Embed Size (px)
Citation preview

Cytology of Rosai-DorfmanDisease
Dear Dr. Bedrossian:Sinus histiocytosis with massive lymphadenopathy
(SHML), or so-called “Rosai-Dorfman disease,” is a rareclinicopathologic disorder primarily affecting the cervicallymph nodes in children and adolescents, with a Black malepredominance. Up to 40% of cases present extranodal in-volvement; the commonest sites being the skin, upper re-spiratory tract, and bone. SHML is frequently associatedwith fever, mild anemia, hypergammaglobulinemia, and anelevated erythrocyte sedimentation rate. In most cases, thelymph nodes regress spontaneously, but in some cases,principally with extranodal involvement, the prognosis ispoorer and the patients may require specific therapy (sur-gery, radiation, chemotherapy). The exact etiology remainsunknown, although some infectious and/or immune mech-anisms have been proposed. The morphologic features ofSHML are well-known, but are mainly histologically basedand only a few reports have documented cytologic features.
Recently, inDiagnostic Cytopathology, Deshpande et al.1
described 4 patients presenting SHML who were diagnosedcytologically. The authors underlined that 1) the consistentpresence of large histiocytes with an abundant, pale, foamycytoplasm, and distinct cell membranes showing phagocy-tosis of apparently viable lymphocytes (emperipolesis), and2) the inconsistent presence of plasma-cell phagocytosis,intracellular Russel bodies, and multinucleated histiocytesare characteristic cytologic patterns allowing the accuratediagnosis of this disease.
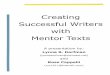
At the Institut Curie we have seen a 7-yr-old Blackfemale with massive bilateral cervical swelling of 6 moduration, without fever, sweating, or asthenia (Fig. 1). Pastmedical history revealed asthma. On clinical examination,large, palpable (9 cm on left and 7 cm on right), and firmcervical lymph nodes were present. Chest X-ray examina-tion and abdominal ultrasonography were normal, with nolymphadenopathy or hepatosplenomegaly. The laboratoryfindings revealed anemia (Hb, 8 g/100 cc), elevated eryth-rocyte sedimentation rate (ESR, 60), and hypergamma-globulinemia (33 g/l). A serologic test demonstrated highToxoplasmaantibody titers. A clinical diagnosis of lym-phoma was proposed. Both cervical lymph nodes wereexamined cytologically. Fine-needle sampling demon-
strated a moderately cellular smear composed of a polymor-phous lymphocytic background containing numerous largehistiocytes with emperipolesis (Fig. 2). Phagocytosed lym-phocytes were numerous, sometimes masking the underly-ing histiocytic nucleus which was usually ovoid in shape,with reticulated chromatin and small but distinct nucleoli.Nuclear grooves were not observed. There was no eryth-rophagocytosis. Some cohesive epithelioid histiocytes werealso present, but Ziehl-Nielsen staining failed to demon-strate microorganisms. No other cytochemical stain or mi-
Fig. 1. Massive bilateral cervical lymphadenopathy (9 cm on left and 7 cmon right), clinically suggestive of lymphoma.
298 Diagnostic Cytopathology, Vol 24, No 4 © 2001 WILEY-LISS, INC.

crobial culture was performed. The cytologic diagnosis ofSHML was subsequently confirmed histologically aftersurgery.
Clinically and morphologically, SHML should be differ-entiated from non-Hodgkin’s and Hodgkin’s lymphomas,nonspecific hyperplasias, infectious disorders, Langerhanscell histiocytosis, hemophagocytic syndrome, and dermato-pathic lymphadenopathy. Non-Hodgkin’s and Hodgkin’slymphomas are characterized cytologically by the presenceof malignant lymphocytes or Reed-Sternberg cells, respec-tively. In reactive nonspecific lymphadenopathies, emperi-polesis is absent. Infectious disorders such as salmonella,rhinoscleroma, and histoplasmosis may show emperipole-sis, but special stains, cultures, and clinical presentationallow the differential diagnosis. Granulomatous lymphade-nitis related to tuberculosis, and sarcoidosis, are character-ized cytologically by cohesive aggregates of epithelioidhistiocytes. These cells, contrary to those seen in SHML,have ill-defined cytoplasm and, while they may containnecrotic debris, they do not show emperipolesis. Langer-hans cell histiocytosis is characterized by the presence oflarge histiocytes with nuclear grooves associated withprominent eosinophilic infiltrates. Hemophagocytic syn-
drome is characterized by hemophagocytosis, but not lym-phophagocytosis. In addition, the suggestive clinical ap-pearance helps to distinguish between these two syndromes.Dermatopathic lymphadenopathy is characterized by thepresence of Langerhans cells and histiocytes that containiron and melanin pigment.
A review of the literature1–13 shows that only 19 patientspresenting SHML were initially studied cytologically and cor-related with histology (Table I). Patients’ ages ranged from1–71 yr (mean, 23.2; median, 14). There were 10 males and 9females. Clinically, patients presented with massive bilateralcervical lymphadenopathy in 11 cases,1,4,7–10,12unilateral cer-vical lymphadenopathy in 4 patients,2,3,5,10 and inguinallymphadenopathy in 1 case.10 Interestingly, 3 patients pre-sented as having a breast tumor,6,11,13and 3 patients presentedextranodal disease.4,7,10 Fifteen of these 19 cases were accu-rately diagnosed; 2 were misdiagnosed as nonspecific lymph-adenitis;2,8 and 2 were false-suspicious,11,13 leading to histo-logical verification.
In conclusion, the presence of histiocytes with emperi-polesis is highly characteristic of Rosai-Dorfman disease.We therefore agree with Deshpande et al.1 and other au-thors8,9 who claimed that the diagnosis of this entity may be
Fig. 2. Fine-needle sampling of lymphadenopathy composed of polymorphous lymphocytic background containing numerous large histiocytes withemperipolesis (May-Gru¨nwald-Giemsa stain,3200).
CYTOLOGY OF ROSAI-DORFMAN DISEASE
Diagnostic Cytopathology, Vol 24, No 4 299

based exclusively on cytologic findings, especially in theappropriate clinical setting. Histological examination maybe indicated when cytology is not conclusive.
Christian Lussier,M.D. Jerzy Klijanienko,M.D.
HerveBrisse,M.D. Erica Quintana,M.D.
Philippe Vielh,M.D., Ph.D.
Institut CurieParis, France
Nicole Brousse,M.D.
Hopital Necker-Enfants MaladesParis, France
References1. Deshpande AH, Nayak S, Munshi MM. Cytology of sinus histiocytosis
with massive lymphadenopathy (Rosai-Dorfman disease). Diagn Cy-topathol 2000;22:181–185.
2. Layfield LJ. Fine needle aspiration cytologic findings in a case of sinushistiocytosis with massive lymphadenopathy (Rosai-Dorfman syn-drome). Acta Cytol 1990;34:767–770.
3. Pettinato G, Manivel JC, d’Amore ESG, Petrella G. Fine needleaspiration cytology and immunocytochemical characterization of thehistiocytes in sinus histiocytosis with massive lymphadenopathy (Ro-sai-Dorfman syndrome). Acta Cytol 1990;6:771–777.
4. Trautman BC, Stanley MW, Goding GS, Rosai J. Sinus histiocytosiswith massive lymphadenopathy (Rosai-Dorfman disease) diagnosis byfine-needle aspiration. Diagn Cytopathol 1991;7:513–516.
5. Chang Y. Sinus histiocytosis with massive lymphadenopathy: report ofa case with fine needle aspiration cytology. Acta Cytol 1993;37:186–190.
6. Perez-Guillermo M, Sola-Pe´rez J, Rodriguez-Bermejo M. Malakopla-kia and Rosai-Dorfman disease: two entities of histiocytic origininfrequently localized in the female breast—the cytologic aspect inaspirates obtained via fine-needle aspiration cytology. Diagn Cyto-pathol 1993;9:698–704.
7. Alegret RA, Martinez A, Ramirez T, Ga`llego P, Martinez D, Julia`nGG. Sinus histiocytosis with massive lymphadenopathy (Rosai-Dorf-man disease): diagnosis with fine-needle aspiration in a case withnodal and nasal involvement. Diagn Cytopathol 1995;13:333–335.
8. Gupta S, Gupta DC. Cytologic appearance of sinus histiocytosis withmassive lymphadenopathy: a case report. Acta Cytol 1996;40:595–598.
9. Patel KD, Rege JD, Naik LP. Fine-needle aspiration cytology of sinushistiocytosis with massive lymphadenopathy: a case report. DiagnCytopathol 1996;15:221–223.
10. Stastny JF, Wilkerson ML, Hamati HF, Kornstein MJ. Cytologicfeatures of sinus histiocytosis with massive lymphadenopathy: a reportof three cases. Acta Cytol 1997;41:871–876.
11. Hummel P, Waisman J, Chhieng D, Yan Z, Cohen JM, Cangiarella J.Fine-needle aspiration cytology of Rosai-Dorfman disease of thebreast: a case report. Diagn Cytopathol 1999;21:287–291.
12. Viguer JM, Jime´nez-Heffernan JA, Lopez-Ferrer P, Vicardi B. Impor-tance of Papanicolaou-stained smears and immunocytochemistry inthe diagnosis of Rosai-Dorfman disease. Acta Cytol 1999;43:328–329.
13. Ng SB, Tan LHC, Tan PH. Rosai-Dorfman disease of the breast: amimic of breast malignancy. Pathology 2000;32:10–15.
Table I.Sinus Histiocytosis With Massive Lymphadenopathya
Reference Age (yr) Sex
Laboratory testsClinical
presentationClinical
diagnosis Cytologyg-pathy ESR
2 5 M ND ND Neck ML, U ND Inflammatory3 3 M N N Neck ML, U Lymphoma SHML4 14 M ND ND Neck ML, B Inflammatory SHML5 30 M N N Neck ML, U ND SHML6 71 F ND ND Breast Fibroadenoma SHML7 62 F ND ND Neck ML, B Lymphoma SHML8 14 M ND E Neck ML, B Lymphoma Inflammatory9 12 M N N Neck ML, B Lymphoma SHML10 10 F ND ND Neck ML, U ND SHML
21 F N E Inguinal ML ND SHML6 F ND E Neck ML, B Inflammatory SHML
11 52 F ND ND Breast ND Suspicious12 3 M ND ND Neck ML, B ND SHML
1 F ND ND Neck ML, B ND SHML13 61 F N ND Breast Cancer Suspicious1 17 M N E Neck ML, B Lymphoma SHML
22 M N E Neck ML, B Lymphoma SHML25 M N E Neck ML, B Tuberculosis SHML12 F E E Neck ML, B Lymphoma SHML
Our case 7 F E E Neck ML, B Lymphoma SHMLaCases diagnosed by fine-needle sampling and verified by histology. ESR, erythrocyte sedimentation rate; M, male; ND, not done; N, normal; ML, multiplelymphadenopathy; U, unilateral; SHML, sinus histiocytosis with massive lymphadenopathy; B, bilateral; F, female; E, elevated.
CHRISTIAN ET AL.
300 Diagnostic Cytopathology, Vol 24, No 4