Embed Size (px)
Citation preview
28
CYSTICERCOSIS (TIENIA SOLIU1lf).
By ?\[A,TOR n. 13. .1'. DIXO~, 1\I,C" Royal Army .llieclic(i,l CO'1'PS,
ANT>
D. 'V. Sl\IITHERS, l\LB., n.CHIR., Civilian Mc(lieal l)raditioner
From The Queen .A lexandra, Mili,iary HospUal, Millbank.
(Oontimwcl from p. 380, vol. lxiv.)
X.-DIAGNOSIS.
The greatest obstacle to correct diagnosis is undoubtedly Lhe failure to consider cysticercosis as a possible cause of the symptoms that the patient presents. As has already been stated the disease bas been largely forgotten in this country and nntil the present work was started there was no evidence tbat a case of cysticercosis in England to-day was anything but a. medical curiosity.
Even in the London teaching hospitals quite obvious cases have recently remained undiagnosed, and when the ohstacles to a final diagnosis in difficult or suspicious cases are appreciated it is not surprising tbat many cases are missed.
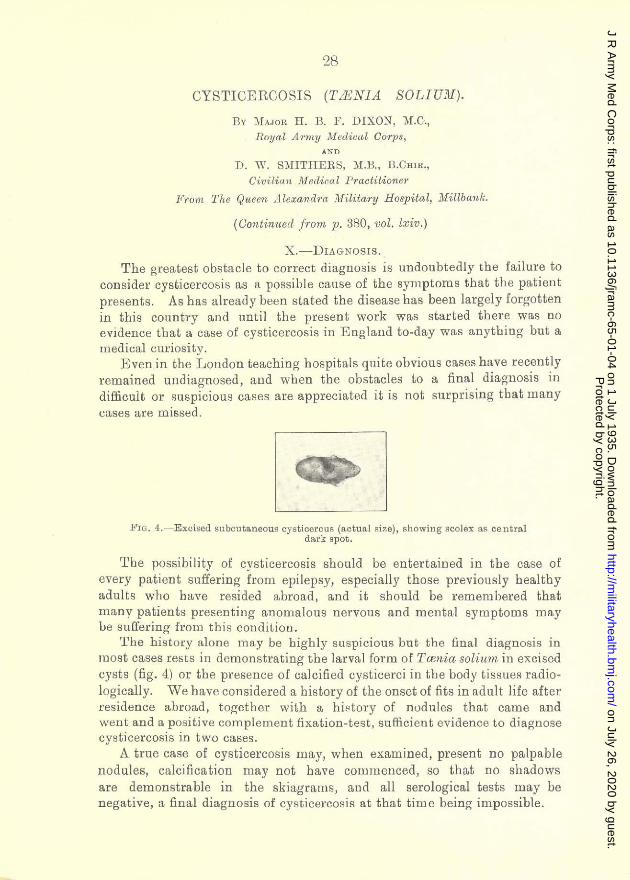
FIG. 4. - Excised subcutaneous cysticerous (a.ctua.l !'!ize), showing scolex as central dark spot.
'rbe possibility of cysticercosis should be entertained in the case of every patient suffering from epilepsy, especially those previously healthy adults who have resided abroad, and it shonld be remembered that many patients presenting anomalous nervous and mental symptoms may be suffering from this condition.
The history alone may be bighly suspicious but the final diagnosis in most cases rests ill demonstrating the larval form of Twnia solinm in excised cysts (fig. 4) or the presence of calcified cysticerci in the body tissues radiologically. We have considered a bistory of the onset of fits in adult life after residence abroad, to~ether with a history of nodules that came and went and a positive complement fixation-test, sufficient evidence to diagnose cysticercosis in two cases.
A true case of cysticercosis may, when examined, present no palpable nodules, calcification may not bave cOllJmenced, so that no shadows are demonstrable in the skiagrams, and all serological tests may be negative, a, final diagnosis of cysticercosis at that time being impossible.
Protected by copyright.
on July 26, 2020 by guest.http://m
ilitaryhealth.bmj.com
/J R
Arm
y Med C
orps: first published as 10.1136/jramc-65-01-04 on 1 July 1935. D
ownloaded from
H. B. P. Dixon and D. W. Smithe,"" '29
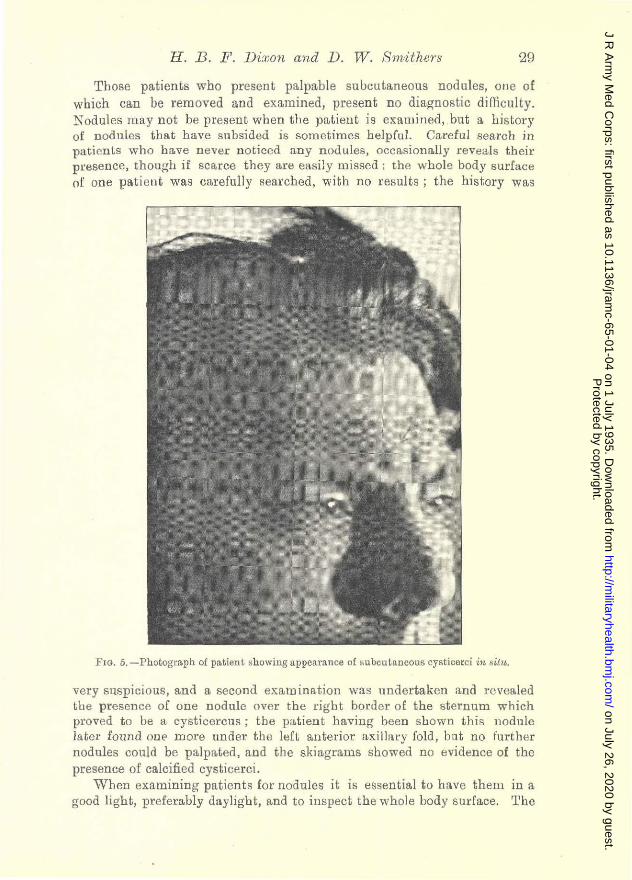
Those patients who present palpable subcuLaneous nodules, one of which can be removed and examined, present no diagnostic difficulty. Nodules may not be present when the patient is examined, but a history of nodules that have subsided is sometimes helpful. Careful search in patients who have never noticed any nodules, occasionally reveals their presence, though if scarce they are easi1y lllissec1; the \vhole body surface of one patient was cllrefully searched, with no results; the history was
PIG. 5, -Photograph of patient showing appearance of !>ubcutancous cysticerci in situ.
very suspicious, and a second examina.tion was undertaken and revealed the presence of one nodule over tbe rigbt border of the sternum which proved to be a cysticerclls; the pa.tient having been shown this llodnle latcr found ooe more under the left anterior axillary fold, but no further nodules coold be palpated, and tbe skiagrams showed no evidence of the presence of calcified cysticerci.
When examining patients lor nodules it is essential to have them 10 a good light, preferably daylight, and to inspect the whole body surface. 'rhe
Protected by copyright.
on July 26, 2020 by guest.http://m
ilitaryhealth.bmj.com
/J R
Arm
y Med C
orps: first published as 10.1136/jramc-65-01-04 on 1 July 1935. D
ownloaded from
30 Cysticercosis (Tffin ia solium)
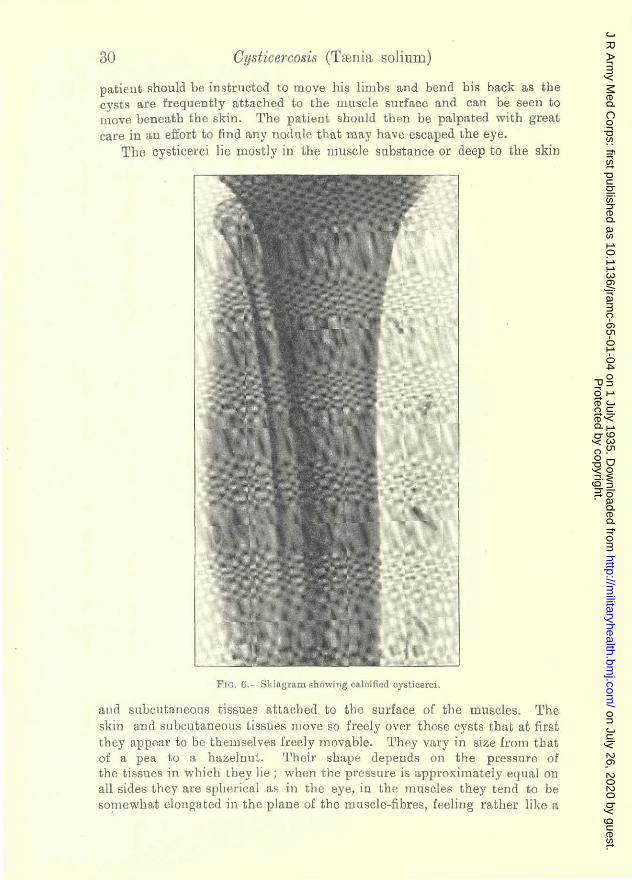
patient should be instructed to move his limbs and bend bis back as tbe cysts are frequently attached to the muscle surface and can be seen to move beneath the skin. Tbe patient should then be palpated with great care in an effort to find any nodule that may have escaped the eye.
The cysticerci lie mostly in tbe muscle substance or deep to the skill
FIG. 6.- Skiagram showing ca.l cifi ed cysticerci.
alld subcutaneous tissues attached to the surface of the muscles. The skin and subcutaneous tissues lllove so freely over these cysts that at first they appear to be tbemselves freely movable. They vary in size from tbat of a. pea t.o a hazelnut. rrheir shape depends on the pl'eS!;Ure of the ti ssues in which LLey lie ; \vben the pressure is approximately equal on all s ides t.hey are spherical as in the eye, ill the muscles they t.end to be somewhat elollgated in the plane of the muscle-fibres, leeliug rather like a
Protected by copyright.
on July 26, 2020 by guest.http://m
ilitaryhealth.bmj.com
/J R
Arm
y Med C
orps: first published as 10.1136/jramc-65-01-04 on 1 July 1935. D
ownloaded from
H. B. F. Dixon and D. lV. 8mithers 31
small gelatine capsule. Their consistency depends on the amonnt of fluid contained or tenseness of the cyst and 'Varies cOllsiderably, the ma.jority being tense fLnd hard. 'llbeyare quite painless and there is no skin reaction over them. In our ser.ies there wa.s onc exception to this rule a.lready mentioned; the patient developed considerable pain in the nodules, accom-
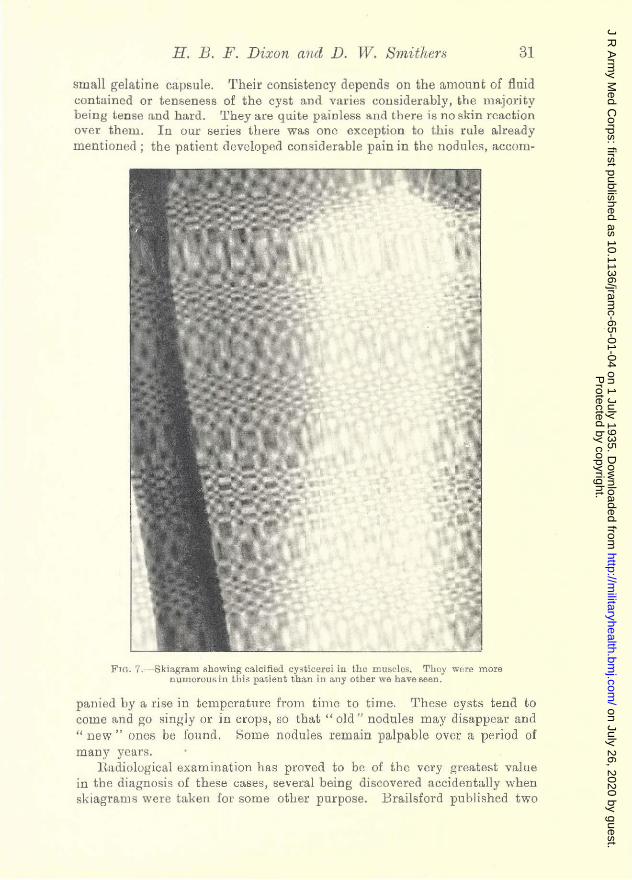
FIG. 7. - Ski:1gram showing calcified cy!;ticerci ill the mU!:ic1cs, Thoy were more llUllH,JCOusin thiil pa.tient than ill any other we ha.veseen,
panied by a rise in temperature from time to time. These cysts tend to COlle and go singly or in crops, so that" old" nodules llay disappear and " new" ones be found. Some nodules remain palpable over a period of many years.
H:L<liological examination has proved to be of the very greatest value in the diagnosis of these cases, se'v"eral being discovered accidentally when skiagram. were taken for SOllle other purpose. Brailsford published two
Protected by copyright.
on July 26, 2020 by guest.http://m
ilitaryhealth.bmj.com
/J R
Arm
y Med C
orps: first published as 10.1136/jramc-65-01-04 on 1 July 1935. D
ownloaded from
3'2 Cysticercosis (Tamia soliuUll
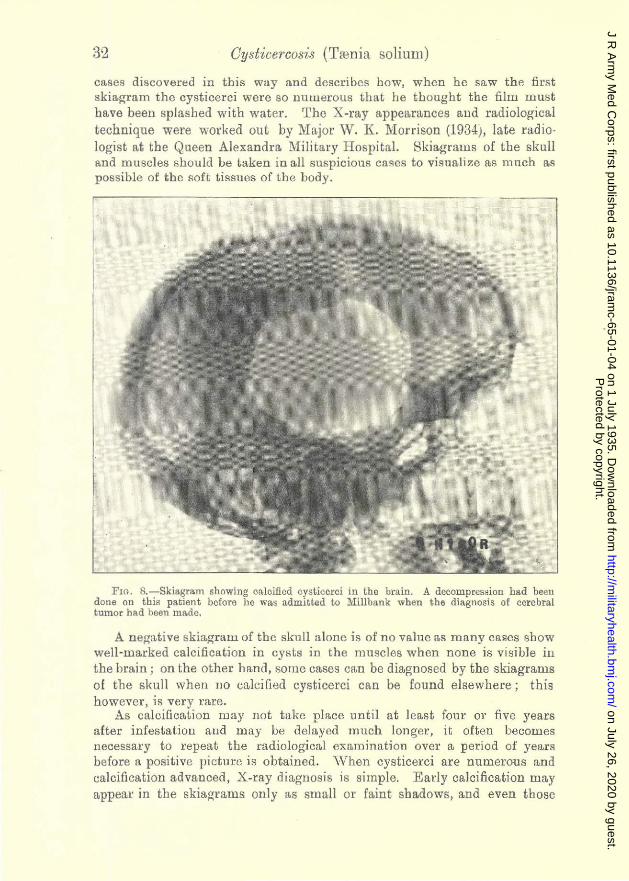
cases discovered in this way and describe!; how, when he saw the first skiagram the cysticerci were BD nUlUerous thaL he thought the film must have been splasbed with water. Tbe X-ray appearances and radiological technique were worked out by Major W. K. Morrison (1934), late radiologist at tbe Queen Alexandra Military Hospital. Skiagrams of the skull and muscles should be taken in a.ll suspicious cases to visualize as much as possible of the soft tissues of the body.
PlO. S.-Skiagram showing calcified cystioeroi in the brain. A decompression had been done on tbiR patient before he was admitted to Millbank when the diagnosis of cerebra.l turnor had been ma.de.
A negati ve skiagralll of the skull alone is of no value as many cases show well-marked calcification in cysts in the muscles when nODe is visible ill tbe brain; on the other hand, some cases can be diagnosed by tbe skiagrams of the skull when 110 calcified cysticerci can be fonnd elsewhere; this however, 18 very rare.
As calciiication may not take place until at least four or five years after infestation and Illay be delayed mnch longer, it often becomes necessary to repeat the radiological eXl1mination over a period of years before a positive picture is obtained. "When cysticerci are numerous and calcification advanced, X-ray diagnosis is simple. Early calcification may appear in the skiagrams only as small or faint shadows, and even those
Protected by copyright.
on July 26, 2020 by guest.http://m
ilitaryhealth.bmj.com
/J R
Arm
y Med C
orps: first published as 10.1136/jramc-65-01-04 on 1 July 1935. D
ownloaded from
H. B. F. Dixolt mu7 D. W. Smithcrs 33
familiar with the X-ray appearances may be forced to postpone tbeir diagnosis until further deposition of calcium makes the diagnosis certain. Oysts may be so scarce that unless skiagl'aIllS of the whole body are taken the shadows may be missed. The n.diologist must be prepared to search for suspicious shadows throughout the various skiagrams and to repeat
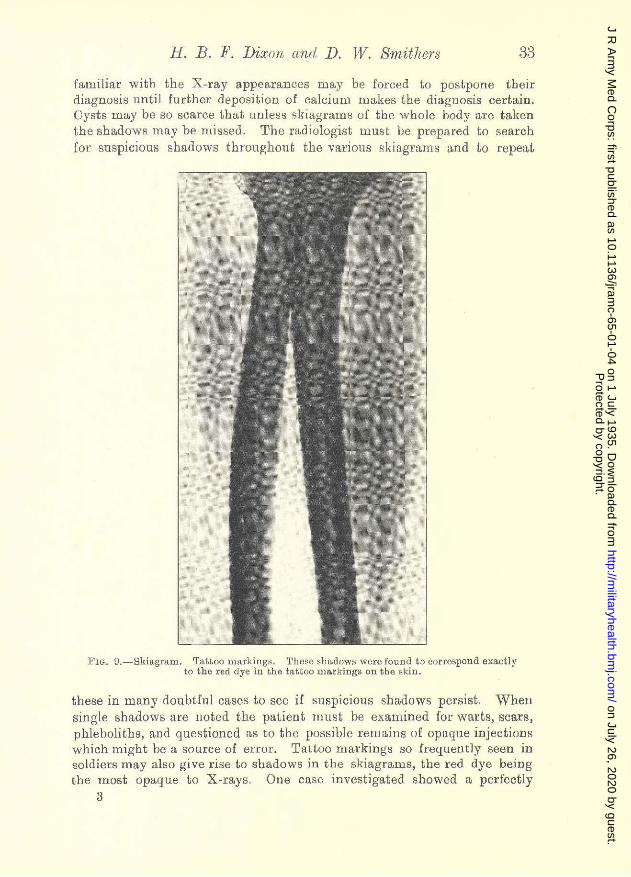
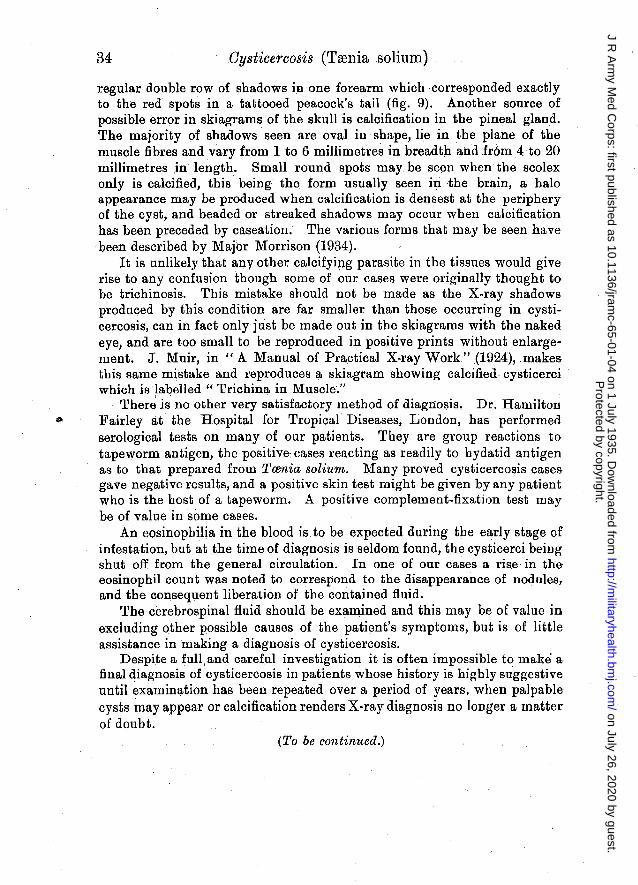
FIG. O.-Skill.gmlll. TatLoo marl<ings. These ~L[~dows wore found t.o correspond exa.ctly to the red dye in che tattoo ma.rkings on the I',kin.
these in many doubtful cases to see if suspicious shadows persist. When single shadows are noted the patient Hlllst be examined for warts, scars, phleboliths, and questioned as to the possible remains of opaque injections which might be a source of error. Tattoo markings so frequently seen in soldiers may also give rise to sbado .... vs in the skiagrams, the red dye being the most opaque to X-rays. Oue case investigated showed a perfectly
3
Protected by copyright.
on July 26, 2020 by guest.http://m
ilitaryhealth.bmj.com
/J R
Arm
y Med C
orps: first published as 10.1136/jramc-65-01-04 on 1 July 1935. D
ownloaded from
34 Oysticercosis (Trenia solium)
regular double row of shadows in one forearm which corresponded exactly to the red spots in a tattooed peacock's tail (fig. 9). Another source of possible error in skiagrams of the skull is calcification in the pineal gland. The majority of shadows seen are oval ill shape, lie in the plane of the muscle fibres and vary from 1 to 6 millimetres in breadth and fr6m4 to 20 millimetres .in length. Small round spots may be seen when the scolex only is calcified, this being the form usually seen in the brain, a halo appearance may be produced when calcification is densest at the periphery of the cyst, and beaded or streaked shadows may occur when calcification has been preceded by caseation. The various forms that may be seen have been described by Major Morrison (1934).
It is unlikely that any other calcifying parasite in the tissues would give rise to any confusion though some of our cases were originally thought to be trichinosis. This mistake should not be made as the X-ray shadows produced by this condition are far smaller than those occurring in cysticercosis, can in fact only just be made out in the skiagrams with the naked eye, and are too small to be reproduced in positive prints without enlargement. J. Muir, in " A Manual of Practical X-ray Work" (1924), .makes this same mistake and reproduces a skiagram showing calcified· cysticerci which is labelled " Trichina in Muscle."
There is no other very satisfactory method of diagnosis. Dr. Hamilton Pairley at· the Hospital for Tropical Diseases, London, has performed serological tests on many of our patients. They are group reactions to tapeworm antigen, the positive: cases reacting as readily to hydatid antigen as to that prepared from Tcenia Bolium. Many proved cysticercosis cases gave negative results, and a positive skin test might be given by any patient who is the host of a tapeworm. A positive complement-fixation test may be of value in some cases.
An eosinophilia in the blood is. to be expected during the early stage of infestation, but at the time of diagnosis is seldom found, the cysticerci being shut off from the general circulation. In one of our cases a rise in the eosinophil count was noted to correspond to the disappearance of nodules, and the consequent liberation of the contained fluid. .
The cerebrospinal fluid should be examined and this may be of value in excluding other possible causes of the patient's symptoms, but is of little assistance in making a diagnosis of cysticercosis.
Despite a full and careful investigation it is often impossible to make' a final qiagnosis of cysticercosis in patients whose history is highly suggestive until examination has been repeated over a period of years, when palpable cysts may appear or calcification renders X-ray diagnosis no longer a matter of doubt.
(To be continued.)
Protected by copyright.
on July 26, 2020 by guest.http://m
ilitaryhealth.bmj.com
/J R
Arm
y Med C
orps: first published as 10.1136/jramc-65-01-04 on 1 July 1935. D
ownloaded from