Embed Size (px)
Citation preview

Optometry (2010) 81, 157-161
Current treatment for vitreous floaters
David P. Sendrowski, O.D.,a and Mark A. Bronstein, M.D.b
aSouthern California College of Optometry, Fullerton, California; and bUCI Medical School, lrvine, California.
KEYWORDS Abstract Vitreous floaters are a common complaint in the ophthalmic care setting. Patients seek
Co
Ca
152
doi
Vitreous floaters;YAG laser;Vitreolysis;
Vitrectomyexplanation and advice regarding possible treatment options. Because the condition is considered be-nign, ophthalmic care practitioners have little to offer regarding treatment options. The majority ofcases encountered are managed with patient education and reassurance. Although almost all patientsaccept the conservative management option, there is a small subset of patients who may desire a moreaggressive treatment intervention for resolution of their visual symptoms. Information with regard totreatment options is readily available to patients through Internet searches and non–peer reviewed ed-ucational Web sites. The risks and benefits for these treatment options are not fully covered. Manage-ment of floaters should include education regarding ‘‘off-label’’ procedures as well as discussion aboutbenefits and risks associated with such treatment options. It is vital that eye care practitioners adviseand counsel patients with symptomatic floaters for optimum ocular health care. This article reviews thecurrent conventional and ‘‘off-label’’ treatment options for symptomatic patients with vitreous floaters.Optometry 2010;81:157-161
Vitreous: structure and function
To understand the symptomology of floaters one mustbecome refamiliarized with the basic structure of thehuman vitreous. The vitreous is composed primarily ofwater. Collagen is an important structural protein in thevitreous.1 Many different types of collagen are found in thehuman vitreous; type II collagen, a homotrimer composedof 3 identical alpha chains, comprises 75% of the total col-lagen in the structure.1 The vitreous body is also composedof a group of noncollagenous structural proteins.2,3 Colla-gen filaments and hyaluronic acid (HA) comprise the solidcomponent of the vitreous gel.3 The ability of HA to retainwater molecules is an important factor in maintaining thegel consistency of the vitreous.
Corresponding author: David P. Sendrowski, O.D., Southern California
llege of Optometry, Ocular Disease, 2575 Yorba Linda Blvd., Fullerton,
lifornia 92831.
E-mail: [email protected]
9-1839/10/$ -see front matter � 2010 American Optometric Association. Al
:10.1016/j.optm.2009.09.018
One of the more common age-related events occurring inthe vitreous is a posterior vitreous detachment (PVD).Complete PVD can be defined as a separation between theposterior vitreous cortex and the internal limiting lamina(ILL) of the retina.4,5 The separation can be localized, partial,or total (complete) in nature. The optometric clinician shoulddistinguish the complete PVD from other forms of vitreousseparation, because the increased likelihood of ocular mor-bidity (retina breaks or tears) exists with partial or focal PVD.
Over the years, much has been learned about theepidemiology, pathogenesis, and the sequelae of a PVD.About half the patients with PVD are over age 50 with twothirds of patients having experienced the event by age 65.6
Several studies have found a higher incidence of PVD inwomen, a finding that suggests hormonal changes aftermenopause as a possible contributing factor to the PVD, af-fecting the biochemical components of the vitreous.7,8 Onestudy found that high estrogen levels were found to be pro-tective against PVD and that lowered estrogen levels asso-ciated with menopause may lead to changes in the vitreous,
l rights reserved.

158 Optometry, Vol 81, No 3, March 2010
predisposing an individual to a PVD. Higher levels of vita-min B6 were also associated with the development of PVDin premenopausal women, which may be attributed to anantiestrogen effect from that vitamin.8
The pathogenesis of a PVD results from9 liquid vitreousformation and destabilized collagen fibrils, both related toage. This destabilization, along with rotational eye move-ments, causes syneresis and collapse of the vitreous body.The volume displacement from the central vitreous to thesubretinal space creates separation of the vitreous fromthe ILL, typically located at the posterior pole near or atthe optic disc.10-12 HA depolymerizes with age and meta-bolic and environmental stress. This depolymerizationcauses HA to release water molecules and to ultimatelyform lacunae (pockets or localized areas of liquefied vitre-ous). Collagen filaments aggregate to form larger fibrils,which, in turn, cause further collapse of the vitreous struc-ture. Collagen fibrils may float in these lacunae giving thepatient the perception of floaters.
Balazs et al.13 found evidence of liquid vitreous occur-ring as early as age 4 and observed that by the time the hu-man eye reaches its adult size (ages 14 to 18) up to 12.5% ofthe total vitreous volume consists of liquid vitreous. Thus,the speed at which vitreous liquefies can vary dependingon the HA and collagen interaction, oxidative effects, andvarying degrees of light exposure as the patient ages.14
Formation of vitreous floaters
In the younger patient, collagen aggregates into fibrils andmobilizes in lacunae and is associated with floater sympto-mology. These floaters tend to be fewer in number andmore linear in form in comparison with older patients.Location along the visual axis produces the greatest visualdiscomfort. Thus, vitreous floaters can occur with orwithout the advent of a PVD. The onset of floaters in aneye with an attached vitreous suggests degenerative orpathologic changes associated with the vitreous body’sultrastructure or the result of cellular or acellular materialintroduced into the vitreous.9,10,13
Refractive etiologies, such as axial myopia, are associ-ated typically with a liquefied vitreous observed amongyoung patients with floater symptomology. Younger pa-tients between the ages of 20 and 50 who have moderatemyopia were found to manifest vitreous liquefaction andPVDs sooner than their age-matched counterparts whowere emmetropic or hyperopic.13 Vitreous liquefaction hasbeen found to be greater in myopes of 6 diopters or more.13
Other pathologic changes associated with vitreous liq-uefaction and structural integrity loss in a younger patientinclude Marfan’s, Ehlers-Danlos, and Stickler’s syndromesand diabetic vitreoretinopathy (secondary to elevated levelsof glucose).
Floater symptomology in older patients usually presentswith floaters that move with vitreous displacement duringnormal eye movement and scatter incident light,15 casting a
shadow on the retina that is perceived by the patient as agrey, silhouettelike object(s) or a ‘‘spider web–like’’ imagethat moves across the visual plane. Patients typically con-vey that these floaters move rapidly in the visual planewhen they attempt to focus on them.15 Uniform back-grounds such as a clear blue sky or white wall allow betterperception of these vitreous floaters. Patients should be toldto expect the floaters to become more prominent with thesebackground conditions.
In addition, floater symptomology may be related to anewly formed PVD, which scatters light and casts varyingdegrees of shadows on the retina. This phenomenon iscreated by glial tissue of papillary origin that has adhered tothe posterior vitreous cortex,16 known as a Weiss Ring (seeFigure 1). A patient complaining of acute floaters with orwithout the presence of an associated Weiss Ring requiresa dilated fundus examination to evaluate for possible retinalhemorrhage, retinal breaks, or detachment induced by thevitreous separation.17
Because a sudden onset of vitreous floaters in eitheryoung or older patients may also be associated with severalretinal conditions, such as a retinal detachment, retinalbreak(s), preretinal or vitreous hemorrhage, retinal vascu-lopathies (ie., proliferative diabetic retinopathy), and pos-terior uveitis, a comprehensive dilated fundus evaluation isa necessity in all cases.
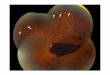
Patients with benign symptomatic floaters do not usuallycomplain about a dramatic loss of vision or visual acuitywhen the floater interrupts the visual axis. There are rareexceptions in which the floater is exceptionally large or ispositioned on or near the patient’s visual axis or line ofsight. Figure 2 represents a large pigmented floater presentin a patient who showed visual acuity loss when the vitre-ous floater obscured the visual axis. These types of vitreousfloaters are rare but may require further management,which may include alternate treatment options.
Conventional therapy
Conventional management of most vitreous floaters typi-cally requires only reassurance and education. Explanationof the visual phenomenon should be given to the patientalong with the doctors’ advice for follow-up care. In thepresence of a symptomatic acute PVD, the patient shouldbe re-evaluated with a dilated fundus examination period-ically until the symptoms or vitreous traction has subsided.(2 weeks to 3 months depending on accompanying symp-toms of photopsia).5
A complicated PVD associated with either Shafer’s Sign(tobacco dust sign) or preretinal/vitreous hemorrhage war-rants a more careful dilated fundus examination, because anincreased risk of retinal break or detachment exists. If noretinal break or detachment is noted, a retinal consult orclose follow-ups with dilated fundus examination should beconsidered. All patients should be advised of the signs andsymptoms of an associated retinal detachment. These may

Figure 1 The appearance of a Weiss Ring usually indicates a fresh pos-
terior vitreous detachment. This patient had a sudden onset of a floater in
their vision with associated posterior vitreous detachment.
Figure 2 A large congenital vitreous floater located in the central vi-
sual axis of the patient’s eye. Encapsulated primary vitreous that became
dislodged later in life. Movement of the floater across the visual axis
caused temporary loss of visual acuity and distortion.
Sendrowski and Bronstein Review Article 159
include, but are not limited to, an increase in floaters orflashes or an appearance of a persistent curtain or shadow inthe field of vision. Patients need to be told to return to theoffice immediately if any of these symptoms occur.
The symptomatic floater patient should be given time togenerate questions of concern and, in rare cases, options forsecondary treatment should be discussed. If secondarytreatment is requested, advice should include the risksand benefits of each treatment option along with recom-mendations for a second opinion.
‘‘Off-label’’ treatment options for floaters
Laser therapy
The yttirum aluminum garnet (YAG) laser has become ac-cepted as ‘‘the standard of care’’ for many ophthalmic sur-geries. Yet, the use of the YAG for treatment of vitreousfloaters has not been accepted widely by the ophthalmicprofession and remains an ‘‘off label’’ treatment optionfor select cases. It is critical in these selected cases thatthe doctor and patient have an open and frank discussion re-garding the off-label YAG treatment for floaters. Patientshave access to vast amounts of information through the in-ternet. With regard to vitreous floaters, many of these sitesdo offer patients an ‘‘option,’’ both laser and surgical, toremedy their visual symptoms. These remedies are notwell described, and complications are rarely discussed.Thus, education is critical.
There is little clinical research utilizing a YAG for thetreatment of vitreous floaters and its impact on patient’ssymptoms. One study performed by Tsai et al., reported theuse of a YAG laser to treat vitreous floaters in one eye ofpatients with severe psychological reactions to the vitreous
floaters.18 The Tsai group18 treated 15 patients who met thefollowing criteria for laser treatment: floaters caused by lo-calized vitreous opacities; symptoms persisted for at least3 months without evidence of regression; patients sufferedfrom fear, depression, or anxiety; and patients had a strongdesire for a fast cure. None of the patients had a history ofretinal detachment, diabetic retinopathy, or any retinal dis-eases.18 Each patient had a thorough preoperative ophthal-mic examination, which included a binocular indirectophthalmoscopic examination with scleral depression 360�
to rule out retinal breaks or tears. The study concluded thatall patients were satisfied with their YAG treatment duringa 12-month follow-up, and no patients showed any signifi-cant visual deterioration or recurrence of their subjectivefloaters.18 This study included only 15 highly motivated pa-tients, making it hard to draw sound clinical conclusions.
In a later study by Delaney et al., 42 eyes of 31 patientswere enrolled in 2 treatment groups: a YAG laser group anda surgical (pars plana vitrectomy) group.19 Preoperative ex-amination of the vitreous and retina was performed to con-firm the presence of a complete PVD to determine theposition of the vitreous opacity and to exclude any coexist-ing retinal disease. Laser treatment was not undertaken ifthe vitreous floater was located within 2 mm of the retinaor the crystalline lens. At the end of their treatment, all la-ser vitreolysis (noninvasive photodisruption of vitreousstrands, floaters, or adhesion bands) patients were given aquestionnaire asking them to choose 1 of 4 postoperativeassessments. Assessments included: failure, partial success,significant success, and complete success. In no eye was la-ser treatment 100% successful in eliminating symptoms.Results showed only 15 eyes benefited to some measurein that patients felt that the moderate benefit gained fromlaser vitreolysis of the vitreous floaters was adequate in

Figure 3 Before and after 23-gauge microincisional vitrectomy. Patient had asteroid hyalosis, which made the evaluation of the wet age-related macular
degeneration difficult and required vitrectomy to better monitor the condition.
160 Optometry, Vol 81, No 3, March 2010
relieving symptoms so as to alleviate the need for furthersurgery.19 Clinical improvement for most patients wasonly moderate in degree. None of the subjects reported acomplete resolution of symptoms. In fact, 7.7% of the pa-tients had a worsening of symptoms after their laser treat-ment. There were no ocular complications or adverseevents from YAG treatment of vitreous floaters in this par-ticular study. Based on these results, the authors concludedthat laser vitreolysis for vitreous floaters was safe but led toonly a moderate improvement of symptoms in only a thirdof the patients.19
A major deterrent in the utilization of the YAG laser forvitreous floaters is the lack of U.S. Food and DrugAdministration approval for such use. It remains an ‘‘off-label’’ use of the procedure and requires greater patienteducation and documentation by the physician. In addition,most insurance companies will not reimburse physicians forthis particular use of the laser, requiring the patient to self-finance the procedure.
Appropriate patient selection is vital for success in YAGvitreolysis treatment.18,19 The size and location of thefloaters, the amount of laser treatment necessary to obliter-ate the lesion, the number of treatment sessions, and therisk to adjacent ocular structures must be considered. Fur-thermore, current methods to assess functional impairmentinduced by vitreous floaters have not been established orstandardized. Studies have found that some well-selectedpatients can expect some degree of resolution from theirfloaters, but patient satisfaction will vary greatly.18 Obvi-ously, promoting realistic expectations will influence ulti-mate patient satisfaction and treatment decisions.
There are several inherent problems and potential risksthat are not apparent with other ocular uses of the YAGlaser. Unlike YAG capsulotomies and iridotomies, theophthalmic tissue being treated is in motion. Vitreousfloaters make both aiming and utilization of the treatmentenergy more difficult than with other YAG laser procedures.Second, location of symptomatic vitreous floaters is nearthe posterior pole of the eye, more specifically the opticnerve head and retinal vascular regions.20,21 Miscalcula-tions with applied laser energy or treatment site could resultin potentially sight-threatening complications. Serious ocu-lar side effects could include retinal tears, vitreo-retinal
hemorrhages, or retinal detachments.22 Certainly, better tar-geting computerization and alignment would be helpfulwith future laser vitreolysis. These options are not currentlyavailable on current instrumentation, which relies more onsurgical skill and experience with the laser.22,23 Research islimited with regard to information about the effects andsafety of such treatment options on floater symptomology.
Surgical intervention
Combined cataract surgery with anterior vitrectomy hasbeen described as a treatment option for patients with bothcataracts and symptomatic vitreous floaters.23 This tech-nique has been reserved for older patients with early or ad-vancing lens opacification.
New surgical techniques, such as microincision vitrec-tomy, may offer a more complete cure from symptomaticvitreous floaters than laser vitreolysis. It might be a betteroption for treatment of patients who demand resolutionfrom their symptomatic vitreous floaters (see Figure 3). Al-though no clinical studies have been done to show its effec-tiveness, this ‘‘off-label’’ use of microincisional vitrectomyhas been used to treat patients with symptomatic vitreousfloaters.
Currently, some common indications for microincisionalvitrectomy use are macular pucker, macular holes, diabeticretinopathy without extensive membrane dissection, vitre-ous hemorrhage, and tractional retinal detachment.24,25
There remains a general reluctance in the ophthalmologiccommunity to perform this ocular surgery on eyes with cor-rected acuity of 20/20. Some of the reluctance may be re-lated to the natural history of vitreous floaters and PVDand the resolution of both conditions with a combinationof time and conservative treatment. Additionally there arepotential risks (i.e., endophthalmitis, retinal tears, bleeds,or detachments) associated with vitrectomy surgery.24
These risks might be unacceptable for patients and sur-geons with benign symptomatic vitreous floaters.24 Patientselection and education is absolutely vital for this treatmentoption for symptomatic vitreous floaters when considering‘‘off-label’’ microincisional vitrectomy. As with YAG vitre-olysis, surgical experience and ocular risks must all be well

Sendrowski and Bronstein Review Article 161
understood by the patient. Future studies are needed to de-termine both the risk and benefits of these treatment optionsfor patients with floaters symptomology.
Conclusions
Today the best treatment options for symptomatic vitreousfloaters remain conservative ones, with close follow-up andeducation. Time and patient reassurance will, for the mostpart, result in reduction or resolution of initial symptomsand has, over time, shown to be a sound treatment option.
In terms of ‘‘off-label’’ treatment, laser and surgicaloptions for vitreous floaters have not been adequately defined.The primary purpose of ‘‘off-label’’ laser and surgical optionsare the alleviation of symptoms associated with vitreousfloaters.25 A secondary benefit may be the reduction of the pa-tient’s mental stress created by the floaters. Alternately, theprimary risks of ‘‘off-label’’ use of laser and surgical optionsare the unwanted ocular complications of retinal tears, vitre-oretinal hemorrhages, endophthalmitis, and retinal detach-ments. Currently, there are no clinical studies that provideadequate information about the ocular benefits or complica-tions associated with such treatment options. Although pa-tient symptomology from vitreous floaters can be reducedor in some cases alleviated by laser or surgical intervention,the patient benefit may not offset the potential risk from theprocedure. The decision for treatment of symptomatic vitre-ous floaters should be done on a case-by-case basis. Patientannoyance, stress, and anxiety created by the vitreous floatersis an important factor in that decision-making process.
Regardless of the treatment option agreed upon by thepatient and doctor, it is important to educate patients bybecoming familiar with ‘‘off-label’’ treatment options, onthe risks and benefits of all treatment procedures, and toallow time for the patient and doctor to consider what isbest for the visual health of the patient.
References
1. Bishop PN. Structural macromolecular and supramolecular organiza-
tion of the vitreous gel. Prog Retinal Eye Res 2000;19:323.
2. Sebag J, Balazs EA. Morphology and ultrastructure of human vitreous
fibers. Invest Ophthalmol Vis Sci 1989;30:1867.
3. Reardon AJ, LeGoff M, Briggs MD, et al. Identification in vitreous
and molecular cloning of optcin, a novel member of the family of leu-
cine-rich repeat proteins of the extracellular matrix. J Biol Chem 2000;
275:2123.
4. Foos RY, Wheeler NC. Vitreoretinal juncture. Synchysis senilis and
posterior vitreous detachment. Ophthalmology 1982;89:1502.
5. Hikichi T, Trempe CL. Relationship between floaters, light flashes, or
both, and complications of posterior vitreous detachment. Am J Oph-
thalmol 1994;117:593-8.
6. Linder B. Acute posterior vitreous detachment and its retinal compli-
cations. Acta Ophthalmol 1966;87(suppl):1.
7. Sirek OV, Sirek A, Fikar K. The effect of sex hormones on glycosam-
inoglycan content of canine aorta and coronary arteries. Atherosclero-sis 1977;27:227.
8. Chou JY, Lee TY, Hollands H, et al. Risk factors for posterior vitreous
detachment. Am J Ophthalmol 2006;142:931-7.
9. Mayne R, Brewton RG, Wright DW, et al. Morphological and bio-
chemical studies of the structure of the vitreous and the zonular fibres.
Biochem Soc Trans 1991;19:868-71.
10. Sebag J. The vitreous: structure, function and pathobiology. New
York: Springer-Verlag; 1989:60-61.
11. Spaide RF. Measurement of the posterior precortical vitreous pocket in
fellow eyes with posterior vitreous detachment and macular holes. Ret-
ina 2003;23:481-5.
12. Deiter P, Wolf E, Geer S. Glare and scatter of light in the vitreous: Ef-
fect in postoperative retinal detachment patients. Arch Ophthalmol
1972;87:12.
13. Balazs EA, Denlinger JL. Aging changes in the vitreous. In: Aging and
human visual function. New York: Alan R. Liss; 1982:45-57.
14. Roth M, Trittibach P, Loerner F, et al. Pars plana vitrectomy for idiopathic
vitreous floaters. Klin Monastble Augenheilled 2005;222(9):728-32.
15. Murakami K, Jalkh AE, Avila MD, et al. Vitreous floaters. Ophthal-
mology 1983;90:1271.
16. Jaffe NS: Vitreous traction at the posterior pole of the fundus due to
alterations in the posterior vitreous. Trans Am Acad Ophthalmol Oto-laryngol 1967;71:642.
17. Chern KC. Emergency ophthalmology: a rapid treatment guide. New
York: McGraw-Hill Medical Publishing Division; 2002:155-9.
18. Tsai WF, Chen YC, Su CY. Treatment of vitreous floaters with neo-
dymium YAG laser. Br J Ophthalmol 1993;77:485-8.
19. Delaney YM, Oyinloye A, Benhamin L. Nd:YAG vitreolysis and pars plana
vitrectomy: surgical treatment for vitreous floaters. Eye 2002;16:21-6.
20. Jagger JD, Hamilton AM, Polkinghorne P. Q-switched neodymium
YAG laser vitreolysis in the therapy of posterior segment disease.
Graefes Arch Clin Exp Ophthalmol 1990;228:222-5.
21. Little HL, Jack RL. Q switched neodymium: YAG laser surgery of the
vitreous. Graefes Arch Clin Exp Ophthalmol 1986;224:240-6.
22. Carvouris PE, Holz ER. Management of retinal breaks and conditions
predisposing to retinal detachment. Comp Ophthalmol Update 2006;
7(1):13-22.
23. Mossa F, Delaney YM, Rosen PH, et al. Folaterectomy: combined
phacoemulsification and deep anterior vitrectomy. J Cataract Refract
Surg 2002;28:589-92.
24. Agrawal RN, de Juan E Jr. Do the advantages of 25 gauge vitrectomy
outweigh the disadvantages? Retinal Physician 2004;1:51-2.
25. Toczolowski J, Katski W. Use of Nd:YAG laser in treatment of vitre-
ous floaters. Klinika Oczna 1998;100:155-7.