Embed Size (px)
Citation preview

Craniotomy and Internal Carotid Blood Flow *
ANIBAL GALINDO, M/I.D., V. P. SAVOLAINEN,** M.D., Toivo SUUTARINEN, M.D.
Bethesda, Maryland
IN MIAN, a change from the horizontal tothe erect posture has little or no effect on
cerebral blood flow.9 This cerebral homeo-stasis is supposedly maintained by simul-taneous vascular modifications subsequentto changes in intracranial pressure.10 Theefficacy of these mechanisms during crani-otomy (and coincidental change in headposition) has been examined through re-
cording of internal carotid blood flow andintracranial pressure. Thus the internal ca-
rotid blood flow and its vascular resistancehave been studied before, during and aftercraniotomy in several head positions. Theo-retically, there is enough information topredict changes, after craniotomy, in cere-
bral blood flow and cerebrovascular resist-ance. They have practical application inneurosurgery and could explain some ofthe present problems related to bulging ofthe brain, or the high incidence of circula-tory collapse reported in the sitting posi-tion.6' 7
Method
Eleven Rhesus monkeys of 3 to 8 Kg.body weight were used. Induction was ac-
complished with light ether anesthesia. Atracheostomy was rapidly performed andan endotracheal cannula tightly fixed. Arti-ficial respiration was immediately started
Submitted for publication March 4, 1963.Section on Neuro-anesthesiology, Branch of
Surgical Neurology, National Institute of Neuro-logical Diseases and Blindness.
Anesthesiology Department, Clinical Cen-ter, National Institutes of Health, USPHS, De-partment of Health, Education and Welfare, Beth-esda 14, Maryland.
437
using 100 per cent oxygen in a Bird respira-tor with a non-rebreathing valve. Etherwas discontinued and the animals werekept paralyzed with 1 per cent succinyl-choline, 1 to 2 mg./Kg. body weight, everyfive to ten minutes. Changes in the arterialCO., were obtained by decreasing the min-ute volume.
Plastic catheters were advanced through:the femoral vein to the inferior vena cava;the femoral artery to the abdominal aorta;and the left external jugular vein, or theaxillary vein, to the superior vena cava.A plastic cannula was inserted in the leftlateral cerebral ventricle. The left externalcarotid artery was dissected in the leftlateral cerebral ventricle. The left externalcarotid artery was dissected and its bifur-cation exposed. A 1 mm. probe for electro-magnetic blood flow measurements wasplaced proximal to the bifurcation. By thismeans it was possible to determine andrecord in a Sanborn 150 recording unit theinferior and superior vena cava pressures,arterial blood pressure, intraventricularpressure, and carotid blood flow. The vas-cular resistance was calculated as the rela-tionship: Arterial blood pressure-superiorvena cava pressure in mm. Hg over internalcarotid blood flow in cc./min., and theresult-was given arbitrarily in units.
Statham pressure transducers were usedfor pressure determinations. The transduc-cers were calibrated before each experi-ment with standard mercury and watermanometers. The mean arterial blood pres-sure was obtained by means of an elec-
GALINI)O, SAVOLAINEN AND SUUTARINEN Aninals of SurgeryNMarch 1964
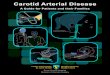
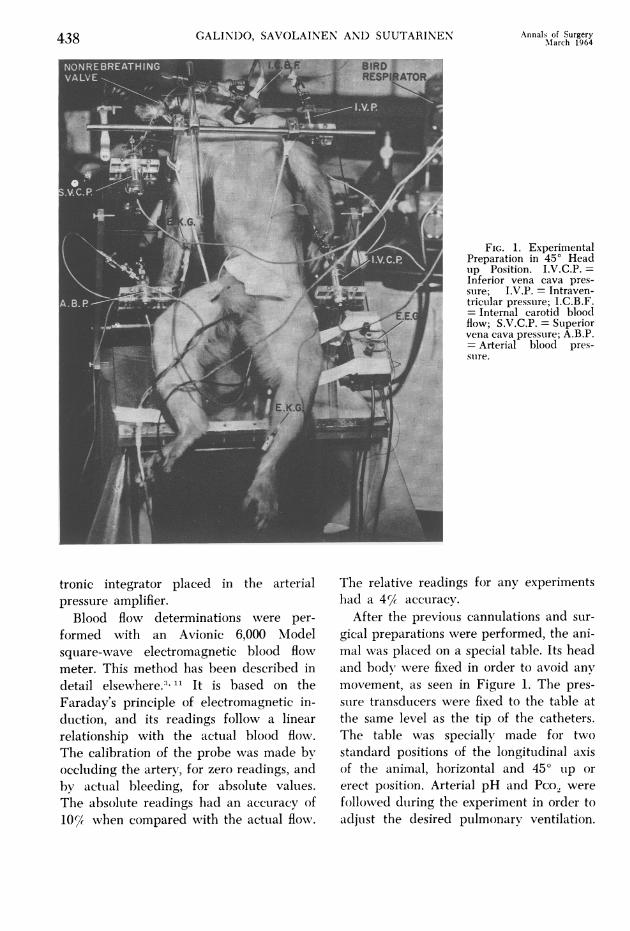
FIG. 1. ExperimentalPreparation in 450 Headup Position. I.V.C.P. =Inferior vena cava pres-sure; I.V.P. = Intraven-trictular pressure; I.C.B.F.= Internal carotid bloodflow; S.V.C.P. = Superiorvena cava pressuire; A.B.P.= Arterial blood pres-sture.
tronic integrator placed in the arterialpressure amplifier.
Blood flow determinations were per-
formed with an Avionic 6,000 Modelsquare-wave electromagnetic blood flowmeter. This method has been described indetail elsewhere.) It is based on theFaraday's principle of electromagnetic in-duction, and its readings follow a linearrelationship with the actual blood flow.The calibration of the probe was made byoccluding the artery, for zero readings, andby actual bleeding, for absolute values.The absolute readings had an accuracy of10% when compared with the actual flow.
The relative readings for any experimentshad a 4% accuracy.
After the previous cannulations and sur-
gical preparations were performed, the ani-mal was placed on a special table. Its headand body wvere fixed in order to avoid any
movement, as seen in Figure 1. The pres-
sure transducers were fixed to the table atthe same level as the tip of the catheters.The table w%vas specially made for twostandard positions of the longitudinal axisof the animal, horizontal and 450 up or
erect position. Arterial pH and Pco. were
followed during the experiment in order to
adjust the desired pulmonary ventilation.
438
CRANIOTOMY ANI) INTERNAL CAROTII) 13LO01) FLOW
Samples of arterial blood (2 cc.) were
analyzed in a Severinghauis electrode and
a Beckman pH electrode (InstrumentationLaboratory Model 105). Determinationsvere made at body temperature.
EKG II lead and fronto-occipital EEGlead were recorded continuously. The ex-
periment can be summarized as follows:1. Common carotid blood flow determinations
were recorded simu-illtaneouisly with the other pa-
raimeters.2. The external carotid artery was tied, leaving
only the internal carotid blood flow throuigh thecommon carotid artery. Arterial Pco2 was keptconstant during both determinations.
3. All parameters were recorded in the hori-zontal position.
4. The animal was placed in the erect positionand recordings were repeated. The Pco2 was com-
parable to valuies obtained in the horizontal posi-tion.
5. In fouir animals, hallothane was administeredand the same positional changes were performeddturing halothane anesthesia. This was repeatedseveral times in both directions and at the same
arterial Pco2.
6. A standard size craniotomy, 2.5 cm. in di-ameter, was performed. Then recordings were re-
peated before the opening of the dura.7. The dtura mater was opened. The arterial
Pco2 was kept constant for a minimumilm of 20 min-utes.
8. The position of the body was changed sev-
eral times, from horizontal to the erect position,similar to changes performed before craniotomy.The arterial Pco2 was kept at a constant value.
Only observations in which the arterialPco., were the same (+ 5 mm. Hg) were
included in this study. The effective perfu-sion pressure was calculated from the meanarterial blood pressure minus the superiorvena cava pressure.
In order to obtain higher internal ca-
rotid blood flows, the arterial Pco., was
maintained at high levels in most experi-
ments.
Results
The internal carotid blood flow, as a per-
centage of the common carotid blood flow,was dependent on the arterial Pco_. It was
50 per cent with an arterial Pco., of 30 mm.Hg, and 75 per cent for 70 imm. Hg.
Effect of Positional Changes BeforeCraniotomy. This determination was madeunder two circumstances: in succinylcho-line paralyzed animals and in animalstunder halothane anesthesia.
Succinylcholine Paralyzed Animals(Table 1, Fig. 2). There was no differencein the internal carotid blood flow from hori-zontal (25.6 cc./min.) to the erect position(25.2 cc./min.). The arterial Pco2 (normalto high) apparently had no influence on
these results. Similar stability was observedwith normal arterial Pco., or with high ar-
terial Pco. (Table 1). The effective perfu-sion pressure (mean arterial blood pressure
minus superior vena cava pressure) in-
creased slightly from 105.6 mm. Hg inhorizontal position, to 111.8 mm. Hg inthe erect position. The intracranial pres-
sure fell from 34.8 cm. H.,O in the hori-zontal position to 16.5 cm. 1J20 when thetable was elevated to 450. There was an
increase of 10 per cent in the resistance ofthe internal carotid artery.Halothane Anesthesia (Table 1). There
was a 29.7 per cent decrease in the effec-tive perfusion pressure when the axis ofthe table was raised to a 450 angle. Theinternal carotid blood flow decreased 44.5per cent and its vascular resistance in-creased 16.5 per cent. At the same time,the intracranial pressure decreased by 18.7cm. H.O. The postural hypotension and theinternal carotid blood flow decrease were
related with the depth of anesthesia.Effects Produced by Craniotomy. There
was no significant change in any of theparameters when the bone was removed;however, the opening of the dura (Table2, Fig. 3) was followed by small, but sig-nificant changes. They were not immediate,and were complete only 15 to 20 minutesafter the opening. The internal carotidblood flow increased 22.6 per cent while itsvascular resistance decreased 19.1 per cent.There were no changes in the effective per-
Volunie 159Number 3 439
GALINDO, SAVOLAINEN AND SUUTARINEN Annals of SurgeryMarch 1964
TABLE 1
Before Craniotomv:Succinvlcholine paralyzed animals
I.C.B.F.
H. 450
E.P.P.
H. 450
I.V.P.
H. 450 Pco2
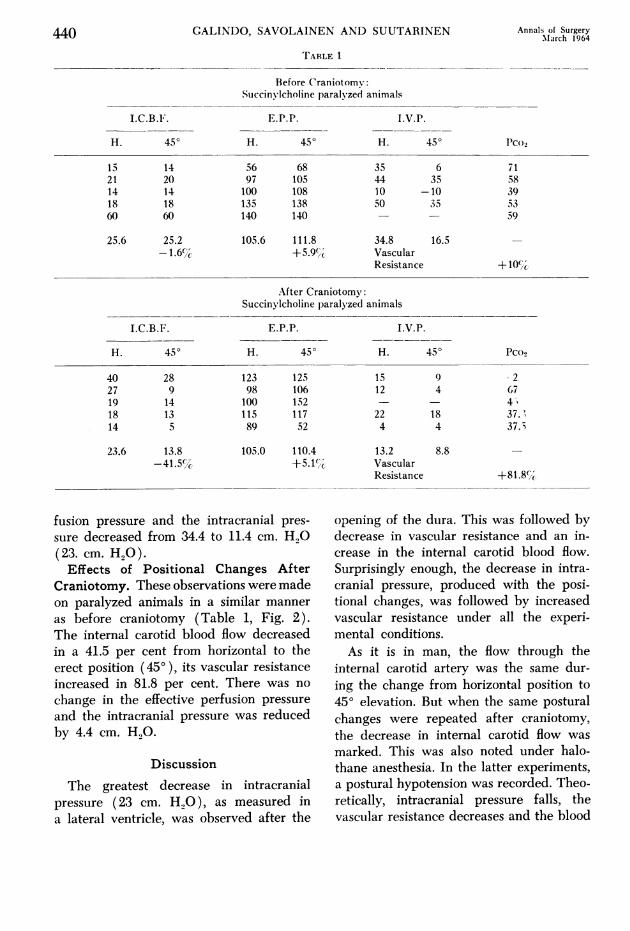
15 14 56 68 35 6 7121 20 97 105 44 35 5814 14 100 108 10 -10 3918 18 135 138 50 35 5360 60 140 140 - - 59
25.6 25.2 105.6 111.8 34.8 16.5 -
-1.6% +5.9%1 VascularResistance +10C(/C
After Craniotomy:Succinylcholine paralyzed animals
I.C.B.F. E.P.P. I.V.P.
H. 450 H. 450 H. 450 Pco9
40 28 123 125 15 9 227 9 98 106 12 4 6719 14 100 152 - - 4%18 13 115 117 22 18 37.'14 5 89 52 4 4 37.3
23.6 13.8 105.0 110.4 13.2 8.8 -
-41.5% +5.14,,, VascularResistance +81.8c/%
fusion pressure and the intracranial pres-
sure decreased from 34.4 to 11.4 cm. H,O(23. cm. H,0).Effects of Positional Changes After
Craniotomy. These observations were madeon paralyzed animals in a similar manner
as before craniotomy (Table 1, Fig. 2).The internal carotid blood flow decreasedin a 41.5 per cent from horizontal to theerect position (450 ), its vascular resistanceincreased in 81.8 per cent. There was no
change in the effective perfusion pressureand the intracranial pressure was reducedby 4.4 cm. HO.
Discussion
The greatest decrease in intracranialpressure (23 cm. H.,O), as measured ina lateral ventricle, was observed after the
opening of the dura. This was followed bydecrease in vascular resistance and an in-crease in the internal carotid blood flow.Surprisingly enough, the decrease in intra-cranial pressure, produced with the posi-tional changes, was followed by increasedvascular resistance under all the experi-mental conditions.As it is in man, the flow through the
internal carotid artery was the same dur-ing the change from horizontal position to450 elevation. But when the same posturalchanges were repeated after craniotomy,the decrease in internal carotid flow was
marked. This was also noted under halo-thane anesthesia. In the latter experiments,a postural hypotension was recorded. Theo-retically, intracranial pressure falls, thevascular resistance decreases and the blood
440
Volume 159Number 3
CRANIOTOMY AND INTERNAL CAROTID BLOOD FLOW
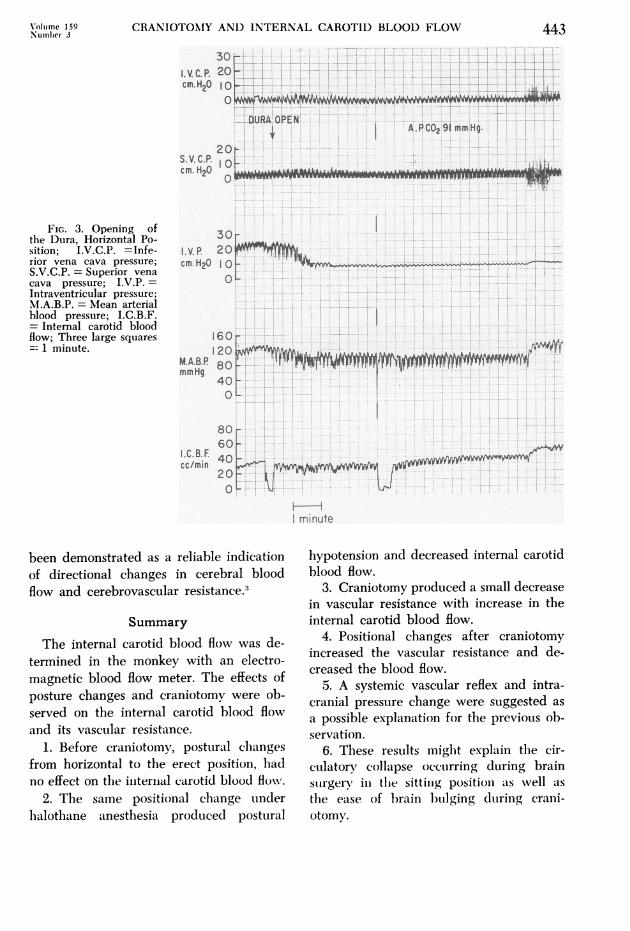
TABLE 1. (Continued)The Effects of Craniotomv
I.C.B.F. E.P.P. I.V.P.
B. A. B. A. B. A. Pco2
39 54 128 128 48 20 9021 27 97 98 44 12 6220 17 112 112 25 5 4814 17 100 102 10 -4 3812 15 63 59 45 24 37
21.2 26.0 100 99.8 34.4 11.4 -
+22.6%C -2% VascularResistance -19.1'
Halothane Anesthesia Before Craniotomv
I.C.B.F. E.P.P. I.V.P.
H. 450 H. 450 H. 450 Pco2
32 14 91 in 35 3 7120 10 103 56 12 8 3414 10 85 57 45 25 5329 19 94 94 - - 29
23.8 13.2 93.2 65.5 30.7 12.0 --44.5%;c -29.7% Vascular
Resistance + 16.3'iC
H = Horizontal A = After craniotomy B = Before craniotomy.I.C.B.F. = Internal carotid blood flow in relative values (cc./min.).E.P.P. = Effective perfusion pressure in mm. Hg.I.V.P. = Intraventricular pressure in cm. H20.Pco2 = Arterial Pco2 in mm. Hg.Vasc. Res. = Vascular resistance in the intemal carotid arterv in units. Relative change from control.
flow increases. This occurred after crani-otomy in the horizontal position. But whenthe head was raised after craniotomy, thevascular resistance increased. The smallincrease in effective perfusion pressure, as
in the case of paralyzed animals, was dueto a decrease in superior vena cava pres-
sure. Therefore, there was a difference be-tween the effects of the lower intracranialpressure producd by postural changes andthose produced by craniotomy. This para-doxical difference is explained through a
pressure reflex triggered by the posturalchanges 4 in which the systemic vascularbed, incltuding the brain, is constricted. Atthe same time, a regional compensationproduced by the lower intracranial pres-
sure takes place in the cerebrovascular bed.
The existence of this reflex is suggestedby the postural hypotension during halo-thane anesthesia and the lack of compen-
sation after craniotomy. In the latter case,
it could be manifested by an increase inresistance and a decrease in flow (as was
observed). A decrease in cardiac outputin the erect position has been demonstratedin man.5 12 An increase in vascular tonewas found in the liver 2 and the hand.'This postural vasoconstriction is suggestedand discussed by Rushmer.8 We have stud-ied this reflex vasoconstriction in the erectposition. Our findings are in agreementwitlh these observations.4Craniotomy decreased the vascuLlar re-
sistance in the internal carotid artery andincreased its flow. This in turn is reflected
441
GALINDO, SAVOLAINEN AND SUUTARINEN Annals of SurgeryMarch 1964
BEFORE CRANIOTOMYV
AFTER CRANIOTOMYHH
.-__~~~~~~~
FIi Iii
302 1.V.C.P.10 cm.H2p0
I-APC02z 58.61mm Hg.
10 S.V.C.PI0 Min
I Mingle
40
-1,-.L
.V. P.eellz
APCO2 67.3mm Hg.-
100
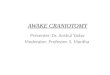
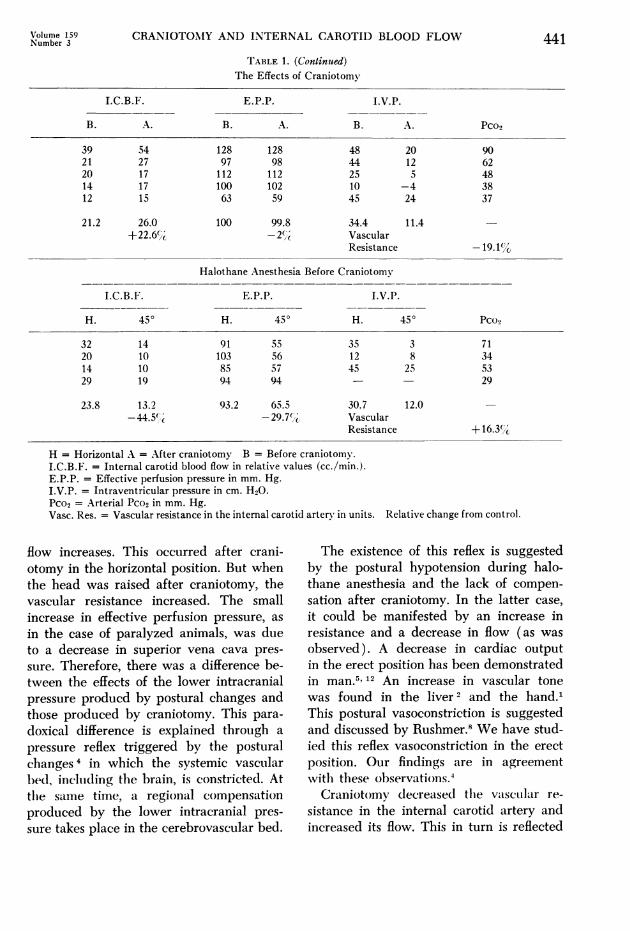
FIG. 2. PositionalChanges: V = 450 headup; H =horizontal. I.V.C.P. = Inferior vena cavapressure; S.V.C.P. = Su-perior vena cava pres-sure; I.V.P. = Intraven-tricular pressure; M.A.B.P. = Mean arterial bloodpressure; L.I.C.B.F. =Left internal carotid bloodflow.
M.A.LP.mm. Ho.
L.lC.B.F.
i40 cc. /min.
la
by an increase in brain size which may
set the stage for dangerous bulging at thecraniotomy site. Thus there is a need formore careful respiratory and postural con-
trol during craniotomy.However, when this flow has been de-
creased by the combination of craniotomyand the sitting position, a rapid and per-
haps dangerous decrease in cerebral bloodflow may occur. This sharp reduction inblood flow seems a more likely cause ofaccident in the sitting position than doesthe so-called air embolism. Supposedly, airemibolisim is the imiain causal factor in such
mishaps. The fact that its incidence ishligher dtirinig artificial respiration lhas sug-
gested the use of spontaneous respiration,or high jugular venous pressure as preven-
tive measures.' It is difficult to under-stand how spontaneous respiration can pre-
vent air embolism in the sitting position,and how artificial respiration increases itsincidence. There is a greater negative intra-thoracic pressure during the former typeof respiration which would bring exactlythe opposite result. It seems more likelythat the presence of a higher arterial Pco.,during spontaneous respiration (which, inturn, causes higher cerebral blood flows)xvould explain the advantage of this typeof respiration. On the other hand, artificialrespirationi is likely to lower the arterialPco., decreasiing the cerebral blood flow.The internial carotid artery of the muon-
kev lhas been taken as a sample of thecerebrovascular bed. Its modifications have
442
V
r
CRANIOTO0MY AND INTERNAL CAROTID BLOOD FLOW
3 --44-I-l I 'It44--:4TF?:-:-I- F-1-
A
2S.V.C.P Icm. H20
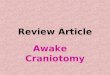
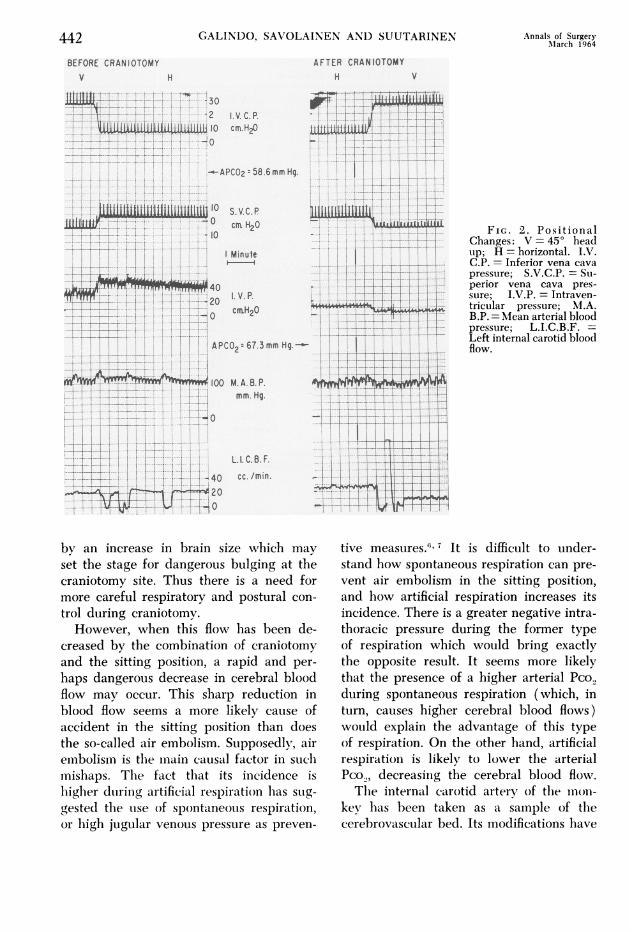
FIG. 3. Opening ofthe Dura, Horizontal Po-sition; I.V.C.P. =Infe-rior vena cava pressure;S.V.C.P. = Superior venacava pressure; I.V.P. =Intraventricular pressure;M.A.B.P. = Mean arterialblood pressure; I.C.B.F.= Internal carotid bloodflow; Three large squares=- 1 minute.
!00
30I.V.p. 20CEIIH20O 0
n
.-.. ,... .
.- . ... 1 ..
__I...
- 1 .. i..--i .-:.1- - -4 &- I
160120
KA.&P. 80mmHg40
01.
I.C.LEcclmin
60~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~- ----i---...l; ....'','-t-t,,...40~~~~~~~~~~ . . .X..
6 ... .......
Ofl . t-'--19.-|--' 't,~~~~~~V I. ...: . .......,--i: :tl:ti+ i:-FIl l-
I minute
been demonstrated as a reliable indicationof directional changes in cerebral bloodflow and cerebrovascular resistance.3
Summary
The internal carotid blood flow was de-termined in the monkey with an electro-magnetic blood flow meter. The effects ofposture changes and craniotomy were ob-served on the internal carotid blood flowand its vascular resistance.
1. Before craniotomy, postural clhangesfrom horizontal to the erect position, hadno effect on thte initernal carotid blood flow.
2. The same positional chalnge underhalothane anesthesia produced postural
hypotension and decreased internal carotidblood flow.
3. Craniotomy produced a small decreasein vascular resistance with increase in theinternal carotid blood flow.
4. Positional changes after craniotomyincreased the vascular resistance and de-creased the blood flow.
5. A systemic vascular reflex and intra-cranial pressure change were suggested as
a possible explanation for the previous ob-servation.
6. These restults miglht explain the cir-culatory collapse occurring during brainsUrgery in the sittinig positioni as wvell as
the ease of l)rain builging during crani-otomy.
Xoltime 159Number 3 443
- -1
if
..-L---L-.-.- ----
0 -1 'r,
I--]-1I..S.- -& ........
F-'l.--- |~ir-TI ,---
... !I i ... !..-A ....... ...
i ----------;........ .I
444 GALINDO, SAVOLAINEN AND SUUTARINEN Annals of SurgeryX-M--m ~~~~~~~~~~~~~~~~~~~~~~March1964
Bibliography
1. Beaconsfield, P. and J. Ginsburg: The Effectof Body Posture on the Hand Blood Flow.J. Physiol. (Lon.), 130:467, 1955.
2. Culbertson, J. W., R. W. Wilkins, F. J. Ingel-finger and S. E. Bradley: The Effect of theUpright Posture upon Hepatic Blood Flowin Normotensive and Hypertensive Subjects.J. Clin. Invest., 30:305, 1951.
3. Galindo, A. and M. Baldwin: Electromag-netic Blood Flow Determinations in the In-ternal Carotid Artery. Intracranial Pressureand Intemal Carotid Blood Flow DuringHalothane Anesthesia in the Dog. (In prepa-ration)
4. Galindo, A., V. P. Savolainen and T. Suuta-rinen: Reflex Mechanism of Postural Vaso-constriction in the Erect Position. (TheSpinal-Postural-Vasopressor Reflex.) (Inpreparation)
5. Hellebrandt, F. A. and E. B. Franseen: Physi-ological Study of Vertical Stance of Man.Physiol. Rev., 23:220, 1943.
6. Hewer, A. J. and V. Logue: Methods of In-creasing the Safety of Neuroanesthesia inthe Sitting Position. Anesthesia, 17:476,1962.
7. Hunter, A. R.: Air Embolism in the SittingPosition. Anesthesia, 17:467, 1962.
8. Rushmer, R. F.: Cardiovascular Dynamics.2nd Ed., pp. 171-192. Philadelphia, W. B.Saunders, 1961.
9. Shenkin, H. A., W. G. Scheuerman, E. B.Spitz and R. A. Groff: Effect of Change ofPosition upon the Cerebral Circulation ofMan. J. Appl. Physiol., 2:317, 1949-1950.
10. Sokoloff, L.: The Action of Drugs on theCerebral Circulation. Pharmacol. Rev., 11:1,1959.
11. Spencer, M. P. and A. B. Denison, Jr.: Square-wave Electromagnetic Flowmeter for Sur-gical and Experimental Application. Meth.Med. Res., 8:321, 1960.
12. Weissler, A. M., J. J. Leonard and J. V. War-ren: Effects of Posture and Atropine on theCardiac Output. J. Clin. Invest., 36:1656,1957.