Embed Size (px)
Citation preview
CT Lung Cancer Screening How to Incorporate Lung Cancer
Screening into Your Practice
John Panaccione M.D.
Lung Cancer is a Bad Disease • 228,000 new cases/yr 160,000 deaths/yr • -70% incurable at presentation • Lung Cancer deaths/yr > breast + colon +
prostate • New cases:
-21% current smokers -60% former smokers -19% female never smokers, 9% male never smokers
• Five Year Total Survival 16% -Prostate 81% Colon: 65% -Breast 60%
Cigarette Smoking •Causes 75% of lung cancer worldwide •Risk highest for small cell and squamous cell •15% of U.S. adults are smokers •10%-15% of average-heavy smokers will get lung Ca •16% 5 year survival
Dela Cruz et al. Clinics in chest medicine. 2011 Dec;32(4):605-44.
Non Small Cell Lung Cancer (NSCLC) •Adenocarcinoma (40% of lung cancers) •Squamous cell carcinoma (25% of lung cancers) •Large cell carcinoma (10% of lung cancers) Small Cell Cancer (15% of Lung cancers) http://www.cancer.gov/types/lung/hp/non-small-cell-lung-treatment-pdq#section/_359
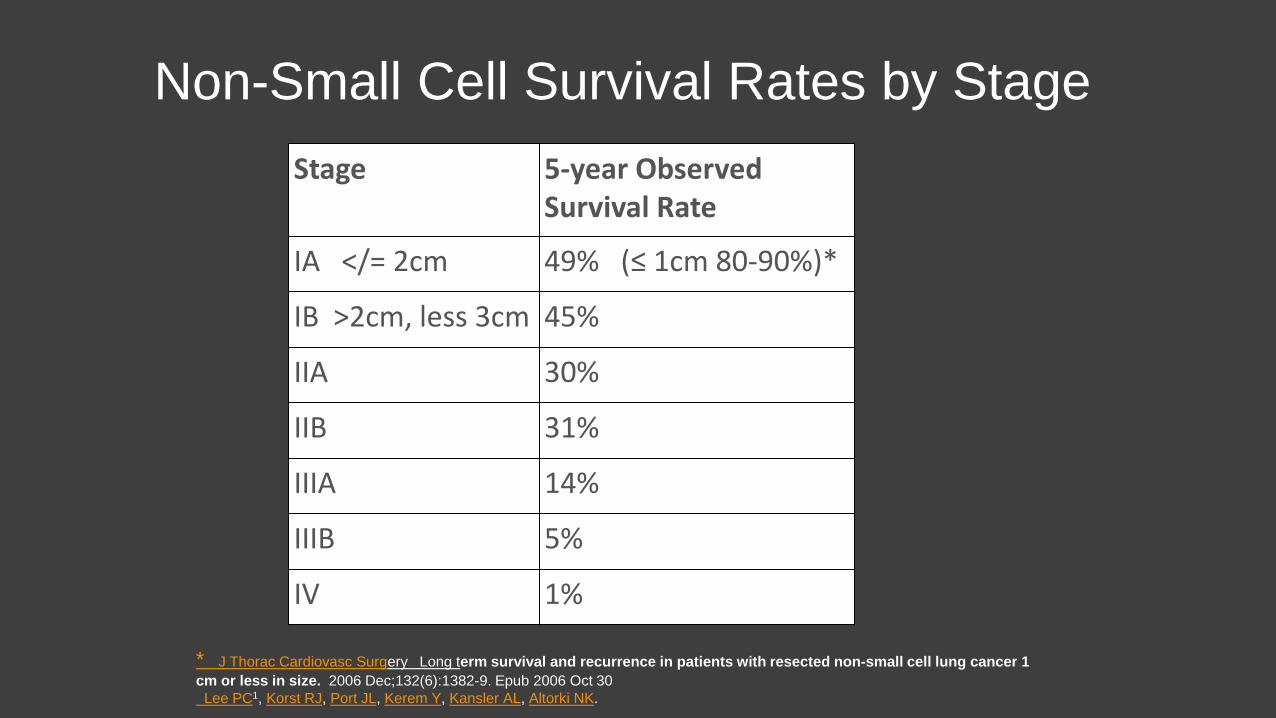
Non-Small Cell Survival Rates by Stage Stage 5-year Observed
Survival Rate
IA </= 2cm 49% (≤ 1cm 80-90%)*
IB >2cm, less 3cm 45%
IIA 30%
IIB 31%
IIIA 14%
IIIB 5%
IV 1%
* J Thorac Cardiovasc Surgery Long term survival and recurrence in patients with resected non-small cell lung cancer 1 cm or less in size. 2006 Dec;132(6):1382-9. Epub 2006 Oct 30 Lee PC1, Korst RJ, Port JL, Kerem Y, Kansler AL, Altorki NK.
Lung Cancer: CXR Screening • 4 RCT studies in 60’s and 70’s, CXR/sputum • PLCO trial 1993-2001 CXR vs Usual care • Disease was discovered at an earlier stage • Survival time increased from diagnosis to death • No decrease in lung cancer mortality Marcus PM. J Clin Oncol 2001; 19: 83S-86S Marcus PM et al. J Natl Cancer Inst 2000; 92: 1308-1316
International Early Lung Cancer Action Project (I-ELCAP) 1993-2005 • Annual LDCT and CXR • Asymptomatic high risk age 40 or above, 10+ pack yrs. • Positive scan: 5mm solid nodule • LDCT detected malignant disease 4X rate CXR (prior trails) • LDCT: 85% stage 1 vs prior trails CXR 15% stage 1 • Estimated 88% 10-yr survival rate in stage 1 patients • Limitations : No controls, variable eligibility and work-up
•Henschke CI, Yankelevitz DF, Libby DM, Pasmantier MW, Smith JP, and Miettinen OS. Survival of patients with stage I lung cancer detected on CT screening. New England Journal of Medicine 2006; 355: 1763-71
The National Lung Cancer Screening Trail: Study Design •Prospective randomized trial: 2002-2009 •53,454 individuals @ high risk at 33 sites •1:1 randomization LDCT or CXR •3 annual screens •Primary analysis: lung cancer mortality NLST Research Team. Radiology 2011; 258(1):243-253 The National Lung Screening Trial Research Team. N Engl J Med 2011;365(5):395-409
NLST: Eligibility •Asymptomatic for lung cancer •Ages 55-74 •30+ pack year smoking history •No prior lung cancer NLST Research Team. Radiology 2011; 258(1):243-253
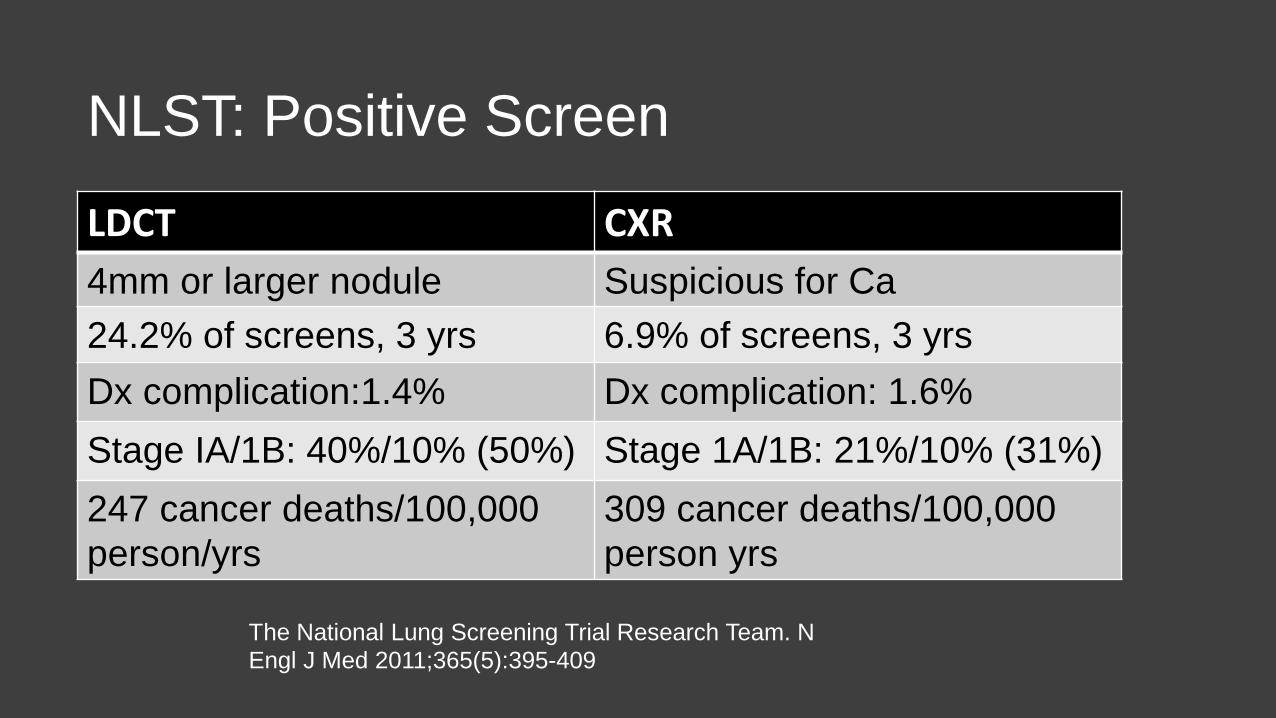
NLST: Positive Screen
The National Lung Screening Trial Research Team. N Engl J Med 2011;365(5):395-409
LDCT CXR 4mm or larger nodule Suspicious for Ca 24.2% of screens, 3 yrs 6.9% of screens, 3 yrs Dx complication:1.4% Dx complication: 1.6% Stage IA/1B: 40%/10% (50%) Stage 1A/1B: 21%/10% (31%) 247 cancer deaths/100,000 person/yrs
309 cancer deaths/100,000 person yrs
NLST: Summary • Prospective Randomized Trail • > 90% compliance.
• 20% Lung Cancer specific mortality reduction • 7% all cause mortality reduction • 320 individuals screened to prevent 1 lung cancer death • High positive screen/recall rate. • Over diagnosis: ~3-11%? • False negatives
Reducing the High False + Rate
• NLST and I-ELCAP data reevaluated • 6 mm threshold for “positive” scan • Reduction of positive/recall rate >50% • Trade-off: Decrease in sensitivity (8-15%)
Yip R, Henschke CL, et al CT Screening for Lung Cancer: Alternate Definitions of Positive Test Results Based on the National Lung Screening Trail and International Early Lung Cancer Action Program Radiology 2014;273(4):591-596
Lung-RADS
• Lung Reporting And Data System
• Source: American College Of Radiology (ACR) Lung Cancer Committee Subgroup
• Purpose: Standardization of lung cancer screening practice and communication of results
• Content: Assessment categories and systematic management recommendations for screen detected lung nodules
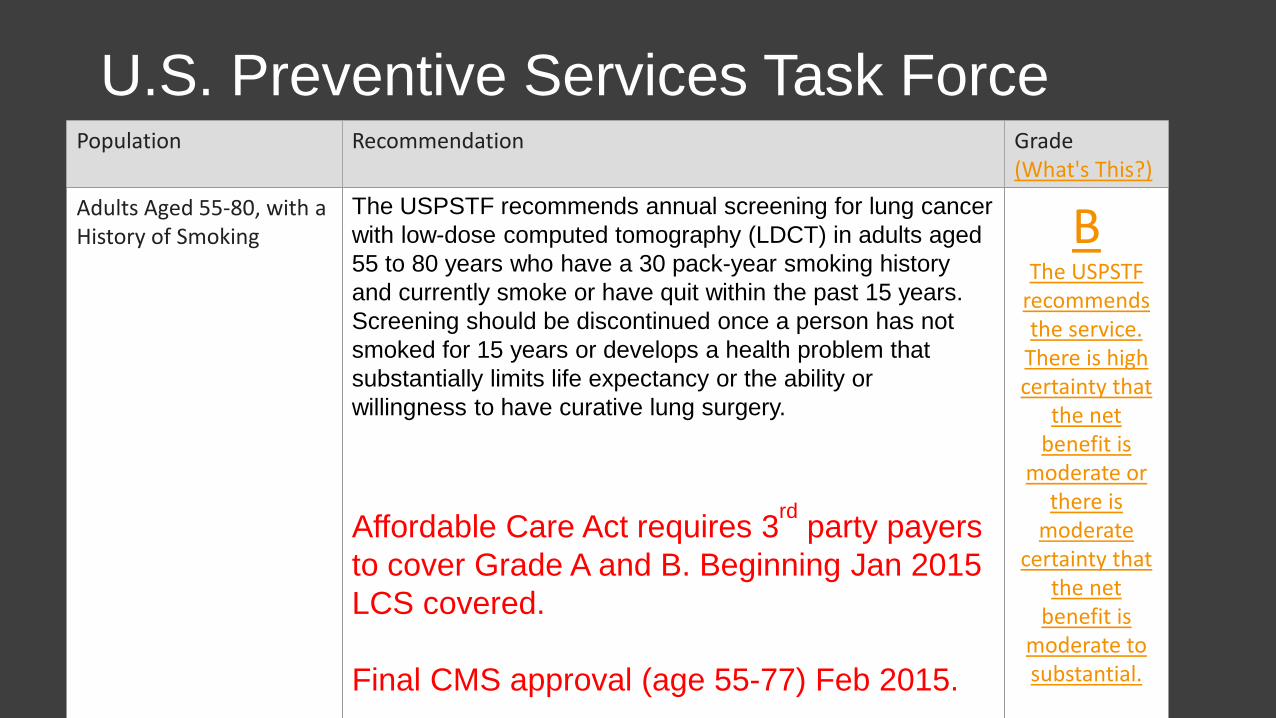
U.S. Preventive Services Task Force Population Recommendation Grade
(What's This?)
Adults Aged 55-80, with a History of Smoking
The USPSTF recommends annual screening for lung cancer with low-dose computed tomography (LDCT) in adults aged 55 to 80 years who have a 30 pack-year smoking history and currently smoke or have quit within the past 15 years. Screening should be discontinued once a person has not smoked for 15 years or develops a health problem that substantially limits life expectancy or the ability or willingness to have curative lung surgery. Affordable Care Act requires 3rd party payers to cover Grade A and B. Beginning Jan 2015 LCS covered. Final CMS approval (age 55-77) Feb 2015.
B The USPSTF
recommends the service.
There is high certainty that
the net benefit is
moderate or there is
moderate certainty that
the net benefit is
moderate to substantial.
Lung Cancer Screening Low Dose CT Chest
• Lung Cancer Screening and for F/U pulmonary nodule • Dose: 1.0-2.0 mSv. BMI based. Standard CT: 8 mSv • Thin Slices:1.25mm vs 2.5mm - 5.0mm for standard CT • Limitations: Mediastinum and upper abdomen • Lung-RADS: Standardized Reporting and Management • Structured Report • MMC is an ACR Designated Lung Cancer Screening Center
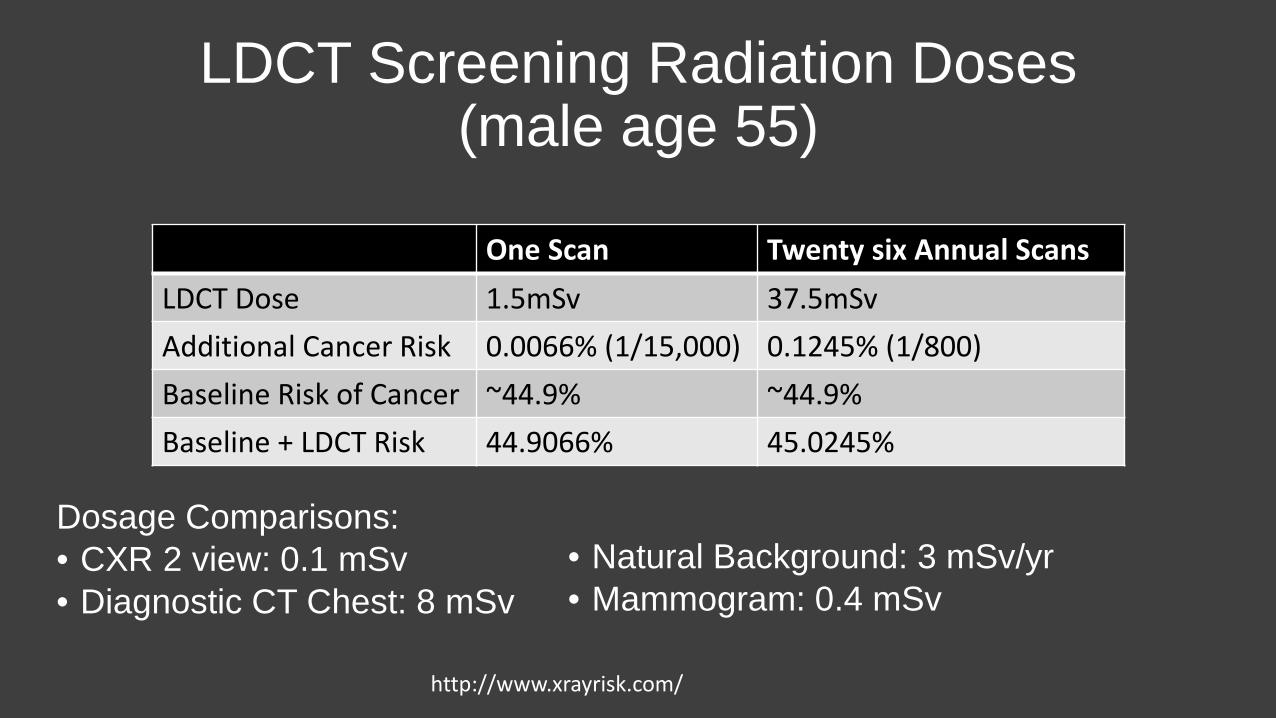
LDCT Screening Radiation Doses (male age 55)
Dosage Comparisons: • CXR 2 view: 0.1 mSv • Diagnostic CT Chest: 8 mSv
• Natural Background: 3 mSv/yr • Mammogram: 0.4 mSv
http://www.xrayrisk.com/
One Scan Twenty six Annual Scans LDCT Dose 1.5mSv 37.5mSv Additional Cancer Risk 0.0066% (1/15,000) 0.1245% (1/800) Baseline Risk of Cancer ~44.9% ~44.9% Baseline + LDCT Risk 44.9066% 45.0245%
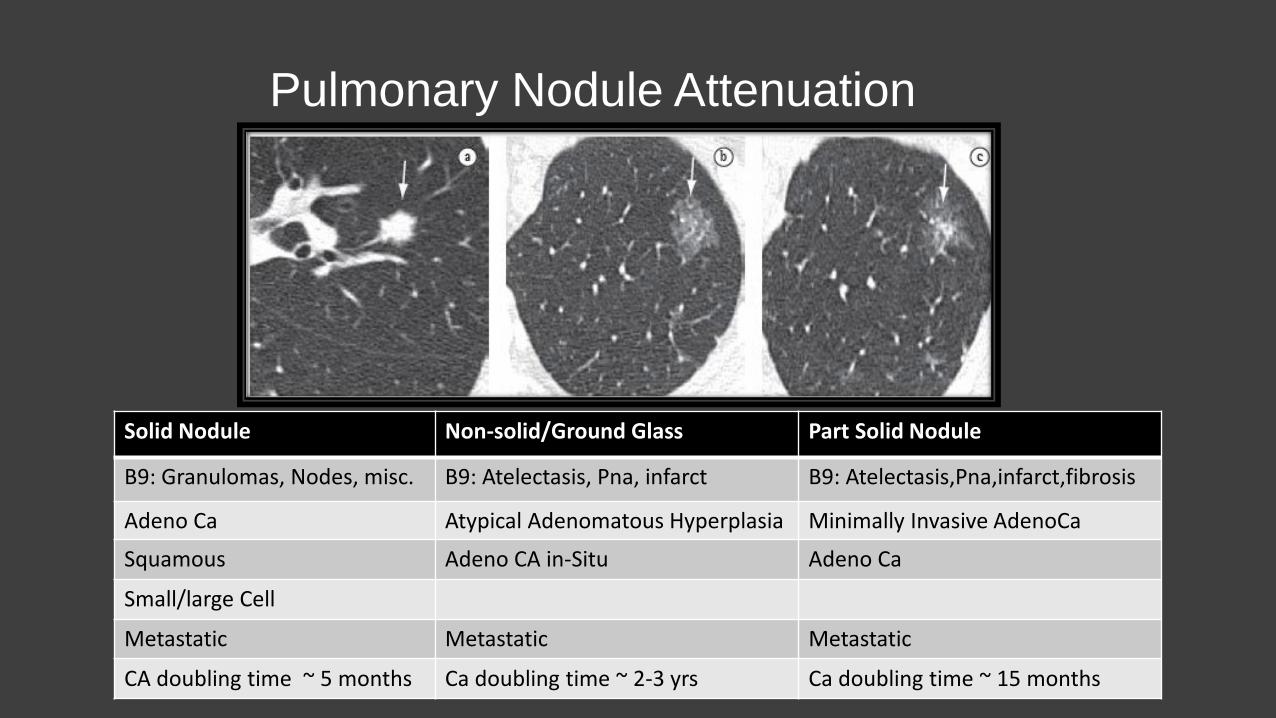
Pulmonary Nodule Attenuation
Solid Nodule Non-solid/Ground Glass Part Solid Nodule
B9: Granulomas, Nodes, misc. B9: Atelectasis, Pna, infarct B9: Atelectasis,Pna,infarct,fibrosis
Adeno Ca Atypical Adenomatous Hyperplasia Minimally Invasive AdenoCa
Squamous Adeno CA in-Situ Adeno Ca
Small/large Cell
Metastatic Metastatic Metastatic
CA doubling time ~ 5 months Ca doubling time ~ 2-3 yrs Ca doubling time ~ 15 months
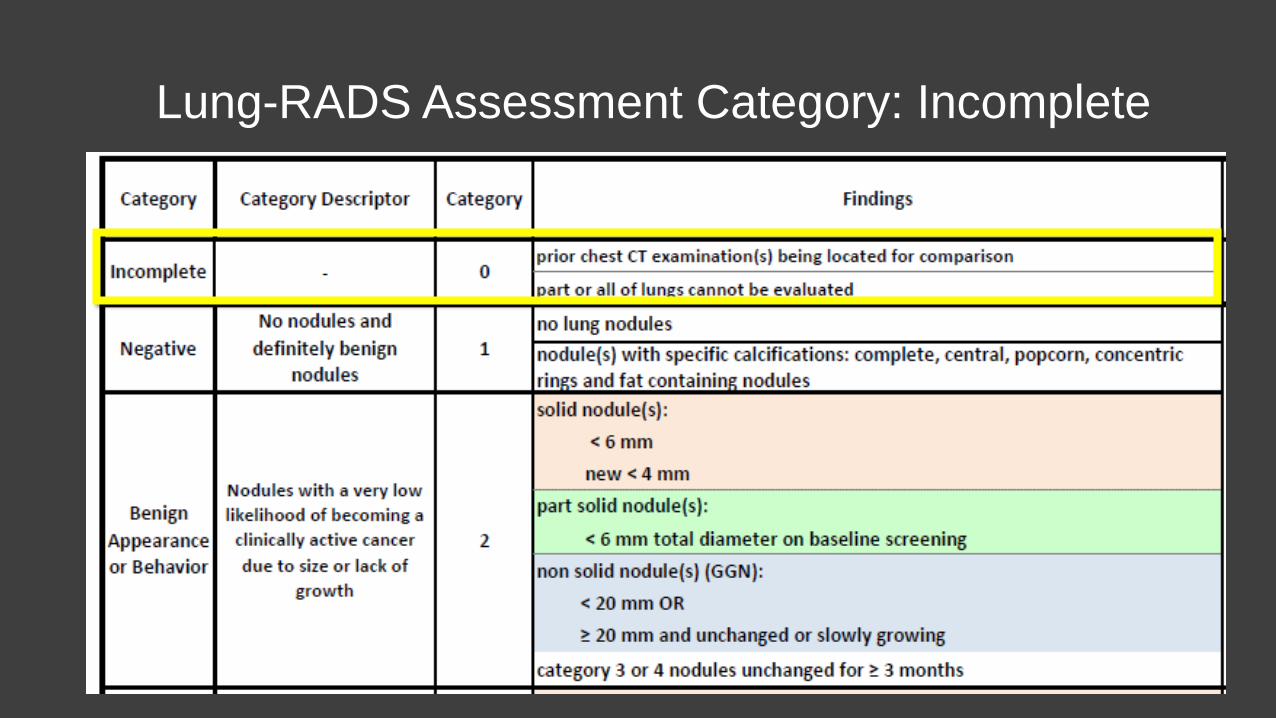
Lung-RADS Assessment Category: Incomplete
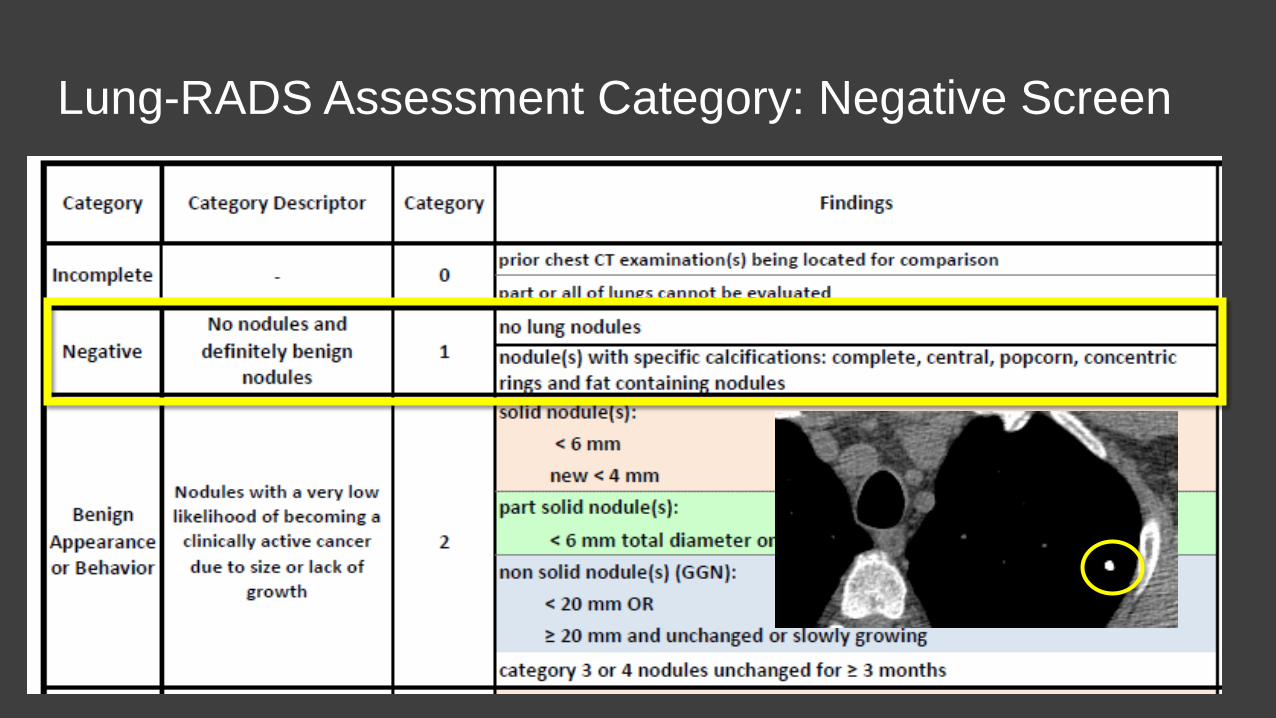
Lung-RADS Assessment Category: Negative Screen
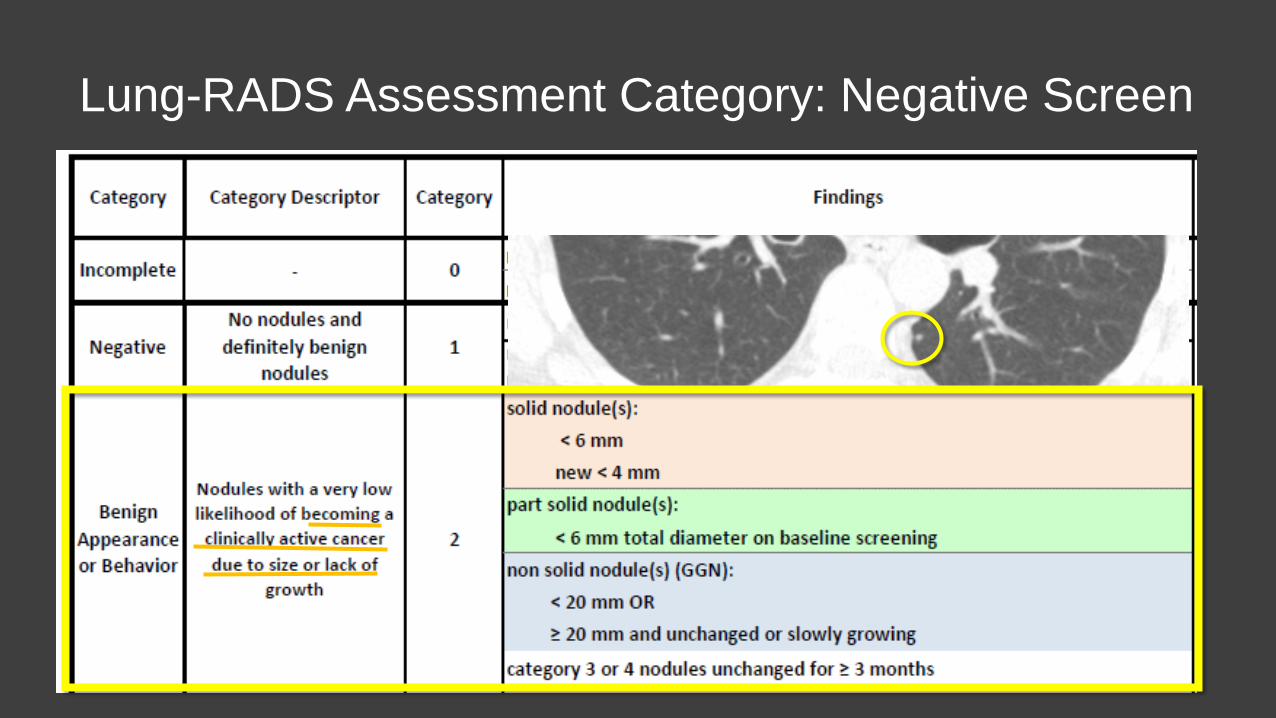
Lung-RADS Assessment Category: Negative Screen
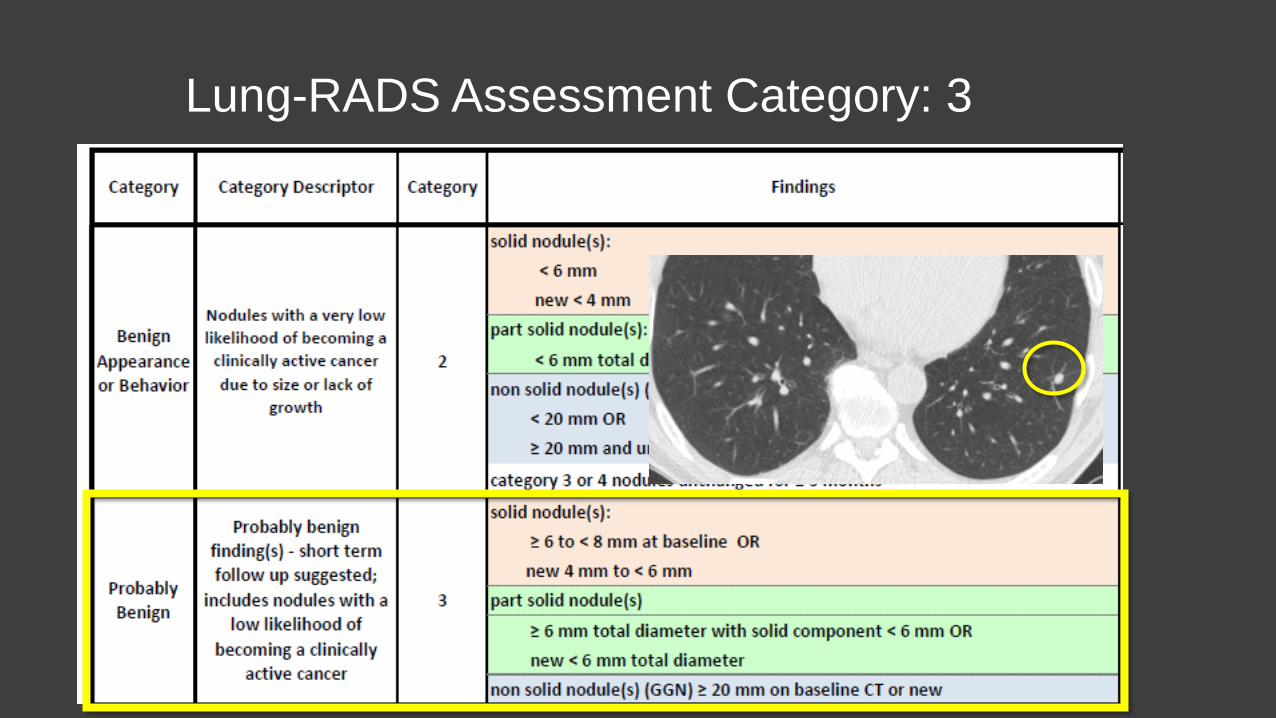
Lung-RADS Assessment Category: 3
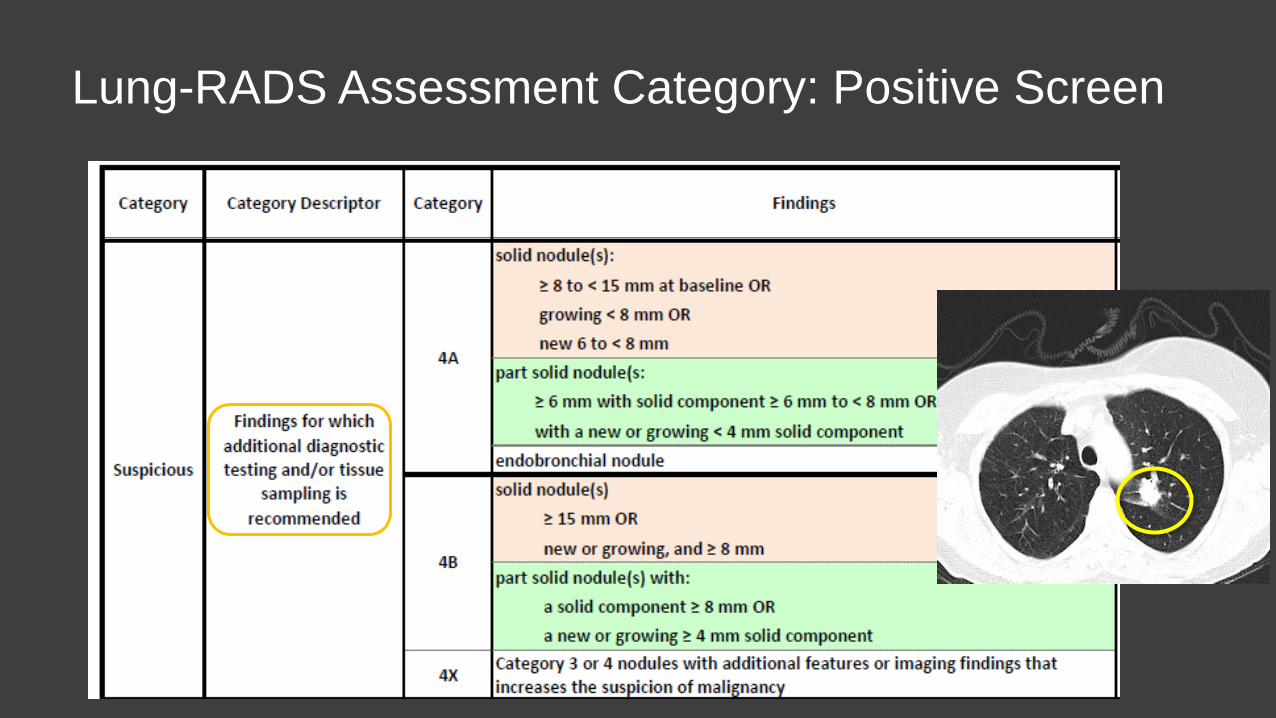
Lung-RADS Assessment Category: Positive Screen
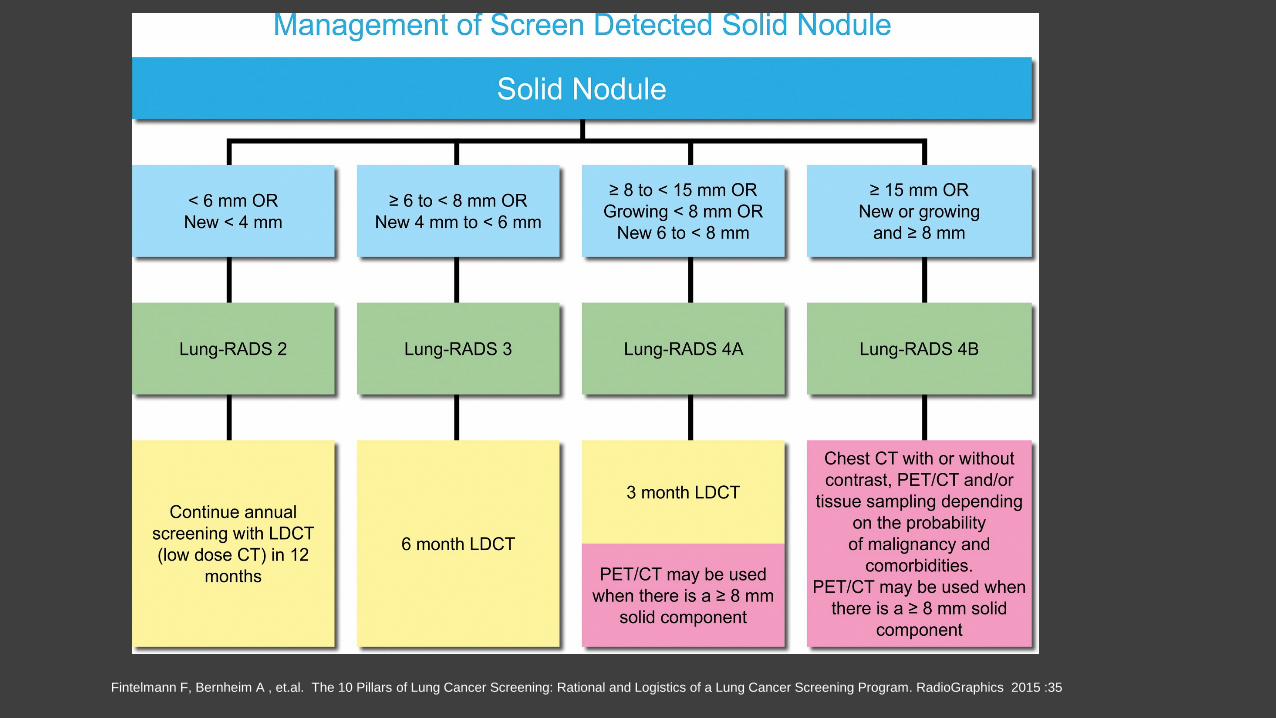
Fintelmann F, Bernheim A , et.al. The 10 Pillars of Lung Cancer Screening: Rational and Logistics of a Lung Cancer Screening Program. RadioGraphics 2015 :35
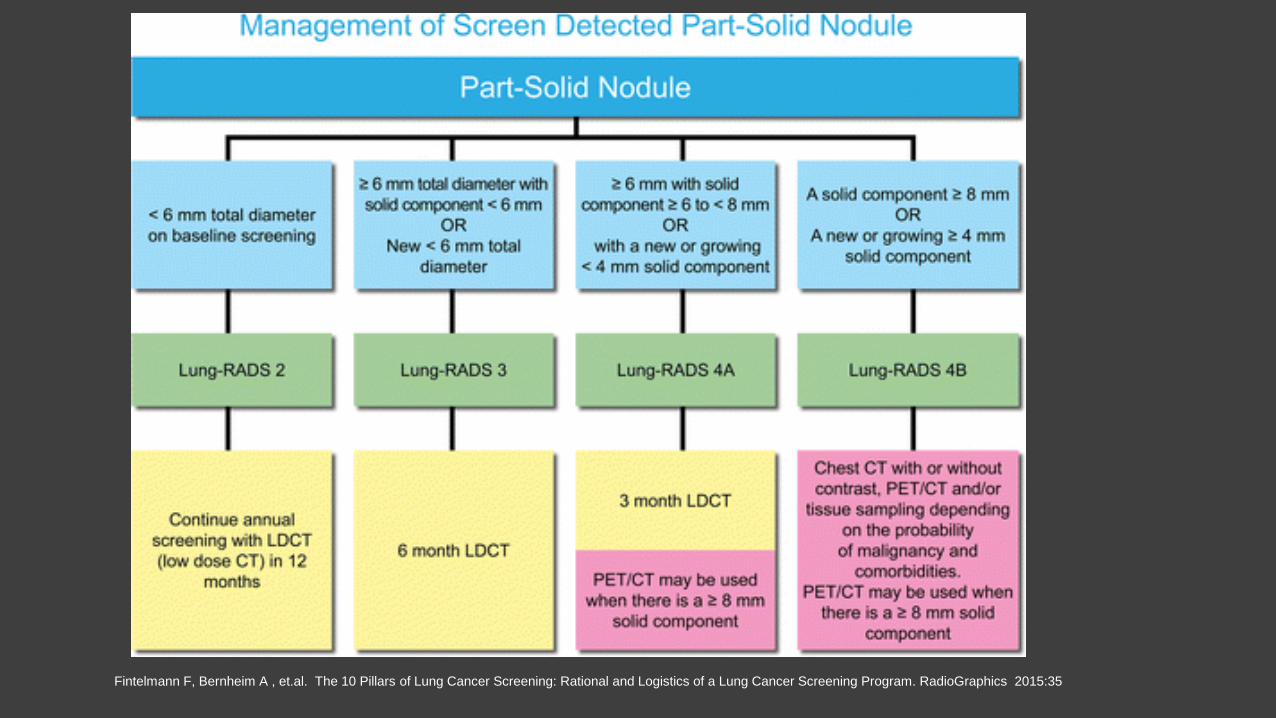
Fintelmann F, Bernheim A , et.al. The 10 Pillars of Lung Cancer Screening: Rational and Logistics of a Lung Cancer Screening Program. RadioGraphics 2015:35
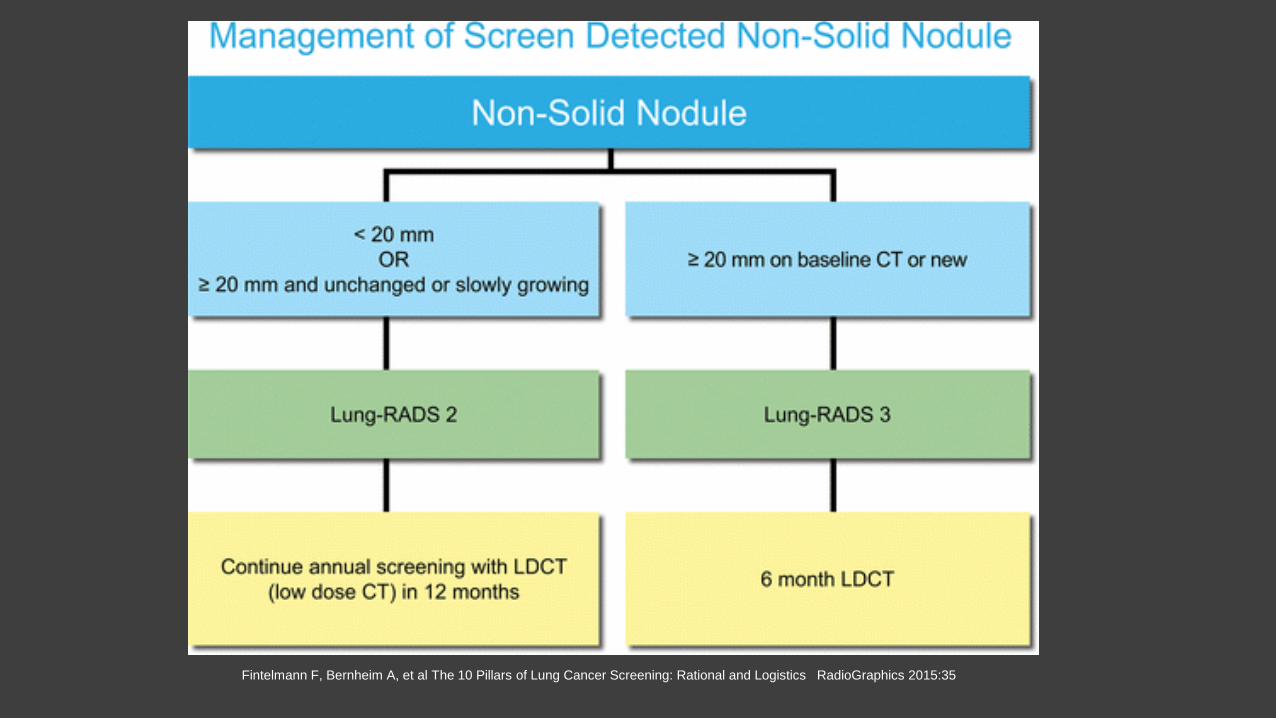
Fintelmann F, Bernheim A, et al The 10 Pillars of Lung Cancer Screening: Rational and Logistics RadioGraphics 2015:35
The Lung Ca Screening CT Report • Standardized Report Template • Nodule Description and other findings • Impression and Recommendations: Management based on
Lung-RADS Assessment categories
• Lung-Rads 1 and 2: Negative. < 1% risk of Malignancy • Lung-Rads 3: Probably Benign. 1-2% risk of Malignancy • Lung-Rads 4A: Suspicious. 5-15% risk of Malignancy • Lung-Rads 4B/4X: Suspicious. >15% risk of Malignancy
“A Negative screen does not mean that an individual does not have lung cancer.” In other words, the presence of only a category 1 or 2 finding on screening CT should not be interpreted as meaning “there is no lung cancer”, but rather that nothing is seen that meets criteria for possible or probable clinically active lung cancer and therefore, continued annual screening should take place.
Follow-up of MMC Screening Patients • Patient presented at Thoracic Oncology Conference if there is a
abnormal finding. • Patients physician’s office is informed of the recommended
follow up. • Lung Navigator will follow up with physician office and patient to
make sure recommended follow up is completed • Patient information is put into the Lung Cancer Registry by Lung
Navigator (Medicare patients). • Lung Navigator may request additional info from physician’s
office to better evaluate the patient.
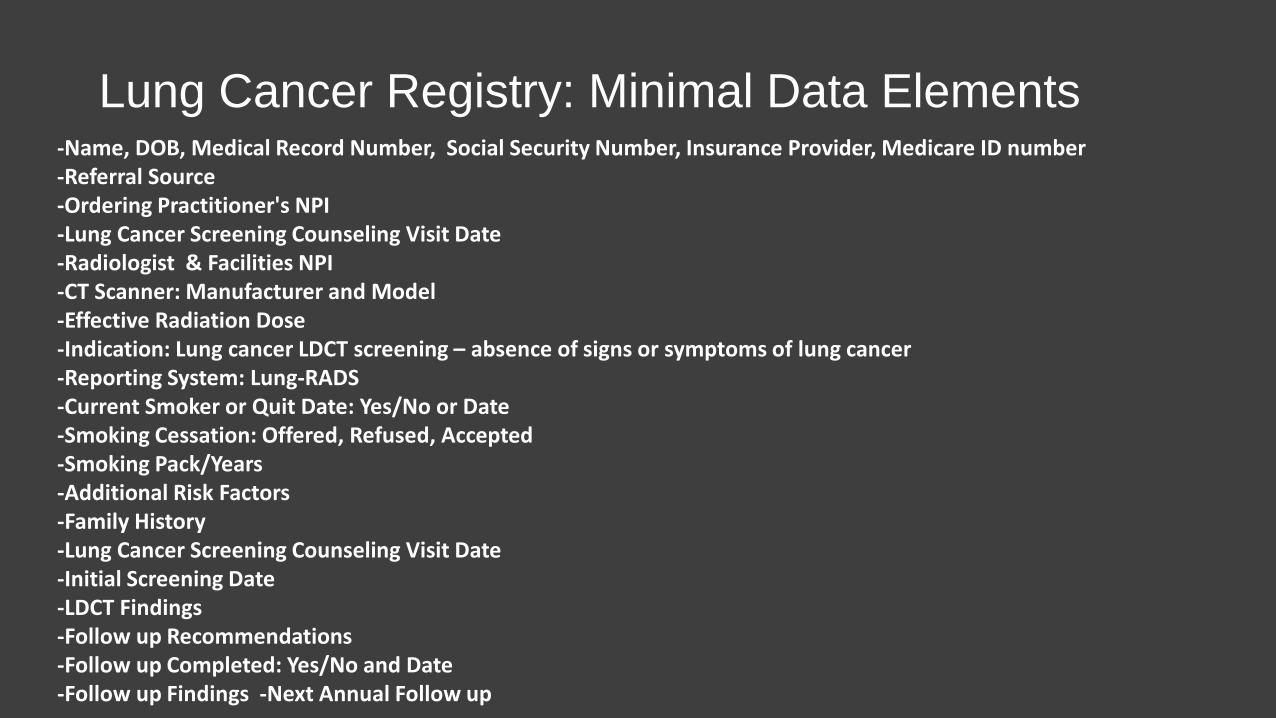
Lung Cancer Registry: Minimal Data Elements -Name, DOB, Medical Record Number, Social Security Number, Insurance Provider, Medicare ID number -Referral Source -Ordering Practitioner's NPI -Lung Cancer Screening Counseling Visit Date -Radiologist & Facilities NPI -CT Scanner: Manufacturer and Model -Effective Radiation Dose -Indication: Lung cancer LDCT screening – absence of signs or symptoms of lung cancer -Reporting System: Lung-RADS -Current Smoker or Quit Date: Yes/No or Date -Smoking Cessation: Offered, Refused, Accepted -Smoking Pack/Years -Additional Risk Factors -Family History -Lung Cancer Screening Counseling Visit Date -Initial Screening Date -LDCT Findings -Follow up Recommendations -Follow up Completed: Yes/No and Date -Follow up Findings -Next Annual Follow up
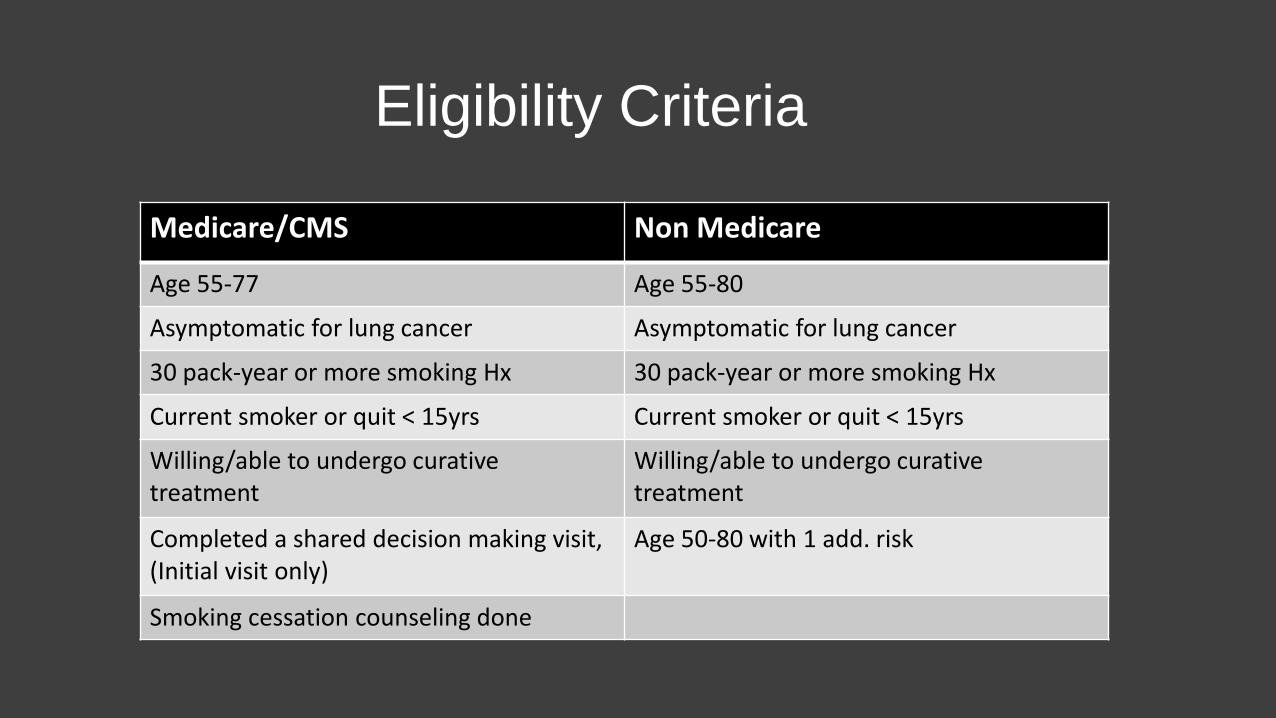
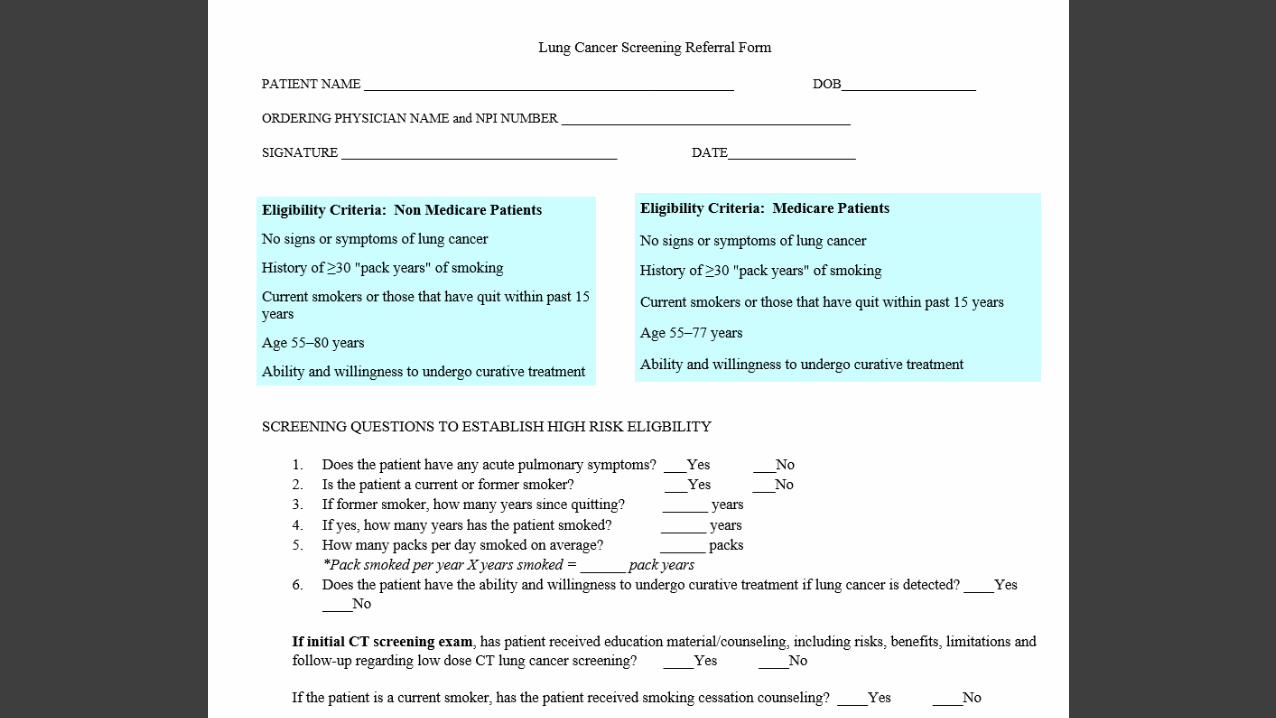
Eligibility Criteria
Medicare/CMS Non Medicare Age 55-77 Age 55-80 Asymptomatic for lung cancer Asymptomatic for lung cancer 30 pack-year or more smoking Hx 30 pack-year or more smoking Hx Current smoker or quit < 15yrs Current smoker or quit < 15yrs Willing/able to undergo curative treatment
Willing/able to undergo curative treatment
Completed a shared decision making visit, (Initial visit only)
Age 50-80 with 1 add. risk
Smoking cessation counseling done
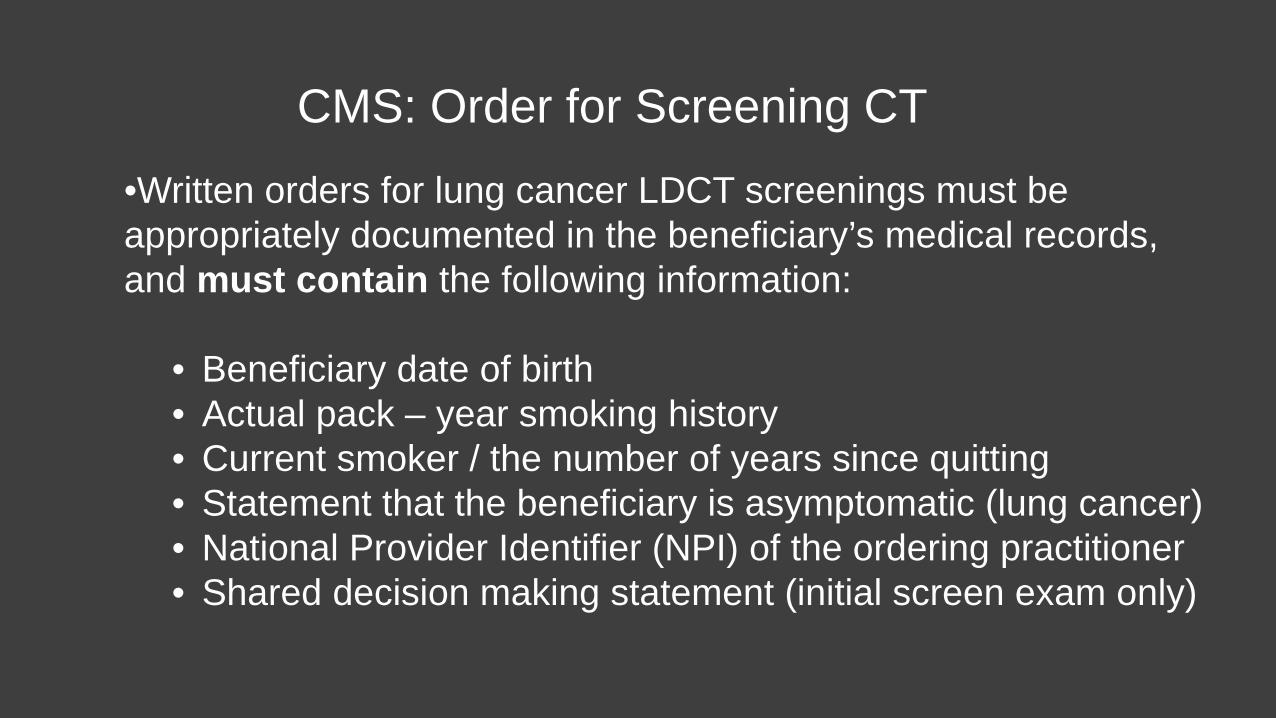
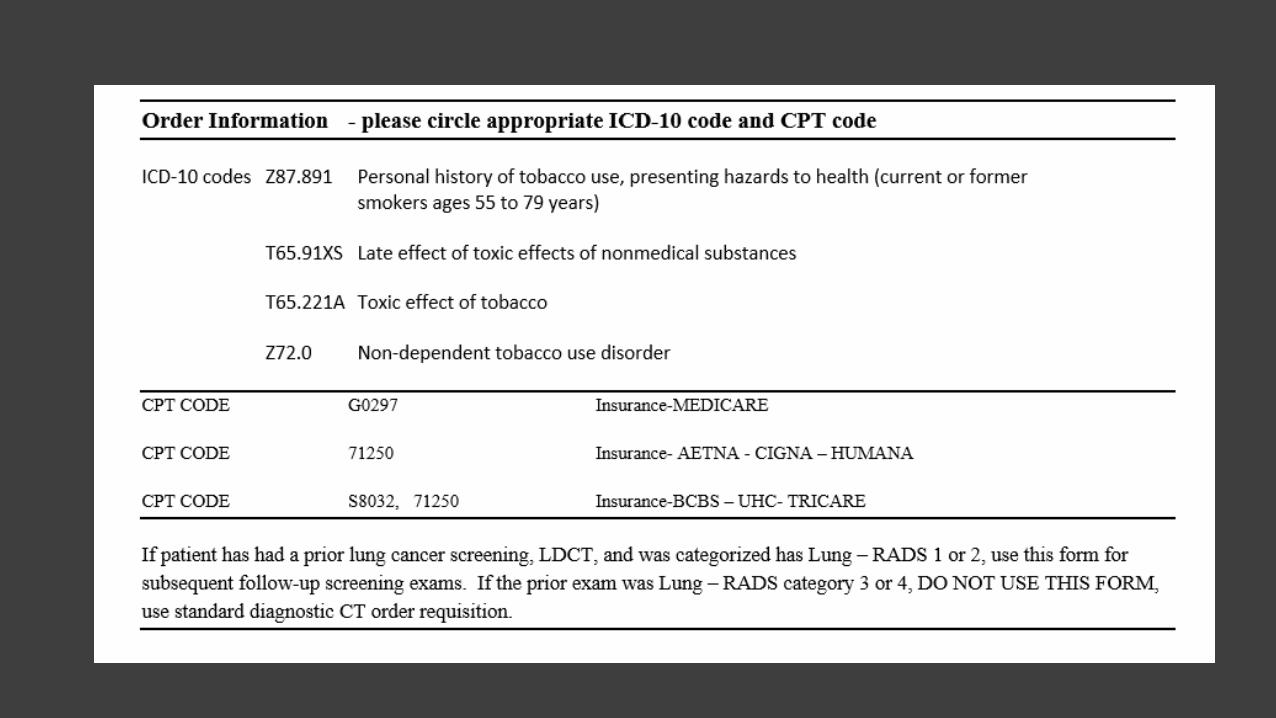
CMS: Order for Screening CT
•Written orders for lung cancer LDCT screenings must be appropriately documented in the beneficiary’s medical records, and must contain the following information:
• Beneficiary date of birth • Actual pack – year smoking history • Current smoker / the number of years since quitting • Statement that the beneficiary is asymptomatic (lung cancer) • National Provider Identifier (NPI) of the ordering practitioner • Shared decision making statement (initial screen exam only)
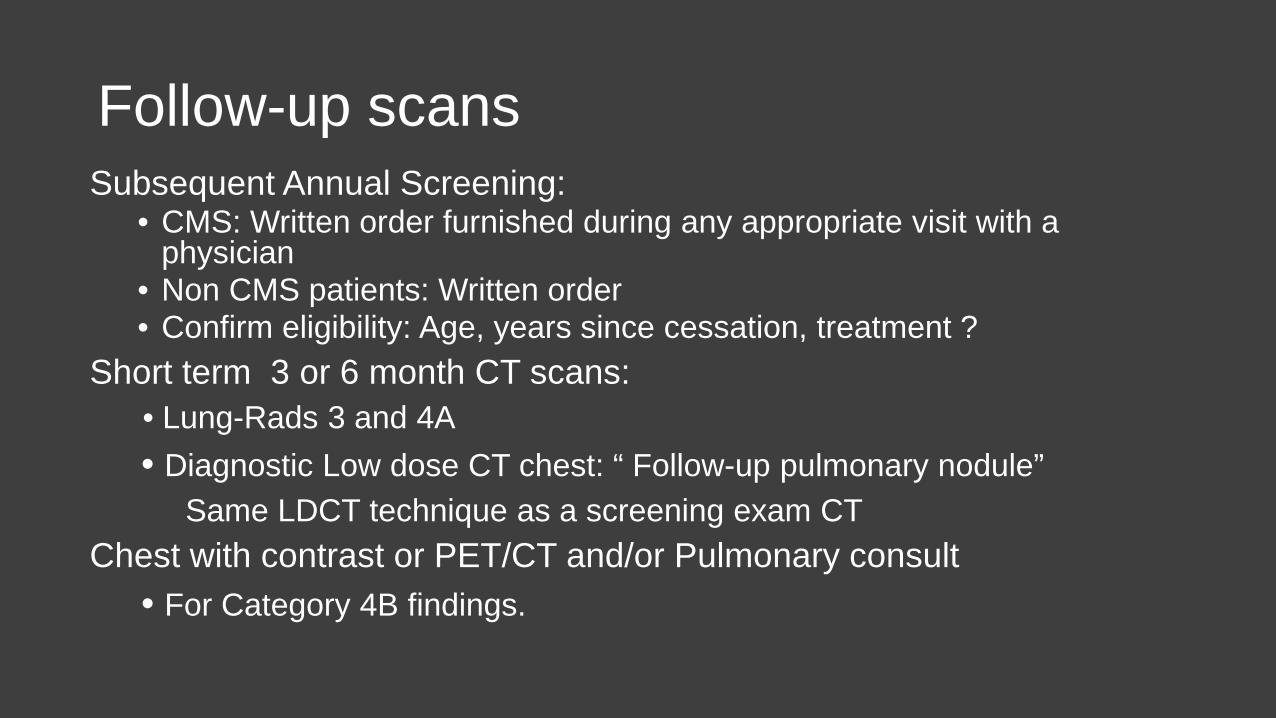
Follow-up scans Subsequent Annual Screening:
• CMS: Written order furnished during any appropriate visit with a physician
• Non CMS patients: Written order • Confirm eligibility: Age, years since cessation, treatment ?
Short term 3 or 6 month CT scans: • Lung-Rads 3 and 4A • Diagnostic Low dose CT chest: “ Follow-up pulmonary nodule” Same LDCT technique as a screening exam CT Chest with contrast or PET/CT and/or Pulmonary consult • For Category 4B findings.
Counseling and Shared Decision Making Visit •Must be furnished by a physician or qualified non-physician practitioner (meaning a physician assistant, nurse practitioner, or clinical nurse specialist).
•Must include all of the following elements: • Determination of beneficiary eligibility including age, absence of signs or symptoms of lung
cancer, a specific calculation of cigarette smoking pack-years; and if a former smoker, the number of years since quitting;
• Shared decision making, including the use of one or more decision aids, to include benefits and harms of screening, follow-up diagnostic testing, over-diagnosis, false positive rate, total radiation exposure and not all patients with screen detected lung cancer will avoid death
• Counseling on the importance of adherence to annual lung cancer LDCT screening, impact of comorbidities and ability or willingness to undergo diagnosis and treatment
• Counseling on the importance of maintaining cigarette smoking abstinence if former smoker; or the importance of smoking cessation if current smoker and, if appropriate, furnishing of information about tobacco cessation interventions
Counseling and Shared Decision Making Visit
• G0296 – Counseling visit to discuss need for lung cancer screening (LDCT) using low dose CT scan (service is for eligibility determination and shared decision making).
•Proposed RVU: 0.52 • Z87.891(ICD-10) Personal history of tobacco use/nicotine
dependence •May be billed on same day as an E&M visit ?? Use -25 modifier?
Counseling and Shared Decision Making
• Resources University of Michigan http://www.shouldiscreen.com
American Thoracic Society http://www.thoracic.org/patients/patient- resources/resources/decision-aid-lcs.pdf • Handout
Smoking Cessation • $25 billion state and federal tobacco tax collected annually,
~2% spent on promoting cessation • ~ 70% of smokers want to quit • Pharmacologic agents covered by some insurers • 1-800-QUIT-NOW (CDC) • http://www.tobaccofreeflorida.com • 1-800-LUNGUSA
Future Directions of Lung Cancer Screening
• Smoking Cessation: Long term solution to 80% of Lung Ca • Eligibility: Better selection, molecular markers ( miR-Test) • Lower CT Dose • Reduce False Positives: Volumetric analysis/CAD • Quantitative Coronary Calcification Scoring





























