Embed Size (px)
Citation preview
CULTURAL COMPETENCE IN
DERMATOLOGYLindsey Lawrence, PA-S

INTRODUCTION The purpose of my literature review is to bring awareness to the gaps in the education that practitioners receive with regards to dermatology and ethnic populations.
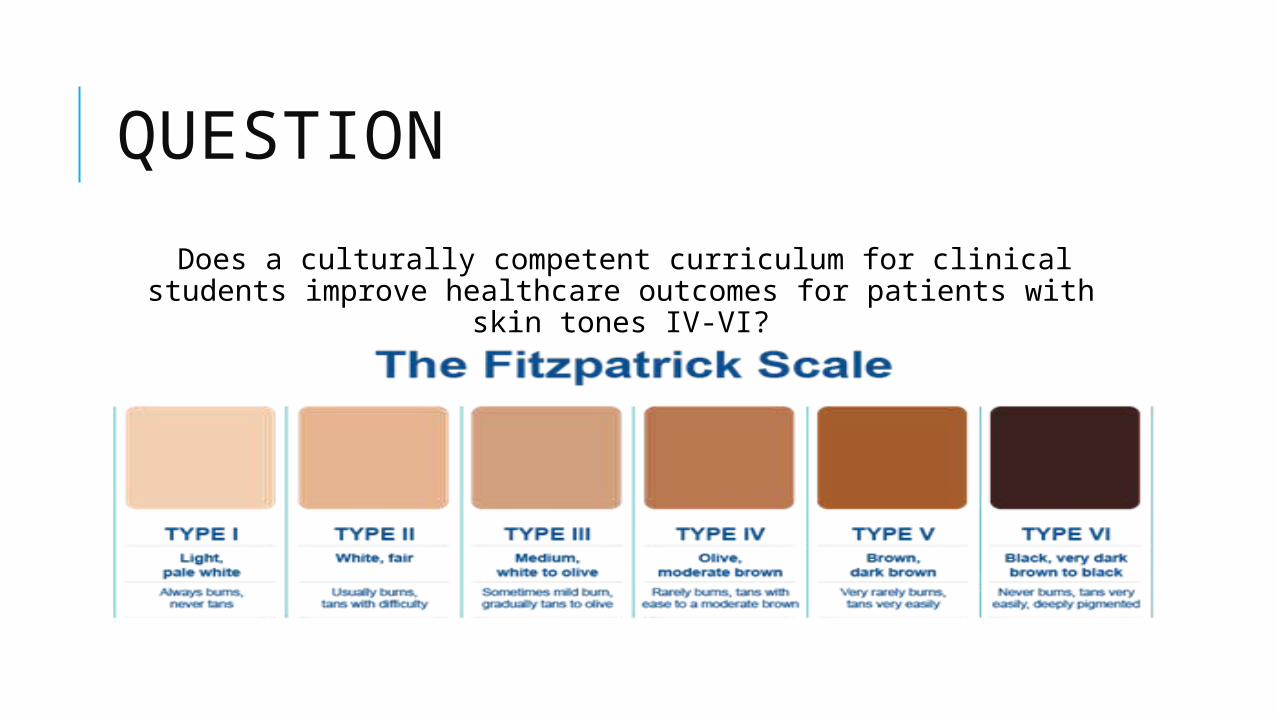
QUESTION Does a culturally competent curriculum for clinical students
improve healthcare outcomes for patients with skin tones IV-VI?
METHODOLOGYMy literature review covered the following topics:
- summarizing dermatologic education and training- detailing the usage of primary care for skin disease- cultural competence- the cost of dermatologic healthcare- patient education
Search terms: Health care disparities, Healthcare inequities, Dermatology, cultural competence, dermatology in primary care, ethnicities, race, dermatology in emergency care, dermatology education, skin cancer, ethnic dermatology
Inclusion: Skin types IV-VI, Exclusion: Skin types I-III and Articles not in English Databases: PubMed, Google Scholarly Articles, peer-reviewed articles, online magazines, government websites and databases
DEFINITIONS Acral Lentiginous Melanoma (ALM) Breslow Depth Cultural Competence Fitzpatrick Skin Phototypescale/Fitzpatrick Scale Malignant Melanoma (MM)/Melanoma
BACKGROUND The average medical school student spends about 20.5 classroom hours on dermatology (Drucker et al., 2013)
The top five most common skin diseases seen by non-dermatologists are: contact dermatitis, cellulitis/abscess, rash, epidermoid cyst and tinea (Wilmer et al., 2014)
Dermatologists treat only 30%–40% of patients with skin disease (Awadalla et al., 2008)
The mean wait time for a new patient visit to a dermatologist is approximately 33 days (Jack et al., 2011)
47% of dermatologists and dermatology residents reported that their medical training was inadequate in training them on skin conditions in blacks (Buster et al., 2012)

LITERATURE REVIEW
SKIN CANCER RISK PERCEPTIONS: A COMPARISON ACROSS ETHNICITY, AGE, EDUCATION, GENDER, AND INCOME
Objective: We evaluated skin cancer (SC) risk perceptions across race and other demographic markers and compared them to discover differences in perception that may contribute to the disparities in SC diagnosis and treatment.
Methods: Respondents with no history of SC were randomly selected to answer questions assessing perceived risk and knowledge of preventive strategies of SC.
Results: Blacks, the elderly, and people with less education perceived themselves as at lower risk of developing SC.
Conclusion: Uncertainty and altered perceptions are more common in the SC risk perceptions of ethnic minorities, the elderly, and those with less education.
MALIGNANT MELANOMA IN PIGMENTED SKIN: DOES THE CURRENT INTERVENTIONAL MODEL FIT A DIFFERENT CLINICAL, HISTOLOGIC, AND MOLECULAR ENTITY? BACKGROUND Although the incidence of malignant melanoma in African Americans is considerably lower than in Caucasians, African Americans have a less-favorable prognosis related to later presentation and more deeply invasive lesions at diagnosis
OBJECTIVE To review the current literature addressing the specific clinical, histopathologic, and molecular features of melanoma in darkly pigmented individuals
RESULTS Several studies have suggested differences between lightly and darkly pigmented populations with regard to clinicopathologic character and the underlying genetic processes affecting its pathogenesis.
CONCLUSION Such research may help to ameliorate the disparities in melanoma outcomes through improved screening, public health measures aimed at prevention, and potentially novel targeted therapeutic approaches.
DERMATOLOGIC DISEASE IN FAMILY MEDICINE Background and Objectives: Because dermatologic complaints are encountered frequently in primary care, the education of PCPs about skin disorders is important
Methods: Study researchers analyzed the National Ambulatory Medical Care Survey data from 2002 to 2005 for dermatologic diagnoses and most common prescriptions by family physicians. The data from 2002–2005 were compared to data from 1990–1994
Results: Skin conditions accounted for 8% of all visits to family physicians in 2002–2005
Conclusions: Family physicians diagnose a wide range of skin disorders and prescribe drugs to treat them. Family physicians make more dermatologic diagnoses and prescribe more treatments than previously
TEACHING DERMATOLOGY TO INTERNAL MEDICINE RESIDENTS: NEEDS ASSESSMENT SURVEY AND POSSIBLE DIRECTIONS Background: Internal medicine trainees receive limited teaching and training in dermatology and may feel inadequately prepared to assess and manage patients with dermatologic complaints.
Objective: To determine internal medicine residents’ comfort in assessing and managing dermatologic issues and their educational needs in dermatology.
Methods: An electronic survey was conducted of first-, second-, and third-year internal medicine residents at the University of Toronto.
Results: Fifty-four of 186 internal medicine trainees responded to our survey (response rate 5 29%). Each respondent did not answer every question. Residents were generally uncomfortable or very uncomfortable assessing and managing dermatologic issues in the emergency department (40 of 47, 85%), ward or intensive care unit (39 of 47, 83%), and ambulatory clinic (40 of 47, 85%).
Conclusions: An effort should be made to increase the availability of relevant dermatology teaching and clinical exposures for internal medicine residents.
MEDICAL SCHOOL DERMATOLOGY CURRICULUM: ARE WE ADEQUATELY PREPARING PRIMARY CARE PHYSICIANS? Background: There is a lack of information regarding the dermatology learning needs of primary care physicians and residents.
Objective: To determine dermatologic topics that primary care physicians consider important and to determine primary care residents’ ratings of the teaching adequacy of these topics in the undergraduate medical curriculum.
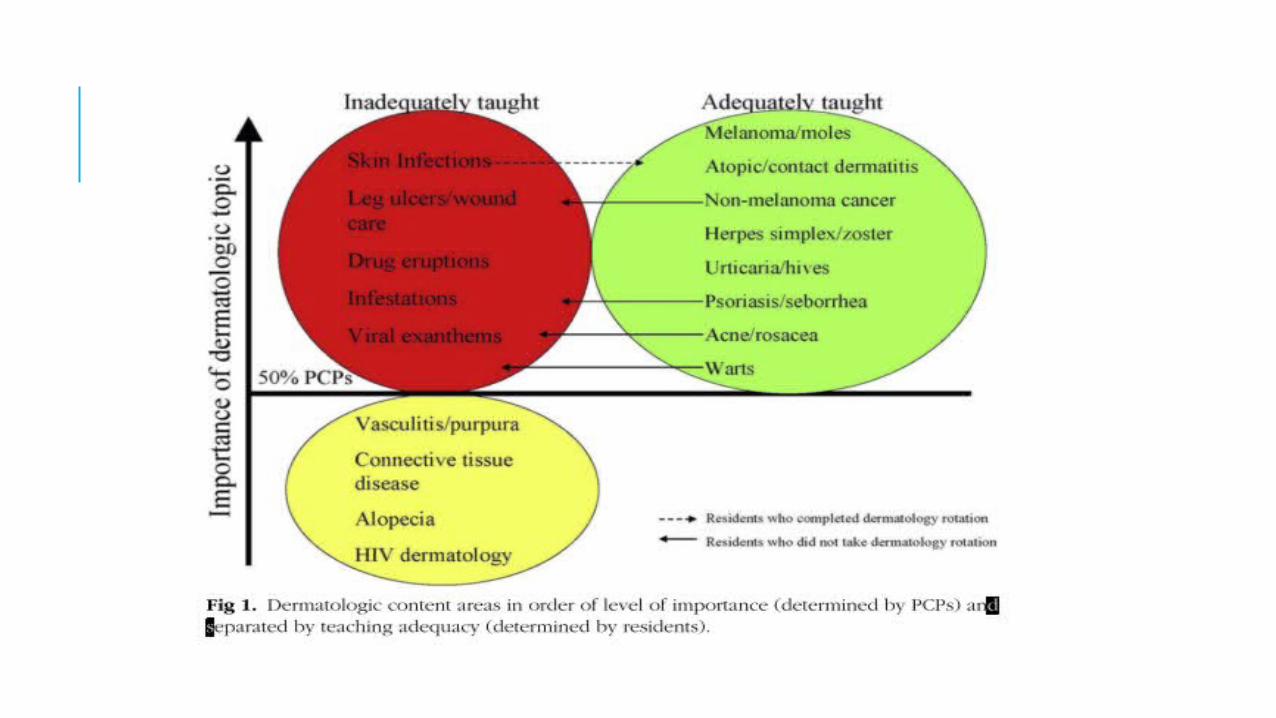
Methods: Primary care physicians and residents were surveyed regarding the importance and teaching adequacy of 17 dermatologic content areas
Conclusion: Seventeen content areas can be divided into 3 categories: dermatologic topics that are important and adequately taught, topics that are unimportant, and a group of important, yet inadequately taught content areas. This latter group should be further integrated into dermatology curricula at U.S. medical schools.
SKIN OF COLOR – A BASIC OUTLINE Darker skin differs from white skin in presentation, a tendency toward pronounced scarring, and pathophysiology of skin diseases common to those with skin of color.
Recent studies highlight differences beyond the surface, which include issues of treatment, scar formation, collagen production, basic structure, and skin cancer development.
Cultural Competence: being familiar with the healthcare beliefs, practices and needs of diverse patients in order to close the gap in healthcare outcomes
THE BURDEN OF SKIN DISEASES:A JOINT PROJECT OF THE AMERICAN ACADEMY OF DERMATOLOGY ASSOCIATION AND THE SOCIETY FOR INVESTIGATIVE DERMATOLOGYBackground: Skin disease is one of the top 15 groups of medical conditions for which prevalence and health care spending increased the most between 1987 and 2000Objective: This study closes the gap by estimating the prevalence, economic burden, and impact on quality of life for 22 leading categories of skin disease.Method: Data for estimating the clinical and economic burden of skin diseases were obtained primarily from several nationally representative public and private databases, including the National Health Interview Survey (NHIS), the National Ambulatory Medical Care Survey, the National Hospital Ambulatory Medical Care Survey (NHAMCS), and the Surveillance, Epidemiology, and End Results database of the National Cancer Institute (NCI)Conclusion: Many of the 22 categories of skin disease addressed here disproportionately affect women, minorities, and the elderly in their prevalence, severity, and costs. Also disproportionately affected are those without health insurance coverage or who lack access to health care services because of socioeconomic status or other factors.
THE COST OF INITIATING APPROPRIATE THERAPY FORSKIN DISEASES: A COMPARISON OF DERMATOLOGISTS AND FAMILY PHYSICIANS
A prospective survey examining how forty-one dermatologists and forty-one family practitioners manage patients with skin diseases.
The results show that dermatologists diagnose more conditions accurately, refer patients less often, charge more in professional fees, prescribe more medicines at higher cost to the patient but order laboratory tests costing less than do family physicians.
LIMITATIONS OF RESEARCH There is little research on the adequacy of current dermatologic training to produce dermatologists with cross cultural competence, confidence, and skill in treating patients from diverse backgrounds.
A PubMed search of the terms dermatology, residency, and education reveals just 1 manuscript since 2000 that addresses residency training and ethnic skin
There is also very little research that has been done that includes ethnic populations as part of the test groups for common dermatologic conditions
AREAS FOR FURTHER RESEARCH Didactic Education Multi-tonal photos
References and Presentations Discussion
Clinical Education Increased exposure to rotations
diverse patient populations Confidence Surveys
Clinicians and Patients
WHY IS THIS IMPORTANT FOR ME AS A PA? The importance of cultural competence for physician assistants entering and currently in the field is that PA’s are the future of primary care.
Growing DiversityFinancialPatient SatisfactionProvider Time
CONCLUSION Cultural competency is an important and growing facet of American healthcare. You cannot treat effectively a person you don’t understand. If patients don’t trust that you understand them and can help them they will find a practitioner that does.
REFERENCES Alexandrescu, D. T., Maslin, B., Kauffman, C. L., Ichim, T. E., & Dasanu, C. A. (2013). Malignant melanoma in pigmented skin: does the current interventional model fit a different clinical, histologic, and molecular entity? Dermatol Surg, 39(9), 1291-1303. doi: 10.1111/dsu.12251
Awadalla, F., Rosenbaum, D. A., Camacho, F., Fleischer, A. B., Jr., & Feldman, S. R. (2008). Dermatologic disease in family medicine. Fam Med, 40(7), 507-511.
Bickers, D. R., Lim, H. W., Margolis, D., Weinstock, M. A., Goodman, C., Faulkner, E., . . . Dall, T. (2006). The burden of skin diseases: 2004 a joint project of the American Academy of Dermatology Association and the Society for Investigative Dermatology. J Am Acad Dermatol, 55(3), 490-500. doi: 10.1016/j.jaad.2006.05.048
Buster, K. J., You, Z., Fouad, M., & Elmets, C. (2012). Skin cancer risk perceptions: a comparison across ethnicity, age, education, gender, and income. J Am Acad Dermatol, 66(5), 771-779. doi: 10.1016/j.jaad.2011.05.021
Clark, R. A., & Rietschel, R. L. (1983). The cost of initiating appropriate therapy for skin diseases: a comparison of dermatologists and family physicians. J Am Acad Dermatol, 9(5), 787-796.
Czerkasij, V. (2013). Skin of color: a basic outline of unique differences. Nurse Pract, 38(5), 34-40; quiz 40-31. doi: 10.1097/01.npr.0000428813.26762.66
Drucker, A. M., Cavalcanti, R. B., Wong, B. M., & Walsh, S. R. (2013). Teaching dermatology to internal medicine residents: needs assessment survey and possible directions. J Cutan Med Surg, 17(1), 39-45.
Hansra, N. K., O'Sullivan, P., Chen, C. L., & Berger, T. G. (2009). Medical school dermatology curriculum: are we adequately preparing primary care physicians? J Am Acad Dermatol, 61(1), 23-29.e21. doi: 10.1016/j.jaad.2008.11.912
Jack, A. R., Spence, A. A., Nichols, B. J., Chong, S., Williams, D. T., Swadron, S. P., & Peng, D. H. (2011). Cutaneous conditions leading to dermatology consultations in the emergency department. West J Emerg Med, 12(4), 551-555. doi: 10.5811/westjem.2010.4.1653
Ramsay, D. L., & Weary, P. E. (1996). Primary care in dermatology: whose role should it be? J Am Acad Dermatol, 35(6), 1005-1008. Wilmer, E. N., Gustafson, C. J., Ahn, C. S., Davis, S. A., Feldman, S. R., & Huang, W. W. (2014). Most common dermatologic conditions encountered by dermatologists and nondermatologists. Cutis, 94(6), 285-292.
QUESTIONS?