Embed Size (px)
Citation preview
Acc
epte
d A
rtic
le
This article has been accepted for publication and undergone full peer review but has not
been through the copyediting, typesetting, pagination and proofreading process, which may
lead to differences between this version and the Version of Record. Please cite this article as
doi: 10.1111/1755-5922.12230
This article is protected by copyright. All rights reserved.
Received Date : 29-Jun-2016
Revised Date : 02-Sep-2016
Accepted Date : 19-Sep-2016
Article type : Original Research Article
Cytochrome P450 2C9 gene polymorphism and warfarin maintenance dosage in
pediatric patients: A systematic review and meta-analysis
running title: CYP2C9 gene and warfarin maintenance dosage
Jinhua Zhang 1,1
, Lihong Tian1,2
,Jinlong Huang 2, 3
, Sihan Huang 3, 3
,Tingting Chai4,3
,Jianzhen
Shen*, 3
1Department of Pharmacy, Fujian Medical University Union Hospital, Fuzhou 350001, PR
China
2Department of Hematology/ Rheumatology, the Second Hospital of Xiamen, Xiamen361021, PR
China.
3Fujian Institute of Hematology, Fujian Provincial Key Laboratory on Hematology, Fujian
Medical University Union Hospital, Fuzhou 350001, PR China
1 Lihong Tian and Jinhua Zhang contributed equally to this work.
*Correspondence to:
Dr.Jianzhen Shen;Department of Hematology, Fujian Medical University Union Hospital,
Xinquan Road #29, Fuzhou, China, 350001. Tel.: +86 591 83357896-8301; Email:
Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
Abstract
Aim: To assess the effect of Cytochrome P450 2C9 (CYP2C9) gene polymorphism on
pediatric warfarin maintenance dosage requirement.
Methods:A previously developed search strategy was conducted in PubMed, EMBASE,
and the Cochrane Library. Eligible studies published prior to January 27, 2016, were
identified and compared against strict inclusion/exclusion criteria. Required data were
extracted, and researchers were consulted for additional data if needed. Review Manager
Version 5.2.3 software was used to analyze the relationship between CYP2C9 polymorphisms
and warfarin maintenance doses in pediatric patients. Eight articles with a combined total of
507 pediatric patients were included in the meta-analysis.
Results:Maintenance warfarin doses in patients with CYP2C9 *1/*2 genotype, CYP2C9
*1/*3 genotype, and CYP2C9 variant carriers which contain at least one variant allele (*2 or
*3) were from 15% to 41% lower than doses in patients with the wild type allele (CYP2C9
*1/*1): all differences were significant with P-values <0.05. The Fontan procedure as a
medical indication for anticoagulation was also associated with a lower warfarin maintenance
dose; however, target INR range was not.
Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
Conclusions: We found that CYP2C9 gene polymorphism(referring to the presence of *1/*2,
*1/*3, and variant genotypes in the population in addition to the wild type) was significantly
associated with decreased warfarin maintenance dose requirements. Additionally, a specific
indication for warfarin, the Fontan procedure, was associated with a lower daily warfarin
dose. However, the results of our study require confirmation from more research with larger
numbers of pediatric patients.
Keywords: Warfarin, Pediatric patients, CYP2C9, Gene polymorphisms, Systematic review,
Meta-analysis
Introduction
Warfarin, a vitamin K antagonist used as an oral anticoagulant, is widely prescribed for
preventing the thrombosis. However, proper dosing can be clinically challenging due to its
narrow therapeutic range as well as an almost twenty-fold difference in the dosages required
for adequate anticoagulation. The prothrombin time (PT) and international normalized ratio
(INR) should be monitored to ensure the desired antithrombotic effect while minimizing the
risk of bleeding.
Over the past decade, researchers have proven that two genes, CYP2C9 and VKORC1,
explain up to 40% of the variability seen in maintenance warfarin dosing requirements of
adults.[1-3]CYP2C9is highly polymorphic, which can lead to a significant influence on the
metabolism of drugs.[4]In 1999,Aithal et al. have demonstrated that there is a strong association
Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
between CYP2C9 variant alleles and warfarin dose requirement[5]. After that, many studies have
certified the significant effect of CYP2C9on warfarin doses in adult patients[6-11].Moreover, a
dosing algorithm for adult patients has been established by the US Food and Drug
Administration and International Warfarin Pharmacogenetics Consortium[1,2]. However, due
to several factors,the pharmacogenetic model for adults cannot be directly used for pediatric
patients, and need for pediatric-focused pharmacogenomic studies[12,13].One is that the
maturation of metabolic enzymes, which is age-related, has a significant effect on warfarin
dose requirements [14].In addition, there are dietary differences in vitamin K intake among
pediatric patients (e.g., breast milk vs. formula diets in infants), which affect warfarin
activity[15].Furthermore, clinical characteristics, such as indication for warfarin and the target
INR range, cause great variability in the dose requirement for warfarin in children.
CYP2C9 is located on human chromosome 10q24.2 and is approximately 55kb in length.
In adults, CYP2C9mutant types require a 19.6 to 78.1% lower warfarin dose for proper
anticoagulation[6]. There have also been studies that focused on CYP2C9 polymorphism and
warfarin dosing in pediatric patients [16-23].Questions about the effects of CYP2C9
polymorphism on pediatric warfarin dosing and about the possible development of a
pharmacogenetic model for children remain unanswered. For this reason, it has been
proposed that a meta-analysis be performed [4].Therefore, we conducted a systematic review
to analyze the relationship between warfarin maintenance dosage and gene polymorphism in
pediatric patients.
Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
Methods and Materials
Search strategy
A comprehensive search was conducted in PubMed, EMBASE, and the Cochrane
library for relevant English-language research articles published prior to January 27, 2016
(the date the search was completed). The search field strategy used was (CYP2C9 OR
cytochromes OR Cytochrome-p-450 OR Cytochrome p-450 OR “Cytochrome P450”) OR
(warfarin AND [gene OR genotype OR genetics OR alleles OR polymorphisms OR
pharmacogenetics] AND (neonate OR infant OR child OR adolescents OR pediatrics OR
pediatric). The included literature references were examined and the authors were consulted
for any additional information.
Study inclusion criteria
A strict set of inclusion criteria was used to find eligible studies: (1) the focus was on the
relationship between CYP2C9 polymorphism and warfarin maintenance dosing; (2) the
sample size and mean warfarin maintenance dose and standard deviation [SD] for each
CYP2C9 genotype group was provided; (3) data was given for patients in the pediatric age
group (ages <19 years); (4) the mean age of subjects and information about their ethnicities
were given. No restrictions were set for other clinical characteristics, such as possible
interacting drugs, clinical indications for warfarin, or the sex ratio of patients.
Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
Study exclusion criteria
Studies were excluded from the meta-analysis if (1) data were not provided, or could not
be obtained, on the mean warfarin dose and SD, patient sample size, patient age, or patient
ethnicity; (2) data were not provided specifically for a population of pediatric patients; (3) the
data were already reported in a previous article; and (4) the publication type was an abstract,
conference proceeding, review article, letter, or case report.
Data extraction
All required data were extracted independently by two researchers. To avoid potential
data extraction errors, cross-checking was performed. If there was a question about any
extracted data, there was discussion to reach a consensus regarding the data’s inclusion.
Additional required data was obtained by consulting researchers when necessary. Information
extracted included names of the first authors, publication years, target INR ranges,
predominant patient ethnicities, mean ages, sex ratios, indications for warfarin use, sample
sizes, allele frequencies, and warfarin maintenance doses (means with SDs) for single
nucleotide polymorphism (SNP) genotypes.
Quality assessment
The criteria predefined by Lindh JD et al.[24]were used to conduct a Quality Score
Assessment. The quality criteria were (1) analytical validity of genotyping (including sample
types, time of sample collection, genotyping method, and quality control measures); (2)
selection of study subjects (including geographic area(s), recruitment period, methods,
exclusion criteria for cases and controls, sample size, mean age with SD or age range of study
Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
subjects, and sex ratio); (3) population stratification (including identified potential correlates
of the genotype and potential correlates taken into consideration for design or analysis); (4)
statistical issues (including the number of subjects included in the analysis, analysis method,
software used to perform the analysis, and confidence intervals [CIs]). Studies were graded as
“++”, “+”or “-”, respectively, depending on whether most criteria, some criteria, or no
criteria were fulfilled.
Statistical analysis
In our meta-analysis, we defined CYP2C9 *1/*1genotype (the wild type) as the
reference group, and included any genotype containing at least one variant allele (*2 or *3) in
the variant group. To reduce the existence of any heterogeneity due to pharmacodynamic
differences in warfarin sensitivity among study populations, warfarin maintenance doses
(mean ± SD) for each genotype group (including the variant group) were normalized using
the method of Lindh et al[6] ( dividing the mean maintenance dose of reference group).The
normalized mean daily warfarin dose (MDWDs) of the genotype groups were compared with
the MDWD of the reference group. However, due to the normalization procedure, results
were not expressed as absolute difference, but as relative differences (e.g., a mean difference
of 0.5 indicates a 50% increase in the MDWD.)[6].
Meta-analysis was conducted using Review Manager Software version 5.2.3. The inverse
variance method was used to weight each study, and the mean difference (MD) was
employed to determine the effect of each CYP2C9 genotype on the MDWD. The Weighted
Mean Difference (WMD) could be acquired by multiplying each MD by the relative weight
Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
of each study. The total WMD in each comparison was obtained by adding each WMD of the
included studies, indicating the effect of each SNP on the MDWD. The influence of genotype
polymorphism was considered statistically significant when the P-value was less than 0.05.
Heterogeneity among studies for each comparison group was tested by Cochran's Q test
(Mantel-Haenszel chi-squared test), and expressed by the PH value and I2. A PH value >0.1 or
I2
< 25% was defined as negative for heterogeneity[6].Then, a fixed effect model was used in
the absence of heterogeneity; whereas, a random effect model was used if it was present.
Sensitivity analyses were performed using a one by one study elimination process.
Publication bias was also assessed using tests from Begg[25] and Egger's test[26].
Results
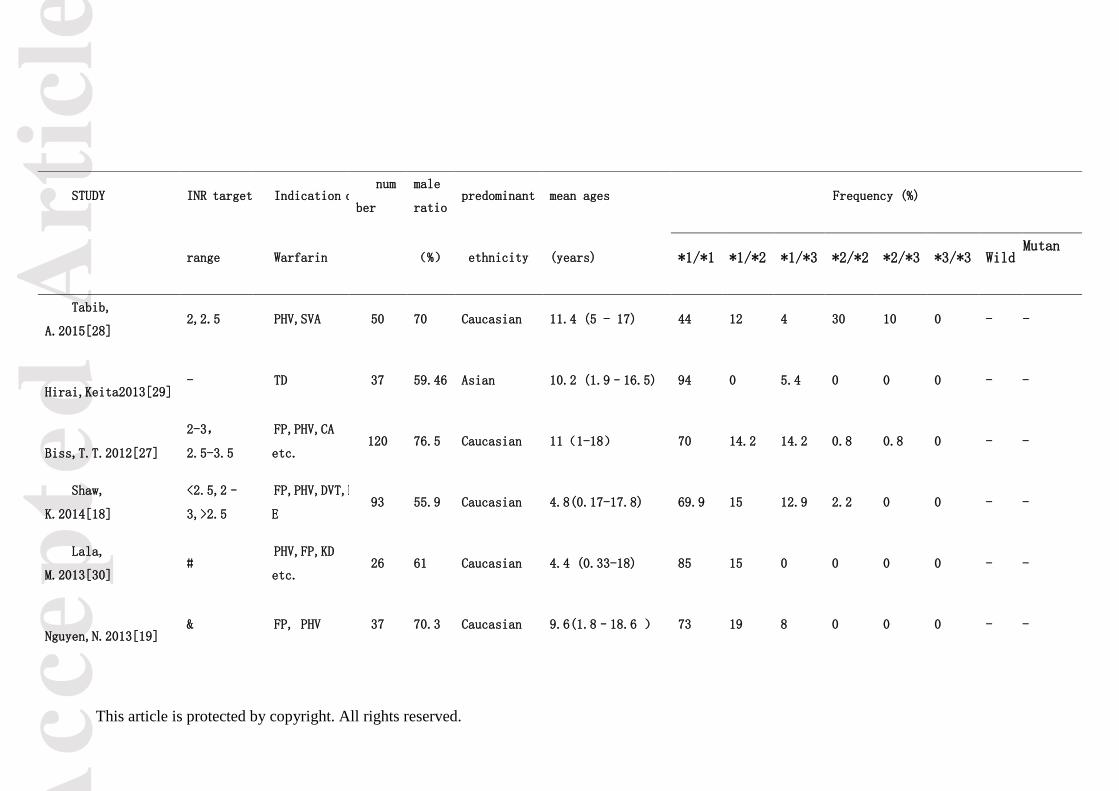
Study identification and characteristics
A total of 210 articles were screened through the literature search. Use of strict
inclusion/exclusion criteria resulted in only eight articles with a total of 507 pediatric patients
remaining for meta-analysis [16-19,27-30].The flow diagram for study selection is shown in
Supplementary Figure S1. All studies are of high quality, being graded as “++”. Some studies
were excluded for insufficient data [20-22,31]. All of the included remaining studies were
published in English and primarily consisted of Caucasian patients, except for the one by
Hirai et al[29].Years of publication ranged from 2012 to 2015. Characteristics of selected
studies are shown in Table 1.
Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
The frequency of *1/*1 (wild type), *1/*2, *1/*3, *2/*2, and *2/*3 was calculated as
70.4%, 13.8%, 10.7%, 3.6%, and 1.6, respectively. No pediatric patients in the remaining
studies had the CYP2C9 *3/*3 genotype. Comparison of CYP2C9 genotype frequencies
between adult and pediatric patients is shown in Supplementary Table S1.
Meta-analysis
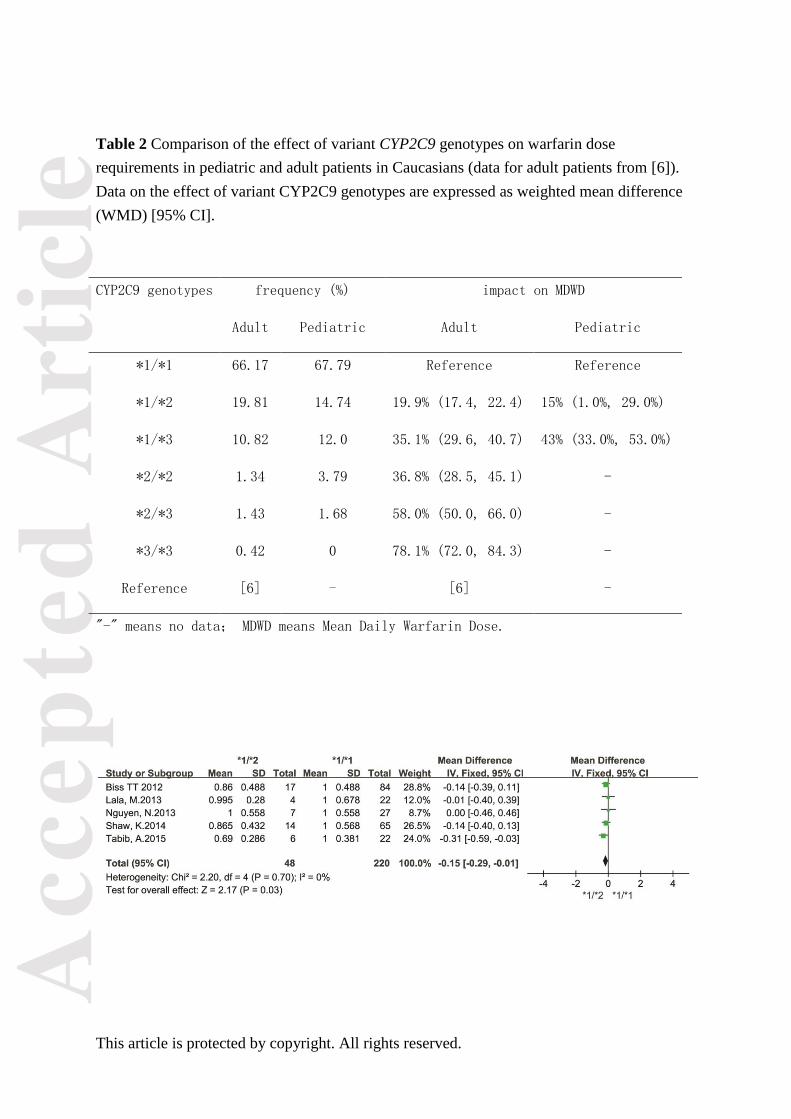
The relationship between CYP2C9 *1/*2 and warfarin maintenance dosage
There were five studies investigating the impact of the CYP2C9 *1/*2 genotype on
warfarin maintenance dosage [18,19,27,28,30]. The result of the meta-analysis is shown in
Fig. 1. Analysis revealed that the CYP2C9 *1/*2 genotype was associated with a warfarin
maintenance dose that was 15% lower than that found with CYP2C9*1/*1 (wild) genotype
(P = 0.03, WMD = -0.15, 95% CI -0.29 to -0.01). (No heterogeneity was found in the
meta-analysis [I2
= 0%, PH = 0.70], so a fixed-model was used.) The effect of CYP2C9
*1/*2on warfarin maintenance dosage in Caucasians pediatric patients was compared to adult
patients, and is shown in Supplementary Table S1.
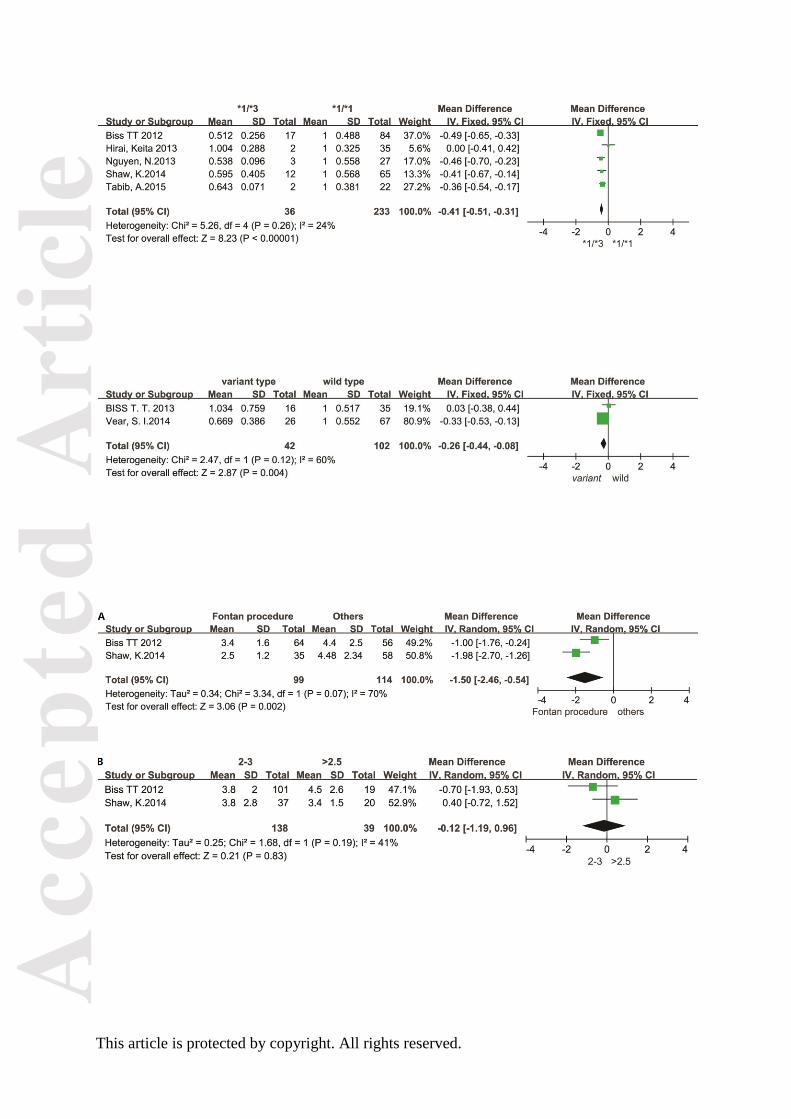
The relationship between CYP2C9 *1/*3 and warfarin maintenance dosage
There were also five studies included for meta-analysis which gave data for the CYP2C9
*1/*3 genotype [18,19,27-29].Compared with the wild genotype, pediatric patients with
CYP2C9 *1/*3 required a 41% lower warfarin maintenance dose (P < 0.00001, WMD=
-0.41, 95% CI -0.51 to -0.31). (Again, the fixed-model was applied due to lack of
Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
heterogeneity [I2
< 25%, PH = 0.26]). The result is presented in Fig. 2. A comparison of the
CYP2C9 *1/*3 genotype between pediatric and adult patients in Caucasians is found in
Supplementary Table S1.
The relationship between CYP2C9 variant carriers and warfarin maintenance dosage
Two studies focused on the relationship between the CYP2C9 variant genotype and
warfarin maintenance dosage[16,17].The results of meta-analysis are shown in Fig. 3, which
indicate that pediatric patients with a variant carriers required significantly lower warfarin
maintenance dosage than those with the wild-type (P = 0.004, WMD = -0.26, 95% CI -0.44
to -0.08). (A fixed model method was used because analysis showed homogeneity
[PH = 0.12]).
The effect of clinical characteristics on warfarin maintenance dosage
Included studies provided data on the significance of only two clinical factors in pediatric
patients—namely, indication for warfarin and target INR range[18,27].For analyzing data, we
divided target INR ranges into a 2–3 INR range group and a >2.5 INR group, as we had in a
previous study[32]. Indications for warfarin were also divided into two groups, Fontan
procedure vs. “others”. Meta-analysis revealed that the Fontan procedure indication was
associated with a lower warfarin maintenance dose requirement (WMD = -1.50, 95% CI
-2.46 to -0.54), while the target INR had no effect on the dose requirement (WMD = -0.12,
95% CI -1.19 to 0.96). The random effect model was used in the two meta-analyses (I2
≥
41%). The results were similar to those of our previous study[32] and are shown in Fig.4A
and 4B
Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
Sensitivity analysis and Publication bias
Sensitivity analysis was conducted using the method of eliminating studies one by one.
There were no significant differences or revisal changes, which meant that the results of this
analysis were stable. Both Begg's[25] and Egger's tests[26] were applied to detect publication
bias in each analysis, and none was found. These analyses indicate that our results are stable
and reliable.
Discussion
The results of meta-analysis showed that comparing to the CYP2C9 *1/*1genotype,
the CYP2C9 *1/*2genotype required15% lower warfarin maintain doses (95% CI -0.29
to -0.01), the CYP2C9*1/*3 genotyperequired 41% lower warfarin maintain doses
(95% CI -0.51 to -0.31), and the CYP2C9 variant carriers were required 26% lower
warfarin maintain doses (95% CI -0.44 to -0.08), respectively. The indication of Fontan
procedure was also associated with a lower warfarin maintenance dose (WMD=-1.50,
95% CI -2.46 to -0.54), while the target INR range was not related to the dosage level (P >
0.05).
It is well known that gene polymorphisms affect warfarin maintenance dose
requirements for adult patients, and that warfarin dosing algorithms should be used to address
the presence of variant genotypes and other factors[2,6,11,33-35].Taskın et al. have certified
Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
that pediatric Patients with allelic variants (VKORC1 and CYP2C9) required lower warfarin
doses, and a 64.5% correlation could be found between their calculated ideal doses and
administered warfarin doses[36].The effect of VKORC1 −1639 SNPs on pediatric warfarin
maintenance dosage has been examined[32], and the result was consistent with a previous
study in adult patients[37].Many studies have indicated that CYP2C9 polymorphisms
significantly influence warfarin maintenance dose in pediatric patients[16,18,27].The variant
genotypes CYP2C9 *1/*2 and *1/*3 are the most common and have been found to be
important factors related to warfarin dosage in adults [6].Therefore, we chose to conduct a
meta-analysis examining these two genotypes (*1/*2 and *1/*3) and warfarin dosing in
pediatric patients, and obtained results similar to those found with adult patients[6].
In addition, we believe clinical factors should be taken into consideration in the
determination of warfarin maintenance doses. Sixteen years ago, Streif et
al.[38]demonstrated, based on data from 319 patients, that age and the clinical indication for
warfarin use was associated with the actual maintenance dose needed. Since then, more
studies have shown that various clinical factors (age, weight, indication for warfarin, and
target INR range) significantly affect the maintenance dose requirement[16,18,19,27].In this
meta-analysis, the effect of two factors (target INR range and indication of warfarin) were
analyzed and results showed that pediatric patients on warfarin for a history of Fontan
procedure needed significantly lower warfarin doses, whereas the target INR range did not
influence dosage requirements.
Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
We performed a comparison of the CYP2C9 genotype frequency and the association
between CYP2C9 genotypes and warfarin maintenance dose for adult and pediatric patients in
Caucasian. The results were similar (see Supplementary Table S1). However, due to the low
frequencies of the CYP2C9 *2/*2, CYP2C9 *2/*3, and CYP2C9 *3/*3 genotypes, and the
small number of articles and pediatric sample sizes, the impact of these genotypes on
warfarin maintenance dose requirement is uncertain.
Sensitivity analysis and other tests revealed no publication bias or heterogeneity,
showing that the results of our meta-analysis are stable and reliable.
Considering the results of this study in combination with those from our previous study
that focused on VKORC1 polymorphism and pediatric warfarin maintenance dosing[32],we
believe that gene polymorphisms do significantly affect warfarin maintenance dosage
requirements in children. Although studies in pediatric patients to date are limited in terms of
sample size and lack of ethnic diversity, considering the data from adult studies, we do feel
that the addition of genotype to current warfarin dosing algorithms for pediatric patients
would be beneficial. Genotyping should certainly be considered for all pediatric patients who
are at high risk of bleeding complications, who are warfarin-resistant, or who suffer adverse
events while receiving warfarin.
Limitations and Perspectives
Although sensitivity analysis reflected stable results without publication bias, the results
of this meta-analysis should be considered with caution, due to the limited number of studies
meeting selection criteria and overall low numbers of pediatric patients. Moreover, the effects
Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
of the CYP2C9 *3/*3, *2/*2, and *2/*3 genotypes on warfarin maintenance dosage are still
uncertain, because rare research mentioned them. In addition, all studies except for one study
[29] involved in primarily Caucasian patients; therefore, the effect of CYP2C9 polymorphism
on warfarin dose requirements in Asian and African pediatric patients is undefined. More
studies looking at the relationship between CYP2C9 polymorphism and warfarin are
necessary in the future. More research examining the impact of clinical factors, such as the
medical indication for anticoagulation and age, are also needed and anticipated. Finally,
future studies, which will update this meta-analysis, and pharmacogenetic dosing algorithms,
which will be developed for pediatric patients as they have been for adults, were hope.
Conclusion
This meta-analysis firstly focused on the relationship between CYP2C9 polymorphism
and warfarin maintenance dose in pediatric patients, and we found that the CYP2C9 *1/*2,
CYP2C9 *1/*3, and CYP2C9 variant genotypes required significantly lower warfarin daily
doses. It was also shown that pediatric patients needing anticoagulation after a Fontan
procedure required significantly lower warfarin maintenance doses. A larger number of
studies is required to ensure against publication bias and confirm generalizability. More data
is also needed to build pharmacogenetic dosing algorithms for pediatric patients. Ideally,
these algorithms will include both genotype data (CYP2C9 and VKORC1) and clinical factors
(such as age, indication for warfarin, weight and possibly others).
Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
Funding sources
This work was supported by grants from the National Natural Science Foundation of
China (81370629), National and Fujian Provincial Key Clinical Specialty Discipline
Construction Program, P.R.C, the Scientific Research Foundation for the Returned Overseas
Chinese Scholars, State Education Ministry (2015B001) and the Fujian Medical Innovation
Project (2014-CX-18).
Conflict of Interest
The authors declared no conflict of interest.
References
[1] Klein TE, Altman RB, Eriksson N, Gage BF, Kimmel SE, Lee MT, et al. Estimation
of the warfarin dose with clinical and pharmacogenetic data. N Engl J of Med
2009;360:753-764.
[2] Gage BF, Lesko LJ. Pharmacogenetics of warfarin: regulatory, scientific, and clinical
issues. J Thromb Thrombolysis 2007;25:45-51.
[3] Sconce EA, Khan TI, Wynne HA, Avery P, Monkhouse L, King BP, et al. The impact
of CYP2C9 and VKORC1 genetic polymorphism and patient characteristics upon
warfarin dose requirements: proposal for a new dosing regimen. Blood.
2005;106:2329-2333.
[4] Vear SI, Stein CM, Ho RH. Warfarin pharmacogenomics in children. Pediatric blood
& cancer 2013:60(9):1402-1407.
[5] Aithal GP, Day CP, Kesteven PJ, Daly AK. Association of polymorphisms in the
cytochrome P450 CYP2C9 with warfarin dose requirement and risk of bleeding
complications. The Lancet 1999:353(9154):717-719.
Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
[6] Lindh JD, Holm L, Andersson ML, Rane A. Influence of CYP2C9 genotype on
warfarin dose requirements—a systematic review and meta-analysis. European
journal of clinical pharmacology. 2009;65:365-75.
[7] Gao L, He L, Luo J, Xu B, Yang J, Zhang YX, et al. Extremely low warfarin dose in
patients with genotypes of CYP2C9*3/*3 and VKORC1-1639A/A. Chin Med J.
2011:124(17):2767-2770.
[8] Tatarūnas V, Lesauskaite V, Veikutiene A, Grybauskas P, Jakuska P, Benetis R. The
combined effects of clinical factors and CYP2C9 and VKORC1 gene polymorphisms
on initiating warfarin treatment in patients after cardiac valve surgery. J Heart Valve
Dis 2012:21(5):628-635.
[9] Krajciova L, Deziova L, Petrovic R, Luha J, Turcani P, Chandoga J. Frequencies of
polymorphisms in CYP2C9 and VKORC1 genes influencing warfarin metabolism in
Slovak population: implication for clinical practice. Bratisl Lek Listy
2014:115(9):563-568.
[10] Ghozlan MF, Foad DA, Darwish YW, Saad AA. Impact of CYP2C9 and VKORC1
genetic polymorphisms upon warfarin dose requirements in Egyptian patients with
acute coronary syndrome. Blood Coagul Fibrinolysis 2015:26(5):499-504.
[11] Jorgensen AL, FitzGerald RJ, Oyee J, Pirmohamed M, Williamson PR. Influence of
CYP2C9 and VKORC1 on patient response to warfarin: a systematic and
Meta-Analysis. PLoS One 2012:7(8): e44064.
[12] Hamberg AK, Friberg LE, Hanseus K, Ekman-Joelsson BM, Sunnegårdh J, et al.
Warfarin dose prediction in children using pharmacometric bridging--comparison
with published pharmacogenetic dosing algorithms. Eur J Clin Pharmacol
2013:69(6):1275-1283.
[13] Visscher H, Amstutz U, Sistonen J, ,Ross CJ, Hayden MR, Carleton BC.
Pharmacogenomics of cardiovascular drugs and adverse effects in pediatrics. J
Cardiovasc Pharmacol 2011:58(3):228-239.
[14] Hamberg AK, Wadelius M. Pharmacogenetics-based warfarin dosing in children.
Pharmacogenomics 2014:15(3):361-374.
[15] Monagle P, Newall F, Campbell J. Anticoagulation in neonates and children: Pitfalls
and dilemmas. Blood Rev 2010:24(4-5):151-162.
Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
[16] Vear SI, Ayers GD, Van Driest SL, Sidonio RF, Stein CM, Ho RH. The impact of age
and CYP2C9 and VKORC1 variants on stable warfarin dose in the paediatric
population. British journal of haematology.2014:165(6):832-835.
[17] Biss TT, Avery PJ, Williams MD, Brandao LR, Grainger JD, Kamali F. The
VKORC1 and CYP2C9 genotypes are associated with over-anticoagulation during
initiation of warfarin therapy in children. Journal of thrombosis and haemostasis :
JTH 2013:11(2):373-375.
[18] Shaw K, Amstutz U, Hildebrand C, Rassekh S. R, Hosking M, Neville K, et al.
VKORC1 and CYP2C9 genotypes are predictors of warfarin-related outcomes in
children. Pediatric Blood and Cancer 2014;61:1055-1062.
[19] Nguyen. N, Anley. P, Yu. MY, Zhang. G, Thompson. AA, Jennings. LJ. Genetic and
clinical determinants influencing warfarin dosing in children with heart disease.
Pediatric cardiology 2013;34:984-990.
[20] Moreau. C, Bajolle. F, Siguret. V, Lasne. D, Golmard. JL, Elie. C, et al. Vitamin K
antagonists in children with heart disease: height and VKORC1 genotype are the main
determinants of the warfarin dose requirement. Blood 2012;119:861--867.
[21] Nowak-Gottl U, Dietrich K, Schaffranek D, Eldin NS, Yasui Y, Geisen C, et al. In
pediatric patients, age has more impact on dosing of vitamin K antagonists than
VKORC1 or CYP2C9 genotypes. Blood 2010;116:6101-6105.
[22] Kamal El-Din MA, Farhan MS, El Shiha RI, El-Kaffas RMH, Mousa SM. Frequency
of CYP2C9 and VKORC1 gene polymorphisms and their influence on warfarin dose
in Egyptian pediatric patients. Pediatric Drugs 2014;16:337-41.
[23] Kato Y, Ichida F, Saito K, Watanabe K, Hirono K, Miyawaki T, et al. Effect of the
VKORC1 genotype on warfarin dose requirements in Japanese pediatric patients.
Drug Metab Pharmacokinet 2011;26:295-299.
[24] Little J, Bradley L, Bray MS, Clyne M, Dorman J, Ellsworth DL, et al. Reporting,
appraising, and integrating data on genotype prevalence and gene-disease
associations. Am J Epidemiol 2002:156(4):300-310.
[25] Begg CB, Mazumdar M. Operating characteristics of a rank correlation test for
publication bias. Biometrics 1994:50(4):1088-1101.
[26] Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by
a simple, graphical test. Bmj 1997:315(7109):629-634.
Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
[27] Biss TT, Avery PJ, Brandão LR, Chalmers EA, Williams MD, Grainger JD, et al.
VKORC1 and CYP2C9 genotype and patient characteristics explain a large
proportion of the variability in warfarin dose requirement among children. Blood
2012:119(3):868-873.
[28] Tabib A, Najibi B, Dalili M, Baghaei R, Poopak B. Enzyme Polymorphism in
Warfarin Dose Management After Pediatric Cardiac Surgery. Res Cardiovasc Med
2015:4(3):e27963.
[29] Hirai K, Hayashi H, Ono Y, Izumiya K, Tanaka M, et al. Influence of CYP4F2
Polymorphisms and Plasma Vitamin K Levels on Warfarin Sensitivity in Japanese
Pediatric Patients. Drug Metab Pharmacokinet 2013:28(2):132-137.
[30] Lala M, Burckart GJ, Takao CM, Pravica V, Momper JD, Gobburu JV.
Genetics-based pediatric warfarin dosage regimen derived using pharmacometric
bridging. J Pediatr Pharmacol Ther 2013:18(3):209-219.
[31] Ruud E, Holmstrøm H, Bergan S, Wesenberg F. Oral anticoagulation with warfarin is
significantly influenced by steroids and CYP2C9 polymorphisms in children with
cancer. Pediatr Blood Cancer 2008:50(3):710-713.
[32] Zhang J, Tian L, Zhang Y, Shen J. The influence of VKORC1 gene polymorphism on
warfarin maintenance dosage in pediatric patients: A systematic review and
meta-analysis. Thromb Res 2015;136: 955-961.
[33] Sun Y, Wu Z, Li S, Qin X, Li T, Xie L, et al. Impact of gamma-glutamyl carboxylase
gene polymorphisms on warfarin dose requirement: A systematic review and
meta-analysis. Thromb Res 2015:135(4):739-747.
[34] Liang R, Wang C, Zhao H, Huang J, Hu D, Sun Y. Influence of CYP4F2 genotype on
warfarin dose requirement–a systematic review and meta-analysis. Thromb Res
2012:130(1):38-44.
[35] Tian LH, Zhang JH, Xiao SJ, Huang JH, Zhang YY, Shen JZ. Impact of
polymorphisms of the GGCX gene on maintenance warfarin dose in Chinese
populations: Systematic review and meta-analysis. Meta Gene 2015:5:43-54.
[36] Dilge Taskin B, Kula S, Ergun MA, et al. The effect of CYP2C9 and VKORC1
genetic polymorphisms on warfarin dose requirements in a pediatric population.
Anatol J Cardiol 2016: 16: 000-000.
Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
[37] Yang L, Ge W, Yu F, Zhu H. Impact of VKORC1 gene polymorphism on
interindividual and interethnic warfarin dosage requirement— A systematic review
and meta analysis. Thromb Res 2010:125(4):e159-e166.
[38] Streif W1, Andrew M, Marzinotto V, Massicotte P, Chan AK, Julian JA, et al. .
Blood. 1999;94:3007-3014.
Figure Legends
Figure 1: Forest plot showing the influence of CYP2C9 *1/*2 on warfarin maintenance
dosage, compared with individuals with the CYP2C9 *1/*1 genotype (wild type). SD:
standard deviation of normalized mean warfarin doses associated with each genotype. CI:
confidence interval. Brackets denote 95% CIs.
Figure.2: Forest plot showing the influence of CYP2C9 *1/*3 on warfarin maintenance
dosage, compared with individuals with the CYP2C9 *1/*1 genotype (wild type). SD:
standard deviation of normalized mean warfarin doses associated with each genotype. CI:
confidence interval. Brackets denote 95% CIs.
Figure. 3: Forest plot showing the influence of CYP2C9 variant genotype (any genotype
containing at least one variant allele) on warfarin maintenance dosage, compared with
individuals with the CYP2C9 *1/*1 genotype (wild type). SD: standard deviation of
normalized mean warfarin doses associated with each genotype. CI: confidence interval.
Brackets denote 95% CIs.
Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
Figure. 4A and 4B: Forest plot showing the influence of clinical characteristics on warfarin
maintenance dosage. (A)The reduction in warfarin dose requirement associated with the
indication of Fontan procedure; (B) The influence of target INR range on warfarin
maintenance dosage. SD: standard deviation of normalized mean warfarin doses associated
with each genotype. CI: confidence interval. Brackets denote 95% CIs.
Supplementary Figure S1: Flow diagram of the literature screening process.
Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
STUDY INR target Indication of num
ber
male
ratio predominant mean ages Frequency (%)
range Warfarin
(%) ethnicity (years) *1/*1 *1/*2 *1/*3 *2/*2 *2/*3 *3/*3 Wild Mutan
t
Tabib,
A.2015[28] 2,2.5 PHV,SVA 50 70 Caucasian 11.4 (5 - 17) 44 12 4 30 10 0 - -
Hirai,Keita2013[29] - TD 37 59.46 Asian 10.2 (1.9–16.5) 94 0 5.4 0 0 0 - -
Biss,T.T.2012[27]
2-3,
2.5-3.5
FP,PHV,CA
etc. 120 76.5 Caucasian 11(1-18) 70 14.2 14.2 0.8 0.8 0 - -
Shaw,
K.2014[18]
<2.5,2–
3,>2.5
FP,PHV,DVT,P
E 93 55.9 Caucasian 4.8(0.17-17.8) 69.9 15 12.9 2.2 0 0 - -
Lala,
M.2013[30] #
PHV,FP,KD
etc. 26 61 Caucasian 4.4 (0.33-18) 85 15 0 0 0 0 - -
Nguyen,N.2013[19] & FP, PHV 37 70.3 Caucasian 9.6(1.8–18.6 ) 73 19 8 0 0 0 - -
Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
Table 1: Characteristics of included studies.
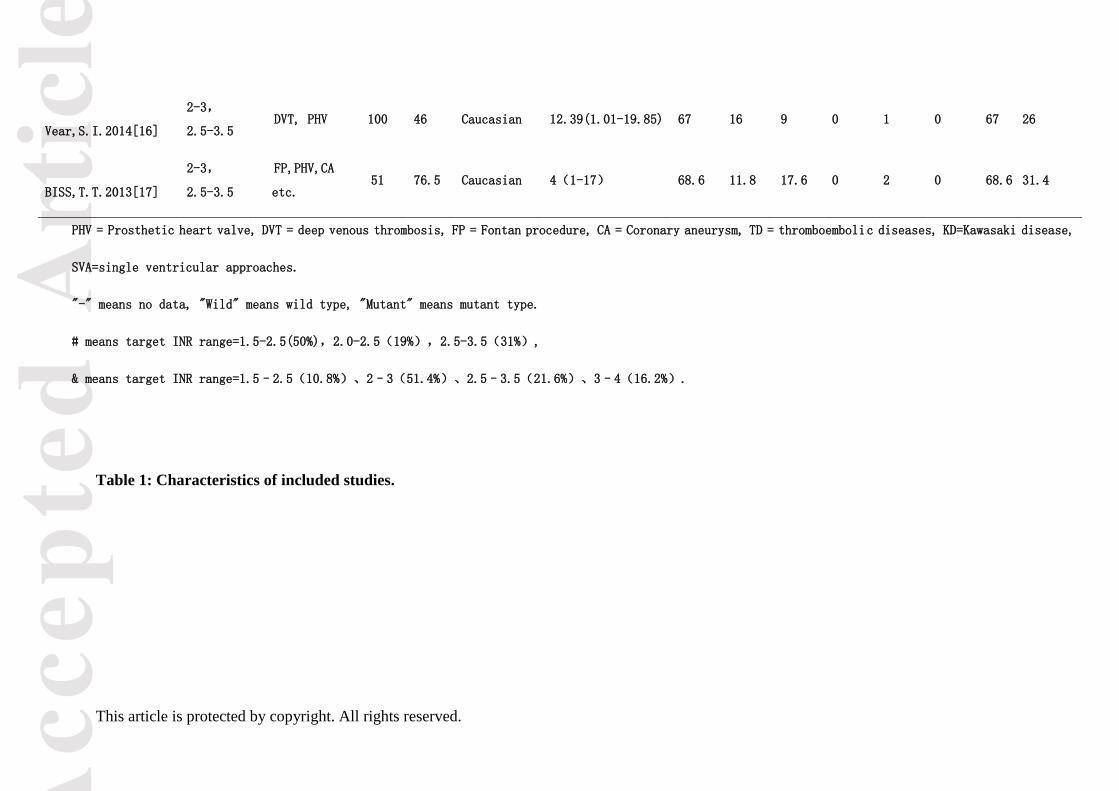
Vear,S.I.2014[16]
2-3,
2.5-3.5 DVT, PHV 100 46 Caucasian 12.39(1.01-19.85) 67 16 9 0 1 0 67 26
BISS,T.T.2013[17]
2-3,
2.5-3.5
FP,PHV,CA
etc. 51 76.5 Caucasian 4(1-17) 68.6 11.8 17.6 0 2 0 68.6 31.4
PHV = Prosthetic heart valve, DVT = deep venous thrombosis, FP = Fontan procedure, CA = Coronary aneurysm, TD = thromboembolic diseases, KD=Kawasaki disease,
SVA=single ventricular approaches.
"-" means no data, "Wild" means wild type, "Mutant" means mutant type.
# means target INR range=1.5-2.5(50%),2.0-2.5(19%),2.5-3.5(31%),
& means target INR range=1.5–2.5(10.8%)、2–3(51.4%)、2.5–3.5(21.6%)、3–4(16.2%).
Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
Table 2 Comparison of the effect of variant CYP2C9 genotypes on warfarin dose
requirements in pediatric and adult patients in Caucasians (data for adult patients from [6]).
Data on the effect of variant CYP2C9 genotypes are expressed as weighted mean difference
(WMD) [95% CI].
CYP2C9 genotypes frequency (%) impact on MDWD
Adult Pediatric Adult Pediatric
*1/*1 66.17 67.79 Reference Reference
*1/*2 19.81 14.74 19.9% (17.4, 22.4) 15% (1.0%, 29.0%)
*1/*3 10.82 12.0 35.1% (29.6, 40.7) 43% (33.0%, 53.0%)
*2/*2 1.34 3.79 36.8% (28.5, 45.1) -
*2/*3 1.43 1.68 58.0% (50.0, 66.0) -
*3/*3 0.42 0 78.1% (72.0, 84.3) -
Reference [6] - [6] -
"-" means no data; MDWD means Mean Daily Warfarin Dose.
Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
本文献由“学霸图书馆-文献云下载”收集自网络,仅供学习交流使用。
学霸图书馆(www.xuebalib.com)是一个“整合众多图书馆数据库资源,
提供一站式文献检索和下载服务”的24 小时在线不限IP
图书馆。
图书馆致力于便利、促进学习与科研,提供最强文献下载服务。
图书馆导航:
图书馆首页 文献云下载 图书馆入口 外文数据库大全 疑难文献辅助工具





























