 5.0). This section focuses onthe use of actigraphy as an outcome measure in other sleep interventiontrials and in comparative studies of sleep or activity.
In a placebo-controlled clinical trial of controlled-release melatonintreatment for insomnia in older people (mean age 76 years), Garfinkel etal. reported that melatonin administration resulted in greater sleep effi-ciency and shorter wake after sleep onset, both estimated by wrist actig-raphy (evidence level 4C-b).135 Friedman et al. used multiple modali-ties, including actigraphy, to measure sleep outcomes in a trial compar-ing the effects of sleep restriction and sleep hygiene treatments on thesleep of older adults (aged 55 years or older) with insomnia (evidencelevel 2B).136 The main study outcomes found few between-group differ-ences in treatment efficacy. However, in a sub-sample of 16 subjectswho had simultaneous wrist actigraphy and polysomnography for 3nights, wrist actigraphy estimation significantly correlated withpolysomnographic estimation of total sleep time (r = .96), sleep effi-ciency (r = .63), sleep latency (r = .72) and wake after sleep onset (r =.68). In this study, wrist actigraph variables correlated more highly thansleep log data with polysomnography results.
Maus et al. performed actigraphy in a study of circulating cate-cholamines and aqueous flow in the eyes of normal subjects and in thosewith severe obstructive sleep apnea (evidence level 4C-b).137 Sleepapnea subjects, who were untreated on the night of testing, had a signif-icantly higher nighttime activity index as measured by actigraphy(p<.001) and lower sleep efficiency (p<.001) compared to healthy con-trols. In addition, there were significant differences in activity index andsleep efficiency in controls who were kept awake during the night ver-sus those allowed to sleep.
Pollak et al. studied a small group of community-dwelling elderlypeople who frequently used bedtime medications (including benzodi-azepines, minor analgesics, antihistamines and antidepressants) andcompared them to elderly controls who did not have sleeping difficulty
and did not use hypnotics (evidence level 4C-b).138 Although there wereno differences between groups when the 24-hour period was consideredas a whole, post-hoc comparisons in the early morning hours indicatedthat subjects using bedtime medications became active, as measured byactigraphy, about 1.5 hours earlier in the morning than controls.
7.2 Actigraphy in Studies of Healthy Adults
Several studies involving normal individuals under differing testingsituations have used actigraphy as a measure of sleep/wake or circadianrhythms. Duka et al. measured wrist movement in a placebo-controlledstudy of the effects of a beta-carboline benzodiazepine receptor antago-nist on night sleep pattern in healthy male volunteers (evidence level 5D-a).139 Compared to placebo, the benzodiazepine receptor antagonistinduced activation as measured by actigraphy (i.e., frequency of move-ment and intensity of movement). French et al. used actigraphy to mea-sure sleep patterns in military aircraft crew members undergoing simu-lated, long duration bomber missions (evidence level 4C-b).140 Theyfound shorter sleep duration and greater wrist activity during sleep peri-ods during the first mission, with evidence of improvement in sleep insubsequent missions. In a study of the effects on sleep from caffeinatedbeverages in healthy volunteers, Hindmarch et al. found a dose-depen-dent negative effect (of caffeine) on total sleep time as estimated bywrist actigraphy (evidence level 4C-b).141 In another study, Hindmarchet al. found that promethazine (a sedating antihistamine) caused a sig-nificant increase in percent sleep, as estimated by wrist actigraphy, dur-ing the daytime and across the study period compared with differentdoses of fexofenadine, loratadine and placebo (evidence level 4C-b).142
Jean-Louis et al. analyzed actigraphy data in a large sample (N=273)of community-dwelling residents of San Diego who had been identifiedby random telephone survey (evidence level 4C-b).143 In this cross-sec-tional study, they found significant differences between men andwomen, and between Caucasian and minority subjects, in sleep variablesestimated by wrist actigraphy. In a second smaller community-basedsample (n=32), Jean-Louis et al. used wrist actigraphy in healthy volun-teers and again found significant gender differences, with women hav-ing a better sleep profile than men (evidence level 4C-b).122
Mendlowicz et al. performed an observational study using wrist actig-raphy in community dwelling volunteers. In regression analysis theyfound several significant predictors of depressed mood, including thefollowing variables estimated by actigraphy: daytime activity level,sleep onset latency, wake after sleep onset, total sleep time and total timein bed (evidence level 5D-a).144 Moorcroft et al. used nocturnal actigra-phy to estimate sleep and wake periods and time of final awakening inpeople who reported the ability to self-awaken at a self-predeterminedtime without external means and found that they were in fact able to doso (with a 95% confidence interval of 4.1-10.7 minutes) (evidence level5D-b).145
Pankhurst et al., studying the influence of bed partners on nighttimewrist activity in community dwelling adults living in the United King-dom, found that subjects sleeping with bed partners had a greater num-ber of movements than subjects who slept alone, and movementsdecreased during the temporary absence of the usual bed partner (evi-dence level 4C-b).146 In a similar but larger sample in the UK, Reyner etal. found a significant decline with age in average movement as mea-sured by wrist actigraphy, with men having more nighttime movementthan women (evidence level 4C-b).147 The authors compared sleep logreports of time of sleep onset with actigraphy estimation of sleep onset,and found that the time difference between the two methods was small;however, the actual time difference was not reported in the manuscript.
7.3 Actigraphy in Studies of Cancer-related Fatigue
Actigraphy has also been used in descriptive studies of cancer-relatedfatigue. In an observational study of breast cancer patients, Berger et al.found that greater reported cancer-related fatigue was significantly asso-ciated with a higher number of nighttime awakenings, lower amplitude
Actigraphy Review Paper—Ancoli-Israel et alSLEEP, Vol. 26, No. 3, 2003 351

and lower peak activity as measured by wrist actigraphy (evidence level4C-b).148 In an observational study of cancer patients undergoing radia-tion therapy for bony metastases, Miaskowski et al. did not find a sig-nificant association between wrist actigraphy estimation of nighttimesleep and self-ratings of quality of sleep and feeling rested (evidencelevel 4C-b).149 Using wrist actigraphy to measure circadian rhythms,Mormont et al. found that cancer patients with marked activity rhythmshad better quality of life, reported less fatigue and had longer survivalcompared to those with rhythm alteration (evidence level 4C-b).150 Inmultivariate analysis, rest-activity rhythm remained a significant predic-tor of one-year survival.
In a series of articles, Berger et al. reported findings from wrist actig-raphy performed in women with breast cancer undergoing several cyclesof chemotherapy (both evidence levels 4C-b).148,151 They found thatfatigue ratings were higher during chemotherapy, and negatively corre-lated with activity as estimated by wrist actigraphy. Subjects with lowercircadian measures (specifically lower peak activity) had greater fatigue.
7.4 Actigraphy in Studies of Psychiatric Patients
Actigraphy has been used to investigate movement and sleep distur-bance in psychiatric patients (circadian activity disturbance is discussedabove in section 6.0. Circadian Rhythms). Dursun et al. conducted adescriptive study of wrist actigraphy estimation of sleep in outpatientswith schizophrenia prescribed risperidone compared to those on “typi-cal” antipsychotics, and to normal controls (evidence level 5D-a).152
They found a greater degree of nighttime wrist movement (i.e., highermovement index) in patients on a typical antipsychotic compared tothose on risperidone. Friedman et al. compared wrist actigraphy datawith measures of behavioral problems in a sample of patients withAlzheimer’s disease (AD) who were participating in a larger longitudi-nal study (evidence level 4C-b).126 They found that greater behavioraldisturbance was correlated with lower actigraphically estimated sleepefficiency (r=-.35, p<.05) and greater wake after sleep onset (r=.43,p<.01).
Lemke et al. used wrist actigraphy to estimate mean activity levels inpsychiatric unit inpatients with major depressive disorder (evidencelevel 4C-b).153 They found that subjects whose Pittsburgh Sleep QualityIndex indicated poor sleep had higher mean nighttime motor activitylevels that those who reported good sleep. In addition, subjects withfewer depressive symptoms had lower mean nighttime motor activitylevels than those with greater depressive symptomatology.
7.5 Actigraphy in Studies of Adults with Other Specific Medical Conditions
Actigraphy has been used in a variety of clinical studies involvingadults with other specific medical conditions. Baker et al. comparedwrist actigraphy findings between menopausal women and controls, andfound that menopausal women had more arousals and greater sleep dis-ruption. In a study of sleep disturbance in cirrhosis, Cordoba et al. foundthat compared to normal controls, cirrhosis patients had decreased motoractivity, more fragmentation of sleep and dampened rhythms, as mea-sured by actigraphy (evidence level 4C-b).154
Redeker et al. reported a series of studies using actigraphy in adultsundergoing coronary artery bypass graft surgery (CABG), and in adultshospitalized for cardiac conditions (all with evidence level 4C-b). In onestudy, 25 women (mean age 63.7 years) undergoing CABG had wristactigraphy applied after admission to the open-heart recoveryroom/intensive care unit, and wore the actigraphs continuously through-out their hospital stays. Findings from the first postoperative week afterCABG, indicated that, after controlling for preoperative functional sta-tus, there was a relationship between both recovery from surgery andlength of stay with the rhythmic and linear patterns of activity. Positivelinear trends in circadian activity periods were related to better func-tioning and shorter length of stay.155 When wrist actigraphy was repeat-ed up to four times over the 6 months following CABG, sleep consoli-dated and daytime sleep decreased and subjects’ perceived sleep
improvements were consistent with results of actigraphy.156 In anothersample of 22 men and women undergoing CABG, Redeker et al. foundthat activity levels and strength of circadian rhythms increased over days2 to 5 post-operatively, with a longer time for recovery of activity inolder adults.155 Finally, in another sample of 33 men and women admit-ted to the hospital for acute myocardial infarction or unstable angina,Redeker et al. found that previous severity of heart disease was thestrongest predictor of lower sleep efficiency and longer duration ofawakenings during hospitalization.157
7.6 Actigraphy in Studies of Older Adults
Actigraphy is particularly useful in studies involving older adults,both in the community and in the nursing home. In addition to the com-munity-based studies described above, which included healthy olderpeople in their sample, studies specifically targeting the elderly haveused actigraphy as outcome measures. Pollak et al. used wrist actigraphyin a descriptive study of 44 pairs of older people (aged 65 years or older)with disruptive nocturnal behaviors such as complaining and calling forhelp, and their principal caregiver (evidence level 4C-b).158 Twenty-twoof the elders met criteria for dementia. Both the older person and theircaregiver wore wrist actigraphs. Activity level was less similar duringthe daytime between the older person and their caregiver, as comparedto nighttime. In addition, actigraphy suggested that at night it was theelders that initiated the elder-caregiver interaction, thus disturbing thesleep of the caregiver.
Sleep and circadian rhythm variables deduced from actigraph record-ings have been used as outcome measures in multiple studies of nursinghome residents, a population that had been understudied and in whichPSG is particularly difficult. Ancoli-Israel et al. found significant sleepdisruption (with frequent nighttime awakening and frequent daytimesleeping, based on actigraphy) in a sample of 25 nursing home residents(evidence level 4C-b).159 In another study, Ancoli-Israel et al. comparednursing home residents with severe dementia to those with moderate,mild or no dementia, and found that the severely demented group hadlower activity mesor, lower amplitude and were more phase delayed thanthose with moderate, mild or no dementia (evidence level 4C-b).112
Hourly profiles of sleep and wakefulness in this group suggested that theseverely demented residents had more sleepiness during the day andnight and residents with moderate or mild dementia had more wakeful-ness during the night (evidence level 4C-b).160 Actigraphy with lightexposure was also used to study the relationship between sleep and lightexposure with results suggesting that higher light levels predicted fewernighttime awakenings and later activity acrophase (evidence level 4C-b).161 Additionally, when these same patients were treated with 10 daysof bright light therapy, although there was no improvement in sleep atnight, morning bright light delayed the peak of the activity rhythm (i.e.,acrophase), increased the mean activity level (i.e., increased the mesor)and improved activity rhythmicity (evidence level 4C-b).110
Alessi et al. used wrist actigraphy estimation of sleep as an outcomevariable in a controlled clinical trial of physical activity in nursing homeresidents (evidence level 4C-b).162 They found no significant improve-ment in sleep associated with improved physical function. Likewise, inan observational study of incontinent nursing home residents, Alessi etal. found no significant differences in nighttime sleep variables betweensubjects on psychotropic medications and subjects not on these medica-tions (evidence level 5D-b).163 However, in a controlled trial of a com-bined physical activity and environmental intervention in nursing homeresidents, Alessi et al. found a higher percent sleep at night estimated bywrist actigraphy in the intervention group compared to controls (evi-dence level 4C-b).164
Cruise et al. performed an observational study in nursing home resi-dents to study the nighttime environment and incontinence care practicesin nursing home residents (evidence level 4C-b).165 They found that 42%of nighttime waking episodes identified by wrist actigraphy were asso-ciated with noise, light or incontinence care. Ouslander et al. found that
Actigraphy Review Paper—Ancoli-Israel et alSLEEP, Vol. 26, No. 3, 2003 352

nighttime urinary incontinence was not related to sleep disruption (evi-dence level 5D-b).166
7.7 Actigraphy in Studies of Children
Actigraphy has been increasingly used in children, particularly instudies involving children with behavioral, psychiatric or neurologicalillness. Corkum et al. compared wrist actigraphy estimates of sleep inchildren with attention deficit/hyperactivity disorder (ADHD) to normalcontrols and found no statistically significant differences in total sleepduration, sleep onset and number of nighttime awakenings by wristactigraphy (evidence level 5D-b).167 Glod et al. used waist placement ofactigraphs in children who were victims of abuse, comparing their sleepto that of children with major depression or dysthymia, and with that ofnormal controls (evidence level 4C-b).168 In this study, abused childrenhad higher levels of nocturnal activity than both normal controls anddepressed children, and the abused children had more difficulty fallingand staying asleep. Hatonen et al. tested for differences in motor activi-ty rhythms with melatonin treatment versus placebo in 5 children aged12-19 with a neurodegenerative disease, neuronal ceroid lipofuscinosis(NCL) (evidence level 5D-b).117 In these children, there were no differ-ences between melatonin and placebo in actigraphic motor activitybased on period analysis by maximum entropy spectral, autocorrelationor harmonic analyses. In a controlled trial of melatonin therapy in chil-dren with Rett syndrome (an X-linked genetic disorder with motor andcognitive impairment, and often severe sleep dysfunction), McArthur etal. found high variability in subject responsiveness to melatonin, but asa group, sleep onset latency was significantly reduced with melatoninduring the first 3 weeks of the trial (evidence level 4C-b).169
Mennella et al. tested the immediate, short-term effects of ethanol inbreast milk on actigraphy estimation of sleep in infants from 15 mother-infant pairs (evidence level 4C-b).170 They found lower total sleep time,lower active sleep and shorter sleep bouts when infants received breastmilk with ethanol compared to breast milk without ethanol.
Sadeh and colleagues, in two separate studies, used actigraphy tomeasure sleep in relation to cognitive functioning in preterm infants andschool-age children.171,172 In the first study, early mature patterns ofsleep were related to later cognitive maturity (evidence level 4C-b).171 Inthe second study, children with fragmented sleep had lower performanceon measures of neurobehavioral functioning, particularly among themore complex tasks and behavior problems were more prevalent amongpoor sleepers (evidence level 4C-b).172
7.8 Summary
Actigraphy is increasingly being used in clinical research involvingindividuals of various ages, who are of normal health or with a varietyof health conditions, and in a number of different settings. In the major-ity of these studies, actigraphy was used to measure sleep and activityrhythms that might not otherwise be available using traditional (e.g.,PSG) techniques. In a growing number of sleep intervention trials, actig-raphy performed for multiple days and nights of testing was reported toshow evidence of beneficial treatment effects. Actigraphy has also beenused in studies involving otherwise healthy adults to demonstrate sedat-ing effects of various medications and to show differences in sleep dur-ing periods of sleep deprivation, for example, among military aircraftpersonnel on long flights. In addition, several large studies have usedactigraphy in community-based samples to demonstrate differencesbetween individuals based on age, gender, ethnicity, depressed mood,and other characteristics.
Another growing area of research is cancer-related fatigue, wherestudies involving multiple days and nights of actigraphy have demon-strated that cancer patients with more robust circadian rhythms of activ-ity report less fatigue, better quality of life and have longer survival.Likewise, in a series of studies involving adults undergoing coronaryartery bypass surgery, the strength of circadian activity rhythms as mea-sured by actigraphy in the post-operative period was related to recovery
from surgery and length of stay. Actigraphy has been used extensively in studies involving older peo-
ple, particularly in the nursing home setting. These studies have demon-strated significant sleep disruption among nursing home residents, andsleep and circadian rhythm disturbances have been shown to be moresevere among residents with more severe dementia. In addition, actigra-phy has been used to measure treatment effects in sleep interventionresearch in the nursing home setting, where other measures, such asPSG, would be extremely problematic to perform.
Finally, there is a growing literature using actigraphy in children. Forexample, actigraphy has been used to demonstrate differences in sleepbetween abused children and those with depression or normal controls.Actigraphy has also been used to test treatment effects of melatonin ther-apy in children with severe neurological disorders.
Taken as a whole, these clinical studies demonstrate the increasingexperience in the use of actigraphy in a variety of populations, condi-tions and settings. Unfortunately, the majority of these studies do notreport adequate detail on the technical aspects of the specific actigraph-ic devices used. However, it seems clear from these trials that the use ofactigraphy enables studies involving multiple days and nights of testing,and allows populations that might otherwise not be studied, such aspatients with dementia or young children, to participate in research stud-ies and clinical trials of sleep/wake activity and circadian rhythms
8.0 DISCUSSION
The last published practice parameters for actigraphy only consideredthe use of actigraphy for the clinical assessment of sleep disorders.1
Their conclusion in 1995 was that actigraphy should not be used for theclinical diagnosis of any sleep disorder, but that it might be a usefuladjunct to a good history and examination, particularly if multiple daysof information were needed, if objective data on the pattern of sleep wasneeded or in order to clarify the effects of compliance with treatment.2
Since that time advances have been made in actigraphs and in thealgorithms that process their data both within the apparatus and on com-puters following downloading of the data. Additionally, over 210 articlesand case studies have been published which have further examined thevalidity of actigraphy. As summarized in a recent review article bySadeh and Acebo,173 the number of yearly publications on sleep andactigraphy has risen steadily in the last ten years. In the research setting,actigraphs have been used for studying sleep disorders and circadianrhythms. Actigraphic variables have also been used as outcome mea-sures in clinical trials, often as a replacement for the more traditional, butmore expensive and cumbersome PSG.
One consistent finding of the current studies was that, when comparedto PSG, actigraphy was found to be moderately valid and reliable for dif-ferentiating sleep from wake in normal, healthy adult populations butless reliable for identifying sleep as sleep became more disturbed. Takentogether, these studies provide evidence that important applications ofthe actigraph may be in the assessment and in the measurement of thesleep variability found in patients with insomnia, in assisting in the diag-nosis of circadian rhythm disorders, in characterizing and monitoringcircadian rhythm disturbances that often accompany psychiatric disor-ders, in studying sleep/wake patterns in populations where PSG wouldbe difficult if not impossible, and in the assessment of treatment effectsand follow-up studies.
It is important to remember that actigraphy is not polysomnography.Although actigraphy may not be 100% accurate when compared to PSG,one still can get reliable information in situations where PSG is not prac-tical. Actigraphy makes home recordings more accessible, permitting theevaluation of patients in their natural sleeping environment and mini-mizing laboratory effects that may alter a patient’s typical sleep patterns.Actigraphy may provide an opportunity for subjects to adhere moreclosely to their scheduled bedtime and wakeup time than a PSG record-ing, thus providing a more accurate estimate of typical sleep durationthan does PSG.
Actigraphy Review Paper—Ancoli-Israel et alSLEEP, Vol. 26, No. 3, 2003 353

LIMITATIONS
In general, when actigraphy was compared to PSG, it was found to beboth somewhat valid and apparently reliable in normal, healthy adultpopulations. Overall, actigraphy is best at estimating total sleep time.However, as sleep became more fragmented, the actigraph became lessaccurate in the detection of sleep and wake. Newer studies agree witholder studies (e.g., Webster et al.,11) in suggesting that actigraphy mayoverestimate sleep and thus underestimate wake, particularly during theday when an individual is more likely to sit quietly while awake. In aneffort to reduce this error, early investigators developed secondary algo-rithms that rescore sleep epochs as wake if adjacent to many wakeepochs.11
While some data suggest that actigraphy consistently yields estimatesof total sleep time and the number of awakenings that are higher thanestimates on sleep logs, these results are more difficult to interpret, par-ticularly since sleep logs themselves do not correlate highly with datafrom PSG. It is not unusual for clinicians to report that their patients areseen filling out a week’s worth of sleep logs while in the waiting room,waiting to be evaluated. This brings up two questions. First, what is themeaning of a reliability study when the comparison is made with some-thing other than a gold standard, such as when actigraphy is compared tosleep logs? For example, although the actigraphic estimates of totalsleep time may have been higher than that reported in sleep logs, how dowe know that the actigraph estimations were not actually more accuratethan the sleep log estimation?
The second question is which is more important, the subjective reportof the sleep log or the objective estimation of actigraphy? Many clini-cal trials are now using subjective reports as their final outcome mea-sures, particularly in studies of insomnia, as they believe that if thepatients feel they are sleeping better, it may not matter what the objec-tive data show. If that is the case, then neither actigraphy nor PSG arenecessary. If, however, a more objective estimate is desired, then actig-raphy is a less expensive approach than PSG and has the added benefitof being able to record for multiple days and nights. When PSG is notfeasible, the best approach may be to use a combination of actigraphywith sleep logs. When there is agreement between the two methods, con-fidence is increased in the results of both. When there is disagreement,it may reveal problems with one or the other.
Other problems with actigraphy relate to the determination of sleeponset latency and variables whose calculations depend on it, for exam-ple, sleep efficiency and wake after sleep onset. First, it is impossible todetermine sleep onset latency accurately without either an accuratemarker of bedtime, such as a very accurate sleep log or an event markerpushed at lights out. Activity monitors coupled with light sensors may beuseful for objectively determining the time of lights out, although a bed-partner may continue to use lights after the person wearing the actigraphhas gone to sleep. Second, studies to date have often reported pooragreement between sleep onset latency estimated by actigraphy and thatdetermined by EEG. The problem may lie in the method of scoring, how-ever, and not in the intrinsic properties of actigraphy. Cole et al.28 foundthat the actigraph was more accurate (i.e., had a higher correlation) foridentifying sleep onset latency than any other sleep variable, when anappropriate scoring algorithm was used (see section 4.3. Comparisons toPSG). If this finding could be replicated, it might be possible to sub-stantially improve actigraphic estimates of sleep latency, sleep efficien-cy and wake time after sleep onset.
FUTURE RESEARCH
Standardization of acceptable norms needs to be established beforeactigraphy can be more generally used with full confidence in the realmof sleep/wake studies. More development and research of both thedevices that record the data and the algorithms that process the data isneeded. In addition, disclosure of types of algorithms used should berequired in all manuscripts.
The question of the best placement of the actigraph must also be
answered. The data suggest that the wrist in general is more accurate forsleep estimation than other placements. Although traditionally actigra-phy has been recorded from the non-dominant wrist, newer data suggestthat movement from the dominant wrist may reflect sleep and wakemore accurately than movements recorded from the non-dominant wrist.
The problem of overestimating sleep must also be addressed. A poten-tial approach to this problem might be the development of separate algo-rithms for scoring sleep from daytime vs. nighttime activity records. Itwould be desirable for future research to systematically evaluate these orother ways to overcome the actigraph’s tendency to overestimate sleep.It may be that a different scoring algorithm is needed for periods whenthe individual is expected to be awake (out-of-bed periods) than the onecurrently used for periods during which the individual is expected to beasleep (in-bed periods). Studies of actigraphy compared to EEG outsideof the traditional sleep period, in patients that are known to fall asleepduring the day, need to be done to more reliably determine the effec-tiveness of actigraphy during waking hours.
SUMMARY
In summary, although actigraphy is not as accurate as PSG for deter-mining some sleep measurements, studies are in general agreement thatactigraphy, with its ability to record continuously for long time periods,is more reliable than sleep logs which rely on the patients’ recall of howmany times they woke up or how long they slept during the night and ismore reliable than observations which only capture short time periods.Actigraphy can provide information obtainable in no other practical way.It can also have a role in the medical care of patients with sleep disor-ders. However, it should not be held to the same expectations aspolysomnography. Actigraphy is one-dimensional, whereas polysomno-graphy comprises at least 3 distinct types of data (EEG, EOG, EMG),which jointly determine whether a person is asleep or awake. It is there-fore doubtful whether actigraphic data will ever be informationallyequivalent to the PSG, although progress on hardware and data process-ing software is continuously being made.
Although the 1995 practice parameters paper determined that actigra-phy was not appropriate for the diagnosis of sleep disorders, more recentstudies suggest that for some disorders, actigraphy may be more practi-cal than PSG. While actigraphy is still not appropriate for the diagnosisof sleep disordered breathing or of periodic limb movements in sleep, itis highly appropriate for examining the sleep variability (i.e., night-to-night variability) in patients with insomnia. Actigraphy is also appropri-ate for the assessment of and stability of treatment effects of anythingfrom hypnotic drugs to light treatment to CPAP, particularly if assess-ments are done before and after the start of treatment. A recent indepen-dent review of the actigraphy literature by Sadeh and Acebo reachedmany of these same conclusions.173
Some of the research studies failed to find relationships between sleepmeasures and health-related symptoms. The interpretation of these datais also not clear-cut. Is it that the actigraph is not reliable enough to theaccess the relationship between sleep changes and quality of life mea-sures, or, is it that, in fact, there is no relationship between sleep in thatpopulation and quality of life measures? Other studies of sleep disor-dered breathing, where actigraphy was not used and was not an outcomemeasure also failed to find any relationship with quality of life. Is it thenthe actigraph that is not reliable or that the associations just do not exist?
The one area where actigraphy can be used for clinical diagnosis is inthe evaluation of circadian rhythm disorders. Actigraphy has been shownto be very good for identifying rhythms. Results of actigraphic record-ings correlate well with measurements of melatonin and of core bodytemperature rhythms. Activity records also show sleep disturbance whensleep is attempted at an unfavorable phase of the circadian cycle. Actig-raphy therefore would be particularly good for aiding in the diagnosis ofdelayed or advanced sleep phase syndrome, non-24-hour-sleep syn-drome and in the evaluation of sleep disturbances in shift workers. Itmust be remembered, however, that overt rest-activity rhythms are sus-ceptible to various masking effects, so they may not always show the
Actigraphy Review Paper—Ancoli-Israel et alSLEEP, Vol. 26, No. 3, 2003 354

underlying rhythm of the endogenous circadian pacemaker.In conclusion, the latest set of research articles suggest that in the clin-
ical setting, actigraphy is reliable for evaluating sleep patterns in patientswith insomnia, for studying the effect of treatments designed to improvesleep, in the diagnosis of circadian rhythm disorders (including shiftwork), and in evaluating sleep in individuals who are less likely to tol-erate PSG, such as infants and demented elderly. While actigraphy hasbeen used in research studies for many years, up to now, methodologicalissues had not been systematically addressed in clinical research andpractice. Those issues have now been addressed and actigraphy maynow be reaching the maturity needed for application in the clinical arena.
9.0 REFERENCES
1. Sadeh A, Hauri PJ, Kripke DF, Lavie P. The Role of Actigraphy in the Evaluation ofSleep Disorders. Sleep 1995; 18(4):288-302.
2. Standards of Practice Committee A. An American Sleep Disorders Association Report:Practice parameters for the use of actigraphy in the clinical assessment of sleep disor-ders. Sleep 1995; 18:285-287.
3. Broughton R, Fleming J, Fleetham J. Home assessment of sleep disorders by portablemonitoring. J Clin NeuroPhysiol 1996; 13(4):272-284.
4. Teicher MH. Actigraphy and motion analysis: New tools for psychiatry. Harvard Reviewof Psychiatry 1995; 3(1):18-35.
5. Ancoli-Israel S. Actigraphy. In: Kryger MH, Roth T, Dement WC, editors. Principles andPractice of Sleep Medicine. Philadelphia: W.B. Saunders, 2000: 1295-1301.
6. Kupfer DJ, Weiss BL, Foster FG, Detre TP, Delgado J, McPartland RJ. Psychomotoractivity in affective states. Arch Gen Psychiatry 1974; 30:765-768.
7. McPartland RJ, Kupfer DJ, Foster FG. The movement-activated recording monitor: Athird generation motor-activity monitoring system. Behavior Research Methods &Instrumentation 1976; 8:357-360.
8. Colburn TR, Smith BM, Cuarini JJ, Simmons NM. An ambulatory activity monitor withsolid state memory. ISA Transactions 1976; 15:149-154.
9. Kripke DF, Mullaney DJ, Messin S, Wyborney VG. Wrist actigraphic measures of sleepand rhythms. Electroencephalogr Clin Neurophysiol 1978; 44:674-76.
10. Mullaney DJ, Kripke DF, Messin S. Wrist-actigraphic estimation of sleep time. Sleep1980; 3:83-92.
11. Webster JB, Kripke DF, Messin S, Mullaney DJ, Wyborney G. An activity-based sleepmonitor system for ambulatory use. Sleep 1982; 5:389-99.
12. Jean-Louis G, Kripke DF, Cole RJ, Assmus JD, Langer RD. Sleep detection with anacceleromether actigraph: comparisons with polysomnography. Physiol Behav 2001;72:21-28.
13. Redmond DP, Hegge FW. The design of human activity monitors. In: Scheving LE, Hal-berg F, Ehret CF, editors. Chronobiology and Chronobiological Engineering. Dordrecht:Martinus Nijhoff Publishers, 1987: 202-15.
14. Van Someren EJW, Lazeron RH, Vonk BF. Wrist acceleration and consequences for acti-graphic rest-activity registration in young and elderly subjects. Sleep-Wake Research inthe Netherlands 1995;6123-6125.
15. Gorny SW, Spiro JR. Comparing different methodologies used in wrist actigraphy. SleepReview 2001; Summer:40-42.
16. Jean-Louis G, von Gizycki H, Zizi F, Spielman A, Hauri P, Taub H. The actigraph dataanalysis software: I. A novel approach to scoring and interpreting sleep-wake activity.Percept Mot Skills 1997; 85(1):207-216.
17. Sadeh A, Sharkey KM, Carskadon MA. Activity-based sleep-wake identification: Anempirical test of methodological issues. Sleep 1994; 17:201-207.
18. Pollak CP, Stokes PE, Wagner DR. Direct comparision of two widely used activityrecorders. Sleep 1998; 21(2):207-212.
19. Kushida CA, Chang A, Gadkary C, Guilleminault C, Carrillo O, Dement WC. Compar-ison of actigraphic, polysomnographic, and subjective asessment of sleep parameters insleep-disordered patients. Sleep Med 2001;398-396.
20. Tryon WW. Activity and sleep. Act Measure Psychol Med 1991;149-195.21. Pollak C, Tryon WW, Nagaraja H, Dzwonczyk R. How accurately does wrist actigraphy
identify states of sleep and wakefulness? Sleep 2001; 24(8):957-965.22. Jean-Louis G, von Gizycki H, Zizi F et al. Determination of sleep and wakefulness with
the actigraph data analysis software (ADAS). Sleep 1996; 19(9):739-743.23. Blood ML, Sack RL, Percy DC, Pen JC. A comparison of sleep detection by wrist actig-
raphy, behavioral response, and polysomnography. Sleep 1997; 20(6):388-395.24. Jean-Louis G. Sleep estimation from wrist movement quantified by different actigraph-
ic modalities. J Neurosci Methods 2001; 105(2):185-191.25. Reid K, Dawson D. Correlation between wrist activity monitor and electrophysiological
measures of sleep in a simulated shiftwork environment for younger and older subjects.Sleep 1999; 52(2):157-159.
26. Ancoli-Israel S, Clopton P, Klauber MR, Fell R, Mason WJ. Use of wrist activity formonitoring sleep/wake in demented nursing home patients. Sleep 1997; 20(1):24-27.
27. Shinkoda H, Matsumoto K, Hamasaki J, Seo YJ, Park YM, Park KP. Evaluation ofhuman activites and sleep-wake identification using wrist actigraphy. Psychiatry 1998;52(2):157-159.
28. Cole RJ, Kripke DF, Gruen W, Mullaney DJ, Gillin JC. Automatic sleep/wake identifi-cation from wrist activity. Sleep 1992; 15(5):461-469.
29. Lockley SW, Skene DJ, Arendt J. Comparison between subjective and actigraphic mea-surement of sleep and sleep rhythms. J Sleep Res 1999; 8(3):175-184.
30. Krahn L, Lin SC, Wisbey J, Rummans T, O’Connor MK. Assessing sleep in psychiatricinpatients: nurse and patient reports versus wrist actigraphy. Annals of Clinical Psychi-
atry 1999; 9(4):203-210.31. Monk T, Buysse D, Rose LR. Wrist actigraphic measures of sleep in space. Sleep 1999;
22(7):948-954.32. Dijk DJ, Wyatt JK, Wyatt JK et al. Sleep, performance, circadian rhythms, and light-dark
cycles during two space shuttle flights. American journal of physiology Regulatory, inte-grative and comparative physiology 2001; 281(5):R1647-R1664.
33. Sadeh A. Evaluating night wakings in sleep-disturbed infants: a methodological study ofparental reports and actigraphy. Sleep 1996; 19(10):757-762.
34. Tikotzky L, Sadeh A. Sleep patterns and sleep disruptions in kindergarten children. Jour-nal of Clinical and Child Psychology 2001; 30(4):581-591.
35. Sadeh A. Assessment of intervention for infant night waking: Parental reports and activ-ity-based home monitoring. J Consult Clin Psychol 1994; 62(1):63-68.
36. Acebo C, Sadeh A, Seifer R et al. Estimating sleep patterns with activity monitoring inchildren and adolescents: How many nights are necessary for reliable measures? Sleep1999; 22(1):95103.
37. Roehrs T, Turner L, Roth T. Effects of sleep loss on waking actigraphy. Sleep 2000;23(6):793-797.
38. Kazenwadel J, Pollmacher T, Trenkwalder C et al. New actigraphic assessment methodfor periodic leg movements (PLM). Sleep 1995; 18(8):689-697.
39. Sforza E, Zamagni M, Petiav C, Krieger J. Actigraphy and leg movements during sleep:a validation study. J Clin Neurophysiol 1999; 16(2):154-160.
40. Middelkoop HA, Van Dam E, Smilde-van den Doel DA, Van Dijk G. 45-hour continu-ous quintuple-site actimetry: relations between trunk and limb movements and effects ofcircadian sleep-wake rythmicity. Psychophysiol 2002; 34(2):199-203.
41. Middelkoop HA, Van Dam E, Smilde-van den Doel DA. 45-hour multiple-site actime-try in 20 healthy subjects: relations between body and limb movements and the effectsof circadian sleep-wakefulness. Sleep-Wake Research in the Netherlands 1995;681-684.
42. Violani C, Testa P, Casagrande M. Actigraphic motor asymmetries during sleep. Sleep1998; 21(5):472-476.
43. Youngstedt SD, Kripke DF, Elliott JA, Klauber MR. Circadian abnormalities in olderadults. J Pineal Res 2001; 31:264-272.
44. Cole RJ, Smith JS, Alcala YC, Elliott JA, Kripke DF. Bright-light mask treatment ofdelayed sleep phase syndrome. J Biol Rhythms 2002; 17(1):89-101.
45. Minors D, Akerstedt T, Atkinson G et al. The difference between activity when in bedand out of bed. I. Healthy subjects and selected patients. Chronobiol Intl 1996; 13:27-34.
46. Jean-Louis G, Kripke D, Mason WJ, Ancoli-Israel S. Relationships among illumination,activity and sleep patterns. In: Holick MF, Jung EG, editors. Biological Effects of Light.Kluver Academic Publishers, 1999: 37-39.
47. Rechtschaffen A, Kales A, (eds). A Manual of Standardized Terminology, Techniquesand Scoring System for Sleep Stages of Human Subjects. Los Angeles: Brain Informa-tion Service, Brain Research Institute, UCLA, 1973.
48. Karacan I, Williams RL, Littell RC, Sails PJ. Insomniacs: Unpredictable and idiosyn-cratic sleepers. In: Koella WP, Levin P, editors. Sleep: Physiology, Biochemistry, Phar-macology, Clinical Implications. Basel: Karger, 1972: 120-132.
49. Hauri PJ, Wisbey J. Wrist actigraphy in insomnia. Sleep 1992; 15(4):293-301.50. Chambers MJ. Actigraphy and insomnia: A closer look Part I. Sleep 1994; 17(5):405-
408.51. Guilleminault C, Clerk A, Black J, Labanowski M, Pelayo R, Claman D. Nondrug treat-
ment trials in psychophysiologic insomnia. Ann Intern Med 1995; 155:838-844.52. Wilson KG, Watson ST, Currie SR. Daily diary and ambulatory activity monitoring of
sleep in patients with insomnia associated with chronic musculoskeletal pain. Pain 1998;75(1):75-84.
53. Jean-Louis G, Kripke D, Ancoli-Israel S. Sleep and quality of well-being. Sleep 2000;23(8):1115-1121.
54. Dagan Y, Zinger Y, Lavie P. Acitgraphic sleep montoring in post-traumatic stress disor-der (PTSD) patients. J Psychosom Res 1997; 42(6):577-581.
55. Wicklow A, Espie CA. Intrusive thoughts and their relationship to actigraphic measure-ment of sleep: Towards a cognitive model of insomnia. Behav Res Ther 2000; 38:679-693.
56. Kerkhof G, Van Vianen B. Circadian phase estimation of chronic insomniacs relates totheir sleep characteristics. Archives of Physiology and Biochemistry 1999; 107(5):383-392.
57. Dagan Y, Yovel I, Hallis D, Eisenstein M, Raichik I. Evaluating the role of melatonin inthe long-term treatment of delayed sleep phase syndrome (DSPS). Chronobiol Int 1998;15(2):181-190.
58. Okawa M, Urata J, Uchiyama M et al. Melatonin treatment for circadian rhythm sleepdisorders. Psychiatry and Clinical Neurosciences 1998; 52(2):259-260.
59. Quinto C, Gellido C, Chokroverty S, Masdeu J. Posttraumatic delayed sleep phase syn-drome. Neurology 2000; 54(1):250-252.
60. Nagtegaal J, Kerkhof GA, Smits MG, Swart AC, Van Der Meer YG. Traumatic braininjury-associated delayed sleep phase syndrome. Functional Neurology 1997;12(6):345-348.
61. Nagtegaal J, Kerkhof GA, Smits MG, Swart AC, Van Der Meer YG. Delayed sleep phasesyndrome: a placebo-controlled cross-over study on the effects of melatonin adminis-tered five hours before the individual dim light melatonin onset. J Sleep Res 1998;7(2):135-143.
62. Franck LS, Johnson LM, Lee K et al. Sleep disturbances in children with human immun-odeficiency virus infection. Pediatrics 1999; 104(5).
63. Hering E, Epstein R, Elroy S, Iancu DR, Zelnik N. Sleep patterns in autistic children.Journal of Autism and Developmental Disorders 1999; 29(2):143-147.
64. Sadeh A, Dark I, Vohr BR. Newborns’ sleep-wake patterns: The role of maternal, deliv-ery and infant factors. Early Hum Dev 1996; 44:113-126.
65. Etzioni A, Luboshitzky R, Tiosano D, Ben-Harush M, Goldsher D, Lavie P. Melatoninreplacement corrects sleep disturbances in a child with pineal tumor. Neurology 1996;
Actigraphy Review Paper—Ancoli-Israel et alSLEEP, Vol. 26, No. 3, 2003 355
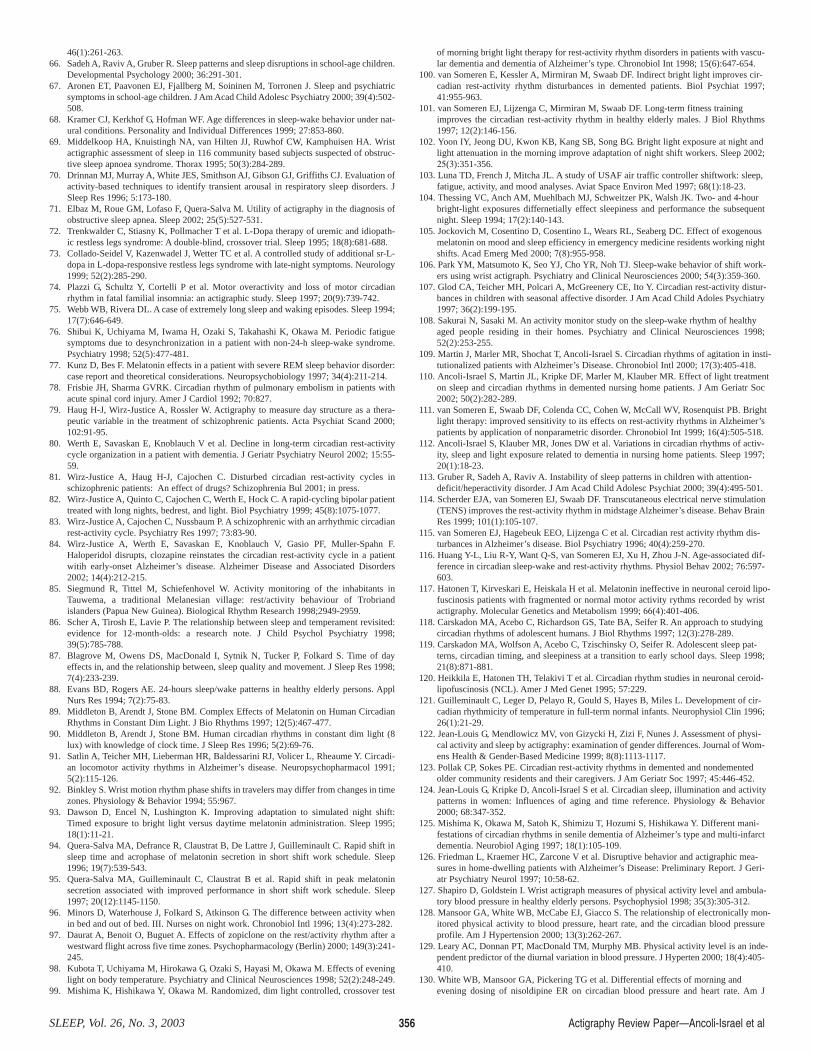
46(1):261-263.66. Sadeh A, Raviv A, Gruber R. Sleep patterns and sleep disruptions in school-age children.
Developmental Psychology 2000; 36:291-301.67. Aronen ET, Paavonen EJ, Fjallberg M, Soininen M, Torronen J. Sleep and psychiatric
symptoms in school-age children. J Am Acad Child Adolesc Psychiatry 2000; 39(4):502-508.
68. Kramer CJ, Kerkhof G, Hofman WF. Age differences in sleep-wake behavior under nat-ural conditions. Personality and Individual Differences 1999; 27:853-860.
69. Middelkoop HA, Knuistingh NA, van Hilten JJ, Ruwhof CW, Kamphuisen HA. Wristactigraphic assessment of sleep in 116 community based subjects suspected of obstruc-tive sleep apnoea syndrome. Thorax 1995; 50(3):284-289.
70. Drinnan MJ, Murray A, White JES, Smithson AJ, Gibson GJ, Griffiths CJ. Evaluation ofactivity-based techniques to identify transient arousal in respiratory sleep disorders. JSleep Res 1996; 5:173-180.
71. Elbaz M, Roue GM, Lofaso F, Quera-Salva M. Utility of actigraphy in the diagnosis ofobstructive sleep apnea. Sleep 2002; 25(5):527-531.
72. Trenkwalder C, Stiasny K, Pollmacher T et al. L-Dopa therapy of uremic and idiopath-ic restless legs syndrome: A double-blind, crossover trial. Sleep 1995; 18(8):681-688.
73. Collado-Seidel V, Kazenwadel J, Wetter TC et al. A controlled study of additional sr-L-dopa in L-dopa-responsive restless legs syndrome with late-night symptoms. Neurology1999; 52(2):285-290.
74. Plazzi G, Schultz Y, Cortelli P et al. Motor overactivity and loss of motor circadianrhythm in fatal familial insomnia: an actigraphic study. Sleep 1997; 20(9):739-742.
75. Webb WB, Rivera DL. A case of extremely long sleep and waking episodes. Sleep 1994;17(7):646-649.
76. Shibui K, Uchiyama M, Iwama H, Ozaki S, Takahashi K, Okawa M. Periodic fatiguesymptoms due to desynchronization in a patient with non-24-h sleep-wake syndrome.Psychiatry 1998; 52(5):477-481.
77. Kunz D, Bes F. Melatonin effects in a patient with severe REM sleep behavior disorder:case report and theoretical considerations. Neuropsychobiology 1997; 34(4):211-214.
78. Frisbie JH, Sharma GVRK. Circadian rhythm of pulmonary embolism in patients withacute spinal cord injury. Amer J Cardiol 1992; 70:827.
79. Haug H-J, Wirz-Justice A, Rossler W. Actigraphy to measure day structure as a thera-peutic variable in the treatment of schizophrenic patients. Acta Psychiat Scand 2000;102:91-95.
80. Werth E, Savaskan E, Knoblauch V et al. Decline in long-term circadian rest-activitycycle organization in a patient with dementia. J Geriatr Psychiatry Neurol 2002; 15:55-59.
81. Wirz-Justice A, Haug H-J, Cajochen C. Disturbed circadian rest-activity cycles inschizophrenic patients: An effect of drugs? Schizophrenia Bul 2001; in press.
82. Wirz-Justice A, Quinto C, Cajochen C, Werth E, Hock C. A rapid-cycling bipolar patienttreated with long nights, bedrest, and light. Biol Psychiatry 1999; 45(8):1075-1077.
83. Wirz-Justice A, Cajochen C, Nussbaum P. A schizophrenic with an arrhythmic circadianrest-activity cycle. Psychiatry Res 1997; 73:83-90.
84. Wirz-Justice A, Werth E, Savaskan E, Knoblauch V, Gasio PF, Muller-Spahn F.Haloperidol disrupts, clozapine reinstates the circadian rest-activity cycle in a patientwitih early-onset Alzheimer’s disease. Alzheimer Disease and Associated Disorders2002; 14(4):212-215.
85. Siegmund R, Tittel M, Schiefenhovel W. Activity monitoring of the inhabitants inTauwema, a traditional Melanesian village: rest/activity behaviour of Trobriandislanders (Papua New Guinea). Biological Rhythm Research 1998;2949-2959.
86. Scher A, Tirosh E, Lavie P. The relationship between sleep and temperament revisited:evidence for 12-month-olds: a research note. J Child Psychol Psychiatry 1998;39(5):785-788.
87. Blagrove M, Owens DS, MacDonald I, Sytnik N, Tucker P, Folkard S. Time of dayeffects in, and the relationship between, sleep quality and movement. J Sleep Res 1998;7(4):233-239.
88. Evans BD, Rogers AE. 24-hours sleep/wake patterns in healthy elderly persons. ApplNurs Res 1994; 7(2):75-83.
89. Middleton B, Arendt J, Stone BM. Complex Effects of Melatonin on Human CircadianRhythms in Constant Dim Light. J Bio Rhythms 1997; 12(5):467-477.
90. Middleton B, Arendt J, Stone BM. Human circadian rhythms in constant dim light (8lux) with knowledge of clock time. J Sleep Res 1996; 5(2):69-76.
91. Satlin A, Teicher MH, Lieberman HR, Baldessarini RJ, Volicer L, Rheaume Y. Circadi-an locomotor activity rhythms in Alzheimer’s disease. Neuropsychopharmacol 1991;5(2):115-126.
92. Binkley S. Wrist motion rhythm phase shifts in travelers may differ from changes in timezones. Physiology & Behavior 1994; 55:967.
93. Dawson D, Encel N, Lushington K. Improving adaptation to simulated night shift:Timed exposure to bright light versus daytime melatonin administration. Sleep 1995;18(1):11-21.
94. Quera-Salva MA, Defrance R, Claustrat B, De Lattre J, Guilleminault C. Rapid shift insleep time and acrophase of melatonin secretion in short shift work schedule. Sleep1996; 19(7):539-543.
95. Quera-Salva MA, Guilleminault C, Claustrat B et al. Rapid shift in peak melatoninsecretion associated with improved performance in short shift work schedule. Sleep1997; 20(12):1145-1150.
96. Minors D, Waterhouse J, Folkard S, Atkinson G. The difference between activity whenin bed and out of bed. III. Nurses on night work. Chronobiol Intl 1996; 13(4):273-282.
97. Daurat A, Benoit O, Buguet A. Effects of zopiclone on the rest/activity rhythm after awestward flight across five time zones. Psychopharmacology (Berlin) 2000; 149(3):241-245.
98. Kubota T, Uchiyama M, Hirokawa G, Ozaki S, Hayasi M, Okawa M. Effects of eveninglight on body temperature. Psychiatry and Clinical Neurosciences 1998; 52(2):248-249.
99. Mishima K, Hishikawa Y, Okawa M. Randomized, dim light controlled, crossover test
of morning bright light therapy for rest-activity rhythm disorders in patients with vascu-lar dementia and dementia of Alzheimer’s type. Chronobiol Int 1998; 15(6):647-654.
100. van Someren E, Kessler A, Mirmiran M, Swaab DF. Indirect bright light improves cir-cadian rest-activity rhythm disturbances in demented patients. Biol Psychiat 1997;41:955-963.
101. van Someren EJ, Lijzenga C, Mirmiran M, Swaab DF. Long-term fitness trainingimproves the circadian rest-activity rhythm in healthy elderly males. J Biol Rhythms1997; 12(2):146-156.
102. Yoon IY, Jeong DU, Kwon KB, Kang SB, Song BG. Bright light exposure at night andlight attenuation in the morning improve adaptation of night shift workers. Sleep 2002;25(3):351-356.
103. Luna TD, French J, Mitcha JL. A study of USAF air traffic controller shiftwork: sleep,fatigue, activity, and mood analyses. Aviat Space Environ Med 1997; 68(1):18-23.
104. Thessing VC, Anch AM, Muehlbach MJ, Schweitzer PK, Walsh JK. Two- and 4-hourbright-light exposures differnetially effect sleepiness and performance the subsequentnight. Sleep 1994; 17(2):140-143.
105. Jockovich M, Cosentino D, Cosentino L, Wears RL, Seaberg DC. Εffect of exogenousmelatonin on mood and sleep efficiency in emergency medicine residents working nightshifts. Acad Emerg Med 2000; 7(8):955-958.
106. Park YM, Matsumoto K, Seo YJ, Cho YR, Noh TJ. Sleep-wake behavior of shift work-ers using wrist actigraph. Psychiatry and Clinical Neurosciences 2000; 54(3):359-360.
107. Glod CA, Teicher MH, Polcari A, McGreenery CE, Ito Y. Circadian rest-activity distur-bances in children with seasonal affective disorder. J Am Acad Child Adoles Psychiatry1997; 36(2):199-195.
108. Sakurai N, Sasaki M. An activity monitor study on the sleep-wake rhythm of healthyaged people residing in their homes. Psychiatry and Clinical Neurosciences 1998;52(2):253-255.
109. Martin J, Marler MR, Shochat T, Ancoli-Israel S. Circadian rhythms of agitation in insti-tutionalized patients with Alzheimer’s Disease. Chronobiol Intl 2000; 17(3):405-418.
110. Ancoli-Israel S, Martin JL, Kripke DF, Marler M, Klauber MR. Effect of light treatmenton sleep and circadian rhythms in demented nursing home patients. J Am Geriatr Soc2002; 50(2):282-289.
111. van Someren E, Swaab DF, Colenda CC, Cohen W, McCall WV, Rosenquist PB. Brightlight therapy: improved sensitivity to its effects on rest-activity rhythms in Alzheimer’spatients by application of nonparametric disorder. Chronobiol Int 1999; 16(4):505-518.
112. Ancoli-Israel S, Klauber MR, Jones DW et al. Variations in circadian rhythms of activ-ity, sleep and light exposure related to dementia in nursing home patients. Sleep 1997;20(1):18-23.
113. Gruber R, Sadeh A, Raviv A. Instability of sleep patterns in children with attention-deficit/heperactivity disorder. J Am Acad Child Adolesc Psychiat 2000; 39(4):495-501.
114. Scherder EJA, van Someren EJ, Swaab DF. Transcutaneous electrical nerve stimulation(TENS) improves the rest-activity rhythm in midstage Alzheimer’s disease. Behav BrainRes 1999; 101(1):105-107.
115. van Someren EJ, Hagebeuk EEO, Lijzenga C et al. Circadian rest activity rhythm dis-turbances in Alzheimer’s disease. Biol Psychiatry 1996; 40(4):259-270.
116. Huang Y-L, Liu R-Y, Want Q-S, van Someren EJ, Xu H, Zhou J-N. Age-associated dif-ference in circadian sleep-wake and rest-activity rhythms. Physiol Behav 2002; 76:597-603.
117. Hatonen T, Kirveskari E, Heiskala H et al. Melatonin ineffective in neuronal ceroid lipo-fuscinosis patients with fragmented or normal motor activity rythms recorded by wristactigraphy. Molecular Genetics and Metabolism 1999; 66(4):401-406.
118. Carskadon MA, Acebo C, Richardson GS, Tate BA, Seifer R. An approach to studyingcircadian rhythms of adolescent humans. J Biol Rhythms 1997; 12(3):278-289.
119. Carskadon MA, Wolfson A, Acebo C, Tzischinsky O, Seifer R. Adolescent sleep pat-terns, circadian timing, and sleepiness at a transition to early school days. Sleep 1998;21(8):871-881.
120. Heikkila E, Hatonen TH, Telakivi T et al. Circadian rhythm studies in neuronal ceroid-lipofuscinosis (NCL). Amer J Med Genet 1995; 57:229.
121. Guilleminault C, Leger D, Pelayo R, Gould S, Hayes B, Miles L. Development of cir-cadian rhythmicity of temperature in full-term normal infants. Neurophysiol Clin 1996;26(1):21-29.
122. Jean-Louis G, Mendlowicz MV, von Gizycki H, Zizi F, Nunes J. Assessment of physi-cal activity and sleep by actigraphy: examination of gender differences. Journal of Wom-ens Health & Gender-Based Medicine 1999; 8(8):1113-1117.
123. Pollak CP, Sokes PE. Circadian rest-activity rhythms in demented and nondementedolder community residents and their caregivers. J Am Geriatr Soc 1997; 45:446-452.
124. Jean-Louis G, Kripke D, Ancoli-Israel S et al. Circadian sleep, illumination and activitypatterns in women: Influences of aging and time reference. Physiology & Behavior2000; 68:347-352.
125. Mishima K, Okawa M, Satoh K, Shimizu T, Hozumi S, Hishikawa Y. Different mani-festations of circadian rhythms in senile dementia of Alzheimer’s type and multi-infarctdementia. Neurobiol Aging 1997; 18(1):105-109.
126. Friedman L, Kraemer HC, Zarcone V et al. Disruptive behavior and actigraphic mea-sures in home-dwelling patients with Alzheimer’s Disease: Preliminary Report. J Geri-atr Psychiatry Neurol 1997; 10:58-62.
127. Shapiro D, Goldstein I. Wrist actigraph measures of physical activity level and ambula-tory blood pressure in healthy elderly persons. Psychophysiol 1998; 35(3):305-312.
128. Mansoor GA, White WB, McCabe EJ, Giacco S. The relationship of electronically mon-itored physical activity to blood pressure, heart rate, and the circadian blood pressureprofile. Am J Hypertension 2000; 13(3):262-267.
129. Leary AC, Donnan PT, MacDonald TM, Murphy MB. Physical activity level is an inde-pendent predictor of the diurnal variation in blood pressure. J Hyperten 2000; 18(4):405-410.
130. White WB, Mansoor GA, Pickering TG et al. Differential effects of morning andevening dosing of nisoldipine ER on circadian blood pressure and heart rate. Am J
Actigraphy Review Paper—Ancoli-Israel et alSLEEP, Vol. 26, No. 3, 2003 356
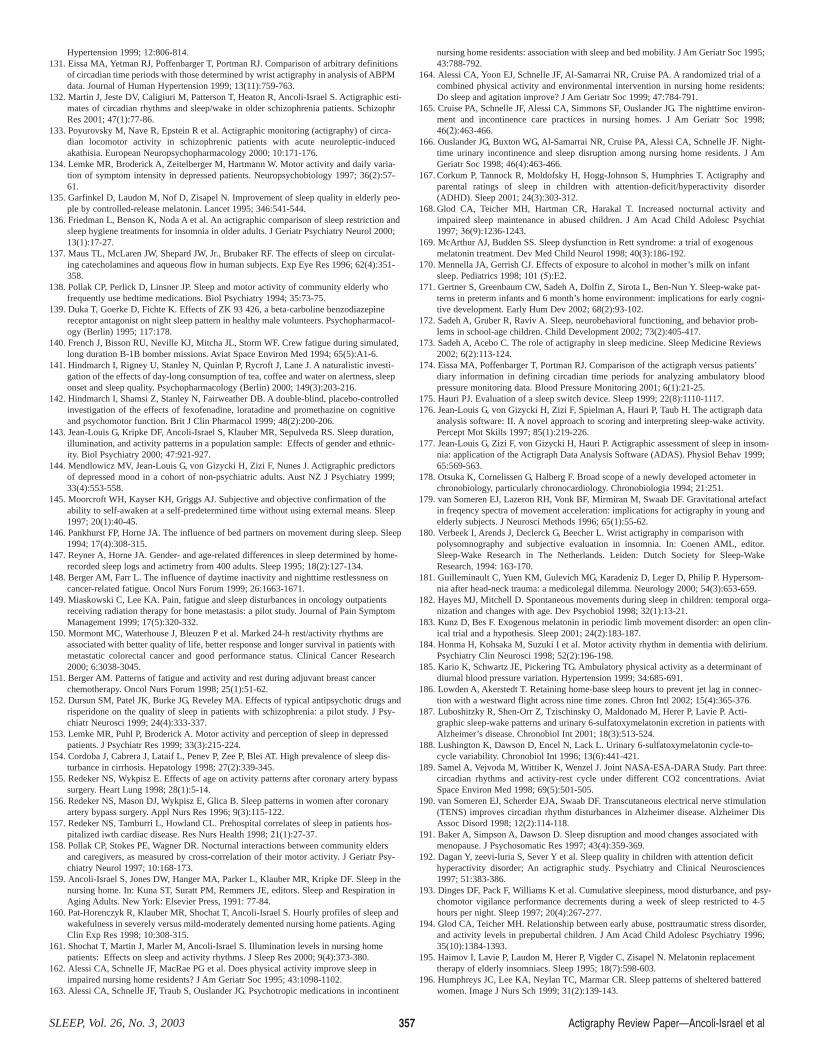
Hypertension 1999; 12:806-814.131. Eissa MA, Yetman RJ, Poffenbarger T, Portman RJ. Comparison of arbitrary definitions
of circadian time periods with those determined by wrist actigraphy in analysis of ABPMdata. Journal of Human Hypertension 1999; 13(11):759-763.
132. Martin J, Jeste DV, Caligiuri M, Patterson T, Heaton R, Ancoli-Israel S. Actigraphic esti-mates of circadian rhythms and sleep/wake in older schizophrenia patients. SchizophrRes 2001; 47(1):77-86.
133. Poyurovsky M, Nave R, Epstein R et al. Actigraphic monitoring (actigraphy) of circa-dian locomotor activity in schizophrenic patients with acute neuroleptic-inducedakathisia. European Neuropsychopharmacology 2000; 10:171-176.
134. Lemke MR, Broderick A, Zeitelberger M, Hartmann W. Motor activity and daily varia-tion of symptom intensity in depressed patients. Neuropsychobiology 1997; 36(2):57-61.
135. Garfinkel D, Laudon M, Nof D, Zisapel N. Improvement of sleep quality in elderly peo-ple by controlled-release melatonin. Lancet 1995; 346:541-544.
136. Friedman L, Benson K, Noda A et al. An actigraphic comparison of sleep restriction andsleep hygiene treatments for insomnia in older adults. J Geriatr Psychiatry Neurol 2000;13(1):17-27.
137. Maus TL, McLaren JW, Shepard JW, Jr., Brubaker RF. The effects of sleep on circulat-ing catecholamines and aqueous flow in human subjects. Exp Eye Res 1996; 62(4):351-358.
138. Pollak CP, Perlick D, Linsner JP. Sleep and motor activity of community elderly whofrequently use bedtime medications. Biol Psychiatry 1994; 35:73-75.
139. Duka T, Goerke D, Fichte K. Effects of ZK 93 426, a beta-carboline benzodiazepinereceptor antagonist on night sleep pattern in healthy male volunteers. Psychopharmacol-ogy (Berlin) 1995; 117:178.
140. French J, Bisson RU, Neville KJ, Mitcha JL, Storm WF. Crew fatigue during simulated,long duration B-1B bomber missions. Aviat Space Environ Med 1994; 65(5):A1-6.
141. Hindmarch I, Rigney U, Stanley N, Quinlan P, Rycroft J, Lane J. A naturalistic investi-gation of the effects of day-long consumption of tea, coffee and water on alertness, sleeponset and sleep quality. Psychopharmacology (Berlin) 2000; 149(3):203-216.
142. Hindmarch I, Shamsi Z, Stanley N, Fairweather DB. A double-blind, placebo-controlledinvestigation of the effects of fexofenadine, loratadine and promethazine on cognitiveand psychomotor function. Brit J Clin Pharmacol 1999; 48(2):200-206.
143. Jean-Louis G, Kripke DF, Ancoli-Israel S, Klauber MR, Sepulveda RS. Sleep duration,illumination, and activity patterns in a population sample: Effects of gender and ethnic-ity. Biol Psychiatry 2000; 47:921-927.
144. Mendlowicz MV, Jean-Louis G, von Gizycki H, Zizi F, Nunes J. Actigraphic predictorsof depressed mood in a cohort of non-psychiatric adults. Aust NZ J Psychiatry 1999;33(4):553-558.
145. Moorcroft WH, Kayser KH, Griggs AJ. Subjective and objective confirmation of theability to self-awaken at a self-predetermined time without using external means. Sleep1997; 20(1):40-45.
146. Pankhurst FP, Horne JA. The influence of bed partners on movement during sleep. Sleep1994; 17(4):308-315.
147. Reyner A, Horne JA. Gender- and age-related differences in sleep determined by home-recorded sleep logs and actimetry from 400 adults. Sleep 1995; 18(2):127-134.
148. Berger AM, Farr L. The influence of daytime inactivity and nighttime restlessness oncancer-related fatigue. Oncol Nurs Forum 1999; 26:1663-1671.
149. Miaskowski C, Lee KA. Pain, fatigue and sleep disturbances in oncology outpatientsreceiving radiation therapy for bone metastasis: a pilot study. Journal of Pain SymptomManagement 1999; 17(5):320-332.
150. Mormont MC, Waterhouse J, Bleuzen P et al. Marked 24-h rest/activity rhythms areassociated with better quality of life, better response and longer survival in patients withmetastatic colorectal cancer and good performance status. Clinical Cancer Research2000; 6:3038-3045.
151. Berger AM. Patterns of fatigue and activity and rest during adjuvant breast cancerchemotherapy. Oncol Nurs Forum 1998; 25(1):51-62.
152. Dursun SM, Patel JK, Burke JG, Reveley MA. Effects of typical antipsychotic drugs andrisperidone on the quality of sleep in patients with schizophrenia: a pilot study. J Psy-chiatr Neurosci 1999; 24(4):333-337.
153. Lemke MR, Puhl P, Broderick A. Motor activity and perception of sleep in depressedpatients. J Psychiatr Res 1999; 33(3):215-224.
154. Cordoba J, Cabrera J, Lataif L, Penev P, Zee P, Blei AT. High prevalence of sleep dis-turbance in cirrhosis. Hepatology 1998; 27(2):339-345.
155. Redeker NS, Wykpisz E. Effects of age on activity patterns after coronary artery bypasssurgery. Heart Lung 1998; 28(1):5-14.
156. Redeker NS, Mason DJ, Wykpisz E, Glica B. Sleep patterns in women after coronaryartery bypass surgery. Appl Nurs Res 1996; 9(3):115-122.
157. Redeker NS, Tamburri L, Howland CL. Prehospital correlates of sleep in patients hos-pitalized iwth cardiac disease. Res Nurs Health 1998; 21(1):27-37.
158. Pollak CP, Stokes PE, Wagner DR. Nocturnal interactions between community eldersand caregivers, as measured by cross-correlation of their motor activity. J Geriatr Psy-chiatry Neurol 1997; 10:168-173.
159. Ancoli-Israel S, Jones DW, Hanger MA, Parker L, Klauber MR, Kripke DF. Sleep in thenursing home. In: Kuna ST, Suratt PM, Remmers JE, editors. Sleep and Respiration inAging Adults. New York: Elsevier Press, 1991: 77-84.
160. Pat-Horenczyk R, Klauber MR, Shochat T, Ancoli-Israel S. Hourly profiles of sleep andwakefulness in severely versus mild-moderately demented nursing home patients. AgingClin Exp Res 1998; 10:308-315.
161. Shochat T, Martin J, Marler M, Ancoli-Israel S. Illumination levels in nursing homepatients: Effects on sleep and activity rhythms. J Sleep Res 2000; 9(4):373-380.
162. Alessi CA, Schnelle JF, MacRae PG et al. Does physical activity improve sleep inimpaired nursing home residents? J Am Geriatr Soc 1995; 43:1098-1102.
163. Alessi CA, Schnelle JF, Traub S, Ouslander JG. Psychotropic medications in incontinent
nursing home residents: association with sleep and bed mobility. J Am Geriatr Soc 1995;43:788-792.
164. Alessi CA, Yoon EJ, Schnelle JF, Al-Samarrai NR, Cruise PA. A randomized trial of acombined physical activity and environmental intervention in nursing home residents:Do sleep and agitation improve? J Am Geriatr Soc 1999; 47:784-791.
165. Cruise PA, Schnelle JF, Alessi CA, Simmons SF, Ouslander JG. The nighttime environ-ment and incontinence care practices in nursing homes. J Am Geriatr Soc 1998;46(2):463-466.
166. Ouslander JG, Buxton WG, Al-Samarrai NR, Cruise PA, Alessi CA, Schnelle JF. Night-time urinary incontinence and sleep disruption among nursing home residents. J AmGeriatr Soc 1998; 46(4):463-466.
167. Corkum P, Tannock R, Moldofsky H, Hogg-Johnson S, Humphries T. Actigraphy andparental ratings of sleep in children with attention-deficit/hyperactivity disorder(ADHD). Sleep 2001; 24(3):303-312.
168. Glod CA, Teicher MH, Hartman CR, Harakal T. Increased nocturnal activity andimpaired sleep maintenance in abused children. J Am Acad Child Adolesc Psychiat1997; 36(9):1236-1243.
169. McArthur AJ, Budden SS. Sleep dysfunction in Rett syndrome: a trial of exogenousmelatonin treatment. Dev Med Child Neurol 1998; 40(3):186-192.
170. Mennella JA, Gerrish CJ. Effects of exposure to alcohol in mother’s milk on infantsleep. Pediatrics 1998; 101 (5):Ε2.
171. Gertner S, Greenbaum CW, Sadeh A, Dolfin Z, Sirota L, Ben-Nun Y. Sleep-wake pat-terns in preterm infants and 6 month’s home environment: implications for early cogni-tive development. Early Hum Dev 2002; 68(2):93-102.
172. Sadeh A, Gruber R, Raviv A. Sleep, neurobehavioral functioning, and behavior prob-lems in school-age children. Child Development 2002; 73(2):405-417.
173. Sadeh A, Acebo C. The role of actigraphy in sleep medicine. Sleep Medicine Reviews2002; 6(2):113-124.
174. Eissa MA, Poffenbarger T, Portman RJ. Comparison of the actigraph versus patients’diary information in defining circadian time periods for analyzing ambulatory bloodpressure monitoring data. Blood Pressure Monitoring 2001; 6(1):21-25.
175. Hauri PJ. Evaluation of a sleep switch device. Sleep 1999; 22(8):1110-1117.176. Jean-Louis G, von Gizycki H, Zizi F, Spielman A, Hauri P, Taub H. The actigraph data
analysis software: II. A novel approach to scoring and interpreting sleep-wake activity.Percept Mot Skills 1997; 85(1):219-226.
177. Jean-Louis G, Zizi F, von Gizycki H, Hauri P. Actigraphic assessment of sleep in insom-nia: application of the Actigraph Data Analysis Software (ADAS). Physiol Behav 1999;65:569-563.
178. Otsuka K, Cornelissen G, Halberg F. Broad scope of a newly developed actometer inchronobiology, particularly chronocardiology. Chronobiologia 1994; 21:251.
179. van Someren EJ, Lazeron RH, Vonk BF, Mirmiran M, Swaab DF. Gravitational artefactin freqency spectra of movement acceleration: implications for actigraphy in young andelderly subjects. J Neurosci Methods 1996; 65(1):55-62.
180. Verbeek I, Arends J, Declerck G, Beecher L. Wrist actigraphy in comparison withpolysomnography and subjective evaluation in insomnia. In: Coenen AML, editor.Sleep-Wake Research in The Netherlands. Leiden: Dutch Society for Sleep-WakeResearch, 1994: 163-170.
181. Guilleminault C, Yuen KM, Gulevich MG, Karadeniz D, Leger D, Philip P. Hypersom-nia after head-neck trauma: a medicolegal dilemma. Neurology 2000; 54(3):653-659.
182. Hayes MJ, Mitchell D. Spontaneous movements during sleep in children: temporal orga-nization and changes with age. Dev Psychobiol 1998; 32(1):13-21.
183. Kunz D, Bes F. Exogenous melatonin in periodic limb movement disorder: an open clin-ical trial and a hypothesis. Sleep 2001; 24(2):183-187.
184. Honma H, Kohsaka M, Suzuki I et al. Motor activity rhythm in dementia with delirium.Psychiatry Clin Neurosci 1998; 52(2):196-198.
185. Kario K, Schwartz JE, Pickering TG. Ambulatory physical activity as a determinant ofdiurnal blood pressure variation. Hypertension 1999; 34:685-691.
186. Lowden A, Akerstedt T. Retaining home-base sleep hours to prevent jet lag in connec-tion with a westward flight across nine time zones. Chron Intl 2002; 15(4):365-376.
187. Luboshitzky R, Shen-Orr Z, Tzischinsky O, Maldonado M, Herer P, Lavie P. Acti-graphic sleep-wake patterns and urinary 6-sulfatoxymelatonin excretion in patients withAlzheimer’s disease. Chronobiol Int 2001; 18(3):513-524.
188. Lushington K, Dawson D, Encel N, Lack L. Urinary 6-sulfatoxymelatonin cycle-to-cycle variability. Chronobiol Int 1996; 13(6):441-421.
189. Samel A, Vejvoda M, Wittiber K, Wenzel J. Joint NASA-ESA-DARA Study. Part three:circadian rhythms and activity-rest cycle under different CO2 concentrations. AviatSpace Environ Med 1998; 69(5):501-505.
190. van Someren EJ, Scherder EJA, Swaab DF. Transcutaneous electrical nerve stimulation(TENS) improves circadian rhythm disturbances in Alzheimer disease. Alzheimer DisAssoc Disord 1998; 12(2):114-118.
191. Baker A, Simpson A, Dawson D. Sleep disruption and mood changes associated withmenopause. J Psychosomatic Res 1997; 43(4):359-369.
192. Dagan Y, zeevi-luria S, Sever Y et al. Sleep quality in children with attention deficithyperactivity disorder; An actigraphic study. Psychiatry and Clinical Neurosciences1997; 51:383-386.
193. Dinges DF, Pack F, Williams K et al. Cumulative sleepiness, mood disturbance, and psy-chomotor vigilance performance decrements during a week of sleep restricted to 4-5hours per night. Sleep 1997; 20(4):267-277.
194. Glod CA, Teicher MH. Relationship between early abuse, posttraumatic stress disorder,and activity levels in prepubertal children. J Am Acad Child Adolesc Psychiatry 1996;35(10):1384-1393.
195. Haimov I, Lavie P, Laudon M, Herer P, Vigder C, Zisapel N. Melatonin replacementtherapy of elderly insomniacs. Sleep 1995; 18(7):598-603.
196. Humphreys JC, Lee KA, Neylan TC, Marmar CR. Sleep patterns of sheltered batteredwomen. Image J Nurs Sch 1999; 31(2):139-143.
Actigraphy Review Paper—Ancoli-Israel et alSLEEP, Vol. 26, No. 3, 2003 357
197. Ito T, Yamadera H, Ito R, Suzuki H, Asayama K, Endo S. Effects of vitamin B12 onbright light on cognitive and sleep–wake rhythm in Alzheimer-type dementia. Psychia-try and Clinical Neurosciences 2001; 55:281-282.
198. Jean-Louis G, Mendlowicz MV, Gillin JC et al. Sleep estimation from wrist activity inpatients with major depression. Physiol Behav 2000; 70:49-53.
199. Jean-Louis G, von Gizycki H, Zizi F. Melatonin effects on sleep, mood, and cognition inelderly with mild cognitive impairment. J Pineal Res 2002; 25(3):177-183.
200. Kario K, Schwartz JE, Davidson KW, Pickering TG. Gender differences in associationsof diurnal blood pressure variation, awake physical activity, and sleep quality with neg-ative affect: the work site blood pressure study. Hypertension 2001; 38(5):997-1002.
201. Lee KA, Portillo CJ, Miramontes H. The influence of sleep and activity patterns onfatigue in women with HIV/AIDS. J Assoc Nurses AIDS Care 2001; 12 Suppl:19-27.
202. McCarten JR, Kovera C, Maddox MK, Cleary JP. Triazolam in Alzheimer’s disease:pilot study on sleep and memory effects. Pharmacol Biochem Behav 1995; 52(2):447-452.
203. Miller LG, Kraft IA. Application of actigraphy in the clinical setting: use in childrenwith attention-deficit hyperactivity disorder. Pharmacotherapy 1994; 14(2):219-223.
204. Paul MA, Pigeau RA, Weinberg H. CC130 pilot fatigue during re-supply missions toformer Yugoslavia. Aviat Space Environ Med 2001; 72(11):965-973.
205. Redeker NS, Mason DJ, Wykpisz E, Glica B, Miner C. First postoperative week activi-ty patterns and recovery in women after coronary bypass surgery. Nurs Res 1994;43(3):168-173.
206. Sadeh A, Horowitz I, Wolach-Benodis L, Wolach B. Sleep and pulmonary function inchildren with well-controlled, stable asthma. Sleep 1998; 21(4):379-384.
207. Sadeh A, Mcguire J, Sachs H et al. Sleep and psychological characteristics of childrenon a psychiatric inpatient unit. J Am Acad Child Adolesc Psychiatry 1995; 34(6):813-819.
208. Schlesinger I, Hering-Hanit R, Dagan Y. Sleep disturbances after whiplash injury: objec-tive and subjective findings. Headache 2001; 41(6):586-589.
209. Schnelle JF, Alessi CA, Al-Samarrai NR, Fricker RD, Ouslander JG. The nursing homeat night: effects of an intervention on noise, light and sleep. J Am Geriatr Soc 1999;47:430-438.
210. Schweitzer PK, Muehlbach MJ, Walsh JK. Sleepiness and performance during three-dayadministration of cetirizine or diphenhydramine. J Allergy Clin Immunol 1994;94(4):716-724.
211. Shamir E, Laudon M, Barak Y et al. Melatonin improves sleep quality of patients withchronic schizophrenia. J Clin Psychiatry 2000; 65(5):373-377.
212. Shilo L, Dagan Y, Smorjik Y et al. Patients in the intensive care unit suffer from severelack of sleep associated with loss of normal melatonin secretion pattern. Am J Med Sci1999; 317(5):278-281.
213. Shilo L, Dagan Y, Smorjik Y et al. Effect of melatonin on sleep quality of COPD inten-sive care patients: a pilot study. Chronobiol Int 2000; 17(1):71-76.
214. Shinkoda H, Matsumoto K, Park YM. Changes in sleep-wake cycle during the periodfrom late pregnancy to puerperium identified through the wrist actigraph and sleep logs.Psychiatry Clin Neurosci 1999; 53(2):133-135.
215. Shirota A, Tamaki M, Tanaka H, Hayashi M, Shirakawa S, Hori T. Effects of volitionallifestyle on rest-activity cycle in the aged. Psychiatry Clin Neurosci 1999; 53(2):271-272.
216. Stein MA, Blondis TA, Schnitzer ER et al. Methlyphenidate dosing: Twice daily versusthree times daily. Pediatrics 1996;98(4):748-756.
217. Usui A, Ishizuka Y, Obinata I, Okado T, Fukuzawa H, Kanba S. Validity of sleep logcompared with actigraphic sleep-wake state. Psychiatry Clin Neurosci 1998; 52(2):161-163.
218. Usui A, Ishizuka Y, Obinata I, Okado T, Fukuzawa H, Kanba S. Validity of sleep logcompared with actigraphic sleep-wake state II. Psychiatry Clin Neurosci 1999;53(2):183-184.
219. Usui A, Ishizuka Y, Matsushita Y, Fukuzawa H, Kanba S. Bright light treatment fornight-time insomnia and daytime sleepiness in elderly people: comparison with a short-acting hypnotic. Psychiatry Clin Neurosci 2000; 54(3):374-376.
220. van Londen L, Kerkhof GA, van den Berg F et al. Plasma arginine vasopressin andmotor activity in major depression. Biol Psychiatry 1998; 43(3):196-204.
221. Van Der Meer YG, Swanink CM, Zitman FG et al. Randomised, double-blind, placebo-controlled study of fluoxetine in chronic fatigue syndrome. Lancet 1996; 347:858-861.
222. Wallace-Guy GM, Kripke DF, Jean-Louis G, Langer RD, Elliott JA, Tuunainen A.Evening light exposure: implications for sleep and depression. J Am Geriatr Soc 2002;50(4):738-739.
223. Wolter TD, Hauri PJ, Schroeder DR et al. Effects of 24-hr nicotine replacement on sleepand daytime activity during smoking cessation. Prev Med 1996; 25(5):601-610.
224. Yesavage JA, Taylor JL, Kraemer H, Noda A, Friedman L, Tinklenberg JR. Sleep/Wakecycle disturbance in Alzheimer’s disease: how much is due to an inherent trait? Int Psy-chogeriatr 2002; 14(1):73-81.
225. Zhdanova IV, Wurtman RJ, Wagstaff J. Effects of a low dose of melatonin on sleep inchildren with Angelman syndrome. J Pediatr Endocrinol Metab 1999; 12(1):57-67.
APPENDIX A. ABBREVIATIONS
ACT - actigraphy ADAS - Actigraph Data Analysis Software ADHD - Attention deficit hyper-activity disorderAIMS – Abnormal Involuntary Movement ScaleANOVA - analysis of varianceASA – Actigraphic Scoring Analysis BL - baseline
BP - blood pressure BRM - behavioral response monitoring BT - bedtime CES-D - Center for Epidemiologic Studies-Depression scale CR - circadian rhythmCSQP – Child Sleep Questionnaire ParentD - day DB - double-blinded DSPS - delayed sleep phase syndromedesats - desaturation events DLMO - Dim Light Melatonin Onsetdom - dominant dur - duration Dx - diagnosisECG - electrocardiogram EDS - excessive daytime sleepiness EMG - electromyogram epi - epinephrine EPS – Simpson Angus Extrapyramidal Symptom ScaleF- female f/u - follow-upg-gramsGH - growth hormoneGrp - group h/o- history ofHADS – Hospital Anxiety and Depression ScaleHAMD - Hamilton Depression ScaleHR - heart rate h – hour(s)IS: interdaily stabilityIV: interdaily variabilitylog - sleep log or diary LSEQ - Leeds Sleep Evaluation QuestionnaireLt - left M - male meds - medicationsmel – melatoninMID – multi-infarct dementiamins – minutesMML – Mini-MotionLogger (AMI – Ambulatory Monitoring, Inc)MMDG - mild-moderately demented group MMNDG - Moderate, Mild or No Dementia Group MMSE - Mini-Mental State Exammo - monthMSLT - multiple sleep latency test ndom -non dominantNINCDS-ADRDA – National Institute of Neurological and Commu-nicative Disorders and Stroke and the Alzheimer’s Disease and RelatedDisorders AssociationNH - nursing homenorepi - norepinephrineNS - not stated Nt - night num - number OBJ - objectiveOCP - oral contraceptive OSAS - obstructive sleep apnea syndrome PLM - periodic limb movements PLMD/RLS - periodic limb movement disorder/restless legs syndrome POMS-Profile of Mood StatesPRMT - Probed recall memory testPSG - polysomnography PSQI - Pittsburgh Sleep Quality IndexPTSD – Post Traumatic Stress Disorderpts - patients PVT - psychomotor vigilance task
Actigraphy Review Paper—Ancoli-Israel et alSLEEP, Vol. 26, No. 3, 2003 358
QOL - quality of lifeQWB - Quality of Well Beingr - correlation coefficient RA- relative amplitudeRCT - randomized controlled trialRDI – respiratory disturbance indexRt- rightRx - drugSAD – Seasonal Affective DisorderSANS – Scale for the Assessment of Negative SymptomsSAPS – Scale for the Assessment of Positive SymptomsSB - single-blinded SBJ - subjective SDAT – Senile Dementia of Alzheimer’s typesecs - secondsSDG - Severe Dementia Group, Sdur - Sleep duration SE - sleep efficiency SEI – Sleep Efficiency IndexSH - sleep hygieneSHAPS-D - Snaith-Hamilton-Pleasure-Scale SL - sleep latencySOff - sleep offsetSOL - sleep onset latency SOn -sleep onsetSP-sleep periodSQ - sleep qualitySSS - Stanford Sleepiness Scale STAI- State Trait Anxiety InventoryS/W - sleep/wakeSWT - sleep wake transitionstemp - temperatureTENS - transcutaneous electrical nerve stimulation TIB - time in bed TST - total sleep time TWT - total wake timeTx - treatmentVAS - visual analogue scaleW - wake w/ - withw/o - without w/i - withinWASO - wake after sleep onset wk - weekyr - year6SMT - 6-sulphatoxymelatonin
CompaniesAMI - Ambulatory Monitoring, Inc.MM - Mini Mitter
Actigraphy Review Paper—Ancoli-Israel et alSLEEP, Vol. 26, No. 3, 2003 359
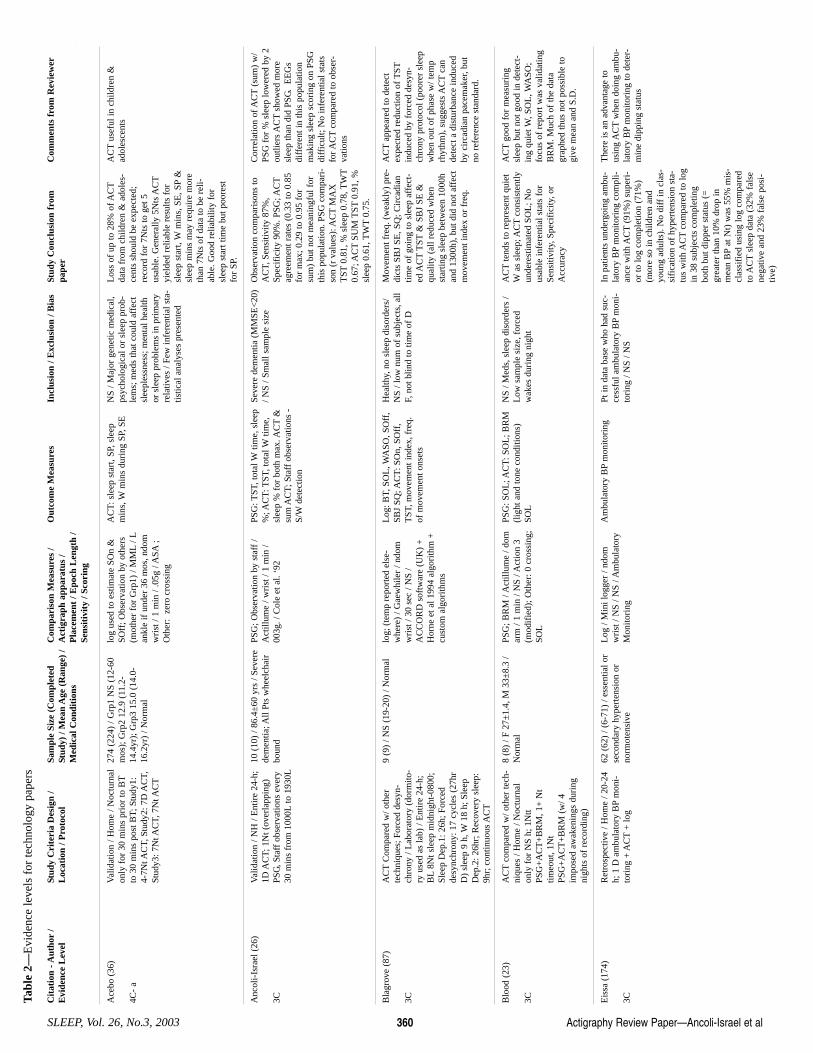
Actigraphy Review Paper—Ancoli-Israel et alSLEEP, Vol. 26, No.3, 2003 360
Cit
atio
n - A
utho
r/
Evi
denc
e L
evel
St
udy
Cri
teri
a D
esig
n /
Loc
atio
n / P
roto
col
Sam
ple
Size
(C
ompl
eted
Stud
y) /
Mea
n A
ge (
Ran
ge)
/M
edic
al C
ondi
tion
s
Com
pari
son
Mea
sure
s /
Act
igra
ph a
ppar
atus
/P
lace
men
t / E
poch
Len
gth
/Se
nsit
ivit
y / S
cori
ng
Out
com
e M
easu
res
Incl
usio
n / E
xclu
sion
/ B
ias
Stud
y C
oncl
usio
n fr
ompa
per
Com
men
ts f
rom
Rev
iew
er
Anc
oli-
Isra
el (
26)
3C
Val
idat
ion
/ NH
/ E
ntir
e 24
-h;
1D A
CT;
1N
t (ov
erla
ppin
g)PS
G, S
taff
obs
erva
tions
eve
ry30
min
s fr
om 1
000L
to 1
930L
10 (
10)
/ 86.
4±60
yrs
/ Se
vere
dem
entia
; All
Pts
whe
elch
air
boun
d
PSG
; Obs
erva
tion
by s
taff
/A
ctill
ume
/ wri
st /
1 m
in /
003g
. / C
ole
et a
l. ‘9
2
PSG
: TST
, tot
al W
time,
sle
ep%
; AC
T: T
ST, t
otal
Wtim
e,sl
eep
% f
or b
oth
max
. AC
T&
sum
AC
T; S
taff
obs
erva
tions
-S/
Wde
tect
ion
Seve
re d
emen
tia (
MM
SE<
20)
/ NS
/ Sm
all s
ampl
e si
ze
Obs
erva
tion
com
pari
sons
toA
CT,
Sen
sitiv
ity 8
7%,
Spec
ific
ity 9
0%. P
SG; A
CT
agre
emen
t rat
es (
0.33
to 0
.85
for
max
; 0.2
9 to
0.9
5 fo
rsu
m)
but n
ot m
eani
ngfu
l for
this
pop
ulat
ion.
PSG
com
pari
-so
n (r
val
ues)
: AC
TM
AX
TST
0.81
, % s
leep
0.7
8, T
WT
0.67
; AC
TSU
M T
ST0.
91, %
slee
p 0.
61, T
WT
0.75
.
Cor
rela
tion
of A
CT
(sum
) w
/PS
G f
or %
sle
ep lo
wer
ed b
y 2
outli
ers
AC
Tsh
owed
mor
esl
eep
than
did
PSG
. E
EG
sdi
ffer
ent i
n th
is p
opul
atio
nm
akin
g sl
eep
scor
ing
on P
SGdi
ffic
ult;
No
infe
rent
ial s
tats
for A
CT
com
pare
d to
obs
er-
vatio
ns
Ace
bo (
36)
4C-
a
Val
idat
ion
/ Hom
e / N
octu
rnal
only
for
30
min
s pr
ior
to B
Tto
30
min
s po
st B
T; S
tudy
1:4-
7Nt A
CT,
Stu
dy2:
7D
AC
T,St
udy3
: 7N
t AC
T, 7
Nt A
CT
274
(224
) / G
rp1
NS
(12-
60m
os);
Grp
2 12
.9 (
11.2
-14
.4yr
); G
rp3
15.0
(14
.0-
16.2
yr)
/ Nor
mal
log
used
to e
stim
ate
SOn
&SO
ff; O
bser
vatio
n by
oth
ers
(mot
her
for
Grp
1) /
MM
L/ L
ankl
e if
und
er 3
6 m
os, n
dom
wri
st /
1 m
in /
.05g
/ A
SA;
Oth
er:
zero
cro
ssin
g
AC
T: s
leep
sta
rt, S
P, s
leep
min
s, W
min
s du
ring
SP,
SE
N
S / M
ajor
gen
etic
med
ical
,ps
ycho
logi
cal o
r sl
eep
prob
-le
ms;
med
s th
at c
ould
aff
ect
slee
ples
snes
s; m
enta
l hea
lthor
sle
ep p
robl
ems
in p
rim
ary
rela
tives
/ Fe
w in
fere
ntia
l sta
-tis
tical
ana
lyse
s pr
esen
ted
Los
s of
up
to 2
8% o
f AC
Tda
ta f
rom
chi
ldre
n &
ado
les-
cent
s sh
ould
be
expe
cted
;re
cord
for
7N
ts to
get
5us
able
. Gen
eral
ly 5
Nts
AC
Tyi
elde
d re
liabl
e re
sults
for
slee
p st
art,
Wm
ins,
SE
, SP
&sl
eep
min
s m
ay r
equi
re m
ore
than
7N
ts o
f da
ta to
be
reli-
able
. Goo
d re
liabi
lity
for
slee
p st
art t
ime
but p
oore
stfo
r SP
.
AC
Tus
eful
in c
hild
ren
&ad
oles
cent
s
Tabl
e 2—
Evi
denc
e le
vels
for
tech
nolo
gy p
aper
s
Bla
grov
e (8
7)
3C
AC
TC
ompa
red
w/ o
ther
tech
niqu
es; F
orce
d de
syn-
chro
ny /
Lab
orat
ory
(dor
mito
-ry
use
d as
lab)
/ E
ntir
e 24
-h;
BL
8Nt s
leep
mid
nigh
t-08
00;
Slee
p D
ep.1
: 26h
; For
ced
desy
nchr
ony:
17
cycl
es (
27hr
D)
slee
p 9
h, W
18 h
; Sle
epD
ep.2
: 26h
r; R
ecov
ery
slee
p:9h
r; c
ontin
uous
AC
T
9 (9
) / N
S (1
9-20
) / N
orm
al
log;
(te
mp
repo
rted
els
e-w
here
) / G
aew
hile
r / n
dom
wri
st /
30 s
ec /
NS
/A
CC
OR
D s
oftw
are
(UK
) +
Hor
ne e
t al 1
994
algo
rith
m +
cust
om a
lgor
ithm
s
Log
: BT,
SO
L, W
ASO
, SO
ff,
SBJ
SQ; A
CT
: SO
n, S
Off
,T
ST, m
ovem
ent i
ndex
, fre
q.of
mov
emen
t ons
ets
Hea
lthy,
no
slee
p di
sord
ers/
NS
/ low
num
of
subj
ects
, all
F, n
ot b
lind
to ti
me
of D
Mov
emen
t fre
q. (
wea
kly)
pre
-di
cts
SBJ
SE, S
Q; C
irca
dian
time
of g
oing
to s
leep
aff
ect-
ed A
CT
TST
& S
BJ
SE &
qual
ity (
all r
educ
ed w
hen
star
ting
slee
p be
twee
n 10
00h
and
1300
h), b
ut d
id n
ot a
ffec
tm
ovem
ent i
ndex
or
freq
.
AC
Tap
pear
ed to
det
ect
expe
cted
red
uctio
n of
TST
indu
ced
by f
orce
d de
syn-
chro
ny p
roto
col (
poor
er s
leep
whe
n ou
t of
phas
e w
/ tem
prh
ythm
), s
ugge
sts
AC
Tca
nde
tect
a d
istu
rban
ce in
duce
dby
cir
cadi
an p
acem
aker
, but
no r
efer
ence
sta
ndar
d.
Blo
od (
23)
3C
AC
Tco
mpa
red
w/ o
ther
tech
-ni
ques
/ H
ome
/ Noc
turn
alon
ly f
or N
S h;
1N
ttPS
G+
AC
T+
BR
M, 1
+ N
ttim
eout
, 1N
tPS
G+
AC
T+
BR
M (
w/ 4
impo
sed
awak
enin
gs d
urin
gni
ghts
of
reco
rdin
g)
8 (8
) / F
27±
1.4,
M 3
3±8.
3 /
Nor
mal
PS
G; B
RM
/ A
ctill
ume
/ dom
arm
/ 1
min
/ N
S / A
ctio
n 3
(mod
ifie
d); O
ther
: 0 c
ross
ing;
SOL
PSG
: SO
L; A
CT
: SO
L; B
RM
(lig
ht a
nd to
ne c
ondi
tions
)SO
L
NS
/ Med
s, s
leep
dis
orde
rs /
Low
sam
ple
size
, for
ced
wak
es d
urin
g ni
ght
AC
Tte
nds
to r
epre
sent
qui
etW
as s
leep
; AC
Tco
nsis
tent
lyun
dere
stim
ated
SO
L; N
ous
able
infe
rent
ial s
tats
for
Sens
itivi
ty, S
peci
fici
ty, o
rA
ccur
acy
AC
Tgo
od f
or m
easu
ring
slee
p bu
t not
goo
d in
det
ect-
ing
quie
t W, S
OL
, WA
SO;
focu
s of
rep
ort w
as v
alid
atin
gB
RM
. Muc
h of
the
data
grap
hed
thus
not
pos
sibl
e to
give
mea
n an
d S.
D.
Eis
sa (
174)
3C
Ret
rosp
ectiv
e / H
ome
/ 20-
24h;
1 D
am
bula
tory
BP
mon
i-to
ring
+ A
CT
+ lo
g
62 (
62)
/ (6-
71)
/ ess
entia
l or
seco
ndar
y hy
pert
ensi
on o
rno
rmot
ensi
ve
Log
/ M
ini l
ogge
r / n
dom
wri
st /
NS
/ NS
/ Am
bula
tory
Mon
itori
ng
Am
bula
tory
BP
mon
itori
ng
Pt in
dat
a ba
se w
ho h
ad s
uc-
cess
ful a
mbu
lato
ry B
Pm
oni-
tori
ng /
NS
/ NS
In p
atie
nts
unde
rgoi
ng a
mbu
-la
tory
BP
mon
itori
ng c
ompl
i-an
ce w
ith A
CT
(91%
) su
peri
-or
to lo
g co
mpl
etio
n (7
1%)
(mor
e so
in c
hild
ren
and
youn
g ad
ults
). N
o di
ff in
cla
s-si
fica
tion
of h
yper
tens
ion
sta-
tus
with
AC
Tco
mpa
red
to lo
gin
38
subj
ects
com
plet
ing
both
but
dip
per
stat
us (
=gr
eate
r th
an 1
0% d
rop
inm
ean
BP
at N
t) w
as 5
5% m
is-
clas
sifi
ed u
sing
log
com
pare
dto
AC
Tsl
eep
data
(32
% f
alse
nega
tive
and
23%
fal
se p
osi-
tive)
The
re is
an
adva
ntag
e to
usin
g A
CT
whe
n do
ing
ambu
-la
tory
BP
mon
itori
ng to
det
er-
min
e di
ppin
g st
atus
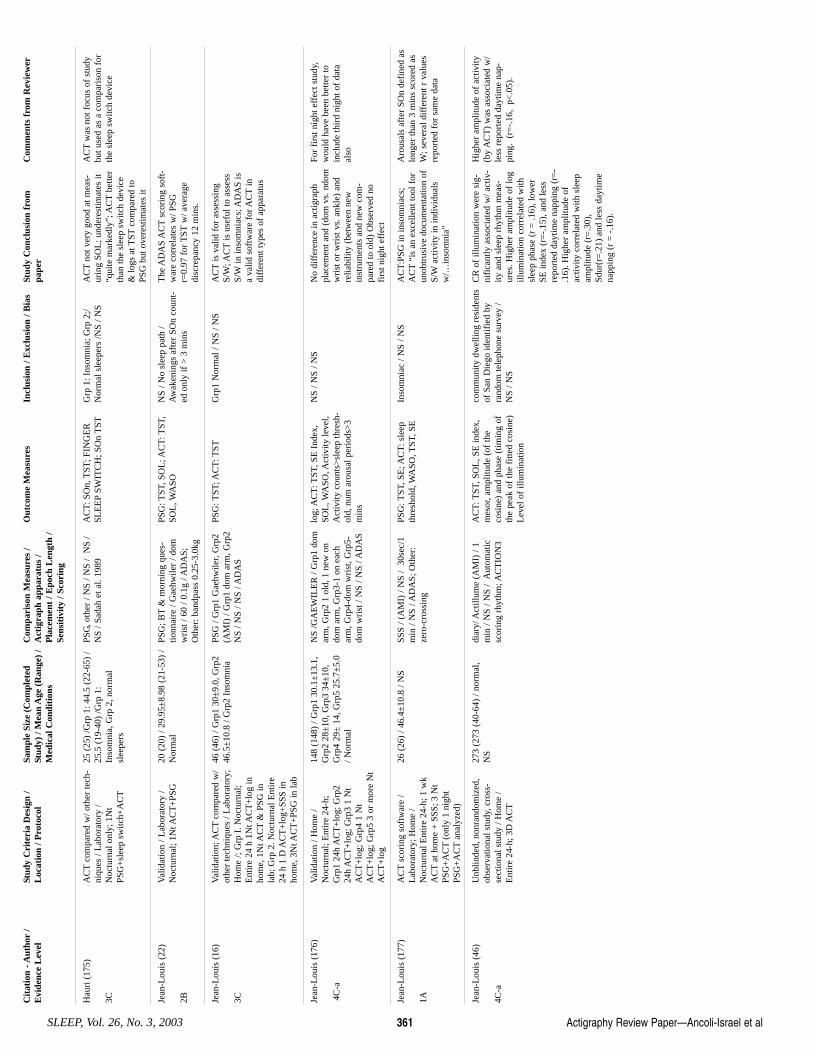
Cit
atio
n - A
utho
r/
Evi
denc
e L
evel
St
udy
Cri
teri
a D
esig
n /
Loc
atio
n / P
roto
col
Sam
ple
Size
(C
ompl
eted
Stud
y) /
Mea
n A
ge (
Ran
ge)
/M
edic
al C
ondi
tion
s
Com
pari
son
Mea
sure
s /
Act
igra
ph a
ppar
atus
/P
lace
men
t / E
poch
Len
gth
/Se
nsit
ivit
y / S
cori
ng
Out
com
e M
easu
res
Incl
usio
n / E
xclu
sion
/ B
ias
Stud
y C
oncl
usio
n fr
ompa
per
Com
men
ts f
rom
Rev
iew
er
Actigraphy Review Paper—Ancoli-Israel et alSLEEP, Vol. 26, No. 3, 2003 361
Hau
ri (
175)
3C
AC
Tco
mpa
red
w/ o
ther
tech
-ni
ques
/ L
abor
ator
y /
Noc
turn
al o
nly;
1N
tPS
G+
slee
p sw
itch+
AC
T
25 (
25)
/Grp
1: 4
4.5
(22-
65)
/25
.5 (
19-4
0) /G
rp 1
:In
som
nia,
Grp
2, n
orm
alsl
eepe
rs
PSG
, oth
er /
NS
/ NS
/ N
S /
NS
/ Sad
ah e
t al.
1989
A
CT
: SO
n, T
ST; F
ING
ER
SLE
EP
SWIT
CH
; SO
n T
STG
rp 1
: Ins
omni
a; G
rp 2
;/N
orm
al s
leep
ers
/NS
/ NS
AC
Tno
t ver
y go
od a
t mea
s-ur
ing
SOL
; und
eres
timat
es it
“qui
te m
arke
dly”
; AC
Tbe
tter
than
the
slee
p sw
itch
devi
ce&
logs
at T
STco
mpa
red
toPS
G b
ut o
vere
stim
ates
it
AC
Tw
as n
ot f
ocus
of
stud
ybu
t use
d as
a c
ompa
riso
n fo
rth
e sl
eep
switc
h de
vice
Jean
-Lou
is (
22)
2B
Val
idat
ion
/ Lab
orat
ory
/N
octu
rnal
; 1N
t AC
T+
PSG
20
(20
) / 2
9.95
±8.
98 (
21-5
3) /
Nor
mal
PS
G; B
T&
mor
ning
que
s-tio
nnai
re /
Gae
hwile
r / d
omw
rist
/ 60
/ 0.
1g /
AD
AS;
Oth
er: b
andp
ass
0.25
-3.0
kg
PSG
: TST
, SO
L; A
CT
: TST
,SO
L, W
ASO
N
S / N
o sl
eep
path
/A
wak
enin
gs a
fter
SO
n co
unt-
ed o
nly
if >
3 m
ins
The
AD
AS
AC
Tsc
orin
g so
ft-
war
e co
rrel
ates
w/ P
SGr=
0.97
for
TST
w/ a
vera
gedi
scre
panc
y 12
min
s.
Jean
-Lou
is (
16)
3C
Val
idat
ion;
AC
Tco
mpa
red
w/
othe
r te
chni
ques
/ L
abor
ator
y;H
ome
/; G
rp I
. Noc
turn
al;
Ent
ire
24 h
1N
t AC
T+
log
inho
me,
1N
t AC
T&
PSG
inla
b; G
rp 2
. Noc
turn
al E
ntir
e24
h 1
D A
CT
+lo
g+SS
S in
hom
e, 3
Nt A
CT
+PS
G in
lab
46 (
46)
/ Grp
1 30
±9.
0, G
rp2
46.5
±10
.8 /
Grp
2 In
som
nia
PSG
/ G
rp1
Gae
hwile
r, G
rp2
(AM
I) /
Grp
1 do
m a
rm, G
rp2
NS
/ NS
/ NS
/ AD
AS
PSG
: TST
; AC
T: T
STG
rp1
Nor
mal
/ N
S / N
S A
CT
is v
alid
for
ass
essi
ngS/
W; A
CT
is u
sefu
l to
asse
ssS/
Win
inso
mni
acs;
AD
AS
isa
valid
sof
twar
e fo
r AC
Tin
diff
eren
t typ
es o
f ap
para
tus
Jean
-Lou
is (
176)
4C-a
Val
idat
ion
/ Hom
e /
Noc
turn
al; E
ntir
e 24
-h;
Grp
1 24
h A
CT
+lo
g; G
rp2
24h
AC
T+
log;
Grp
3 1
Nt
AC
T+
log;
Grp
4 1
Nt
AC
T+
log;
Grp
5 3
or m
ore
Nt
AC
T+
log
148
(148
) / G
rp1
30.1
±13
.1,
Grp
2 28
±10
, Grp
3 34
±10
,G
rp4
29±
14,
Grp
5 25
.7±
5.0
/ Nor
mal
NS
/GA
EW
ILE
R /
Grp
1 do
mar
m, G
rp2
1 ol
d, 1
new
on
dom
arm
, Grp
3-1
on e
ach
arm
, Grp
4-do
m w
rist
, Grp
5-do
m w
rist
/ N
S / N
S / A
DA
S
log;
AC
T: T
ST, S
E I
ndex
,SO
L, W
ASO
, Act
ivity
leve
l,A
ctiv
ity c
ount
s>sl
eep
thre
sh-
old,
num
aro
usal
per
iods
>3
min
s
NS
/ NS
/ NS
No
diff
eren
ce in
act
igra
phpl
acem
ent a
nd (
dom
vs.
ndo
mw
rist
or
wri
st v
s. a
nkle
) an
dre
liabi
lity
(bet
wee
n ne
win
stru
men
ts a
nd n
ew c
om-
pare
d to
old
) O
bser
ved
nofi
rst n
ight
eff
ect
For
firs
t nig
ht e
ffec
t stu
dy,
wou
ld h
ave
been
bet
ter
toin
clud
e th
ird
nigh
t of
data
also
Jean
-Lou
is (
177)
1A
AC
Tsc
orin
g so
ftw
are
/L
abor
ator
y; H
ome
/N
octu
rnal
Ent
ire
24-h
; 1 w
kA
CT
at h
ome
+ S
SS; 3
Nt
PSG
+A
CT
(onl
y 1
nigh
tPS
G+
AC
Tan
alyz
ed)
26 (
26)
/ 46.
4±10
.8 /
NS
SSS
/ (A
MI)
/ N
S /
30se
c/1
min
/ N
S / A
DA
S; O
ther
:ze
ro-c
ross
ing
PSG
: TST
, SE
; AC
T: s
leep
thre
shol
d, W
ASO
, TST
, SE
In
som
niac
/ N
S / N
S A
CT
:PSG
in in
som
niac
s;A
CT
“is
an e
xcel
lent
tool
for
unob
trus
ive
docu
men
tatio
n of
S/W
activ
ity in
indi
vidu
als
w/…
inso
mni
a”
Aro
usal
s af
ter
SOn
defi
ned
aslo
nger
than
3 m
ins
scor
ed a
sW
; sev
eral
dif
fere
nt r
val
ues
repo
rted
for
sam
e da
ta
Jean
-Lou
is (
46)
4C-a
Unb
linde
d, n
onra
ndom
ized
,ob
serv
atio
nal s
tudy
, cro
ss-
sect
iona
l stu
dy /
Hom
e /
Ent
ire
24-h
; 3D
AC
T
273
(273
(40
-64)
/ no
rmal
,N
S di
ary/
Act
illum
e (A
MI)
/ 1
min
/ N
S / N
S /
Aut
omat
icsc
orin
g rh
ythm
; AC
TIO
N3
AC
T: T
ST, S
OL
, SE
inde
x,m
esor
, am
plitu
de (
of th
eco
sine
) an
d ph
ase
(tim
ing
ofth
e pe
ak o
f th
e fi
tted
cosi
ne)
Lev
el o
f ill
umin
atio
n
com
mun
ity d
wel
ling
resi
dent
sof
San
Die
go id
entif
ied
byra
ndom
tele
phon
e su
rvey
/N
S / N
S
CR
of
illum
inat
ion
wer
e si
g-ni
fica
ntly
ass
ocia
ted
w/ a
ctiv
-ity
and
sle
ep r
hyth
m m
eas-
ures
. Hig
her
ampl
itude
of
log
illum
inat
ion
corr
elat
ed w
ithsl
eep
phas
e (r
= .1
6), l
ower
SE in
dex
(r=
-.15
), a
nd le
ssre
port
ed d
aytim
e na
ppin
g (r
=-
.16)
. Hig
her
ampl
itude
of
activ
ity c
orre
late
d w
ith s
leep
ampl
itude
(r=
.30)
,Sd
ur(r
=.2
1) a
nd le
ss d
aytim
ena
ppin
g (r
= -
.16)
.
Hig
her
ampl
itude
of
activ
ity(b
y A
CT
) w
as a
ssoc
iate
d w
/le
ss r
epor
ted
dayt
ime
nap-
ping
. (r
=-.
16,
p<.0
5).
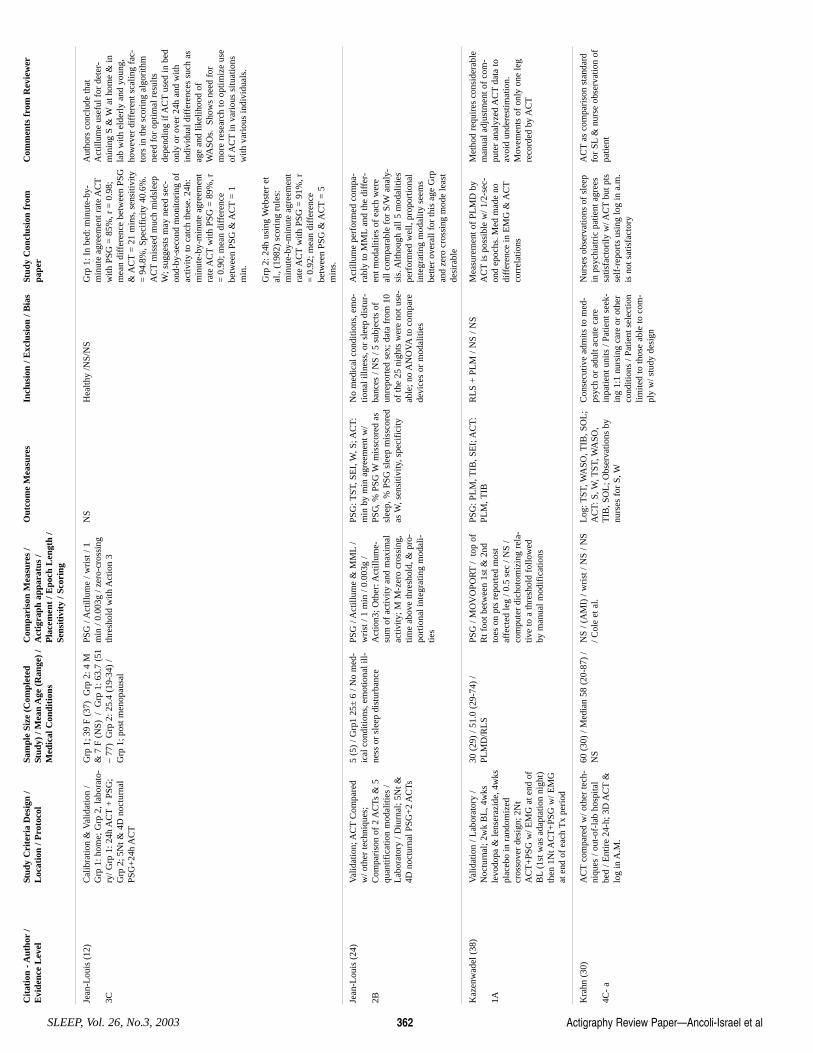
Cit
atio
n - A
utho
r/
Evi
denc
e L
evel
St
udy
Cri
teri
a D
esig
n /
Loc
atio
n / P
roto
col
Sam
ple
Size
(C
ompl
eted
Stud
y) /
Mea
n A
ge (
Ran
ge)
/M
edic
al C
ondi
tion
s
Com
pari
son
Mea
sure
s /
Act
igra
ph a
ppar
atus
/P
lace
men
t / E
poch
Len
gth
/Se
nsit
ivit
y / S
cori
ng
Out
com
e M
easu
res
Incl
usio
n / E
xclu
sion
/ B
ias
Stud
y C
oncl
usio
n fr
ompa
per
Com
men
ts f
rom
Rev
iew
er
Actigraphy Review Paper—Ancoli-Israel et alSLEEP, Vol. 26, No.3, 2003 362
Jean
-Lou
is (
12)
3C
Cal
ibra
tion
& V
alid
atio
n /
Grp
1: h
ome;
Grp
2, l
abor
ato-
ry/ G
rp 1
: 24h
AC
T+
PSG
;G
rp 2
; 5N
t & 4
D n
octu
rnal
PSG
+24
h A
CT
Grp
1; 3
9 F
(37)
Grp
2: 4
M&
7 F
(N
S) /
Grp
1: 6
3.7
(51
– 77
) G
rp 2
: 25.
4 (1
9-34
) /
Grp
1; p
ost m
enop
ausa
l
PSG
/ A
ctill
ume
/ wri
st /
1m
in /
0.00
3g /
zero
-cro
ssin
gth
resh
old
with
Act
ion
3
NS
Hea
lthy
/NS/
NS
Grp
1: I
n be
d: m
inut
e-by
-m
inut
e ag
reem
ent r
ate
AC
Tw
ith P
SG =
85%
, r =
0.9
8;m
ean
diff
eren
ce b
etw
een
PSG
& A
CT
= 2
1 m
ins,
sen
sitiv
ity=
94.
8%, S
peci
fici
ty 4
0.6%
.A
CT
mis
sed
muc
h m
idsl
eep
W; s
ugge
sts
may
nee
d se
c-on
d-by
-sec
ond
mon
itori
ng o
fac
tivity
to c
atch
thes
e. 2
4h:
min
ute-
by-m
inut
e ag
reem
ent
rate
AC
Tw
ith P
SG =
89%
, r=
0.9
0; m
ean
diff
eren
cebe
twee
n PS
G &
AC
T=
1m
in.
Grp
2: 2
4h u
sing
Web
ster
et
al.,
(198
2) s
cori
ng r
ules
:m
inut
e-by
-min
ute
agre
emen
tra
te A
CT
with
PSG
= 9
1%, r
= 0
.92;
mea
n di
ffer
ence
betw
een
PSG
& A
CT
= 5
min
s.
Aut
hors
con
clud
e th
atA
ctill
ume
usef
ul f
or d
eter
-m
inin
g S
& W
at h
ome
& in
lab
with
eld
erly
and
you
ng,
how
ever
dif
fere
nt s
calin
g fa
c-to
rs in
the
scor
ing
algo
rith
mne
ed f
or o
ptim
al r
esul
tsde
pend
ing
if A
CT
used
in b
edon
ly o
r ov
er 2
4h a
nd w
ithin
divi
dual
dif
fere
nces
suc
h as
age
and
likel
ihoo
d of
WA
SOs.
Sho
ws
need
for
mor
e re
sear
ch to
opt
imiz
e us
eof
AC
Tin
var
ious
situ
atio
nsw
ith v
ario
us in
divi
dual
s.
Jean
-Lou
is (
24)
2B
Val
idat
ion;
AC
TC
ompa
red
w/ o
ther
tech
niqu
es;
Com
pari
son
of 2
AC
Ts &
5qu
antif
icat
ion
mod
aliti
es /
Lab
orat
ory
/ Diu
rnal
; 5N
t &4D
noc
turn
al P
SG+
2 A
CTs
5 (5
) / G
rp1
25±
6 /
No
med
-ic
al c
ondi
tions
, em
otio
nal i
ll-ne
ss o
r sl
eep
dist
urba
nce
PSG
/ A
ctill
ume
& M
ML
/w
rist
/ 1
min
/ 0.
003g
/A
ctio
n3; O
ther
: Act
illum
e-su
m o
f ac
tivity
and
max
imal
activ
ity; M
M-z
ero
cros
sing
,tim
e ab
ove
thre
shol
d, &
pro
-po
rtio
nal i
nteg
ratin
g m
odal
i-tie
s
PSG
: TST
, SE
I, W
, S; A
CT
:m
in b
y m
in a
gree
men
t w/
PSG
, % P
SG W
mis
scor
ed a
ssl
eep,
% P
SG s
leep
mis
scor
edas
W, s
ensi
tivity
, spe
cifi
city
No
med
ical
con
ditio
ns, e
mo-
tiona
l illn
ess,
or
slee
p di
stur
-ba
nces
/ N
S / 5
sub
ject
s of
unre
port
ed s
ex; d
ata
from
10
of th
e 25
nig
hts
wer
e no
t use
-ab
le; n
o A
NO
VA
to c
ompa
rede
vice
s or
mod
aliti
es
Act
illum
e pe
rfor
med
com
pa-
rabl
y to
MM
Lan
d th
e di
ffer
-en
t mod
aliti
es o
f ea
ch w
ere
all c
ompa
rabl
e fo
r S/
Wan
aly-
sis.
Alth
ough
all
5 m
odal
ities
perf
orm
ed w
ell,
prop
ortio
nal
inte
grat
ing
mod
ality
see
ms
bette
r ov
eral
l for
this
age
Grp
and
zero
cro
ssin
g m
ode
leas
tde
sira
ble
Kaz
enw
adel
(38
)
1A
Val
idat
ion
/ Lab
orat
ory
/N
octu
rnal
; 2w
k B
L, 4
wks
levo
dopa
& le
nser
azid
e, 4
wks
plac
ebo
in r
ando
miz
edcr
osso
ver
desi
gn; 2
Nt
AC
T+
PSG
w/ E
MG
at e
nd o
fB
L(1
st w
as a
dapt
atio
n ni
ght)
then
1N
t AC
T+
PSG
w/ E
MG
at e
nd o
f ea
ch T
x pe
riod
30 (
29)
/ 51.
0 (2
9-74
) /
PLM
D/R
LS
PSG
/ M
OV
OPO
RT
/ to
p of
Rt f
oot b
etw
een
1st &
2nd
toes
on
pts
repo
rted
mos
taf
fect
ed le
g / 0
.5 s
ec /
NS
/co
mpu
ter
dich
otom
izin
g re
la-
tive
to a
thre
shol
d fo
llow
edby
man
ual m
odif
icat
ions
PSG
: PL
M, T
IB, S
EI;
AC
T:
PLM
, TIB
R
LS
+ P
LM
/ N
S / N
S M
easu
rem
ent o
f PL
MD
by
AC
Tis
pos
sibl
e w
/ 1/2
-sec
-on
d ep
ochs
. Med
mad
e no
diff
eren
ce in
EM
G &
AC
Tco
rrel
atio
ns
Met
hod
requ
ires
con
side
rabl
em
anua
l adj
ustm
ent o
f co
m-
pute
r an
alyz
ed A
CT
data
toav
oid
unde
rest
imat
ion.
Mov
emen
ts o
f on
ly o
ne le
gre
cord
ed b
y A
CT
Kra
hn (
30)
4C-
a
AC
Tco
mpa
red
w/ o
ther
tech
-ni
ques
/ ou
t-of
-lab
hos
pita
lbe
d / E
ntir
e 24
-h; 3
D A
CT
&lo
g in
A.M
.
60 (
30)
/ Med
ian
58 (
20-8
7) /
NS
NS
/ (A
MI)
/ w
rist
/ N
S / N
S/ C
ole
et a
l. L
og: T
ST, W
ASO
, TIB
, SO
L;
AC
T: S
, W, T
ST, W
ASO
,T
IB, S
OL
; Obs
erva
tions
by
nurs
es f
or S
, W
Con
secu
tive
adm
its to
med
-ps
ych
or a
dult
acut
e ca
rein
patie
nt u
nits
/ Pa
tient
see
k-in
g 1:
1 nu
rsin
g ca
re o
r ot
her
cond
ition
s / P
atie
nt s
elec
tion
limite
d to
thos
e ab
le to
com
-pl
y w
/ stu
dy d
esig
n
Nur
ses
obse
rvat
ions
of
slee
pin
psy
chia
tric
pat
ient
agr
ees
satis
fact
orily
w/ A
CT
but p
tsse
lf-r
epor
ts u
sing
log
in a
.m.
is n
ot s
atis
fact
ory
AC
Tas
com
pari
son
stan
dard
for
SL&
nur
se o
bser
vatio
n of
patie
nt
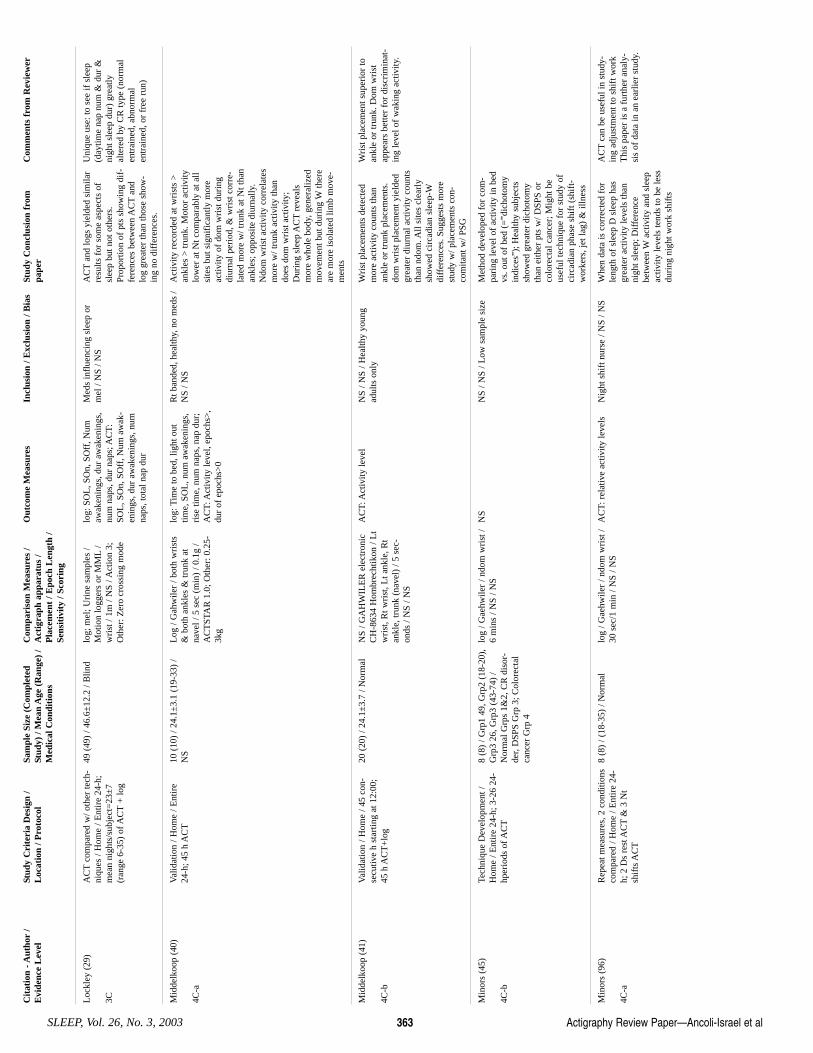
Cit
atio
n - A
utho
r/
Evi
denc
e L
evel
St
udy
Cri
teri
a D
esig
n /
Loc
atio
n / P
roto
col
Sam
ple
Size
(C
ompl
eted
Stud
y) /
Mea
n A
ge (
Ran
ge)
/M
edic
al C
ondi
tion
s
Com
pari
son
Mea
sure
s /
Act
igra
ph a
ppar
atus
/P
lace
men
t / E
poch
Len
gth
/Se
nsit
ivit
y / S
cori
ng
Out
com
e M
easu
res
Incl
usio
n / E
xclu
sion
/ B
ias
Stud
y C
oncl
usio
n fr
ompa
per
Com
men
ts f
rom
Rev
iew
er
Actigraphy Review Paper—Ancoli-Israel et alSLEEP, Vol. 26, No. 3, 2003 363
Loc
kley
(29
)
3C
AC
Tco
mpa
red
w/ o
ther
tech
-ni
ques
/ H
ome
/ Ent
ire
24-h
;m
ean
nigh
ts/s
ubje
ct=
23±
7(r
ange
6-3
5) o
f AC
T+
log
49 (
49)
/ 46.
6±12
.2 /
Blin
d lo
g; m
el; U
rine
sam
ples
/M
otio
n lo
gger
s or
MM
L/
wri
st /
1m /
NS
/ Act
ion
3;O
ther
: Zer
o cr
ossi
ng m
ode
log:
SO
L, S
On,
SO
ff, N
umaw
aken
ings
, dur
aw
aken
ings
,nu
m n
aps,
dur
nap
s; A
CT
:SO
L, S
On,
SO
ff, N
um a
wak
-en
ings
, dur
aw
aken
ings
, num
naps
, tot
al n
ap d
ur
Med
s in
flue
ncin
g sl
eep
orm
el /
NS
/ NS
AC
Tan
d lo
gs y
ield
ed s
imila
rre
sults
for
som
e as
pect
s of
slee
p bu
t not
oth
ers.
Prop
ortio
n of
pts
sho
win
g di
f-fe
renc
es b
etw
een
AC
Tan
dlo
g gr
eate
r th
an th
ose
show
-in
g no
dif
fere
nces
.
Uni
que
use:
to s
ee if
sle
ep(d
aytim
e na
p nu
m &
dur
&ni
ght s
leep
dur
) gr
eatly
alte
red
by C
R ty
pe (
norm
alen
trai
ned,
abn
orm
alen
trai
ned,
or
free
run
)
Mid
delk
oop
(40)
4C-a
Val
idat
ion
/ Hom
e / E
ntir
e24
-h; 4
5 h
AC
T10
(10
) / 2
4.1±
3.1
(19-
33)
/N
S L
og /
Gah
wile
r / b
oth
wri
sts
& b
oth
ankl
es &
trun
k at
nave
l / 5
sec
(m
in)
/ 0.1
g /
AC
TST
AR
1.0
; Oth
er: 0
.25-
3kg
log:
Tim
e to
bed
, lig
ht o
uttim
e, S
OL
, num
aw
aken
ings
,ri
se ti
me,
num
nap
s, n
ap d
ur;
AC
T: A
ctiv
ity le
vel,
epoc
hs>
,du
r of
epo
chs>
0
Rt b
ande
d, h
ealth
y, n
o m
eds
/N
S / N
S A
ctiv
ity r
ecor
ded
at w
rist
s >
ankl
es >
trun
k. M
otor
act
ivity
low
er a
t Nt c
ompa
rabl
y at
all
site
s bu
t sig
nifi
cant
ly m
ore
activ
ity o
f do
m w
rist
dur
ing
diur
nal p
erio
d, &
wri
st c
orre
-la
ted
mor
e w
/ tru
nk a
t Nt t
han
ankl
es; o
ppos
ite d
iurn
ally
.N
dom
wri
st a
ctiv
ity c
orre
late
sm
ore
w/ t
runk
act
ivity
than
does
dom
wri
st a
ctiv
ity;
Dur
ing
slee
p A
CT
reve
als
mor
e w
hole
bod
y, g
ener
aliz
edm
ovem
ent b
ut d
urin
g W
ther
ear
e m
ore
isol
ated
lim
b m
ove-
men
ts
Mid
delk
oop
(41)
4C-b
Val
idat
ion
/ Hom
e / 4
5 co
n-se
cutiv
e h
star
ting
at 1
2:00
;45
h A
CT
+lo
g
20 (
20)
/ 24.
1±3.
7 / N
orm
al
NS
/ GA
HW
ILE
R e
lect
roni
cC
H-8
634
Hom
brec
htik
on /
Lt
wri
st, R
t wri
st, L
t ank
le, R
tan
kle,
trun
k (n
avel
) / 5
sec
-on
ds /
NS
/ NS
AC
T: A
ctiv
ity le
vel
NS
/ NS
/ Hea
lthy
youn
gad
ults
onl
y W
rist
pla
cem
ents
det
ecte
dm
ore
activ
ity c
ount
s th
anan
kle
or tr
unk
plac
emen
ts.
dom
wri
st p
lace
men
t yie
lded
grea
ter
diur
nal a
ctiv
ity c
ount
sth
an n
dom
. All
site
s cl
earl
ysh
owed
cir
cadi
an s
leep
-Wdi
ffer
ence
s. S
ugge
sts
mor
est
udy
w/ p
lace
men
ts c
on-
com
itant
w/ P
SG
Wri
st p
lace
men
t sup
erio
r to
ankl
e or
trun
k. D
om w
rist
appe
ars
bette
r fo
r di
scri
min
at-
ing
leve
l of
wak
ing
activ
ity.
Min
ors
(45)
4C-b
Tech
niqu
e D
evel
opm
ent /
Hom
e / E
ntir
e 24
-h; 3
-26
24-
hper
iods
of A
CT
8 (8
) / G
rp1
49, G
rp2
(18-
20),
Grp
3 26
, Grp
3 (4
3-74
) /
Nor
mal
Grp
s 1&
2, C
R d
isor
-de
r, D
SPS
Grp
3; C
olor
ecta
lca
ncer
Grp
4
log
/ Gae
hwile
r / n
dom
wri
st /
6 m
ins
/ NS
/ NS
NS
NS
/ NS
/ Low
sam
ple
size
M
etho
d de
velo
ped
for
com
-pa
ring
leve
l of
activ
ity in
bed
vs. o
ut o
f be
d (=
”dic
hoto
my
indi
ces”
); H
ealth
y su
bjec
tssh
owed
gre
ater
dic
hoto
my
than
eith
er p
ts w
/ DSP
S or
colo
rect
al c
ance
r; M
ight
be
usef
ul te
chni
que
for
stud
y of
circ
adia
n ph
ase
shif
t (sh
ift-
wor
kers
, jet
lag)
& il
lnes
s
Min
ors
(96)
4C-a
Rep
eat m
easu
res,
2 c
ondi
tions
com
pare
d / H
ome
/ Ent
ire
24-
h; 2
Ds
rest
AC
T&
3 N
tsh
ifts
AC
T
8 (8
) / (
18-3
5) /
Nor
mal
lo
g / G
aehw
iler
/ ndo
m w
rist
/30
sec
/1 m
in /
NS
/ NS
AC
T: r
elat
ive
activ
ity le
vels
N
ight
shi
ft n
urse
/ N
S / N
S W
hen
data
is c
orre
cted
for
leng
th o
f sl
eep
D s
leep
has
grea
ter
activ
ity le
vels
than
nigh
t sle
ep; D
iffe
renc
ebe
twee
n W
activ
ity a
nd s
leep
activ
ity le
vels
tend
s to
be
less
duri
ng n
ight
wor
k sh
ifts
AC
Tca
n be
use
ful i
n st
udy-
ing
adju
stm
ent t
o sh
ift w
ork
Thi
s pa
per
is a
fur
ther
ana
ly-
sis
of d
ata
in a
n ea
rlie
r st
udy.
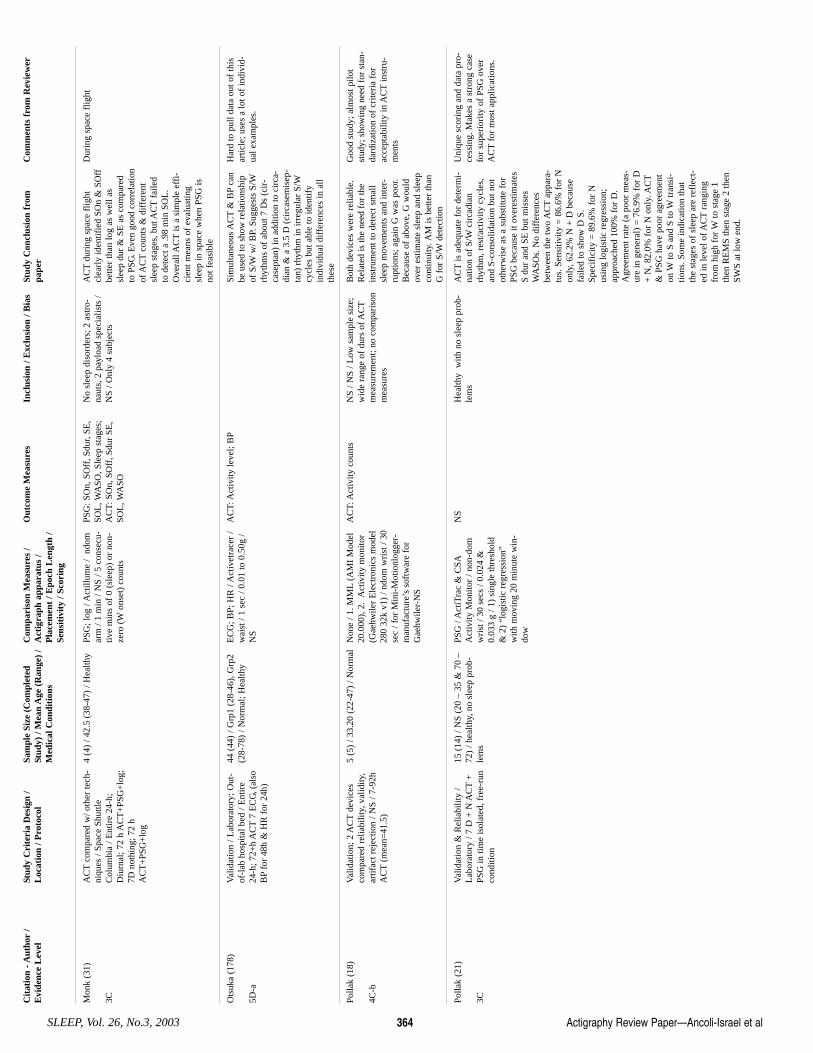
Cit
atio
n - A
utho
r/
Evi
denc
e L
evel
St
udy
Cri
teri
a D
esig
n /
Loc
atio
n / P
roto
col
Sam
ple
Size
(C
ompl
eted
Stud
y) /
Mea
n A
ge (
Ran
ge)
/M
edic
al C
ondi
tion
s
Com
pari
son
Mea
sure
s /
Act
igra
ph a
ppar
atus
/P
lace
men
t / E
poch
Len
gth
/Se
nsit
ivit
y / S
cori
ng
Out
com
e M
easu
res
Incl
usio
n / E
xclu
sion
/ B
ias
Stud
y C
oncl
usio
n fr
ompa
per
Com
men
ts f
rom
Rev
iew
er
Actigraphy Review Paper—Ancoli-Israel et alSLEEP, Vol. 26, No.3, 2003 364
Mon
k (3
1)
3C
AC
Tco
mpa
red
w/ o
ther
tech
-ni
ques
/ Sp
ace
Shut
tleC
olum
bia
/ Ent
ire
24-h
;D
iurn
al; 7
2 h
AC
T+
PSG
+lo
g;7D
not
hing
; 72
hA
CT
+PS
G+
log
4 (4
) / 4
2.5
(38-
47)
/ Hea
lthy
PSG
; log
/ A
ctill
ume
/ nd
omar
m /
1 m
in /
NS
/ 5 c
onse
cu-
tive
min
s of
0 (
slee
p) o
r no
n-ze
ro (
Won
set)
cou
nts
PSG
: SO
n, S
Off
, Sdu
r, SE
,SO
L, W
ASO
, Sle
ep s
tage
s;A
CT
: SO
n, S
Off
, Sdu
r SE
,SO
L, W
ASO
No
slee
p di
sord
ers;
2 a
stro
-na
uts,
2 p
aylo
ad s
peci
alis
ts /
NS
/ Onl
y 4
subj
ects
AC
Tdu
ring
spa
ce f
light
clea
rly
iden
tifie
d SO
n &
SO
ffbe
tter
than
log
as w
ell a
ssl
eep
dur
& S
E a
s co
mpa
red
to P
SG. E
ven
good
cor
rela
tion
of A
CT
coun
ts &
dif
fere
ntsl
eep
stag
es, b
ut A
CT
faile
dto
det
ect a
.98
min
SO
L.
Ove
rall
AC
Tis
a s
impl
e ef
fi-
cien
t mea
ns o
f ev
alua
ting
slee
p in
spa
ce w
hen
PSG
isno
t fea
sibl
e
Dur
ing
spac
e fl
ight
Ots
uka
(178
)
5D-a
Val
idat
ion
/ Lab
orat
ory;
Out
-of
-lab
hos
pita
l bed
/ E
ntir
e24
-h; 7
2+h
AC
T7
EC
G, (
also
BP
for
48h
& H
R f
or 2
4h)
44 (
44)
/ Grp
1 (2
8-46
), G
rp2
(28-
78)
/ Nor
mal
; Hea
lthy
EC
G; B
P; H
R /
Act
ivet
race
r /
wai
st /
1 se
c / 0
.01
to 0
.50g
/N
S
AC
T: A
ctiv
ity le
vel;
BP
Sim
ulta
neou
s A
CT
& B
Pca
nbe
use
d to
sho
w r
elat
ions
hip
of S
/Ww
/ BP.
Sug
gest
s S/
Wrh
ythm
s of
abo
ut 7
Ds
(cir
-ca
sept
an)
in a
dditi
on to
cir
ca-
dian
& a
3.5
D (
circ
asem
isep
-ta
n) r
hyth
m in
irre
gula
r S/
Wcy
cles
but
abl
e to
iden
tify
indi
vidu
al d
iffe
renc
es in
all
thes
e
Har
d to
pul
l dat
a ou
t of
this
artic
le; u
ses
a lo
t of
indi
vid-
ual e
xam
ples
.
Polla
k (1
8)
4C-b
Val
idat
ion;
2 A
CT
devi
ces
com
pare
d re
liabi
lity,
val
idity
,ar
tifac
t rej
ectio
n / N
S / 7
-92h
AC
T(m
ean=
41.5
)
5 (5
) / 3
3.20
(22
-47)
/ N
orm
al
Non
e / 1
. MM
L(A
MI
Mod
el20
.000
), 2
. A
ctiv
ity m
onito
r(G
aehw
iler
Ele
ctro
nics
mod
el28
0 32
k v1
) / n
dom
wri
st /
30se
c / f
or M
ini-
Mot
ionl
ogge
r-m
anuf
actu
re’s
sof
twar
e fo
rG
aehw
iler-
NS
AC
T: A
ctiv
ity c
ount
s N
S / N
S / L
ow s
ampl
e si
ze;
wid
e ra
nge
of d
urs
of A
CT
mea
sure
men
t; no
com
pari
son
mea
sure
s
Bot
h de
vice
s w
ere
relia
ble.
Rel
ated
is th
e ne
ed f
or th
ein
stru
men
t to
dete
ct s
mal
lsl
eep
mov
emen
ts a
nd in
ter-
rupt
ions
; aga
in G
was
poo
r.B
ecau
se o
f ab
ove,
G w
ould
over
est
imat
e sl
eep
and
slee
pco
ntin
uity
. AM
is b
ette
r th
anG
for
S/W
dete
ctio
n
Goo
d st
udy;
alm
ost p
ilot
stud
y; s
how
ing
need
for
sta
n-da
rdiz
atio
n of
cri
teri
a fo
rac
cept
abili
ty in
AC
Tin
stru
-m
ents
Polla
k (2
1)
3C
Val
idat
ion
& R
elia
bilit
y /
Lab
orat
ory
/ 7 D
+ N
AC
T+
PSG
in ti
me
isol
ated
, fre
e-ru
nco
nditi
on
15 (
14)
/ NS
(20
– 35
& 7
0 –
72)
/ hea
lthy,
no
slee
p pr
ob-
lem
s
PSG
/ A
ctiT
rac
& C
SAA
ctiv
ity M
onito
r / n
on-d
omw
rist
/ 30
sec
s / 0
.024
&0.
033
g / 1
) si
ngle
thre
shol
d&
2)
“log
istic
reg
ress
ion”
with
mov
ing
20 m
inut
e w
in-
dow
NS
Hea
lthy
with
no
slee
p pr
ob-
lem
s A
CT
is a
dequ
ate
for
dete
rmi-
natio
n of
S/W
circ
adia
nrh
ythm
, res
t/act
ivity
cyc
les,
and
S-co
nsol
idat
ion
but n
otot
herw
ise
as a
sub
stitu
te f
orPS
G b
ecau
se it
ove
rest
imat
esS
dur
and
SE b
ut m
isse
sW
ASO
s. N
o di
ffer
ence
sbe
twee
n th
e tw
o A
CT
appa
ra-
tus.
Sen
sitiv
ity =
86.
6% f
or N
only
, 62.
2% N
+ D
bec
ause
faile
d to
sho
w D
S.
Spec
ific
ity =
89.
6% f
or N
usin
g lo
gist
ic r
egre
ssio
n;ap
proa
ched
100
% f
or D
.A
gree
men
t rat
e (a
poo
r m
eas-
ure
in g
ener
al)
= 7
6.9%
for
D+
N, 8
2.0%
for
N o
nly.
AC
T&
PSG
hav
e po
or a
gree
men
ton
Wto
S a
nd S
to W
tran
si-
tions
. Som
e in
dica
tion
that
the
stag
es o
f sl
eep
are
refl
ect-
ed in
leve
l of A
CT
rang
ing
from
hig
h fo
r W
to s
tage
1th
en R
EM
S th
en s
tage
2 th
enSW
S at
low
end
.
Uni
que
scor
ing
and
data
pro
-ce
ssin
g. M
akes
a s
tron
g ca
sefo
r su
peri
ority
of
PSG
ove
rA
CT
for
mos
t app
licat
ions
.
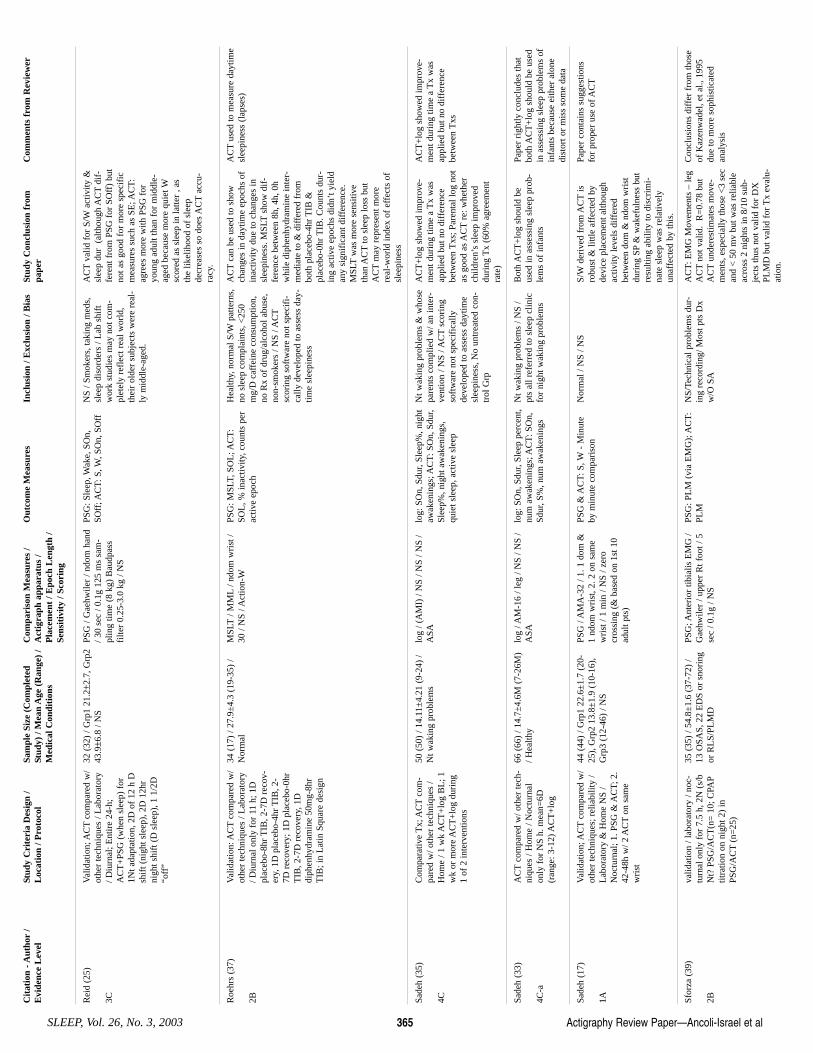
Cit
atio
n - A
utho
r/
Evi
denc
e L
evel
St
udy
Cri
teri
a D
esig
n /
Loc
atio
n / P
roto
col
Sam
ple
Size
(C
ompl
eted
Stud
y) /
Mea
n A
ge (
Ran
ge)
/M
edic
al C
ondi
tion
s
Com
pari
son
Mea
sure
s /
Act
igra
ph a
ppar
atus
/P
lace
men
t / E
poch
Len
gth
/Se
nsit
ivit
y / S
cori
ng
Out
com
e M
easu
res
Incl
usio
n / E
xclu
sion
/ B
ias
Stud
y C
oncl
usio
n fr
ompa
per
Com
men
ts f
rom
Rev
iew
er
Actigraphy Review Paper—Ancoli-Israel et alSLEEP, Vol. 26, No. 3, 2003 365
Rei
d (2
5)
3C
Val
idat
ion;
AC
Tco
mpa
red
w/
othe
r te
chni
ques
/ L
abor
ator
y/ D
iurn
al; E
ntir
e 24
-h;
AC
T+
PSG
(w
hen
slee
p) f
or1N
t ada
ptat
ion,
2D
of
12 h
Dsh
ift (
nigh
t sle
ep),
2D
12h
rni
ght s
hift
(D
sle
ep),
1 1
/2D
“off
”
32 (
32)
/ Grp
1 21
.2±2
.7, G
rp2
43.9±6
.8 /
NS
PSG
/ G
aehw
iler
/ ndo
m h
and
/ 30
sec
/ 0.1
g 12
5 m
s sa
m-
plin
g tim
e (8
kg)
Bau
dpas
sfi
lter
0.25
-3.0
kg
/ NS
PSG
: Sle
ep, W
ake,
SO
n,SO
ff; A
CT
: S, W
, SO
n, S
Off
N
S / S
mok
ers,
taki
ng m
eds,
slee
p di
sord
ers
/ Lab
shi
ftw
ork
stud
ies
may
not
com
-pl
etel
y re
flec
t rea
l wor
ld,
thei
r ol
der
subj
ects
wer
e re
al-
ly m
iddl
e-ag
ed.
AC
Tva
lid f
or S
/Wac
tivity
&sl
eep
dur
(al
thou
gh A
CT
dif-
fere
nt f
rom
PSG
for
SO
ff)
but
not a
s go
od f
or m
ore
spec
ific
mea
sure
s su
ch a
s SE
; AC
T:
agre
es m
ore
with
PSG
for
youn
g ad
ult t
han
for
mid
dle-
aged
bec
ause
mor
e qu
iet W
scor
ed a
s sl
eep
in la
tter
, as
the
likel
ihoo
d of
sle
epde
crea
ses
so d
oes
AC
Tac
cu-
racy
.
Roe
hrs
(37)
2B
Val
idat
ion:
AC
Tco
mpa
red
w/
othe
r te
chni
ques
/ L
abor
ator
y/ D
iurn
al o
nly
for
11 h
; 1D
plac
ebo-
8hr
TIB
, 2-7
D r
ecov
-er
y, 1
D p
lace
bo-4
hr T
IB, 2
-7D
rec
over
y; 1
D p
lace
bo-0
hrT
IB, 2
-7D
rec
over
y, 1
Ddi
phen
hydr
amin
e 50
mg-
8hr
TIB
; in
Lat
in S
quar
e de
sign
34 (
17)
/ 27.
9±4.
3 (1
9-35
) /
Nor
mal
M
SLT
/ MM
L/ n
dom
wri
st /
30 /
NS
/ Act
ion-
WPS
G: M
SLT,
SO
L; A
CT
:SO
L, %
inac
tivity
, cou
nts
per
activ
e ep
och
Hea
lthy,
nor
mal
S/W
patte
rns,
no s
leep
com
plai
nts,
<25
0m
g/D
caf
fein
e co
nsum
ptio
n,no
Rx
of d
rug/
alco
hol a
buse
,no
n-sm
oker
s / N
S / A
CT
scor
ing
soft
war
e no
t spe
cifi
-ca
lly d
evel
oped
to a
sses
s da
y-tim
e sl
eepi
ness
AC
Tca
n be
use
d to
sho
wch
ange
s in
day
time
epoc
hs o
fin
activ
ity d
ue to
cha
nges
insl
eepi
ness
. MSL
Tsh
ow d
if-
fere
nce
betw
een
8h, 4
h, 0
hw
hile
dip
henh
ydra
min
e in
ter-
med
iate
to &
dif
fere
d fr
ombo
th p
lace
bo-4
hr T
IB &
plac
ebo-
0hr
TIB
. Cou
nts
dur-
ing
activ
e ep
ochs
did
n’t y
ield
any
sign
ific
ant d
iffe
renc
e.M
SLT
was
mor
e se
nsiti
veth
an A
CT
to s
leep
loss
but
AC
Tm
ay r
epre
sent
mor
ere
al-w
orld
inde
x of
eff
ects
of
slee
pine
ss
AC
Tus
ed to
mea
sure
day
time
slee
pine
ss (
laps
es)
Sade
h (3
5)
4C
Com
para
tive
Tx;
AC
Tco
m-
pare
d w
/ oth
er te
chni
ques
/H
ome
/ 1 w
k A
CT
+lo
g B
L; 1
wk
or m
ore
AC
T+
log
duri
ng1
of 2
inte
rven
tions
50 (
50)
/ 14.
11±
4.21
(9-
24)
/N
t wak
ing
prob
lem
s lo
g / (
AM
I) /
NS
/ NS
/ NS
/A
SAlo
g: S
On,
Sdu
r, Sl
eep%
, nig
htaw
aken
ings
; AC
T: S
On,
Sdu
r,Sl
eep%
, nig
ht a
wak
enin
gs,
quie
t sle
ep, a
ctiv
e sl
eep
Nt w
akin
g pr
oble
ms
& w
hose
pare
nts
com
plie
d w
/ an
inte
r-ve
ntio
n / N
S / A
CT
scor
ing
soft
war
e no
t spe
cifi
cally
deve
lope
d to
ass
ess
dayt
ime
slee
pine
ss, N
o un
trea
ted
con-
trol
Grp
AC
T+
log
show
ed im
prov
e-m
ent d
urin
g tim
e a
Tx
was
appl
ied
but n
o di
ffer
ence
betw
een
Txs
; Par
enta
l log
not
as g
ood
as A
CT
re: w
heth
erch
ildre
n’s
slee
p im
prov
eddu
ring
Tx
(60%
agr
eem
ent
rate
)
AC
T+
log
show
ed im
prov
e-m
ent d
urin
g tim
e a
Tx
was
appl
ied
but n
o di
ffer
ence
betw
een
Txs
Sade
h (3
3)
4C-a
AC
Tco
mpa
red
w/ o
ther
tech
-ni
ques
/ H
ome
/ Noc
turn
alon
ly f
or N
S h.
mea
n=6D
(ran
ge: 3
-12)
AC
T+
log
66 (
66)
/ 14.
7±4.
6M (
7-26
M)
/ Hea
lthy
log
/ AM
-16
/ leg
/ N
S / N
S /
ASA
log:
SO
n, S
dur,
Slee
p pe
rcen
t,nu
m a
wak
enin
gs; A
CT
: SO
n,Sd
ur, S
%, n
um a
wak
enin
gs
Nt w
akin
g pr
oble
ms
/ NS
/pt
s al
l ref
erre
d to
sle
ep c
linic
for
nigh
t wak
ing
prob
lem
s
Bot
h A
CT
+lo
g sh
ould
be
used
in a
sses
sing
sle
ep p
rob-
lem
s of
infa
nts
Pape
r ri
ghtly
con
clud
es th
atbo
th A
CT
+lo
g sh
ould
be
used
in a
sses
sing
sle
ep p
robl
ems
ofin
fant
s be
caus
e ei
ther
alo
nedi
stor
t or
mis
s so
me
data
Sade
h (1
7)
1A
Val
idat
ion;
AC
Tco
mpa
red
w/
othe
r te
chni
ques
; rel
iabi
lity
/L
abor
ator
y &
Hom
e N
S /
Noc
turn
al; 1
. PSG
& A
CT;
2.
42-4
8h w
/ 2 A
CT
on s
ame
wri
st
44 (
44)
/ Grp
1 22
.6±
1.7
(20-
25),
Grp
2 13
.8±
1.9
(10-
16),
Grp
3 (1
2-46
) / N
S
PSG
/ A
MA
-32
/ 1. 1
dom
&1
ndom
wri
st, 2
. 2 o
n sa
me
wri
st /
1 m
in /
NS
/ zer
ocr
ossi
ng (
& b
ased
on
1st 1
0ad
ult p
ts)
PSG
& A
CT
: S, W
- M
inut
eby
min
ute
com
pari
son
Nor
mal
/ N
S / N
S S/
Wde
rive
d fr
om A
CT
isro
bust
& li
ttle
affe
cted
by
devi
ce p
lace
men
t alth
ough
activ
ity le
vels
dif
fere
dbe
twee
n do
m &
ndo
m w
rist
duri
ng S
P&
wak
eful
ness
but
resu
lting
abi
lity
to d
iscr
imi-
nate
sle
ep w
as r
elat
ivel
yun
affe
cted
by
this
.
Pape
r co
ntai
ns s
ugge
stio
nsfo
r pr
oper
use
of A
CT
Sfor
za (
39)
2B
valid
atio
n / l
abor
ator
y / n
oc-
turn
al o
nly
for
7.5
h, 2
N (
s/b
Nt?
PSG
/AC
T(n
= 1
0; C
PAP
titra
tion
on n
ight
2)
inPS
G/A
CT
(n=
25)
35 (
35)
/ 54.
8±1.
6 (3
7-72
) /
13 O
SAS,
22
ED
S or
sno
ring
or R
LS/
PLM
D
PSG
; Ant
erio
r tib
ialis
EM
G /
Gae
hwile
r / u
pper
Rt f
oot /
5se
c / 0
.1g
/ NS
PSG
: PL
M (
via
EM
G);
AC
T:
PLM
NS/
Tech
nica
l pro
blem
s du
r-in
g re
cord
ing/
Mos
t pts
Dx
w/O
SA
AC
T: E
MG
Mov
emen
ts –
leg
AC
Tno
t val
id.
R=
0.78
but
AC
Tun
dere
stim
ates
mov
e-m
ents
, esp
ecia
lly th
ose
<3
sec
and
< 5
0 m
v bu
t was
rel
iabl
eac
ross
2 n
ight
s in
8/1
0 su
b-je
cts
thus
not
val
id f
or D
XPL
MD
but
val
id f
or T
x ev
alu-
atio
n.
Con
clus
ions
dif
fer
from
thos
eof
Kaz
enw
adel
, et a
l., 1
995
due
to m
ore
soph
istic
ated
anal
ysis
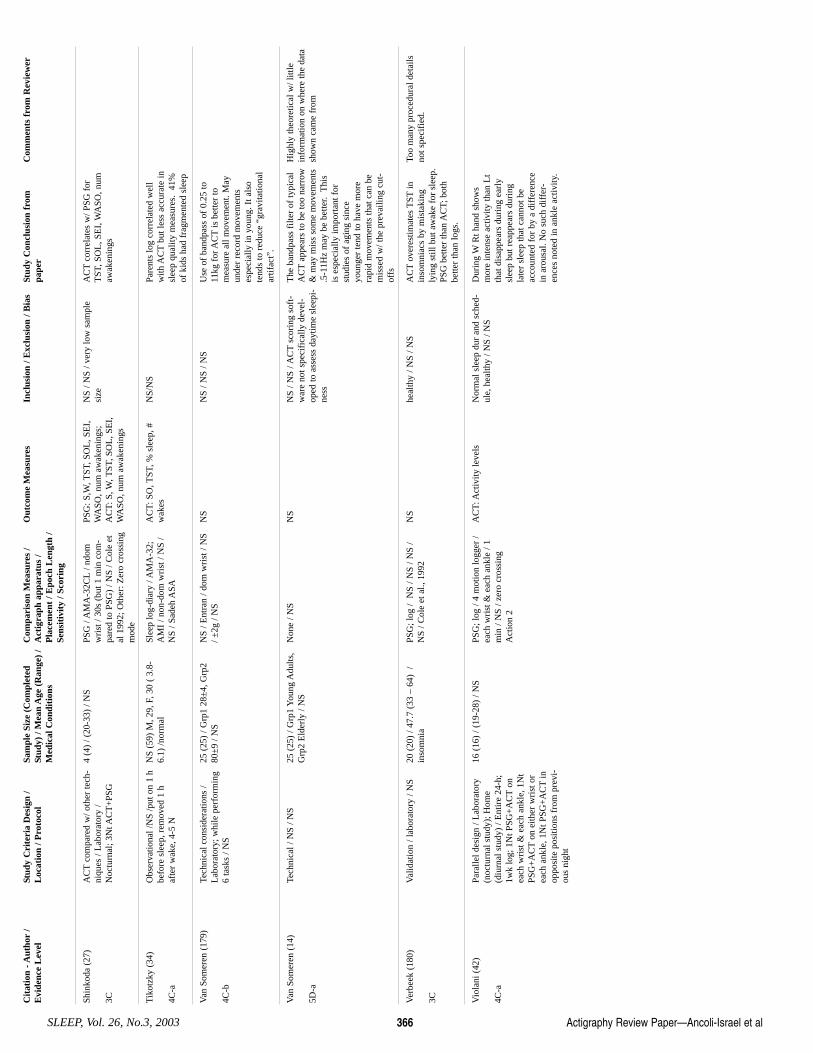
Cit
atio
n - A
utho
r/
Evi
denc
e L
evel
St
udy
Cri
teri
a D
esig
n /
Loc
atio
n / P
roto
col
Sam
ple
Size
(C
ompl
eted
Stud
y) /
Mea
n A
ge (
Ran
ge)
/M
edic
al C
ondi
tion
s
Com
pari
son
Mea
sure
s /
Act
igra
ph a
ppar
atus
/P
lace
men
t / E
poch
Len
gth
/Se
nsit
ivit
y / S
cori
ng
Out
com
e M
easu
res
Incl
usio
n / E
xclu
sion
/ B
ias
Stud
y C
oncl
usio
n fr
ompa
per
Com
men
ts f
rom
Rev
iew
er
Actigraphy Review Paper—Ancoli-Israel et alSLEEP, Vol. 26, No.3, 2003 366
Shin
koda
(27
)
3C
AC
Tco
mpa
red
w/ o
ther
tech
-ni
ques
/ L
abor
ator
y /
Noc
turn
al; 3
Nt A
CT
+PS
G
4 (4
) / (
20-3
3) /
NS
PSG
/ A
MA
-32C
L/ n
dom
wri
st /
30s
(but
1 m
in c
om-
pare
d to
PSG
) / N
S / C
ole
etal
199
2; O
ther
: Zer
o cr
ossi
ngm
ode
PSG
: S,W
, TST
, SO
L, S
EI,
WA
SO, n
um a
wak
enin
gs;
AC
T: S
, W, T
ST, S
OL
, SE
I,W
ASO
, num
aw
aken
ings
NS
/ NS
/ ver
y lo
w s
ampl
esi
ze
AC
Tco
rrel
ates
w/ P
SG f
orT
ST, S
OL
, SE
I, W
ASO
, num
awak
enin
gs
Tik
otzk
y (3
4)
4C-a
Obs
erva
tiona
l /N
S /p
ut o
n 1
hbe
fore
sle
ep, r
emov
ed 1
haf
ter
wak
e, 4
-5 N
NS
(59)
M, 2
9, F
, 30
( 3.
8-6.
1) /n
orm
al
Slee
p lo
g-di
ary
/ AM
A-3
2;A
MI
/ non
-dom
wri
st /
NS
/N
S / S
adeh
ASA
AC
T: S
O, T
ST, %
sle
ep, #
wak
es
NS/
NS
Pare
nts
log
corr
elat
ed w
ell
with
AC
Tbu
t les
s ac
cura
te in
slee
p qu
ality
mea
sure
s. 4
1%of
kid
s ha
d fr
agm
ente
d sl
eep
Van
Som
eren
(17
9)
4C-b
Tech
nica
l con
side
ratio
ns /
Lab
orat
ory;
whi
le p
erfo
rmin
g6
task
s / N
S
25 (
25)
/ Grp
1 28
±4,
Grp
280
±9
/ NS
NS
/ Ent
ran
/ dom
wri
st /
NS
/ ±2g
/ N
S N
S N
S / N
S / N
S U
se o
f ba
ndpa
ss o
f 0.
25 to
11kg
for
AC
Tis
bet
ter
tom
easu
re a
ll m
ovem
ent.
May
unde
r re
cord
mov
emen
tses
peci
ally
in y
oung
. It a
lso
tend
s to
red
uce
“gra
vita
tiona
lar
tifac
t”.
Van
Som
eren
(14
)
5D-a
Tech
nica
l / N
S / N
S 25
(25
) / G
rp1
You
ng A
dults
,G
rp2
Eld
erly
/ N
S N
one
/ NS
NS
NS
/ NS
/ AC
Tsc
orin
g so
ft-
war
e no
t spe
cifi
cally
dev
el-
oped
to a
sses
s da
ytim
e sl
eepi
-ne
ss
The
ban
dpas
s fi
lter
of ty
pica
lA
CT
appe
ars
to b
e to
o na
rrow
& m
ay m
iss
som
e m
ovem
ents
.5-1
1Hz
may
be
bette
r. T
his
is e
spec
ially
impo
rtan
t for
stud
ies
of a
ging
sin
ceyo
unge
r te
nd to
hav
e m
ore
rapi
d m
ovem
ents
that
can
be
mis
sed
w/ t
he p
reva
iling
cut
-of
fs
Hig
hly
theo
retic
al w
/ litt
lein
form
atio
n on
whe
re th
e da
tash
own
cam
e fr
om
Ver
beek
(18
0)
3C
Val
idat
ion
/ lab
orat
ory
/ NS
20 (
20)
/ 47.
7 (3
3 –
64)
/in
som
nia
PSG
; log
/ N
S / N
S / N
S /
NS
/ Col
e et
al.,
199
2 N
S he
alth
y / N
S / N
S A
CT
over
estim
ates
TST
inin
som
niac
s by
mis
taki
ngly
ing
still
but
aw
ake
for
slee
p.PS
G b
ette
r th
an A
CT;
bot
hbe
tter
than
logs
.
Too
man
y pr
oced
ural
det
ails
not s
peci
fied
.
Vio
lani
(42
)
4C-a
Para
llel d
esig
n / L
abor
ator
y(n
octu
rnal
stu
dy);
Hom
e(d
iurn
al s
tudy
) / E
ntir
e 24
-h;
1wk
log;
1N
t PSG
+A
CT
onea
ch w
rist
& e
ach
ankl
e, 1
Nt
PSG
+A
CT
on e
ither
wri
st o
rea
ch a
nkle
, 1N
t PSG
+A
CT
inop
posi
te p
ositi
ons
from
pre
vi-
ous
nigh
t
16 (
16)
/ (19
-28)
/ N
S PS
G; l
og /
4 m
otio
n lo
gger
/ea
ch w
rist
& e
ach
ankl
e / 1
min
/ N
S / z
ero
cros
sing
Act
ion
2
AC
T: A
ctiv
ity le
vels
N
orm
al s
leep
dur
and
sch
ed-
ule,
hea
lthy
/ NS
/ NS
Dur
ing
WR
t han
d sh
ows
mor
e in
tens
e ac
tivity
than
Lt
that
dis
appe
ars
duri
ng e
arly
slee
p bu
t rea
ppea
rs d
urin
gla
ter
slee
p th
at c
anno
t be
acco
unte
d fo
r by
a d
iffe
renc
ein
aro
usal
. No
such
dif
fer-
ence
s no
ted
in a
nkle
act
ivity
.
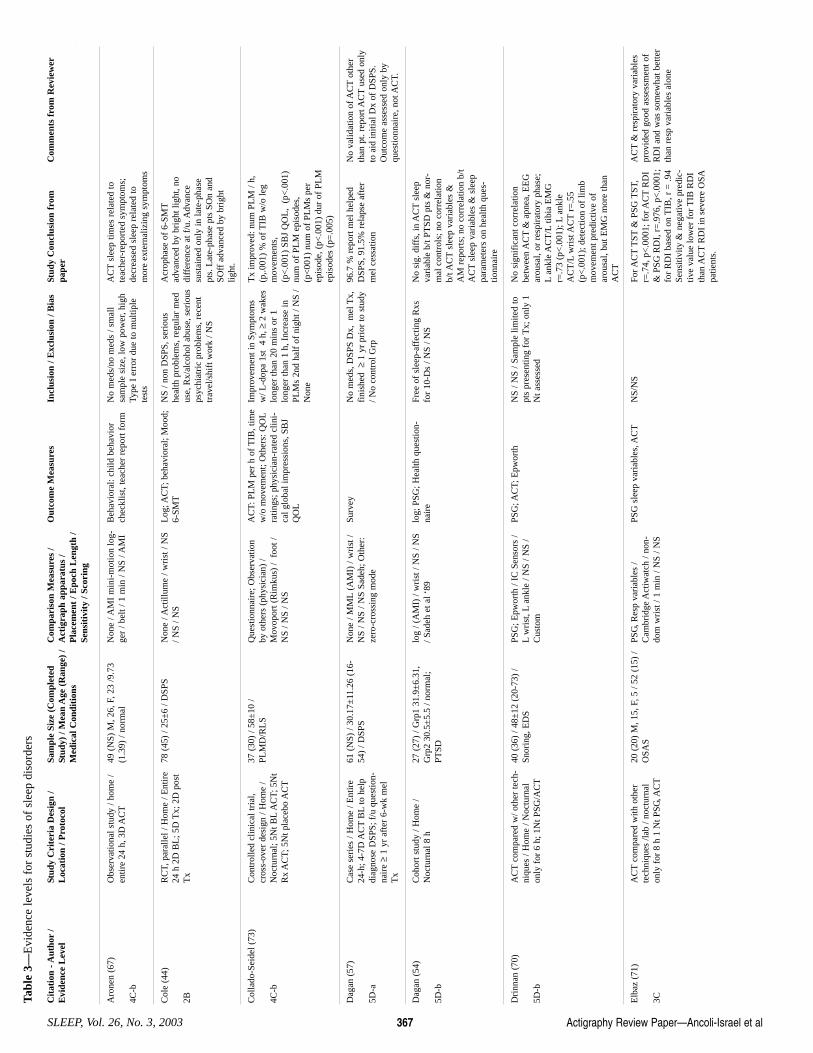
Actigraphy Review Paper—Ancoli-Israel et alSLEEP, Vol. 26, No. 3, 2003 367
Aro
nen
(67)
4C-b
Obs
erva
tiona
l stu
dy /
hom
e /
entir
e 24
h, 3
D A
CT
49 (
NS)
M, 2
6, F
, 23
/9.7
3(1
.39)
/ no
rmal
N
one
/ AM
I m
ini-
mot
ion
log-
ger
/ bel
t / 1
min
/ N
S / A
MI
Beh
avio
ral:
child
beh
avio
rch
eckl
ist,
teac
her
repo
rt f
orm
N
o m
eds/
no m
eds
/ sm
all
sam
ple
size
, low
pow
er, h
igh
Type
I e
rror
due
to m
ultip
lete
sts
AC
Tsl
eep
times
rel
ated
tote
ache
r-re
port
ed s
ympt
oms;
decr
ease
d sl
eep
rela
ted
tom
ore
exte
rnal
izin
g sy
mpt
oms
Cit
atio
n - A
utho
r/
Evi
denc
e L
evel
St
udy
Cri
teri
a D
esig
n /
Loc
atio
n / P
roto
col
Sam
ple
Size
(C
ompl
eted
Stud
y) /
Mea
n A
ge (
Ran
ge)
/M
edic
al C
ondi
tion
s
Com
pari
son
Mea
sure
s /
Act
igra
ph a
ppar
atus
/P
lace
men
t / E
poch
Len
gth
/Se
nsit
ivit
y / S
cori
ng
Out
com
e M
easu
res
Incl
usio
n / E
xclu
sion
/ B
ias
Stud
y C
oncl
usio
n fr
ompa
per
Com
men
ts f
rom
Rev
iew
er
Tabl
e 3—
Evi
denc
e le
vels
for
stu
dies
of
slee
p di
sord
ers
Col
e (4
4)
2B
RC
T, p
aral
lel /
Hom
e / E
ntir
e24
h 2
D B
L; 5
D T
x; 2
D p
ost
Tx
78 (
45)
/ 25±
6 / D
SPS
N
one
/ Act
illum
e / w
rist
/ N
S/ N
S / N
S
Log
; AC
T; b
ehav
iora
l; M
ood;
6-SM
TN
S / n
on D
SPS,
ser
ious
heal
th p
robl
ems,
reg
ular
med
use,
Rx/
alco
hol a
buse
, ser
ious
psyc
hiat
ric
prob
lem
s, r
ecen
ttr
avel
/shi
ft w
ork
/ NS
Acr
opha
se o
f 6-
SMT
adva
nced
by
brig
ht li
ght,
nodi
ffer
ence
at f
/u. A
dvan
cesu
stai
ned
only
in la
te-p
hase
pts.
Lat
e-ph
ase
pts
SOn
and
SOff
adv
ance
d by
bri
ght
light
.
Col
lado
-Sei
del (
73)
4C-b
Con
trol
led
clin
ical
tria
l,cr
oss-
over
des
ign
/ Hom
e /
Noc
turn
al; 5
Nt B
LA
CT;
5N
tR
x A
CT;
5N
t pla
cebo
AC
T
37 (
30)
/ 58±
10 /
PLM
D/R
LS
Que
stio
nnai
re; O
bser
vatio
nby
oth
ers
(phy
sici
an)
/M
ovop
ort (
Rim
kus)
/ f
oot /
NS
/ NS
/ NS
AC
T: P
LM
per
h o
f T
IB, t
ime
w/o
mov
emen
t; O
ther
s: Q
OL
ratin
gs; p
hysi
cian
-rat
ed c
lini-
cal g
loba
l im
pres
sion
s, S
BJ
QO
L
Impr
ovem
ent i
n Sy
mpt
oms
w/ L
-dop
a 1s
t 4
h, ≥
2 w
akes
long
er th
an 2
0 m
ins
or 1
long
er th
an 1
h, I
ncre
ase
inPL
Ms
2nd
half
of
nigh
t / N
S /
Non
e
Tx
impr
oved
: num
PL
M /
h,(p
,.001
) %
of
TIB
w/o
leg
mov
emen
ts,
(p<
.001
) SB
J Q
OL
, (p
<.0
01)
num
of
PLM
epi
sode
s,(p
<00
1) n
um o
f PL
Ms
per
epis
ode,
(p<
.001
) du
r of
PL
Mep
isod
es (
p=.0
05)
Dag
an (
57)
5D-a
Cas
e se
ries
/ H
ome
/ Ent
ire
24-h
; 4-7
D A
CT
BL
to h
elp
diag
nose
DSP
S; f
/u q
uest
ion-
nair
e ≥
1 yr
aft
er 6
-wk
mel
Tx
61 (
NS)
/ 30
.17±
11.2
6 (1
6-54
) / D
SPS
Non
e / M
ML
(AM
I) /
wri
st /
NS
/ NS
/ NS
Sade
h; O
ther
:ze
ro-c
ross
ing
mod
e
Surv
ey
No
med
s, D
SPS
Dx,
mel
Tx,
fini
shed
≥1
yr p
rior
to s
tudy
/ No
cont
rol G
rp
96.7
% r
epor
t mel
hel
ped
DSP
S, 9
1.5%
rel
apse
aft
erm
el c
essa
tion
No
valid
atio
n of
AC
Tot
her
than
pt.
repo
rt A
CT
used
onl
yto
aid
initi
al D
x of
DSP
S.O
utco
me
asse
ssed
onl
y by
ques
tionn
aire
, not
AC
T.
Dag
an (
54)
5D-b
Coh
ort s
tudy
/ H
ome
/N
octu
rnal
8 h
27
(27
) / G
rp1
31.9
±6.
31,
Grp
2 30
.5±
5.5
/ nor
mal
;PT
SD
log
/ (A
MI)
/ w
rist
/ N
S / N
S/ S
adeh
et a
l ‘89
lo
g; P
SG; H
ealth
que
stio
n-na
ire
Free
of
slee
p-af
fect
ing
Rxs
for
10-D
s / N
S / N
S N
o si
g. d
iffs
, in
AC
Tsl
eep
vari
able
b/t
PTSD
pts
& n
or-
mal
con
trol
s; n
o co
rrel
atio
nb/
t AC
Tsl
eep
vari
able
s &
AM
rep
orts
; no
corr
elat
ion
b/t
AC
Tsl
eep
vari
able
s &
sle
eppa
ram
eter
s on
hea
lth q
ues-
tionn
aire
Dri
nnan
(70
)
5D-b
AC
Tco
mpa
red
w/ o
ther
tech
-ni
ques
/ H
ome
/ Noc
turn
alon
ly f
or 6
h; 1
Nt P
SG/A
CT
40 (
36)
/ 48±
12 (
20-7
3) /
Snor
ing,
ED
S PS
G; E
pwor
th /
IC S
enso
rs /
Lw
rist
, Lan
kle
/ NS
/ NS
/C
usto
m
PSG
; AC
T; E
pwor
th
NS
/ NS
/ Sam
ple
limite
d to
pts
pres
entin
g fo
r T
x; o
nly
1N
t ass
esse
d
No
sign
ific
ant c
orre
latio
nbe
twee
n A
CT
& a
pnea
, EE
Gar
ousa
l, or
res
pira
tory
pha
se;
Lan
kle
AC
T/L
tibia
EM
Gr=
.73
(p<
.001
); L
ankl
eA
CT
/Lw
rist
AC
Tr=
.55
(p<
.001
); d
etec
tion
of li
mb
mov
emen
t pre
dict
ive
ofar
ousa
l, bu
t EM
G m
ore
than
AC
T
Elb
az (
71)
3C
AC
Tco
mpa
red
with
oth
erte
chni
ques
/lab
/ no
ctur
nal
only
for
8 h
1 N
t PSG
, AC
T
20 (
20)
M, 1
5, F
, 5 /
52 (
15)
/O
SAS
PSG
, Res
p va
riab
les
/C
ambr
idge
Act
iwat
ch /
non-
dom
wri
st /
1 m
in /
NS
/ NS
PSG
sle
ep v
aria
bles
, AC
TN
S/N
S Fo
r AC
TT
ST&
PSG
TST
,r=
.74,
p<
.000
1; f
or A
CT
RD
I&
PSG
RD
I, r
=.9
76, p
<.0
001;
for
RD
I ba
sed
on T
IB, r
= .9
4Se
nsiti
vity
& n
egat
ive
pred
ic-
tive
valu
e lo
wer
for
TIB
RD
Ith
an A
CT
RD
I in
sev
ere
OSA
patie
nts.
AC
T&
res
pira
tory
var
iabl
espr
ovid
ed g
ood
asse
ssm
ent o
fR
DI
and
was
som
ewha
t bet
ter
than
res
p va
riab
les
alon
e
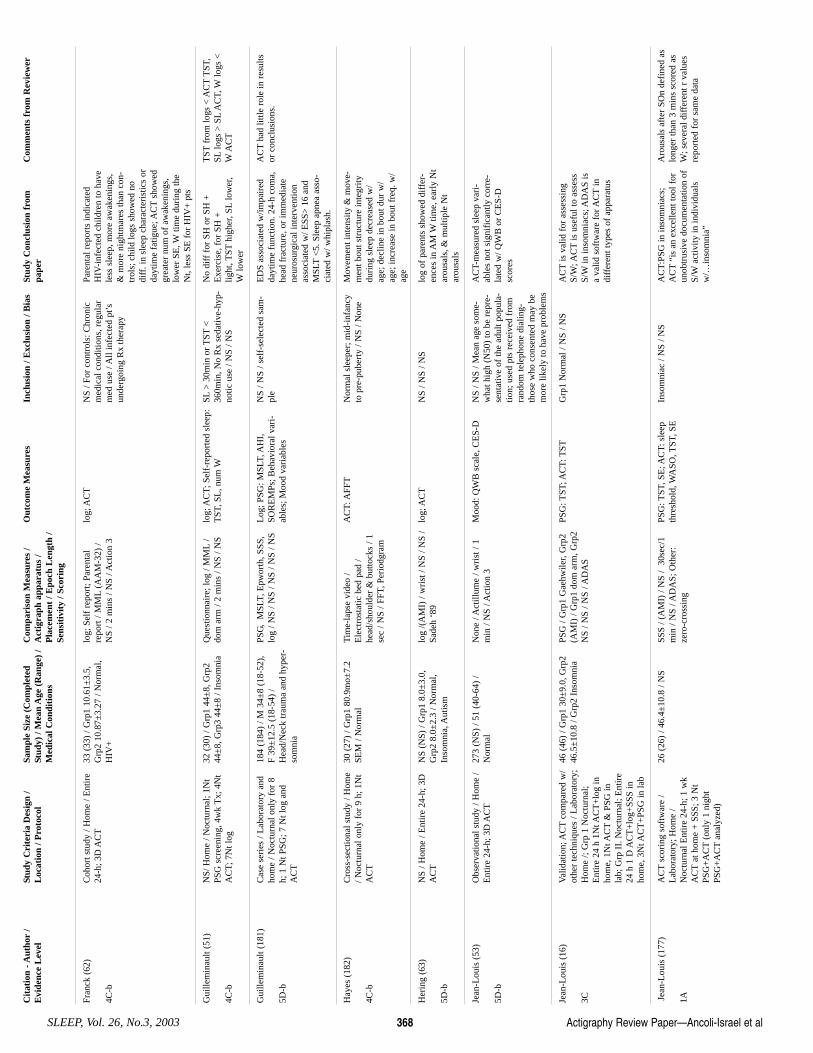
Cit
atio
n - A
utho
r/
Evi
denc
e L
evel
St
udy
Cri
teri
a D
esig
n /
Loc
atio
n / P
roto
col
Sam
ple
Size
(C
ompl
eted
Stud
y) /
Mea
n A
ge (
Ran
ge)
/M
edic
al C
ondi
tion
s
Com
pari
son
Mea
sure
s /
Act
igra
ph a
ppar
atus
/P
lace
men
t / E
poch
Len
gth
/Se
nsit
ivit
y / S
cori
ng
Out
com
e M
easu
res
Incl
usio
n / E
xclu
sion
/ B
ias
Stud
y C
oncl
usio
n fr
ompa
per
Com
men
ts f
rom
Rev
iew
er
Actigraphy Review Paper—Ancoli-Israel et alSLEEP, Vol. 26, No.3, 2003 368
Fran
ck (
62)
4C-b
Coh
ort s
tudy
/ H
ome
/ Ent
ire
24-h
; 3D
AC
T33
(33
) / G
rp1
10.6
1±3.
5,G
rp2
10.8
7±3.
27 /
Nor
mal
,H
IV+
log;
Sel
f re
port
; Par
enta
lre
port
/ M
ML
(AA
M-3
2) /
NS
/ 2 m
ins
/ NS
/ Act
ion
3
log;
AC
TN
S / F
or c
ontr
ols:
Chr
onic
med
ical
con
ditio
ns, r
egul
arm
ed u
se /
All
infe
cted
pt’s
unde
rgoi
ng R
x th
erap
y
Pare
ntal
rep
orts
indi
cate
dH
IV-i
nfec
ted
child
ren
to h
ave
less
sle
ep, m
ore
awak
enin
gs,
& m
ore
nigh
tmar
es th
an c
on-
trol
s; c
hild
logs
sho
wed
no
diff
. in
slee
p ch
arac
teri
stic
s or
dayt
ime
fatig
ue; A
CT
show
edgr
eate
r nu
m o
f aw
aken
ings
,lo
wer
SE
, Wtim
e du
ring
the
Nt,
less
SE
for
HIV
+ p
ts
Gui
llem
inau
lt (5
1)
4C-b
NS/
Hom
e / N
octu
rnal
; 1N
tPS
G s
cree
ning
, 4w
k T
x; 4
Nt
AC
T; 7
Nt l
og
32 (
30)
/ Grp
1 44
±8,
Grp
244
±8,
Grp
3 44
±8
/ Ins
omni
a Q
uest
ionn
aire
; log
/ M
ML
/do
m a
rm /
2 m
ins
/ NS
/ NS
log;
AC
T; S
elf-
repo
rted
sle
ep:
TST
, SL
, num
WSL
> 3
0min
or
TST
<36
0min
, No
Rx
seda
tive-
hyp-
notic
use
/ N
S / N
S
No
diff
for
SH
or
SH +
Exe
rcis
e, f
or S
H +
lig
ht, T
SThi
gher
, SL
low
er,
Wlo
wer
TST
from
logs
< A
CT
TST
,SL
logs
> S
LA
CT,
Wlo
gs <
WA
CT
Gui
llem
inau
lt (1
81)
5D-b
Cas
e se
ries
/ L
abor
ator
y an
dho
me
/ Noc
turn
al o
nly
for
8h;
1 N
t PSG
; 7 N
t log
and
AC
T
184
(184
) / M
34±
8 (1
8-52
),F
39±
12.5
(18
-54)
/H
ead/
Nec
k tr
aum
a an
d hy
per-
som
nia
PSG
, M
SLT,
Epw
orth
, SSS
,lo
g / N
S / N
S / N
S / N
S / N
S L
og; P
SG: M
SLT,
AH
I,SO
RE
MPs
; Beh
avio
ral v
ari-
able
s; M
ood
vari
able
s
NS
/ NS
/ sel
f-se
lect
ed s
am-
ple
ED
S as
soci
ated
w/im
pair
edda
ytim
e fu
nctio
n. 2
4-h
com
a,he
ad f
ract
ure,
or
imm
edia
tene
uros
urgi
cal i
nter
vent
ion
asso
ciat
ed w
/ ESS
> 1
6 an
dM
SLT
<5.
Sle
ep a
pnea
ass
o-ci
ated
w/ w
hipl
ash.
AC
Tha
d lit
tle r
ole
in r
esul
tsor
con
clus
ions
.
Hay
es (
182)
4C-b
Cro
ss-s
ectio
nal s
tudy
/ H
ome
/ Noc
turn
al o
nly
for
9 h;
1N
tA
CT
30 (
27)
/ Grp
1 80
.9m
o±7.
2SE
M /
Nor
mal
T
ime-
laps
e vi
deo
/E
lect
rost
atic
bed
pad
/he
ad/s
houl
der
& b
utto
cks
/ 1se
c / N
S / F
FT, P
erio
dgra
m
AC
T: A
FFT
Nor
mal
sle
eper
; mid
-inf
ancy
to p
re-p
uber
ty /
NS
/ Non
e M
ovem
ent i
nten
sity
& m
ove-
men
t bou
t str
uctu
re in
tegr
itydu
ring
sle
ep d
ecre
ased
w/
age;
dec
line
in b
out d
ur w
/ag
e; in
crea
se in
bou
t fre
q. w
/ag
e
Her
ing
(63)
5D-b
NS
/ Hom
e / E
ntir
e 24
-h; 3
DA
CT
NS
(NS)
/ G
rp1
8.0±
3.0,
Grp
2 8.
0±2.
3 / N
orm
al,
Inso
mni
a, A
utis
m
log
/(A
MI)
/ w
rist
/ N
S / N
S /
Sade
h ‘8
9 lo
g; A
CT
NS
/ NS
/ NS
log
of p
aren
ts s
how
ed d
iffe
r-en
ces
in A
M W
time,
ear
ly N
tar
ousa
ls, &
mul
tiple
Nt
arou
sals
Jean
-Lou
is (
53)
5D-b
Obs
erva
tiona
l stu
dy /
Hom
e /
Ent
ire
24-h
; 3D
AC
T27
3 (N
S) /
51 (
40-6
4) /
Nor
mal
N
one
/ Act
illum
e / w
rist
/ 1
min
/ N
S / A
ctio
n 3
Moo
d: Q
WB
sca
le, C
ES-
D
NS
/ NS
/ Mea
n ag
e so
me-
wha
t hig
h (N
50)
to b
e re
pre-
sent
ativ
e of
the
adul
t pop
ula-
tion;
use
d pt
s re
ceiv
ed f
rom
rand
om te
leph
one
dial
ing-
thos
e w
ho c
onse
nted
may
be
mor
e lik
ely
to h
ave
prob
lem
s
AC
T-m
easu
red
slee
p va
ri-
able
s no
t sig
nifi
cant
ly c
orre
-la
ted
w/ Q
WB
or
CE
S-D
scor
es
Jean
-Lou
is (
16)
3C
Val
idat
ion;
AC
Tco
mpa
red
w/
othe
r te
chni
ques
/ L
abor
ator
y;H
ome
/; G
rp 1
Noc
turn
al;
Ent
ire
24 h
1N
t AC
T+
log
inho
me,
1N
t AC
T&
PSG
inla
b; G
rp I
I. N
octu
rnal
; Ent
ire
24 h
1 D
AC
T+
log+
SSS
inho
me,
3N
t AC
T+
PSG
in la
b
46 (
46)
/ Grp
1 30
±9.
0, G
rp2
46.5
±10
.8 /
Grp
2 In
som
nia
PSG
/ G
rp1
Gae
hwile
r, G
rp2
(AM
I) /
Grp
1 do
m a
rm, G
rp2
NS
/ NS
/ NS
/ AD
AS
PSG
: TST
; AC
T: T
STG
rp1
Nor
mal
/ N
S / N
S A
CT
is v
alid
for
ass
essi
ngS/
W; A
CT
is u
sefu
l to
asse
ssS/
Win
inso
mni
acs;
AD
AS
isa
valid
sof
twar
e fo
r AC
Tin
diff
eren
t typ
es o
f ap
para
tus
Jean
-Lou
is (
177)
1A
AC
Tsc
orin
g so
ftw
are
/L
abor
ator
y; H
ome
/N
octu
rnal
Ent
ire
24-h
; 1 w
kA
CT
at h
ome
+ S
SS; 3
Nt
PSG
+A
CT
(onl
y 1
nigh
tPS
G+
AC
Tan
alyz
ed)
26 (
26)
/ 46.
4±10
.8 /
NS
SSS
/ (A
MI)
/ N
S /
30se
c/1
min
/ N
S / A
DA
S; O
ther
:ze
ro-c
ross
ing
PSG
: TST
, SE
; AC
T: s
leep
thre
shol
d, W
ASO
, TST
, SE
In
som
niac
/ N
S / N
S A
CT
:PSG
in in
som
niac
s;A
CT
“is
an e
xcel
lent
tool
for
unob
trus
ive
docu
men
tatio
n of
S/W
activ
ity in
indi
vidu
als
w/…
inso
mni
a”
Aro
usal
s af
ter
SOn
defi
ned
aslo
nger
than
3 m
ins
scor
ed a
sW
; sev
eral
dif
fere
nt r
val
ues
repo
rted
for
sam
e da
ta
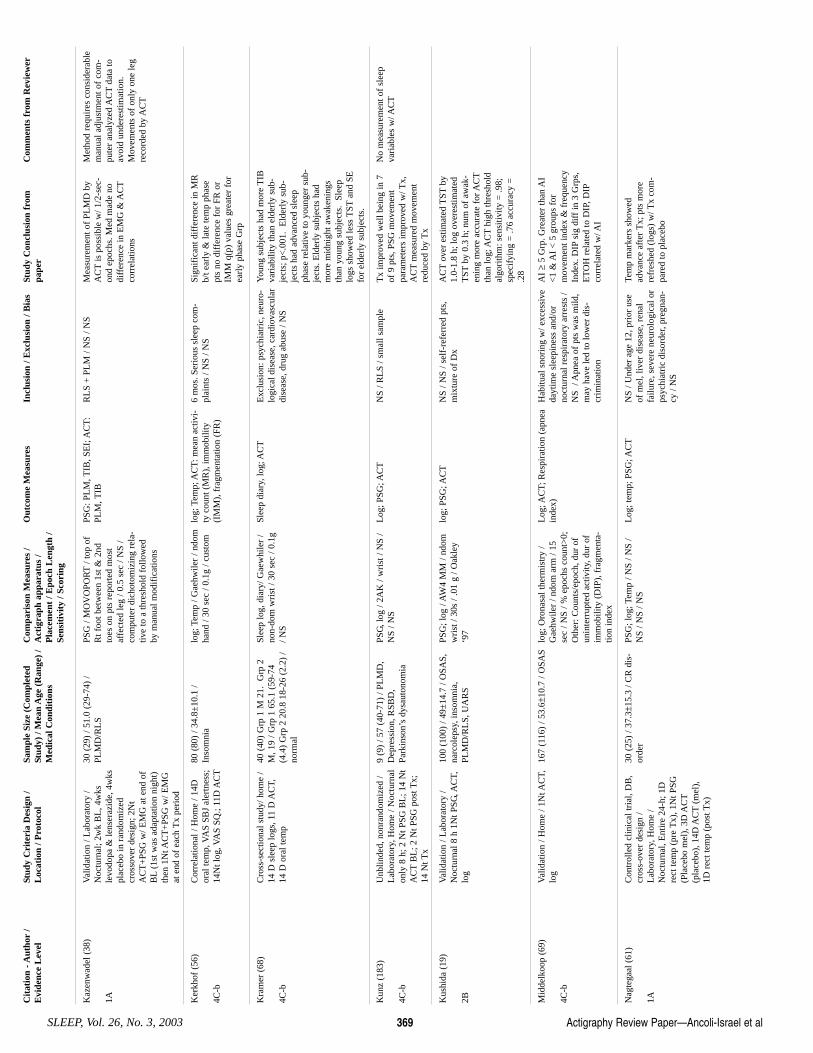
Cit
atio
n - A
utho
r/
Evi
denc
e L
evel
St
udy
Cri
teri
a D
esig
n /
Loc
atio
n / P
roto
col
Sam
ple
Size
(C
ompl
eted
Stud
y) /
Mea
n A
ge (
Ran
ge)
/M
edic
al C
ondi
tion
s
Com
pari
son
Mea
sure
s /
Act
igra
ph a
ppar
atus
/P
lace
men
t / E
poch
Len
gth
/Se
nsit
ivit
y / S
cori
ng
Out
com
e M
easu
res
Incl
usio
n / E
xclu
sion
/ B
ias
Stud
y C
oncl
usio
n fr
ompa
per
Com
men
ts f
rom
Rev
iew
er
Actigraphy Review Paper—Ancoli-Israel et alSLEEP, Vol. 26, No. 3, 2003 369
Kaz
enw
adel
(38
)
1A
Val
idat
ion
/ Lab
orat
ory
/N
octu
rnal
; 2w
k B
L, 4
wks
levo
dopa
& le
nser
azid
e, 4
wks
plac
ebo
in r
ando
miz
edcr
osso
ver
desi
gn; 2
Nt
AC
T+
PSG
w/ E
MG
at e
nd o
fB
L(1
st w
as a
dapt
atio
n ni
ght)
then
1N
t AC
T+
PSG
w/ E
MG
at e
nd o
f ea
ch T
x pe
riod
30 (
29)
/ 51.
0 (2
9-74
) /
PLM
D/R
LS
PSG
/ M
OV
OPO
RT
/ top
of
Rt f
oot b
etw
een
1st &
2nd
toes
on
pts
repo
rted
mos
taf
fect
ed le
g / 0
.5 s
ec /
NS
/co
mpu
ter
dich
otom
izin
g re
la-
tive
to a
thre
shol
d fo
llow
edby
man
ual m
odif
icat
ions
PSG
: PL
M, T
IB, S
EI;
AC
T:
PLM
, TIB
R
LS
+ P
LM
/ N
S / N
S M
easu
rem
ent o
f PL
MD
by
AC
Tis
pos
sibl
e w
/ 1/2
-sec
-on
d ep
ochs
. Med
mad
e no
diff
eren
ce in
EM
G &
AC
Tco
rrel
atio
ns
Met
hod
requ
ires
con
side
rabl
em
anua
l adj
ustm
ent o
f co
m-
pute
r an
alyz
ed A
CT
data
toav
oid
unde
rest
imat
ion.
Mov
emen
ts o
f on
ly o
ne le
gre
cord
ed b
y A
CT
Ker
khof
(56
)
4C-b
Cor
rela
tiona
l / H
ome
/ 14D
oral
tem
p, V
AS
SBJ
aler
tnes
s;14
Nt l
og, V
AS
SQ.;
11D
AC
T
80 (
80)
/ 34.
8±10
.1 /
Inso
mni
a lo
g; T
emp
/ Gae
hwile
r / n
dom
hand
/ 30
sec
/ 0.
1g /
cust
om
log;
Tem
p; A
CT
: mea
n ac
tivi-
ty c
ount
(M
R),
imm
obili
ty(I
MM
), f
ragm
enta
tion
(FR
)
6 m
os. S
erio
us s
leep
com
-pl
aint
s / N
S / N
S Si
gnif
ican
t dif
fere
nce
in M
Rb/
t ear
ly &
late
tem
p ph
ase
pts
no d
iffe
renc
e fo
r FR
or
IMM
q(p
) va
lues
gre
ater
for
earl
y ph
ase
Grp
Kra
mer
(68
)
4C-b
Cro
ss-s
ectio
nal s
tudy
/ hom
e /
14 D
sle
ep lo
gs, 1
1 D
AC
T,14
D o
ral t
emp
40 (
40)
Grp
1 M
21.
Grp
2M
, 19
/ Grp
1 6
5.1
(59-
74(4
.4)
Grp
2 2
0.8
18-2
6 (2
.2)
/no
rmal
Slee
p lo
g, d
iary
/ Gae
whi
ler
/no
n-do
m w
rist
/ 30
sec
/ 0.
1g/ N
S
Slee
p di
ary,
log;
AC
TE
xclu
sion
: psy
chia
tric
, neu
ro-
logi
cal d
isea
se, c
ardi
ovas
cula
rdi
seas
e, d
rug
abus
e / N
S
You
ng s
ubje
cts
had
mor
e T
IBva
riab
ility
than
eld
erly
sub
-je
cts;
p<
.001
. E
lder
ly s
ub-
ject
s ha
d ad
vanc
ed s
leep
phas
e re
lativ
e to
you
nger
sub
-je
cts.
Eld
erly
sub
ject
s ha
dm
ore
mid
nigh
t aw
aken
ings
than
you
ng s
ubje
cts.
Sle
eplo
gs s
how
ed le
ss T
STan
d SE
for
elde
rly
subj
ects
.
Kun
z (1
83)
4C-b
Unb
linde
d, n
onra
ndom
ized
/L
abor
ator
y, H
ome
/ Noc
turn
alon
ly 8
h; 2
Nt P
SG B
L; 1
4 N
tA
CT
BL
; 2 N
t PSG
pos
t Tx;
14 N
t Tx
9 (9
) / 5
7 (4
0-71
) / P
LM
D,
Dep
ress
ion,
RSB
D,
Park
inso
n’s
dysa
uton
omia
PSG
, log
/ 2A
K /
wri
st /
NS
/N
S / N
S
Log
; PSG
; AC
TN
S / R
LS
/ sm
all s
ampl
e T
x im
prov
ed w
ell b
eing
in 7
of 9
pts
, PSG
mov
emen
tpa
ram
eter
s im
prov
ed w
/ Tx,
AC
Tm
easu
red
mov
emen
tre
duce
d by
Tx
No
mea
sure
men
t of
slee
pva
riab
les
w/ A
CT
Kus
hida
(19
)
2B
Val
idat
ion
/ Lab
orat
ory
/N
octu
rnal
8 h
1N
t PSG
, AC
T,lo
g
100
(100
) / 4
9±14
.7 /
OSA
S,na
rcol
epsy
, ins
omni
a,PL
MD
/RL
S, U
AR
S
PSG
; log
/ A
W4
MM
/ nd
omw
rist
/ 30
s / .
01 g
/ O
akle
y‘9
7
log;
PSG
; AC
TN
S / N
S / s
elf-
refe
rred
pts
,m
ixtu
re o
f D
x A
CT
over
est
imat
ed T
STby
1.0-
1.8
h; lo
g ov
eres
timat
edT
STby
0.3
h; n
um o
f aw
ak-
enin
g m
ore
accu
rate
for
AC
Tth
an lo
g; A
CT
high
thre
shol
dal
gori
thm
: sen
sitiv
ity =
.98;
spec
ifyi
ng =
.76
accu
racy
=.2
8
Mid
delk
oop
(69)
4C-b
Val
idat
ion
/ Hom
e / 1
Nt A
CT,
log
167
(116
) / 5
3.6±
10.7
/ O
SAS
log;
Oro
nasa
l the
rmis
try
/G
aehw
iler
/ ndo
m a
rm /
15se
c / N
S / %
epo
chs
coun
t>0;
Oth
er: C
ount
s/ep
och,
dur
of
unin
terr
upte
d ac
tivity
, dur
of
imm
obili
ty (
DIP
), f
ragm
enta
-tio
n in
dex
Log
; AC
T; R
espi
ratio
n (a
pnea
inde
x)
Hab
itual
sno
ring
w/ e
xces
sive
dayt
ime
slee
pine
ss a
nd/o
rno
ctur
nal r
espi
rato
ry a
rres
ts /
NS
/ A
pnea
of
pts
was
mild
,m
ay h
ave
led
to lo
wer
dis
-cr
imin
atio
n
AI ≥
5 G
rp. G
reat
er th
an A
I<
1 &
AI
< 5
gro
ups
for
mov
emen
t ind
ex &
fre
quen
cyIn
dex.
DIP
sig
diff
in 3
Grp
s,E
TO
H r
elat
ed to
DIP
, DIP
corr
elat
ed w
/ AI
Nag
tega
al (
61)
1A
Con
trol
led
clin
ical
tria
l, D
B,
cros
s-ov
er d
esig
n /
Lab
orat
ory,
Hom
e /
Noc
turn
al, E
ntir
e 24
-h; 1
Dre
ct te
mp
(pre
Tx)
, 1N
t PSG
(Pla
cebo
mel
), 3
D A
CT
(pla
cebo
), 1
4D A
CT
(mel
),1D
rec
t tem
p (p
ost T
x)
30 (
25)
/ 37.
3±15
.3 /
CR
dis
-or
der
PSG
; log
; Tem
p / N
S / N
S /
NS
/ NS
/ NS
Log
; tem
p; P
SG; A
CT
NS
/ Und
er a
ge 1
2, p
rior
use
of m
el, l
iver
dis
ease
, ren
alfa
ilure
, sev
ere
neur
olog
ical
or
psyc
hiat
ric
diso
rder
, pre
gnan
-cy
/ N
S
Tem
p m
arke
rs s
how
edad
vanc
e af
ter
Tx;
pts
mor
ere
fres
hed
(log
s) w
/ Tx
com
-pa
red
to p
lace
bo
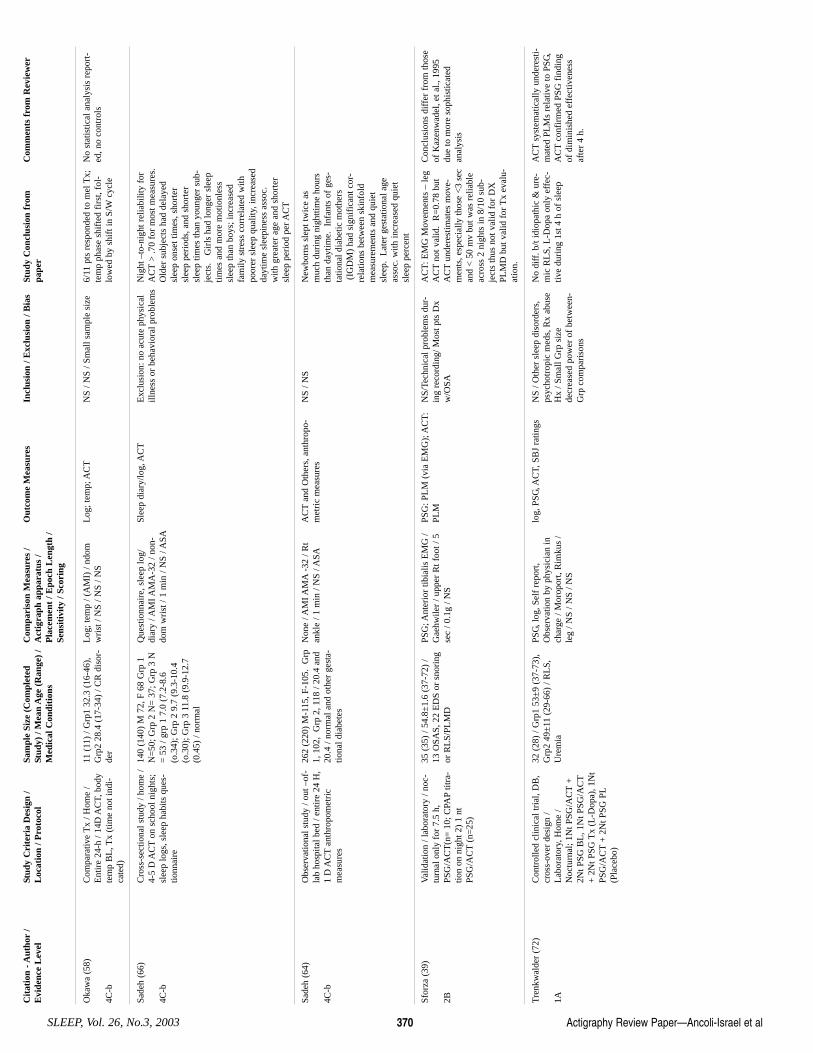
Cit
atio
n - A
utho
r/
Evi
denc
e L
evel
St
udy
Cri
teri
a D
esig
n /
Loc
atio
n / P
roto
col
Sam
ple
Size
(C
ompl
eted
Stud
y) /
Mea
n A
ge (
Ran
ge)
/M
edic
al C
ondi
tion
s
Com
pari
son
Mea
sure
s /
Act
igra
ph a
ppar
atus
/P
lace
men
t / E
poch
Len
gth
/Se
nsit
ivit
y / S
cori
ng
Out
com
e M
easu
res
Incl
usio
n / E
xclu
sion
/ B
ias
Stud
y C
oncl
usio
n fr
ompa
per
Com
men
ts f
rom
Rev
iew
er
Actigraphy Review Paper—Ancoli-Israel et alSLEEP, Vol. 26, No.3, 2003 370
Oka
wa
(58)
4C-b
Com
para
tive
Tx
/ Hom
e /
Ent
ire
24-h
/ 14
D A
CT,
bod
yte
mp
BL
, Tx
(tim
e no
t ind
i-ca
ted)
11 (
11)
/ Grp
1 32
.3 (
16-4
6),
Grp
2 28
.4 (
17-3
4) /
CR
dis
or-
der
Log
; tem
p / (
AM
I) /
ndom
wri
st /
NS
/ NS
/ NS
L
og; t
emp;
AC
TN
S / N
S / S
mal
l sam
ple
size
6/
11 p
ts r
espo
nded
to m
el T
x;te
mp
phas
e sh
ifte
d fi
rst,
fol-
low
ed b
y sh
ift i
n S/
Wcy
cle
No
stat
istic
al a
naly
sis
repo
rt-
ed, n
o co
ntro
ls
Sade
h (6
6)
4C-b
Cro
ss-s
ectio
nal s
tudy
/ ho
me
/4-
5 D
AC
Ton
sch
ool n
ight
s;sl
eep
logs
, sle
ep h
abits
que
s-tio
nnai
re
140
(140
) M
72,
F 6
8 G
rp 1
N=
50; G
rp 2
N=
37;
Grp
3 N
= 5
3 / g
rp 1
7.0
(7.
2-8.
6(o
.34)
; Grp
2 9
.7 (
9.3-
10.4
(o.3
0); G
rp 3
11.
8 (9
.9-1
2.7
(0.4
5) /
norm
al
Que
stio
nnai
re, s
leep
log/
diar
y / A
MI A
MA
-32
/ non
-do
m w
rist
/ 1
min
/ N
S / A
SA
Slee
p di
ary/
log,
AC
TE
xclu
sion
: no
acut
e ph
ysic
alill
ness
or
beha
vior
al p
robl
ems
Nig
ht –
to-n
ight
rel
iabi
lity
for
AC
T>
.70
for
mos
t mea
sure
s.O
lder
sub
ject
s ha
d de
laye
dsl
eep
onse
t tim
es, s
hort
ersl
eep
peri
ods,
and
sho
rter
slee
p tim
es th
an y
oung
er s
ub-
ject
s.
Gir
ls h
ad lo
nger
sle
eptim
es a
nd m
ore
mot
ionl
ess
slee
p th
an b
oys;
incr
ease
dfa
mily
str
ess
corr
elat
ed w
ithpo
orer
sle
ep q
ualit
y, in
crea
sed
dayt
ime
slee
pine
ss a
ssoc
.w
ith g
reat
er a
ge a
nd s
hort
ersl
eep
peri
od p
er A
CT
Sade
h (6
4)
4C-b
Obs
erva
tiona
l stu
dy /
out –
of-
lab
hosp
ital b
ed /
entir
e 24
H,
1 D
AC
Tan
thro
pom
etri
cm
easu
res
262
(220
) M
-115
, F-1
05.
Grp
1, 1
02,
Grp
2, 1
18 /
20.4
and
20.4
/ no
rmal
and
oth
er g
esta
-tio
nal d
iabe
tes
Non
e / A
MI A
MA
-32
/ Rt
ankl
e / 1
min
/ N
S / A
SAA
CT
and
Oth
ers,
ant
hrop
o-m
etri
c m
easu
res
NS
/ NS
New
born
s sl
ept t
wic
e as
muc
h du
ring
nig
httim
e ho
urs
than
day
time.
Inf
ants
of
ges-
tatio
nal d
iabe
tic m
othe
rs(I
GD
M)
had
sign
ific
ant c
or-
rela
tions
bet
wee
n sk
info
ldm
easu
rem
ents
and
qui
etsl
eep.
Lat
er g
esta
tiona
l age
asso
c. w
ith in
crea
sed
quie
tsl
eep
perc
ent
Sfor
za (
39)
2B
Val
idat
ion
/ lab
orat
ory
/ noc
-tu
rnal
onl
y fo
r 7.
5 h,
PSG
/AC
T(n
= 1
0; C
PAP
titra
-tio
n on
nig
ht 2
) 1
ntPS
G/A
CT
(n=
25)
35 (
35)
/ 54.
8±1.
6 (3
7-72
) /
13 O
SAS,
22
ED
S or
sno
ring
or R
LS/
PLM
D
PSG
; Ant
erio
r tib
ialis
EM
G /
Gae
hwile
r / u
pper
Rt f
oot /
5se
c / 0
.1g
/ NS
PSG
: PL
M (
via
EM
G);
AC
T:
PLM
NS/
Tech
nica
l pro
blem
s du
r-in
g re
cord
ing/
Mos
t pts
Dx
w/O
SA
AC
T: E
MG
Mov
emen
ts –
leg
AC
Tno
t val
id.
R=
0.78
but
AC
Tun
dere
stim
ates
mov
e-m
ents
, esp
ecia
lly th
ose
<3
sec
and
< 5
0 m
v bu
t was
rel
iabl
eac
ross
2 n
ight
s in
8/1
0 su
b-je
cts
thus
not
val
id f
or D
XPL
MD
but
val
id f
or T
x ev
alu-
atio
n.
Con
clus
ions
dif
fer
from
thos
eof
Kaz
enw
adel
, et a
l., 1
995
due
to m
ore
soph
istic
ated
anal
ysis
Tre
nkw
alde
r (7
2)
1A
Con
trol
led
clin
ical
tria
l, D
B,
cros
s-ov
er d
esig
n /
Lab
orat
ory,
Hom
e /
Noc
turn
al; 1
Nt P
SG/A
CT
+2N
t PSG
BL
, 1N
t PSG
/AC
T+
2N
t PSG
Tx
(L-D
opa)
, 1N
tPS
G/A
CT
+ 2
Nt P
SG P
L(P
lace
bo)
32 (
28)
/ Grp
1 53
±9
(37-
73),
Grp
2 49
±11
(29
-66)
/ R
LS,
Ure
mia
PSG
, log
, Sel
f re
port
,O
bser
vatio
n by
phy
sici
an in
char
ge /
Mor
opor
t, R
imku
s /
leg
/ NS
/ NS
/ NS
log,
PSG
, AC
T, S
BJ
ratin
gs
NS
/ Oth
er s
leep
dis
orde
rs,
psyc
hotr
opic
med
s, R
x ab
use
Hx
/ Sm
all G
rp s
ize
decr
ease
d po
wer
of
betw
een-
Grp
com
pari
sons
No
diff
. b/t
idio
path
ic &
ure
-m
ic R
LS,
L-D
opa
only
eff
ec-
tive
duri
ng 1
st 4
h o
f sl
eep
AC
Tsy
stem
atic
ally
und
eres
ti-m
ated
PL
Ms
rela
tive
to P
SG,
AC
Tco
nfir
med
PSG
fin
ding
of d
imin
ishe
d ef
fect
iven
ess
afte
r 4
h.
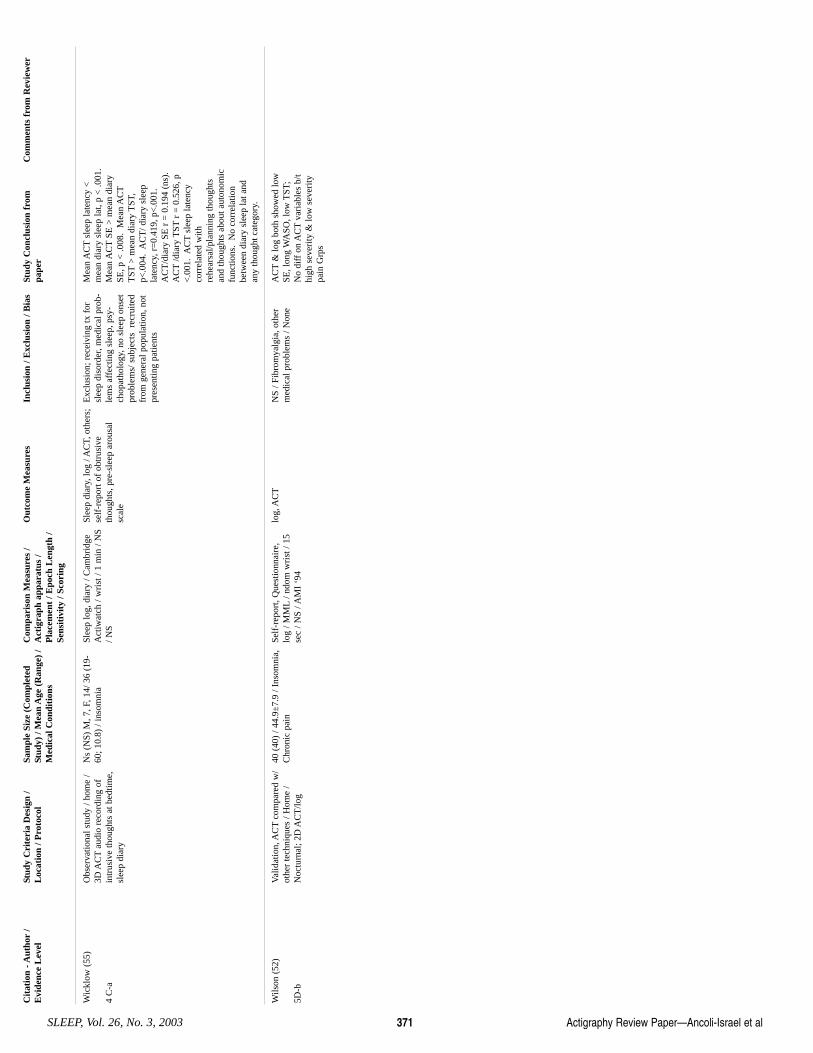
Cit
atio
n - A
utho
r/
Evi
denc
e L
evel
St
udy
Cri
teri
a D
esig
n /
Loc
atio
n / P
roto
col
Sam
ple
Size
(C
ompl
eted
Stud
y) /
Mea
n A
ge (
Ran
ge)
/M
edic
al C
ondi
tion
s
Com
pari
son
Mea
sure
s /
Act
igra
ph a
ppar
atus
/P
lace
men
t / E
poch
Len
gth
/Se
nsit
ivit
y / S
cori
ng
Out
com
e M
easu
res
Incl
usio
n / E
xclu
sion
/ B
ias
Stud
y C
oncl
usio
n fr
ompa
per
Com
men
ts f
rom
Rev
iew
er
Actigraphy Review Paper—Ancoli-Israel et alSLEEP, Vol. 26, No. 3, 2003 371
Wic
klow
(55
)
4 C
-a
Obs
erva
tiona
l stu
dy /
hom
e /
3D A
CT
audi
o re
cord
ing
ofin
trus
ive
thou
ghts
at b
edtim
e,sl
eep
diar
y
Ns
(NS)
M, 7
, F, 1
4/ 3
6 (1
9-60
; 10.
8) /
inso
mni
a Sl
eep
log,
dia
ry /
Cam
brid
geA
ctiw
atch
/ w
rist
/ 1
min
/ N
S/ N
S
Slee
p di
ary,
log
/ AC
T, o
ther
s;se
lf-r
epor
t of
obtr
usiv
eth
ough
ts, p
re-s
leep
aro
usal
scal
e
Exc
lusi
on; r
ecei
ving
tx f
orsl
eep
diso
rder
, med
ical
pro
b-le
ms
affe
ctin
g sl
eep,
psy
-ch
opat
holo
gy, n
o sl
eep
onse
t pr
oble
ms/
sub
ject
s r
ecru
ited
from
gen
eral
pop
ulat
ion,
not
pres
entin
g pa
tient
s
Mea
n A
CT
slee
p la
tenc
y <
mea
n di
ary
slee
p la
t, p
< .0
01.
Mea
n A
CT
SE >
mea
n di
ary
SE, p
< .0
08.
Mea
n A
CT
TST
> m
ean
diar
y T
ST,
p<.0
04.
AC
T/ d
iary
sle
epla
tenc
y, r
=0.
419,
p<
.001
.A
CT
/dia
ry S
E r
= 0
.194
(ns
).A
CT
/dia
ry T
STr
= 0
.526
, p<
.001
. A
CT
slee
p la
tenc
yco
rrel
ated
with
rehe
arsa
l/pla
nnin
g th
ough
tsan
d th
ough
ts a
bout
aut
onom
icfu
nctio
ns.
No
corr
elat
ion
betw
een
diar
y sl
eep
lat a
ndan
y th
ough
t cat
egor
y.
Wils
on (
52)
5D-b
Val
idat
ion,
AC
Tco
mpa
red
w/
othe
r te
chni
ques
/ H
ome
/N
octu
rnal
; 2D
AC
T/lo
g
40 (
40)
/ 44.
9±7.
9 / I
nsom
nia,
Chr
onic
pai
n Se
lf-r
epor
t, Q
uest
ionn
aire
,lo
g / M
ML
/ ndo
m w
rist
/ 15
sec
/ NS
/ AM
I ‘9
4
log,
AC
TN
S / F
ibro
mya
lgia
, oth
erm
edic
al p
robl
ems
/ Non
e A
CT
& lo
g bo
th s
how
ed lo
wSE
, lon
g W
ASO
, low
TST
;N
o di
ff o
n A
CT
vari
able
s b/
thi
gh s
ever
ity &
low
sev
erity
pain
Grp
s
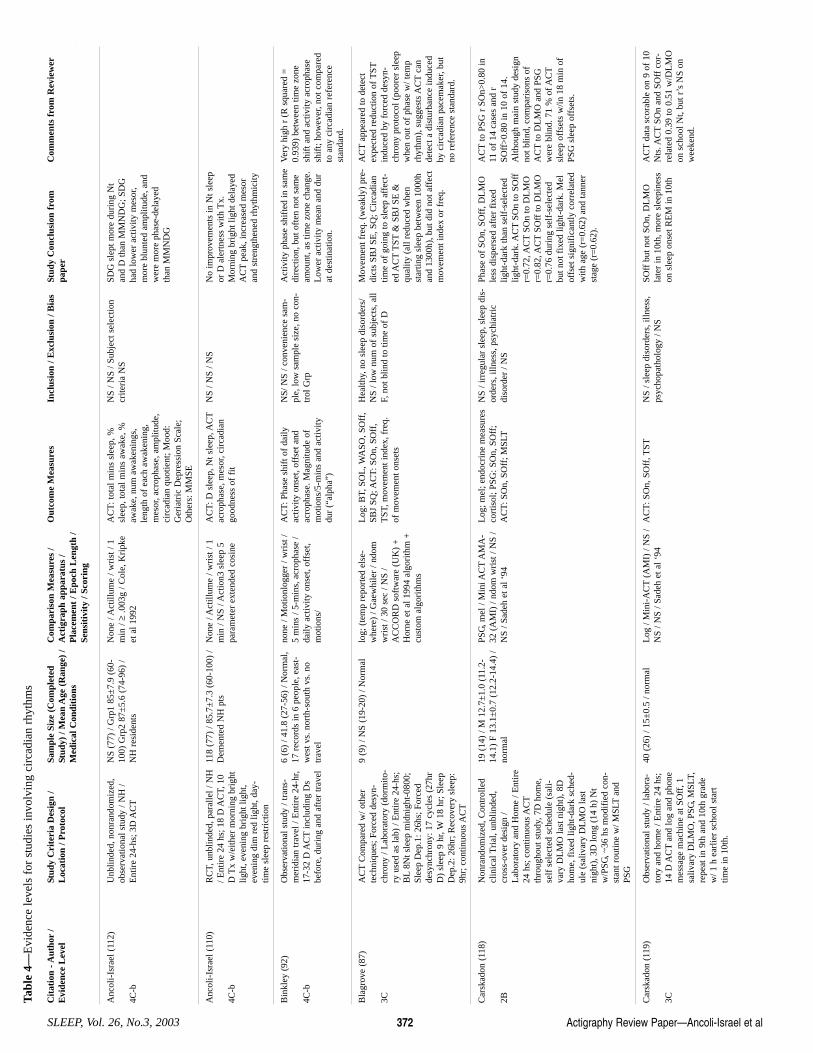
Actigraphy Review Paper—Ancoli-Israel et alSLEEP, Vol. 26, No.3, 2003 372
Anc
oli-
Isra
el (
112)
4C-b
Unb
linde
d, n
onra
ndom
ized
,ob
serv
atio
nal s
tudy
/ N
H /
Ent
ire
24-h
s; 3
D A
CT
NS
(77)
/ G
rp1
85±
7.9
(60-
100)
Grp
2 87
±5.
6 (7
4-96
) /
NH
res
iden
ts
Non
e / A
ctill
ume
/ wri
st /
1m
in / ≥
.003
g / C
ole,
Kri
pke
et a
l 199
2
AC
T: t
otal
min
s sl
eep,
%sl
eep,
tota
l min
s aw
ake,
%aw
ake,
num
aw
aken
ings
,le
ngth
of
each
aw
aken
ing,
mes
or, a
crop
hase
, am
plitu
de,
circ
adia
n qu
otie
nt; M
ood:
Ger
iatr
ic D
epre
ssio
n Sc
ale;
Oth
ers:
MM
SE
NS
/ NS
/ Sub
ject
sel
ectio
ncr
iteri
a N
S SD
G s
lept
mor
e du
ring
Nt
and
D th
an M
MN
DG
; SD
Gha
d lo
wer
act
ivity
mes
or,
mor
e bl
unte
d am
plitu
de, a
ndw
ere
mor
e ph
ase-
dela
yed
than
MM
ND
G
Cit
atio
n - A
utho
r/
Evi
denc
e L
evel
St
udy
Cri
teri
a D
esig
n /
Loc
atio
n / P
roto
col
Sam
ple
Size
(C
ompl
eted
Stud
y) /
Mea
n A
ge (
Ran
ge)
/M
edic
al C
ondi
tion
s
Com
pari
son
Mea
sure
s /
Act
igra
ph a
ppar
atus
/P
lace
men
t / E
poch
Len
gth
/Se
nsit
ivit
y / S
cori
ng
Out
com
e M
easu
res
Incl
usio
n / E
xclu
sion
/ B
ias
Stud
y C
oncl
usio
n fr
ompa
per
Com
men
ts f
rom
Rev
iew
er
Tabl
e 4—
Evi
denc
e le
vels
for
stu
dies
invo
lvin
g ci
rcad
ian
rhyt
hms
Anc
oli-
Isra
el (
110)
4C-b
RC
T, u
nblin
ded,
par
alle
l / N
H/ E
ntir
e 24
hs;
18
D A
CT,
10
D T
x w
/eith
er m
orni
ng b
righ
tlig
ht, e
veni
ng b
righ
t lig
ht,
even
ing
dim
red
ligh
t, da
y-tim
e sl
eep
rest
rict
ion
118
(77)
/ 85
.7±
7.3
(60-
100)
/D
emen
ted
NH
pts
N
one
/ Act
illum
e / w
rist
/ 1
min
/ N
S / A
ctio
n3 s
leep
5pa
ram
eter
ext
ende
d co
sine
AC
T: D
sle
ep, N
t sle
ep, A
CT
acro
phas
e, m
esor
, cir
cadi
ango
odne
ss o
f fi
t
NS
/ NS
/ NS
No
impr
ovem
ents
in N
t sle
epor
D a
lert
ness
with
Tx.
Mor
ning
bri
ght l
ight
del
ayed
AC
Tpe
ak, i
ncre
ased
mes
oran
d st
reng
then
ed r
hyth
mic
ity
Bin
kley
(92
)
4C-b
Obs
erva
tiona
l stu
dy /
tran
s-m
erid
ian
trav
el /
Ent
ire
24-h
r,17
-32
D A
CT
incl
udin
g D
sbe
fore
, dur
ing
and
afte
r tr
avel
6 (6
) / 4
1.8
(27-
56)
/ Nor
mal
,17
rec
ords
in 6
peo
ple,
eas
t-w
est v
s. n
orth
-sou
th v
s. n
otr
avel
none
/ M
otio
nlog
ger
/ wri
st /
5 m
ins
/ 5-m
ins,
acr
opha
se /
daily
act
ivity
ons
et, o
ffse
t,m
otio
ns/
AC
T: P
hase
shi
ft o
f da
ilyac
tivity
ons
et, o
ffse
t and
acro
phas
e. M
agni
tude
of
mot
ions
/5-m
ins
and
activ
itydu
r (“
alph
a”)
NS/
NS
/ con
veni
ence
sam
-pl
e, lo
w s
ampl
e si
ze, n
o co
n-tr
ol G
rp
Act
ivity
pha
se s
hift
ed in
sam
edi
rect
ion,
but
oft
en n
ot s
ame
amou
nt, a
s tim
e zo
ne c
hang
e.L
ower
act
ivity
mea
n an
d du
rat
des
tinat
ion.
Ver
y hi
gh r
(R
squ
ared
=0.
939)
bet
wee
n tim
e zo
nesh
ift a
nd a
ctiv
ity a
crop
hase
shif
t; ho
wev
er, n
ot c
ompa
red
to a
ny c
irca
dian
ref
eren
cest
anda
rd.
Bla
grov
e (8
7)
3C
AC
TC
ompa
red
w/ o
ther
tech
niqu
es; F
orce
d de
syn-
chro
ny /
Lab
orat
ory
(dor
mito
-ry
use
d as
lab)
/ E
ntir
e 24
-hs;
BL
8Nt s
leep
mid
nigh
t-08
00;
Slee
p D
ep.1
: 26h
s; F
orce
dde
sync
hron
y: 1
7 cy
cles
(27
hrD
) sl
eep
9 hr
, W18
hr;
Sle
epD
ep.2
: 26h
r; R
ecov
ery
slee
p:9h
r; c
ontin
uous
AC
T
9 (9
) / N
S (1
9-20
) / N
orm
al
log;
(te
mp
repo
rted
els
e-w
here
) / G
aew
hile
r / n
dom
wri
st /
30 s
ec /
NS
/A
CC
OR
D s
oftw
are
(UK
) +
Hor
ne e
t al 1
994
algo
rith
m +
cust
om a
lgor
ithm
s
Log
: BT,
SO
L, W
ASO
, SO
ff,
SBJ
SQ; A
CT
: SO
n, S
Off
,T
ST, m
ovem
ent i
ndex
, fre
q.of
mov
emen
t ons
ets
Hea
lthy,
no
slee
p di
sord
ers/
NS
/ low
num
of
subj
ects
, all
F, n
ot b
lind
to ti
me
of D
Mov
emen
t fre
q. (
wea
kly)
pre
-di
cts
SBJ
SE, S
Q; C
irca
dian
time
of g
oing
to s
leep
aff
ect-
ed A
CT
TST
& S
BJ
SE &
qual
ity (
all r
educ
ed w
hen
star
ting
slee
p be
twee
n 10
00h
and
1300
h), b
ut d
id n
ot a
ffec
tm
ovem
ent i
ndex
or
freq
.
AC
Tap
pear
ed to
det
ect
expe
cted
red
uctio
n of
TST
indu
ced
by f
orce
d de
syn-
chro
ny p
roto
col (
poor
er s
leep
whe
n ou
t of
phas
e w
/ tem
prh
ythm
), s
ugge
sts
AC
Tca
nde
tect
a d
istu
rban
ce in
duce
dby
cir
cadi
an p
acem
aker
, but
no r
efer
ence
sta
ndar
d.
Car
skad
on (
118)
2B
Non
rand
omiz
ed, C
ontr
olle
dcl
inic
al T
rial
, unb
linde
d,cr
oss-
over
des
ign
/L
abor
ator
y an
d H
ome
/ Ent
ire
24 h
s; c
ontin
uous
AC
Tth
roug
hout
stu
dy, 7
D h
ome,
self
sel
ecte
d sc
hedu
le (
sali-
vary
DL
MO
last
nig
ht),
8D
hom
e, f
ixed
ligh
t-da
rk s
ched
-ul
e (s
aliv
ary
DL
MO
last
nigh
t), 3
D lo
ng (
14 h
) N
tw
/PSG
, ~36
hs
mod
ifie
d co
n-st
ant r
outin
e w
/ MSL
Tan
dPS
G
19 (
14)
/ M 1
2.7±
1.0
(11.
2-14
.1)
F 13
.1±
0.7
(12.
2-14
.4)
/no
rmal
PSG
, mel
/ M
ini A
CT
AM
A-
32 (
AM
I) /
ndom
wri
st /
NS
/N
S / S
adeh
et a
l ‘94
Log
; mel
; end
ocri
ne m
easu
res
cort
isol
; PSG
: SO
n, S
Off
;A
CT
: SO
n, S
Off
; MSL
T
NS
/ irr
egul
ar s
leep
, sle
ep d
is-
orde
rs, i
llnes
s, p
sych
iatr
icdi
sord
er /
NS
Phas
e of
SO
n, S
Off
, DL
MO
less
dis
pers
ed a
fter
fix
edlig
ht-d
ark
than
sel
f-se
lect
edlig
ht-d
ark.
AC
TSO
n to
SO
ffr=
0.72
, AC
TSO
n to
DL
MO
r=0.
82, A
CT
SOff
to D
LM
Or=
0.76
dur
ing
self
-sel
ecte
dbu
t not
fix
ed li
ght-
dark
. Mel
offs
et s
igni
fica
ntly
cor
rela
ted
with
age
(r=
0.62
) an
d ta
nner
stag
e (r
=0.
62).
AC
Tto
PSG
r S
On>
0.80
in11
of
14 c
ases
and
rSO
ff>
0.80
in 1
0 of
14.
Alth
ough
mai
n st
udy
desi
gnno
t blin
d, c
ompa
riso
ns o
fA
CT
to D
LM
O a
nd P
SGw
ere
blin
d. 7
1 %
of A
CT
slee
p of
fset
s w
/in 1
8 m
in o
fPS
G s
leep
off
sets
.
Car
skad
on (
119)
3C
Obs
erva
tiona
l stu
dy /
labo
ra-
tory
and
hom
e / E
ntir
e 24
hs;
14 D
AC
Tan
d lo
g an
d ph
one
mes
sage
mac
hine
at S
Off
, 1sa
livar
y D
LM
O, P
SG, M
SLT,
repe
at in
9th
and
10t
h gr
ade
w/ 1
h e
arlie
r sc
hool
sta
rttim
e in
10t
h.
40 (
26)
/ 15±
0.5
/ nor
mal
L
og /
Min
i-A
CT
(AM
I) /
NS
/N
S / N
S / S
adeh
et a
l ‘94
A
CT
: SO
n, S
Off
, TST
NS
/ sle
ep d
isor
ders
, illn
ess,
psyc
hopa
thol
ogy
/ NS
SOff
but
not
SO
n, D
LM
Ola
ter
in 1
0th,
mor
e sl
eepi
ness
on s
leep
ons
et R
EM
in 1
0th
AC
Tda
ta s
cora
ble
on 9
of
10N
ts. A
CT
SOn
and
SOff
cor
-re
late
d 0.
39 to
0.5
1 w
/DL
MO
on s
choo
l Nt,
but r
’s N
S on
wee
kend
.
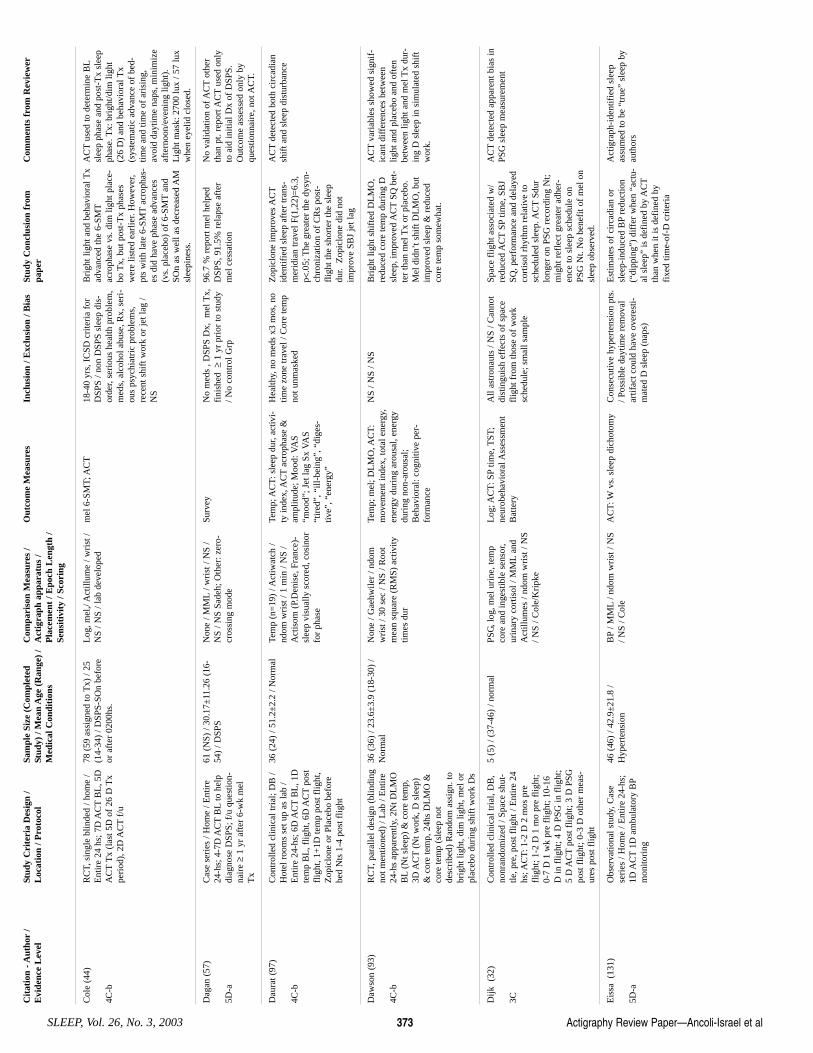
Cit
atio
n - A
utho
r/
Evi
denc
e L
evel
St
udy
Cri
teri
a D
esig
n /
Loc
atio
n / P
roto
col
Sam
ple
Size
(C
ompl
eted
Stud
y) /
Mea
n A
ge (
Ran
ge)
/M
edic
al C
ondi
tion
s
Com
pari
son
Mea
sure
s /
Act
igra
ph a
ppar
atus
/P
lace
men
t / E
poch
Len
gth
/Se
nsit
ivit
y / S
cori
ng
Out
com
e M
easu
res
Incl
usio
n / E
xclu
sion
/ B
ias
Stud
y C
oncl
usio
n fr
ompa
per
Com
men
ts f
rom
Rev
iew
er
Actigraphy Review Paper—Ancoli-Israel et alSLEEP, Vol. 26, No. 3, 2003 373
Col
e (4
4)
4C-b
RC
T, s
ingl
e bl
inde
d / h
ome
/E
ntir
e 24
hs;
7D
AC
TB
L, 5
DA
CT
Tx
(las
t 5D
of
26 D
Tx
peri
od),
2D
AC
Tf/
u
78 (
59 a
ssig
ned
to T
x) /
25(1
4-34
) / D
SPS-
SOn
befo
reor
aft
er 0
200h
s.
Log
, mel
,/ A
ctill
ume
/ wri
st /
NS
/ NS
/ lab
dev
elop
edm
el 6
-SM
T; A
CT
18-4
0 yr
s, I
CSD
cri
teri
a fo
rD
SPS
/ non
DSP
S sl
eep
dis-
orde
r, se
riou
s he
alth
pro
blem
,m
eds,
alc
ohol
abu
se, R
x, s
eri-
ous
psyc
hiat
ric
prob
lem
s,re
cent
shi
ft w
ork
or je
t lag
/N
S
Bri
ght l
ight
and
beh
avio
ral T
xad
vanc
ed th
e 6-
SMT
acro
phas
e vs
. dim
ligh
t pla
ce-
bo T
x, b
ut p
ost-
Tx
phas
esw
ere
liste
d ea
rlie
r. H
owev
er,
pts
with
late
6-S
MT
acro
phas
-es
did
hav
e ph
ase
adva
nces
(vs.
pla
cebo
) of
6-S
MT
and
SOn
as w
ell a
s de
crea
sed
AM
slee
pine
ss.
AC
Tus
ed to
det
erm
ine
BL
slee
p ph
ase
and
post
-Tx
slee
pph
ase.
Tx:
bri
ght/d
im li
ght
(26
D)
and
beha
vior
al T
x(s
yste
mat
ic a
dvan
ce o
f be
d-tim
e an
d tim
e of
ari
sing
,av
oid
dayt
ime
naps
, min
imiz
eaf
tern
oon/
even
ing
light
).L
ight
mas
k: 2
700
lux
/ 57
lux
whe
n ey
elid
clo
sed.
Dag
an (
57)
5D-a
Cas
e se
ries
/ H
ome
/ Ent
ire
24-h
s; 4
-7D
AC
TB
Lto
hel
pdi
agno
se D
SPS;
f/u
que
stio
n-na
ire ≥
1 yr
aft
er 6
-wk
mel
Tx
61 (
NS)
/ 30
.17±
11.2
6 (1
6-54
) / D
SPS
Non
e / M
ML
/ wri
st /
NS
/N
S / N
S Sa
deh;
Oth
er: z
ero-
cros
sing
mod
e
Surv
ey
No
med
s , D
SPS
Dx,
mel
Tx,
fini
shed
≥1
yr p
rior
to s
tudy
/ No
cont
rol G
rp
96.7
% r
epor
t mel
hel
ped
DSP
S, 9
1.5%
rel
apse
aft
erm
el c
essa
tion
No
valid
atio
n of
AC
Tot
her
than
pt.
repo
rt A
CT
used
onl
yto
aid
initi
al D
x of
DSP
S.O
utco
me
asse
ssed
onl
y by
ques
tionn
aire
, not
AC
T.
Dau
rat (
97)
4C-b
Con
trol
led
clin
ical
tria
l; D
B /
Hot
el r
oom
s se
t up
as la
b /
Ent
ire
24-h
s; 6
D A
CT
BL
, 1D
tem
p B
L, f
light
, 6D
AC
Tpo
stfl
ight
, 1+
1D te
mp
post
flig
ht,
Zop
iclo
ne o
r Pl
aceb
o be
fore
bed
Nts
1-4
pos
t flig
ht
36 (
24)
/ 51.
2±2.
2 / N
orm
al
Tem
p (n
=19
) / A
ctiw
atch
/nd
om w
rist
/ 1
min
/ N
S /
Act
isom
(P.
Den
ise,
Fra
nce)
-sl
eep
visu
ally
sco
red,
cos
inor
for
phas
e
Tem
p; A
CT
: sle
ep d
ur, a
ctiv
i-ty
inde
x, A
CT
acro
phas
e &
ampl
itude
; Moo
d: V
AS
“moo
d”; J
et la
g Sx
VA
S“t
ired
”, “
ill-b
eing
”, “
dige
s-tiv
e”, “
ener
gy”
Hea
lthy,
no
med
s x3
mos
, no
time
zone
trav
el /
Cor
e te
mp
not u
nmas
ked
Zop
iclo
ne im
prov
es A
CT
iden
tifie
d sl
eep
afte
r tr
ans-
mer
idia
n tr
avel
F(1
,22)
=6.
3,p<
.05;
The
gre
ater
the
dysy
n-ch
roni
zatio
n of
CR
s po
st-
flig
ht th
e sh
orte
r th
e sl
eep
dur.
Zop
iclo
ne d
id n
otim
prov
e SB
J je
t lag
AC
Tde
tect
ed b
oth
circ
adia
nsh
ift a
nd s
leep
dis
turb
ance
Daw
son
(93)
4C-b
RC
T, p
aral
lel d
esig
n (b
lindi
ngno
t men
tione
d) /
Lab
/ E
ntir
e24
-hs
appa
rent
ly, 2
Nt D
LM
OB
L(N
t sle
ep)
& c
ore
tem
p,3D
AC
T(N
t wor
k, D
sle
ep)
& c
ore
tem
p, 2
4hs
DL
MO
&co
re te
mp
(sle
ep n
otde
scri
bed)
Ran
dom
ass
ign.
tobr
ight
ligh
t, di
m li
ght,
mel
or
plac
ebo
duri
ng s
hift
wor
k D
s
36 (
36)
/ 23.
6±3.
9 (1
8-30
) /
Nor
mal
N
one
/ Gae
hwile
r / n
dom
wri
st /
30 s
ec /
NS
/ Roo
tm
ean
squa
re (
RM
S) a
ctiv
itytim
es d
ur
Tem
p; m
el; D
LM
O, A
CT
:m
ovem
ent i
ndex
, tot
al e
nerg
y,en
ergy
dur
ing
arou
sal,
ener
gydu
ring
non
-aro
usal
;B
ehav
iora
l: co
gniti
ve p
er-
form
ance
NS
/ NS
/ NS
Bri
ght l
ight
shi
fted
DL
MO
,re
duce
d co
re te
mp
duri
ng D
slee
p, im
prov
ed A
CT
SQ b
et-
ter
than
mel
Tx
or p
lace
bo.
Mel
did
n’t s
hift
DL
MO
, but
impr
oved
sle
ep &
red
uced
core
tem
p so
mew
hat.
AC
Tva
riab
les
show
ed s
igni
f-ic
ant d
iffe
renc
es b
etw
een
light
and
pla
cebo
and
oft
enbe
twee
n lig
ht a
nd m
el T
x du
r-in
g D
sle
ep in
sim
ulat
ed s
hift
wor
k.
Dijk
(32
)
3C
Con
trol
led
clin
ical
tria
l, D
B,
nonr
ando
miz
ed /
Spac
e sh
ut-
tle, p
re, p
ost f
light
/ E
ntir
e 24
hs; A
CT
: 1-2
D 2
mos
pre
flig
ht; 1
-2 D
1 m
o pr
e fl
ight
;0-
7 D
1 w
k pr
e fl
ight
; 10-
16D
in f
light
; 4 D
PSG
in f
light
;5
D A
CT
post
flig
ht; 3
D P
SGpo
st f
light
; 0-3
D o
ther
mea
s-ur
es p
ost f
light
5 (5
) / (
37-4
6) /
norm
al
PSG
, log
, mel
uri
ne, t
emp
core
and
inge
stib
le s
enso
r,ur
inar
y co
rtis
ol /
MM
Lan
dA
ctill
umes
/ nd
om w
rist
/ N
S/ N
S / C
ole/
Kri
pke
Log
; AC
T: S
Ptim
e, T
ST;
neur
obeh
avio
ral A
sses
smen
tB
atte
ry
All
astr
onau
ts /
NS
/ Can
not
dist
ingu
ish
effe
cts
of s
pace
flig
ht f
rom
thos
e of
wor
ksc
hedu
le; s
mal
l sam
ple
Spac
e fl
ight
ass
ocia
ted
w/
redu
ced
AC
TSP
time,
SB
JSQ
, per
form
ance
and
del
ayed
cort
isol
rhy
thm
rel
ativ
e to
sche
dule
d sl
eep.
AC
TSd
urlo
nger
on
PSG
rec
ordi
ng N
t;m
ight
ref
lect
gre
ater
adh
er-
ence
to s
leep
sch
edul
e on
PSG
Nt.
No
bene
fit o
f m
el o
nsl
eep
obse
rved
.
AC
Tde
tect
ed a
ppar
ent b
ias
inPS
G s
leep
mea
sure
men
t
Eis
sa (
131)
5D-a
Obs
erva
tiona
l stu
dy, C
ase
seri
es /
Hom
e / E
ntir
e 24
-hs;
1D A
CT
1D a
mbu
lato
ry B
Pm
onito
ring
46 (
46)
/ 42.
9±21
.8 /
Hyp
erte
nsio
n B
P/ M
ML
/ ndo
m w
rist
/ N
S/ N
S / C
ole
AC
T: W
vs. s
leep
dic
hoto
my
Con
secu
tive
hype
rten
sion
pts
./ P
ossi
ble
dayt
ime
rem
oval
artif
act c
ould
hav
e ov
eres
ti-m
ated
D s
leep
(na
ps)
Est
imat
es o
f ci
rcad
ian
orsl
eep-
indu
ced
BP
redu
ctio
n(“
dipp
ing”
) di
ffer
whe
n “a
ctu-
al s
leep
” is
def
ined
by
AC
Tth
an w
hen
it is
def
ined
by
fixe
d tim
e-of
-D c
rite
ria
Act
igra
ph-i
dent
ifie
d sl
eep
assu
med
to b
e “t
rue”
sle
ep b
yau
thor
s
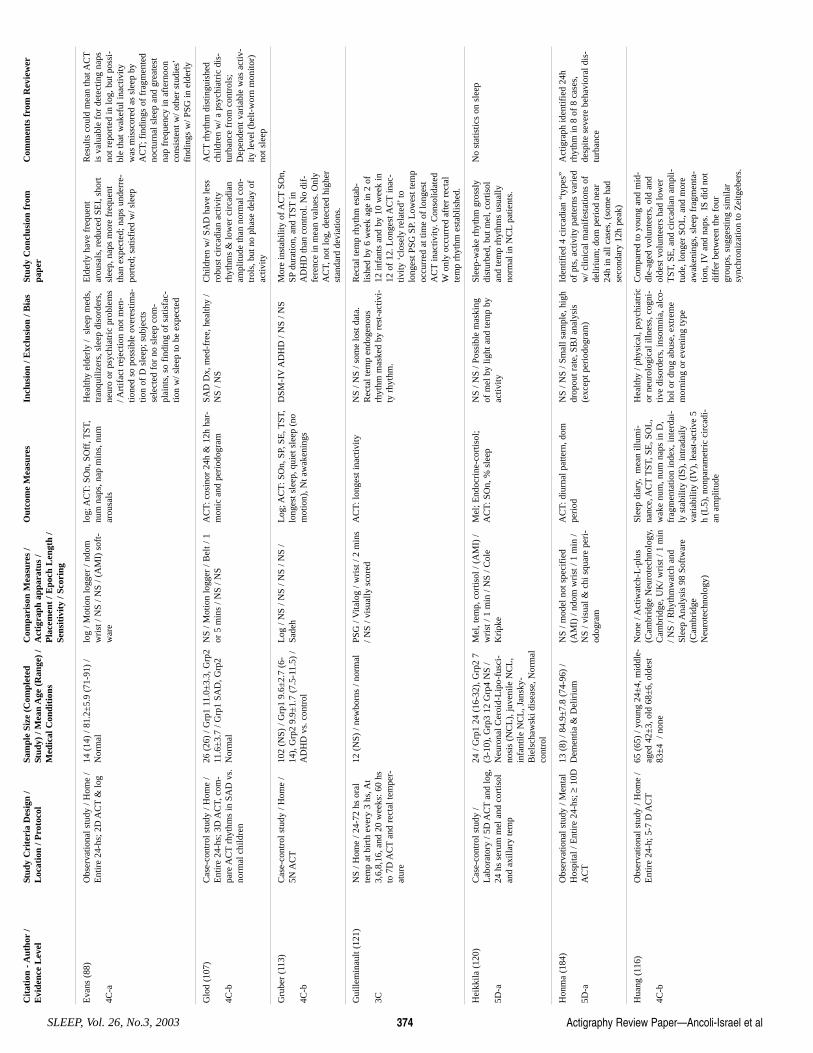
Cit
atio
n - A
utho
r/
Evi
denc
e L
evel
St
udy
Cri
teri
a D
esig
n /
Loc
atio
n / P
roto
col
Sam
ple
Size
(C
ompl
eted
Stud
y) /
Mea
n A
ge (
Ran
ge)
/M
edic
al C
ondi
tion
s
Com
pari
son
Mea
sure
s /
Act
igra
ph a
ppar
atus
/P
lace
men
t / E
poch
Len
gth
/Se
nsit
ivit
y / S
cori
ng
Out
com
e M
easu
res
Incl
usio
n / E
xclu
sion
/ B
ias
Stud
y C
oncl
usio
n fr
ompa
per
Com
men
ts f
rom
Rev
iew
er
Actigraphy Review Paper—Ancoli-Israel et alSLEEP, Vol. 26, No.3, 2003 374
Eva
ns (
88)
4C-a
Obs
erva
tiona
l stu
dy /
Hom
e /
Ent
ire
24-h
s; 2
D A
CT
& lo
g 14
(14
) / 8
1.2±
5.9
(71-
91)
/N
orm
al
log
/ Mot
ion
logg
er /
ndom
wri
st /
NS
/ NS
/ (A
MI)
sof
t-w
are
log;
AC
T: S
On,
SO
ff, T
ST,
num
nap
s, n
ap m
ins,
num
arou
sals
Hea
lthy
elde
rly
/ sl
eep
med
s,tr
anqu
ilize
rs, s
leep
dis
orde
rs,
neur
o or
psy
chia
tric
pro
blem
s/ A
rtif
act r
ejec
tion
not m
en-
tione
d so
pos
sibl
e ov
eres
tima-
tion
of D
sle
ep; s
ubje
cts
sele
cted
for
no
slee
p co
m-
plai
nts,
so
find
ing
of s
atis
fac-
tion
w/ s
leep
to b
e ex
pect
ed
Eld
erly
hav
e fr
eque
ntar
ousa
ls, r
educ
ed S
EI,
sho
rtsl
eep,
nap
s m
ore
freq
uent
than
exp
ecte
d; n
aps
unde
rre-
port
ed; s
atis
fied
w/ s
leep
Res
ults
cou
ld m
ean
that
AC
Tis
val
uabl
e fo
r de
tect
ing
naps
not r
epor
ted
in lo
g, b
ut p
ossi
-bl
e th
at w
akef
ul in
activ
ityw
as m
issc
ored
as
slee
p by
AC
T; f
indi
ngs
of f
ragm
ente
dno
ctur
nal s
leep
and
gre
ates
tna
p fr
eque
ncy
in a
fter
noon
cons
iste
nt w
/ oth
er s
tudi
es’
find
ings
w/ P
SG in
eld
erly
Glo
d (1
07)
4C-b
Cas
e-co
ntro
l stu
dy /
Hom
e /
Ent
ire
24-h
s; 3
D A
CT,
com
-pa
re A
CT
rhyt
hms
in S
AD
vs.
norm
al c
hild
ren
26 (
26)
/ Grp
1 11
.0±
3.3,
Grp
211
.6±
3.7
/ Grp
1 SA
D, G
rp2
Nor
mal
NS
/ Mot
ion
logg
er /
Bel
t / 1
or 5
min
s / N
S / N
S A
CT
: cos
inor
24h
& 1
2h h
ar-
mon
ic a
nd p
erio
dogr
am
SAD
Dx,
med
-fre
e, h
ealth
y /
NS
/ NS
Chi
ldre
n w
/ SA
D h
ave
less
robu
st c
irca
dian
act
ivity
rhyt
hms
& lo
wer
cir
cadi
anam
plitu
de th
an n
orm
al c
on-
trol
s, b
ut n
o ph
ase
dela
y of
activ
ity
AC
Trh
ythm
dis
tingu
ishe
dch
ildre
n w
/ a p
sych
iatr
ic d
is-
turb
ance
fro
m c
ontr
ols;
Dep
ende
nt v
aria
ble
was
act
iv-
ity le
vel (
belt-
wor
n m
onito
r)no
t sle
ep
Gru
ber
(113
)
4C-b
Cas
e-co
ntro
l stu
dy /
Hom
e /
5N A
CT
102
(NS)
/ G
rp1
9.6±
2.7
(6-
14),
Grp
2 9.
9±1.
7 (7
.5-1
1.5)
/A
DH
D v
s. c
ontr
ol
Log
/ N
S / N
S / N
S / N
S /
Sade
h L
og; A
CT
: SO
n, S
P, S
E, T
ST,
long
est s
leep
, qui
et s
leep
(no
mot
ion)
, Nt a
wak
enin
gs
DSM
-IV
AD
HD
/ N
S / N
S M
ore
inst
abili
ty o
f AC
TSO
n,SP
dura
tion,
and
TST
inA
DH
D th
an c
ontr
ol. N
o di
f-fe
renc
e in
mea
n va
lues
. Onl
yA
CT,
not
log,
det
ecte
d hi
gher
stan
dard
dev
iatio
ns.
Gui
llem
inau
lt (1
21)
3C
NS
/ Hom
e / 2
4-72
hs
oral
tem
p at
bir
th e
very
3 h
s, A
t3,
6,8,
16, a
nd 2
0 w
eeks
: 60
hsto
7D
AC
Tan
d re
ctal
tem
per-
atur
e
12 (
NS)
/ ne
wbo
rns
/ nor
mal
PS
G /
Vita
log
/ wri
st /
2 m
ins
/ NS
/ vis
ually
sco
red
AC
T: l
onge
st in
activ
ity
NS
/ NS
/ som
e lo
st d
ata.
Rec
tal t
emp
endo
geno
usrh
ythm
mas
ked
by r
est-
activ
i-ty
rhy
thm
.
Rec
tal t
emp
rhyt
hm e
stab
-lis
hed
by 6
wee
k ag
e in
2 o
f12
infa
nts
and
by 1
0 w
eek
in12
of
12. L
onge
st A
CT
inac
-tiv
ity ‘
clos
ely
rela
ted’
tolo
nges
t PSG
SP.
Low
est t
emp
occu
rred
at t
ime
of lo
nges
tA
CT
inac
tivity
. Con
solid
ated
Won
ly o
ccur
red
afte
r re
ctal
tem
p rh
ythm
est
ablis
hed.
Hei
kkila
(12
0)
5D-a
Cas
e-co
ntro
l stu
dy /
Lab
orat
ory
/ 5D
AC
Tan
d lo
g,24
hs
seru
m m
el a
nd c
ortis
olan
d ax
illar
y te
mp
24 /
Grp
1 24
(16
-32)
, Grp
2 7
(3-1
0), G
rp3
12 G
rp4
NS
/N
euro
nal C
eroi
d-L
ipo-
fusc
i-no
sis
(NC
L),
juve
nile
NC
L,
infa
ntile
NC
L, J
ansk
y-B
iels
chaw
ski d
isea
se, N
orm
alco
ntro
l
Mel
, tem
p, c
ortis
ol /
(AM
I) /
wri
st /
1 m
in /
NS
/ Col
eK
ripk
e
Mel
; End
ocri
ne-c
ortis
ol;
AC
T: S
On,
% s
leep
N
S / N
S / P
ossi
ble
mas
king
of m
el b
y lig
ht a
nd te
mp
byac
tivity
Slee
p-w
ake
rhyt
hm g
ross
lydi
stur
bed,
but
mel
, cor
tisol
and
tem
p rh
ythm
s us
ually
norm
al in
NC
Lpa
tient
s.
No
stat
istic
s on
sle
ep
Hon
ma
(184
)
5D-a
Obs
erva
tiona
l stu
dy /
Men
tal
Hos
pita
l / E
ntir
e 24
-hs;
≥10
DA
CT
13 (
8) /
84.9
±7.
8 (7
4-96
) /
Dem
entia
& D
elir
ium
N
S / m
odel
not
spe
cifi
ed(A
MI)
/ nd
om w
rist
/ 1
min
/N
S / v
isua
l & c
hi s
quar
e pe
ri-
odog
ram
AC
T: d
iurn
al p
atte
rn, d
ompe
riod
N
S / N
S / S
mal
l sam
ple,
hig
hdr
opou
t rat
e, S
BJ
anal
ysis
(exc
ept p
erio
dogr
am)
Iden
tifie
d 4
circ
adia
n “t
ypes
”of
pts
, act
ivity
pat
tern
s va
ried
w/ c
linic
al m
anif
esta
tions
of
delir
ium
; dom
per
iod
near
24h
in a
ll ca
ses,
(so
me
had
seco
ndar
y 12
h pe
ak)
Act
igra
ph id
entif
ied
24h
rhyt
hm in
8 o
f 8
case
s,de
spite
sev
ere
beha
vior
al d
is-
turb
ance
Hua
ng (
116)
4C-b
Obs
erva
tiona
l stu
dy /
Hom
e /
Ent
ire
24-h
; 5-7
D A
CT
65 (
65)
/ you
ng 2
4±4,
mid
dle-
aged
42±
3, o
ld 6
8±6,
old
est
83±
4 /
none
Non
e / A
ctiw
atch
-L-p
lus
(Cam
brid
ge N
euro
tech
nolo
gy,
Cam
brid
ge, U
K/ w
rist
/ 1
min
/ NS
/ Rhy
thm
wat
ch a
ndSl
eep
Ana
lysi
s 98
Sof
twar
e(C
ambr
idge
Neu
rote
chno
logy
)
Slee
p di
ary,
mea
n ill
umi-
nanc
e, A
CT
TST
, SE
, SO
L,
wak
e nu
m, n
um n
aps
in D
,fr
agm
enta
tion
inde
x, in
terd
ai-
ly s
tabi
lity
(IS)
, int
rada
ilyva
riab
ility
(IV
), le
ast-
activ
e 5
h (L
5), n
onpa
ram
etri
c ci
rcad
i-an
am
plitu
de
Hea
lthy
/ phy
sica
l, ps
ychi
atri
cor
neu
rolo
gica
l illn
ess,
cog
ni-
tive
diso
rder
s, in
som
nia,
alc
o-ho
l or
drug
abu
se, e
xtre
me
mor
ning
or
even
ing
type
Com
pare
d to
you
ng a
nd m
id-
dle-
aged
vol
unte
ers,
old
and
olde
st v
olun
teer
s ha
d lo
wer
TST
, SE
, and
cir
cadi
an a
mpl
i-tu
de, l
onge
r SO
L, a
nd m
ore
awak
enin
gs, s
leep
fra
gmen
ta-
tion,
IV
and
naps
. IS
did
not
diff
er b
etw
een
the
four
grou
ps, s
ugge
stin
g si
mila
rsy
nchr
oniz
atio
n to
Zei
tgeb
ers.
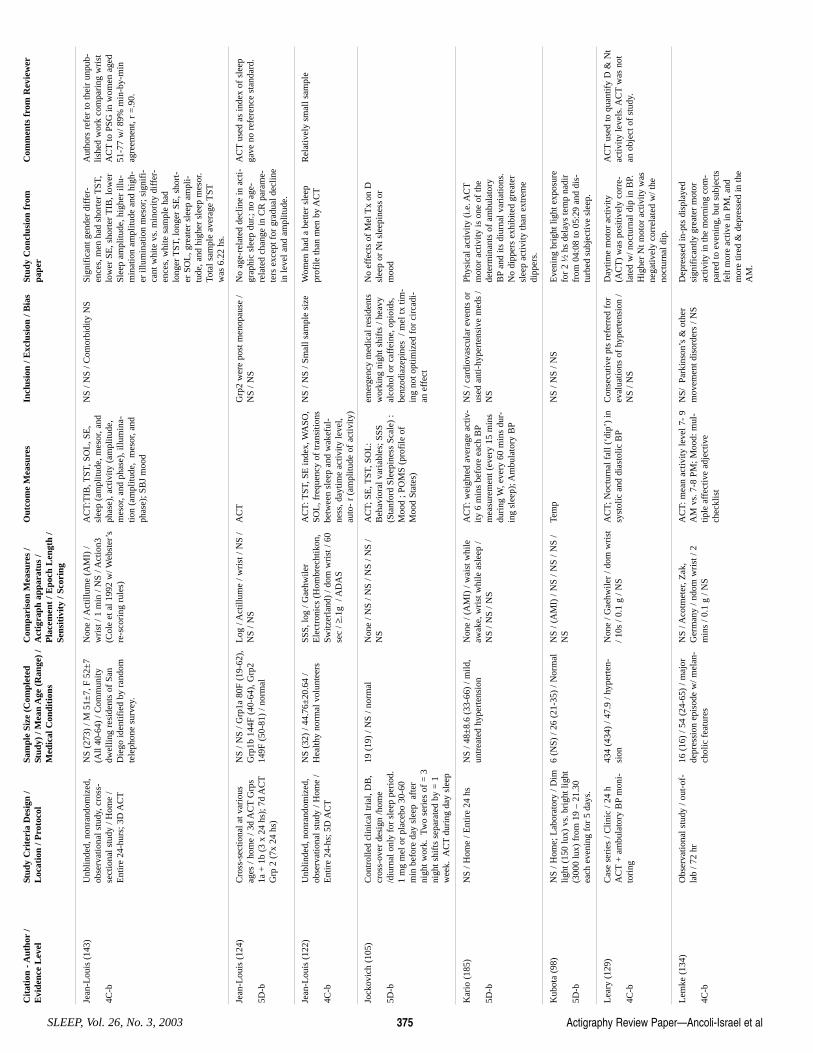
Cit
atio
n - A
utho
r/
Evi
denc
e L
evel
St
udy
Cri
teri
a D
esig
n /
Loc
atio
n / P
roto
col
Sam
ple
Size
(C
ompl
eted
Stud
y) /
Mea
n A
ge (
Ran
ge)
/M
edic
al C
ondi
tion
s
Com
pari
son
Mea
sure
s /
Act
igra
ph a
ppar
atus
/P
lace
men
t / E
poch
Len
gth
/Se
nsit
ivit
y / S
cori
ng
Out
com
e M
easu
res
Incl
usio
n / E
xclu
sion
/ B
ias
Stud
y C
oncl
usio
n fr
ompa
per
Com
men
ts f
rom
Rev
iew
er
Actigraphy Review Paper—Ancoli-Israel et alSLEEP, Vol. 26, No. 3, 2003 375
Jean
-Lou
is (
143)
4C-b
Unb
linde
d, n
onra
ndom
ized
,ob
serv
atio
nal s
tudy
, cro
ss-
sect
iona
l stu
dy /
Hom
e /
Ent
ire
24-h
urs;
3D
AC
T
NS
(273
) / M
51±
7, F
52±
7(A
ll 40
-64)
/ C
omm
unity
dwel
ling
resi
dent
s of
San
Die
go id
entif
ied
by r
ando
mte
leph
one
surv
ey.
Non
e / A
ctill
ume
(AM
I) /
wri
st /
1 m
in /
NS
/ Act
ion3
(Col
e et
al 1
992
w/ W
ebst
er’s
re-s
cori
ng r
ules
)
AC
T:T
IB, T
ST, S
OL
, SE
,sl
eep
(am
plitu
de, m
esor
, and
phas
e), a
ctiv
ity (
ampl
itude
,m
esor
, and
pha
se),
illu
min
a-tio
n (a
mpl
itude
, m
esor
, and
phas
e); S
BJ
moo
d
NS
/ NS
/ Com
orbi
dity
NS
Sign
ific
ant g
ende
r di
ffer
-en
ces,
men
had
sho
rter
TST
,lo
wer
SE
, sho
rter
TIB
, low
erSl
eep
ampl
itude
, hig
her
illu-
min
atio
n am
plitu
de a
nd h
igh-
er il
lum
inat
ion
mes
or; s
igni
fi-
cant
whi
te v
s. m
inor
ity d
iffe
r-en
ces,
whi
te s
ampl
e ha
dlo
nger
TST
, lon
ger
SE, s
hort
-er
SO
L, g
reat
er s
leep
am
pli-
tude
, and
hig
her
slee
p m
esor
.To
tal s
ampl
e av
erag
e T
STw
as 6
.22
hs.
Aut
hors
ref
er to
thei
r un
pub-
lishe
d w
ork
com
pari
ng w
rist
AC
Tto
PSG
in w
omen
age
d51
-77
w/ 8
9% m
in-b
y-m
inag
reem
ent,
r =
.90.
Jean
-Lou
is (
124)
5D-b
Cro
ss-s
ectio
nal a
t var
ious
ages
/ ho
me
/ 3d
AC
TG
rps
1a +
1b
(3 x
24
hs);
7d
AC
TG
rp 2
(7x
24
hs)
NS
/ NS
/ Grp
1a 8
0F (
19-6
2),
Grp
1b 1
44F
(40-
64),
Grp
214
9F (
50-8
1) /
norm
al
Log
/ A
ctill
ume
/ wri
st /
NS
/N
S / N
S A
CT
Grp
2 w
ere
post
men
opau
se /
NS
/ NS
No
age-
rela
ted
decl
ine
in a
cti-
grap
hic
slee
p du
r.; n
o ag
e-re
late
d ch
ange
in C
R p
aram
e-te
rs e
xcep
t for
gra
dual
dec
line
in le
vel a
nd a
mpl
itude
.
AC
Tus
ed a
s in
dex
of s
leep
gave
no
refe
renc
e st
anda
rd.
Jean
-Lou
is (
122)
4C-b
Unb
linde
d, n
onra
ndom
ized
,ob
serv
atio
nal s
tudy
/ H
ome
/E
ntir
e 24
-hs;
5D
AC
T
NS
(32)
/ 44
.76±
20.6
4 /
Hea
lthy
norm
al v
olun
teer
s SS
S, lo
g / G
aehw
iler
Ele
ctro
nics
(H
ombr
echt
ikon
,Sw
itzer
land
) / d
om w
rist
/ 60
sec
/ ≥.1
g /
AD
AS
AC
T: T
ST, S
E in
dex,
WA
SO,
SOL
, fre
quen
cy o
f tr
ansi
tions
betw
een
slee
p an
d w
akef
ul-
ness
, day
time
activ
ity le
vel,
auto
- r
(am
plitu
de o
f ac
tivity
)
NS
/ NS
/ Sm
all s
ampl
e si
ze
Wom
en h
ad a
bet
ter
slee
ppr
ofile
than
men
by
AC
TR
elat
ivel
y sm
all s
ampl
e
Jock
ovic
h (1
05)
5D-b
Con
trol
led
clin
ical
tria
l, D
B,
cros
s-ov
er d
esig
n /h
ome
/diu
rnal
onl
y fo
r sl
eep
peri
od.
1 m
g m
el o
r pl
aceb
o 30
-60
min
bef
ore
day
slee
p a
fter
nigh
t wor
k. T
wo
seri
es o
f =
3ni
ght s
hift
s se
para
ted
by =
1w
eek.
AC
Tdu
ring
day
sle
ep
19 (
19)
/ NS
/ nor
mal
N
one
/ NS
/ NS
/ NS
/ NS
/N
S
AC
T; S
E, T
ST, S
OL
:B
ehav
iora
l var
iabl
es; S
SS
(Sta
nfor
d Sl
eepi
ness
Sca
le)
:M
ood
; PO
MS
(pro
file
of
Moo
d St
ates
)
emer
genc
y m
edic
al r
esid
ents
wor
king
nig
ht s
hift
s / h
eavy
alco
hol o
r ca
ffei
ne, o
pioi
ds,
benz
odia
zepi
nes
/ m
el tx
tim
-in
g no
t opt
imiz
ed f
or c
irca
di-
an e
ffec
t
No
effe
cts
of M
el T
x on
Dsl
eep
or N
t sle
epin
ess
orm
ood
Kar
io (
185)
5D-b
NS
/ Hom
e / E
ntir
e 24
hs
NS
/ 48±
8.6
(33-
66)
/ mild
,un
trea
ted
hype
rten
sion
N
one
/ (A
MI)
/ w
aist
whi
leaw
ake,
wri
st w
hile
asl
eep
/N
S / N
S / N
S
AC
T: w
eigh
ted
aver
age
activ
-ity
6 m
ins
befo
re e
ach
BP
mea
sure
men
t (ev
ery
15 m
ins
duri
ng W
, eve
ry 6
0 m
ins
dur-
ing
slee
p); A
mbu
lato
ry B
P
NS
/ car
diov
ascu
lar
even
ts o
rus
ed a
nti-
hype
rten
sive
med
s /
NS
Phys
ical
act
ivity
(i.e
. AC
Tm
otor
act
ivity
is o
ne o
f th
ede
term
inan
ts o
f am
bula
tory
BP
and
its d
iurn
al v
aria
tions
.N
o di
pper
s ex
hibi
ted
grea
ter
slee
p ac
tivity
than
ext
rem
edi
pper
s.
Kub
ota
(98)
5D-b
NS
/ Hom
e; L
abor
ator
y / D
imlig
ht (
150
lux)
vs.
bri
ght l
ight
(300
0 lu
x) f
rom
19
– 21
.30
each
eve
ning
for
5 d
ays.
6 (N
S) /
26 (
21-3
5) /
Nor
mal
N
S / (
AM
I) /
NS
/ NS
/ NS
/N
S
Tem
p N
S / N
S / N
S E
veni
ng b
righ
t lig
ht e
xpos
ure
for
2 ½
hs
dela
ys te
mp
nadi
rfr
om 0
4:08
to 0
5:29
and
dis
-tu
rbed
sub
ject
ive
slee
p.
Lea
ry (
129)
4C-b
Cas
e se
ries
/ C
linic
/ 24
hA
CT
+ a
mbu
lato
ry B
Pm
oni-
tori
ng
434
(434
) / 4
7.9
/ hyp
erte
n-si
on
Non
e / G
aehw
iler
/ dom
wri
st/ 1
0s /
0.1
g / N
S A
CT;
Noc
turn
al f
all (
‘dip
’) in
syst
olic
and
dia
stol
ic B
PC
onse
cutiv
e pt
s re
ferr
ed f
orev
alua
tions
of
hype
rten
sion
/N
S / N
S
Day
time
mot
or a
ctiv
ity(A
CT
) w
as p
ositi
vely
cor
re-
late
d w
/ noc
turn
al d
ip in
BP.
Hig
her
Nt m
otor
act
ivity
was
nega
tivel
y co
rrel
ated
w/ t
heno
ctur
nal d
ip.
AC
Tus
ed to
qua
ntif
y D
& N
tac
tivity
leve
ls. A
CT
was
not
an o
bjec
t of
stud
y.
Lem
ke (
134)
4C-b
Obs
erva
tiona
l stu
dy /
out-
of-
lab
/ 72
hr
16 (
16)
/ 54
(24-
65)
/ maj
orde
pres
sion
epi
sode
w/ m
elan
-ch
olic
fea
ture
s
NS
/ Aco
tmet
er, Z
ak,
Ger
man
y / n
dom
wri
st /
2m
ins
/ 0.1
g /
NS
AC
T: m
ean
activ
ity le
vel 7
- 9
AM
vs.
7-8
PM
; Moo
d: m
ul-
tiple
aff
ectiv
e ad
ject
ive
chec
klis
t
NS/
Par
kins
on’s
& o
ther
mov
emen
t dis
orde
rs /
NS
Dep
ress
ed in
-pts
dis
play
edsi
gnif
ican
tly g
reat
er m
otor
activ
ity in
the
mor
ning
com
-pa
red
to e
veni
ng, b
ut s
ubje
cts
felt
mor
e ac
tive
in P
M, a
ndm
ore
tired
& d
epre
ssed
in th
eA
M.
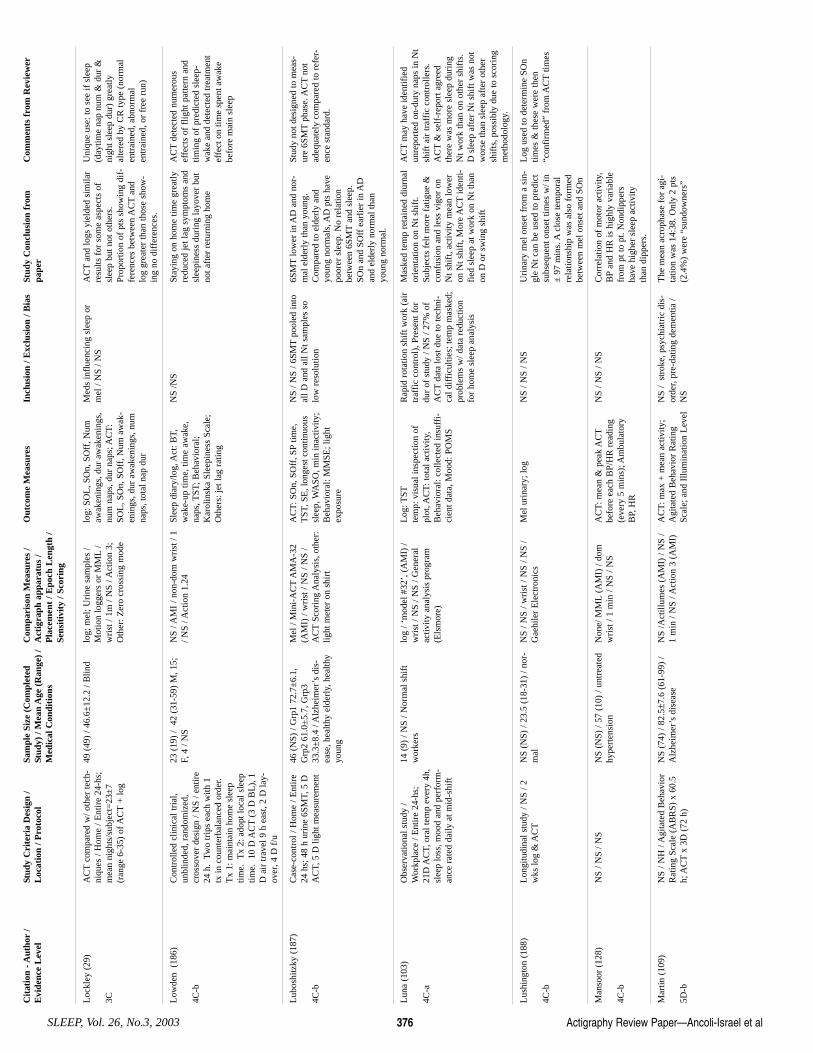
Cit
atio
n - A
utho
r/
Evi
denc
e L
evel
St
udy
Cri
teri
a D
esig
n /
Loc
atio
n / P
roto
col
Sam
ple
Size
(C
ompl
eted
Stud
y) /
Mea
n A
ge (
Ran
ge)
/M
edic
al C
ondi
tion
s
Com
pari
son
Mea
sure
s /
Act
igra
ph a
ppar
atus
/P
lace
men
t / E
poch
Len
gth
/Se
nsit
ivit
y / S
cori
ng
Out
com
e M
easu
res
Incl
usio
n / E
xclu
sion
/ B
ias
Stud
y C
oncl
usio
n fr
ompa
per
Com
men
ts f
rom
Rev
iew
er
Actigraphy Review Paper—Ancoli-Israel et alSLEEP, Vol. 26, No.3, 2003 376
Loc
kley
(29
)
3C
AC
Tco
mpa
red
w/ o
ther
tech
-ni
ques
/ H
ome
/ Ent
ire
24-h
s;m
ean
nigh
ts/s
ubje
ct=
23±
7(r
ange
6-3
5) o
f AC
T+
log
49 (
49)
/ 46.
6±12
.2 /
Blin
d lo
g; m
el; U
rine
sam
ples
/M
otio
n lo
gger
s or
MM
L/
wri
st /
1m /
NS
/ Act
ion
3;O
ther
: Zer
o cr
ossi
ng m
ode
log:
SO
L, S
On,
SO
ff, N
umaw
aken
ings
, dur
aw
aken
ings
,nu
m n
aps,
dur
nap
s; A
CT
:SO
L, S
On,
SO
ff, N
um a
wak
-en
ings
, dur
aw
aken
ings
, num
naps
, tot
al n
ap d
ur
Med
s in
flue
ncin
g sl
eep
orm
el /
NS
/ NS
AC
Tan
d lo
gs y
ield
ed s
imila
rre
sults
for
som
e as
pect
s of
slee
p bu
t not
oth
ers.
Prop
ortio
n of
pts
sho
win
g di
f-fe
renc
es b
etw
een
AC
Tan
dlo
g gr
eate
r th
an th
ose
show
-in
g no
dif
fere
nces
.
Uni
que
use:
to s
ee if
sle
ep(d
aytim
e na
p nu
m &
dur
&ni
ght s
leep
dur
) gr
eatly
alte
red
by C
R ty
pe (
norm
alen
trai
ned,
abn
orm
alen
trai
ned,
or
free
run
)
Low
den
(18
6)
4C-b
Con
trol
led
clin
ical
tria
l,un
blin
ded,
ran
dom
ized
,cr
osso
ver
desi
gn /
NS
/ ent
ire
24 h
. Tw
o tr
ips
each
with
1tx
in c
ount
erba
lanc
ed o
rder
.T
x 1:
mai
ntai
n ho
me
slee
ptim
e. T
x 2:
ado
pt lo
cal s
leep
time.
10
D A
CT
(3 D
BL
), 1
D a
ir tr
avel
9 h
eas
t, 2
D la
y-ov
er, 4
D f
/u
23 (
19)
/ 42
(31
-59)
M, 1
5;F,
4 /
NS
NS
/ AM
I / n
on-d
om w
rist
/ 1
/ NS
/ Act
ion
1.24
Sl
eep
diar
y/lo
g, A
ct: B
T,w
ake-
up ti
me,
tim
e aw
ake,
naps
, TST
; Beh
avio
ral;
Kar
olin
ska
Slee
pine
ss S
cale
;O
ther
s: je
t lag
rat
ing
NS
/NS
Stay
ing
on h
ome
time
grea
tlyre
duce
d je
t lag
sym
ptom
s an
dsl
eepi
ness
dur
ing
layo
ver
but
not a
fter
ret
urni
ng h
ome
AC
Tde
tect
ed n
umer
ous
effe
cts
of f
light
pat
tern
and
timin
g of
pre
dict
ed s
leep
-w
ake
and
dete
cted
trea
tmen
tef
fect
on
time
spen
t aw
ake
befo
re m
ain
slee
p
Lub
oshi
tzky
(18
7)
4C-b
Cas
e-co
ntro
l / H
ome
/ Ent
ire
24 h
s; 4
8 h
urin
e 6S
MT,
5 D
AC
T, 5
D li
ght m
easu
rem
ent
46 (
NS)
/ G
rp1
72.7
±6.
1,G
rp2
61.0
±5.
7, G
rp3
33.3
±8.
4 / A
lzhe
imer
’s d
is-
ease
, hea
lthy
elde
rly,
hea
lthy
youn
g
Mel
/ M
ini-
AC
TA
MA
-32
(AM
I) /
wri
st /
NS
/ NS
/A
CT
Scor
ing
Ana
lysi
s, o
ther
:lig
ht m
eter
on
shir
t
AC
T: S
On,
SO
ff, S
Ptim
e,T
ST, S
E, l
onge
st c
ontin
uous
slee
p, W
ASO
, min
inac
tivity
;B
ehav
iora
l: M
MSE
; lig
htex
posu
re
NS
/ NS
/ 6SM
Tpo
oled
into
all D
and
all
Nt s
ampl
es s
olo
w r
esol
utio
n
6SM
Tlo
wer
in A
D a
nd n
or-
mal
eld
erly
than
you
ng.
Com
pare
d to
eld
erly
and
youn
g no
rmal
s, A
D p
ts h
ave
poor
er s
leep
. No
rela
tion
betw
een
6SM
Tan
d sl
eep.
SOn
and
SOff
ear
lier
in A
Dan
d el
derl
y no
rmal
than
youn
g no
rmal
.
Stud
y no
t des
igne
d to
mea
s-ur
e 6S
MT
phas
e. A
CT
not
adeq
uate
ly c
ompa
red
to r
efer
-en
ce s
tand
ard.
Lun
a (1
03)
4C-a
Obs
erva
tiona
l stu
dy /
Wor
kpla
ce /
Ent
ire
24-h
s;21
D A
CT,
ora
l tem
p ev
ery
4h,
slee
p lo
ss, m
ood
and
perf
orm
-an
ce r
ated
dai
ly a
t mid
-shi
ft
14 (
9) /
NS
/ Nor
mal
shi
ftw
orke
rs
log
/ ‘m
odel
#32
’, (
AM
I) /
wri
st /
NS
/ NS
/ Gen
eral
activ
ity a
naly
sis
prog
ram
(Els
mor
e)
Log
: TST
tem
p: v
isua
l ins
pect
ion
ofpl
ot, A
CT
: tot
al a
ctiv
ity,
Beh
avio
ral:
colle
cted
insu
ffi-
cien
t dat
a, M
ood:
PO
MS
Rap
id r
otat
ion
shif
t wor
k (a
irtr
affi
c co
ntro
l), P
rese
nt f
ordu
r of
stu
dy /
NS
/ 27%
of
AC
Tda
ta lo
st d
ue to
tech
ni-
cal d
iffi
culti
es; t
emp
mas
ked;
prob
lem
s w
/ dat
a re
duct
ion
for
hom
e sl
eep
anal
ysis
Mas
ked
tem
p re
tain
ed d
iurn
alor
ient
atio
n on
Nt s
hift
.Su
bjec
ts f
elt m
ore
fatig
ue &
conf
usio
n an
d le
ss v
igor
on
Nt s
hift
, act
ivity
mea
n lo
wer
on N
t shi
ft, M
ore
AC
Tid
enti-
fied
sle
ep a
t wor
k on
Nt t
han
on D
or
swin
g sh
ift
AC
Tm
ay h
ave
iden
tifie
dun
repo
rted
on-
duty
nap
s in
Nt
shif
t air
traf
fic
cont
rolle
rs.
AC
T&
sel
f-re
port
agr
eed
ther
e w
as m
ore
slee
p du
ring
Nt w
ork
than
on
othe
r sh
ifts
.D
sle
ep a
fter
Nt s
hift
was
not
wor
se th
an s
leep
aft
er o
ther
shif
ts, p
ossi
bly
due
to s
cori
ngm
etho
dolo
gy.
Lus
hing
ton
(188
)
4C-b
Lon
gitu
dina
l stu
dy /
NS
/ 2w
ks lo
g &
AC
TN
S (N
S) /
23.5
(18
-31)
/ no
r-m
al
NS
/ NS
/ wri
st /
NS
/ NS
/G
aehi
ler
Ele
ctro
nics
M
el u
rina
ry; l
og
NS
/ NS
/ NS
Uri
nary
mel
ons
et f
rom
a s
in-
gle
Nt c
an b
e us
ed to
pre
dict
subs
eque
nt o
nset
tim
es w
/ in
± 9
7 m
ins.
Acl
ose
tem
pora
lre
latio
nshi
p w
as a
lso
form
edbe
twee
n m
el o
nset
and
SO
n
Log
use
d to
det
erm
ine
SOn
times
& th
ese
wer
e th
en“c
onfi
rmed
” fr
om A
CT
times
Man
soor
(12
8)
4C-b
NS
/ NS
/ NS
NS
(NS)
/ 57
(10
) / u
ntre
ated
hype
rten
sion
N
one/
MM
L(A
MI)
/ do
mw
rist
/ 1
min
/ N
S / N
S A
CT
: mea
n &
pea
k A
CT
befo
re e
ach
BP/
HR
rea
ding
(eve
ry 5
min
s); A
mbu
lato
ryB
P, H
R
NS
/ NS
/ NS
Cor
rela
tion
of m
otor
act
ivity
,B
Pan
d H
R is
hig
hly
vari
able
from
pt t
o pt
. Non
dipp
ers
have
hig
her
slee
p ac
tivity
than
dip
pers
.
Mar
tin (
109)
5D-b
NS
/ NH
/ A
gita
ted
Beh
avio
rR
atin
g Sc
ale
(AB
RS)
x 6
0.5
h; A
CT
x 3D
(72
h)
NS
(74)
/ 82
.5±7
.6 (
61-9
9) /
Alz
heim
er’s
dis
ease
N
S /A
ctill
umes
(A
MI)
/ N
S /
1 m
in /
NS
/ Act
ion
3 (A
MI)
A
CT
: max
+ m
ean
activ
ity;
Agi
tate
d B
ehav
ior
Rat
ing
Scal
e; a
nd I
llum
inat
ion
Lev
el
NS
/ st
roke
, psy
chia
tric
dis
-or
der,
pre-
datin
g de
men
tia /
NS
The
mea
n ac
roph
ase
for
agi-
tatio
n w
as 1
4:38
. Onl
y 2
pts
(2.4
%)
wer
e “s
undo
wne
rs”
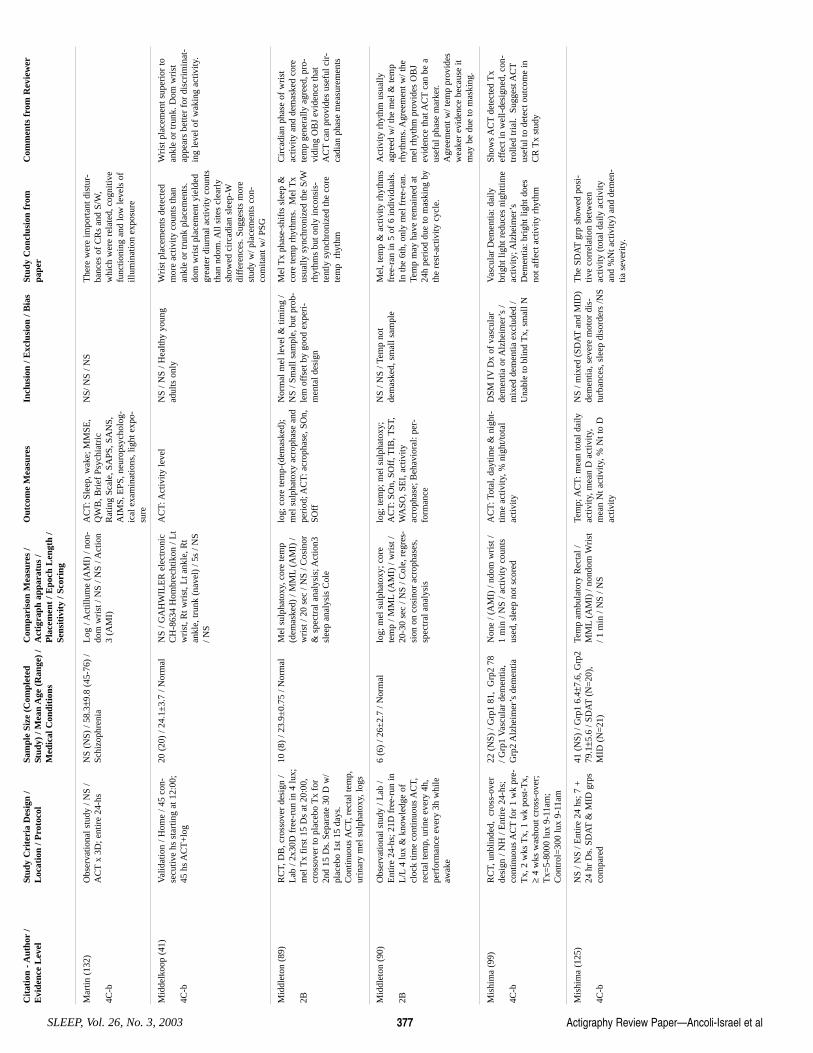
Cit
atio
n - A
utho
r/
Evi
denc
e L
evel
St
udy
Cri
teri
a D
esig
n /
Loc
atio
n / P
roto
col
Sam
ple
Size
(C
ompl
eted
Stud
y) /
Mea
n A
ge (
Ran
ge)
/M
edic
al C
ondi
tion
s
Com
pari
son
Mea
sure
s /
Act
igra
ph a
ppar
atus
/P
lace
men
t / E
poch
Len
gth
/Se
nsit
ivit
y / S
cori
ng
Out
com
e M
easu
res
Incl
usio
n / E
xclu
sion
/ B
ias
Stud
y C
oncl
usio
n fr
ompa
per
Com
men
ts f
rom
Rev
iew
er
Actigraphy Review Paper—Ancoli-Israel et alSLEEP, Vol. 26, No. 3, 2003 377
Mar
tin (
132)
4C-b
Obs
erva
tiona
l stu
dy /
NS
/A
CT
x 3D
; ent
ire
24-h
s N
S (N
S) /
58.3±9
.8 (
45-7
6) /
Schi
zoph
reni
a L
og /
Act
illum
e (A
MI)
/ no
n-do
m w
rist
/ N
S / N
S / A
ctio
n3
(AM
I)
AC
T: S
leep
, wak
e; M
MSE
,Q
WB
, Bri
ef P
sych
iatr
icR
atin
g Sc
ale,
SA
PS, S
AN
S,A
IMS,
EPS
, neu
rops
ycho
log-
ical
exa
min
atio
ns, l
ight
exp
o-su
re
NS/
NS
/ NS
The
re w
ere
impo
rtan
t dis
tur-
banc
es o
f C
Rs
and
S/W
,w
hich
wer
e re
late
d, c
ogni
tive
func
tioni
ng a
nd lo
w le
vels
of
illum
inat
ion
expo
sure
Mid
delk
oop
(41)
4C-b
Val
idat
ion
/ Hom
e / 4
5 co
n-se
cutiv
e hs
sta
rtin
g at
12:
00;
45 h
s A
CT
+lo
g
20 (
20)
/ 24.
1±3.
7 / N
orm
al
NS
/ GA
HW
ILE
R e
lect
roni
cC
H-8
634
Hom
brec
htik
on /
Lt
wri
st, R
t wri
st, L
t ank
le, R
tan
kle,
trun
k (n
avel
) / 5
s / N
S/ N
S
AC
T: A
ctiv
ity le
vel
NS
/ NS
/ Hea
lthy
youn
gad
ults
onl
y W
rist
pla
cem
ents
det
ecte
dm
ore
activ
ity c
ount
s th
anan
kle
or tr
unk
plac
emen
ts.
dom
wri
st p
lace
men
t yie
lded
grea
ter
diur
nal a
ctiv
ity c
ount
sth
an n
dom
. All
site
s cl
earl
ysh
owed
cir
cadi
an s
leep
-Wdi
ffer
ence
s. S
ugge
sts
mor
est
udy
w/ p
lace
men
ts c
on-
com
itant
w/ P
SG
Wri
st p
lace
men
t sup
erio
r to
ankl
e or
trun
k. D
om w
rist
appe
ars
bette
r fo
r di
scri
min
at-
ing
leve
l of
wak
ing
activ
ity.
Mid
dlet
on (
89)
2B
RC
T, D
B, c
ross
over
des
ign
/L
ab /
2x30
D f
ree-
run
in 4
lux;
mel
Tx
firs
t 15
Ds
at 2
0:00
,cr
osso
ver
to p
lace
bo T
x fo
r2n
d 15
Ds.
Sep
arat
e 30
D w
/pl
aceb
o 1s
t 15
days
.C
ontin
uous
AC
T, r
ecta
l tem
p,ur
inar
y m
el s
ulph
atox
y, lo
gs
10 (
8) /
23.9
±0.
75 /
Nor
mal
M
el s
ulph
atox
y, c
ore
tem
p(d
emas
ked)
/ M
ML
(AM
I) /
wri
st /
20 s
ec /
NS
/ Cos
inor
& s
pect
ral a
naly
sis;
Act
ion3
slee
p an
alys
is C
ole
log;
cor
e te
mp-
(dem
aske
d);
mel
sul
phat
oxy
acro
phas
e an
dpe
riod
; AC
T: a
crop
hase
, SO
n,SO
ff
Nor
mal
mel
leve
l & ti
min
g /
NS
/ Sm
all s
ampl
e, b
ut p
rob-
lem
off
set b
y go
od e
xper
i-m
enta
l des
ign
Mel
Tx
phas
e-sh
ifts
sle
ep &
core
tem
p rh
ythm
s. M
el T
xus
ually
syn
chro
nize
d th
e S/
Wrh
ythm
s bu
t onl
y in
cons
is-
tent
ly s
ynch
roni
zed
the
core
tem
p r
hyth
m
Cir
cadi
an p
hase
of
wri
stac
tivity
and
dem
aske
d co
rete
mp
gene
rally
agr
eed,
pro
-vi
ding
OB
J ev
iden
ce th
atA
CT
can
prov
ides
use
ful c
ir-
cadi
an p
hase
mea
sure
men
ts
Mid
dlet
on (
90)
2B
Obs
erva
tiona
l stu
dy /
Lab
/E
ntir
e 24
-hs;
21D
fre
e-ru
n in
L/L
4 lu
x &
kno
wle
dge
ofcl
ock
time
cont
inuo
us A
CT,
rect
al te
mp,
uri
ne e
very
4h,
perf
orm
ance
eve
ry 3
h w
hile
awak
e
6 (6
) / 2
6±2.
7 / N
orm
al
log;
mel
sul
phat
oxy;
cor
ete
mp
/ MM
L(A
MI)
/ w
rist
/20
-30
sec
/ NS
/ Col
e, r
egre
s-si
on o
n co
sino
r ac
roph
ases
,sp
ectr
al a
naly
sis
log;
tem
p; m
el s
ulph
atox
y;A
CT
: SO
n, S
Off
, TIB
, TST
,W
ASO
, SE
I, a
ctiv
ityac
roph
ase;
Beh
avio
ral:
per-
form
ance
NS
/ NS
/ Tem
p no
tde
mas
ked,
sm
all s
ampl
e M
el, t
emp
& a
ctiv
ity r
hyth
ms
free
-ran
in 5
of
6 in
divi
dual
s.In
the
6th,
onl
y m
el f
ree-
ran.
Tem
p m
ay h
ave
rem
aine
d at
24h
peri
od d
ue to
mas
king
by
the
rest
-act
ivity
cyc
le.
Act
ivity
rhy
thm
usu
ally
agre
ed w
/ the
mel
& te
mp
rhyt
hms.
Agr
eem
ent w
/ the
mel
rhy
thm
pro
vide
s O
BJ
evid
ence
that
AC
Tca
n be
aus
eful
pha
se m
arke
r.A
gree
men
t w/ t
emp
prov
ides
wea
ker
evid
ence
bec
ause
itm
ay b
e du
e to
mas
king
.
Mis
him
a (9
9)
4C-b
RC
T, u
nblin
ded,
cro
ss-o
ver
desi
gn /
NH
/ E
ntir
e 24
-hs;
cont
inuo
us A
CT
for
1 w
k pr
e-T
x, 2
wks
Tx,
1 w
k po
st-T
x,≥
4 w
ks w
asho
ut c
ross
-ove
r;T
x=5-
8000
lux
9-11
am;
Con
trol
=30
0 lu
x 9-
11am
22 (
NS)
/ G
rp1
81,
Grp
2 78
/ Grp
1 V
ascu
lar
dem
entia
,G
rp2
Alz
heim
er’s
dem
entia
Non
e / (
AM
I) /
ndom
wri
st /
1 m
in /
NS
/ act
ivity
cou
nts
used
, sle
ep n
ot s
core
d
AC
T: T
otal
, day
time
& n
ight
-tim
e ac
tivity
, % n
ight
/tota
lac
tivity
DSM
IV
Dx
of v
ascu
lar
dem
entia
or A
lzhe
imer
’s /
mix
ed d
emen
tia e
xclu
ded
/U
nabl
e to
blin
d T
x, s
mal
l N
Vas
cula
r D
emen
tia: d
aily
brig
ht li
ght r
educ
es n
ight
time
activ
ity; A
lzhe
imer
’sD
emen
tia: b
righ
t lig
ht d
oes
not a
ffec
t act
ivity
rhy
thm
Show
s A
CT
dete
cted
Tx
effe
ct in
wel
l-de
sign
ed, c
on-
trol
led
tria
l. S
ugge
st A
CT
usef
ul to
det
ect o
utco
me
inC
R T
x st
udy
Mis
him
a (1
25)
4C-b
NS
/ NS
/ Ent
ire
24 h
s; 7
+24
hr
Ds.
SD
AT
& M
ID g
rps
com
pare
d
41 (
NS)
/ G
rp1
6.4±
7.6,
Grp
279
.1±5
.6 /
SDA
T(N
=20
),M
ID (
N=
21)
Tem
p am
bula
tory
Rec
tal /
MM
L(A
MI)
/ no
ndom
Wri
st/ 1
min
/ N
S / N
S
Tem
p; A
CT
: mea
n to
tal d
aily
activ
ity, m
ean
D a
ctiv
ity,
mea
n N
t act
ivity
, % N
t to
Dac
tivity
NS
/ mix
ed (
SDA
Tan
d M
ID)
dem
entia
, sev
ere
mot
or d
is-
turb
ance
s, s
leep
dis
orde
rs /N
S
The
SD
AT
grp
show
ed p
osi-
tive
corr
elat
ion
betw
een
activ
ity (
tota
l dai
ly a
ctiv
ityan
d %
Nt a
ctiv
ity)
and
dem
en-
tia s
ever
ity.
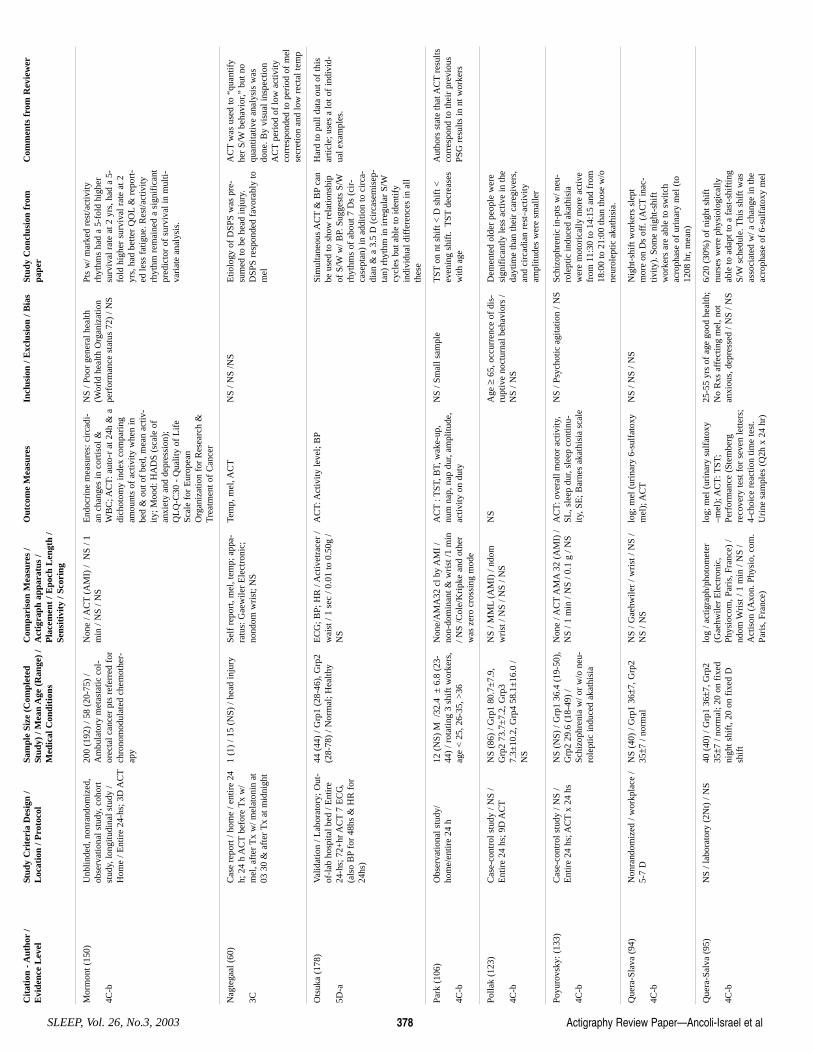
Cit
atio
n - A
utho
r/
Evi
denc
e L
evel
St
udy
Cri
teri
a D
esig
n /
Loc
atio
n / P
roto
col
Sam
ple
Size
(C
ompl
eted
Stud
y) /
Mea
n A
ge (
Ran
ge)
/M
edic
al C
ondi
tion
s
Com
pari
son
Mea
sure
s /
Act
igra
ph a
ppar
atus
/P
lace
men
t / E
poch
Len
gth
/Se
nsit
ivit
y / S
cori
ng
Out
com
e M
easu
res
Incl
usio
n / E
xclu
sion
/ B
ias
Stud
y C
oncl
usio
n fr
ompa
per
Com
men
ts f
rom
Rev
iew
er
Actigraphy Review Paper—Ancoli-Israel et alSLEEP, Vol. 26, No.3, 2003 378
Mor
mon
t (15
0)
4C-b
Unb
linde
d, n
onra
ndom
ized
,ob
serv
atio
nal s
tudy
, coh
ort
stud
y, lo
ngitu
dina
l stu
dy /
Hom
e / E
ntir
e 24
-hs;
3D
AC
T
200
(192
) / 5
8 (2
0-75
) /
Am
bula
tory
met
asta
tic c
ol-
orec
tal c
ance
r pt
s re
ferr
ed f
orch
rono
mod
ulat
ed c
hem
othe
r-ap
y
Non
e / A
CT
(AM
I) /
NS
/ 1m
in /
NS
/ NS
End
ocri
ne m
easu
res:
cir
cadi
-an
cha
nges
in c
ortis
ol &
WB
C; A
CT
: aut
o-r
at 2
4h &
adi
chot
omy
inde
x co
mpa
ring
amou
nts
of a
ctiv
ity w
hen
inbe
d &
out
of
bed,
mea
n ac
tiv-
ity; M
ood:
HA
DS
(sca
le o
fan
xiet
y an
d de
pres
sion
);Q
LQ
-C30
- Q
ualit
y of
Lif
eSc
ale
for
Eur
opea
nO
rgan
izat
ion
for
Res
earc
h &
Tre
atm
ent o
f C
ance
r
NS
/ Poo
r ge
nera
l hea
lth(W
orld
hea
lth O
rgan
izat
ion
perf
orm
ance
sta
tus
72)
/ NS
Pts
w/ m
arke
d re
st/a
ctiv
ityrh
ythm
s ha
d a
5-fo
ld h
ighe
rsu
rviv
al r
ate
at 2
yrs
, had
a 5
-fo
ld h
ighe
r su
rviv
al r
ate
at 2
yrs,
had
bet
ter
QO
L&
rep
ort-
ed le
ss f
atig
ue. R
est/a
ctiv
ityrh
ythm
rem
aine
d a
sign
ific
ant
pred
icto
r of
sur
viva
l in
mul
ti-va
riat
e an
alys
is.
Nag
tega
al (
60)
3C
Cas
e re
port
/ ho
me
/ ent
ire
24h;
24
h A
CT
befo
re T
x w
/m
el, a
fter
Tx
w/ m
elat
onin
at
03 3
0 &
aft
er T
x at
mid
nigh
t
1 (1
) / 1
5 (N
S) /
head
inju
ry
Self
rep
ort,
mel
, tem
p; a
ppa-
ratu
s: G
aew
iler
Ele
ctro
nic;
nond
om w
rist
; NS
Tem
p, m
el, A
CT
NS
/ NS
/NS
Etio
logy
of
DSP
S w
as p
re-
sum
ed to
be
head
inju
ry.
DSP
S re
spon
ded
favo
rabl
y to
mel
AC
Tw
as u
sed
to “
quan
tify
her
S/W
beha
vior
,” b
ut n
oqu
antit
ativ
e an
alys
is w
asdo
ne. B
y vi
sual
insp
ectio
nA
CT
peri
od o
f lo
w a
ctiv
ityco
rres
pond
ed to
per
iod
of m
else
cret
ion
and
low
rec
tal t
emp
Ots
uka
(178
)
5D-a
Val
idat
ion
/ Lab
orat
ory;
Out
-of
-lab
hos
pita
l bed
/ E
ntir
e24
-hs;
72+
hr A
CT
7 E
CG
,(a
lso
BP
for
48hs
& H
R f
or24
hs)
44 (
44)
/ Grp
1 (2
8-46
), G
rp2
(28-
78)
/ Nor
mal
; Hea
lthy
EC
G; B
P; H
R /
Act
ivet
race
r /
wai
st /
1 se
c / 0
.01
to 0
.50g
/N
S
AC
T: A
ctiv
ity le
vel;
BP
Sim
ulta
neou
s A
CT
& B
Pca
nbe
use
d to
sho
w r
elat
ions
hip
of S
/Ww
/ BP.
Sug
gest
s S/
Wrh
ythm
s of
abo
ut 7
Ds
(cir
-ca
sept
an)
in a
dditi
on to
cir
ca-
dian
& a
3.5
D (
circ
asem
isep
-ta
n) r
hyth
m in
irre
gula
r S/
Wcy
cles
but
abl
e to
iden
tify
indi
vidu
al d
iffe
renc
es in
all
thes
e
Har
d to
pul
l dat
a ou
t of
this
artic
le; u
ses
a lo
t of
indi
vid-
ual e
xam
ples
.
Park
(10
6)
4C-b
Obs
erva
tiona
l stu
dy/
hom
e/en
tire
24 h
12
(N
S) M
/32
.4 ±
6.8
(23
-44
) / r
otat
ing
3 sh
ift w
orke
rs,
age
< 2
5, 2
6-35
, >36
Non
e/A
MA
32 c
l by
AM
I /
non-
dom
inan
t & w
rist
/1 m
in/ N
S /C
ole/
Kri
pke
and
othe
rw
as z
ero
cros
sing
mod
e
AC
T: T
ST, B
T, w
ake-
up,
num
nap
, nap
dur
, am
plitu
de,
activ
ity o
n du
ty
NS
/ Sm
all s
ampl
e T
STon
nt s
hift
< D
shi
ft <
even
ing
shif
t. T
STde
crea
ses
with
age
Aut
hors
sta
te th
at A
CT
resu
ltsco
rres
pond
to th
eir
prev
ious
PSG
res
ults
in n
t wor
kers
Polla
k (1
23)
4C-b
Cas
e-co
ntro
l stu
dy /
NS
/E
ntir
e 24
hs;
9D
AC
TN
S (8
6) /
Grp
1 80
.7±
7.9,
Grp
2 73
.7±
7.2,
Grp
37.
3±10
.2, G
rp4
58.1
±16
.0 /
NS
NS
/ MM
L(A
MI)
/ nd
omw
rist
/ N
S / N
S / N
S N
S A
ge ≥
65, o
ccur
renc
e of
dis
-ru
ptiv
e no
ctur
nal b
ehav
iors
/N
S / N
S
Dem
ente
d ol
der
peop
le w
ere
sign
ific
antly
less
act
ive
in th
eda
ytim
e th
an th
eir
care
give
rs,
and
circ
adia
n re
st–a
ctiv
ityam
plitu
des
wer
e sm
alle
r
Poyu
rovs
ky: (
133)
4C-b
Cas
e-co
ntro
l stu
dy /
NS
/E
ntir
e 24
hs;
AC
Tx
24 h
s N
S (N
S) /
Grp
1 36
.4 (
19-5
0),
Grp
2 29
.6 (
18-4
9) /
Schi
zoph
reni
a w
/ or
w/o
neu
-ro
lept
ic in
duce
d ak
athi
sia
Non
e / A
CT
AM
A32
(A
MI)
/N
S / 1
min
/ N
S / 0
.1 g
/ N
S A
CT
: ove
rall
mot
or a
ctiv
ity,
SL, s
leep
dur
, sle
ep c
ontin
u-ity
, SE
; Bar
nes
akat
hisi
a sc
ale
NS
/ Psy
chot
ic a
gita
tion
/ NS
Schi
zoph
reni
c in
-pts
w/ n
eu-
role
ptic
indu
ced
akat
hisi
aw
ere
mot
oric
ally
mor
e ac
tive
from
11:
30 to
14:
15 a
nd f
rom
18:0
0 to
21:
00 th
an th
ose
w/o
neur
olep
tic a
kath
isia
.
Que
ra-S
lava
(94
)
4C-b
Non
rand
omiz
ed /
wor
kpla
ce /
5-7
D
NS
(40)
/ G
rp1
36±7
, Grp
235±7
/ no
rmal
N
S / G
aehw
iler
/ wri
st /
NS
/N
S / N
S lo
g; m
el (
urin
ary
6-su
lfat
oxy
mel
); A
CT
NS
/ NS
/ NS
Nig
ht-s
hift
wor
kers
sle
ptm
ore
on D
s of
f. (
AC
Tin
ac-
tivity
). S
ome
nigh
t-sh
ift
wor
kers
are
abl
e to
sw
itch
acro
phas
e of
uri
nary
mel
(to
1208
hr,
mea
n)
Que
ra-S
alva
(95
)
4C-b
NS
/ lab
orat
ory
(2N
t) /
NS
40 (
40)
/ Grp
1 36±7
, Grp
235±7
/ no
rmal
; 20
on f
ixed
nigh
t shi
ft, 2
0 on
fix
ed D
shif
t
log
/ act
igra
ph/p
hoto
met
er(G
aehw
iler
Ele
ctro
nic,
Phys
ioco
m, P
aris
, Fra
nce)
/nd
om W
rist
/ 1
min
/ N
S /
Act
ison
(A
xon.
Phy
sio,
com
.Pa
ris,
Fra
nce)
log;
mel
(ur
inar
y su
lfat
oxy
–mel
); A
CT
: TST
;Pe
rfor
man
ce (
Stem
berg
reco
very
test
for
sev
en le
tters
;4-
choi
ce r
eact
ion
time
test
.U
rine
sam
ples
(Q
2h x
24
hr)
25-5
5 yr
s of
age
goo
d he
alth
;N
o R
xs a
ffec
ting
mel
, not
anxi
ous,
dep
ress
ed /
NS
/ NS
6/20
(30
%)
of n
ight
shi
ftnu
rses
wer
e ph
ysio
logi
cally
able
to a
dapt
to a
fas
t-sh
iftin
gS/
Wsc
hedu
le. T
his
shif
t was
asso
ciat
ed w
/ a c
hang
e in
the
acro
phas
e of
6-s
ulfa
toxy
mel
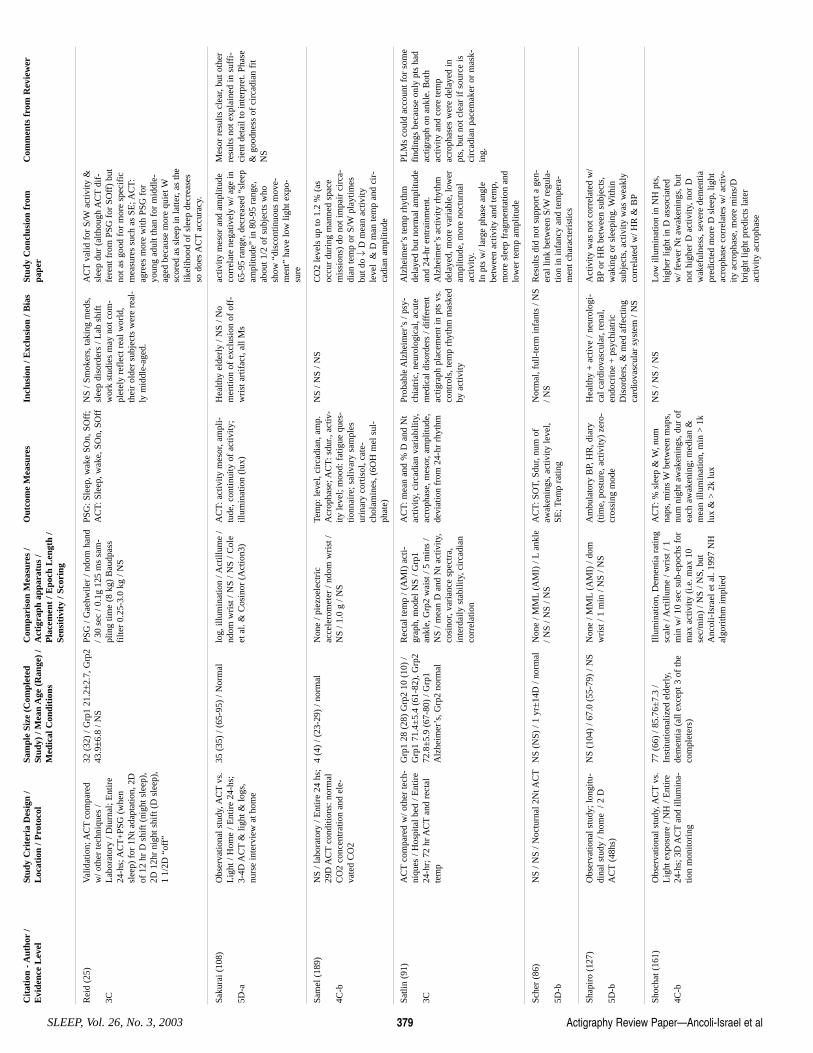
Cit
atio
n - A
utho
r/
Evi
denc
e L
evel
St
udy
Cri
teri
a D
esig
n /
Loc
atio
n / P
roto
col
Sam
ple
Size
(C
ompl
eted
Stud
y) /
Mea
n A
ge (
Ran
ge)
/M
edic
al C
ondi
tion
s
Com
pari
son
Mea
sure
s /
Act
igra
ph a
ppar
atus
/P
lace
men
t / E
poch
Len
gth
/Se
nsit
ivit
y / S
cori
ng
Out
com
e M
easu
res
Incl
usio
n / E
xclu
sion
/ B
ias
Stud
y C
oncl
usio
n fr
ompa
per
Com
men
ts f
rom
Rev
iew
er
Actigraphy Review Paper—Ancoli-Israel et alSLEEP, Vol. 26, No. 3, 2003 379
Rei
d (2
5)
3C
Val
idat
ion;
AC
Tco
mpa
red
w/ o
ther
tech
niqu
es /
Lab
orat
ory
/ Diu
rnal
; Ent
ire
24-h
s; A
CT
+PS
G (
whe
nsl
eep)
for
1N
t ada
ptat
ion,
2D
of 1
2 hr
D s
hift
(ni
ght s
leep
),2D
12h
r ni
ght s
hift
(D
sle
ep),
1 1/
2D “
off”
32 (
32)
/ Grp
1 21
.2±2
.7, G
rp2
43.9±6
.8 /
NS
PSG
/ G
aehw
iler
/ ndo
m h
and
/ 30
sec
/ 0.1
g 12
5 m
s sa
m-
plin
g tim
e (8
kg)
Bau
dpas
sfi
lter
0.25
-3.0
kg
/ NS
PSG
: Sle
ep, w
ake
SOn,
SO
ff;
AC
T: S
leep
, wak
e, S
On,
SO
ff
NS
/ Sm
oker
s, ta
king
med
s,sl
eep
diso
rder
s / L
ab s
hift
wor
k st
udie
s m
ay n
ot c
om-
plet
ely
refl
ect r
eal w
orld
,th
eir
olde
r su
bjec
ts w
ere
real
-ly
mid
dle-
aged
.
AC
Tva
lid f
or S
/Wac
tivity
&sl
eep
dur
(alth
ough
AC
Tdi
f-fe
rent
fro
m P
SG f
or S
Off
) bu
tno
t as
good
for
mor
e sp
ecif
icm
easu
res
such
as
SE; A
CT
:ag
rees
mor
e w
ith P
SG f
oryo
ung
adul
t tha
n fo
r m
iddl
e-ag
ed b
ecau
se m
ore
quie
t Wsc
ored
as
slee
p in
latte
r, as
the
likel
ihoo
d of
sle
ep d
ecre
ases
so d
oes
AC
Tac
cura
cy.
Saku
rai (
108)
5D-a
Obs
erva
tiona
l stu
dy, A
CT
vs.
Lig
ht /
Hom
e / E
ntir
e 24
-hs;
3-4D
AC
T&
ligh
t & lo
gs,
nurs
e in
terv
iew
at h
ome
35 (
35)
/ (65
-95)
/ N
orm
al
log,
illu
min
atio
n / A
ctill
ume
/nd
om w
rist
/ N
S / N
S / C
ole
et a
l. &
Cos
inor
(A
ctio
n3)
AC
T: a
ctiv
ity m
esor
, am
pli-
tude
, con
tinui
ty o
f ac
tivity
;ill
umin
atio
n (l
ux)
Hea
lthy
elde
rly
/ NS
/ No
men
tion
of e
xclu
sion
of
off-
wri
st a
rtif
act,
all M
s
activ
ity m
esor
and
am
plitu
deco
rrel
ate
nega
tivel
y w
/ age
in65
-95
rang
e, d
ecre
ased
“sl
eep
ampl
itude
” in
80-
95 r
ange
,ab
out 1
/2 o
f su
bjec
ts w
hosh
ow “
disc
ontin
uous
mov
e-m
ent”
hav
e lo
w li
ght e
xpo-
sure
Mes
or r
esul
ts c
lear
, but
oth
erre
sults
not
exp
lain
ed in
suf
fi-
cien
t det
ail t
o in
terp
ret.
Phas
e&
goo
dnes
s of
cir
cadi
an f
itN
S
Sam
el (
189)
4C-b
NS
/ lab
orat
ory
/ Ent
ire
24 h
s;29
D A
CT
cond
ition
s: n
orm
alC
O2
conc
entr
atio
n an
d el
e-va
ted
CO
2
4 (4
) / (
23-2
9) /
norm
al
Non
e / p
iezo
elec
tric
acce
lero
met
er /
ndom
wri
st /
NS
/ 1.0
g /
NS
Tem
p: le
vel,
circ
adia
n, a
mp.
Acr
opha
se; A
CT
: sdu
r., a
ctiv
-ity
leve
l; m
ood:
fat
igue
que
s-tio
nnai
re; s
aliv
ary
sam
ples
urin
ary
cort
isol
, cat
e-ch
olam
ines
, (6O
H m
el s
ul-
phat
e)
NS
/ NS
/ NS
CO
2 le
vels
up
to 1
.2 %
(as
occu
r du
ring
man
ned
spac
em
issi
ons)
do
not i
mpa
ir c
irca
-di
an te
mp
or S
/Wpl
aytim
esbu
t do ↓
D m
ean
activ
ityle
vel
& D
man
tem
p an
d ci
r-ca
dian
am
plitu
de
Satli
n (9
1)
3C
AC
Tco
mpa
red
w/ o
ther
tech
-ni
ques
/ H
ospi
tal b
ed /
Ent
ire
24-h
r; 7
2 hr
AC
Tan
d re
ctal
tem
p
Grp
1 28
(28
) G
rp2
10 (
10)
/G
rp1
71.4
±5.
4 (6
1-82
), G
rp2
72.8
±5.
9 (6
7-80
) / G
rp1
Alz
heim
er’s
, Grp
2 no
rmal
Rec
tal t
emp
/ (A
MI)
act
i-gr
aph,
mod
el N
S / G
rp1
ankl
e, G
rp2
wai
st /
5 m
ins
/N
S / m
ean
D a
nd N
t act
ivity
,co
sino
r, va
rian
ce s
pect
ra,
inte
rdai
ly s
tabi
lity,
cir
cadi
anco
rrel
atio
n
AC
T: m
ean
and
% D
and
Nt
activ
ity, c
irca
dian
var
iabi
lity,
acro
phas
e, m
esor
, am
plitu
de,
devi
atio
n fr
om 2
4-hr
rhy
thm
Prob
able
Alz
heim
er’s
/ ps
y-ch
iatr
ic, n
euro
logi
cal,
acut
em
edic
al d
isor
ders
/ di
ffer
ent
actig
raph
pla
cem
ent i
n pt
s vs
.co
ntro
ls, t
emp
rhyt
hm m
aske
dby
act
ivity
Alz
heim
er’s
tem
p rh
ythm
dela
yed
but n
orm
al a
mpl
itude
and
24-h
r en
trai
nmen
t.A
lzhe
imer
’s a
ctiv
ity r
hyth
mde
laye
d, m
ore
vari
able
, low
eram
plitu
de, m
ore
noct
urna
lac
tivity
.In
pts
w/ l
arge
pha
se a
ngle
betw
een
activ
ity a
nd te
mp,
mor
e sl
eep
frag
men
tatio
n an
dlo
wer
tem
p am
plitu
de
PLM
s co
uld
acco
unt f
or s
ome
find
ings
bec
ause
onl
y pt
s ha
dac
tigra
ph o
n an
kle.
Bot
hac
tivity
and
cor
e te
mp
acro
phas
es w
ere
dela
yed
inpt
s, b
ut n
ot c
lear
if s
ourc
e is
circ
adia
n pa
cem
aker
or
mas
k-in
g.
Sche
r (8
6)
5D-b
NS
/ NS
/ Noc
turn
al 2
Nt A
CT
NS
(NS)
/ 1
yr±
14D
/ no
rmal
N
one
/ MM
L(A
MI)
/ L
ankl
e/ N
S / N
S / N
S A
CT
: SO
T, S
dur,
num
of
awak
enin
gs, a
ctiv
ity le
vel,
SE; T
emp
ratin
g
Nor
mal
, ful
l-te
rm in
fant
s / N
S/ N
S R
esul
ts d
id n
ot s
uppo
rt a
gen
-er
al li
nk b
etw
een
S/W
regu
la-
tion
in in
fanc
y an
d te
mpe
ra-
men
t cha
ract
eris
tics
Shap
iro
(127
)
5D-b
Obs
erva
tiona
l stu
dy; l
ongi
tu-
dina
l stu
dy /
hom
e /
2 D
AC
T(4
8hs)
NS
(104
) / 6
7.0
(55-
79)
/ NS
Non
e / M
ML
(AM
I) /
dom
wri
st /
1 m
in /
NS
/ NS
Am
bula
tory
BP,
HR
, dia
ry(t
ime,
pos
ture
, act
ivity
) ze
ro-
cros
sing
mod
e
Hea
lthy
+ a
ctiv
e / n
euro
logi
-ca
l car
diov
ascu
lar,
rena
l,en
docr
ine
+ p
sych
iatr
icD
isor
ders
, & m
ed a
ffec
ting
card
iova
scul
ar s
yste
m /
NS
Act
ivity
was
not
cor
rela
ted
w/
BP
or H
R b
etw
een
subj
ects
,w
akin
g or
sle
epin
g. W
ithin
subj
ects
, act
ivity
was
wea
kly
corr
elat
ed w
/ HR
& B
P
Shoc
hat (
161)
4C-b
Obs
erva
tiona
l stu
dy, A
CT
vs.
Lig
ht e
xpos
ure
/ NH
/ E
ntir
e24
-hs;
3D
AC
Tan
d ill
umin
a-tio
n m
onito
ring
77 (
66)
/ 85.
76±
7.3
/In
stitu
tiona
lized
eld
erly
,de
men
tia (
all e
xcep
t 3 o
f th
eco
mpl
eter
s)
Illu
min
atio
n, D
emen
tia r
atin
gsc
ale
/ Act
illum
e / w
rist
/ 1
min
w/ 1
0 se
c su
b-ep
ochs
for
max
act
ivity
(i.e
. max
10
sec/
min
) / N
S / N
S, b
utA
ncol
i-Is
rael
et a
l. 19
97 N
Hal
gori
thm
impl
ied
AC
T: %
sle
ep &
W, n
umna
ps, m
ins
Wbe
twee
n m
aps,
num
nig
ht a
wak
enin
gs, d
ur o
fea
ch a
wak
enin
g; m
edia
n &
mea
n ill
umin
atio
n, m
in >
1k
lux
& >
2k
lux
NS
/ NS
/ NS
Low
illu
min
atio
n in
NH
pts
,hi
gher
ligh
t in
D a
ssoc
iate
dw
/ few
er N
t aw
aken
ings
, but
not h
ighe
r D
act
ivity
, nor
Dw
akef
ulne
ss, s
ever
e de
men
tiapr
edic
ted
mor
e D
sle
ep, l
ight
acro
phas
e co
rrel
ates
w/ a
ctiv
-ity
acr
opha
se, m
ore
min
s/D
brig
ht li
ght p
redi
cts
late
rac
tivity
acr
opha
se
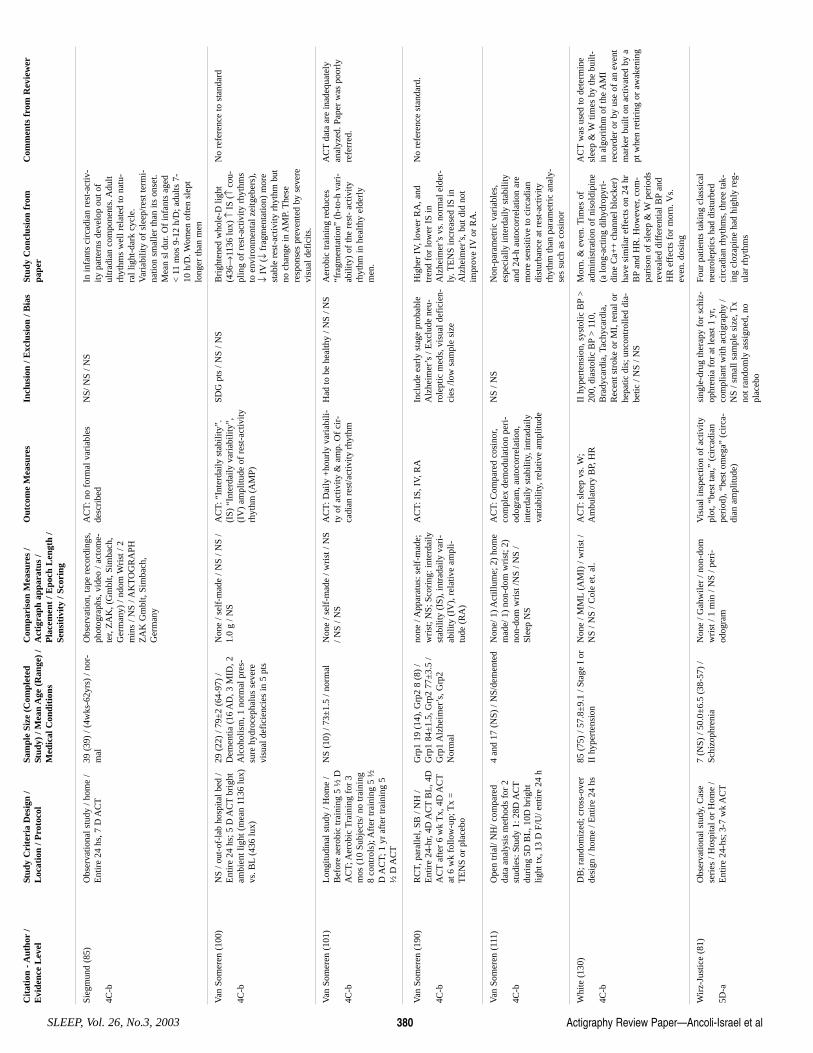
Cit
atio
n - A
utho
r/
Evi
denc
e L
evel
St
udy
Cri
teri
a D
esig
n /
Loc
atio
n / P
roto
col
Sam
ple
Size
(C
ompl
eted
Stud
y) /
Mea
n A
ge (
Ran
ge)
/M
edic
al C
ondi
tion
s
Com
pari
son
Mea
sure
s /
Act
igra
ph a
ppar
atus
/P
lace
men
t / E
poch
Len
gth
/Se
nsit
ivit
y / S
cori
ng
Out
com
e M
easu
res
Incl
usio
n / E
xclu
sion
/ B
ias
Stud
y C
oncl
usio
n fr
ompa
per
Com
men
ts f
rom
Rev
iew
er
Actigraphy Review Paper—Ancoli-Israel et alSLEEP, Vol. 26, No.3, 2003 380
Sieg
mun
d (8
5)
4C-b
Obs
erva
tiona
l stu
dy /
hom
e /
Ent
ire
24 h
s, 7
D A
CT
39 (
39)
/ (4w
ks-6
2yrs
) / n
or-
mal
O
bser
vatio
n, ta
pe r
ecor
ding
s,ph
otog
raph
s, v
ideo
/ ac
tom
e-te
r, Z
AK
, (G
mbl
t, Si
mba
ch,
Ger
man
y) /
ndom
Wri
st /
2m
ins
/ NS
/ AK
TO
GR
APH
ZA
K G
mbl
t, Si
mba
ch,
Ger
man
y
AC
T: n
o fo
rmal
var
iabl
esde
scri
bed
NS/
NS
/ NS
In in
fant
s ci
rcad
ian
rest
-act
iv-
ity p
atte
rns
deve
lop
out o
ful
trad
ian
com
pone
nts.
Adu
ltrh
ythm
s w
ell r
elat
ed to
nat
u-ra
l lig
ht-d
ark
cycl
e.V
aria
bilit
y of
sle
ep/r
est t
erm
i-na
tion
smal
ler
than
its
onse
t.M
ean
sl d
ur. O
f in
fant
s ag
ed<
11
mos
9-1
2 h/
D; a
dults
7-
10 h
/D. W
omen
oft
en s
lept
long
er th
an m
en
Van
Som
eren
(10
0)
4C-b
NS
/ out
-of-
lab
hosp
ital b
ed /
Ent
ire
24 h
s; 5
D A
CT
brig
htam
bien
t lig
ht (
mea
n 11
36 lu
x)vs
. BL
(436
lux)
29 (
22)
/ 79±
2 (6
4-97
) /
Dem
entia
(16
AD
, 3 M
ID, 2
Alc
ohol
ism
, 1 n
orm
al p
res-
sure
hyd
roce
phal
us s
ever
evi
sual
def
icie
ncie
s in
5 p
ts
Non
e / s
elf-
mad
e / N
S / N
S /
1.0
g / N
S
AC
T: “
Inte
rdai
ly s
tabi
lity”
.(I
S) “
Inte
rdai
ly v
aria
bilit
y”,
(IV
) am
plitu
de o
f re
st-a
ctiv
ityrh
ythm
(A
MP)
SDG
pts
/ N
S / N
S B
righ
tene
d w
hole
-D li
ght
(436→
1136
lux)
↑IS
(↑
cou-
plin
g of
res
t-ac
tivity
rhy
thm
sto
env
iron
men
tal z
eitg
eber
s),
↓IV
(↓fr
agm
enta
tion)
mor
est
able
res
t-ac
tivity
rhy
thm
but
no c
hang
e in
AM
P. T
hese
resp
onse
s pr
even
ted
by s
ever
evi
sual
def
icits
.
No
refe
renc
e to
sta
ndar
d
Van
Som
eren
(10
1)
4C-b
Lon
gitu
dina
l stu
dy /
Hom
e /
Bef
ore
aero
bic
trai
ning
5 ½
DA
CT;
Aer
obic
Tra
inin
g fo
r 3
mos
(10
Sub
ject
s/ n
o tr
aini
ng8
cont
rols
); A
fter
trai
ning
5 ½
D A
CT;
1 y
r af
ter
trai
ning
5½
D A
CT
NS
(10)
/ 73
±1.
5 / n
orm
al
Non
e / s
elf-
mad
e / w
rist
/ N
S/ N
S / N
S A
CT
: Dai
ly +
hour
ly v
aria
bili-
ty o
f ac
tivity
& a
mp.
Of
cir-
cadi
an r
est/a
ctiv
ity r
hyth
m
Had
to b
e he
alth
y / N
S / N
S A
erob
ic tr
aini
ng r
educ
es“f
ragm
enta
tion”
(h-
to-h
var
i-ab
ility
) of
the
rest
- ac
tivity
rhyt
hm in
hea
lthy
elde
rly
men
.
AC
Tda
ta a
re in
adeq
uate
lyan
alyz
ed. P
aper
was
poo
rly
refe
rred
.
Van
Som
eren
(19
0)
4C-b
RC
T, p
aral
lel,
SB /
NH
/E
ntir
e 24
-hr,
4D A
CT
BL
, 4D
AC
Taf
ter
6 w
k T
x, 4
D A
CT
at 6
wk
follo
w-u
p; T
x =
TE
NS
or p
lace
bo
Grp
1 19
(14
), G
rp2
8 (8
) /
Grp
1 84
±1.
5, G
rp2
77±
3.5
/G
rp1
Alz
heim
er’s
, Grp
2N
orm
al
none
/ A
ppar
atus
: sel
f-m
ade;
wri
st; N
S; S
cori
ng: i
nter
daily
stab
ility
(IS
), in
trad
aily
var
i-ab
ility
(IV
), r
elat
ive
ampl
i-tu
de (
RA
)
AC
T: I
S, I
V, R
AIn
clud
e ea
rly
stag
e pr
obab
leA
lzhe
imer
’s /
Exc
lude
neu
-ro
lept
ic m
eds,
vis
ual d
efic
ien-
cies
/low
sam
ple
size
Hig
her
IV, l
ower
RA
, and
tren
d fo
r lo
wer
IS
inA
lzhe
imer
’s v
s. n
orm
al e
lder
-ly
. TE
NS
incr
ease
d IS
inA
lzhe
imer
’s, b
ut d
id n
otim
prov
e IV
or R
A.
No
refe
renc
e st
anda
rd.
Van
Som
eren
(11
1)
4C-b
Ope
n tr
ial/
NH
/ com
pare
dda
ta a
naly
sis
met
hods
for
2st
udie
s: S
tudy
1: 2
8D A
CT
duri
ng 5
D B
L, 1
0D b
righ
tlig
ht tx
, 13
D F
/U/ e
ntir
e 24
h
4 an
d 17
(N
S) /
NS/
dem
ente
d N
one/
1) A
ctill
ume;
2)
hom
em
ade/
1)
non-
dom
wri
st; 2
)no
n-do
m w
rist
/NS
/ NS
/Sl
eep
NS
AC
T: C
ompa
red
cosi
nor,
com
plex
dem
odul
atio
n pe
ri-
odog
ram
, aut
ocor
rela
tion,
inte
rdai
ly s
tabi
lity,
intr
adai
lyva
riab
ility
, rel
ativ
e am
plitu
de
NS
/ NS
Non
-par
amet
ric
vari
able
s,es
peci
ally
inte
rdai
ly s
tabi
lity
and
24-h
aut
ocor
rela
tion
are
mor
e se
nsiti
ve to
cir
cadi
andi
stur
banc
e at
res
t-ac
tivity
rhyt
hm th
an p
aram
etri
c an
aly-
ses
such
as
cosi
nor
Whi
te (
130)
4C-b
DB
; ran
dom
ized
; cro
ss-o
ver
desi
gn /
hom
e / E
ntir
e 24
hs
85 (
75)
/ 57.
8±9.
1 / S
tage
I o
rII
hyp
erte
nsio
n N
one
/ MM
L(A
MI)
/ w
rist
/N
S / N
S / C
ole
et. a
l.
AC
T: s
leep
vs.
W;
Am
bula
tory
BP,
HR
II
hyp
erte
nsio
n, s
ysto
lic B
P>
200,
dia
stol
ic B
P>
110
,B
rady
card
ia, T
achy
card
ia,
Rec
ent s
trok
e or
MI,
ren
al o
rhe
patic
dis
; unc
ontr
olle
d di
a-be
tic /
NS
/ NS
Mor
n. &
eve
n. T
imes
of
adm
inis
trat
ion
of n
isol
dipi
ne(a
long
-act
ing
dihy
drop
yri-
dine
Ca+
+ c
hann
el b
lock
er)
have
sim
ilar
effe
cts
on 2
4 hr
BP
and
HR
. How
ever
, com
-pa
riso
n of
sle
ep &
Wpe
riod
sre
veal
ed d
iffe
rent
ial B
Pan
dH
R e
ffec
ts f
or m
orn.
Vs.
even
. dos
ing
AC
Tw
as u
sed
to d
eter
min
esl
eep
& W
times
by
the
built
-in
alg
orith
m o
f th
e A
MI
reco
rder
or
by u
se o
f an
eve
ntm
arke
r bu
ilt o
n ac
tivat
ed b
y a
pt w
hen
retir
ing
or a
wak
enin
g
Wir
z-Ju
stic
e (8
1)
5D-a
Obs
erva
tiona
l stu
dy, C
ase
seri
es /
Hos
pita
l or
Hom
e /
Ent
ire
24-h
s; 3
-7 w
k A
CT
7 (N
S) /
50.0
±6.
5 (3
8-57
) /
Schi
zoph
reni
a N
one
/ Gah
wile
r / n
on-d
omw
rist
/ 1
min
/ N
S / p
eri-
odog
ram
Vis
ual i
nspe
ctio
n of
act
ivity
plot
, “be
st ta
u,”
(cir
cadi
anpe
riod
), “
best
om
ega”
(ci
rca-
dian
am
plitu
de)
sing
le-d
rug
ther
apy
for
schi
z-op
hren
ia f
or a
t lea
st 1
yr,
com
plia
nt w
ith a
ctig
raph
y /
NS
/ sm
all s
ampl
e si
ze, T
xno
t ran
dom
ly a
ssig
ned,
no
plac
ebo
Four
pat
ient
s ta
king
cla
ssic
alne
urol
eptic
s ha
d di
stur
bed
circ
adia
n rh
ythm
s, th
ree
tak-
ing
cloz
apin
e ha
d hi
ghly
reg
-ul
ar r
hyth
ms
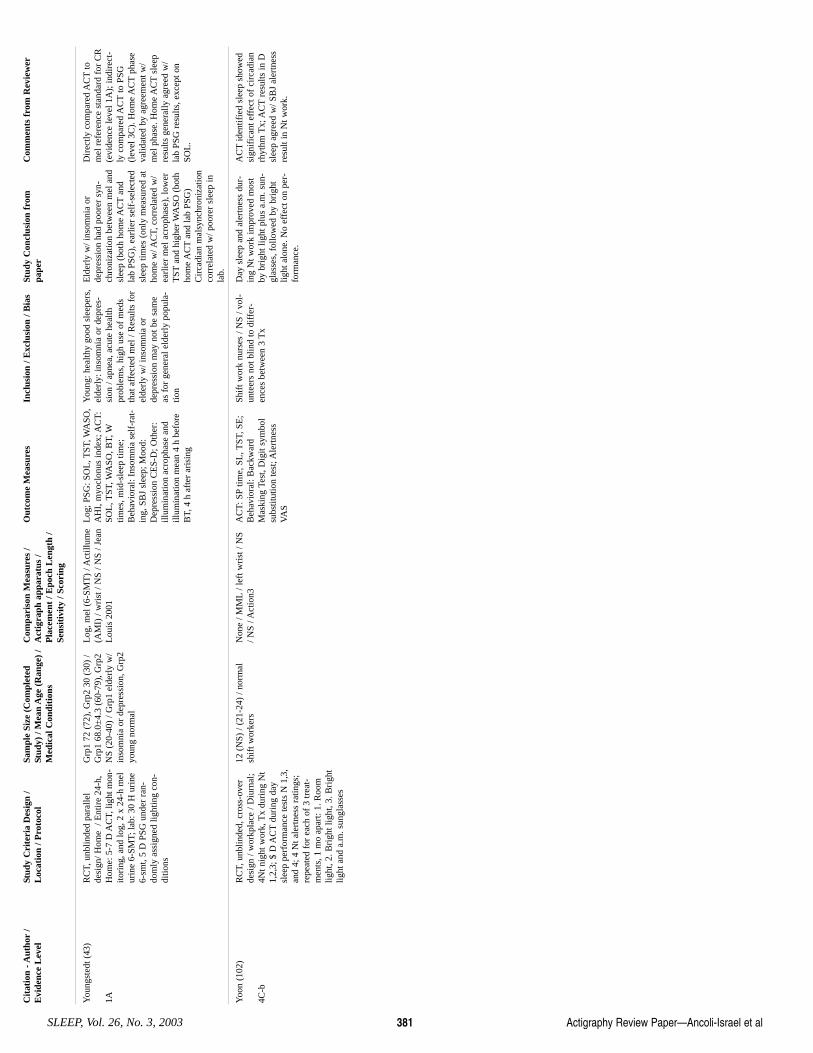
Cit
atio
n - A
utho
r/
Evi
denc
e L
evel
St
udy
Cri
teri
a D
esig
n /
Loc
atio
n / P
roto
col
Sam
ple
Size
(C
ompl
eted
Stud
y) /
Mea
n A
ge (
Ran
ge)
/M
edic
al C
ondi
tion
s
Com
pari
son
Mea
sure
s /
Act
igra
ph a
ppar
atus
/P
lace
men
t / E
poch
Len
gth
/Se
nsit
ivit
y / S
cori
ng
Out
com
e M
easu
res
Incl
usio
n / E
xclu
sion
/ B
ias
Stud
y C
oncl
usio
n fr
ompa
per
Com
men
ts f
rom
Rev
iew
er
Actigraphy Review Paper—Ancoli-Israel et alSLEEP, Vol. 26, No. 3, 2003 381
You
ngst
edt (
43)
1A
RC
T, u
nblin
ded
para
llel
desi
gn/ H
ome
/ E
ntir
e 24
-h,
Hom
e: 5
-7 D
AC
T, li
ght m
on-
itori
ng, a
nd lo
g, 2
x 2
4-h
mel
urin
e 6-
SMT;
lab:
30
H u
rine
6-sm
t, 5
D P
SG u
nder
ran
-do
mly
ass
igne
d lig
htin
g co
n-di
tions
Grp
1 72
(72
), G
rp2
30 (
30)
/G
rp1
68.0
±4.
3 (6
0-79
), G
rp2
NS
(20-
40)
/ Grp
1 el
derl
y w
/in
som
nia
or d
epre
ssio
n, G
rp2
youn
g no
rmal
Log
, mel
(6-
SMT
) / A
ctill
ume
(AM
I) /
wri
st /
NS
/ NS
/ Jea
nL
ouis
200
1
Log
; PSG
: SO
L, T
ST, W
ASO
,A
HI,
myo
clon
us in
dex;
AC
T:
SOL
, TST
, WA
SO, B
T, W
times
, mid
-sle
ep ti
me;
Beh
avio
ral:
Inso
mni
a se
lf-r
at-
ing,
SB
J sl
eep;
Moo
d:D
epre
ssio
n C
ES-
D; O
ther
:ill
umin
atio
n ac
roph
ase
and
illum
inat
ion
mea
n 4
h be
fore
BT,
4 h
aft
er a
risi
ng
You
ng: h
ealth
y go
od s
leep
ers,
elde
rly:
inso
mni
a or
dep
res-
sion
/ ap
nea,
acu
te h
ealth
prob
lem
s, h
igh
use
of m
eds
that
aff
ecte
d m
el /
Res
ults
for
elde
rly
w/ i
nsom
nia
orde
pres
sion
may
not
be
sam
eas
for
gen
eral
eld
erly
pop
ula-
tion
Eld
erly
w/ i
nsom
nia
orde
pres
sion
had
poo
rer
syn-
chro
niza
tion
betw
een
mel
and
slee
p (b
oth
hom
e A
CT
and
lab
PSG
), e
arlie
r se
lf-s
elec
ted
slee
p tim
es (
only
mea
sure
d at
hom
e w
/ AC
T, c
orre
late
d w
/ea
rlie
r m
el a
crop
hase
), lo
wer
TST
and
high
er W
ASO
(bo
thho
me
AC
Tan
d la
b PS
G)
Cir
cadi
an m
alsy
nchr
oniz
atio
nco
rrel
ated
w/ p
oore
r sl
eep
inla
b.
Dir
ectly
com
pare
d A
CT
tom
el r
efer
ence
sta
ndar
d fo
r C
R(e
vide
nce
leve
l 1A
); in
dire
ct-
ly c
ompa
red
AC
Tto
PSG
(lev
el 3
C).
Hom
e A
CT
phas
eva
lidat
ed b
y ag
reem
ent w
/m
el p
hase
. Hom
e A
CT
slee
pre
sults
gen
eral
ly a
gree
d w
/la
b PS
G r
esul
ts, e
xcep
t on
SOL
.
Yoo
n (1
02)
4C-b
RC
T, u
nblin
ded,
cro
ss-o
ver
desi
gn /
wor
kpla
ce /
Diu
rnal
;4N
t nig
ht w
ork,
Tx
duri
ng N
t1,
2,3;
$ D
AC
Tdu
ring
day
slee
p pe
rfor
man
ce te
sts
N 1
,3,
and
4; 4
Nt a
lert
ness
rat
ings
;re
peat
ed f
or e
ach
of 3
trea
t-m
ents
, 1 m
o ap
art:
1. R
oom
light
, 2. B
righ
t lig
ht, 3
. Bri
ght
light
and
a.m
. sun
glas
ses
12 (
NS)
/ (2
1-24
) / n
orm
alsh
ift w
orke
rs
Non
e / M
ML
/ lef
t wri
st /
NS
/ NS
/ Act
ion3
A
CT
: SP
time,
SL
, TST
, SE
;B
ehav
iora
l: B
ackw
ard
Mas
king
Tes
t, D
igit
sym
bol
subs
titut
ion
test
; Ale
rtne
ssV
AS
Shif
t wor
k nu
rses
/ N
S / v
ol-
unte
ers
not b
lind
to d
iffe
r-en
ces
betw
een
3 T
x
Day
sle
ep a
nd a
lert
ness
dur
-in
g N
t wor
k im
prov
ed m
ost
by b
righ
t lig
ht p
lus
a.m
. sun
-gl
asse
s, f
ollo
wed
by
brig
htlig
ht a
lone
. No
effe
ct o
n pe
r-fo
rman
ce.
AC
Tid
entif
ied
slee
p sh
owed
sign
ific
ant e
ffec
t of
circ
adia
nrh
ythm
Tx;
AC
Tre
sults
in D
slee
p ag
reed
w/ S
BJ
aler
tnes
sre
sult
in N
t wor
k.
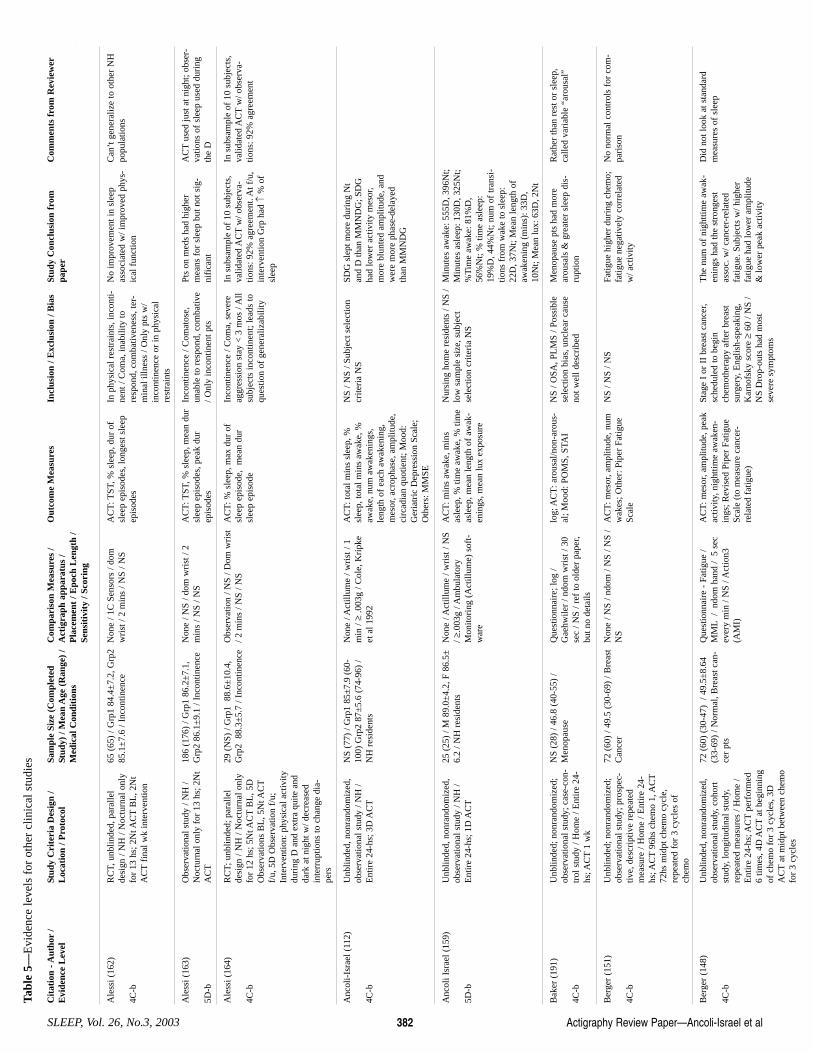
Actigraphy Review Paper—Ancoli-Israel et alSLEEP, Vol. 26, No.3, 2003 382
Ale
ssi (
162)
4C-b
RC
T, u
nblin
ded,
par
alle
lde
sign
/ N
H /
Noc
turn
al o
nly
for
13 h
s; 2
Nt A
CT
BL
, 2N
tA
CT
fina
l wk
inte
rven
tion
65 (
65)
/ Grp
1 84
.4±
7.2,
Grp
285
.1±
7.6
/ Inc
ontin
ence
N
one
/ 1C
Sen
sors
/ do
mw
rist
/ 2
min
s / N
S / N
S A
CT
: TST
, % s
leep
, dur
of
slee
p ep
isod
es, l
onge
st s
leep
epis
odes
In p
hysi
cal r
estr
aint
s, in
cont
i-ne
nt /
Com
a, in
abili
ty to
resp
ond,
com
bativ
enes
s, te
r-m
inal
illn
ess
/ Onl
y pt
s w
/in
cont
inen
ce o
r in
phy
sica
lre
stra
ints
No
impr
ovem
ent i
n sl
eep
asso
ciat
ed w
/ im
prov
ed p
hys-
ical
fun
ctio
n
Can
’t g
ener
aliz
e to
oth
er N
Hpo
pula
tions
Cit
atio
n - A
utho
r/
Evi
denc
e L
evel
St
udy
Cri
teri
a D
esig
n /
Loc
atio
n / P
roto
col
Sam
ple
Size
(C
ompl
eted
Stud
y) /
Mea
n A
ge (
Ran
ge)
/M
edic
al C
ondi
tion
s
Com
pari
son
Mea
sure
s /
Act
igra
ph a
ppar
atus
/P
lace
men
t / E
poch
Len
gth
/Se
nsit
ivit
y / S
cori
ng
Out
com
e M
easu
res
Incl
usio
n / E
xclu
sion
/ B
ias
Stud
y C
oncl
usio
n fr
ompa
per
Com
men
ts f
rom
Rev
iew
er
Tabl
e 5—
Evi
denc
e le
vels
for
oth
er c
linic
al s
tudi
es
Ale
ssi (
163)
5D-b
Obs
erva
tiona
l stu
dy /
NH
/N
octu
rnal
onl
y fo
r 13
hs;
2N
tA
CT
186
(176
) / G
rp1
86.2
±7.
1,G
rp2
86.1
±9.
1 / I
ncon
tinen
ce
Non
e / N
S / d
om w
rist
/ 2
min
s / N
S / N
S A
CT
: TST
, % s
leep
, mea
n du
rsl
eep
epis
odes
, pea
k du
rep
isod
es
Inco
ntin
ence
/ C
omat
ose,
unab
le to
res
pond
, com
bativ
e/ O
nly
inco
ntin
ent p
ts
Pts
on m
eds
had
high
erm
eans
for
sle
ep b
ut n
ot s
ig-
nifi
cant
AC
Tus
ed ju
st a
t nig
ht; o
bser
-va
tions
of
slee
p us
ed d
urin
gth
e D
Ale
ssi (
164)
4C-b
RC
T; u
nblin
ded;
par
alle
lde
sign
/ N
H /
Noc
turn
al o
nly
for
12 h
s; 5
Nt A
CT
BL
, 5D
Obs
erva
tions
BL
, 5N
t AC
Tf/
u, 5
D O
bser
vatio
n f/
u;In
terv
entio
n: p
hysi
cal a
ctiv
itydu
ring
D a
nd e
xtra
qui
te a
ndda
rk a
t nig
ht w
/ dec
reas
edin
terr
uptio
ns to
cha
nge
dia-
pers
29 (
NS)
/ G
rp1
88.
6±10
.4,
Grp
2 8
8.3±
5.7
/ Inc
ontin
ence
O
bser
vatio
n / N
S / D
om w
rist
/ 2 m
ins
/ NS
/ NS
AC
T: %
sle
ep, m
ax d
ur o
fsl
eep
epis
ode,
mea
n du
rsl
eep
epis
ode
Inco
ntin
ence
/ C
oma,
sev
ere
aggr
essi
on s
tay
< 3
mos
/ A
llsu
bjec
ts in
cont
inen
t; le
ads
toqu
estio
n of
gen
eral
izab
ility
In s
ubsa
mpl
e of
10
subj
ects
,va
lidat
ed A
CT
w/ o
bser
va-
tions
: 92%
agr
eem
ent.
At f
/u,
inte
rven
tion
Grp
had
↑%
of
slee
p
In s
ubsa
mpl
e of
10
subj
ects
,va
lidat
ed A
CT
w/ o
bser
va-
tions
: 92%
agr
eem
ent
Anc
oli-
Isra
el (
112)
4C-b
Unb
linde
d, n
onra
ndom
ized
,ob
serv
atio
nal s
tudy
/ N
H /
Ent
ire
24-h
s; 3
D A
CT
NS
(77)
/ G
rp1
85±
7.9
(60-
100)
Grp
2 87
±5.
6 (7
4-96
) /
NH
res
iden
ts
Non
e / A
ctill
ume
/ wri
st /
1m
in / ≥
.003
g / C
ole,
Kri
pke
et a
l 199
2
AC
T: t
otal
min
s sl
eep,
%sl
eep,
tota
l min
s aw
ake,
%aw
ake,
num
aw
aken
ings
,le
ngth
of
each
aw
aken
ing,
mes
or, a
crop
hase
, am
plitu
de,
circ
adia
n qu
otie
nt; M
ood:
Ger
iatr
ic D
epre
ssio
n Sc
ale;
Oth
ers:
MM
SE
NS
/ NS
/ Sub
ject
sel
ectio
ncr
iteri
a N
S SD
G s
lept
mor
e du
ring
Nt
and
D th
an M
MN
DG
; SD
Gha
d lo
wer
act
ivity
mes
or,
mor
e bl
unte
d am
plitu
de, a
ndw
ere
mor
e ph
ase-
dela
yed
than
MM
ND
G
Anc
oli I
srae
l (15
9)
5D-b
Unb
linde
d, n
onra
ndom
ized
,ob
serv
atio
nal s
tudy
/ N
H /
Ent
ire
24-h
s; 1
D A
CT
25 (
25)
/ M 8
9.0±
4.2,
F 8
6.5±
6.2
/ NH
res
iden
ts
Non
e / A
ctill
ume
/ wri
st /
NS
/ ≥.0
03g
/ Am
bula
tory
Mon
itori
ng (
Act
illum
e) s
oft-
war
e
AC
T: m
ins
awak
e, m
ins
asle
ep, %
tim
e aw
ake,
% ti
me
asle
ep, m
ean
leng
th o
f aw
ak-
enin
gs, m
ean
lux
expo
sure
Nur
sing
hom
e re
side
nts
/ NS
/lo
w s
ampl
e si
ze, s
ubje
ctse
lect
ion
crite
ria
NS
Min
utes
aw
ake:
555
D, 3
96N
t;M
inut
es a
slee
p: 1
30D
, 325
Nt;
%T
ime
awak
e: 8
1%D
,56
%N
t; %
tim
e as
leep
:19
%D
, 44%
Nt;
num
of
tran
si-
tions
fro
m w
ake
to s
leep
:22
D, 3
7Nt;
Mea
n le
ngth
of
awak
enin
g (m
ins)
: 33D
,10
Nt;
Mea
n lu
x: 6
3D, 2
Nt
Bak
er (
191)
4C-b
Unb
linde
d; n
onra
ndom
ized
;ob
serv
atio
nal s
tudy
; cas
e-co
n-tr
ol s
tudy
/ H
ome
/ Ent
ire
24-
hs; A
CT
1 w
k
NS
(28)
/ 46
.8 (
40-5
5) /
Men
opau
se
Que
stio
nnai
re; l
og /
Gae
hwile
r / n
dom
wri
st /
30se
c / N
S / r
ef to
old
er p
aper
,bu
t no
deta
ils
log;
AC
T: a
rous
al/n
on-a
rous
-al
; Moo
d: P
OM
S, S
TAI
NS
/ OSA
, PL
MS
/ Pos
sibl
ese
lect
ion
bias
, unc
lear
cau
seno
t wel
l des
crib
ed
Men
opau
se p
ts h
ad m
ore
arou
sals
& g
reat
er s
leep
dis
-ru
ptio
n
Rat
her
than
res
t or
slee
p,ca
lled
vari
able
“ar
ousa
l”
Ber
ger
(151
)
4C-b
Unb
linde
d; n
onra
ndom
ized
;ob
serv
atio
nal s
tudy
; pro
spec
-tiv
e, d
escr
iptiv
e re
peat
edm
easu
re /
Hom
e / E
ntir
e 24
-hs
; AC
T96
hs c
hem
o 1,
AC
T72
hs m
idpt
che
mo
cycl
e,re
peat
ed f
or 3
cyc
les
ofch
emo
72 (
60)
/ 49.
5 (3
0-69
) / B
reas
tC
ance
r N
one
/ NS
/ ndo
m /
NS
/ NS
/N
S A
CT
: mes
or, a
mpl
itude
, num
wak
es; O
ther
: Pip
er F
atig
ueSc
ale
NS
/ NS
/ NS
Fatig
ue h
ighe
r du
ring
che
mo;
fatig
ue n
egat
ivel
y co
rrel
ated
w/ a
ctiv
ity
No
norm
al c
ontr
ols
for
com
-pa
riso
n
Ber
ger
(148
)
4C-b
Unb
linde
d, n
onra
ndom
ized
,ob
serv
atio
nal s
tudy
, coh
ort
stud
y, lo
ngitu
dina
l stu
dy,
repe
ated
mea
sure
s / H
ome
/E
ntir
e 24
-hs;
AC
Tpe
rfor
med
6 tim
es, 4
D A
CT
at b
egin
ning
of c
hem
o fo
r 3
cycl
es, 3
DA
CT
at m
idpt
bet
wee
n ch
emo
for
3 cy
cles
72 (
60)
(30-
47)
/ 49
.5±
8.64
(33-
69)
/ Nor
mal
, Bre
ast c
an-
cer
pts
Que
stio
nnai
re -
Fat
igue
/M
ML
/ nd
om h
and
/ 5
sec
ever
y m
in /
NS
/ Act
ion3
(AM
I)
AC
T: m
esor
, am
plitu
de, p
eak
activ
ity, n
ight
time
awak
en-
ings
; Rev
ised
Pip
er F
atig
ueSc
ale
(to
mea
sure
can
cer-
rela
ted
fatig
ue)
Stag
e I
or I
I br
east
can
cer,
sche
dule
d to
beg
inch
emot
hera
py a
fter
bre
ast
surg
ery,
Eng
lish-
spea
king
,K
arno
fsky
sco
re ≥
60 /
NS
/N
S D
rop-
outs
had
mos
tse
vere
sym
ptom
s
The
num
of
nigh
ttim
e aw
ak-
enin
gs h
ad th
e st
rong
est
asso
c. w
/ can
cer-
rela
ted
fatig
ue. S
ubje
cts
w/ h
ighe
rfa
tigue
had
low
er a
mpl
itude
& lo
wer
pea
k ac
tivity
Did
not
look
at s
tand
ard
mea
sure
s of
sle
ep
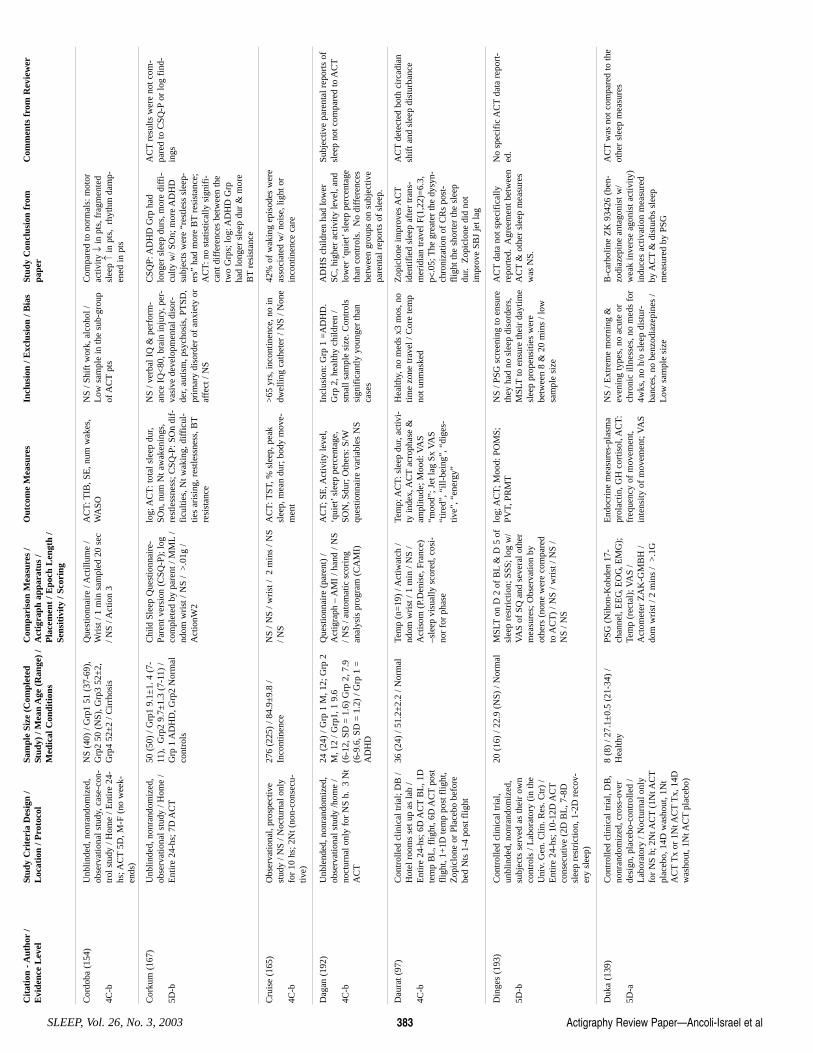
Cit
atio
n - A
utho
r/
Evi
denc
e L
evel
St
udy
Cri
teri
a D
esig
n /
Loc
atio
n / P
roto
col
Sam
ple
Size
(C
ompl
eted
Stud
y) /
Mea
n A
ge (
Ran
ge)
/M
edic
al C
ondi
tion
s
Com
pari
son
Mea
sure
s /
Act
igra
ph a
ppar
atus
/P
lace
men
t / E
poch
Len
gth
/Se
nsit
ivit
y / S
cori
ng
Out
com
e M
easu
res
Incl
usio
n / E
xclu
sion
/ B
ias
Stud
y C
oncl
usio
n fr
ompa
per
Com
men
ts f
rom
Rev
iew
er
Actigraphy Review Paper—Ancoli-Israel et alSLEEP, Vol. 26, No. 3, 2003 383
Cor
doba
(15
4)
4C-b
Unb
linde
d, n
onra
ndom
ized
,ob
serv
atio
nal s
tudy
, cas
e-co
n-tr
ol s
tudy
/ H
ome
/ Ent
ire
24-
hs; A
CT
5D, M
-F (
no w
eek-
ends
)
NS
(40)
/ G
rp1
51 (
37-6
9),
Grp
2 50
(N
S), G
rp3
52±
2,G
rp4
52±
2 / C
irrh
osis
Que
stio
nnai
re /
Act
illum
e /
Wri
st /
1 m
in s
ampl
ed 2
0 se
c/ N
S / A
ctio
n 3
AC
T: T
IB, S
E, n
um w
akes
,W
ASO
N
S / S
hift
wor
k, a
lcoh
ol /
Low
sam
ple
in th
e su
b-gr
oup
of A
CT
pts
Com
pare
d to
nor
mal
s: m
otor
activ
ity ↓
in p
ts, f
ragm
ente
dsl
eep ↑
in p
ts,
rhyt
hm d
amp-
ened
in p
ts
Cor
kum
(16
7)
5D-b
Unb
linde
d, n
onra
ndom
ized
,ob
serv
atio
nal s
tudy
/ H
ome
/E
ntir
e 24
-hs;
7D
AC
T
50 (
50)
/ Grp
1 9.
1±1.
4 (
7-11
), G
rp2
9.7±
1.3
(7-1
1) /
Grp
1 A
DH
D, G
rp2
Nor
mal
cont
rols
Chi
ld S
leep
Que
stio
nnai
re-
Pare
nt v
ersi
on (
CSQ
-P);
log
com
plet
ed b
y pa
rent
/ M
ML
/nd
om w
rist
/ N
S /
>.0
1g /
Act
ionW
2
log;
AC
T: t
otal
sle
ep d
ur,
SOn,
num
Nt a
wak
enin
gs,
rest
less
ness
; CSQ
-P: S
On
dif-
ficu
lties
, Nt w
akin
g, d
iffi
cul-
ties
aris
ing,
res
tless
ness
, BT
resi
stan
ce
NS
/ ver
bal I
Q &
per
form
-an
ce I
Q<
80, b
rain
inju
ry, p
er-
vasi
ve d
evel
opm
enta
l dis
or-
der,
autis
m, p
sych
osis
, PT
SD,
prim
ary
diso
rder
of
anxi
ety
oraf
fect
/ N
S
CSQ
P: A
DH
D G
rp h
adlo
nger
sle
ep d
urs,
mor
e di
ffi-
culty
w/ S
On;
mor
e A
DH
Dsu
bjec
ts w
ere
“res
tless
sle
ep-
ers”
had
mor
e B
Tre
sist
ance
;A
CT
: no
stat
istic
ally
sig
nifi
-ca
nt d
iffe
renc
es b
etw
een
the
two
Grp
s; lo
g: A
DH
D G
rpha
d lo
nger
sle
ep d
ur &
mor
eB
Tre
sist
ance
AC
Tre
sults
wer
e no
t com
-pa
red
to C
SQ-P
or lo
g fi
nd-
ings
Cru
ise
(165
)
4C-b
Obs
erva
tiona
l, pr
ospe
ctiv
est
udy
/ NS
/ Noc
turn
al o
nly
for
10 h
s; 2
Nt (
non-
cons
ecu-
tive)
276
(225
) / 8
4.9±
9.8
/In
cont
inen
ce
NS
/ NS
/ wri
st /
2 m
ins
/ NS
/ NS
AC
T: T
ST, %
sle
ep, p
eak
slee
p, m
ean
dur;
bod
y m
ove-
men
t
>65
yrs
, inc
ontin
ence
, no
indw
ellin
g ca
thet
er /
NS
/ Non
e 42
% o
f w
akin
g ep
isod
es w
ere
asso
ciat
ed w
/ noi
se, l
ight
or
inco
ntin
ence
car
e
Dag
an (
192)
4C-b
Unb
lend
ed, n
onra
ndom
ized
,ob
serv
atio
nal s
tudy
/hom
e /
noct
urna
l onl
y fo
r N
S h.
3 N
tA
CT
24 (
24)
/ Grp
1 M
, 12;
Grp
2M
, 12
/ Grp
1, 1
9.6
(6
-12,
SD
= 1
.6)
Grp
2, 7
.9(6
-9.6
, SD
= 1
.2)
/ Grp
1 =
AD
HD
Que
stio
nnai
re (
pare
nt)
/A
ctig
raph
– A
MI
/ han
d / N
S/ N
S / a
utom
atic
sco
ring
anal
ysis
pro
gram
(C
AM
I)
AC
T; S
E, A
ctiv
ity le
vel,
‘qui
et’s
leep
per
cent
age,
SON
, Sdu
r; O
ther
s: S
/Wqu
estio
nnai
re v
aria
bles
NS
Incl
usio
n: G
rp 1
=A
DH
D.
Grp
2, h
ealth
y ch
ildre
n /
smal
l sam
ple
size
. Con
trol
ssi
gnif
ican
tly y
oung
er th
anca
ses
AD
HS
child
ren
had
low
erSC
, hig
her
activ
ity le
vel,
and
low
er ‘
quie
t’sl
eep
perc
enta
geth
an c
ontr
ols.
No
diff
eren
ces
betw
een
grou
ps o
n su
bjec
tive
pare
ntal
rep
orts
of
slee
p.
Subj
ectiv
e pa
rent
al r
epor
ts o
fsl
eep
not c
ompa
red
to A
CT
Dau
rat (
97)
4C-b
Con
trol
led
clin
ical
tria
l; D
B /
Hot
el r
oom
s se
t up
as la
b /
Ent
ire
24-h
s; 6
D A
CT
BL
, 1D
tem
p B
L, f
light
, 6D
AC
Tpo
stfl
ight
, 1+
1D te
mp
post
flig
ht,
Zop
iclo
ne o
r Pl
aceb
o be
fore
bed
Nts
1-4
pos
t flig
ht
36 (
24)
/ 51.
2±2.
2 / N
orm
al
Tem
p (n
=19
) / A
ctiw
atch
/nd
om w
rist
/ 1
min
/ N
S /
Act
isom
(P.
Den
ise,
Fra
nce)
–sle
ep v
isua
lly s
core
d, c
osi-
nor
for
phas
e
Tem
p; A
CT
: sle
ep d
ur, a
ctiv
i-ty
inde
x, A
CT
acro
phas
e &
ampl
itude
; Moo
d: V
AS
“moo
d”; J
et la
g Sx
VA
S“t
ired
”, “
ill-b
eing
”, “
dige
s-tiv
e”, “
ener
gy”
Hea
lthy,
no
med
s x3
mos
, no
time
zone
trav
el /
Cor
e te
mp
not u
nmas
ked
Zop
iclo
ne im
prov
es A
CT
iden
tifie
d sl
eep
afte
r tr
ans-
mer
idia
n tr
avel
F(1
,22)
=6.
3,p<
.05;
The
gre
ater
the
dysy
n-ch
roni
zatio
n of
CR
s po
st-
flig
ht th
e sh
orte
r th
e sl
eep
dur.
Zop
iclo
ne d
id n
otim
prov
e SB
J je
t lag
AC
Tde
tect
ed b
oth
circ
adia
nsh
ift a
nd s
leep
dis
turb
ance
Din
ges
(193
)
5D-b
Con
trol
led
clin
ical
tria
l,un
blin
ded,
non
rand
omiz
ed,
subj
ects
ser
ved
as th
eir
own
cont
rols
/ L
abor
ator
y (i
n th
eU
niv.
Gen
. Clin
. Res
. Ctr
) /
Ent
ire
24-h
s; 1
0-12
D A
CT
cons
ecut
ive
(2D
BL
, 7-8
Dsl
eep
rest
rict
ion,
1-2
D r
ecov
-er
y sl
eep)
20 (
16)
/ 22.
9 (N
S) /
Nor
mal
M
SLT
on D
2 o
f B
L&
D 5
of
slee
p re
stri
ctio
n; S
SS; l
og w
/V
AS
of S
Q a
nd s
ever
al o
ther
mea
sure
s; O
bser
vatio
n by
othe
rs (
none
wer
e co
mpa
red
to A
CT
) / N
S / w
rist
/ N
S /
NS
/ NS
log;
AC
T; M
ood:
PO
MS;
PVT,
PR
MT
NS
/ PSG
scr
eeni
ng to
ens
ure
they
had
no
slee
p di
sord
ers,
MSL
Tto
ens
ure
thei
r da
ytim
esl
eep
prop
ensi
ties
wer
ebe
twee
n 8
& 2
0 m
ins
/ low
sam
ple
size
AC
Tda
ta n
ot s
peci
fica
llyre
port
ed.
Agr
eem
ent b
etw
een
AC
T&
oth
er s
leep
mea
sure
sw
as N
S.
No
spec
ific
AC
Tda
ta r
epor
t-ed
.
Duk
a (1
39)
5D-a
Con
trol
led
clin
ical
tria
l, D
B,
nonr
ando
miz
ed, c
ross
-ove
rde
sign
, pla
cebo
-con
trol
led
/L
abor
ator
y / N
octu
rnal
onl
yfo
r N
S h;
2N
t AC
T(1
Nt A
CT
plac
ebo,
14D
was
hout
, 1N
tA
CT
Tx
or 1
Nt A
CT
Tx,
14D
was
hout
, 1N
t AC
Tpl
aceb
o)
8 (8
) / 2
7.1±
0.5
(21-
34)
/H
ealth
y
PSG
(N
ihon
-Koh
den
17-
chan
nel,
EE
G, E
OG
, EM
G);
Tem
p (r
ecta
l); V
AS
/A
ctom
eter
ZA
K-G
MB
H /
dom
wri
st /
2 m
ins
/ >
.1G
End
ocri
ne m
easu
res-
plas
ma
prol
actin
, GH
cor
tisol
, AC
T:
freq
uenc
y of
mov
emen
t,in
tens
ity o
f m
ovem
ent;
VA
S
NS
/ Ext
rem
e m
orni
ng &
even
ing
type
s, n
o ac
ute
orch
roni
c ill
ness
es, n
o m
eds
for
4wks
, no
h/o
slee
p di
stur
-ba
nces
, no
benz
odia
zepi
nes
/L
ow s
ampl
e si
ze
B-c
arbo
line
ZK
934
26 (
ben-
zodi
azep
ine
anta
goni
st w
/w
eak
inve
rse
agon
ist a
ctiv
ity)
indu
ces
activ
atio
n m
easu
red
by A
CT
& d
istu
rbs
slee
pm
easu
red
by P
SG
AC
Tw
as n
ot c
ompa
red
to th
eot
her
slee
p m
easu
res
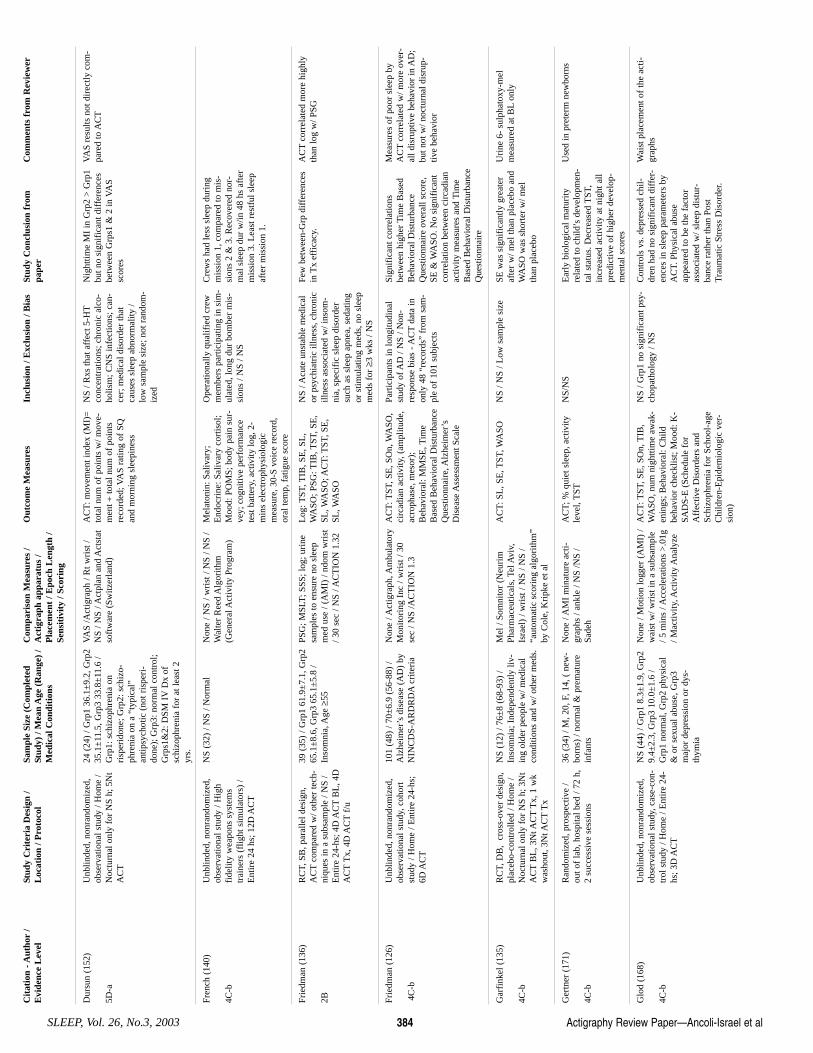
Cit
atio
n - A
utho
r/
Evi
denc
e L
evel
St
udy
Cri
teri
a D
esig
n /
Loc
atio
n / P
roto
col
Sam
ple
Size
(C
ompl
eted
Stud
y) /
Mea
n A
ge (
Ran
ge)
/M
edic
al C
ondi
tion
s
Com
pari
son
Mea
sure
s /
Act
igra
ph a
ppar
atus
/P
lace
men
t / E
poch
Len
gth
/Se
nsit
ivit
y / S
cori
ng
Out
com
e M
easu
res
Incl
usio
n / E
xclu
sion
/ B
ias
Stud
y C
oncl
usio
n fr
ompa
per
Com
men
ts f
rom
Rev
iew
er
Actigraphy Review Paper—Ancoli-Israel et alSLEEP, Vol. 26, No.3, 2003 384
Dur
sun
(152
)
5D-a
Unb
linde
d, n
onra
ndom
ized
,ob
serv
atio
nal s
tudy
/ H
ome
/N
octu
rnal
onl
y fo
r N
S h;
5N
tA
CT
24 (
24)
/ Grp
1 36
.1±
9.2,
Grp
235
.1±
11.5
, Grp
3 33
.8±
11.6
/G
rp1:
sch
izop
hren
ia o
nri
sper
idon
e; G
rp2:
sch
izo-
phre
nia
on a
“ty
pica
l”an
tipsy
chot
ic (
not r
ispe
ri-
done
); G
rp3:
nor
mal
con
trol
;G
rps1
&2:
DSM
IV
Dx
ofsc
hizo
phre
nia
for
at le
ast 2
yrs.
VA
S /A
ctig
raph
/ R
t wri
st /
NS
/ NS
/ Act
plan
and
Act
stat
soft
war
e (S
witz
erla
nd)
AC
T: m
ovem
ent i
ndex
(M
I)=
tota
l num
of
poin
ts w
/ mov
e-m
ent ÷
tota
l num
of
poin
tsre
cord
ed; V
AS
ratin
g of
SQ
and
mor
ning
sle
epin
ess
NS
/ Rxs
that
aff
ect 5
-HT
conc
entr
atio
ns; c
hron
ic a
lco-
holis
m; C
NS
infe
ctio
ns; c
an-
cer;
med
ical
dis
orde
r th
atca
uses
sle
ep a
bnor
mal
ity /
low
sam
ple
size
; not
ran
dom
-iz
ed
Nig
httim
e M
I in
Grp
2 >
Grp
1bu
t no
sign
ific
ant d
iffe
renc
esbe
twee
n G
rps1
& 2
in V
AS
scor
es
VA
S re
sults
not
dir
ectly
com
-pa
red
to A
CT
Fren
ch (
140)
4C-b
Unb
linde
d, n
onra
ndom
ized
,ob
serv
atio
nal s
tudy
/ H
igh
fide
lity
wea
pons
sys
tem
str
aine
rs (
flig
ht s
imul
ator
s) /
Ent
ire
24 h
s; 1
2D A
CT
NS
(32)
/ N
S / N
orm
al
Non
e / N
S / w
rist
/ N
S / N
S /
Wal
ter
Ree
d A
lgor
ithm
(Gen
eral
Act
ivity
Pro
gram
)
Mel
aton
in: S
aliv
ary;
End
ocri
ne: S
aliv
ary
cort
isol
;M
ood:
PO
MS;
bod
y pa
in s
ur-
vey;
cog
nitiv
e pe
rfor
man
cete
st b
atte
ry, a
ctiv
ity lo
g, 2
-m
ins
elec
trop
hysi
olog
icm
easu
re, 3
0-S
voic
e re
cord
,or
al te
mp,
fat
igue
sco
re
Ope
ratio
nally
qua
lifie
d cr
ewm
embe
rs p
artic
ipat
ing
in s
im-
ulat
ed, l
ong
dur
bom
ber
mis
-si
ons
/ NS
/ NS
Cre
ws
had
less
sle
ep d
urin
gm
issi
on 1
, com
pare
d to
mis
-si
ons
2 &
3. R
ecov
ered
nor
-m
al s
leep
dur
w/in
48
hs a
fter
mis
sion
3. L
east
res
tful
sle
epaf
ter
mis
sion
1.
Frie
dman
(13
6)
2B
RC
T, S
B, p
aral
lel d
esig
n,A
CT
com
pare
d w
/ oth
er te
ch-
niqu
es in
a s
ubsa
mpl
e / N
S /
Ent
ire
24-h
s; 4
D A
CT
BL
, 4D
AC
TT
x, 4
D A
CT
f/u
39 (
35)
/ Grp
1 61
.9±
7.1,
Grp
265
.1±
8.6,
Grp
3 65
.1±
5.8
/In
som
nia,
Age
≥55
PSG
; MSL
T; S
SS; l
og; u
rine
sam
ples
to e
nsur
e no
sle
epm
ed u
se /
(AM
I) /
ndom
wri
st/ 3
0 se
c / N
S / A
CT
ION
1.3
2
Log
: TST
, TIB
, SE
, SL
,W
ASO
; PSG
: TIB
, TST
, SE
,SL
, WA
SO; A
CT
: TST
, SE
,SL
, WA
SO
NS
/ Acu
te u
nsta
ble
med
ical
or p
sych
iatr
ic il
lnes
s, c
hron
icill
ness
ass
ocia
ted
w/ i
nsom
-ni
a, s
peci
fic
slee
p di
sord
ersu
ch a
s sl
eep
apne
a, s
edat
ing
or s
timul
atin
g m
eds,
no
slee
pm
eds
for ≥3
wks
/ N
S
Few
bet
wee
n-G
rp d
iffe
renc
esin
Tx
effi
cacy
. A
CT
corr
elat
ed m
ore
high
lyth
an lo
g w
/ PSG
Frie
dman
(12
6)
4C-b
Unb
linde
d, n
onra
ndom
ized
,ob
serv
atio
nal s
tudy
, coh
ort
stud
y / H
ome
/ Ent
ire
24-h
s;6D
AC
T
101
(48)
/ 70
±6.
9 (5
6-88
) /
Alz
heim
er’s
dis
ease
(A
D)
byN
INC
DS-
AR
DR
DA
crite
ria
Non
e / A
ctig
raph
, Am
bula
tory
Mon
itori
ng I
nc /
wri
st /
30se
c / N
S /A
CT
ION
1.3
AC
T: T
ST, S
E, S
On,
WA
SO,
circ
adia
n ac
tivity
, (am
plitu
de,
acro
phas
e, m
esor
);B
ehav
iora
l: M
MSE
, Tim
eB
ased
Beh
avio
ral D
istu
rban
ceQ
uest
ionn
aire
, Alz
heim
er’s
Dis
ease
Ass
essm
ent S
cale
Part
icip
ants
in lo
ngitu
dina
lst
udy
of A
D /
NS
/ Non
-re
spon
se b
ias
- AC
Tda
ta in
only
48
“rec
ords
” fr
om s
am-
ple
of 1
01 s
ubje
cts
Sign
ific
ant c
orre
latio
nsbe
twee
n hi
gher
Tim
e B
ased
Beh
avio
ral D
istu
rban
ceQ
uest
ionn
aire
ove
rall
scor
e,SE
& W
ASO
. No
sign
ific
ant
corr
elat
ion
betw
een
circ
adia
nac
tivity
mea
sure
s an
d T
ime
Bas
ed B
ehav
iora
l Dis
turb
ance
Que
stio
nnai
re
Mea
sure
s of
poo
r sl
eep
byA
CT
corr
elat
ed w
/ mor
e ov
er-
all d
isru
ptiv
e be
havi
or in
AD
;bu
t not
w/ n
octu
rnal
dis
rup-
tive
beha
vior
Gar
fink
el (
135)
4C-b
RC
T, D
B,
cros
s-ov
er d
esig
n,pl
aceb
o-co
ntro
lled
/ Hom
e /
Noc
turn
al o
nly
for
NS
h; 3
Nt
AC
TB
L, 3
Nt A
CT
Tx,
1 w
kw
asho
ut, 3
Nt A
CT
Tx
NS
(12)
/ 76
±8
(68-
93)
/In
som
nia;
Ind
epen
dent
ly li
v-in
g ol
der
peop
le w
/ med
ical
cond
ition
s an
d w
/ oth
er m
eds.
Mel
/ So
mni
tor
(Neu
rim
Phar
mac
eutic
als,
Tel
Avi
v,Is
rael
) / w
rist
/ N
S / N
S /
“aut
omat
ic s
cori
ng a
lgor
ithm
”by
Col
e, K
ripk
e et
al
AC
T: S
L, S
E, T
ST, W
ASO
N
S / N
S / L
ow s
ampl
e si
ze
SE w
as s
igni
fica
ntly
gre
ater
afte
r w
/ mel
than
pla
cebo
and
WA
SO w
as s
hort
er w
/ mel
than
pla
cebo
Uri
ne 6
- su
lpha
toxy
-mel
mea
sure
d at
BL
only
Ger
tner
(17
1)
4C-b
Ran
dom
ized
, pro
spec
tive
/ou
t of
lab,
hos
pita
l bed
/ 72
h,
2 su
cces
sive
ses
sion
s
36 (
34)
/ M, 2
0, F
, 14,
( n
ew-
born
s) /
norm
al &
pre
mat
ure
infa
nts
Non
e / A
MI
min
atur
e ac
ti-gr
aphs
/ an
kle
/ NS
/NS
/Sa
deh
AC
T; %
qui
et s
leep
, act
ivity
leve
l, T
STN
S/N
S E
arly
bio
logi
cal m
atur
ityre
late
d to
chi
ld’s
dev
elop
men
-ta
l sta
tus.
Dec
reas
ed T
ST,
incr
ease
d ac
tivity
at n
ight
all
pred
ictiv
e of
hig
her
deve
lop-
men
tal s
core
s
Use
d in
pre
term
new
born
s
Glo
d (1
68)
4C-b
Unb
linde
d, n
onra
ndom
ized
,ob
serv
atio
nal s
tudy
, cas
e-co
n-tr
ol s
tudy
/ H
ome
/ Ent
ire
24-
hs; 3
D A
CT
NS
(44)
/ G
rp1
8.3±
1.9,
Grp
29.
4±2.
3, G
rp3
10.0
±1.
6 /
Grp
1 no
rmal
, Grp
2 ph
ysic
al&
or
sexu
al a
buse
, Grp
3m
ajor
dep
ress
ion
or d
ys-
thym
ia
Non
e / M
otio
n lo
gger
(A
MI)
/w
aist
w/ w
rist
in a
sub
sam
ple
/ 5 m
ins
/ Acc
eler
atio
ns >
.01g
/ Mac
tivity
, Act
ivity
Ana
lyze
AC
T: T
ST, S
E, S
On,
TIB
,W
ASO
, num
nig
httim
e aw
ak-
enin
gs; B
ehav
iora
l: C
hild
beha
vior
che
cklis
t; M
ood:
K-
SAD
S-E
(Sc
hedu
le f
orA
ffec
tive
Dis
orde
rs a
ndSc
hizo
phre
nia
for
Scho
ol-a
geC
hild
ren-
Epi
dem
iolo
gic
ver-
sion
)
NS
/ Grp
1 no
sig
nifi
cant
psy
-ch
opat
holo
gy /
NS
Con
trol
s vs
. dep
ress
ed c
hil-
dren
had
no
sign
ific
ant d
iffe
r-en
ces
in s
leep
par
amet
ers
byA
CT.
Phy
sica
l abu
seap
pear
ed to
be
the
fact
oras
soci
ated
w/ s
leep
dis
tur-
banc
e ra
ther
than
Pos
tT
raum
atic
Str
ess
Dis
orde
r.
Wai
st p
lace
men
t of
the
acti-
grap
hs
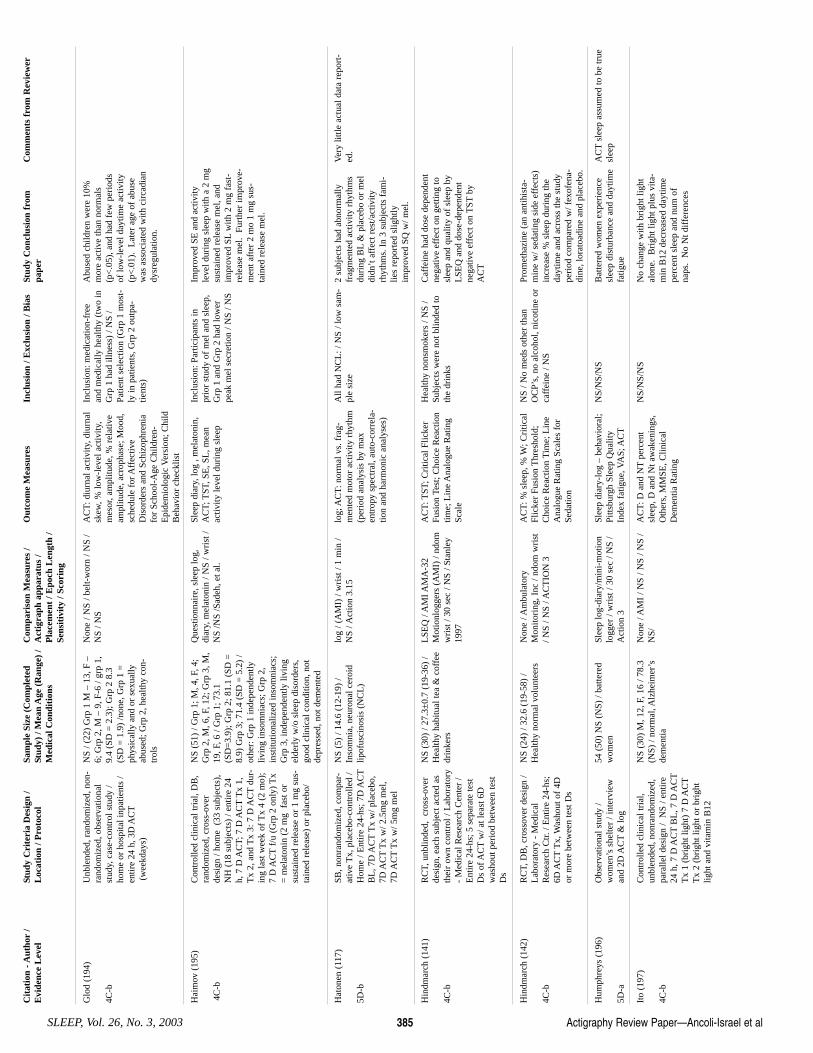
Cit
atio
n - A
utho
r/
Evi
denc
e L
evel
St
udy
Cri
teri
a D
esig
n /
Loc
atio
n / P
roto
col
Sam
ple
Size
(C
ompl
eted
Stud
y) /
Mea
n A
ge (
Ran
ge)
/M
edic
al C
ondi
tion
s
Com
pari
son
Mea
sure
s /
Act
igra
ph a
ppar
atus
/P
lace
men
t / E
poch
Len
gth
/Se
nsit
ivit
y / S
cori
ng
Out
com
e M
easu
res
Incl
usio
n / E
xclu
sion
/ B
ias
Stud
y C
oncl
usio
n fr
ompa
per
Com
men
ts f
rom
Rev
iew
er
Actigraphy Review Paper—Ancoli-Israel et alSLEEP, Vol. 26, No. 3, 2003 385
Glo
d (1
94)
4C-b
Unb
lend
ed, r
ando
miz
ed, n
on-
rand
omiz
ed, o
bser
vatio
nal
stud
y, c
ase-
cont
rol s
tudy
/ho
me
or h
ospi
tal i
npat
ient
s /
entir
e 24
h, 3
D A
CT
(wee
kday
s)
NS
/ (22
) G
rp 1
M –
13,
F –
6; G
rp 2
, M –
9, F
-6 /
grp
1,9.
4 (S
D =
2.3
); G
rp 2
8.3
(S
D =
1.9
) /n
one,
Grp
1 =
phys
ical
ly a
nd o
r se
xual
lyab
used
; Grp
2, h
ealth
y co
n-tr
ols
Non
e / N
S / b
elt-
wor
n / N
S /
NS
/ NS
AC
T: d
iurn
al a
ctiv
ity, d
iurn
alsk
ew, %
low
-lev
el a
ctiv
ity,
mes
or, a
mpl
itude
, % r
elat
ive
ampl
itude
, acr
opha
se; M
ood,
sche
dule
for
Aff
ectiv
eD
isor
ders
and
Sch
izop
hren
iafo
r Sc
hool
-Age
Chi
ldre
n-E
pide
mio
logi
c V
ersi
on; C
hild
Beh
avio
r ch
eckl
ist
Incl
usio
n: m
edic
atio
n-fr
eean
d m
edic
ally
hea
lthy
(tw
o in
Grp
1 h
ad il
lnes
s) /
NS
/Pa
tient
sel
ectio
n (G
rp 1
mos
t-ly
in p
atie
nts,
Grp
2 o
utpa
-tie
nts)
Abu
sed
child
ren
wer
e 10
%m
ore
activ
e th
an n
orm
als
(p<
.05)
, and
had
few
per
iods
of lo
w-l
evel
day
time
activ
ity
(p<
.01)
. L
ater
age
of
abus
ew
as a
ssoc
iate
d w
ith c
irca
dian
dysr
egul
atio
n.
Hai
mov
(19
5)
4C-b
Con
trol
led
clin
ical
tria
l, D
B,
rand
omiz
ed, c
ross
-ove
rde
sign
/ ho
me
(33
sub
ject
s),
NH
(18
sub
ject
s) /
entir
e 24
h, 7
D A
CT;
7 D
AC
TT
x 1,
Tx
2, a
nd T
x 3:
7 D
AC
Tdu
r-in
g la
st w
eek
of T
x 4
(2 m
o);
7 D
AC
Tf/
u (G
rp 2
onl
y) T
x=
mel
aton
in (
2 m
g f
ast o
rsu
stai
ned
rele
ase
or 1
mg
sus-
tain
ed r
elea
se)
or p
lace
bo/
NS
(51)
/ G
rp 1
; M, 4
, F, 4
;G
rp 2
, M, 6
, F, 1
2; G
rp 3
, M,
19, F
, 6 /
Grp
1; 7
3.1
(SD
=3.
9); G
rp 2
; 81.
1 (S
D =
8.9)
Grp
3; 7
1.4
(SD
= 5
.2)
/ot
her:
Grp
1 in
depe
nden
tlyliv
ing
inso
mni
acs;
Grp
2,
inst
itutio
naliz
ed in
som
niac
s;G
rp 3
, ind
epen
dent
ly li
ving
elde
rly
w/o
sle
ep d
isor
ders
,go
od c
linic
al c
ondi
tion,
not
depr
esse
d, n
ot d
emen
ted
Que
stio
nnai
re, s
leep
log,
diar
y, m
elat
onin
/ N
S / w
rist
/N
S /N
S /S
adeh
, et a
l.
Slee
p di
ary,
log
, mel
aton
in,
AC
T; T
ST, S
E, S
L, m
ean
activ
ity le
vel d
urin
g sl
eep
Incl
usio
n: P
artic
ipan
ts in
prio
r st
udy
of m
el a
nd s
leep
,G
rp 1
and
Grp
2 h
ad lo
wer
peak
mel
sec
retio
n / N
S / N
S
Impr
oved
SE
and
act
ivity
leve
l dur
ing
slee
p w
ith a
2 m
gsu
stai
ned
rele
ase
mel
, and
impr
oved
SL
with
2 m
g fa
st-
rele
ase
mel
. Fu
rthe
r im
prov
e-m
ent a
fter
2 m
o 1
mg
sus-
tain
ed r
elea
se m
el.
Hat
onen
(11
7)
5D-b
SB, n
onra
ndom
ized
, com
par-
ativ
e T
x, p
lace
bo-c
ontr
olle
d /
Hom
e / E
ntir
e 24
-hs;
7D
AC
TB
L, 7
D A
CT
Tx
w/ p
lace
bo,
7D A
CT
Tx
w/ 2
.5m
g m
el,
7D A
CT
Tx
w/ 5
mg
mel
NS
(5)
/ 14.
6 (1
2-19
) /
Inso
mni
a, n
euro
nal c
eroi
dlip
ofus
cino
sis
(NC
L)
log
/ (A
MI)
/ w
rist
/ 1
min
/N
S / A
ctio
n 3.
15
log;
AC
T: n
orm
al v
s. f
rag-
men
ted
mot
or a
ctiv
ity r
hyth
m(p
erio
d an
alys
is b
y m
axen
trop
y sp
ectr
al, a
uto-
corr
ela-
tion
and
harm
onic
ana
lyse
s)
All
had
NC
L: /
NS
/ low
sam
-pl
e si
ze
2 su
bjec
ts h
ad a
bnor
mal
lyfr
agm
ente
d ac
tivity
rhy
thm
sdu
ring
BL
& p
lace
bo o
r m
eldi
dn’t
aff
ect r
est/a
ctiv
ityrh
ythm
s. I
n 3
subj
ects
fam
i-lie
s re
port
ed s
light
lyim
prov
ed S
Q w
/ mel
.
Ver
y lit
tle a
ctua
l dat
a re
port
-ed
.
Hin
dmar
ch (
141)
4C-b
RC
T, u
nblin
ded,
cro
ss-o
ver
desi
gn, e
ach
subj
ect a
cted
as
thei
r ow
n co
ntro
l / L
abor
ator
y-
Med
ical
Res
earc
h C
ente
r /
Ent
ire
24-h
s; 5
sep
arat
e te
stD
s of
AC
Tw
/ at l
east
6D
was
hout
per
iod
betw
een
test
Ds
NS
(30)
/ 27
.3±
0.7
(19-
36)
/H
ealth
y ha
bitu
al te
a &
cof
fee
drin
kers
LSE
Q /
AM
I AM
A-3
2M
otio
nlog
gers
(A
MI)
/ nd
omw
rist
/ 30
sec
/ N
S / S
tanl
ey19
97
AC
T: T
ST; C
ritic
al F
licke
rFu
sion
Tes
t; C
hoic
e R
eact
ion
time;
Lin
e A
nalo
gue
Rat
ing
Scal
e
Hea
lthy
nons
mok
ers
/ NS
/Su
bjec
ts w
ere
not b
linde
d to
the
drin
ks
Caf
fein
e ha
d do
se d
epen
dent
nega
tive
effe
ct o
n ge
tting
tosl
eep
and
qual
ity o
f sl
eep
byL
SEQ
and
dos
e-de
pend
ent
nega
tive
effe
ct o
n T
STby
AC
T
Hin
dmar
ch (
142)
4C-b
RC
T, D
B, c
ross
over
des
ign
/L
abor
ator
y -
Med
ical
Res
earc
h C
tr. /
Ent
ire
24-h
s;6D
AC
TT
x, W
asho
ut o
f 4D
or m
ore
betw
een
test
Ds
NS
(24)
/ 32
.6 (
19-5
8) /
Hea
lthy
norm
al v
olun
teer
s N
one
/ Am
bula
tory
Mon
itori
ng, I
nc /
ndom
wri
st/ N
S / N
S / A
CT
ION
3
AC
T: %
sle
ep, %
W; C
ritic
alFl
icke
r Fu
sion
Thr
esho
ld;
Cho
ice
Rea
ctio
n T
ime;
Lin
eA
nalo
gue
Rat
ing
Scal
es f
orSe
datio
n
NS
/ No
med
s ot
her
than
OC
P’s,
no
alco
hol,
nico
tine
orca
ffei
ne /
NS
Prom
etha
zine
(an
ant
ihis
ta-
min
e w
/ sed
atin
g si
de e
ffec
ts)
incr
ease
% s
leep
dur
ing
the
dayt
ime
and
acro
ss th
e st
udy
peri
od c
ompa
red
w/ f
exof
ena-
dine
, lor
atoa
dine
and
pla
cebo
.
Hum
phre
ys (
196)
5D-a
Obs
erva
tiona
l stu
dy /
wom
en’s
she
lter
/ int
ervi
ewan
d 2D
AC
T&
log
54 (
50)
NS
(NS)
/ ba
ttere
dw
omen
Sl
eep
log-
diar
y/m
ini-
mot
ion
logg
er /
wri
st /
30 s
ec /
NS
/A
ctio
n 3
Slee
p di
ary-
log
– be
havi
oral
;Pi
ttsbu
rgh
Slee
p Q
ualit
yIn
dex
fatig
ue, V
AS;
AC
T
NS/
NS/
NS
Bat
tere
d w
omen
exp
erie
nce
slee
p di
stur
banc
e an
d da
ytim
efa
tigue
AC
Tsl
eep
assu
med
to b
e tr
uesl
eep
Ito
(197
)
4C-b
Con
trol
led
clin
ical
tria
l,un
blen
ded,
non
rand
omiz
ed,
para
llel d
esig
n /
NS
/ ent
ire
24 h
, 7 D
AC
TB
L, 7
D A
CT
Tx
1 (b
righ
t lig
ht)
7 D
AC
TT
x 2
(bri
ght l
ight
or
brig
htlig
ht a
nd v
itam
in B
12
NS
(30)
M, 1
2, F
, 16
/ 78.
3(N
S) /
norm
al, A
lzhe
imer
’sde
men
tia
Non
e / A
MI
/ NS
/ NS
/ NS
/N
S/
AC
T: D
and
NT
perc
ent
slee
p, D
and
Nt a
wak
enin
gs,
Oth
ers,
MM
SE, C
linic
alD
emen
tia R
atin
g
NS/
NS/
NS
No
chan
ge w
ith b
righ
t lig
htal
one.
Bri
ght l
ight
plu
s vi
ta-
min
B12
dec
reas
ed d
aytim
epe
rcen
t sle
ep a
nd n
um o
fna
ps.
No
Nt d
iffe
renc
es
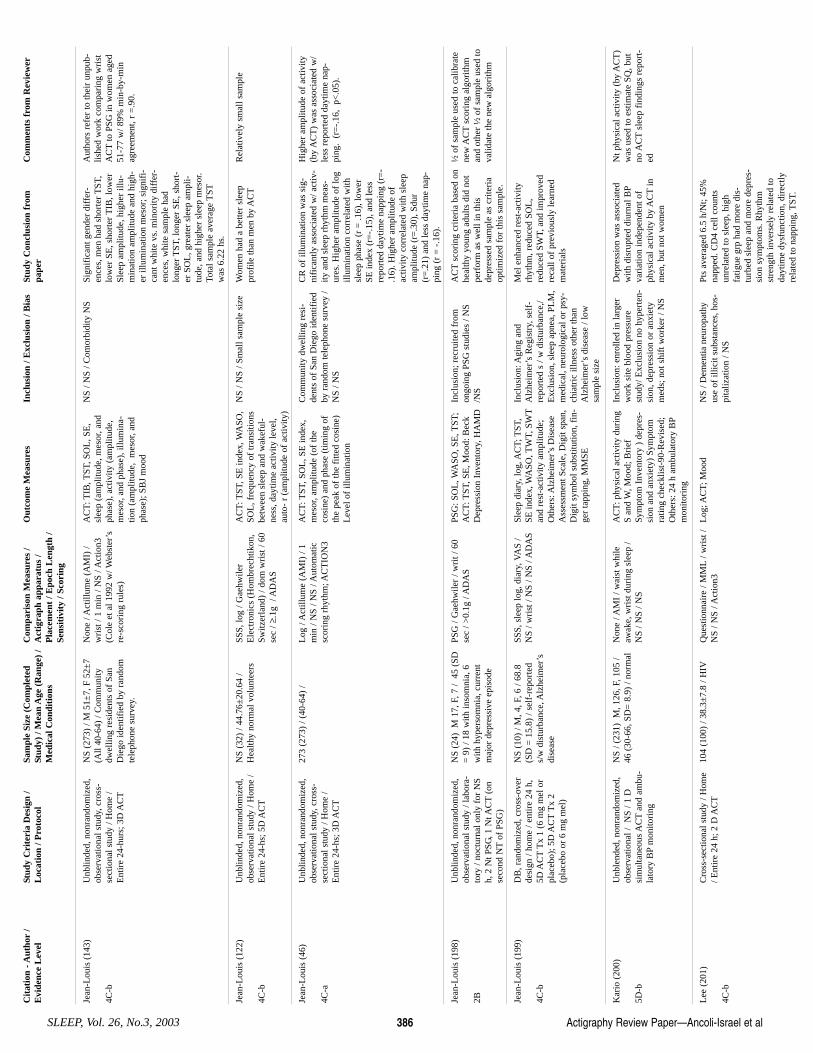
Cit
atio
n - A
utho
r/
Evi
denc
e L
evel
St
udy
Cri
teri
a D
esig
n /
Loc
atio
n / P
roto
col
Sam
ple
Size
(C
ompl
eted
Stud
y) /
Mea
n A
ge (
Ran
ge)
/M
edic
al C
ondi
tion
s
Com
pari
son
Mea
sure
s /
Act
igra
ph a
ppar
atus
/P
lace
men
t / E
poch
Len
gth
/Se
nsit
ivit
y / S
cori
ng
Out
com
e M
easu
res
Incl
usio
n / E
xclu
sion
/ B
ias
Stud
y C
oncl
usio
n fr
ompa
per
Com
men
ts f
rom
Rev
iew
er
Actigraphy Review Paper—Ancoli-Israel et alSLEEP, Vol. 26, No.3, 2003 386
Jean
-Lou
is (
143)
4C-b
Unb
linde
d, n
onra
ndom
ized
,ob
serv
atio
nal s
tudy
, cro
ss-
sect
iona
l stu
dy /
Hom
e /
Ent
ire
24-h
urs;
3D
AC
T
NS
(273
) / M
51±
7, F
52±
7(A
ll 40
-64)
/ C
omm
unity
dwel
ling
resi
dent
s of
San
Die
go id
entif
ied
by r
ando
mte
leph
one
surv
ey.
Non
e / A
ctill
ume
(AM
I) /
wri
st /
1 m
in /
NS
/ Act
ion3
(Col
e et
al 1
992
w/ W
ebst
er’s
re-s
cori
ng r
ules
)
AC
T: T
IB, T
ST, S
OL
, SE
,sl
eep
(am
plitu
de, m
esor
, and
phas
e), a
ctiv
ity (
ampl
itude
,m
esor
, and
pha
se),
illu
min
a-tio
n (a
mpl
itude
, m
esor
, and
phas
e); S
BJ
moo
d
NS
/ NS
/ Com
orbi
dity
NS
Sign
ific
ant g
ende
r di
ffer
-en
ces,
men
had
sho
rter
TST
,lo
wer
SE
, sho
rter
TIB
, low
erSl
eep
ampl
itude
, hig
her
illu-
min
atio
n am
plitu
de a
nd h
igh-
er il
lum
inat
ion
mes
or; s
igni
fi-
cant
whi
te v
s. m
inor
ity d
iffe
r-en
ces,
whi
te s
ampl
e ha
dlo
nger
TST
, lon
ger
SE, s
hort
-er
SO
L, g
reat
er s
leep
am
pli-
tude
, and
hig
her
slee
p m
esor
.To
tal s
ampl
e av
erag
e T
STw
as 6
.22
hs.
Aut
hors
ref
er to
thei
r un
pub-
lishe
d w
ork
com
pari
ng w
rist
AC
Tto
PSG
in w
omen
age
d51
-77
w/ 8
9% m
in-b
y-m
inag
reem
ent,
r =
.90.
Jean
-Lou
is (
122)
4C-b
Unb
linde
d, n
onra
ndom
ized
,ob
serv
atio
nal s
tudy
/ H
ome
/E
ntir
e 24
-hs;
5D
AC
T
NS
(32)
/ 44
.76±
20.6
4 /
Hea
lthy
norm
al v
olun
teer
s SS
S, lo
g / G
aehw
iler
Ele
ctro
nics
(H
ombr
echt
ikon
,Sw
itzer
land
) / d
om w
rist
/ 60
sec
/ ≥.1
g /
AD
AS
AC
T: T
ST, S
E in
dex,
WA
SO,
SOL
, fre
quen
cy o
f tr
ansi
tions
betw
een
slee
p an
d w
akef
ul-
ness
, day
time
activ
ity le
vel,
auto
- r
(am
plitu
de o
f ac
tivity
)
NS
/ NS
/ Sm
all s
ampl
e si
ze
Wom
en h
ad a
bet
ter
slee
ppr
ofile
than
men
by
AC
TR
elat
ivel
y sm
all s
ampl
e
Jean
-Lou
is (
46)
4C-a
Unb
linde
d, n
onra
ndom
ized
,ob
serv
atio
nal s
tudy
, cro
ss-
sect
iona
l stu
dy /
Hom
e /
Ent
ire
24-h
s; 3
D A
CT
273
(273
) / (
40-6
4) /
L
og /
Act
illum
e (A
MI)
/ 1
min
/ N
S / N
S / A
utom
atic
scor
ing
rhyt
hm; A
CT
ION
3
AC
T: T
ST, S
OL
, SE
inde
x,m
esor
, am
plitu
de (
of th
eco
sine
) an
d ph
ase
(tim
ing
ofth
e pe
ak o
f th
e fi
tted
cosi
ne)
Lev
el o
f ill
umin
atio
n
Com
mun
ity d
wel
ling
resi
-de
nts
of S
an D
iego
iden
tifie
dby
ran
dom
tele
phon
e su
rvey
/N
S / N
S
CR
of
illum
inat
ion
was
sig
-ni
fica
ntly
ass
ocia
ted
w/ a
ctiv
-ity
and
sle
ep r
hyth
m m
eas-
ures
. Hig
her
ampl
itude
of
log
illum
inat
ion
corr
elat
ed w
ithsl
eep
phas
e (r
= .1
6), l
ower
SE in
dex
(r=
-.15
), a
nd le
ssre
port
ed d
aytim
e na
ppin
g (r
=-
.16)
. Hig
her
ampl
itude
of
activ
ity c
orre
late
d w
ith s
leep
ampl
itude
(r=
.30)
, Sdu
r(r
=.2
1) a
nd le
ss d
aytim
e na
p-pi
ng (
r =
-.1
6).
Hig
her
ampl
itude
of
activ
ity(b
y A
CT
) w
as a
ssoc
iate
d w
/le
ss r
epor
ted
dayt
ime
nap-
ping
. (r
=-.
16,
p<.0
5).
Jean
-Lou
is (
198)
2B
Unb
linde
d, n
onra
ndom
ized
,ob
serv
atio
nal s
tudy
/ la
bora
-to
ry /
noct
urna
l onl
y fo
r N
Sh,
2 N
t PSG
, 1 N
t AC
T(o
nse
cond
NT
of P
SG)
NS
(24)
M 1
7, F
, 7 /
45
(SD
= 9
) / 1
8 w
ith in
som
nia,
6w
ith h
yper
som
nia,
cur
rent
maj
or d
epre
ssiv
e ep
isod
e
PSG
/ G
aehw
iler
/ wri
t / 6
0se
c / >
0.1g
/ A
DA
S PS
G: S
OL
, WA
SO, S
E, T
ST;
AC
T: T
ST, S
E, M
ood:
Bec
kD
epre
ssio
n In
vent
ory,
HA
MD
Incl
usio
n; r
ecru
ited
from
ongo
ing
PSG
stu
dies
/ N
S/N
S
AC
Tsc
orin
g cr
iteri
a ba
sed
onhe
alth
y yo
ung
adul
ts d
id n
otpe
rfor
m a
s w
ell i
n th
isde
pres
sed
sam
ple
as c
rite
ria
optim
ized
for
this
sam
ple.
½ o
f sa
mpl
e us
ed to
cal
ibra
tene
w A
CT
scor
ing
algo
rith
man
d ot
her
½ o
f sa
mpl
e us
ed to
valid
ate
the
new
alg
orith
m
Jean
-Lou
is (
199)
4C-b
DB
, ran
dom
ized
, cro
ss-o
ver
desi
gn /
hom
e / e
ntir
e 24
h,
5D A
CT
Tx
1 (6
mg
mel
or
plac
ebo)
; 5D
AC
TT
x 2
(pla
cebo
or
6 m
g m
el)
NS
(10)
/ M
, 4, F
, 6 /
68.8
(SD
= 1
5.8)
/ se
lf-r
epor
ted
s/w
dis
turb
ance
, Alz
heim
er’s
dise
ase
SSS,
sle
ep lo
g, d
iary
, VA
S /
NS
/ wri
st /
NS
/ NS
/ AD
AS
Slee
p di
ary,
log,
AC
T; T
ST,
SE in
dex,
WA
SO, T
WT,
SW
Tan
d re
st-a
ctiv
ity a
mpl
itude
;O
ther
s: A
lzhe
imer
’s D
isea
seA
sses
smen
t Sca
le, D
igit
span
,D
igit
sym
bol s
ubst
itutio
n, f
in-
ger
tapp
ing,
MM
SE
Incl
usio
n: A
ging
and
Alz
heim
er’s
Reg
istr
y, s
elf-
repo
rted
s /
w d
istu
rban
ce,/
Exc
lusi
on, s
leep
apn
ea, P
LM
,m
edic
al, n
euro
logi
cal o
r ps
y-ch
iatr
ic il
lnes
s ot
her
than
Alz
heim
er’s
dis
ease
/ lo
wsa
mpl
e si
ze
Mel
enh
ance
d re
st-a
ctiv
ityrh
ythm
, red
uced
SO
L,
redu
ced
SWT,
and
impr
oved
reca
ll of
pre
viou
sly
lear
ned
mat
eria
ls
Kar
io (
200)
5D-b
Unb
lend
ed, n
onra
ndom
ized
,ob
serv
atio
nal /
NS
/ 1 D
sim
ulta
neou
s A
CT
and
ambu
-la
tory
BP
mon
itori
ng
NS
/ (23
1) M
, 126
, F, 1
05 /
46 (
30-6
6, S
D=
8.9
) / n
orm
al
Non
e / A
MI
/ wai
st w
hile
awak
e, w
rist
dur
ing
slee
p /
NS
/ NS
/ NS
AC
T: p
hysi
cal a
ctiv
ity d
urin
gS
and
W, M
ood;
Bri
efSy
mpt
om I
nven
tory
) d
epre
s-si
on a
nd a
nxie
ty)
Sym
ptom
ratin
g ch
eckl
ist-
90-R
evis
ed;
Oth
ers:
24
h am
bula
tory
BP
mon
itori
ng
Incl
usio
n: e
nrol
led
in la
rger
wor
k si
te b
lood
pre
ssur
est
udy/
Exc
lusi
on n
o hy
pert
en-
sion
, dep
ress
ion
or a
nxie
tym
eds;
not
shi
ft w
orke
r / N
S
Dep
ress
ion
was
ass
ocia
ted
with
dis
rupt
ed d
iurn
al B
Pva
riat
ion
inde
pend
ent o
fph
ysic
al a
ctiv
ity b
y A
CT
inm
en, b
ut n
ot w
omen
Nt p
hysi
cal a
ctiv
ity (
by A
CT
)w
as u
sed
to e
stim
ate
SQ, b
utno
AC
Tsl
eep
find
ings
rep
ort-
ed
Lee
(20
1)
4C-b
Cro
ss-s
ectio
nal s
tudy
/ H
ome
/ Ent
ire
24 h
; 2 D
AC
T10
4 (1
00)
/ 38.
3±7.
8 / H
IVQ
uest
ionn
aire
/ M
ML
/ wri
st /
NS
/ NS
/ Act
ion3
L
og; A
CT;
Moo
d N
S / D
emen
tia n
euro
path
yus
e of
illic
it su
bsta
nces
, hos
-pi
taliz
atio
n / N
S
Pts
aver
aged
6.5
h/N
t; 45
%na
pped
. CD
4 ce
ll co
unts
unre
late
d to
sle
ep, h
igh
fatig
ue g
rp h
ad m
ore
dis-
turb
ed s
leep
and
mor
e de
pres
-si
on s
ympt
oms.
Rhy
thm
stre
ngth
inve
rsel
y re
late
d to
dayt
ime
dysf
unct
ion,
dir
ectly
rela
ted
to n
appi
ng, T
ST.
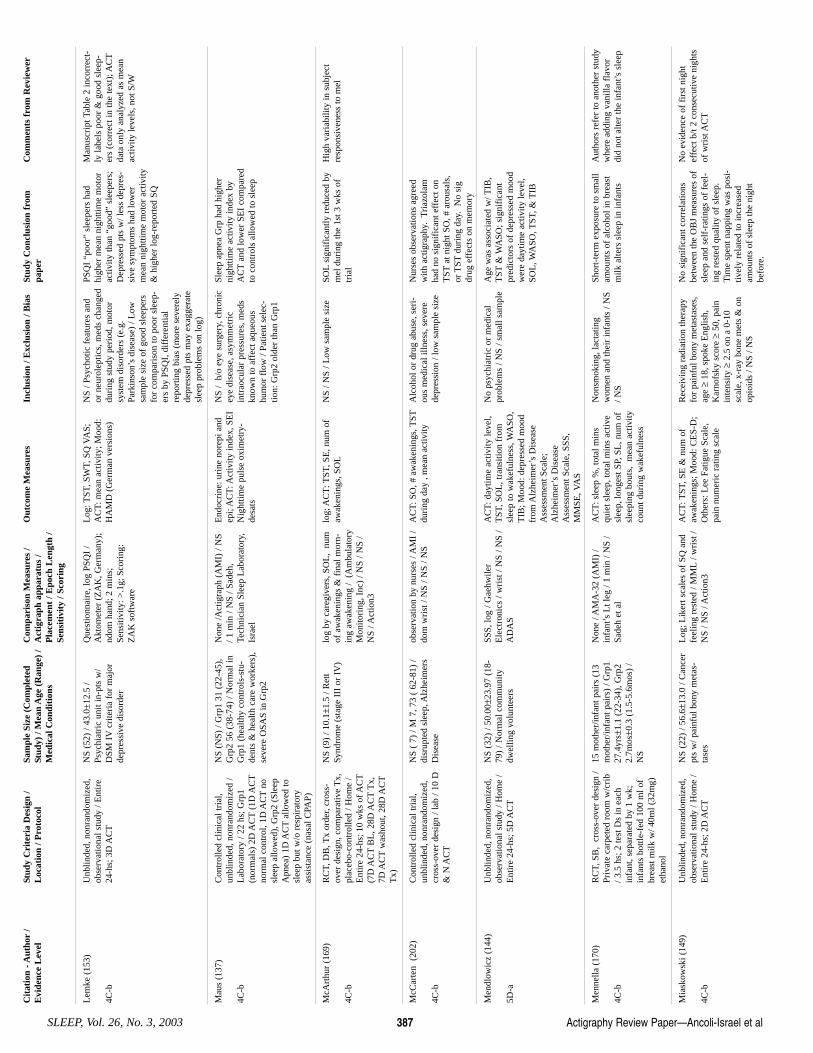
Cit
atio
n - A
utho
r/
Evi
denc
e L
evel
St
udy
Cri
teri
a D
esig
n /
Loc
atio
n / P
roto
col
Sam
ple
Size
(C
ompl
eted
Stud
y) /
Mea
n A
ge (
Ran
ge)
/M
edic
al C
ondi
tion
s
Com
pari
son
Mea
sure
s /
Act
igra
ph a
ppar
atus
/P
lace
men
t / E
poch
Len
gth
/Se
nsit
ivit
y / S
cori
ng
Out
com
e M
easu
res
Incl
usio
n / E
xclu
sion
/ B
ias
Stud
y C
oncl
usio
n fr
ompa
per
Com
men
ts f
rom
Rev
iew
er
Actigraphy Review Paper—Ancoli-Israel et alSLEEP, Vol. 26, No. 3, 2003 387
Lem
ke (
153)
4C-b
Unb
linde
d, n
onra
ndom
ized
,ob
serv
atio
nal s
tudy
/ E
ntir
e24
-hs;
3D
AC
T
NS
(52)
/ 43
.0±
12.5
/Ps
ychi
atri
c un
it in
-pts
w/
DSM
IV
crite
ria
for
maj
orde
pres
sive
dis
orde
r
Que
stio
nnai
re, l
og P
SQI
/A
ktom
eter
(Z
AK
, Ger
man
y);
ndom
han
d; 2
min
s;Se
nsiti
vity
: >.1
g; S
cori
ng:
ZA
K s
oftw
are
Log
: TST
, SW
T, S
Q V
AS;
AC
T: m
ean
activ
ity; M
ood:
HA
MD
(G
erm
an v
ersi
ons)
NS
/ Psy
chot
ic f
eatu
res
and
or n
euro
lept
ics,
med
s ch
ange
ddu
ring
stu
dy p
erio
d, m
otor
syst
em d
isor
ders
(e.
g.Pa
rkin
son’
s di
seas
e) /
Low
sam
ple
size
of
good
sle
eper
sfo
r co
mpa
riso
n to
poo
r sl
eep-
ers
by P
SQI,
dif
fere
ntia
lre
port
ing
bias
(m
ore
seve
rely
depr
esse
d pt
s m
ay e
xagg
erat
esl
eep
prob
lem
s on
log)
PSQ
I “p
oor”
sle
eper
s ha
dhi
gher
mea
n ni
ghtti
me
mot
orac
tivity
than
“go
od”
slee
pers
;D
epre
ssed
pts
w/ l
ess
depr
es-
sive
sym
ptom
s ha
d lo
wer
mea
n ni
ghtti
me
mot
or a
ctiv
ity&
hig
her
log-
repo
rted
SQ
Man
uscr
ipt T
able
2 in
corr
ect-
ly la
bels
poo
r &
goo
d sl
eep-
ers
(cor
rect
in th
e te
xt);
AC
Tda
ta o
nly
anal
yzed
as
mea
nac
tivity
leve
ls, n
ot S
/W
Mau
s (1
37)
4C-b
Con
trol
led
clin
ical
tria
l,un
blin
ded,
non
rand
omiz
ed /
Lab
orat
ory
/ 22
hs; G
rp1
(nor
mal
s) 2
D A
CT
(1D
AC
Tno
rmal
con
trol
, 1D
AC
Tno
slee
p al
low
ed),
Grp
2 (S
leep
Apn
ea)
1D A
CT
allo
wed
tosl
eep
but w
/o r
espi
rato
ryas
sist
ance
(na
sal C
PAP)
NS
(NS)
/ G
rp1
31 (
22-4
5),
Grp
2 56
(38
-74)
/ N
orm
al in
Grp
1 (h
ealth
y co
ntro
ls-s
tu-
dent
s &
hea
lth c
are
wor
kers
),se
vere
OSA
S in
Grp
2
Non
e /A
ctig
raph
(A
MI)
/ N
S/ 1
min
/ N
S / S
adeh
,Te
chni
cian
Sle
ep L
abor
ator
y,Is
rael
End
ocri
ne: u
rine
nor
epi a
ndep
i; A
CT
: Act
ivity
inde
x, S
EI
Nig
httim
e pu
lse
oxim
etry
-de
sats
NS
/ h/
o ey
e su
rger
y, c
hron
icey
e di
seas
e, a
sym
met
ric
intr
aocu
lar
pres
sure
s, m
eds
know
n to
aff
ect a
queo
ushu
mor
flo
w /
Patie
nt s
elec
-tio
n: G
rp2
olde
r th
an G
rp1
Slee
p ap
nea
Grp
had
hig
her
nigh
ttim
e ac
tivity
inde
x by
AC
Tan
d lo
wer
SE
I co
mpa
red
to c
ontr
ols
allo
wed
to s
leep
McA
rthu
r (1
69)
4C-b
RC
T, D
B, T
x or
der,
cros
s-ov
er d
esig
n, c
ompa
rativ
e T
x,pl
aceb
o-co
ntro
lled
/ Hom
e /
Ent
ire
24-h
s; 1
0 w
ks o
f AC
T(7
D A
CT
BL
, 28D
AC
TT
x,7D
AC
Tw
asho
ut, 2
8D A
CT
Tx)
NS
(9)
/ 10.
1±1.
5 / R
ett
Synd
rom
e (s
tage
III
or
IV)
lo
g by
car
egiv
ers,
SO
L,
num
of a
wak
enin
gs &
fin
al m
orn-
ing
awak
enin
g /
(Am
bula
tory
Mon
itori
ng, I
nc)
/ NS
/ NS
/N
S / A
ctio
n3
log;
AC
T: T
ST, S
E, n
um o
faw
aken
ings
, SO
LN
S / N
S / L
ow s
ampl
e si
ze
SOL
sign
ific
antly
red
uced
by
mel
dur
ing
the
1st 3
wks
of
tria
l
Hig
h va
riab
ility
in s
ubje
ctre
spon
sive
ness
to m
el
McC
arte
n (
202)
4C-b
Con
trol
led
clin
ical
tria
l,un
blin
ded,
non
rand
omiz
ed,
cros
s-ov
er d
esig
n / l
ab /
10 D
& N
AC
T
NS
( 7)
/ M
7, 7
3 (
62-8
1) /
disr
upte
d sl
eep,
Alz
heim
ers
Dis
ease
obse
rvat
ion
by n
urse
s / A
MI
/do
m w
rist
/ N
S / N
S / N
S
AC
T: S
O, #
aw
aken
ings
, TST
duri
ng d
ay ,
mea
n ac
tivity
A
lcoh
ol o
r dr
ug a
buse
, ser
i-ou
s m
edic
al il
lnes
s, s
ever
ede
pres
sion
/ lo
w s
ampl
e si
ze
Nur
ses
obse
rvat
ions
agr
eed
with
act
igra
phy.
Tri
azol
amha
d no
sig
nifi
cant
eff
ect o
nT
STat
nig
ht S
O, #
aro
usal
s,or
TST
duri
ng d
ay.
No
sig
drug
eff
ects
on
mem
ory
Men
dlow
icz
(144
)
5D-a
Unb
linde
d, n
onra
ndom
ized
,ob
serv
atio
nal s
tudy
/ H
ome
/E
ntir
e 24
-hs;
5D
AC
T
NS
(32)
/ 50
.00±
23.9
7 (1
8-79
) / N
orm
al c
omm
unity
dwel
ling
volu
ntee
rs
SSS,
log
/ Gae
hwile
rE
lect
roni
cs /
wri
st /
NS
/ NS
/A
DA
S
AC
T: d
aytim
e ac
tivity
leve
l,T
ST, S
OL
, tra
nsiti
on f
rom
slee
p to
wak
eful
ness
, WA
SO,
TIB
; Moo
d: d
epre
ssed
moo
dfr
om A
lzhe
imer
’s D
isea
seA
sses
smen
t Sca
le;
Alz
heim
er’s
Dis
ease
Ass
essm
ent S
cale
, SSS
,M
MSE
, VA
S
No
psyc
hiat
ric
or m
edic
alpr
oble
ms
/ NS
/ sm
all s
ampl
e A
ge w
as a
ssoc
iate
d w
/ TIB
,T
ST&
WA
SO; s
igni
fica
ntpr
edic
tors
of
depr
esse
d m
ood
wer
e da
ytim
e ac
tivity
leve
l,SO
L, W
ASO
, TST
, & T
IB
Men
nella
(17
0)
4C-b
RC
T, S
B,
cros
s-ov
er d
esig
n /
Priv
ate
carp
eted
roo
m w
/cri
b/ 3
.5 h
s; 2
test
Ds
in e
ach
infa
nt, s
epar
ated
by
1 w
k;in
fant
s bo
ttle-
fed
100
ml o
fbr
east
milk
w/ 4
0ml (
32m
g)et
hano
l
15 m
othe
r/in
fant
pai
rs (
13m
othe
r/in
fant
pai
rs)
/ Grp
127
.4yr
s±1.
1 (2
2-34
), G
rp2
2.7m
os±0
.3 (
1.5-
5.6m
os)
/N
S
Non
e / A
MA
-32
(AM
I) /
infa
nt’s
Lt l
eg /
1 m
in /
NS
/Sa
deh
et a
l
AC
T: s
leep
%, t
otal
min
squ
iet s
leep
, tot
al m
ins
activ
esl
eep,
long
est S
P, S
L, n
um o
fsl
eepi
ng b
outs
, m
ean
activ
ityco
unt d
urin
g w
akef
ulne
ss
Non
smok
ing,
lact
atin
gw
omen
and
thei
r in
fant
s / N
S/ N
S
Shor
t-te
rm e
xpos
ure
to s
mal
lam
ount
s of
alc
ohol
in b
reas
tm
ilk a
lters
sle
ep in
infa
nts
Aut
hors
ref
er to
ano
ther
stu
dyw
here
add
ing
vani
lla f
lavo
rdi
d no
t alte
r th
e in
fant
’s s
leep
Mia
skow
ski (
149)
4C-b
Unb
linde
d, n
onra
ndom
ized
,ob
serv
atio
nal s
tudy
/ H
ome
/E
ntir
e 24
-hs;
2D
AC
T
NS
(22)
/ 56
.6±1
3.0
/ Can
cer
pts
w/ p
ainf
ul b
ony
met
as-
tase
s
Log
; Lik
ert s
cale
s of
SQ
and
feel
ing
rest
ed /
MM
L/ w
rist
/N
S / N
S / A
ctio
n3
AC
T: T
ST, S
E &
num
of
awak
enin
gs; M
ood:
CE
S-D
;O
ther
s: L
ee F
atig
ue S
cale
,pa
in n
umer
ic r
atin
g sc
ale
Rec
eivi
ng r
adia
tion
ther
apy
for
pain
ful b
ony
met
asta
ses,
age ≥
18, s
poke
Eng
lish,
Kar
nofs
ky s
core
≥50
, pai
nin
tens
ity ≥
2.5
on a
0-1
0sc
ale,
x-r
ay b
one
met
s &
on
opio
ids
/ NS
/ NS
No
sign
ific
ant c
orre
latio
nsbe
twee
n th
e O
BJ
mea
sure
s of
slee
p an
d se
lf-r
atin
gs o
f fe
el-
ing
rest
ed q
ualit
y of
sle
ep.
Tim
e sp
ent n
appi
ng w
as p
osi-
tivel
y re
late
d to
incr
ease
dam
ount
s of
sle
ep th
e ni
ght
befo
re.
No
evid
ence
of
firs
t nig
htef
fect
b/t
2 co
nsec
utiv
e ni
ghts
of w
rist
AC
T
Cit
atio
n - A
utho
r/
Evi
denc
e L
evel
St
udy
Cri
teri
a D
esig
n /
Loc
atio
n / P
roto
col
Sam
ple
Size
(C
ompl
eted
Stud
y) /
Mea
n A
ge (
Ran
ge)
/M
edic
al C
ondi
tion
s
Com
pari
son
Mea
sure
s /
Act
igra
ph a
ppar
atus
/P
lace
men
t / E
poch
Len
gth
/Se
nsit
ivit
y / S
cori
ng
Out
com
e M
easu
res
Incl
usio
n / E
xclu
sion
/ B
ias
Stud
y C
oncl
usio
n fr
ompa
per
Com
men
ts f
rom
Rev
iew
er
Actigraphy Review Paper—Ancoli-Israel et alSLEEP, Vol. 26, No.3, 2003 388
Mill
er (
203)
5D-a
Unb
lend
ed, n
onra
ndom
ized
,ca
se s
erie
s / h
ome
/ ent
ire
24h,
AC
TB
L, A
CT
plac
ebo,
AC
TT
x (
with
met
hylp
heni
date
or
pem
o-lin
e), n
um d
ays
AC
TN
S
NS
(15)
Grp
1m
ethy
lphe
nida
te, M
-6; F
-2;
Grp
2 P
emol
ine,
M-5
, F-3
/G
rp 1
; 7.5
(SD
= 2
.1)
Grp
29.
1 (S
D =
2.3
)/ n
orm
al,
AD
HD
, Grp
1 r
ecei
ved
met
hylp
heni
date
, Grp
2re
ceiv
ed p
emol
ine
Non
e / N
S /N
S /N
S /N
S/ N
S A
CT
: mot
or a
ctiv
ity “
whi
leaw
ake”
and
“w
hile
asl
eep”
,O
ther
s: C
onno
rs p
aren
ts’r
at-
ing
scal
e (h
yper
activ
ity);
Glo
bal r
atin
g sc
ale
(of
impr
ovem
ent)
NS/
NS/
low
sam
ple
size
W
ake
activ
ity, s
leep
act
ivity
and
hype
ract
ivity
dec
reas
edw
ith m
ethy
lphe
nida
te.
Aw
ake
activ
ity in
crea
sed
and
asle
epac
tivity
and
hyp
erac
tivity
inde
x de
crea
sed
with
pem
o-lin
e (s
tatis
tical
test
ing
NS)
Min
imal
spe
cifi
c in
form
atio
non
the
stud
y’s
met
hodo
logy
and
the
lack
of
stat
istic
al te
st-
ing
repo
rted
mak
es th
e fi
nd-
ings
dif
ficu
lt to
inte
rpre
t.
Mis
him
a (9
9)
4C-b
RC
T, u
nblin
ded,
cro
ssov
erde
sign
/ N
H /
Ent
ire
24-h
s;co
ntin
uous
AC
Tfo
r 1
wk
pre-
Tx,
2 w
ks T
x, 1
wk
post
-Tx,
≥4
wks
was
hout
cro
ss-o
ver;
Tx=
5-80
00 lu
x 9-
11am
;C
ontr
ol=
300
lux
9-11
am
22 (
NS)
/ G
rp1
81, G
rp2
78 /
Grp
1 V
ascu
lar
dem
entia
,G
rp2
Alz
heim
er’s
dem
entia
Non
e / (
AM
I) /
ndom
wri
st /
1 m
in /
NS
/ act
ivity
cou
nts
used
, sle
ep n
ot s
core
d
AC
T: T
otal
, day
time
& n
ight
-tim
e ac
tivity
, % n
ight
/tota
lac
tivity
DSM
IV
Dx
of v
ascu
lar
dem
entia
or A
lzhe
imer
’s /
mix
ed d
emen
tia e
xclu
ded
/U
nabl
e to
blin
d T
x, s
mal
l N
Vas
cula
r D
emen
tia: d
aily
brig
ht li
ght r
educ
es n
ight
time
activ
ity; A
lzhe
imer
’sD
emen
tia: b
righ
t lig
ht d
oes
not a
ffec
t act
ivity
rhy
thm
Show
s A
CT
dete
cted
Tx
effe
ct in
wel
l-de
sign
ed, c
on-
trol
led
tria
l. S
ugge
st A
CT
usef
ul to
det
ect o
utco
me
inC
R T
x st
udy
Moo
rcro
ft (
145)
5D-b
Unb
linde
d, n
onra
ndom
ized
,ob
serv
atio
nal s
tudy
/ H
ome
/N
octu
rnal
onl
y fr
om 8
:00p
mun
til 1
0 m
ins
afte
r aw
aken
-in
g; 3
Nt A
CT
NS
(15)
/ (1
9-62
) / P
eopl
eab
le to
sel
f-aw
aken
at a
sel
f-pr
edet
erm
ined
tim
e w
/o e
xter
-na
l mea
ns
log
to g
et in
tend
ed W
time
for
the
next
mor
ning
/Act
igra
ph(A
MI)
/ N
S / N
S / N
S / N
S
log;
AC
T: S
leep
& W
peri
ods,
time
of f
inal
aw
aken
ing
Abl
e to
sel
f-aw
aken
/ N
S /
Low
sam
ple
size
D
ata
sugg
este
d th
at th
ese
peop
le c
ould
aw
aken
at a
sel
f-de
term
ined
tim
e.
Mor
mon
t (15
0)
4C-b
Unb
linde
d, n
onra
ndom
ized
,ob
serv
atio
nal s
tudy
, coh
ort
stud
y, lo
ngitu
dina
l stu
dy /
Hom
e / E
ntir
e 24
-hs;
3D
AC
T
200
(192
) / 5
8 (2
0-75
) /
Am
bula
tory
met
asta
tic c
ol-
orec
tal c
ance
r pt
s re
ferr
ed f
orch
rono
mod
ulat
ed c
hem
othe
r-ap
y
Non
e / A
CT
(AM
I) /
NS
/ 1m
in /
NS
/ NS
End
ocri
ne m
easu
res:
cir
cadi
-an
cha
nges
in c
ortis
ol &
WB
C; A
CT
: aut
o-r
at 2
4h &
adi
chot
omy
inde
x co
mpa
ring
amou
nts
of a
ctiv
ity w
hen
inbe
d &
out
of
bed,
mea
n ac
tiv-
ity; M
ood:
HA
DS
(sca
le o
fan
xiet
y an
d de
pres
sion
);Q
LQ
-C30
(Q
OL
)
NS
/ Poo
r ge
nera
l hea
lth(W
HO
per
form
ance
sta
tus
72)
/ NS
Pts
w/ m
arke
d re
st/a
ctiv
ityrh
ythm
s ha
d a
5-fo
ld h
ighe
rsu
rviv
al r
ate
at 2
yrs
, had
a 5
-fo
ld h
ighe
r su
rviv
al r
ate
at 2
yrs,
had
bet
ter
QO
L&
rep
ort-
ed le
ss f
atig
ue. R
est/a
ctiv
ityrh
ythm
rem
aine
d a
sign
ific
ant
pred
icto
r of
sur
viva
l in
mul
ti-va
riat
e an
alys
is.
Ous
land
er (
166)
5D-b
Cas
e se
ries
, des
crip
tive
/ NH
/N
octu
rnal
onl
y fo
r 9
hs; A
CT
1 N
t BL
, 2 m
os la
ter,
AC
T1
Nt 2
nd B
L
73 (
73)
/ 86.
9±7.
2 /
Inco
ntin
ence
N
S / N
S / N
S / 2
min
s / N
S /
NS
A
CT
: Sle
ep in
terv
als
NS
/ NS
/ No
info
rmat
ion
onho
w (
slee
p) A
CT
reco
rded
In
cont
inen
ce w
as n
ot r
elat
edto
sle
ep d
isru
ptio
n B
uilt
own
actig
raph
Pank
hurs
t (1
46)
4C-b
Unb
linde
d, n
onra
ndom
ized
,ob
serv
atio
nal s
tudy
, coh
ort
stud
y, c
ross
-sec
tiona
l stu
dy /
Hom
e / N
octu
rnal
for
NS
hs;
8Nt A
CT
Stud
y1 9
6 (9
2) /
(23-
67)
/co
uple
s sl
ept t
oget
her,
Stud
y2 (
95)
/ NS
/ sub
ject
sw
ho s
lept
alo
ne. A
ll su
bjec
tsw
ere
com
mun
ity d
wel
ling
peop
le li
ving
nea
r 4
UK
air
-po
rts
Log
/ G
aehw
iler
Ele
ctro
nics
Hom
brec
htik
on, S
witz
erla
nd /
NS
/ 30
sec
/ >
.1g
/A
CC
OR
D (
auth
or’s
ow
n pr
o-gr
am)
log;
AC
T:”
actib
lip”
inci
-de
nces
N
S / H
ypno
tics,
pai
n th
atse
riou
sly
disr
upte
d sl
eep
/C
omor
bidi
ty w
as n
otad
dres
sed
Men
had
mor
e m
ovem
ents
.Fo
r sl
eep
part
ners
, 1/3
of
mov
emen
ts w
ere
com
mon
tobo
th p
artn
ers;
sub
ject
s sl
eep-
ing
w/ p
artn
er h
ad m
ore
mov
emen
ts; m
ovem
ents
decr
ease
d w
hen
part
ner
abse
nt
AC
Tda
ta n
ot s
core
d as
S/W
but a
s “a
ctib
lips”
(m
ovem
ent)
Pat-
Hor
encz
yk (
160)
4C-b
Unb
linde
d, n
onra
ndom
ized
,ob
serv
atio
nal s
tudy
/ N
H /
Ent
ire
24-h
s; 1
D A
CT
77 (
67)
/ Grp
1 85
, Grp
2 87
,A
ll 85±7
.3 (
60-1
00)
/ NH
res
-id
ents
w/ d
emen
tia; S
DG
-M
MSE
<20
, MM
DG
-MM
SE≥2
0
Non
e / A
ctill
ume
/ NS
/ NS
/≥.
003g
/ N
S A
CT
: min
s as
leep
eac
h hr
,fu
lly a
slee
p ea
ch h
r, fu
llyaw
ake
each
hr
NS
/ Non
e (m
ost p
ts h
ad m
ul-
tiple
med
ical
dia
gnos
es a
ndw
ere
taki
ng m
ultip
le m
eds)
/N
S
SDG
sle
pt m
ore
at e
ach
hr,
and
mor
e th
an d
urin
g m
eal
times
. Pea
k of
sle
ep o
ccur
red
2 hs
ear
lier
in S
DG
Grp
,M
MD
G h
ad m
ore
wak
eful
-ne
ss a
t nig
ht a
nd S
DG
had
mor
e sl
eepi
ness
dur
ing
D
Paul
(20
4)
4C-b
Unb
lend
ed, n
onra
ndom
ized
,ob
serv
atio
nal s
tudy
/hom
e /
entir
e 24
h, A
CT
5 D
pri
or to
re-s
uppl
y m
issi
on a
nd u
ntil
mis
sion
com
plet
ed
NS
(N
S) N
S (N
S) /
norm
al
Non
e / P
reci
sion
con
trol
Des
ign
/ wri
st /
1 m
inut
e / N
S/ W
in A
ct 1
.2
AC
T: n
um a
nd d
ur o
f sl
eep
epis
odes
; Oth
ers,
psy
chom
o-to
r ta
sks;
ser
ial c
hoic
e re
ac-
tion
time,
logi
cal r
easo
ning
task
ser
ial s
ubtr
actio
n ta
skan
d m
ultit
ask
Incl
usio
n: C
anad
ian
Air
Com
man
d pi
lots
and
co-
pilo
ts/ N
S/ N
S
Am
ount
of
daily
sle
epde
crea
sed
duri
ng th
e 3
Dpr
ior
to m
issi
on.
Dur
ing
mis
-si
on, w
orst
sle
ep o
n ni
ght 2
.D
urin
g m
issi
on, d
ecre
ased
self
-rat
ed a
lert
ness
and
incr
ease
d fa
tigue
Cit
atio
n - A
utho
r/
Evi
denc
e L
evel
St
udy
Cri
teri
a D
esig
n /
Loc
atio
n / P
roto
col
Sam
ple
Size
(C
ompl
eted
Stud
y) /
Mea
n A
ge (
Ran
ge)
/M
edic
al C
ondi
tion
s
Com
pari
son
Mea
sure
s /
Act
igra
ph a
ppar
atus
/P
lace
men
t / E
poch
Len
gth
/Se
nsit
ivit
y / S
cori
ng
Out
com
e M
easu
res
Incl
usio
n / E
xclu
sion
/ B
ias
Stud
y C
oncl
usio
n fr
ompa
per
Com
men
ts f
rom
Rev
iew
er
Actigraphy Review Paper—Ancoli-Israel et alSLEEP, Vol. 26, No. 3, 2003 389
Polla
k (1
38)
4C-b
Cas
e-co
ntro
l stu
dy /
Hom
e /
Ent
ire
24-h
s; 1
2 N
t&D
AC
T15
(15
) / G
rp1
75.9
, Grp
272
.0 /
NS
Non
e / V
italo
g PM
S-8
/ wri
st/ 1
min
/ N
S / N
S lo
g; A
CT
: act
ivity
N
S / N
S / S
mal
l sam
ple
size
R
x us
es (
i.e. t
hose
taki
ngm
eds
at B
T)
beco
me
activ
e1.
5 hs
ear
lier
in th
e m
orni
ng
Polla
k (1
58)
4C-b
Cas
e se
ries
/ H
ome
/ Ent
ire
24-h
s; 9
D&
Nt A
CT
88 (
44 p
airs
) / G
rp1
77.9
(64
-92
) G
rp2
61.9
(29
-86)
/ N
S N
S / M
ML
/ Ndo
m w
rist
/0.
5 m
in /
NS
/ NS
log;
AC
T: a
ctiv
ity le
vel
65+
; hav
e ca
re g
iver
; dis
rup-
tive
noct
urna
l beh
avio
r(D
NB
) / N
S / N
S
Beh
avio
r of
eld
ers
& c
are-
give
rs w
ere
less
sim
ilar
inda
ytim
e th
an a
t Nt;
at N
t it
was
eld
ers
that
initi
ated
inte
r-ac
tion,
thus
dis
turb
ing
slee
pof
car
egiv
er
Pres
ents
a p
artia
l mat
hem
ati-
cal m
odel
of
spon
tane
ous
mot
or b
ehav
ior.
Use
d vi
deo
at N
t to
wat
ch in
tera
ctio
nsbe
twee
n el
der
& c
areg
iver
Red
eker
(15
6)
4C-b
Obs
erva
tiona
l stu
dy; l
ongi
tu-
dina
l stu
dy /
Hom
e; o
ut-o
f-la
b ho
spita
l bed
/ E
ntir
e 24
-hs
; 7D
pos
tope
rativ
e in
hos
pi-
tal,
7D E
arly
rec
over
y at
hom
e, 7
D r
esum
e ac
tiviti
es,
7D c
ompl
ete
resu
mpt
ion
ofac
tiviti
es
22 (
13)
/ Grp
1 63
.7±9
.9 (
43-
83),
Grp
2 62±1
0.76
(43
-78)
/C
oron
ary
arte
ry b
ypas
s gr
aft
surg
ery
NS
/ MM
L/ n
dom
wri
st /
1m
in /
NS
/ AC
TIO
N
AC
T: T
ST, n
um w
akes
, mea
nW
time,
mea
n sl
eep
inte
rval
,%
sle
ep; S
ickn
ess
Impa
ctPr
ofile
NS
/ NS
/ Low
sam
ple
in f
ol-
low
-up
Sign
ific
ant d
aytim
e sl
eep
&fr
agm
ente
d ni
ghtti
me
slee
pdu
ring
hos
pita
lizat
ion;
Ove
r 6
mos
per
iod
post
-sur
gery
,sl
eep
cons
olid
ated
& d
aytim
esl
eep
low
er; P
erce
ived
sle
epim
prov
emen
ts c
onsi
sten
t w/
AC
Tm
easu
res
Nic
e lo
ngitu
dina
l fol
low
-up
(6 m
os)
Red
eker
(20
5)
4C-b
Cas
e se
ries
, tim
e se
ries
/ O
ut-
of-l
ab h
ospi
tal b
ed /
Ent
ire
24-h
s; C
ontin
uous
for
ent
ire
hosp
ital D
25 (
17)
/ Grp
1 63
.67±
9.86
(42.
83)
/ Cor
onar
y by
pass
surg
ery
Non
e / M
ML
/ ndo
m /
1-m
in/ N
S / A
ctio
n A
CT
: Act
ivity
cou
nts;
Sick
ness
Im
pact
Pro
file
N
S / N
S / S
mal
l sam
ple
Rel
atio
nshi
p be
twee
n rh
yth-
mic
& li
near
pat
tern
s of
act
iv-
ity w
/ rec
over
y; i.
e. P
ositi
vere
latio
nshi
p be
twee
n le
ngth
of
stay
& d
ysfu
nctio
n w
/ sho
rter
activ
ity p
erio
ds a
ssoc
iate
d w
/le
ss d
ysfu
nctio
n. P
ositi
ve c
ir-
cadi
an a
ctiv
ity p
erio
ds w
ere
rela
ted
to b
ette
r fu
nctio
ning
& s
hort
er s
tay
Loo
ked
at r
hyth
ms
as a
n ou
t-co
me
Red
eker
(15
7)
4C-b
Obs
erva
tiona
l stu
dy, d
escr
ip-
tive,
cor
rela
tiona
l / O
ut-o
f-la
bho
spita
l bed
/ E
ntir
e 24
-hs;
Con
tinuo
us f
or c
ours
e of
hos
-pi
tal s
tay
(ran
ge =
1-1
0D)
40 (
33)
/ M 5
6.1±
11.9
, F59
.5±1
0.9
/ Car
diac
dis
ease
:ac
ute
myo
card
ial i
nfar
ctio
n,un
stab
le a
ngin
a
Non
e / M
ML
/ ndo
m /
1-m
in /
NS
/ Act
ion
3 A
CT
: Nig
ht in
terv
al, T
ST,
SE, n
um w
akes
, dur
of
slee
pin
terv
al, d
ur o
f w
akes
; Ver
an&
Syn
der-
Hal
pern
Sle
epSc
ale-
pts.
Per
cept
ion
of th
eir
slee
p; S
leep
loss
sub
scal
e of
pt. S
leep
scr
eene
r
Exc
lusi
on: K
now
n sl
eep
dis-
orde
rs, p
sych
otro
pic
med
s,bl
indn
ess,
dea
fnes
s / N
S
pre-
hosp
ital e
ndog
enou
s va
ri-
able
s, a
ge, g
ende
r, &
New
Yor
k H
eart
Ass
ocia
tion
func
-tio
nal c
lass
ific
atio
n an
d pr
e-ho
sp s
leep
loss
all
rela
ted
toSE
& d
ur o
f w
akes
onc
e ho
s-pi
taliz
ed. P
re-h
osp
seve
rity
of
card
iac
dise
ase
grea
test
cor
re-
late
Red
eker
(15
5)
4C-b
Cas
e se
ries
/ O
ut-o
f-la
b ho
s-pi
tal b
ed /
Ent
ire
24-h
s;C
ontin
uous
for
hos
pita
l sta
y
22 (
NS)
/ G
rp1
57.1
2±6.
6(4
7-65
), G
rp2
72.3
6±4.
1 (6
6-77
) / C
oron
ary
arte
ry b
ypas
s
Non
e / M
ML
/ ndo
m /
1 m
in/ N
S / A
CT
ION
3
AC
T: a
ctiv
ity c
ount
s, c
osin
orpa
ram
eter
s; S
ickn
ess
Impa
ctPr
ofile
Exc
lusi
on: H
/o o
f ps
ychi
atri
cdi
sord
er, n
euro
mus
cula
r di
s-or
der,
chro
nic
rena
l fai
lure
,bl
indn
ess,
dea
fnes
s / S
mal
lSa
mpl
e
Act
ivity
leve
ls &
str
engt
h of
CR
s in
crea
sed
over
Ds
2-5
post
-ope
rativ
e. I
n ol
der
adul
tsit
took
long
er (
at a
slo
wer
rate
)
Exa
min
ed th
e ef
fect
of
age
Rey
ner
(147
)
4C-b
Unb
linde
d, n
onra
ndom
ized
,ob
serv
atio
nal s
tudy
/ H
ome
/N
octu
rnal
onl
y fo
r N
S hs
;15
Nt A
CT
NS
(400
) / G
rp1
(20-
34),
Grp
2 (3
5-49
), G
rp3
(50-
70)
/ Sle
ep n
orm
al C
omm
unity
dwel
ling
peop
le li
ving
nea
r 4
UK
air
port
s
log
/ “Sw
iss-
type
” G
aehw
iler
elec
tron
ics
/ wri
st /
30 s
ec /
NS
/ Hor
ne e
t al,
“SO
n al
go-
rith
m”
log;
AC
T: t
ime
of S
On,
SQ
do
or-t
o-do
or s
urve
y / s
leep
-pr
omot
ing
med
s or
exc
essi
veal
coho
l / N
S
Tim
e of
SO
n w
as e
ffec
ted
byge
nder
& a
ge; a
nd d
iffe
red
from
log
and
AC
T; A
vera
gem
ovem
ent d
eclin
ed w
/ age
,an
d m
en h
ad m
ore
mov
emen
tth
an w
omen
Sade
h (1
72)
4C-b
Obs
erva
tiona
l., lo
ngtit
udin
al /
hom
e / n
octu
rnal
, 5N
13
5/13
5 / M
, 69,
F, 6
6, N
S(7
.2-1
2.7)
/ no
rmal
, NS
Non
e / M
ini-
mot
ionl
ogge
r(A
MI)
/ no
n-do
m w
rist
/ 1-
min
/ N
S / S
adeh
act
igra
phic
scor
ing
algo
rith
m
AC
T; S
O, m
orni
ng u
p tim
e,to
tal s
leep
per
iod,
% s
leep
, #aw
akes
, lon
gest
sle
ep p
erio
d,qu
iet s
leep
%, n
euro
psyc
hte
sts
NS
/ NS
K
ids
frag
men
ted
slee
p ha
dlo
wer
per
form
ance
and
mor
ebe
havi
or p
robl
ems
Cit
atio
n - A
utho
r/
Evi
denc
e L
evel
St
udy
Cri
teri
a D
esig
n /
Loc
atio
n / P
roto
col
Sam
ple
Size
(C
ompl
eted
Stud
y) /
Mea
n A
ge (
Ran
ge)
/M
edic
al C
ondi
tion
s
Com
pari
son
Mea
sure
s /
Act
igra
ph a
ppar
atus
/P
lace
men
t / E
poch
Len
gth
/Se
nsit
ivit
y / S
cori
ng
Out
com
e M
easu
res
Incl
usio
n / E
xclu
sion
/ B
ias
Stud
y C
oncl
usio
n fr
ompa
per
Com
men
ts f
rom
Rev
iew
er
Actigraphy Review Paper—Ancoli-Israel et alSLEEP, Vol. 26, No.3, 2003 390
Sade
h (2
06)
4C-b
Cas
e-co
ntro
l stu
dy /
Hom
e /
Ent
ire
24 h
s 3-
4D
NS
(NS)
/ G
rp1
12.1
(8.
2-15
.4),
Grp
2 12
.4 (
8.9-
14.7
) /
asth
ma
Non
e / A
MA
-32
(AM
I) /
ndom
/ 1
min
/ N
S / A
SApr
o-gr
am
AC
T: S
OL
, TST
, s1e
ep p
er-
cent
, lon
gest
SP,
% q
uiet
slee
p; a
ctiv
ity le
vel;
Pulm
onar
y fu
nctio
n, a
sthm
ase
veri
ty, s
leep
Q b
y ch
ild &
pare
nt
NS
/ NS
/ NS
Ast
hma
kids
wer
e m
ore
activ
e du
ring
sle
ep &
had
less
% q
uiet
sle
ep; b
oys
w/ a
sth-
ma
fell
asl
eep
fast
er th
angi
rls;
con
trol
gir
ls f
ell a
slee
pfa
ster
than
boy
s; %
slee
p &
mea
n ac
tivity
cor
rela
ted
w/
even
ing
& m
orni
ngPu
lmon
ary
peak
exp
irat
ory
flow
mea
sure
s &
poo
r sl
eep
asso
ciat
ed w
/ mor
e se
vere
asth
ma
Was
fir
st h
ome-
base
d ev
alua
-tio
n of
ast
hma
& s
leep
inch
ildre
n
Sade
h (2
07)
4C-b
Obs
erva
tiona
l stu
dy /
out o
fla
b ho
spita
l bed
/ E
ntir
e 24
hrs;
3D
39 (
NS)
/ G
rp1
9.51
±1.
9 (7
-14
) / S
ever
e ps
ychi
atri
c pr
ob-
lem
s
Non
e / A
MA
-32
/ non
-dom
/1
min
/ N
S / A
SAA
CT
: SO
, TSP
, % s
leep
, tru
esl
eep
time,
long
est s
leep
per
-ce
nt, %
qui
et s
leep
; WIS
C -
R, D
epre
ssio
n sc
ale,
psy
cho-
logi
cal t
ests
, Abu
se h
isto
ry
NS
/ NS
/ NS
Low
er S
Q d
urin
g ho
spita
liza-
tion
stro
ngly
ass
ocia
ted
w/
self
rep
ort o
n de
pres
sion
,ho
pele
ssne
ss &
low
sel
fes
teem
in c
hild
ren
w/ s
ever
ebe
havi
or d
isor
ders
Saka
kiba
ra (
207)
4C-b
Unb
linde
d; R
ando
miz
ed;
cros
s-ov
er d
esig
n / H
ome
/E
ntir
e 24
-hs;
5N
t AC
T, P
SGla
st 2
Nt
10 (
10)
/ 59.
7 (5
0-69
) /
Nor
mal
N
S / M
ML
/ ndo
m /
NS
/ NS
/ Col
e et
al
log;
PSG
; AC
T: m
ean
activ
i-ty
, mov
emen
t ind
ex, d
aytim
eac
tivity
leve
l
Exc
lusi
on: O
n m
eds,
men
tally
ill, p
hysi
cally
ill /
Sm
all s
am-
ple
60 m
ins
of b
righ
t lig
ht in
the
mor
ning
red
uced
noc
turn
alac
tivity
Sche
rder
(11
4)
4C-b
Ran
dom
ized
/ N
S / E
ntir
e 24
-hs
; 4D
AC
TB
L1,
4D
AC
Taf
ter
6wk
Tx;
4D
AC
Taf
ter
6wks
no
Tx
16 (
15)
/ Grp
1 81
.7 (
70-9
1) /
Alz
heim
er’s
Dis
ease
N
S / N
o in
fo
AC
T: i
s (i
nter
daily
sta
bilit
y);
IVin
terd
aily
var
iabi
lity;
RA
rela
tive
ampl
itude
Exc
lusi
on: A
lcoh
olis
m, P
sych
illne
ss, c
ereb
ral t
raum
a,C
ereb
rova
scul
ar d
is, E
pile
psy,
etc.
/ N
ot e
noug
h in
fo
TE
NS
incr
ease
d IS
Schl
esin
ger
(208
)
4C-b
Unb
lend
ed, n
onra
ndom
ized
,ob
serv
atio
nal s
tudy
/hom
e /
noct
urna
l onl
y fo
r N
S h
/ 3 N
tA
fter
whi
plas
h in
jury
and
3N
t f/
u (3
-5 m
onth
s la
ter
NS
(34)
Grp
1, M
, 4, F
, 14;
Grp
2, M
, 5, F
, 11
/ Grp
1,
36.5
, (2
0-48
, SD
= 8
.5)
Grp
2, 3
3.2,
(20
-50,
SD
= 8
.0)
,no
rmal
, Grp
1; a
cute
whi
plas
hin
jury
in tr
affi
c ac
cide
nt, G
rp2,
nor
mal
con
trol
s
Non
e / A
MI
/ wri
st /
NS
/ NS
/ Act
igra
ph S
tatis
tical
ana
lysi
s Sl
eep
diar
y, lo
g; A
CT,
SL
,to
tal c
umul
ativ
e S
dur,
SEan
d nu
m a
rous
als
Exc
lusi
on G
rp 2
: no
med
s, n
osl
eep
prob
lem
s, n
o h/
ow
hipl
ash
inju
ry
No
sign
ific
ant d
iffe
renc
es in
AC
Tm
easu
red
slee
p be
twee
nw
hipl
ash
pts
and
cont
rols
. In
slee
p lo
gs, w
hipl
ash
pts
had
prol
onge
d SL
, and
impa
ired
SQ.
In w
hipl
ash
pts,
gre
ater
sign
s/sy
mpt
oms
of w
hipl
ash
corr
elat
ed w
ith g
reat
er n
umar
ousa
ls a
nd lo
wer
SE
.
Schn
elle
(20
9)
5D-b
Con
trol
led
clin
ical
tria
l,un
blin
ded,
non
rand
omiz
ed,
cros
s-ov
er d
esig
n / N
H /
Noc
turn
al f
or 1
0 hs
; 5N
t AC
T
267
(184
) / N
o in
fo /
NS
NS
/ NS
AC
T: P
eak
activ
ity; m
ean
activ
ity
Noi
se &
ligh
t red
uced
cor
re-
late
d w
/ cha
nge
in %
sle
epbu
t no
chan
ge in
D s
leep
(by
obse
rvat
ion)
or
actu
al s
leep
vari
able
s
Mea
sure
d no
ise
leve
ls, u
sed
AC
Ton
ly a
t Nt,
used
obs
er-
vatio
n of
sle
ep d
urin
g D
Schw
ietz
er (
210)
5D-b
RC
T; D
B; c
ompa
rativ
e T
x /
Lab
orat
ory
/ 3D
AC
TN
S (1
2) /
31.3
±8.
1 / N
orm
al;
Hyp
erse
nsiti
vity
to e
nvir
on-
men
tal a
llerg
en
MSL
T/ (
AM
I) /
NS
/ 1 m
in /
NS
/ NS
Log
: VA
S; M
SLT,
sim
ulat
edas
sem
bly
line
task
N
o A
CT
resu
lts r
epor
ted.
afte
r 3
Ds
amou
nt o
f sl
eepi
-ne
ss r
epor
ted
and
on M
SLT,
sam
e in
all
Grp
s
Not
giv
en a
ny in
fo o
n ac
ti-gr
aph
resu
lts
Sham
ir (
211)
4C-b
RC
T; D
B; c
ross
-ove
r de
sign
;co
mpa
rativ
e T
x / N
S / 3
Nt
AC
Tdu
ring
eac
h T
x ph
ase
2mg
mel
vs.
pla
cebo
27 (
19)
/ 42±
5 (2
4-67
) /
Inso
mni
a; S
chiz
ophr
enia
N
S / S
omni
tor
/ NS
/ NS
/ NS
/ NS
AC
T: S
E, S
OL
, TST
, WA
SO,
Frag
men
tatio
n in
dex,
num
wak
es
Exc
lusi
on: L
iver
or
rena
l dis
-ea
se o
r ot
her
psyc
h di
sord
ers,
seve
re p
hysi
cal i
llnes
s / M
uch
info
rmat
ion
mis
sing
on
AC
T
SE im
prov
ed w
/ mel
com
-pa
red
to p
lace
bo in
thos
e w
host
arte
d ou
t w/ p
oor
slee
p
Ana
lyze
d th
ose
w/ p
oor
slee
pto
sta
rt o
ut w
/ sep
arat
ely
Shilo
(21
2)
4C-b
Obs
erva
tiona
l stu
dy /
Out
-of-
lab
hosp
ital b
ed /
Ent
ire
24-
hs; 7
2 hs
AC
T
NS
(14)
/ G
rp1
61±
11 (
39-7
6)G
rp2
59±
11 (
49-7
4) /
All
onIC
U
NS
/ Som
nito
r / N
S / N
S / N
S/ N
S M
elat
onin
; AC
T: T
STV
ery
little
sle
ep in
a 7
2-h
peri
od 6
-SM
Tab
norm
al in
all
w/ n
o no
ctur
nal r
ise
Shilo
(21
3)
4C-b
Com
para
tive
Tx
(mel
/pla
ce-
bo)
/ Out
-of-
lab
hosp
ital b
ed /
Ent
ire
24-h
s; 3
D A
CT
NS
(8)
/ 62±
14 (
30-7
2) /
On
pulm
onar
y IC
U-C
OPD
N
S / S
omni
tor
/ ndo
m w
rist
/1m
in /
NS
/ NS
AC
T: T
ST, n
um a
wak
enin
gs
NS
/ NS
/ Sm
all s
ampl
e bu
tun
ders
tate
d po
pula
tion
Mel
aton
in im
prov
ed s
leep
-bo
th d
urat
ion
& q
ualit
y
Cit
atio
n - A
utho
r/
Evi
denc
e L
evel
St
udy
Cri
teri
a D
esig
n /
Loc
atio
n / P
roto
col
Sam
ple
Size
(C
ompl
eted
Stud
y) /
Mea
n A
ge (
Ran
ge)
/M
edic
al C
ondi
tion
s
Com
pari
son
Mea
sure
s /
Act
igra
ph a
ppar
atus
/P
lace
men
t / E
poch
Len
gth
/Se
nsit
ivit
y / S
cori
ng
Out
com
e M
easu
res
Incl
usio
n / E
xclu
sion
/ B
ias
Stud
y C
oncl
usio
n fr
ompa
per
Com
men
ts f
rom
Rev
iew
er
Actigraphy Review Paper—Ancoli-Israel et alSLEEP, Vol. 26, No. 3, 2003 391
Shin
koda
(21
4)
4C-b
Obs
erva
tiona
l stu
dy /
Hom
e /
Ent
ire
24-h
s; ~
4 m
os A
CT
NS
(4)
/ (26
-31)
/ N
orm
al;
preg
nant
or
post
-del
iver
y N
S / A
MA
-32C
L(A
MI)
/nd
om w
rist
/ 1
min
/ N
S / N
S lo
g / A
CT
: TST
, SE
, SO
L,
Nap
s, W
ASO
N
S / N
S / L
ow s
ampl
e bu
tun
usua
l pop
ulat
ion
Aft
er d
eliv
ery,
sle
ep b
ecam
eir
regu
lar
& W
ASO
wen
t up
Shir
ota
(215
)
4C-b
Obs
erva
tiona
l stu
dy /
Hom
e /
Ent
ire
24-h
s; 1
0-14
D A
CT
NS
(28)
/ G
rp1
74.1
±4.
9,G
rp2
73.0
±5.
0 / N
orm
al
NS
/ NS
/ nd
om /
NS
/ NS
/N
S
log
/ AC
T: m
ean
act
ivity
,T
ST, S
OL
, TST
-nap
N
S / N
S / N
S H
i vol
ition
al a
ged
pts
had
wel
l str
uctu
red
slee
p an
dm
ost t
ook
1400
h na
p; lo
wvo
litio
nal h
ad p
oor
stru
ctur
edsl
eep
& to
ol ti
me-
depe
nden
tna
p ~
8h a
fter
aw
aken
ing
Stei
n (2
16)
5D-b
Con
trol
led
clin
ical
tria
l; D
B;
cros
s-ov
er d
esig
n / H
ome
/N
octu
rnal
onl
y fo
r 16
hs;
2-
18h
peri
ods
duri
ng e
ach
of 4
wks
of
prot
ocol
NS
(25)
/ 8±
1.8
(6-1
2) /
AD
HD
N
S / N
S / N
S / N
S / N
S / N
S lo
g; A
CT
: act
ivity
leve
l, SO
L,
TST
, num
aw
ake,
dur
atio
n of
wak
es
NS
/ NS
/ NS
Slep
t les
s w
hen
Rx
give
n T
IBth
an in
pla
cebo
The
ssin
g (1
04)
5D-b
Cro
ss-s
ectio
nal s
tudy
/L
abor
ator
y / D
iurn
al o
nly
for
8 hs
; 1D
AC
T(w
hile
asl
eep
in la
b du
ring
D)
30 (
24)
/ 21
(18-
29)
/ Nor
mal
N
S /(
AM
I) /
wri
st /
1 m
in /
NS
/ NS
log;
AC
T: T
ST, W
ASO
N
S / N
S / N
S N
o di
ffer
ence
in s
leep
betw
een
the
diff
eren
t lig
htco
nditi
ons
Test
ed s
hift
wor
kers
dur
ing
the
D a
fter
a n
ight
w/ b
righ
tlig
ht T
x
Usu
i (21
7)
4C-a
AC
Tco
mpa
red
with
oth
erte
chni
ques
/hom
e/en
tire
24 h
,5-
7 D
AC
T&
Log
s
18 (
18)
M, 1
1, F
, 7/ 3
0.1
(NS)
norm
al
Slee
p lo
g, d
iary
/Mot
ionl
ogge
r-A
MI/
non
-dom
wri
st /
1 m
in /0
.01
g/ra
d/s
/N
S
Slee
p di
ary,
log,
AC
T: s
leep
min
utes
, wak
e m
inut
es
NS/
NS/
low
sam
ple
size
Se
nsiti
vity
(sl
eep)
bet
wee
nA
CT
and
log
was
86.
7% a
ndsp
ecif
icity
(w
ake)
was
97.0
4%
Use
d A
CT
as g
old
stan
dard
tova
lidat
e sl
eep
log
in h
ealth
yad
ults
Usu
i (21
8)
4C-a
AC
Tco
mpa
red
with
oth
erte
chni
ques
/hom
e/ 2
-7D
AC
T&
log
35 (
35)
Grp
1; 2
7.6
, (N
S)G
rp 2
; 74.
3, (
NS)
Grp
3,
42.1
; (N
S) n
orm
al, n
arco
lep-
sy, o
ther
; sle
ep s
tate
mis
con-
cept
ion,
idio
path
ic h
yper
som
-ni
a, D
SPS
Slee
p lo
g, d
iary
/Mot
ionl
ogge
r –
AM
I / n
on-
dom
wri
st /
1 m
in /
0.01
g/ra
d/s
/ Col
e
Slee
p di
ary,
log
, AC
T: s
leep
& w
ake
min
utes
N
S/N
S/N
S Sl
eep
log
does
not
alw
ays
dete
ct s
leep
sta
te. A
gree
men
tdr
oppe
d du
ring
sle
ep-w
ake
tran
sitio
n pe
riod
s. S
ensi
tivity
was
low
er in
pat
ient
s w
ithsl
eep
diso
rder
s th
an n
orm
als.
Use
d ac
tigra
phy
as g
old
stan
-da
rd to
val
idat
e sl
eep
logs
inhe
alth
y vs
. eld
erly
vs.
sle
epdi
sord
ered
pat
ient
s
Usu
i (21
9)
5D-a
Unb
lend
ed, r
ando
miz
ed,
cros
s-ov
er d
esig
n, c
ase
seri
es/ h
ome
/ ent
ire
24 h
3D
AC
TB
L, 4
D A
CT
Tx
1, 3
D A
CT
was
hout
, 4 D
AC
TT
x 2.
Tx
=2
h br
ight
ligh
t 250
0 lu
x at
BT
or tr
iazo
lam
.125
mg
4 (3
) / N
S (
64-8
0) /
norm
al,
NS
Slee
p lo
g, d
iary
, VA
S-sl
eepi
-ne
ss /
Mot
ionl
ogge
r, A
MI
/no
n-do
m w
rist
/ N
S / .
01 g
/C
ole
et a
l
Slee
p di
ary,
log;
AC
T; d
ayT
ST, n
ight
TST
; Oth
ers:
sle
eplo
g va
riab
les:
Son
tim
e, S
Off
time,
day
TST
in m
aps
NS/
NS/
low
sam
ple
size
, no
plac
ebo
Dec
reas
ed D
and
Nt T
ST(b
yA
CT
) w
ith b
righ
t lig
ht.
Incr
ease
d N
TT
ST(b
y A
CT
with
tria
zola
m.
Find
ings
less
-en
ed o
ver
the
4 D
for
bot
hT
x.
Van
Lon
den
(220
)
4C-b
Obs
erva
tiona
l stu
dy /
NS
/E
ntir
e 24
-hs;
5D
AC
TN
S (7
8) /
Grp
1 45
.2±
14.4
(22-
77),
Grp
2 42
.2±
16.3
(19
-73
) / D
epre
ssio
n
NS
/ Gae
hwile
r / n
dom
/ 30
sec
/ NS
/ NS
log
/ AC
T: m
ean
activ
ity d
ur-
ing
W&
sle
ep; i
mm
obili
tydu
ring
sle
ep; f
ragm
enta
tion
NS
/ NS
/ NS
Dur
ing
W: p
ts <
mea
n ac
tivi-
ty th
an c
ontr
ols;
pts
low
erfr
agm
enta
tion
& lo
wer
TST
;D
urin
g sl
eep:
pts
had
hig
her
activ
ity
Van
Som
eren
(11
5)
4C-b
Obs
erva
tiona
l stu
dy /
Hom
e18
=N
t; N
H 1
6=N
t / E
ntir
e24
-hs;
155
hs
AC
T
42 (
34)
/ 72±
1.2
/A
lzhe
imer
’s
NS
/ NS
/ wri
st /
NS
/ NS
/E
EPR
OM
A
CT
: IS
(int
erda
ily s
tabi
lity)
,IV
(int
rada
ily v
aria
bilit
y)
NS
/ NS
/ NS
Rhy
thm
dis
turb
ance
in m
ost
Alz
heim
er’s
Dis
ease
pts
, no
sund
owni
ng, r
hyth
ms
in N
Hle
ss s
tabl
e th
an h
ome
part
icu-
larl
y in
IS
Ver
coul
en (
221)
5D-b
RC
T; D
B; p
aral
lel d
esig
n /
NS
/ Ent
ire
24-h
s; 1
2D A
CT
NS
(96)
/ G
rp1
38.5
±10
.1,
Grp
2 39
.9±
8.6,
Grp
337
.8±
11.9
, Grp
4 39
.8±
7.4
/C
hron
ic f
atig
ue s
yndr
ome;
depr
essi
on
NS
/ Act
omet
er /
ankl
e / N
S /
NS
/ NS
log;
AC
T: m
ean
activ
ity;
Moo
d: B
eck,
SIP
(SIP
-sic
k-ne
ss im
pact
pro
file
)
Exc
lusi
on: O
ther
psy
ch d
isor
-de
rs
No
diff
eren
ce in
any
out
com
em
easu
res
betw
een
the
4 G
rps
Wal
lace
-Guy
(22
2)
4C-b
Unb
lend
ed, n
onra
ndom
ized
,ob
serv
atio
nal s
tudy
/ ho
me
/en
tire
24 h
7D
AC
T
NS
(154
) F
, 154
/ 66
.7 (
51-
81)
/ nor
mal
, pos
tmen
opau
sal
wom
en
Non
e / A
ctill
ume
(AM
I) /
wri
st /
1 m
in /1
0 se
c / N
S /
NS
AC
T: l
ux, i
n-be
d sl
eep,
out
of
bed
slee
p, S
E, S
L, w
ake
with
-in
sle
ep, T
ST, s
leep
tim
ing,
amou
nt o
f da
ytim
e na
ppin
g;M
ood:
dep
ress
ion
brie
fsc
reen
ing
ques
tionn
aire
Incl
usio
n: p
artic
ipan
ts in
wom
ens’
heal
th in
itiat
ive
obse
rvat
iona
l stu
dy /
Exc
lusi
on/ p
hysi
cally
una
ble
to p
artic
ipat
e or
not
like
ly t
osu
rviv
e fe
w m
onth
s / N
S
Gre
ater
24-
h ill
umin
atio
n co
r-re
late
d w
ith s
hort
er S
L,
redu
ced
wak
e w
ithin
sle
ep,
and
grea
ter
depr
esse
d m
ood.
Eve
ning
ligh
t exp
osur
e w
asno
t ass
ocia
ted
with
thes
e va
ri-
able
s.
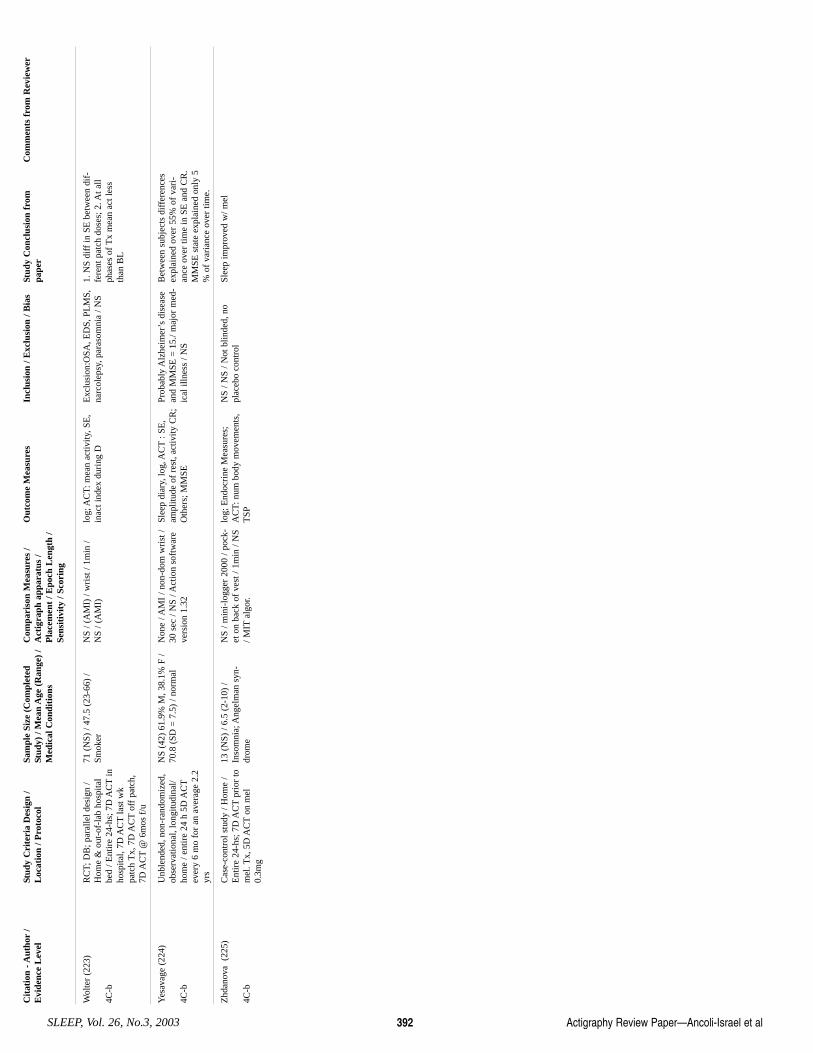
Cit
atio
n - A
utho
r/
Evi
denc
e L
evel
St
udy
Cri
teri
a D
esig
n /
Loc
atio
n / P
roto
col
Sam
ple
Size
(C
ompl
eted
Stud
y) /
Mea
n A
ge (
Ran
ge)
/M
edic
al C
ondi
tion
s
Com
pari
son
Mea
sure
s /
Act
igra
ph a
ppar
atus
/P
lace
men
t / E
poch
Len
gth
/Se
nsit
ivit
y / S
cori
ng
Out
com
e M
easu
res
Incl
usio
n / E
xclu
sion
/ B
ias
Stud
y C
oncl
usio
n fr
ompa
per
Com
men
ts f
rom
Rev
iew
er
Actigraphy Review Paper—Ancoli-Israel et alSLEEP, Vol. 26, No.3, 2003 392
Wol
ter
(223
)
4C-b
RC
T; D
B; p
aral
lel d
esig
n /
Hom
e &
out
-of-
lab
hosp
ital
bed
/ Ent
ire
24-h
s; 7
D A
CT
inho
spita
l, 7D
AC
Tla
st w
kpa
tch
Tx,
7D
AC
Tof
f pa
tch,
7D A
CT
@ 6
mos
f/u
71 (
NS)
/ 47
.5 (
23-6
6) /
Smok
er
NS
/ (A
MI)
/ w
rist
/ 1m
in /
NS
/ (A
MI)
lo
g; A
CT
: mea
n ac
tivity
, SE
,in
act i
ndex
dur
ing
D
Exc
lusi
on:O
SA, E
DS,
PL
MS,
narc
olep
sy, p
aras
omni
a / N
S 1.
NS
diff
in S
E b
etw
een
dif-
fere
nt p
atch
dos
es; 2
. At a
llph
ases
of
Tx
mea
n ac
t les
sth
an B
L
Yes
avag
e (2
24)
4C-b
Unb
lend
ed, n
on-r
ando
miz
ed,
obse
rvat
iona
l, lo
ngitu
dina
l/ho
me
/ ent
ire
24 h
5D
AC
Tev
ery
6 m
o fo
r an
ave
rage
2.2
yrs
NS
(42)
61.
9% M
, 38.
1% F
/70
.8 (
SD =
7.5
) / n
orm
al
Non
e / A
MI
/ non
-dom
wri
st /
30 s
ec /
NS
/ Act
ion
soft
war
eve
rsio
n 1.
32
Slee
p di
ary,
log,
AC
T: S
E,
ampl
itude
of
rest
, act
ivity
CR
;O
ther
s; M
MSE
Prob
ably
Alz
heim
er’s
dis
ease
and
MM
SE =
15.
/ maj
or m
ed-
ical
illn
ess
/ NS
Bet
wee
n su
bjec
ts d
iffe
renc
esex
plai
ned
over
55%
of
vari
-an
ce o
ver
time
in S
E a
nd C
R.
MM
SE s
tate
exp
lain
ed o
nly
5%
of
vari
ance
ove
r tim
e.
Zhd
anov
a (
225)
4C-b
Cas
e-co
ntro
l stu
dy /
Hom
e /
Ent
ire
24-h
s; 7
D A
CT
prio
r to
mel
. Tx,
5D
AC
Ton
mel
0.3m
g
13 (
NS)
/ 6.
5 (2
-10)
/In
som
nia;
Ang
elm
an s
yn-
drom
e
NS
/ min
i-lo
gger
200
0 / p
ock-
et o
n ba
ck o
f ve
st /
1min
/ N
S/ M
ITal
gor.
log;
End
ocri
ne M
easu
res;
AC
T: n
um b
ody
mov
emen
ts,
TSP
NS
/ NS
/ Not
blin
ded,
no
plac
ebo
cont
rol
Slee
p im
prov
ed w
/ mel