Embed Size (px)
Citation preview
CentralBringing Excellence in Open Access
JSM Brain Science
Cite this article: Sharma RR, Sharma A (2017) Cranio-Cerebral Abscesses in Nocardiosis and Actinomycosis: Assessment and Management Strategies. JSM Brain Sci 2(2): 1013.
*Corresponding authorRR Sharma, Senior Consultant Neurosurgeon, PO Box-397, PC-118, Al Harthy Complex, Qurum, Muscat, Oman, Tel: 00 968 24567339/24811688; 00 968 99241189; Email:
Submitted: 11 July 2017
Accepted: 05 August 2017
Published: 06 August 2017Copyright© 2017 Sharma et al.ISSN: 2573-1289
OPEN ACCESS
Keywords•Nocardiosis; Actinomycosis; Cerebral; Abscess;
Granulomas; Management strategies; Morbidities; Mortality; Prognosis
Review Article
Cranio-Cerebral Abscesses in Nocardiosis and Actinomycosis: Assessment and Management StrategiesRewati Raman Sharma1* and Apollina Sharma2
1Department of Neurosurgery, Atlas Hospitals, Oman2Graduate Student International Masters of Health Leadership, McGill University, Canada
Abstract
The CNS infections, such as nocardiosis and actinomycosis, are extremely rare conditions secondary to the primary focus elsewhere i.e., commonly in the lungs, skin, oro-dental areas, paranasal sinuses, and cervico-facial regions; less commonly abdomen and rarely, the pelvic region. These CNS infections are usually sub-acute or chronic disease processes and only occasionally, an acute presentation does occur mainly in nocardiosis. Brain abscesses in nocardiosis and actinomycosis are usually due to chronically continued inflammation and gradual collection of the infected material with and without granulomatous component. Acute and sub-acute clinical presentations usually occur in cerebral abscesses and the chronic clinical features are seen more in granulomas. Interestingly, in many patients, both abscesses and granulomas coexist. The CNS infections can be insidious in onset, slowly progressive and without usual features of systemic infection. The late clinical presentation may be with headaches, behavioral changes, focal neurological deficits, raised intracranial pressure (progressive headaches, episodic transient loss of vision (visual obscuration), neck stiffness, and vomiting) and fever.
The brain imaging (Computerized Tomography of the head (CT head) and Magnetic resonance imaging (MRI)) is carried out to evaluate the extent of the CNS involvement with cerebral mass lesions, such as cerebral abscesses and granulomas or other parenchymal features of the raised intracranial pressure. The hematological, biochemical and microbiological studies help in further defining the etiology, local/general spreads and the secondary effects. Fortunately, these infections show good response to the appropriate antibiotics such as co-trimoxazole which is the drug of choice (DOC) for nocardiosis and penicillin-G (DOC) for actinomycosis with excellent results as the cure is achievable in some patients.
Therefore, the overall management includes the control of CNS infection, elimination of the primary focus, and containment of dissemination. Mainly the anti-microbial drugs, analgesics, anti-emetics and the surgical interventions are used wherever indicated. Surgical management consists of image guided aspirations of cerebral abscesses and excision of granulomas as well as debridement of the involved tissues.
Unfortunately, despite much advancement in the modern diagnostics and therapeutics, there is still appreciable morbidity. These patients need long periods of treatment and the mortality of 20-30% is still high.
In future, we need to focus on the preventive measures (public educational activities, immune-prophylaxis and chemo-prophylaxis), as well as on the modern diagnostics and appropriate treatment strategies to achieve optimum results.
INTRODUCTIONActinomycetes, distributed worldwide, are Gram positive
bacilli in branching filaments which are essentially consisting of vegetative bacterial cells contiguously arranged in long chains and therefore, superficially resembling the appearance of fungi [1-3]. The common ones belong to species of Nocardia (aerobic) and Actinomyces (anaerobic). Nocardia bacillus is a weak acid fast organism present in the soil, decaying vegetation, and stagnant water [2,3]. Actinomyces bacillus is also present in the soil and found as normal flora in the mouth and intestine. Both, opportunistic bacteria usually causing infections in immune compromised individuals. Nocardia bacillus primarily causes pulmonary, and less commonly, the cutaneous and paranasal sinus infections; whereas, Actinomyces commonly results in oro-dental, cervico-facial, cranio-facial and intestinal abscesses
with cutaneous sinus tracts draining sulfur granules. These opportunistic infections, although in rare instances, secondarily cause solitary or multiple brain abscesses and granulomas in immune compromised patients but rarely, cause infections in the immune competent individuals.
CLASSIFICATION [3-5]Edmond I E Nocard (French veterinarian (1850-1903) in
1888) discovered aerobic acid fast Actinomycetes in cattle which were named by Trevisan as Nocardia farcinica. Soon afterwards Eppinger in 1891, had described primary pulmonary nocardiosis and secondary/ metastatic cerebral abscess in a glass blower.
Among the Gram positive group of bacteria, Actinobacteria are classified into three groups: Actinomycineae, Corynebacterineae and Bifido-bacteriaceae. Actinomycineae is further subclassified

CentralBringing Excellence in Open Access
Sharma et al. (2017)Email:
JSM Brain Sci 2(2): 1013 (2017) 2/10
into Actinomycetaceae and Propioni-bacteriaceae: Actinomyces belongs to the former and Propionibacterium acnes to the latter. Corynebacterineae is also further subdivided into Mycobacteriaceae (Tuberculous bacilli, Lepra bacilli), Nocardiaceae (N. asteroides, N. farcinica, N. brasilliences) and Corynebacteriaceae (Corynebacterium diphtheria). Majority of these organisms are basically opportunistic bacteria.
In broad terms, the clinically important Gram positive bacilli can also be classified into three broad groups:
1. Spore forming bacilli: Clostridium bacilli
2. Non-spore forming bacilli: Corynebacterium, Listeria, Lactobacillus
3. Branching filamentous bacilli: Actinomyces, Nocardia
BRAIN ABSCESSES DUE TO ACTINOBACTERIA [3-6]
There are many Gram positive bacteria belonging to Actinobacteria; however, amongst them, the organisms most commonly causing the CNS infections are Nocardia and Actinomyces. There are many similarities and differences in the clinical characteristics of nocardiosis and actinomycosis which are important to be realized for their proper assessment, diagnosis and management.
THE CNS NOCARDIOSIS: BRAIN ABSCESS [3-7]
Introduction
Nocardiosis, although a rare infection caused by Actinomycetes species of Nocardia, is ubiquitous with worldwide distribution. As stated earlier, Nocardia bacillus is a common habitant in the soil, decaying vegetation and stagnant water. They are important environmental saprophytes with excellent growth potentials over a wide range of temperature. Nocardia species are strictly aerobic Actinomycetes, a large diverse group of bacteria that appear on microscopy as branching filamentous cells mimicking fungi. Nocardia therefore appears as a thin, less than 1µm thick gram positive branching filament. It is focally acid fast when decolorized with 1% of sulphuric acid.
Types of nocardia species
The common human pathogenic Nocardia species are N. asteroides, N. farcinica, N. nova, N. brasiliensis, N. pseudo-brasiliensis, N. otitidiscaviarum and N. transvalensis. N. asteroidis and, closely resembling, N. farcinica cause most human infections (80-90 %) but N. brasiliensis is a common pathogen in Central and South America. In USA alone, yearly about 900-1100 cases are reported. Among all varieties of Nocardia species, Nocardia farcinica appears to be more virulent [5-8]
The transmission, dissemination and co-morbid etiological factors [7-8]
The transmission of Nocardia bacilli is usually airborne, or caused by direct contact, vectors, trauma, and endo-vascular interventional procedures. Therefore, the primary infection is usually pulmonary (Figure 1) or cutaneous and if it occurs following trauma then it is a chronic granulomatous disease of
the bone at the site of the trauma. Hematogenous or contiguous spread of infection to the CNS occurs from the lungs, skin, para-nasal sinuses and oral cavity. It is more common in immune compromised hosts (diabetes mellitus, steroid therapy, leukemia, lymphoma, cytotoxic drugs, immune suppression, pulmonary alveolar proteinosis, sarcoidosis, ulcerative colitis, intestinal lypodystrophy, collagen diseases, etc.) but only 15-30% cases occur in immune-competent individuals. Nocardia species is, therefore, considered primarily as opportunistic pathogens.
Clinical symptomatology [7-10]
Nocardiosis affects men (60-70%) more than women (30-40%) in their middle ages (fourth through sixth decades of life). It occurs in three primary clinical syndromes in order of frequency: pulmonary (70-75% cases), cutaneous (20-25%), and subcutaneous such as mycetoma of the foot and paranasal sinuses (5-10%). Nocardia species has special affinity for the neural tissues. About 25-40 % cases of systemic nocardiosis develop CNS infections and about 10-15% cases have the renal problems. Interestingly, within the cerebro-spinal parenchyma, nocardial infection occurs insidiously without any symptom initially and then spreads slowly with development of the progressive symptoms giving an impression of an evolving mass lesion such as a brain or spinal tumor. There are many forms of secondary CNS nocardial lesions: single abscess, multiple brain abscesses, diffuse cerebritis, and meningitis, granulomas mimicking neoplasms, vasculitis, and strokes. Meningitis is a less common presentation of nocardiosis as compared to the brain abscesses and granulomas. The clinical presentation of CNS nocardiosis is therefore commonly due to the local mass effects of an abscess and a granuloma. The spinal cord involvement is the least common among all clinical CNS presentations.
In substantial number of cases, the common clinical features of bacterial inflammation, such as fever, rigors, sweating, headaches, toxic look, vomits, neck stiffness, etc may be missing in initial presentations of the CNS nocardiosis. Therefore, in the initial clinical stages, the diagnosis and the treatment of nocardiosis become very difficult and its spread in CNS becomes unchecked to a stage when sudden catastrophe might happen.
The usual clinical presentation of CNS nocardiosis [11-14]
It is a solitary brain abscess in immune compromised patients but in N. farcinica, multiple brain abscesses may develop due to
Figure 1 Nocardial Pulmonary abscess in the left upper lobe.
CentralBringing Excellence in Open Access
Sharma et al. (2017)Email:
JSM Brain Sci 2(2): 1013 (2017) 3/10
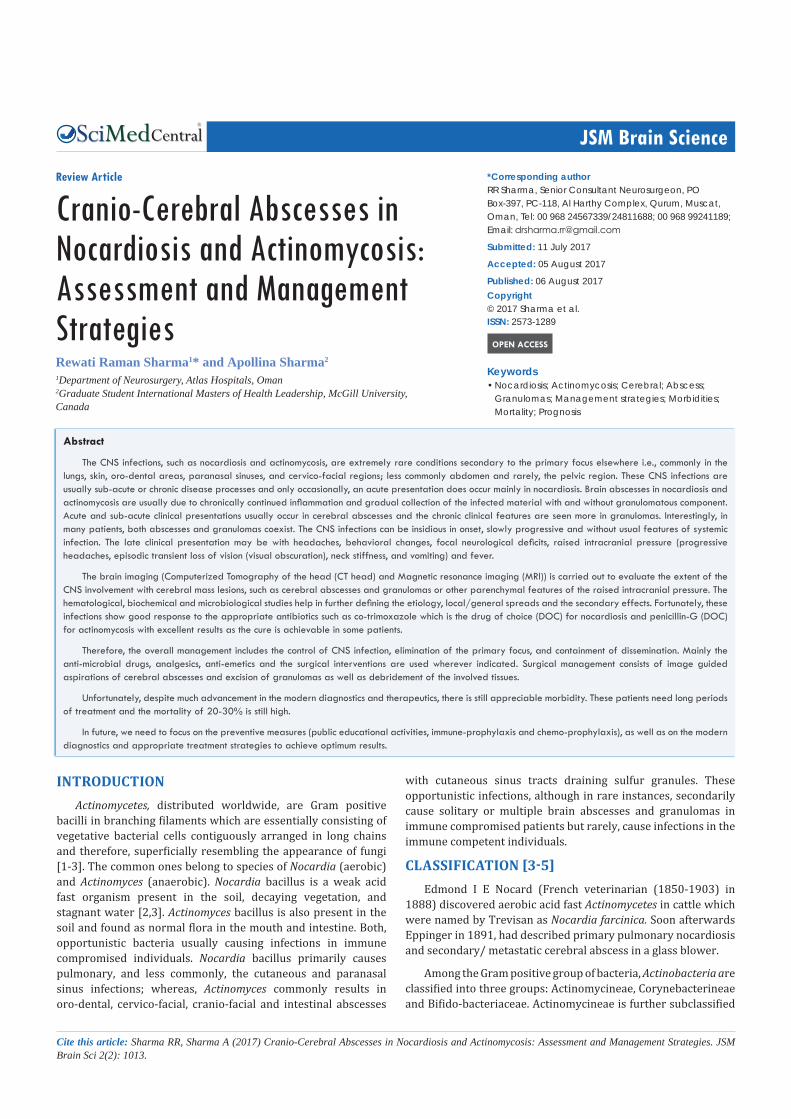
its more virulent nature and higher chances of resistance to the antibiotics (Figure 2). Nocardia species accounts for only 1-2% of all the cases of brain abscesses. Nocardiosis usually progresses over months to years with focal neurological deficits. Frontal and or temporal nocardiosis present with personality changes, behavioral disorders and gross psychiatric manifestations. Some cases of large nocardial cerebral abscesses or granulomas have a rapidly progressive clinical course with focal neurological deficits such as occurring in the fungal vasculopathy and strokes [15] depending upon the location of the brain lesions. Suddenly, the raised intracranial pressure may develop which may cause rupture of the nocardial brain abscess into the subarachnoid spaces or ventricles consequently developing purulent meningitis or ventriculitis with their typical clinical features.
Neuropathology and microbiology [1-3,6]
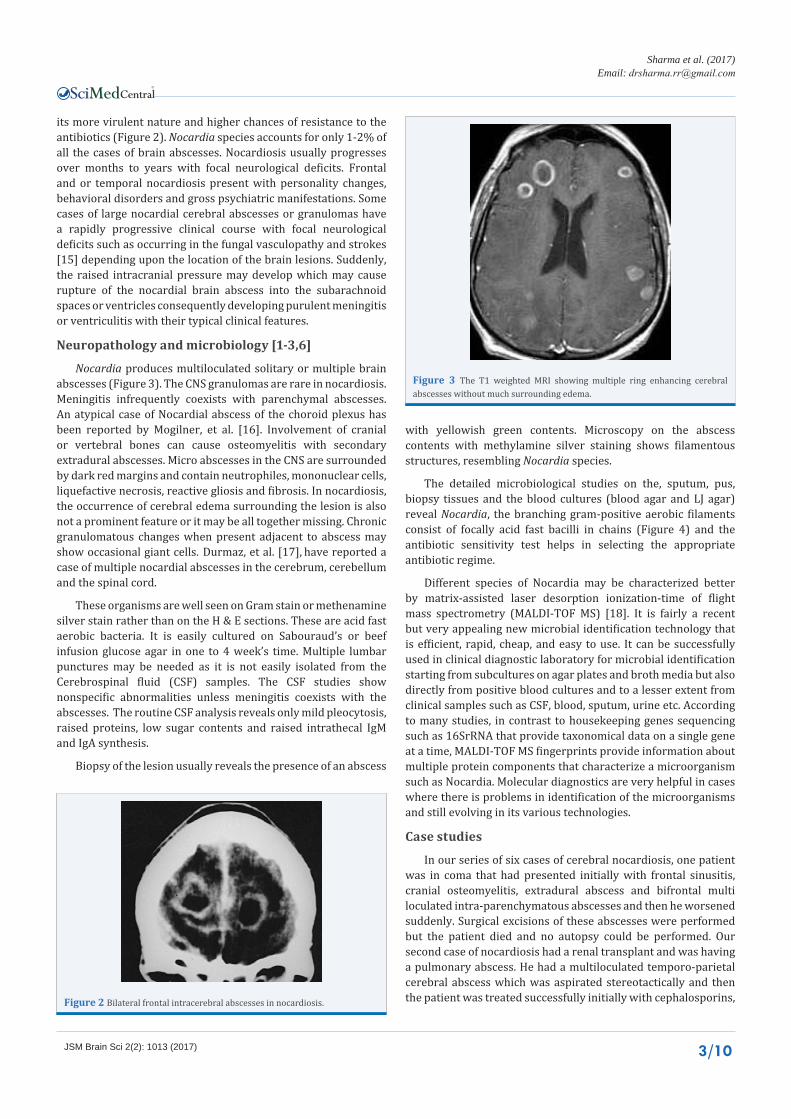
Nocardia produces multiloculated solitary or multiple brain abscesses (Figure 3). The CNS granulomas are rare in nocardiosis. Meningitis infrequently coexists with parenchymal abscesses. An atypical case of Nocardial abscess of the choroid plexus has been reported by Mogilner, et al. [16]. Involvement of cranial or vertebral bones can cause osteomyelitis with secondary extradural abscesses. Micro abscesses in the CNS are surrounded by dark red margins and contain neutrophiles, mononuclear cells, liquefactive necrosis, reactive gliosis and fibrosis. In nocardiosis, the occurrence of cerebral edema surrounding the lesion is also not a prominent feature or it may be all together missing. Chronic granulomatous changes when present adjacent to abscess may show occasional giant cells. Durmaz, et al. [17], have reported a case of multiple nocardial abscesses in the cerebrum, cerebellum and the spinal cord.
These organisms are well seen on Gram stain or methenamine silver stain rather than on the H & E sections. These are acid fast aerobic bacteria. It is easily cultured on Sabouraud’s or beef infusion glucose agar in one to 4 week’s time. Multiple lumbar punctures may be needed as it is not easily isolated from the Cerebrospinal fluid (CSF) samples. The CSF studies show nonspecific abnormalities unless meningitis coexists with the abscesses. The routine CSF analysis reveals only mild pleocytosis, raised proteins, low sugar contents and raised intrathecal IgM and IgA synthesis.
Biopsy of the lesion usually reveals the presence of an abscess
with yellowish green contents. Microscopy on the abscess contents with methylamine silver staining shows filamentous structures, resembling Nocardia species.
The detailed microbiological studies on the, sputum, pus, biopsy tissues and the blood cultures (blood agar and LJ agar) reveal Nocardia, the branching gram-positive aerobic filaments consist of focally acid fast bacilli in chains (Figure 4) and the antibiotic sensitivity test helps in selecting the appropriate antibiotic regime.
Different species of Nocardia may be characterized better by matrix-assisted laser desorption ionization-time of flight mass spectrometry (MALDI-TOF MS) [18]. It is fairly a recent but very appealing new microbial identification technology that is efficient, rapid, cheap, and easy to use. It can be successfully used in clinical diagnostic laboratory for microbial identification starting from subcultures on agar plates and broth media but also directly from positive blood cultures and to a lesser extent from clinical samples such as CSF, blood, sputum, urine etc. According to many studies, in contrast to housekeeping genes sequencing such as 16SrRNA that provide taxonomical data on a single gene at a time, MALDI-TOF MS fingerprints provide information about multiple protein components that characterize a microorganism such as Nocardia. Molecular diagnostics are very helpful in cases where there is problems in identification of the microorganisms and still evolving in its various technologies.
Case studies
In our series of six cases of cerebral nocardiosis, one patient was in coma that had presented initially with frontal sinusitis, cranial osteomyelitis, extradural abscess and bifrontal multi loculated intra-parenchymatous abscesses and then he worsened suddenly. Surgical excisions of these abscesses were performed but the patient died and no autopsy could be performed. Our second case of nocardiosis had a renal transplant and was having a pulmonary abscess. He had a multiloculated temporo-parietal cerebral abscess which was aspirated stereotactically and then the patient was treated successfully initially with cephalosporins, Figure 2 Bilateral frontal intracerebral abscesses in nocardiosis.
Figure 3 The T1 weighted MRI showing multiple ring enhancing cerebral abscesses without much surrounding edema.

CentralBringing Excellence in Open Access
Sharma et al. (2017)Email:
JSM Brain Sci 2(2): 1013 (2017) 4/10
and then cotrimoxazole (960/480 mg QID daily) on long term drug therapy. The third case of pulmonary nocardiosis had right fronto-temporal brain abscess which was micro-surgically excised. It was then diagnosed as nocardiosis and treated with co-trimoxazole on long term basis with good results. Two other cases of brain abscesses had initially fronto-ethmoidal sinusitis which was treated with antibiotics prior to the diagnosis and then antifungal medications. Later these patients have developed frontal brain abscesses, which were aspirated stereo-tactically and the diagnosis of nocardiosis was established. Aggressive management of the nocardial sinusitis as well as cerebral abscesses had resulted in a excellent results in these cases. One case of nocardiosis has typically presented with meningitis/ventriculitis which later progressed to hydrocephalus. He initially needed CSF diversion procedure in the form of external ventricular drain and then the right ventriculo-peritoneal shunt was carried out. He did clinically very well.
Spinal cord compression
This is following vertebral osteomyelitis and intramedullary spinal abscess may rarely occur in nocardiosis [19-21]. Spinal nocardiosis occurs commonly in cervical and thoracic regions. It usually develops by hematogenous spread from a pulmonary focus and presents as localized pain, radiculopathy and or myelopathy. Intramedullary spinal cord abscess has been described although very rarely. Vertebral bodies are commonly involved and para-spinal abscesses may be present [19-21].
Diagnosis [3,6,7-10]
The brain MRI usually shows single or multiple cerebral ring enhancing lesions (T1 weighted with gadolinium infusion) with partial diffusion restriction. In case of brain abscess with multiple loculi, a wide confluent heterogeneous hyper intensity lesion is noted on FLAIR (fluid-attenuated inversion recovery) images. The cerebral edema surrounding the lesions is minimal or may be absent. Mild dural thickening (Dural tail sign) and enhancement are present. In cases of intraventricular rupture of nocardia brain abscess, the MR fluid attenuation inversion recovery (FLAIR) imaging may reveal a clear hyperintense component in the ventricle and a nevous formation inside the intracerebral lesion
indicating the state of intraventricular rupture of the nocardial brain abscess [22].
The CT scans show ring enhancing intraparenchymal lesions in cases of nocardial cerebral abscesses. It demonstrates mainly hypo-attenuation lesions with contrast-enhancing peripheral rims and very little surrounding edema. Indium-111 labeled leukocytes scanning may differentiate abscesses from the cerebral neoplasms.
The diagnosis predominantly depends on the detailed microbiological and histopathological studies on the specimens of pus and the tissues obtained from the cerebral lesions usually at the craniotomy or stereotactic/ image guided burr-hole aspirates and biopsies, as detailed earlier.
Treatment [3-6,8-10,17,22,23]
Successful treatment of the nocardial cerebral abscesses or granulomas is achieved by the combination of most effective anti-nocardial medications and timely guided stereotactic or open surgical procedures such as the drainage of the abscess. Extensive excisional debridement of the infected cranio-cerebral or spinal abscesses or granulomatous tissues via craniotomy or laminectomy should be performed wherever possible.
Among the medications, Sulfonamides are the drug of choice (DOC). Recommended primary treatment is with intravenous trimethoprim with sulfamethoxazole, 4-8 grams per day in divided doses for 3-4 months and then the oral preparations for a period of 8-10 months. In patients having allergy to the sulfonamides, many alternative antibiotics are there such as ceftriaxone, imipenem, amikacin, linezolid, clindomycin, minocycline, amoxicillin, and erythromycin, which should be used depending upon the results of the antibiotic sensitivity tests. The third generation cephalosporins and intravenous imipenem (1 gm four times a day) are used with good improvement of neurological conditions in substantial number of cases. In contrast to actinomycosis, the nocardiosis tends to be penicillin resistant.
The follow up treatment with prevention of recurrences are taken care with co-trimoxazole therapy (960/480mg QID daily) for 6-12 months. Even with 4-8 weeks of active management, many comatose patients or the patients with severe neurological deficits show recovery in their neurological symptomatology including in their level of consciousness, disturbed mental faculties, speech disturbances, diplopia, facial weakness, dysmetria and imbalance. Many patients show a substantial regression of cerebral lesions on follow up MRI brain scans.
The progress is best monitored by interval CT/MR scanning in appropriate settings and the periodic assessments of general clinical state of the patient. Although most cases of spinal nocardiosis can be managed with medical therapy, the surgical decompressive procedures may be required in patients with spinal cord and or nerve root compression. Syringomyelia may occur as a delayed complication of the treatment for nocardial spinal abscess [23]. Neuro-nocardiosis is still associated with significant morbidity and mortality rates although the results are better than before. The cure rate in cases of nocardial brain abscess is about 50-70%.
Figure 4 Nocardia Acid Fast Gram Stain.

CentralBringing Excellence in Open Access
Sharma et al. (2017)Email:
JSM Brain Sci 2(2): 1013 (2017) 5/10
Prognosis [1-4,14,17,24]
Mortality with nocardial brain abscess diagnosed ante-mortem is about 20-30% in immune competent patients but increases to 40% in cases of multiple abscesses and about 55% in immune-compromised patients. Mortality in disseminated nocardiosis with severely compromised immune status may approach 60-80%. An appropriate antibiotic therapy and a timely neurosurgical procedure for the abscesses and granulomas (aspiration/excision) form the basis of the essential treatment in the majority of nocardiosis patients.
THE CNS ACTINOMYCOSIS: BRAIN ABSCESS [1-6,25,26]
Introduction
Actinomyces are one of the common bacteria habitant in soil, oral cavity, and colon producing Actinomycosis which is worldwide in distribution. Actinomycosis is a rare infection in humans and is commonly seen clinically as cervico-facial “lumpy jaw” and less commonly, as thoraco-abdominal or pelvic actinomycosis. The males in between the third decade to the sixth decade of their life are affected more than the females in the ratio of 70% to 30 %. This rare infection occurs in the frequency of one case in 250,000 to 400,000 people especially with poor dental hygiene and low socioeconomic communities worldwide without any racial discrimination. Widespread use of antibiotics dramatically improved the prognosis with excellent results nowadays.
The CNS actinomycosis is a rare disease most frequently forming cerebral abscesses and infrequently granulomatous lesions [25-27]. Actinomycosis is characterized by mixed suppurative and granulomatous inflammatory reactions, connective-tissue proliferation, and the presence of pathognomonic sulfur granules. Similar types of granules have been reported in infections due to the organisms such as Nocardia brasiliensis, Streptomyces madurae, and Staphylococcus aureus (botryomycosis). The granules are yellowish particles approximately 0.1-1mm in diameter. Interestingly, many bioactive metabolites of the Actinobacteria (Streptomyces spp.) are used in medicine such as aminoglycosides, chloramphenicol, tetracyclines, macrolide, anthracyclines, etc.
Types of actinomyces [1-3,6,25-28]
Initially, Otto Bollinger had discovered Actinomyces bovis in cattle in 1877, and shortly afterwards James Israel did A. israeli in humans. In 1890, Eugen Bostroem isolated Actinomyces from a culture of grains and soil.
The Actinobacteria in the phylum of Gram positive bacteria belongs to Actinomycineae [29] - family Actinomycetaceae, order Actinomycetales, subclass Actinobacteridae and Streptomyces species, genus Actinomycetes with nearly 25 Actinomyces or “Actinomyces like organisms” identified. Commonly Actinomyces israeli and less commonly Actinomyces bovis are isolated but other important species are Actinomyces gerencseriae, Actinomyces turicensis, Actinomyces radingae, and Actinomyces europaeus. These non-acid fast, non-spore forming, and anaerobic-to-microaerophilic filamentous bacteria are forming colonies with
typical appearance of the “molar teeth”. These bacilli significantly help in biological buffering of the soils and the large water reservoirs by decomposing the organic material to form micro-molecules which are easily taken up by the growing plants. The commonly isolated companion bacteria which magnify the low pathogenic potential of Actinomycetes are Actinobacillus, Actinomycetemcomitans, Peptostreptococcus, Fusobacteruium, Bacteroides, Staphylococcus and Streptococcus.
The transmission, dissemination and co-morbid etiological factors [3,6,29]
Actinomycosis is an indolent, slowly progressive, chronic infection caused by anaerobic or microaerophilic bacteria (Actinomyces israeli and Actinomyces bovis) belonging to genus Actinomyces. Actinomyces israeli is a normal inhabitant of the mouth, colon and vagina and is not found free in nature. It requires devitalized tissue to provide an anaerobic environment for growth. The portal of entry is the damaged mucosal lining. Actinomycosis is basically a chronic suppurative and granulomatous infection characterized by the multi-lobulated or loculated abscesses containing the sulphur granules. The sulphur granules consist of thin (less than 1µm) branching Gram positive actinomycetic filaments in matted tangles which are essentially made up of linearly arranged contiguous Actinomyces bacilli.
The disease has three primary forms: Cervicofacial (mandible), thoraco-abdominal (pulmonary and ileocaecal region) and pelvic. The CNS involvement occurs in 2-5% of all cases by direct tissue invasion or hematogenous dissemination. The organGram Positive Actinomyces israeli contiguous structures without difficulty.
Pathophysiology [1-6,24,25,29]
Actinomyces are normal flora of the oral cavity and seen less frequently in the lower gastrointestinal tract and female genital tract. These are opportunistic microorganisms always co-exist with companion bacteria (co-pathogens) which enhances invasiveness of actinomycosis. These companion bacteria cause a break in the integrity of the mucous membranes and result in devitalized tissues for the invasion of the deeper tissues by the Actinomyces and result in abscesses and granuloma formations. Once infection is established, the host mounts an intense inflammatory response (suppurative, and granulomatous), and in long run, the fibrosis usually follows. Infection typically spreads contiguously, frequently ignoring tissue plane barriers and invading surrounding tissues or the organs in continuity. Ultimately, the infection produces draining sinus tracts. Hematogenous dissemination to distant organs may occur at any stage of actinomycosis, whereas lymphatic dissemination is very unusual.
Cervicofacial actinomycosis is the most common type of the infection, comprising 50-70% of reported cases. This infection typically occurs following oral surgery or in patients with poor dental hygiene. It is characterized in the initial stages by the soft-tissue swelling of the peri-mandibular or parotid area. Direct spread into the adjacent tissues occurs over time, along with development of fistulas (sinus tracts) that discharge purulent material containing granules with yellow sulfur like appearance

CentralBringing Excellence in Open Access
Sharma et al. (2017)Email:
JSM Brain Sci 2(2): 1013 (2017) 6/10
(termed sulfur granules). Invasion of the cranium or the bloodstream may occur if the disease is left untreated.
The risk factors are oro-dental pathology, paranasal sinusitis, thoraco-abdominal abscesses, intrauterine device, alcohol abuse and Rendu-Osler-Weber disease [3,6].
Neuropathology [1-6,25-27,30,31]
As the organisms, Actinomyces, colonize areas of mucous membrane in the body, any breach in the continuity of this membrane (usually caused by the companion bacteria) may lead to invasive actinomycotic infection. Following tissue invasion, Actinomycetes bacilli form tiny visible clumps called grains or sulfur granules. The Actinomycotic lesions are purulent foci surrounded by dense fibroses. Therefore, clinico-pathologically, actinomycosis is characterized by the draining sinuses, extensive fibrosis, pus filled micro-abscesses containing multilobulated sulphur granules. Actinomycosis progresses contiguously across the tissue boundaries, with multiple discharging sinus tracts (resolving and recurring) and is a refractory or a relapsing infection with short term antibiotic treatment.
The most common form of the CNS actinomycosis is the intracerebral abscess [3,6,25-27,30,31]. The abscess is typically a single thick walled multilobulated lesion. In cervicofacial actinomycosis, the meninges are invaded causing epidural and subdural empyemas associated with cranial osteomyelitis. Involvement of the spine in pulmonary actinomycosis occurs as a result of contiguous spread of infection with the production of osteomyelitis and epidural abscess [32]. Microscopically, actinomycotic abscesses have central liquefactive necrosis, neutrophils, mononuclear cells, granulation tissue, fibrosis and bacterial filaments. Lymphocytes, plasma cells and monocytes are present in the abscesses with multinucleated giant cells. Granulomas are seen in patients with long standing infection [1-3,6,27].
In the needle aspirates and the surgical biopsies, one should look for the sulfur granules for a definitive diagnosis. The cultures are placed immediately under anaerobic conditions and incubated at least for 48 hours or more. The sulfur granules are crushed between 2 slides, stained with 1% methylene-blue solution, and examined microscopically for the features characteristic of Actinomyces. At low magnification, the colonies of the sulfur granules look like molar teeth or cauliflower shape and at high magnification (X100), like clumps of filamentous actinomycete micro-colonies surrounded by neutrophils and co-existing companion bacteria.
Gram stain shows actinomycotic micro-colonies as Gram-positive, long beaded, and intertwined branching filamentous rods, with radially arranged, peripheral hyphae. On H & E sections, the basophilic filaments are terminating in eosinophilic clubs. The CSF studies tend to be normal or nonspecific. PCR (polymerase chain reaction) and Nucleic acid probes are being developed for more accurate and rapid diagnosis. The serological tests have no role in the diagnosis. At times, there are difficulties to identify bacteria in the routine practice. New modern technological advances made it possible to more accurately identify the micro-organisms such as Actinomyces i.e., molecular technologies, MALDI-TOF-MS studies, and 16S rRNA gene sequencing. For
some microorganisms, insufficient cell lysis and/or low quantity of sample material can be problematic for efficient MALDI-TOF identification and require the use of alternative identification approaches such as 16S rRNA gene sequencing. A study by Bizzini et al. [33], focusing on the identification of 410 clinical isolates that could not be identified with conventional laboratory methods showed that 133/410 (32.4%) isolates could not be either reliably identified with MALDI-TOF. The failure to obtain a reliable identification was due to the absence of reference spectra in the BioTyper database for 58% (78/133) of the isolates and to poor protein spectral signals for 41.4% (55/133) of the isolates. The authors supposed that the poor spectrum quality observed could be due to either the difficulty to lyse the cell wall of some bacteria such as Gram-positive bacilli and/or to fastidious growth of some isolate, which yielded only small amount of available sample material. Difficult to identify microorganisms belonging to the genera Actinomyces, Nocardia, and Streptomyces could be observed in this study.
Clinical symptoms
As stated earlier, clinically actinomycosis presents in various forms: cervico-facial (Lumpy jaw: poor dental hygiene, oral neoplasm, radio-osteo-necrosis), [34,35] thoracic (aspirations, poor dental hygiene), [36-38] abdominal (perforated appendix, mesenteric ischemic necrosis, foreign bodies) [38,39] and pelvic (intra-uterine contraceptive devices) [40]. Lumpy jaw ( non-tender and woody hard), usually, occurs as a painless reddish-bluish perimandibular swelling with multiple sinus tracks draining pus with h/o remittance and recurrence with progressively increasing difficulty in mastication and intermittent trismus (Figure 5). The exudates show sulfur granules made up of the Actinomyces bacilli. Thoracic actinomycotic abscess presents with chest pains, cough, and blood tinged expectoration, difficulty in breathing and constitutional symptoms (fever, anorexia, lethargy, fatigue, nausea, vomits, loss of body weight, etc.). Abdominal actinomycosis mainly present with constitutional symptoms but occasionally a feeling of a mass lesion in the abdomen as well. Pelvic and perineal pains with vaginal bleeding or discharge occur in pelvic actinomycosis.
Figure 5 Cervico-facial actinomycosis-healed sinus tract in front of the tragus in the mandibulo-parotid region.

CentralBringing Excellence in Open Access
Sharma et al. (2017)Email:
JSM Brain Sci 2(2): 1013 (2017) 7/10
Although no age is immune, actinomycosis commonly occurs in middle ages with male preponderance. Usually, the CNS actinomycosis develops through direct continuity of oro-cervico-facial disease and infrequently via hematogenous spread from lungs and colon [3,6,25,41]. In cases of CNS actinomycosis, cerebral abscess is the most common presentation but in the patients who are repeatedly treated but have poor compliance or inadequate courses of antibiotics, in them the cerebral granulomas become main presentation. This lesion commonly presents with progressive symptoms and signs of raised intracranial pressure and focal neurological deficits appropriate to the location. There may be a single or multiple brain lesions, abscesses or granulomas. Meningitis is a rare presentation. Chronic meningitis in actinomycosis may occur due to the spread from paranasal sinuses and the middle ear cavity or mastoid sinuses.
Acute presentation may occur due to the rupture of the actinomycotic abscess in the subarachnoid spaces or in the ventricle. Rarely, it may also present with acute subarachnoid hemorrhage with fatal outcome.
Spinal actinomycotic infection may occur from direct extension/continuity of infection in the cervical, thoracic and abdominal regions [41-44]. Spinal osteomyelitis with para-dural abscesses may result. The infection runs a relentless course over many years with destruction of contiguous bones and soft tissues.
Case material
Fourteen cases of CNS actinomycosis with cerebral complications in twelve cases and spinal problems in two cases were seen as evaluated by the authors in their case materials. These patients were intermittently treated with multiple courses of antibiotics. Ten patients had cranial osteomyelitis and intracranial granulomas (Figure 6) and in six of these cases cerebral abscesses were associated with granulomas. One patient had presented with an acute fatal subarachnoid hemorrhage and two with spinal actinomycosis. In ten cases, the cranial/intracranial involvement was due to contiguous spread from the scalp, paranasal sinuses and the facial structures and in two cases thoraco-abdominal actinomycosis with the spine involvement
while one case had an extradural granuloma following a dental extraction and one patient with cerebral abscess following orbital actinomycosis. With appropriate antibiotics in their high doses for a prolonged periods, and added neurosurgical management, thirteen patients were either asymptomatic or mildly symptomatic while one expired due to extensive subarachnoid hemorrhage. In this case no autopsy was performed.
Spinal actinomycosis results from direct extension from pulmonary or abdominal actinomycotic foci and it involves vertebral bodies, related ribs, pedicles, laminae and spinous processes but intervertebral discs are commonly spared in actinomycosis. Anterior vertebral body surfaces may show a saw tooth appearance. Para-spinal abscess and pus draining sinuses are common occurrences, whereas the spinal cord compression is rare. One of our cases, as mentioned before, had marked swelling of the cervical soft tissues, destruction of the occipital bone and posterior elements of the upper cervical spine. She was diagnosed with biopsy and treated effectively with long term medical therapy. There was no spinal instability. The other patient had cervico-thoracic extradural actinomycotic granuloma which was excised twice and treated with antibiotics with good improvement.
Laboratory and neuroimaging diagnostic studies [3-6,7-10,25-27,31,32,41-43,45]
The nonspecific hematological features of infection are present in the patients such as mild anemia, raised ESR and CRP values with leucocytosis [1-3,5-7,26-29]. High index of suspicion is needed in patients who have history of facial discharging sinus, dental extraction, appendicectomy or pulmonary actinomycotic infection. Involvement of jaw may show painless swelling, woody induration and sinus tracts with intermittent pus discharges. The diagnosis requires demonstration of sulfur granules (which are actually tightly clumped colonies of the causative organisms-Actinomyces israeli) present in the pus in the draining sinus or in biopsy sections. The organisms grow on microaerophilic or anaerobic cultures. It is necessary to isolate the organisms from the clinical specimens (transported in anaerobic transport devices) taken directly from the draining sinuses, or via CT or ultra sound guided deep needle aspirates or surgical biopsy specimens (Figure 7).
A chest radiograph may reveal a pneumonitis patch, pulmonary mass or a cavity, with pleural involvement but hardly any hilar adenopathy [31,43]. In thoracic actinomycosis, the mass lesion may extend across fissures or pleura, invading into the adjacent chest wall [36-38,43]. It causes local destruction of the thoracic vertebra, ribs or sternum. The CT scans confirm an infiltrative mass lesion with focal areas of decreased attenuation that enhances with contrast infusion. This infiltrative mass tends to invade surrounding tissues without significant lymphadenopathy. There may be evidence of previous thoracotomy or exploratory laparotomy for the diagnostic purposes [39]. The needle aspirates taken via stereotaxy and the surgical biopsy specimens are then subjected to the microbiological and histopathological studies for a confirmatory diagnosis.
Plain skull films may demonstrate paranasal or mastoid sinusitis and cranial osteomyelitis [3,6,29]. Soap bubble
Figure 6 Cranial actinomycosis with intracranial granulomatous component and compressive mass effects on the left parieto-occipital lobes and the left occipital horn and the trigone of the lateral ventricle.

CentralBringing Excellence in Open Access
Sharma et al. (2017)Email:
JSM Brain Sci 2(2): 1013 (2017) 8/10
vertebrae (the area of rarefaction at the site of active infection and the area of sclerosis at the site of chronic long standing infection) may be seen on the spinal x-rays. The CT brain scan usually demonstrates a solitary thick walled ring enhancing abscess with surrounding edema. The abscess wall may be irregular or nodular. Multi-loculations with cerebral edema may be present [3,6,29-32]. Less commonly solid nodules or masses, granulomas (actinomycotic granuloma), are seen as slightly hyper-attenuation lesion with contrast enhancement. The MRI scans with GD-DTPA enhancement show an irregularly enhancing mass lesion mimicking an intracranial meningioma [3,6]. The MRI scan reveals extensive involvement of the neighboring dura, falx and subdural spaces in cases of cranio-spinal osteomyelitis and epidural / subdural empyema.
Treatment [ 3-6,26,29,36-38]
Actinomyces are highly sensitive to penicillins which have revolutionized the management of Actinomycosis. It also clarified that the medical management should be with high doses and for a prolonged period of time. The management basically includes a combined medical and surgical therapy including the surgical aspiration or excision of intracranial actinomycotic lesions. However, initially a cure should be attempted with medical therapy with periodic assessment with neuro-imaging studies to monitor the progress. Large doses of the drug of choice (DOC), intravenous “penicillin G” (at least 18-24 million units per day), is given over a period of 3-4 months and followed by oral therapy with penicillin or amoxicillin for 6-12 months period or more as needed. Penicillin G interferes with synthesis of the bacterial cell wall muco-peptide during active multiplication, resulting in bactericidal activity against susceptible Actinomyces.
The actinomycotic patients with penicillin allergy are treated with alternative antibiotics i.e., erythromycin, doxycyclin, sulfamethoxazole, imipenem, ceftriaxone, ciprofloxacin, rifampicin, lincomycin and clindamycin, on long term basis with hyperbaric oxygen therapy.
In pregnant women with penicillin hypersensitivity, erythromycin is a safe alternative and doxycycline is commonly
used for non-pregnant women as it inhibits protein synthesis during bacterial growth by binding to 30S and possibly 50S ribosomal subunits of susceptible bacteria. In penicillin resistant cases, for both the actinomycosis and the companion bacteria, the medications such as Imipenem/cilastatin, Amoxacillin/clavulanic acid and Clindamycin are used. Cephalosporins (ceftriaxone, ceftazidime) are used to cover both the pathogenic actinomycetes and their companion gram negative bacteria, in moderately severe to severe infections.
Actinomycotic cerebral abscess may be aspirated and intracranial granulomas excised with image guided techniques. Appropriate craniotomy or laminectomy procedures must be undertaken wherever needed as per urgency of the case. Penicillin may bring cure in spinal actinomycosis, however surgical drainage, spinal decompression and stabilization procedures may have to be undertaken where indicated. Because of the optimal antibiotic therapy, the prognosis is far better in actinomycosis than that for true fungal infections. In some cases, a complete resolution of the infection may be achieved by means of surgical treatment and prolonged antibiotic therapy in higher doses.
Prognosis [3-6,26,29-34,36-38,45]
Fortunately, systemic actinomycosis is rare and moreover, its CNS involvement is a further rarity. It responds very well to the antibiotics especially Penicillin-G and if given in adequately higher doses for a prolonged periods of time then the cure is possible and the relapses may be prevented. The availability of other alternative antibiotics (erythromycin, doxycyclin, sulfamethoxazole, imipenem, ceftriaxone, ciprofloxacin, rifampicin, lincomycin and clindamycin) for the penicillin resistant actinomycotic infections has greatly improved the prognosis of all forms of actinomycosis. Surgical management consists of image guided aspirations of cerebral abscesses and excision of granulomas as well as debridement of the involved tissues. At present, the clinical cure rates are high, and neither deformity nor death is common although the morbidities keep challenging the role of awareness and early detection in its management, which if achieved, will further lessen the morbidities and attain higher overall satisfactory results.
CONCLUSIONS The CNS nocardiosis and actinomycosis, although ubiquitous
in worldwide distribution, are rare gram positive bacterial infections with extremely low incidences. The causative bacteria, Actinomyces, are filamentous bacilli mimicking fungi in their morphology. Their symptomatology could be insidious, variable and without usual infective symptoms such as fever, sweating, malaise, tiredness, toxic look etc; which result in delaying the diagnosis and preventing an early treatment. Nocardiosis may present with the primary focus in the lungs, paranasal sinuses, and in the skin and secondarily infect the CNS; whereas, actinomycosis initially manifest as dental, pulmonary, or abdominal problem and then secondarily infect the CNS.
In symptomatic CNS cases, they present mainly with the progressive manifestations of a mass lesion frequently such as cerebral abscess, and less frequently as granulomas but rarely
Figure 7 Gram Positive Actinomyces israeli.

CentralBringing Excellence in Open Access
Sharma et al. (2017)Email:
JSM Brain Sci 2(2): 1013 (2017) 9/10
with cerebritis and meningitis. These manifestations may mimick cerebral neoplasms, strokes, multiple sclerosis, ophthalmological problems, paranasal sinus infections and possibly delaying the correct diagnosis and treatment. Apart from the routine microbiological diagnostics, new modern technological advances made it possible to more accurately identify the micro-organisms such as Actinomyce and Nocardia i.e., molecular technologies, MALDI-TOF-MS Studies, and 16S rRNA gene sequencing and help even in selection of the antibiotics for the bacterial microorganisms.
The CNS nocardiosis and actinomycosis are effectively treatable with their drug of choice, cotrimoxazole for the former and the penicillin-G for the later. In resistant cases alternative medications (erythromycin, doxycyclin, sulfamethoxazole, imipenem, ceftriaxone, ciprofloxacin, rifampicin, lincomycin and clindamycin) have very effective roles. Nocardiac or actinomycotic cerebral abscesses may be aspirated and intracranial granulomas excised with image guided neurosurgical techniques. Appropriate craniotomy or laminectomy procedures must be undertaken wherever needed as per the urgency of the case.
The mortality rates estimated for multiple abscesses due to Nocardia farcinica are significant. Mortality with nocardial brain abscess diagnosed ante-mortem is about 20-30% in immune competent patients but it increases to 40% in cases of multiple abscesses and about 55% in immune-compromised patients. This infection might progress despite a specific therapy and tend to relapse due to antibiotic resistance and inadequate period of therapy. All patients with pulmonary nocardiosis should have MRI brain scans to rule out the subclinical CNS infections. Early identification with appropriate and prolonged treatment (up to one year) is crucial for a favorable outcome and prevention of relapses. At present, the clinical cure rates in the CNS actinomycosis are high, and neither deformity nor death is common although the morbidities are pertaining to the local cerebral damage due to the infection and the mass effect of the lesions. The role of awareness and early detection in its management cannot be over emphasized to further lessen the morbidities and achieve higher overall satisfactory results.
REFERENCES1. Bauserman SC, Schochet Jr. SS. Bacterial, fungal and parasitic diseases
of the central nervous system. In Nelson JS, Parisi JE, Schochet Jr. SS, editors: Principles and Practice of Neuropathology; London: Mosby 1993: 42-74.
2. Kirkpatrick JB. Neurologic Infections due to Bacteria, Fungi and Parasites. In Davis RL, Robertson DM editors: Textbook of Neuropathology. Second edition Baltimore: Williams & Wilkins 1991: 719-803.
3. Sharma RR, Pawar SJ, Lad SD, Mishra GP, Netalkar AS, Rege S. Fungal Infection of the Central Nervous System. In: Alfredo Quinones-Hinojosa, editor. Schmidek & Sweet: Operative Neurosurgical Techniques. Indications, Methods, and Results. Philadelphia PA: WB Saunder Elsevier Inc; 2012 6th Edn, Vol 2. 1691-1732.
4. Könönen E, Wade WG. Actinomyces and related organisms in human infections. Clin Microbiol Rev. 2015; 28: 419-442.
5. Warren NG. Actinomycosis, nocardiosis, and actinomycetoma. Dermatol Clin. 1996; 14: 85-95.
6. Sharma RR, Lad SD, Desai AP, Lynch PG. Surgical Management of fungal infections of the Nervous System. In Schmidek HH editor: Schmidek & Sweet’s Operative Neurosurgical Techniques, Indications, Methods and Results, 4th edn, 2000; 726-755.
7. Lerner PI. Nocardiosis. Clin Infect Dis. 1996; 22: 891-903.
8. Kumar VA, Augustine D, Panikar D, Nandakumar A, Dinesh KR, Karim S, et al. Nocardia farcinica brain abscess: epidemiology, pathophysiology, and literature review. Surg Infect (Larchmt). 2014; 15: 640-646.
9. Lederman ER, Crum NF. A case series and focused review of nocardiosis: Clinical and microbiological aspects. Medicine (Baltimore). 2004; 83: 300-313.
10. Palmer DL, Harvey RL, Wheeler JK. Diagnosis and therapeutic considerations in nocardia asteroides infection. Medicine (Baltimore). 1974; 53: 391-401.
11. Alijani N, Mahmoudzadeh S, Hedayat YM, Geramishoar M, Jafari S. Multiple brain abscesses due to nocardia in an immunocompetent patient. Arch Iran Med. 2013; 16: 192-194.
12. Kennedy KJ, Chung KH, Bowden FJ, Mews PJ, Pik JH, Fuller JW, et al. A cluster of nocardial brain abscesses. Surg Neurol. 2007; 68: 43-49.
13. Lin YJ, Yang KY, Ho JT, Lee TC, Wang HC, Su FW. Nocardial brain abscess. J Clin Neurosci. 2010; 17: 250-253.
14. Sharma RR, Pawar SJ, Ravi RR, Sausa J, Devadas RV, Athale S. A solitary primary Aspergillus Brain abscess in an immuno-competent host: CT guided stereotaxy with an excellent outcome. Pan Arab J Neurosurg. 2002; 6: 62-65.
15. Sharma RR, Gurusinghe NT, Lynch PG. Cerebral infarction due to aspergillus arteritis following glioma surgery. Br J Neurosurg. 1992; 6: 485-490.
16. Mogilner A, Jallo GI, Zagzag D, Kelly PJ. Nocardia abscess of the choroids plexus: clinical and pathological case report. Neurosurgery. 1998; 43: 949-952.
17. Durmaz R, Atasoy MA, Durmaz G, Adapinar B, Arslantas A, Aydinli A, et al. Multiple nocardial abscesses of cerebrum, cerebellum and spinal cord causing quadriplegia. Clin Neurol Neurosurg. 2001; 103: 59-62.
18. Verroken A, Janssens M, Berhin C, Bogaerts P, Huang T-D, Wauters G, et al. Evaluation of Matrix Assisted Laser Desorption Ionization-Time of Flight Mass Spectrometry for identification of Nocardia Species. J Clin Microbiology. 2010; 48: 4015-4021.
19. Laurin JM, Resnik CS, Wheeler D, Needleman BW. Vertebral osteomyelitis caused by Nocardia asteroides: Report and review of the literature. J Rheumatol. 1991; 18: 455-458.
20. Peterson JM, Awad I, Ahmed M, Bay JW, McHenry MC. Nocardia osteomyelitis and epidural abscess in the non-immuno-suppressed host. Cleve Clin Q. 1983; 50: 453-459.
21. Siao P, McCabe P, Yagnik P. Nocardial spinal epidural abscess. Neurology. 1989; 39: 996.
22. Oshiro S, Ohnishi H, Ohta M, Tsuchimochi H. Intraventricular rupture of Nocardia brain abscess-case report. Neurol Med Chir (Tokyo). 2003; 43: 360-363.
23. Young WF. Syringomyelia presenting as a delayed complication of treatment for nocardia brain abscess. Spinal cord. 2000; 38: 265-269.
24. Nandhagopal R, Al-Muharrmi Z, Balkhair A. Nocardia brain abscess. QMJ. 2014; 107: 1041-1042.
25. Lad SD, Chandy MJ. Craniofacial actinomycosis. Brit J Neurosurg. 1991; 5: 361-370.
26. Oostman O, Smego RA. Cervicofacial Actinomycosis. Diagnosis and

CentralBringing Excellence in Open Access
Sharma et al. (2017)Email:
JSM Brain Sci 2(2): 1013 (2017) 10/10
Sharma RR, Sharma A (2017) Cranio-Cerebral Abscesses in Nocardiosis and Actinomycosis: Assessment and Management Strategies. JSM Brain Sci 2(2): 1013.
Cite this article
Management. Curr Infect Dis Rep. 2005; 7: 170-174.
27. Göçmen G, Varol A, Göker K, Basa S. Actinomycosis. Report of a case with a persistent extraoral sinus tract. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2011; 112: 121-123.
28. Sharma RR. Fungal Infections of the Nervous System; Current Perspective and Controversies in Management. Int J Surg. 2010; 8: 591-601.
29. Weese WC, Smith IM. A study of 57 cases of actinomycosis over a 36-year period. A diagnostic ‘failure’ with good prognosis after treatment. Arch Intern Med. 1975; 135: 1562-1568.
30. Bolton CF, Ashenhurst EM. Actinomycosis of the brain. Can Med Ass J. 1964: 90: 922-928.
31. Kim TS, Han J, Koh WJ, Choi JC, Chung MJ, Lee JH, et al. Thoracic Actinomycosis: CT Features with Histopathologic Correlation. AJR Am J Roentgenol. 2006; 186: 225-231.
32. Khosla VK, Banerjee AK, Chopra JS. Intracranial actinomycoma with osteomyelitis simulating meningioma. Case report. J Neurosurg. 1984; 60: 204-207.
33. Bizzini A,Jaton K, Romo D, Bille J, Prod’hem G, Greub G. Matrix-assisted laser desorption ionization- Time of flight mass spectrometry as an alternative to 16S rRNA gene sequencing for identification of difficult-to-identify bacterial strains. J Clin Microbiol. 2011; 49: 693-696.
34. Pulverer G, Schutt-Gerowitt H, Schaal KP. Human cervicofacial actinomycoses: microbiological data for 1997 cases. Clin Infect Dis. 2003; 37: 490-497.
35. Sharma RR, Pawar SJ, Delmendo A, Lad SD, Athale SD. Fatal rhino-orbito-cerebral mucormycosis in an apparently normal host: case report and literature review. J Clin Neurosci. 2001; 8: 583-586.
36. Ferreira Dde F, Amado J, Neves S, Taveira N, Carvalho A, Nogueira R. Treatment of pulmonary actinomycosis with levofloxacin. J Bras Pneumol. 2008; 34: 245-248.
37. Endo S, Murayama F, Yamaguchi T, Yamamoto S, Otani S, Saito N, et al. Surgical considerations for pulmonary actinomycosis. Ann Thorac Surg. 2002; 74: 185-190.
38. Chouabe S, Perdu D, Deslée G, Milosevic D, Marque E, Lebargy F. Endobronchial actinomycosis associated with foreign body: four cases and a review of the literature. Chest. 2002; 121: 2069-2072.
39. Cintron JR, Del Pino A, Duarte B, Wood D. Abdominal actinomycosis. Dis Colon Rectum. 1996; 39: 105-108.
40. Westhoff C. IUDs and colonization or infection with Actinomyces. Contraception. 2007; 75: 48-50.
41. Alday R, Lopez-Ferro MO, Fernandez-Guerrero M, P. Ruiz-Barnés, et al. Spinal intrathecal empyema due to actinomycosis Israelii. Acta Neurochir. 1989; 101: 159-162.
42. David CV, Jayalakshmi P. Actinomycosis of the Spine: Two case reports. Med J Malaysia. 1983: 38: 161.
43. Nolan RL, Ross JD, Chapman SW. Thoracic actinomycosis presenting as spinal cord compression. J Miss State Med Assoc. 1990; 31: 41-45.
44. Ushikoshi S, Koyanagi I, Hida K, Iwasaki Y, Abe H. Spinal intrathecal actinomycosis: a case report. Surg Neurol. 1998; 50: 221-225.
45. Benito León J, Muñoz A, León PG, Rivas JJ, Ramos A. Actinomycotic brain abscess. Neurologia. 1998; 13: 357-361.







![Actinomycosis of the Cheek - National Library of Serbia€¦ · nocardiosis [20]. Lymphatogenous spread of actinomyces is rare because of the size of bacteria; cervical lymphadenopathy](https://img.pdfslide.net/doc/110x75/5ed71fd0c30795314c173dd1/actinomycosis-of-the-cheek-national-library-of-nocardiosis-20-lymphatogenous.jpg)





















