Embed Size (px)
Citation preview

Cryoablation of Small Renal Tumors
Steve Konrad Williams a, Jean J.M.C.H. de la Rosette b, Jaime Landman c,Francis Xavier Keeley Jr.a,*aBristol Urological Institute, Bristol, UKbAcademic Medical Center, Amsterdam, The NetherlandscColumbia University Medical Center, New York, NY, USA
e a u - e b u u p d a t e s e r i e s 5 ( 2 0 0 7 ) 2 0 6 – 2 1 8
avai lable at www.sc iencedi rect .com
journal homepage: www.europeanurology.com
Article info
Keywords:CryoablationCryotherapyKidney cancerSmall renal massRadiofrequency ablationPartial nephrectomyObservation
Abstract
Objectives: To review the worldwide experience with cryoablation ofsmall renal tumors.Methods: A systematic review was made of all English language pub-lications on cryoablation of renal tumors as well as partial nephrectomy,radiofrequency ablation and high intensity focused ultrasound pub-lished prior to September 2006. The literature was reviewed and thefindings analyzed.Results: Data from basic science and clinical trials supports renal cryoa-blation as a safe and effective method for treatment of small renaltumors. Clinical studies document less peri- and post-operative morbid-ity than laparoscopic partial nephrectomy. Basic science and clinicalstudies suggest superior efficacy with cryoablation as compared toradiofrequency ablation. Longer follow-up is needed before its trueefficacy can be established.Conclusion: Laparoscopic renal cryoablation, though evolving, appears tobe a reasonable alternative for the treatment of small renal tumors inselected patients. Meticulous long-term clinical and radiologic follow-upwill be critical for determining local recurrence and cancer-free survivalrates, to establish the ultimate role of renal cryoablation in the manage-ment of small renal tumors.
# 2007 European Association of Urology and European Board of Urology.
Published by Elsevier B.V. All rights reserved.
* Corresponding author.E-mail address: [email protected] (F.X. Keeley Jr.).
1. Introduction
The American Cancer Society estimates 38,890 newcases and 12,840 deaths from cancer of the kidney in2006. Renal cell carcinoma (RCC) represents almost85% of all newly diagnosed malignancies of thekidney, occurring at a rate of 4.4 to 11.1/100,000
1871-2592/$ – see front matter # 2007 European Association of UroloPublished by Elsevier B.V. All rights reserved.
person years. Recent data from the United StatesSurveillance, Epidemiology and End Results pro-gram demonstrate a steady increase in the rate ofrenal cell carcinoma between 1975 and 1995 [1].
Historically, a large percentage of new renalcancer cases were diagnosed with metastases.Widespread application of imaging modalities, has
gy and European Board of Urology. doi:10.1016/j.eeus.2007.05.001

e a u - e b u u p d a t e s e r i e s 5 ( 2 0 0 7 ) 2 0 6 – 2 1 8 207
led to a dramatic increase in the incidental detectionof renal tumors [2–5]. The incidentally detected renalcell cancers tend to be smaller in size, and thesetumors have an improved prognosis. This increasein the diagnosis of tumors smaller than 3 cm overthe past 20 years may be partially attributable toearly detection through widespread use of non-invasive techniques, though this alone cannotexplain the upward trend [5]. The increases aremost notable among persons aged 65 to 84 years andwere generally least pronounced among individualsolder than 85 years.
Historically, most patients have been treated withradical nephrectomy [6]; however, in the manage-ment of small tumors in the last decade, there hasbeen a trend away from radical nephrectomy towardnephron-sparing surgery.
Nephron-sparing surgery, initially developed forpatients with solitary kidneys or compromised renalfunction, is emerging as a viable treatment optionfor renal tumors smaller than 4 cm, even in the non-imperative setting, and is considered the treatmentof choice by some authorities. Three factors havebeen associated with this phenomenon. Firstly, itwas demonstrated that patients undergoing radicalnephrectomy suffer a greater degree of renalcompromise than patients undergoing partialnephrectomy [7]. Preservation of nephrons has beensuggested to be protective against hyperfiltrationinjury with resultant superior long-term global renalfunction. Secondly, several large studies with long-term follow up of conservative treatment of renaltumors <4.5 cm demonstrated no increase in therisk of recurrence [8,9]. These tumors have areportedly slow growth rate (0.35 cm/year) and lowmetastatic potential, with up to 22% of these tumorsbeing benign on final pathology. Thirdly, a contral-ateral renal tumor may develop metachronously inup to 4% to 15% of radical nephrectomy cases [8].
Several minimally invasive nephron-sparing pro-cedures are being advocated for select patients witha small renal tumor, promising comparable onco-logic control while decreasing operative morbidity.Laparoscopic surgery includes extirpative (laparo-scopic partial nephrectomy) and a variety of ablativeprocedures. Laparoscopic partial nephrectomy is atechnically challenging procedure that requiresconsiderable laparoscopic dexterity and time-sen-sitive intracorporeal suturing [10]. Ablative tech-niques include a variety of treatment methods,where the tissue is destroyed in situ rather than bysurgical extirpation. These technologies includecryosurgery, radiofrequency ablation, microwavethermotherapy, interstitial laser, and interstitialphoton radiation. The objective behind these
approaches, besides oncological efficacy and spar-ing renal function, is to decrease pain, morbidity,and hospital stay [10].
2. Natural history of small renal tumors
Renal cell carcinoma represents a single entity witha variety of histological appearances. The mostcommon subtypes of RCC include conventional(clear cell), papillary and chromophobe. RCC is mostcommonly discovered in the seventh decade of life[11], and therefore many patients are older and havesignificant co-morbid disease with an increased riskof perioperative mortality and morbidity. Althoughmorbidity from nephrectomy, whether open orlaparoscopic, has decreased with improved tech-niques, it is still significant and reported in 11% to40% of cases [12,13].
In selected patients, particularly the elderly, or inthe presence of significant co-morbidities, expec-tant management may be a reasonable option [7,8].In retrospective studies, Bosniak et al suggested thattumors less than 3.5 cm in diameter rarely metas-tasize and have a slow growth rate, suggesting a rolefor active surveillance with possible delayed interventionin these patients [3]. Metastases were not reportedfor tumors of this size at nephrectomy. Further-more, Bosniak et al described the growth rate of renaltumors as a mean of up to 0.36 cm per year change indiameter on serial imaging. Most tumors showedlittle or no change in diameter with a smallproportion accounting for most of the growth. Theyhypothesized that these same fast growing tumorsare those that are not curable, even with earlydetection and removal.
In contrast, Oda et al retrospectively reviewed therecords of 16 patients with a mean tumor size of 2 cmwhose lesions were found incidentally and who didnot undergo immediate surgical treatment for solidrenal tumors that were later proven to be RCC [14].They found that the median growth rate of primarylesions was 0.54 cm (range 0.10 to 1.35 cm/year,significantly higher than those reported by Bosniaket al). This may be due to the difference inclinicopathologic features of the patients involvedin the two studies. While the study by Bosniak et alincluded oncocytoma and unknown renal tumors,Oda et al included patients with histologically-proven RCC. Oda et al concluded that candidates forwatchful waiting should be selected very carefully, asthe clinical behavior of renal tumors cannot bepredicted. The implication of this is that the standardpractice of immediate partial or radical nephrectomyin the elderly would need to be reviewed.

e a u - e b u u p d a t e s e r i e s 5 ( 2 0 0 7 ) 2 0 6 – 2 1 8208
Given the natural history of these small renaltumors in the context of strategies aimed at tumorsurveillance, patient selection for active surveil-lance with possible delayed intervention should bebased on a combination of patient co-morbidity aswell as tumor size. The heterogeneity of growth ofrenal tumors dictates that long-term radiographicfollow-up is mandatory.
3. Renal tumor ablation
Ablation of renal tumors has emerged as a viablealternative to resection for local control when partialor complete nephrectomy is undesirable [15]. Animportant aspect in the management of thesetumors is the eradication of neoplastic tissue withpreservation of as much of the adjacent normaltissue as possible.
There are several clinical scenarios where abla-tion may be preferable to resection. In patients likelyto have multiple renal tumors in their lifetime, suchas those with von Hippel-Lindau disease, a mini-mally invasive approach is essential in balancingmanagement of the underlying disease, maintainingquality of life and preserving kidney function. Asstated earlier, the majority of small renal tumors areslow growing tumors, and a less invasive proceduremay be preferable in elderly patients or those withmultiple co-morbidities, as they present a signifi-cant operative risk.
The two ablation modalities that are currentlyclinically viable are cryotherapy and radiofrequencyablation (RFA). These two ablation modalitiesremain early in their development. The mechan-isms of tissue destruction associated with thesetechniques are very different and the best methodfor ablation of renal tumors remains unknown.High-intensity focused ultrasound, microwave ther-motherapy and laser interstitial thermal therapyhave only been tried in animal models or smallpilot studies, thus making any assessment of theirvalue premature. These ablative modalities remainexperimental and should not be used clinicallywithout approved investigational protocols.
4. Renal cryoablation overview
The principle of cryoablation for renal tumors isderived in part from previous experience withcryotherapy for hepatic lesions. The clinical settingof RCC is markedly different, however, as the vastmajority of patients have resectable, curable diseaseand the renal parenchyma is different in its nature
and vascular supply. In using ablation in themanagement of these patients, careful patientselection is warranted, especially until long-termfollow-up is available. With the introduction ofnewer and more sophisticated cryosurgical equip-ment, there has been increasing interest in thewider clinical application of these techniques,particularly in the management of renal tumors.The development of sensitive and sophisticatedimaging modalities, such as intraoperative laparo-scopic ultrasound (IOLUS) for intraoperative mon-itoring, as well as magnetic resonance imaging (MRI)and computerized tomography (CT) for postopera-tive surveillance, has also been important to therenewed interest in renal cryotherapy.
Various clinically-relevant cryogens are available.The boiling point of each of these cryogens deter-mines the nadir temperature that the specificcryoprobe can produce. Liquid argon and liquidnitrogen, the two most commonly used cryogens,have boiling points of �186 8C and �196 8C respec-tively. In addition to the type of cryogen, the physicaland thermal characteristics of a cryolesion alsodepend on the size and area of contact of thecryoprobe, and the rapidity of freezing. Early clinicalexperience with renal cryoablation incorporated theinsertion of a single 3 to 5 mm cryoablation probe.Recently 17 gauge (1.47 mm) cryoprobes have beenintroduced that incorporate a modified heatexchange mechanism [16]. Larger cryoprobes typi-cally result in larger ice balls because of increasedcirculation of the cryogen. Smaller cryoprobesminimize the risk of significant bleeding and allowthe surgeon to shape the ice ball if one dimension ofthe ablation does not seem adequate.
To achieve the goal of reliable cancer cell ablation,cryosurgery should be carried out for small renaltumors (i.e., less than 3 cm). This tumor shouldideally be located away from the major renal bloodvessels, which can interfere with the coolingprocess; however, cryoablation can be carried outfor a tumor abutting the collecting system, whichappears to heal well following freezing. For a larger(>4 cm) tumor, a significantly larger ice ball isnecessary, requiring the use of more cryoprobes,which increases not only the technical complexity ofthe procedure but also the potential for inadequatecryoablation, leaving residual viable cancer cells.Previous ipsilateral renal surgery is a relativecontraindication for renal cryosurgery.
4.1. Renal cryoablation: Experimental studies
Freezing and thawing tissue results in completetissue necrosis within well-defined parameters.

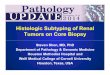
Fig. 1 – Cryo-probe temperature diagram demonstrating
isotherms.
e a u - e b u u p d a t e s e r i e s 5 ( 2 0 0 7 ) 2 0 6 – 2 1 8 209
Experimental studies have helped characterize theprocess of cryoablation and have provided impor-tant guidelines for clinical renal cryotherapy. Inves-tigations in animal models have demonstrated thatrenal cryoablation produces predictable and repro-ducible tissue destruction [17]. On the tissue level,cryoablation causes tissue necrosis by the deposi-tion of intracellular and extracellular ice, an eventthat leads to the disruption of the cell membrane,organelles, proteins and local microvasculature. Inaddition, there is an increase in intracellularosmolarity that adds further injury. Eventually,these changes lead to coagulation necrosis followedby fibrosis and scarring. In swine, it has beendemonstrated that complete renal tissue ablationoccurred at temperatures of�19.4 8C [18]. For cancercells, however, lower temperatures may be requiredand a temperature of�40 8C has been recommendedto ensure cancer cell death.
Baust et al found that a temperature of �40 8C isfound 5–6 mm inside the edge of the forming ice ball[19]. This suggests that extension of the ice ball 1 cmbeyond the tumor edge would ensure adequatetumor ablation. Damage to the vasculature withinthe ice ball causes hyperpermeability of the micro-vasculature, resulting in thrombosis, vascular occlu-sion, regional tissue ischemia, and edema leading todelayed cell death [20]. In vitro studies have shownthat induced apoptosis may also play a role [21]. It isimportant to note that cryotherapy injures not onlyindividual cells at the time of therapy (directdamage) but also the tissue as a whole by impairingthe microvasculature (indirect damage). The indir-ect damage is noted over the ensuing days andmonths.
Two types of cell thaw have been described: apassive or active thaw. Cell thaw and a second freezecycle enhances further tissue destruction; the thawmay be carried out in an active fashion with heliumgas or entirely passively, i.e., a slow thaw. Wooleyet al. [22] compared lesion size as well as volumes ofconfluent necrosis resulting from combinations ofsingle and double freeze-thaw cycles with active andpassive thaws. This study found no differencebetween use of an active and passive thaw. Mostinvestigators, however, recommend a slow thaw,arguing that this allows faster recrystallization tooccur, enhancing direct cell damage [15,23,24]. Thecryobiology literature defines a slow thaw asapproximately 20 8C/min and a fast thaw asapproximately 200 8C/min [25]. Slow thawing ofthe frozen tissue is thought to be a prime destructivefactor and is done by allowing the tissues to thawwith no assistance from heating. The longer theduration of the thaw, the greater the damage to cells
because of the solute effects, ice crystal restructur-ing (recrystallization), prolonged oxidative stressand growth of ice crystals [23]. The mode of icecrystal growth is greatest at �15 to �40 8C andespecially �20 to �25 8C.
Cellular survival depends not only on the freezingand thawing rates but also, most importantly, uponthe lowest temperature reached and the hold time atsubzero temperatures [23]. Experimental modelsshow that over 90% of renal cell carcinoma cellssurvived temperatures above �10 8C, but only 15%survived temperatures of �20 8C [24]. Other studies,using a single-freeze cycle and monitoring tissuewith thermosensors have shown complete celldeath at temperatures below �19.4 8C. The dual-freeze technique, however, increases physicaldamage to tumor cells, and a passive thaw mayhelp to maximize tumor destruction.
Although the temperature at the tip of thecryoprobe (core temperature) is �145 8C to �190 8C,depending upon the cryogen used, there is anincremental increase in temperature as one proceedsradially outwards, with the temperature at the visibleedge of the ice ball being 0 8C. Campbell et al. [26]confirmed that the critical lethal temperature of�19.4 8C was uniformly achieved at a distance of3.1 mm inside the visible margin of the ice ball (Fig. 1).This requires the ice ball to extend at least 3.1 mm

e a u - e b u u p d a t e s e r i e s 5 ( 2 0 0 7 ) 2 0 6 – 2 1 8210
beyond the visible margin of the tumor to achieveuniform destruction of all viable tumor cells.
Weld et al. [16] recently characterized the size andshape of the ablated area as well as the surroundingintermediate zone associated with single and multi-ple rod configurations in a porcine model. Theyfound that the average distance of complete tissueablation beyond the tip of the rod was 4 mm and thatthe intermediate zone around the tip of the rod wasconsistently thinner compared to the width mea-sured on cryolesion cross-sections (1.5 vs. 3 mm). Asanticipated, there was complete tissue destructioncentrally with viable renal cells found only in theintermediate zone. To ensure adequate treatment inclinical use, it is therefore recommended that the iceball be extended 1 cm beyond the tumor margin[16,27]. This may be confirmed by direct laparoscopicobservation superficially and with intraoperativeultrasound guidance for deeper components of thetarget lesion.
The histologic sequelae of renal cryoablation showcharacteristic features of necrosis. At 1 hour, grossexamination demonstrates a well-defined area ofdark red, interstitial hemorrhage with an abrupt lineof demarcation. On light microscopy, generalizedvascular congestion is evident with only subtle signsof early coagulation necrosis. Electron microscopyshows marked ultrastructural evidence of irrever-sible cell death, with chromatin condensation, lossof nuclear membranes and thrombi in almost allglomerular capillaries [28]. At 24 hours, on lightmicroscopy, a well-defined central area of completecoagulative necrosis with a surrounding area ofpartial necrosis is seen [17]. The area of completenecrosis is characterized by loss of cell borders,nuclear pyknosis, absence of cytoplasmic orga-nelles, and ghost renal tubules. The zone of partialnecrosis contains some viable cells, thus represent-ing an area of sublethal injury. On electron micros-copy, tubular cells appear as proteinaceousaggregates, completely devoid of membranes. Glo-meruli are degenerated, and glomerular spaces arefilled with necrotic cellular debris [28]. At 1 month,microscopic examination reveals chronic inflam-mation, fibrotic glomeruli and tubules, hemosiderindeposition, and necrosis with no evidence of viablerenal parenchyma. Fibrosis, scarring and collagendeposition of the mature infarct zone ensue,resulting in the telltale contracted scar typical ofthe chronic, long-term renal cryolesion [28].
4.2. Renal cryoablation: Clinical experience
Renal cryotherapy can be performed open, lapar-oscopically or percutaneously. It appears that the
three approaches offer similar results as long as thetumor can be successfully localized and the probeinserted safely. The preferred approach may ulti-mately depend on the location of the tumor and usercomfort level with the different imaging modalities.
In 1996, Delworth and colleagues [29] reported theearliest series of renal cryoablations in humansubjects with solitary kidneys. These early serieswere performed via an open approach, and renalparenchymal preservation around the tumors aswell as good renal function was noted.
In 1998 Gill et al. [30] performed cryoablation usingthe laparoscopic technique in an initial series of 10cases. The laparoscopic approach has the advantage oflimiting the perioperative morbidity associated witha flank incision while permitting the dual control ofdirect laparoscopic visualization and ultrasono-graphic monitoring to ensure the creation of anadequate ice ball. The anatomic location of the tumoron the kidney determines the laparoscopic approach:posterior tumors are preferably approached retro-peritoneoscopically and anterior and anterolateraltumors transperitoneally.
Gill recently reported on 56 patients each with a3-year follow-up [31]. They noted that the cryole-sions decreased in size by 75% and completelydisappeared in 8%, while needle biopsy confirmedlocally persistent/recurrent tumor in 5.6%. Renalfunction was not compromised and surgical com-plications were minimal. Three-year cancer specificsurvival in 51 patients undergoing cryotherapy for aunilateral, sporadic tumor was 98%.
Schwartz et al. [32] recently reported on 85consecutive patients with an average age of67 years and a mean tumor size of 2.6 cm. Seventycases were treated laparosopically, of which sevenwere converted to the open approach. Theseconversions were early in the authors experienceand were due to failure of progression because ofinadequate exposure or tumor inaccessibility. Aminimum of 3-month follow-up was available on atleast 55 patients. One patient had a suspicious lesionon CT and MRI at the cryosite 12 months after theprocedure was performed. A subsequent needlebiopsy of the lesion revealed RCC, and a radicalnephrectomy was performed. Post cryoablationmean creatinine levels were identical to pre-surgerylevels. The authors concluded that laparoscopiccryoablation was safe with minimal morbidity.
Percutaneous cryoablation is also an option fortreatment of selected small renal tumors. MRI,CT fluoroscopy and real time ultrasound have allbeen used to facilitate needle placement and tomonitor progression and development of thecryolesion.

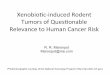
Fig. 2 – Placement of cryoablation needles into 2.8 cm right
anterior renal tumor.
Fig. 3 – Ice ball forming. Note laparoscopic ultrasound probe
positioned posterolaterally to monitor depth of ice ball and
thermocouples to monitor temperature in the center and
at the edge of tumor.
e a u - e b u u p d a t e s e r i e s 5 ( 2 0 0 7 ) 2 0 6 – 2 1 8 211
Uchida first described percutaneous cryotherapyin 1996 in two patients with metastatic RCC [33].Although both patients had metastatic disease atpresentation and died within 10 months of treat-ment, the authors noted shrinkage in size of thelesion and symptomatic improvement. Recently,Shingleton [34] reported on 55 patients undergoingMRI-guided percutaneous cryoablation of renaltumors less than 4 cm in size. With a meanfollow-up of 18 months, 51 showed completeregression; however, 7 (14%) required more thanone treatment session owing to incomplete initialtumor ablation. Two patients had local residualdisease, and four died of non-renal disease. Nocomplications were reported intraoperatively, withone patient requiring a transfusion postoperatively.
Several recent series [35–37] have subsequentlyconfirmed that percutaneous cryoablation is areasonable and safe option for the management ofsmall renal tumors. The image guidance necessaryfor the percutaneous approach is a limitation formost urologists, however, as the approach com-monly requires use of CT fluoroscopy or, rarely, anopen MRI scanner. The procedures can be done byurologists in collaboration with interventional radi-ologists in the execution of these modalities fortreating small renal tumors. Since the entire probe iscooled, care must be taken to avoid cryo-injury tosensory nerves at the body surface.
4.3. Renal cryoablation: Laparoscopic technique
The essential technical steps during laparoscopicrenal cryoablation include complete mobilization ofthe kidney within Gerota’s fascia, excision of theperirenal fat overlying the tumor for histopathologicevaluation, in situ ultrasound imaging of the tumorand the remainder of the kidney, needle biopsy ofthe tumor, puncture cryoablation, and confirmationof hemostasis.
During laparoscopic renal cryoablation, intra-operative laparoscopic ultrasound (IOLUS) is areliable and vital imaging technique [38]. Onikinitially characterized the ultrasound appearancesof the developing cryolesion in an animal model [39].The IOLUS utilizes a flexible, steerable, color Dopplerultrasound probe. On IOLUS the renal tumors aremildly hyperechoic or have a mixed echogenicity,and the hyperechoic renal sinus fat is clearlyvisualized. By placing the IOLUS probe on thesurface of the kidney opposite the tumor, preciseadvancement of the tip of the cryoprobe up to thedeep margin of the tumor and adequate visualiza-tion of the leading edge of the ice ball as it obliteratesthe tumor margins can be achieved. The advancing
front of the ice ball is seen as a hyperechoic rim withpost-acoustic shadowing. The leading edge of the iceball can be visualized on laparoscopic ultrasound toconfirm that it advances approximately 1 cmbeyond the margins of the tumor. This margin isimmediately apparent laparoscopically as well(Figs. 2–4). This is important, as animal modelshave shown that the target temperature occurswithin a few millimeters of the edge of the ice ball asseen on ultrasound; the actual zone of completeablation (lethal ice) is a few millimeters smaller thanthe ice ball [22]. Several studies have corroboratedthis finding and have suggested that the ice balltends to over represent the actual area of ablation.

Fig. 4 – Ice ball fully formed with margin of 1 cm beyond
edge of tumor.
Fig. 5 – CT scan showing anterolateral tumor of left kidney.
Note proximity of bowel to tumor.
e a u - e b u u p d a t e s e r i e s 5 ( 2 0 0 7 ) 2 0 6 – 2 1 8212
Laparoscopy, though more invasive than thetranscutaneous approach, provides better image ofthe ice ball and permits the kidney to be manipulatedonce it has been exposed, thereby protecting adjacentorgans and ensuring adequate tumor ablation.Anterior tumors (Fig. 5) are typically located adjacentto bowel, while lower pole tumors may lie adjacent tothe ureteropelvic junction.
4.4. Renal cryoablation: Percutaneous technique
Percutaneous cryoablation (PRC) offers the leastinvasive method of performing renal cryoablation.PRC may be performed on an outpatient basis, withthe patient under minimal conscious sedation [37].Ultrasound, open gantry MRI and CT scanning are
the currently available modalities for image guid-ance for PRC. Ultrasound guidance was described inthe first clinical application of PRC by Uchida et al.[33]. Ultrasound provides the advantage of readyavailability and low cost, the capacity for real timeguidance of needle placement with non-axial andoblique imaging, and the absence of ionizingradiation. Ultrasound, however, is operator depen-dent, offers less precise visualization of the ice balledge, and provides limited resolution in obesepatients [36]. Open gantry MRI consists of 2 verticalcylinder-shaped magnets with a bore. The surgeonsteps between the vertical magnets on either side ofthe bore to approach and treat the patient. Thisallows a direct hands-on approach with instrumentsintroduced percutaneously. MRI yields 3-dimen-sional pictures that are of greater clarity anddefinition, crisp resolution of the ice ball, dynamicimaging that may be reconstructed in multipleplanes, lack of ionizing radiation and the capacityto provide clinically useful follow-up images [34].Open gantry MRI systems, however, are presentlyexpensive and not widely available.
Reiser et al. [40] first indicated that CT may be auseful continuous monitoring technique for PRC. CTguidance is currently the method of choice forintraprocedural monitoring of PRC because it pro-vides clear visualization of the ice ball and distin-guishes it well from neighboring structures, such asbowel. Overall, the advantages of CT are that it isreadily available, offers excellent visualization ofthe ice ball and critical neighboring structures, andprovides real-time guidance in the CT fluoroscopymode. A major disadvantage, however, is theconsequent high radiation dose to which patientsand cryosurgeons are exposed during real-timefluoroscopy [41]. Radiation protection measuresmust, therefore, be taken for these individuals; thisis not a concern with MRI or ultrasound. Additionalchallenges may arise in cases where oblique anglesmay be difficult to achieve or when intraparen-chymal lesions are not visible on non-contrastimages. Finally, the gantry may interfere withoptimal probe placement. However, this obstaclehas been partially overcome by the use of newerright-angle probes.
4.5. Renal cryoablation: Complications
Complications following laparoscopic renal cryoa-blation include bleeding and injury to adjacentorgans. Several reports have noted that the integrityof some structures is not compromised by exposureto cryogenic temperatures. The renal collectingsystem recovers well after cryosurgery even when

Table 1 – Comparison of perioperative morbidity in various series of renal cryosurgery
References Mean age(yr)
No ofpts.
Mean tumorsize (cm)
Mean operativetime (h)
Blood loss(ml)
Hospitalstay
Complicationrate
Conversionrate
Moon et al, 2004 [43] 61 16 2.6 3.1 40 1.9 6% 6%
Schwartz et al, 2006 [32] 67 70 2.6 N/A 58 3 4% 10%
Cestari et al, 2004 [44] 64 34 2.5 1.9 165.3 3.8 20% 0
Gill et al, 2005 [31] 65.2 56 2.3 3 65.2 1.7 4% 0
e a u - e b u u p d a t e s e r i e s 5 ( 2 0 0 7 ) 2 0 6 – 2 1 8 213
exposed to very low temperatures, unless it isphysically punctured with a probe [42]. Inadvertentcontact of the active cryoprobe or ice ball withsurrounding viscera, however, may cause signifi-cant complications. Complete bowel obstruction,ileus, ureteropelvic junction obstruction and pan-creatic injury have all been described [9,15,26].
Post-operative hemorrhage is less common withcryoablation as compared to laparoscopic partialnephrectomy (see Table 1). Carvalhal et al. [45]reviewed 22 patients who were followed aftercryoablation for a mean of 20.6 months. Nosignificant differences were noted in their pre-operative and postoperative serum creatinine levelsor systolic and diastolic blood pressure values. Amulti-institutional review showed that, followingcryoablation, major and minor complications were1.4 and 12.2% respectively [46].
4.6. Renal cryoablation: Follow-up
There is no consensus algorithm for monitoringpatients radiographically in follow-up after renalcryoablation. The radiologic hallmark of successfulrenal cryoablation is lack of enhancement oncontrast-enhanced CT or MRI. Lesions typically donot disappear for many months or even years butshould progressively decrease in size. Weld et al.[47] recently reported their 3-year experiencewith laparoscopic renal cryoablation. The authorsreported that the ablation zones initially increasedin size by 52% on postoperative day 1 and thensteadily decreased to the original tumor size by6 months after surgery. The ablation zone was notedto shrink on average by 71% relative to the originaltumor size at the three year follow-up period. Werecommend a follow-up protocol of CT or MRI scansat three months and one year.
It is important to note that adherence to therecommended radiologic follow-up protocol may bemixed. Davol et al. [48] recently reported long-termresults on a series of 48 patients followed after renalcryoablation. They found that once the treatedrenal tumor appeared resolved radiologically bothpatients and physicians became less attentive tothe recommended follow-up protocol. Radiologic
appearance of a renal lesion treated with cryoabla-tion is complex, however, and as long as 12 to24 months is required for disease persistence to bedetermined. Failure of a lesion to decrease in size, orany enhancement, mandates further intervention,which may include renal biopsy, repeat cryoabla-tion, partial nephrectomy or radical nephrectomy.
Several studies with intermediate follow-up havedemonstrated safe and effective treatment of smallrenal tumors, as documented by radiographicfollow-up and/or post-treatment needle biopsy[49,50]. It is important to realize, however, thatsalvage or repeat procedures may be required in upto 12.5% of patients [48]. Therefore, individualpatients must provide full informed consent regard-ing the potential for additional procedures andmonitoring relative to other extirpative proceduressuch as laparoscopic partial nephrectomy. A limita-tion of radiographic follow-up is the risk of falsenegative imaging results. Also, negative renal biopsyresults may not be completely reassuring. Tumorcytology is often indeterminate, even in the hands ofan experienced cytologist. Nevertheless, it repre-sents a viable attempt to obtain histopathologic datain a minimally invasive manner in patients who areotherwise doing well from a clinical and radiologicalstandpoint. Ethically, it may be difficult to justify amore thorough laparoscopic or open renal biopsy inpatients with decreasing tumor sizes on follow-upscanning. This underscores the need for meticulouslong-term (at least 10 year) radiological monitoringfollowing renal cryoablation.
5. Other minimally invasive modalities
Laparoscopic partial nephrectomy (LPN) may be per-formed either transperitoneally or retroperitoneally.Despite advanced laparoscopic techniques, LPNposes several challenges, LPN has a steep learningcurve and a high complication rate (up to 50%), withconversion to open surgery in up to a third of cases[51], possible renal injury caused by warm ischemia[52,53], urine extravasation due to late necrosis ofthe coagulated surface [53] and delayed bleeding[54]. LPN offers a more definitive oncological

Table 2 – Comparison of various series of Laparoscopic partial nephrectomy
References No ofpts.
Tumorsize(cm)
Conversionrate
Meanoperativetime (h)
Bloodloss(ml)
Complicationrate
Warmischemia
time (min)
Tumormarginstatus
Yoshikawa et al 2005 [55] 17 2.5 6 4.5 301 24 25 All negative
Kim et al 2003 [56] 79 2.5 3 3.03 391.2 15 26.7 2 positive
Gill et al 2005 [57] 100 3.7 0 3 270 16 27.8 All negative
Simon et al 2003 [58] 19 2.1 0 2.2 120 21 N/A All negative
e a u - e b u u p d a t e s e r i e s 5 ( 2 0 0 7 ) 2 0 6 – 2 1 8214
outcome than cryoablation, albeit with a slightlyhigher major complication rate, longer hospital stay,and greater blood loss (Table 2). These results arehighly dependent on the surgeon’s experience –laparoscopic partial nephrectomy is among themost challenging surgical procedures.
Radiofrequency ablation (RFA) works by convertingRF waves into heat, resulting in thermal damage toparenchymal tissue [53,60]. When the temperatureof tumor cells increases to >70 8C there is directcytological destruction [53]. Zlotta and colleaguesfirst described RFA for renal tumors [59]. Severalproblems associated with RFA exist, includingintraprocedural radiofrequency interference of theultrasound images, even with shielding the USprobe, irregularly shaped lesions of variable sizethat make it challenging to ensure consistentablation of tumors without injuring sizable portionsof normal parenchyma or surrounding structures.The most significant concern regarding RFA is thefinding of ‘skip lesions’ of viable tissue in some RFAstudies [61–63]. Although RFA has low short-termmorbidity, the data from these studies (see Table 3)suggests that RFA at this time remains unprovenuntil consistent and reproducible long-term onco-logical efficacy is demonstrated.
Newer energy sources for tumor ablation includehigh intensity focused ultrasound, laser, and micro-wave coagulators. Theoretic and experimentalevidence suggests that the primary mechanism oftissue destruction by high intensity focused ultrasound(HIFU) is thermo-necrosis. HIFU generates beams ofthe required frequency region of a few MHz byresonant electrical excitation of the thin plates of apiezoceramic. Intersitial laser ablation is another
Table 3 – Comparison of various series of renal radiofrequenc
References Approach No. of pts.(No. tumors)
Gervais et al 2003 [64] PC 55
Roy-Choudhury 2003 [65] PC 8
Su et al 2003 [66] PC 29
Farrell et al 2003 [67] PC 20
Matsumoto et al 2004 [68] LP & PC 64
PC = percutaneous; LP = laparoscopic.
emerging thermoablative minimally invasive moda-lity that has been investigated as a treatmentoption for a variety of neoplasms, including thebrain and breast [69,70]. Interstitial laser ablationutilizes optical fibres to deliver a high-energy laserto the target lesion. MR imaging is used both forthe placement of the laser in the tumor andfor monitoring progress of the thermocoagulation.Though interstial laser ablation is an emergingtechnique, evidence of viable cells within treat-ment zone of benign parenchyma of an animalmodel mandates further refinement of the techni-que before further application in humans [70].Microwave thermotherapy utilizes microwaves in the300–3000 MHz range of the electromagnetic spec-trum [71]. These waves interact with tissue andproduce heat. The depth of tissue penetration isinversely related to the frequency and the watercontent of the targeted tissue. The initial report ofmicrowave therapy in renal tissue was made byHradec [72] in 1969. There have, however, been veryfew reports on its effectiveness since then. Kigureet al. [73] reported on its application on a tumormodel in rabbit kidneys and found no difference inthe survival between rabbits treated with laparo-scopic microwave therapy and those undergoingopen nephrectomy. These reports are encouraging,but further investigation is required to confirm theclinical utility of this modality.
6. The role of needle biopsy
Needle biopsy is essential in the diagnosis of renaltumors and should no longer be a source of
y ablation
Mean tumorsize (cm)
Mean follow-up(months)
Successrate
3.2 13.2 100%
3 17.1 88%
2.2 9 94%
1.7 9 100%
2.3 13.7 98.5%

e a u - e b u u p d a t e s e r i e s 5 ( 2 0 0 7 ) 2 0 6 – 2 1 8 215
continuing controversy. At our institution, needlebiopsy is performed under laparoscopic guidanceimmediately before the ablation procedure. Biopsyresults are used primarily to guide the intensity offollow-up [74]. A substantial number of biopsies areread as non-diagnostic by the pathologist on finalhistologic analysis. We treat these cases as RCCunless proven otherwise and maintain the samefollow-up regimen as in patients with biopsy provenmalignancies.
The argument has been made that a biopsy maytheoretically cause seeding or implantation; triggersignificant bleeding, particularly as a result ofneovascularization; and prove indeterminate [75].Clinical parameters, especially with modern ima-ging techniques, it is argued, are accurate enough inthe vast majority of cases to make a definitivediagnosis.
Despite these limitations, we believe that needlebiopsy represents the standard of care, given thatonly histology can provide a definitive diagnosis. Inthe largest series to date, Gill et al. [31] reportedthat intraoperative precryoablation needle biopsyconfirmed renal cell carcinoma in 36 of 56 patients(64%), oncocytoma in 6 (11%) and benign tissuein 12 (21%). For renal tumors less than 3 cm indiameter, one would expect this proportion ofbiopsies to show renal cell carcinoma, given that68% of small renal tumors in modern laparoscopicpartial nephrectomy series [10] are found to containRCC. One must assume, therefore, that not everysmall renal tumor is malignant. Biopsy results arevery useful in guiding follow-up, given that con-ventional clear cell RCC has a significantly worseprognosis than other histologic subtypes; however,frozen section evaluation of intraoperative needlebiopsy samples is not generally considered anecessary prerequisite to proceeding to renalcryoablation.
7. Conclusion
In conclusion, initial experience with laparoscopicrenal cryoablation suggests that it is a safe andfeasible technique, with minimal patient morbidityand excellent short-term efficacy. Laparoscopicrenal cryoablation has definite advantages com-pared to partial nephrectomy in that there is lessblood loss, it does not involve hilar clamping andwarm ischemia, does not involve technically diffi-cult reconstructive technique, does not result inurine leaks, and decreases the need for ureteralstenting. It also offers advantages compared topartial nephrectomy in that it is easier to treat less
exophytic tumors because of ultrasonic monitoringof the ice ball. Partial nephrectomy has advantagesin that its margin status is known and follow-upbiopsy is unnecessary.
Although cryodestruction of a renal tumor can beperformed in a well-monitored and reproduciblefashion, longer follow-up is needed before the trueefficacy of this procedure can be determined.Meticulous follow-up with serial radiographic imag-ing of the cryoablated site is imperative, and anyevidence of either enlargement or absence ofreduction in the size of the cryoablated tumorshould be investigated with a needle biopsyor laparoscopic or open exploration. Preliminaryexperimental data into renal RFA have identifiedviable tumor cells within a treated lesion, castingdoubts regarding the efficacy of the procedure.Based on the available data, RFA at this time cannotbe recommended as a first line treatment modality.
References
[1] Hock LM, Lynch J, Bajali KC. Increasing incidence of all
stages of kidney cancer in the last 2 decades in the United
States: an analysis of surveillance, Epidemiology and end
results program data. J Urol 2002;167:57–60.
[2] Motzer RJ, Bander NH, Nanus DM. Renal cell carcinoma.
N Engl J Med 1996;335:865–75.
[3] Bosniak MA. Observation of small incidentally detected
renal tumors. Semin Urol Oncol 1995;13:267–72.
[4] Homma Y, Kawabe K, Kitamura T, et al. Increased inci-
dental detection and reduced mortality in renal cancer:
Recent retrospective analysis at eight institutions. Int J
Urol 1995;2:77–80.
[5] Jayson M, Sanders H. Increased incidence of serendipi-
tously discovered renal cell carcinoma. Urology 1998;51:
203–5.
[6] Robson CJ. Radical nephrectomy for renal cell carcinoma.
J Urol 1963;89:37–42.
[7] Lau WKO, Blute ML, Weaver AL, Torres VE, Zincke H.
Matched comparisons of radical nephrectomy vs.
nephron sparing surgery in patients with unilateral renal
cell carcinoma and a normal contralateral kidney. Mayo
Clin Proc 2000;75:1236–42.
[8] Fergany AF, Hafez KS, Novick AC. Long-term results of
nephron sparing surgery for renal cell carcinoma; 10-year
follow-up. J Urol 2000;163:442–5.
[9] Lee CT, Katz J, Shi W, Thaler HT, Reuter VE, Russo P.
Surgical management of renal tumors 4 cm. or less in a
contemporary cohort. J Urol 2000;163:730–6.
[10] Gill IS, Desai MM, Kaouk JH, et al. Laparoscopic partial
nephrectomy for renal tumor: duplicating open surgical
techniques. J Urol 2002;167:469–76.
[11] Katz DL, Zheng T, Holford TR, Flannery J. Time trends in
the incidence of renal cell carcinoma: analysis of Con-
necticut Tumor Registry data, 1935–1989. Int J Cancer
1994;58:57–63.

e a u - e b u u p d a t e s e r i e s 5 ( 2 0 0 7 ) 2 0 6 – 2 1 8216
[12] Lerner SE, Hawkins CA, Blute ML, et al. Disease outcome
in patients with low stage renal cell carcinoma treated
with nephron sparing or radical surgery. J Urol 1996;155:
1868–73.
[13] Licht MR, Novick AC. Nephron sparing surgery for renal
cell carcinoma. J Urol 1993;149:1–7.
[14] Oda T, Miyao N, Takahashi A, Yanase M, Masumori N, Itoh
N, et al. Growth rates of primary and metastatic lesions of
renal cell carcinoma. Int J Urol 2001;8:473–7.
[15] Desai MM, Gill IS. Current status of cryoablation and
radiofrequency ablation in the management of renal
tumors. Curr Opin Urol 2002;12:387–93.
[16] Weld KJ, Hruby G, Humphrey PA, Ames CD, Landman J.
Precise characterization of renal parenchymal response
to single and multiple cryoablation probes. J Urol 2006;
176:784–6.
[17] Nakada SY, Lee FT, Warner T, Chossy SG, Moon TD.
Laparoscopic cryosurgery of the kidney in the porcine
model: an acute histologic study. Urology 1998;51(5A
suppl):161–6.
[18] Chosy SG, Nakada SY, Lee FT, Warner TF. Monitoring
renal cryosurgery: predictors of tissue necrosis in swine.
J Urol 1998;159:1370–4.
[19] Baust J, Gage AA, Ma H, Zhang ZM. Minimally invasive
cryosurgery-technology advances. Cryobiology 1997;34:
373–84.
[20] Schinohara S, Carroll PR. Cryotherapy for prostate cancer.
In: Walsh PC, Retik AB, Vaughn ED, Wein AJ, editors.
Campbell’s urology, 8th ed., vol 4, chapter 93. Philadel-
phia: WB Saunders Co.; 2002. p. 3171–81.
[21] Baust JM, Van B, Baust JG. Cell viability improves following
inhibition of cryopreservation-induced apoptosis. In Vitro
Cell Dev Biol Anim 2000;36:262–70.
[22] Wooley ML, Schusinger DA, Durand DB, et al. Effect of
freezing parameters on tissue destruction following renal
cryoablation. J Endourol 2002;16:519–22.
[23] Hofmann NE, Bischof JC. The cryobiology of cryosurgical
injury. Urology 2002;60(suppl 1):40–9.
[24] Baust JG, Gage AA. The molecular basis of cryosurgery.
BJU Int 2005;95:1187–91.
[25] Smith DJ, Fahssi WM, Swanlund DJ, Bischof JC. A para-
metric study of freezing injury in AT-1 rat prostate tumor
cells. Cryobiology 1999;39:13–28.
[26] Campbell SC, Krishnamurthy V, Chow G, et al. Renal
cryosurgery: experimental evaluation of treatment param-
eters. Urology 1998;52:29–34.
[27] Gill IS, Novick AC, Schweizer D, et al. Laparoscopic renal
cryoablation in 32 patients. Urology 2000;56:748–53.
[28] Sindelar W, Javadpour N, Bagley D. Histological and ultra-
structural changes in rat kidney after cryosurgery. J Surg
Oncol 1981;18:363–79.
[29] Delworth MG, Pisters LL, Fornage BD, et al. Cryotherapy
for renal cell carcinoma and angiomyolipoma. J Urol
1996;155:252–4.
[30] Gill IS, Novick AC, Soble JJ, et al. Laparoscopic renal cryoa-
blation: initial clinical series. Urology 1998;52:543–51.
[31] Gill IS, Remer EM, Waleed AH, Strzempkowski B, et al.
Renal cryoablation: outcome at 3 years. J Urol 2005;173:
1903–7.
[32] Schwartz BF, Rewcastle JC, Powell T, et al. Cryoablation of
small peripheral renal tumors: a retrospective analysis.
Urology 2006;68:14–8.
[33] Uchida M, Imaide Y, Sujunoto K, et al. Percutaneous
cryosurgery for renal tumours. Br J Urol 1995;75:132–6.
[34] Shingleton WB, Sewell PE. Renal cryoablation performed
by a percutaneous approach with magnetic resonance
image guidance: 18 and 24-month follow-up. J Urol
2002;167:167, abstract 673.
[35] Harada J, Dohi M, Mogami T, et al. Initial experience of
percutaneous renal cryosurgery under the guidance of
a horizontal open MRI system. Radiat Med 2001;19:291–
6.
[36] Bassignani MJ, Moore Y, Watson L, et al. Pilot experience
with real-time ultrasound guided percutaneous renal
tumor cryoablation. J Urol 2004;171:1620–3.
[37] Gupta A, Allaf ME, Warlick CA, et al. Percutaneous renal
tumor cryoablation under CT guidance: initial clinical
experience. J Urol 2005;173:413, abstract 1526.
[38] Fazio LM, Downey D, Nguan CY, et al. Intraoperative
laparoscopic renal ultrasonography: use in advanced
laparoscopic renal surgery. Urology 2006;68:723–7.
[39] Onik GM, Reyes G, Cohen JK, Poterfield B. Ultrasound
characteristics of renal cryosurgery. Urology 1993;42:
212–5.
[40] Reiser M, Drukier AK, Ultsch B, et al. The use of CT in
monitoring cryosurgery. Eur J Radiol 1983;3:123–8.
[41] Wei J, Sandison GA, Chen L, et al. X-ray CT high-density
artifact suppression in cryosurgery. Phys Med Biol
2002;47:N319–26.
[42] Sung GT, Gill IS, Meraney AM. Effect of intentional cryo-
injury to the renal collecting system. J Urol 2000;163:113,
abstract 493.
[43] Johnson DB, Solomon SB, Su LM, et al. Defining the com-
plications of cryoablation and radio frequency ablation of
small renal tumors: a multi-institutional review. J Urol
2004;172:874–7.
[44] Cestari A, Guazzoni G, dell’Acqua V, et al. Laparoscopic
cryoablation of solid renal masses: intermediate term
followup. J Urol 2004;172:1267–70.
[45] Carvalhal EF, Gill IS, Meraney AM, et al. Laparoscopic
renal cryoablation impact on renal function and blood
pressure. Urology 2001;58:357–61.
[46] Johnson DB, Solomon SB, Su Li-Ming, et al. Defining the
complications of cryoablation and radiofrequency abla-
tion of small renal tumors: A multi-institutional review.
J Urol 2004;172:874–7.
[47] Weld KJ, Figenshau RS, Venkatesh R, et al. Laparoscopic
cryoablation for small renal tumors: three-year follow-up.
Urology 2007;69:448–51.
[48] Davol PE, Fulmer BR, Rustkalis DB. Long-term results of
cryoablation for renal cancer and complex renal tumors.
Urology 2006;68:2–6.
[49] Nadler RB, Kim SC, Rubenstein JN, Yap RL, et al. Laparo-
scopic renal cryosurgery: the Northwestern experience.
J Urol 2003;170:1121–5.
[50] Lee DI, McGinnis DE, Field R, Strip SE. Retroperitoneal
laparoscopic cryoablation of small renal tumors: inter-
mediate results. Urology 2003;61:83–8.

e a u - e b u u p d a t e s e r i e s 5 ( 2 0 0 7 ) 2 0 6 – 2 1 8 217
[51] McDougal EM, Elbahnasy AM, Clayman RV. Laparoscopic
wedge resection and partial nephrectomy—the Washing-
ton University experience and review of the literature.
J Soc Laparoscopic Surg 1998;2:15–23.
[52] Novick AC. Renal hypothermia: in vivo and ex vivo. Urol
Clin N Amer 1983;10:637–44.
[53] Campbell SC, Novick AC, Streem SB, Klein E, Licht M.
Complications of nephron sparing surgery for renal
tumors. J Urol 1994;151:1177–80.
[54] Ramani AP, Desai MM, Steinberg AP, et al. Complications
of laparoscopic partial nephrectomy in 200 cases. J Urol
2005;173:42–7.
[55] Yoshikawa Y, Ono Y, Hattori R, et al. Laparoscopic partial
nephrectomy for renal tumor: Nagoya experience. Urol-
ogy 2004;64:259–63.
[56] Kim FJ, Rha KH, Hernandez F, et al. Laparoscopic radical
versus partial nephrectomy: assessment of complica-
tions. J Urol 2003;170:408–11.
[57] Gill IS, Colombo Jr JR, Frank I, et al. Laparoscopic partial
nephrectomy for hilar tumors. J Urol 2005;174:850–3, dis-
cussion 853-4.
[58] Simon SD, Castle EP, Ferrigni RG, et al. Complications of
laparoscopic nephrectomy: the Mayo clinic experience.
J Urol 2004;171:1447–50.
[59] Zlotta AR, Schulman CC. Ablation of renal tumors in a
rabbit model with interstitial saline-augmented radio-
frequency energy. Urology 1999;54:382–3.
[60] Gill IS, Hsu TH, Fox RL, Matamoros A, et al. Laparoscopic
and percutaneous radiofrequency ablation of the kidney:
acute and porcine study. Urology 2000;56:197–200.
[61] Collyer WC, Landman J, Olweny EO, Andreoni C, Kerbl K,
Bostwick DG, et al. Comparison of renal ablation with
cryotherapy, dry radiofrequency and saline augmented
radiofrequency in a porcine model. J Am Coll Surg
2001;193:505–13.
[62] Pavlovich CP, Walther MM, Choyke PL, Paulter SE, Chang
R, et al. Percutaneous radio frequency ablation of small
renal tumors: initial results. J Urol 2002;167:10–5.
[63] Rendon RA, Kachura JR, Sweet JM, et al. The uncertainty of
radiofrequency treatment of renal cell carcinoma: find-
ings at immediate and delayed nephrectomy. J Urol
2002;167:1587–92.
[64] Gervais DA, Arellano RS, Mueller PR. Percutaneous radio-
frequency ablation of renal cell carcinoma. Eur Radiol
2005;15:960–7.
[65] Roy-Choudhury SH, Cast JE, Cooksey G, et al. Early experi-
ence with percutaneous radiofrequency ablation of small
solid renal masses. AJR Am J Roentgenol 2003;180:1055–61.
[66] Su LM, Jarrett TW, Chan DY, et al. Percutaneous computed
tomography-guided radiofrequency ablation of renal
masses in high surgical risk patients: preliminary results.
Urology 2003;61(4 suppl 1):26–33.
[67] Farrell MA, Charboneau WJ, DiMarco DS, et al. Imaging-
guided radiofrequency ablation of solid renal tumors.
AJR Am J Roentgenol 2003;180:1509–13.
[68] Anderson JK, Matsumoto E, Cadeddu JA. Renal radiofre-
quency ablation: technique and results. Urol Oncol
2005;23:355–60.
[69] Leonardi MA, Lumenta CB. Stereotactic guided laser-
induced interstitial thermotherapy (SLITT) in gliomas
with intraoperative morphologic monitoring in an open
MR: clinical experience. Minim Invasiv Neurosurg 2002;
45:201–7.
[70] Hall-Craggs MA, Vaidya JS. Minimally invasive therapy for
the treatment of breast tumors. Eur J Radiol 2002;42:52–7.
[71] de la Rosette JJ, D’Ancona FC, Debruyne FM. Current
status of thermotherapy of the prostate. J Urol 1997;157:
430–8.
[72] Hradec E, Fuchs E. Effect of microwave diathermy of the
kidney. Z Urol Nephrol 1969;62:337–42.
[73] Kigure T, Harada T, Yuri Y, et al. Ultrasound-guided micro-
wave thermotherapy on a VX-2 carcinoma implanted in
rabbit kidney. Ultrasound Med Biol 1995;21:649–55.
[74] Hinshaw JL, Lee Jr FT. Image-guided ablation of renal cell
carcinoma. Magn Reson Imaging Clin North Am 2004;
12:429–47.
[75] Dechet CB, Sebo T, Farrow G, Blute ML, Engen DE, Zincke
H. Prospective analysis of intraoperative frozen needle
biopsy of solid renal tumors in adults. J Urol 1999;162:
1282–5.
CME questions
Please visit www.eu-acme.org/europeanurologyto answer these CME questions on-line. The CMEcredits will then be attributed automatically.
1. Small renal masses (<3 cm)A. Are benign in up to 14% of cases.B. Grow at a rate of 0.35 cm/yr.C. Incidence is increasing, especially in patients
younger than 50 yr of age.D. Radical nephrectomy is associated with less
renal compromise than partial nephrectomy.
2. Indications for ablation as opposed to resection ofrenal masses include:
A. von Hippel-Lindau disease.B. Young age.C. Presence of metastatic disease.D. Large size.
3. CryoablationA. Has a nadir temperature determined by the
freezing point of the gas used.B. Commonly causes urinary leakage when the
collecting system is treated.C. Has been associated with ‘‘skip lesions’’ on
histologic examination.D. Produces a lesion that is affected by the size of
probe and rapidity of freezing.

e a u - e b u u p d a t e s e r i e s 5 ( 2 0 0 7 ) 2 0 6 – 2 1 8218
4. Tissue death in cryoablation is caused by thefollowing mechanism(s):A. Formation of intracellular ice that causes
disruption of cell membranes and organelles.B. Decreased cellular osmolarity leading to
edema.C. Inpermeability of the microvasculature result-
ing in thrombosis leading to immediate celldeath.
D. DNA damage, especially for cells in S phase ofthe cell cycle.
5. Which of the following statements is true regard-ing lethal temperatures in renal cryoablation?A. A temperature of �19.4 8C leads to reliable
tissue ablation in kidney tumors.
B. In vitro, 90% of kidney cancer cells survive�20 8C but only 15% survive �40 8C
C. A single freeze with active thaw maximizestumour destruction.
D. The nadir temperature and hold time atsubzero temperatures affect cellular survival.
6. Renal cryoablation long-term resultsA. Are better for the percutaneous than laparo-
scopic or open approaches.B. Show that the tumour completely disappears
in only 45% of cases.C. Demonstrate a 98% cancer-specific survival at
3 yr of follow-up.D. Rely on needle biopsies as the gold standard
for outcome.