Embed Size (px)
Citation preview

Lecture 7: Exploration of calcium, phosphorus and
magnesium metabolism
2011-2012

Content of lecture 7:
Distribution of calcium in human organism. Hypocalcaemia: clinical features, causes and
changes of lab tests. Hypercalcemia: clinical features, causes and
changes of lab tests. Exploration of phosphorus metabolism. Hypo-
and hyperphosphatemia Exploration of magnesium metabolism.
Magnesium deficiency: clinical features, causes and changes of lab tests.

Calcium carbonate
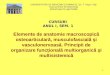
The molecular arrangement of collagen and hydroxyapatite crystals in compact bone. (a) Collagen fibers overlap adjacent fibers as they repeat every 680 Å. Hole zones are areas of low density bone collagen and overlap zones are areas of very high density bone collagen. (b) Hydroxyapatite crystals (Ca10[PO4]6[OH]2) are arranged in layers within each fiber, resenbling overlapping bricks.
Calcium phosphate
Hydroxyapatite

Calcium balance
1 oz= 0.0295 l= 29.5 ml 8 oz= 240 ml 1 ounce= 28,34 g
Sources – dairy products, egg yolk, nutsAbsorbtion – fibres, oxalates, free fatty acids in excess (steatoreea) interfere with absorbtion Requirements: • 600 -800 mg/day – adult• 800-1200 mg/day - children • 1200-1300 mg/day pregnancy, lactation• 1600-1800 g/day olderLosses 100 -200 mg/day in faeces and urine
Vitamin DD2 ergocalciferol –vegetal originD3 colecalciferol –animal origin (milk, egg yolk, liver)

Distribution of calcium
90% in bone 9% intracellular 1% blood
Calcium in bone 60-70% Ca 10 (PO4)6 (OH)2 –calcium phosphate, hydroxyapatite Bone matrix is formed by:
90% collagen (contain Hpro şi Hlys, specific AA of collagen) 10% noncollagenous proteins (OC and OPG).
Bone remodeling is accomplished by 2 types of cells: Osteoclasts – multinucleate cells, responsible for bone
resorption Osteoblasts – young bone cells, responsible for bone
formation

Bone remodelling cycle lasts about 6 months
90% of Ca, 85% of P, and 60% of Mg in whole body are stored in bone

Intracellular calcium
stored in deposits (sarco/endoplasmic reticulum) calcium depletion stopps the cell in G0 stage

Calcium in serum
8 - 11 mg/dl, 2.25-2.75 mmol/l 1/2 protein bound and not difusable a small amount is difusable in non-ionised form (citrate, carbonate) the rest represents the ionised fraction which has a functional role
(coagulation, neuromuscular transmition, maintainance of the cardiac rhythm)
Ionic calcium may be measured directly (selective electrodes) or may be calculated by formula:
(6xCa total – Total Protein/3) Ca++ = ______________________________
Total protein + 6

50% of calcium is in the ionisable form, having a role in muscular contraction, heart contraction, nervous transmition, coagulation.
> 50% is ionised in acidosis < 50% is ionised in alkalosis
Total Ca decreases in hypoalbuminemia without decreasing ionic Ca2+
Decrease of Ca2+ is followed by tetany and neuromuscular convulsions.

Factors that regulate calcium in serum:
1. PTH: in bone stimmulates bone resorbtion and Ca release, intestines (increases calcium absorbtion), kidney (increases calcium reabsorbtion at PCT=proximal contort tubes).
2. Calcitonin – decreases calcium in serum by increasing calcium clearance at kidney level.
3. Vitamin D – increases calcium absorbtion at intestinal level
4. Estrogens and androgens inhibate the osteoclasts, hyperfunction of adrenal cortex or of the thyroid --- hypercalcemia / calcium
bone depletion .
5. Carbohydrates increase Ca absorbtion, and lactose increases absorbtion and retention of calcium.

Control mechanisms:
Decrease of Ca2+ stimulates directly PTH
PTH normalizes Ca level by stimulating at kidney level the formation of the active form of vitamin D = 1,25 di(OH)vitD, which stimulates the absorbtion of calcium at intestinal level and increases reabsorbtion of calcium at kidney level.


Calcium receptors and transporters
Calcium sensing receptors: Calmodulin-binds calcium, involved in inflammation, metabolism, apoptosis Calnexin- Ca binding protein in cytoplasm, chaperone molecule, controling protein folding Calreticulin- binds Ca2+ ions Gelsolin- actin binding protein Neuronal:
Hippocalcin- neuronal calcium-binding protein Neurocalcin- neuronal calcium-binding protein Recoverin- calcium-binding protein detected in the photoreceptors of the eye. It plays a key
role in the inhibition of rhodopsin kinase, a molecule which regulates the phosphorylation of rhodopsin. This ultimately controls the ability of the eye to adapt to, and recover from, exposure to the presence of light.
Calcium binding proteins: Calbindin- mediates the transport of calcium across the enterocytes from the apical side,
where entry is regulated by the calcium channel TRPV6 Matrix Gla Protein (MGP) Osteocalcin (OC) Osteonectin S100 Troponin C

I. Exploration of calcium metabolism
High Ca2+: Hypercalcemia Milkalkali syndrome (Burnett) Calcinosis- Calciphylaxis, Calcinosis cutis Calcification – Metastatic calcification, Dystrophic
calcification
Deficiency Ca2+: Hypocalcemia Osteomalcia Pseudohypoparathyroidism

Hypercalcemia
Clinical features: decreased neuromuscular excitability disturbance of cardiac rhythm kidney stones articular calcifications
Primary hyperparathyroidism -parathyroidian adenoma- autonom synthesis of PTH - in blood: hyipercalcemia, hypophosphatemia, increase of PTH - in urine: increase of phosphates and calcium
Intoxication with vitamin D -prolongued administration of vitamin D (100 μg la adult = 4000UI, 45 μg = 1800 UI la copil) -clinical features:nausea, vomit, head pain, polidipsia, poliuria, hypertension
Malignancies of bone -primary tumours or metastasis – secretion of peptides PTH like
Increased bone turnover – prolongued immobility after bone fractions, hyperthyroidism Sarcoidosis – production of calcitriol in macrofages and in the cells of granulomas
Bone diseases that do not modify calcium levels in serum Osteoporosis Albright disease - Fibrous dysplasia of bone affecting multiple bones Paget disease- otherwise known as osteitis deformans, is a chronic disorder that typically results in enlarged and
deformed bones. It is named after Sir James Paget, the British surgeon who first described this disease. The excessive breakdown and formation of bone tissue that occurs with Paget's disease can cause bone to weaken, resulting in bone pain, arthritis, deformities, and fractures
Hypophosphatasia is a rare inherited metabolic disease of decreased tissue nonspecific alkaline phosphatase (TNSALP) and defective bone mineralization. Both autosomal recessive and autosomal dominant variants of the disease exist. The disease comes in one of five forms, perinatal, infantile, childhood, adult, and odontohypophosphatasia. Perinatal hypophosphatasia is invariably lethal while infantile hypophosphatasia has a roughly 50% mortality rate with symptoms appearing within the first 6th months after birth. The other forms are generally non-lethal. Common symptoms include bone malformations and higher chance of bone fracture. Both the adult form and odontohypophosphatasial form are marked by premature teeth loss
. Toni Debre Fanconi syndrome - There is a defect in the reabsorption of glucose, amino acids, phosphate and potassium.
Aminoaciduria associated with rickets, due to failure of the proximal renal tubules or to dysfunction of the deamination process. Very long list of clinical features may include rickets, polyuria, short stature, microcephaly, mental retardation etc. Both sexes affected, normal at birth and during postnatal period, usual onset at 4 to 6 months of age. Death usually occurs before the age of 10. The syndrome can appear in the 30s and 40s without any apparent precipitating cause. The disorder is probably transmitted as a Mendelian recessive trait.

Distrophic calcification


Calcinosis cutis

Metastatic calcification
Figure: An X-ray showed an intramedullary osteolytic lesion with calcifications in the proximal tibia. 1B, 1C and 1D: CT scans revealed a poorly demarcated tumor with an eccentric, non-uniform calcification.
The tumor invaded through the epiphyseal plate with expansion of the articular surface.
Dedifferentiated Chondrosarcoma: A Case Report And Review Of The Literature. Zenggang Pan M.D., Ph.D.Department of PathologyCreighton University Medical Center; Deba P. Wire M.D. Department of Pathology; Creighton University Medical Center; The Internet Journal of Orthopedic Surgery. 2007 Volume 5 Number 1

Clinical aspects related to hypercalcemia:
Diuretics may lead to hypercalcemia
in dialysed patients an exchange ions resin may be used in order to decrease hyperpotassemia. Using this resin may lead to hypercalcemia.
Ingestion of Mg, P, laxatives may lead to hypocalcaemia.
In some deficiencies Mg administration may correct calcium deficiency.

Hypocalcemia
Clinical features: increased neuromuscular
excitability (fibrilations, fasciculations, muscular pain. Chvostek, Trousseau +
extrem - tetania (mână de mamoş, carpopedalospasm, spasm glotic)
tulb. trofice ale fanerelor

Causes of hypocalcemia Hypoparathyroidism
surgical ablation - ↓ Ca, ↑ P in blood - ↓ P in urine - ↓ PTH în sânge
Pseudohypoparathyrodism – no response of kidney to PTH - PTH= N or increased - administration of PTH (in pseudohypoPTH does not increse urinary phosphates)
Hypersecretion of calcitonin - thyroidian neoplasm - pheocromocitom- peptides calcitonin-like
vitamin D deficiency(rickets, osteomalacia) ↓ vit. D → ↓ absorbţiei intestinale de Ca → ↑ secreţiei de PTH → mobilizarea Ca din
oase La nivel osos are loc proliferarea osteoblastelor → ↑ F.Alc lab: hypocalcemia, hypophosphatemia, hyperphosphaturia, increased PTH and ALP
Vitamin D resistent rickets – alfa-1 hydroxilase deficiency
Chronic kidney insuficiency -increased ureea and organic acids will fixate calcium in an unionisable form -renal hydroxilation defect of vitamin D
Acute Pancreatitis – calcium plus fatty acids (resulted from Triglycerides) form saponines

II. Exploration of magnesium metabolism
24 g Mg / 70 kg adult- metabolic active tissues are rich in Mg – brain, heart, liver, kidney, thyroid.
60% of total --- schelet39% of total Mg --- muşchi scheletic şi miocard1% of total Mg --- extracelular (35% legat de albumină, restul liber, în formă
ionizată).- Biological ranges: 1,9 – 2,5 mg/dl; 0,6 – 1,03 mmol/l,- Sources: green vegetables, fish, meat. Phosphates supress calcium and magnesium
absorbtion- Mg is important for ADP (source of energy) in metabolic processes:
carbohydrates metabolism proteic synthesis nucleic acid synthesis muscular contractions together with calcium , Na, K is involved in neuromuscular iritability blood coagulation.

Physiology of Mg and changes of Mg concentration in serum
-
Ca and Mg are tightly connected: a Mg deficiency may lead to calcium release from bone, responsible of calcifications in aorta or in kidney.
Normally 95% of Mg filtered in glomeruls is reabsorbed in renal tubules. When a deficiency of renal function is occuring, Mg increases in the blood stream.
High Mg2+ : Hypermagnesemia
Deficiency Mg2+ : Hypomagnesemia
Absorbtion of Mg: - pasively and actively (stimulated by vitamin D)- deficient in diarrhoea, steatoreea, intestinal surgery,
irradiation enteropathy and DM. - daily loss 100 mg in urine, as much as absorbed in
intestines (100 mg).

Hypomagnesemia:
In Mg deficiencies – urinary Mg decreases before seric Mg.
Clinical features: tiredness, lack of concentration, vertij, palpitations, muscular cramps.
Chronic diarrhea after hemodialysis chronic kidney disease liver cirrhosis chronic pancreatitis hiperthyroidism and hypoparathiroidism prolongued lactation malabsorbtion chronic alcoholism

Hypermagnesiemia:
Kidney Insuficiency diabetic acidosis hypothyroidism Addison disease antiacids with Mg dehydration diuretics – Tiazide
Interfering factors: prolongued therapy with salicilates, Li – increase Mg in serum, especially if there are kidney
lesions. Gluconatul de Ca interfere with the testing methods - - - decrease Mg Drugs: amfotericin B, aldosteron. Insulin, neomicin, diuretics with mercury - - - decrease Mg
concentrations in serum. Blood Hemolysis.: ¾ of Mg in blood is stored in RBC - - - hemolysis leads to false increase
values.

Clinical problems:
Treatment of diabetic coma leads to hypomagnesiemia. After insulin administration, Mg together with K enters in the cell.
Mg deficiency causes inexplicably hypocalcemia and hypopotasemia. Patients may have gastrointestinal and neurologic signs.
Hyperflexion Tremblings of extremities Carpopedal contractions Chvostek and Trousseau signs positive Tahicardia
Patients with these signs are very susceptible to auditive and visual stimuls
Increased Mg may act as sedative – depressing cardiac activity, neuromuscular activity.
Mg supplementation is reccommended after heart surgery, after MI, or for prevention of cardiac aritmias.
Treatment: hipoMg-emia will be more efficient treated with Mg and vit B6, especially in children.

III. Exploration of phosphorus metabolism
Normal values: adults 0,87 – 1,45 mmol/ l
85% is combined with Ca in bones. Phosphorus – esters, phosphates.
Role of phosphorus in: bone metabolism, carbohydrates and lipid metabolism, acid-base balance, energetic transfere.
Phosphorus enters the cell together with glucose.
High PO4: Hyperphosphatemia
Deficiency PO4: Hypophosphatemia Hypophosphatasia – alkaline phosphatase

High PO4:
in kidney disfunction and uremia kidney insufficiency hypoparatiroidism hypocalcemia excess of alkalin substances excess of vitamin D bone tumours, acromegaly.

Deficiency PO4
Hypophosphatemia hyperparathyroidism rickets diabetic coma hyperinsulinism
Hypophosphatasia – alkaline phosphatase