Embed Size (px)
Citation preview

Cryotherapy during Surgery for Giant Retinal Tears and Intravitreal Dispersion of Viable Retinal Pigment Epithelial Cells
Bert M. Glaser, MD,1 Jesus Vidaurri-Leal, MD,2 Ronald G. Michels, MD, * Peter A. Campochiaro, MrY
Background: Retinal pigment epithelial (RPE) cells are a major component of contractile cellular membranes in proliferative vitreoretinopathy (PVR). Displacement of viable RPE cells into the vitreous cavity is necessary for membrane formation. This study examines the effect of cryotherapy during surgery for giant retinal tears on the dispersion of viable cells into the vitreous cavity.
Methods: A total of seven eyes undergoing vitrectomy and retinal reattachment surgery were studied. Vitreous fluid from three eyes was aspirated immediately after cryotherapy; fluid from four eyes was aspirated after scleral indentation with the cryoprobe, but without cryotherapy. Colonies of pigmented cells routinely grew in flasks inoculated with fluid from eyes treated with cryotherapy. In contrast, flasks inoculated with fluid from eyes not treated with cryotherapy contained significantly fewer viable cells.
Conclusion: Cryotherapy performed during retinal reattachment surgery in eyes with giant retinal tears is likely to enhance intravitreal dispersion of viable RPE cells. The findings in this study suggest that possible harmful effects of cryotherapy should be evaluated further and that alternative methods of creating a chorioretinal adhesion should be considered in cases with an especially high risk of PVR. Ophthalmology 1993; 1 00:466-470
Technical advances have greatly improved the prognosis for successful treatment of retinal detachment in eyes with giant retinal tears. I
-9 However, the prognosis for long
term success is still hampered by a high incidence of postoperative proliferative vitreoretinopathy (PVR). This complication occurred in 58% of eyes with giant retinal tears in a large series of patients. 10
jection ofRPE cells in rabbits results in cellular membrane formation and traction retinal detachment similar to that seen in pVR.16 However, the process by which RPE cells move into the vitreous cavity remains unclear.
It is likely that cellular migration into the vitreous cavity occurs in response to various biochemical stimuli.17
However, in eyes with giant retinal tears, anatomic factors also may be important because RPE cells are exposed to the vitreous cavity over a large area. In this circumstance, mechanical dispersion of RPE cells may playa role. The current study examines the effect of cryotherapy during surgery for giant retinal tears on the dispersion of viable cells into the vitreous cavity.
Retinal pigment epithelial (RPE) cells have been implicated in the pathogenesis of PVR. 11-16 Intravitreal in-
Originally received: May 12, 1992. Revision accepted: November 2, 1992.
I The Retina Center at Saint Joseph Hospital, Baltimore.
2 Centro De Oftalmologia San Jose, Monterrey, N.L. , Mexico.
3 Wilmer Ophthalmological Institute, Johns Hopkins Hospital, Baltimore.
* Deceased.
Reprint requests to Bert M. Glaser, MD, The Retina Center at Saint Joseph Hospital, P.O. Box 20,000, Baltimore, MD 21284.
466
Materials and Methods
The effect of transscleral cryotherapy on the dispersion of cells into the vitreous cavity was examined in eyes with

Glaser et al . Cryotherapy during Surgery
primary retinal detachments due to giant retinal tears that were treated.
Patients, Clinical Findings, and Surgical Procedures
Seven patients 40 to 55 years of age were randomly selected as to whether they received cryotherapy or sham treatment. Informed consent was obtained from all patients. None of the patients had a history of previous ocular surgery, retinal tears, trauma, or uveitis. All eyes had tears measuring between 1800 and 220 0
• All of the detachments became symptomatic between 2 and 5 days before surgery. None of the eyes were judged to have PVR at the time of surgery. None of the eyes had significant cataracts at the time of surgery.
All seven eyes were treated using techniques that we have previously described.9 Surgery was performed under local anesthesia. A 20-gauge infusion cannula was inserted 3.5 mm posterior to the limbus in the inferotemporal quadrant. A second sclerotomy was made 3.5 mm posterior to the limbus in the superotemporal quadrant in right eyes and in the superonasal quadrant in left eyes. A pars plana lensectomy was performed using ultrasonic emulsification.
A third sclerotomy was then made in the opposite superior quadrant 3.5 mm posterior to the limbus. A fiber optic light pipe and the vitrectomy probe were introduced through the two superior sclerotomies. The anterior and posterior lens capsules were removed, and a total vitrectomy was performed. The instruments were removed and the sclerotomies were closed with scleral plugs.
In three of seven eyes, transscleral cryotherapy was then performed in three rows extending 360° around the eye. The cryotherapy was visually monitored by indirect ophthalmoscopy. Pigmented debris was often seen to be dispersed into the vitreous cavity from the sites of cryotherapy. In the other four eyes on which the sham procedure was performed, the cryoprobe was used to indent the eye to simulate the mechanical effects of cryotherapy; however, no freeze was performed.
After either cryotherapy or the sham procedure, approximately 2 ml of fluid were aspirated from the vitreous cavity using the vitrectomy probe. The fluid was then analyzed using the tissue culture methods described below. The vitreous cavity was then lavaged extensively to remove any residual cells.9 All sclerotomies were closed with 7-0 polyglycolate; two white silk (4-0) mattress sutures, with bites 10 or 13 mm apart, were then placed in each quadrant. A #276 exoplant or a #287 exoplant combined with one half of a 3-mm sponge were placed under the sutures.9
The patient was then rotated to the prone position. A total fluid-gas exchange was performed.9 The patient was then rotated back to the supine position, and the scleral sutures were tightened to create a high and broad scleral buckle.
The eyes that were not treated with cryotherapy during the operation received laser treatment along the edge of the retinal tear on the following day. All seven patients
were followed for 6 to 12 months, and PVR did not develop.
Cell Culture
The vitreous aspirate from each eye was immediately inoculated into a 75-cm2 tissue culture flask containing 20 ml of Eagle's Minimum Essential Medium plus 20% fetal calf serum. Each flask was incubated at 37°C and 5% CO2
for 24 hours. After that time, each flask was placed on a transparent grid composed of 10 X lO-mm boxes. The flask and grid were placed on the stage of a Nikon inverted phase-contrast microscope (Nikon, Inc., Instrument Group, Melville, NY) under low power (X 100), and attached cells in 40 grid squares were counted. Cell attachment was ascertained by gently shaking the dish while observing cells. Attached cells were recorded in three categories according to the number of cells clumped together: (1) one to three cells, (2) four to ten cells, and (3) more than ten cells.
After completion of counting, the flasks were returned to the incubator for an additional 4 days. They were then placed on the grid, and attached cells were counted again. At this time, attached cells were ascertained by cell spreading and were recorded in the same three categories listed above, with an additional category listed as "colonies" for those cells that had undergone cell division. Statistical comparisons were made by the unpaired Student's t test.
Results
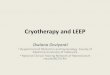
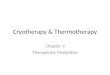
In preliminary experiments, we observed that fluid samples from eyes with giant retinal tears treated with cryotherapy contained RPE cells that could be readily identified microscopically. To determine whether these cells were viable and therefore pathologically significant, we examined cell attachment and colony formation. Flasks plated from eyes treated with cryotherapy had significantly more attached cells at 24 hours than those from eyes not treated with cryotherapy (Fig 1). In addition, there were many more large clumps of attached cells from the eyes treated with cryotherapy. The viability of cells from eyes treated with cryotherapy was demonstrated by their ability to attach and spread on the surface of the flask (Fig 2). These cells were heavily pigmented (Fig 2), suggesting that they were RPE cells.
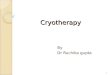
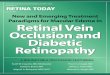
Despite the increased number of attached cells after cryotherapy, it is possible that these cells have limited longevity and are therefore unable to proliferate. To examine this possibility, we incubated the flasks containing dispersed cells for 5 days. Flasks plated from eyes treated with cryotherapy continue to have many more attached cells, and many of these cells proliferated to form colonies (Figs 3 and 4). Thus, cryotherapy enhances the release of cells that are capable of attachment and proliferation.
Discussion
Creation of a chorioretinal scar to seal retinal breaks is a fundamental part of retinal reattachment surgery. Though
467

Ophthalmology Volume 100, Number 4, April 1993
Figure 1. Cell detachment 24 hours after inoculation into tissue culture media. Bar values represent the mean from four eyes in the control group and three eyes in the cryotherapy group. The differences between cryotherapy and control were significant to the P < 0.01 level by the unpaired Student's t test.
Number
Attached
18
16
14
12
10
8
6
4
2
0
diathermy has been used for this purpose, cryotherapy has largely replaced diathermy in recent years because it obviates the need for scleral dissection. As a result, transscleral cryotherapy has frequently been advocated as part of the continuously improving methods to treat complicated retinal detachments, including detachments secondary to giant retinal tears. I- 4 .7-9
Though current improvements in therapy have surmounted many of the difficulties preventing initial anatomic success, there is still a significant incidence of mas-
Figure 2. Retinal pigment epithelial cells from an eye treated with cryotherapy. The appearance of the cells 24 hours after inoculation into culture media is shown (phase contrast microscopy; original magnification, X22S0).
468
o CONTROL
.CRYO
.10 Number of Cells per Group
sive PVR that sometimes causes subsequent failure. This raises the question of an association between therapeutic intervention and PVR. A central issue in the pathogenesis of PVR is the mechanism by which viable RPE cells gain entry into the vitreous cavity, where they later proliferate to form cellular membranes. The current study demonstrates that cryotherapy, when applied transsclerally in eyes with giant retinal tears, enhances the dispersion of viable pigmented cells into the vitreous cavity. In another study, using bovine eyes in an in vitro laboratory model,

Glaser et al . Cryotherapy during Surgery
32--------------------------------~
o CONTROL
.CRYO Figure 3. Cell attachment and colony formation 5 days after inoculation into tissue culture media. Bar values represent the mean from four control eyes and three eyes treated with cryotherapy. The differences between cryotherapy and control in all groups were significant to the P < 0.01 level by the unpaired Student's t test.
Number
Attached
Number of Cells per Group
we demonstrated that transscleral cryotherapy, but not diathermy, enhances dispersion of RPE cells into the vitreous cavity. 18
Others have noted that cryotherapy can cause release of pigment into the vitreous cavity and/or under the retina. 19-
21 Our study demonstrates that cryotherapy releases viable pigmented cells, though it does not determine the reason for this effect. The release of clumps of RPE cells after cryotherapy suggests that it alters cellular adhesion. The area of altered cellular adherence to Bruch's membrane may be more extensive than the area of cell death,
so viable cells around the margin of an area of cryogenic necrosis are released. This is suggested by a histologic study of cryosurgical lesions that demonstrated loosening of RPE cells from their basement membrane, resulting in wandering pigmented macrophages throughout the retina.22
Our study showing dispersion of viable cells after cryotherapy raises questions as to possible adverse clinical effects from this therapy. We have shown that serum components, including fibrin and fibronectin, enhance the ability ofRPE cells to migrate into the vitreous cavity. 17,23
Figure 4. A colony of cells 5 days after inoculation of a vitreous sample from an eye treated with cryotherapy (phase contrast microscopy; original magnification, X600).
469

Ophthalmology Volume 100, Number 4, April 1993
Cryotherapy also causes breakdown of the blood-ocular barriers, allowing the release of these serum components into the vitreous cavity. For these reasons, it is possible that cryotherapy is an exacerbating factor in the pathogenesis of PVR. 17
Perhaps the ill effects of cryotherapy can be prevented or lessened by performing a vitrectomy or lavage of the vitreous fluid after cryotherapy. Most of those eyes, as in the current cases, have a complete air-fluid exchange which probably results in removal of most of the dispersed RPE cells.
There is vast clinical experience indicating that cryotherapy is effective and safe in treating most eyes with retinal detachment. Therefore, we continue to use cryotherapy in most clinical situations. Still, the findings in this study suggest that possible harmful effects of cryotherapy should be evaluated further and that alternative methods of creating a chorioretinal adhesion be considered in patients with an especially high risk of PVR.
References
1. Norton EWD, Aaberg T, Fung W, Curtin VT. Giant retinal tears. I. Clinical management with intravitreal air. Am · J Ophthalmol 1969;68: 10 11-21.
2. Machemer R, Aaberg TM, Norton EWD. Giant retinal tears. II. Experimental production and management with intravitreal air. Am J Ophthalmol 1969;68:1022-9.
3. Scott JD. A new approach to the vitreous base. Mod Probl Ophthalmol 1974;12:407-10.
4. Fung WE, Hall DL, Cleasby GW. Combined technique for a 355 0 traumatic giant retinal break. A case report. Arch Ophthalmol 1975;93:264-6.
5. Machemer R, Allen AW. Retinal tears 1800 and greater: management with vitrectomy and intravitreal gas. Arch Ophthalmol 1976;94: 1340-6.
6. Usui M, Hamazaki S, Takano S, Matsuo H. A new surgical technique for the treatment of giant tear: transvitreoretinal fixation. Jpn J Ophthalmol 1979;23:206-15.
7. Federman JL, Shakin JL, Lanning RC. The microsurgical management of giant retinal tears with trans-scleral retinal sutures. Ophthalmology 1982;89:832-9.
8. Ando F, Kondo J. A plastic tack for the treatment of retinal detachment with giant tear [letter]. Am J Ophthalmol 1983;95:260-1.
470
9. Michels RG, Rice TA, Blankenship G. Surgical techniques for selected giant retinal tears. Retina 1983;3:139-53.
lO. Freeman HM, Castillejos ME. Current management of giant retinal breaks: results with vitrectomy and total air fluid exchange in 95 cases. Trans Am Ophthalmol Soc 1981;79: 89-102.
II. Machemer R, Laqua H. Pigment epithelium proliferation in retinal detachment (massive periretinal proliferation). Am J OphthalmoI1975;80:1-23.
12. Mandelcorn MS, Machemer R, Fineberg E, Hersch S. Proliferation and metaplasia of intravitreal retinal pigment epithelium cell autotransplants. Am J Ophthalmol 1975;80: 227-37.
13. Johnson NF, Foulds WS. Observations on the retinal pigment epithelium and retinal macrophages in experimental retinal detachment. Br J Ophthalmol 1977;61:564-72.
14. Machemer R, van Horn D, Aaberg TM. Pigment epithelial proliferation in human retinal detachment with massive periretinal proliferation. Am J Ophthalmol 1978;85: 181-91.
15. Newsome DA, Rodrigues MM, Machemer R. Human massive periretinal proliferation. In vitro characteristics of cellular components. Arch Ophthalmol 1981 ;99:873-80.
16. Radtke ND, Tano Y, Chandler D, Machemer R. Simulation of massive periretinal proliferation by autotransplantation of retinal pigment epithelial cells in rabbits. Am J Ophthalmol 1981;91:76-87.
17. Campochiaro PA, Jerdan JA, Glaser BM. Serum contains chemoattractants for human retinal pigment epithelial cells. Arch Ophthalmol 1984;102:1830-3.
18. Campochiaro PA, Kaden IH, Vidaurri-Leal J, Glaser BM. Cryotherapy enhances intravitreal dispersion of viable retinal pigment epithelial cells. Arch OphthalmoI1985;103:434-6.
19. Abraham RK, Shea M. Cryopexy for improved results in the prophylaxis of retinal detachment. Trans Ophthalmol Soc UK 1969;88:297-311.
20. Sudarsky RD, Yannuzzi LA. Cryomarcation line and pigment migration after retinal cryosurgery. Arch Ophthalmol 1970;83:395-401.
21. Hilton GF. Subretinal pigment migration. Effects of cryosurgical retinal reattachment. Arch Ophthalmol 1974;91: 445-50.
22. Lincoff H, Kreissig I. The mechanism of the cryosurgical adhesion. IV. Electron microscopy. Am J Ophthalmol 1971 ;71 :674-89.
23. Vidaurri-Leal JS, Glaser BM. Effect of fibrin on morphologic characteristics of retinal pigment epithelial cells. Arch Ophthalmol 1984; 102: 1376-9.




![Intravitreal bevacizumab upregulates transthyretin in ...Branch retinal vein occlusion (BRVO) is one of the most common retinal vascular diseases [ 1]. Loss of visual function in BRVO](https://img.pdfslide.net/doc/110x75/600b825fa382f9522d685c4a/intravitreal-bevacizumab-upregulates-transthyretin-in-branch-retinal-vein-occlusion.jpg)






![Clinical Study Comparison between Intravitreal ...downloads.hindawi.com/journals/isrn/2013/141279.pdfcommon cause of retinal vascular disease following diabetic retinopathy [ ]. Among](https://img.pdfslide.net/doc/110x75/5e881482d74bac340b063934/clinical-study-comparison-between-intravitreal-common-cause-of-retinal-vascular.jpg)