Embed Size (px)
Citation preview

EV0810ePoster Viewing Parasitic disease epidemiology
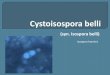
Cystoisospora belli infection: the first case series in Thailand
Benjawan Skulsujirapa*1, Chusana Suankratay1
1Division of Infectious Diseases, Department of Medicine, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand
Background: Cystoisospora (formerly Isospora) belli, a gastrointestinal protozoan endemic in tropical and subtropical areas, can cause intestinal infections in patients with and without HIV infection. We report herein the first case series of C. belli in Thailand.
Material/methods: A retrospective study was carried out in all patients with C. belli infection from 2005 to 2015 at King Chulalongkorn Memorial Hospital, Bangkok, Thailand.
Results: There were 26 patients, but there were only 18 patients with available medical records. Fourteen (77.8%) patients were male with the median age of 43 (IQR: 38, 60) years. Of 18 patients, HIV infection (16 patients, 88.9%) was the most common comorbidity, followed by tuberculosis (3, 0.17%), hepatitis C infection (2, 0.11%), diabetes, liver transplantation, renal carcinoma, systemic lupus erythematosus, glomerulonephritis, tuberculosis, and hypertension (1, 0.06% each). Of 16 HIV-infected patients, 6 and 10 had and had not received antiretroviral treatment, respectively. Of 18 patients, all presented with watery diarrhea and weight loss with the median duration of 16 (IQR: 6, 32) weeks. There were 2 patients (0.11%) with malabsorption syndrome resulting in hypoalbuminemia, hypomagnesemia and abnormal coagulogram. Of 18 patients, there were 4 patients with recurrent courses of watery diarrhea with the duration of 2, 3, 10, and 20 years. Of 13 patients with available complete blood count data, 8 (61.6%) had eosinophil of more than 6% with mild, moderate, and severe degree of eosinophilia of 30.8%, 0.08%, and 0.08%. Of 18 patients, there were 10 (55.5%), 1 (0.05%), 2 (11.1%), and 5 (27.8%) patients receiving cotrimoxazole, ciprofloxacin, albendazole plus metronidazole, and no treatment, respectively. There was dramatic clinical improvement in 9 (90%) of 10 patients treated with cotrimoxazole, without recurrence after a longterm follow-up. There was no mortality.
Conclusions: In our institute, C. belli infection is not an uncommon cause of either acute or chronic watery diarrhea, both in HIV- and non-HIV-infected patients. The clinical course varies from self-limited to treatment-responsible, treatment-refractory, and multiple recurrent courses.
Figure 1 : C. belli oocysts on modified acid-fast stain, 100X magnification (left) and on fresh smear, 400X magnification (right)



![EW09 01 Kortbeek.ppt [Kompatibilitätsmodus] · Strongyloides Cyclospora Cystoisospora belli Enterobius Schistosoma Fasciola Clonorchis Taenia Hymenolepis 19 Adult worms 20 How to](https://img.pdfslide.net/doc/110x75/5e6e13d6b365a9546f424581/ew09-01-kompatibilittsmodus-strongyloides-cyclospora-cystoisospora-belli-enterobius.jpg)