Embed Size (px)
Citation preview

517
Review
www.expert-reviews.com ISSN 1746-9899© 2011 Expert Reviews Ltd10.1586/EOP.11.49
CMECME
Aliza Jap1,2 and Soon-Phaik Chee†1,3,4
1Singapore National Eye Centre, 11 Third Hospital Avenue, 168751, Singapore 2Division of Ophthalmology, Changi General Hospital, 2 Simei Street 3, 529889, Singapore 3Department of Ophthalmology, Yong Loo Lin School of Medicine, National University of Singapore, 10 Kent Ridge Crescent, 119260, Singapore 4Singapore Eye Research Institute, 11 Third Hospital Avenue, 168751, Singapore †Author for correspondence:Tel.: +65 6227 7255 Fax: +65 6226 3395 [email protected]
Cytomegalovirus (CMV) has increasingly been found as a cause of anterior segment infection in immunocompetent patients. This may manifest as an endotheliitis or as an acute episodic or chronic recurrent anterior uveitis, which is often associated with ocular hypertension. Its diagnosis is based on aqueous ana lysis for CMV DNA by PCR or for CMV-specific antibodies. Although it has a high response rate to systemic, intravitreal and ganciclovir implant, the relapse rate is also high, and patients may require prolonged treatment. Topical ganciclovir gel has a lower response rate but also a lower relapse rate and fewer adverse effects. The main cause of visual loss in CMV anterior uveitis is glaucoma, and endothelial failure in endotheliitis. Therefore, early diagnosis and treatment is vital, and glaucoma therapy is an important adjunctive modality of management.
Keywords: anterior uveitis • corneal decompensation • endotheliitis • ganciclovir • ocular hypertension • Posner–Schlossman syndrome • valganciclovir
Cytomegalovirus-associated anterior segment infectionExpert Rev. Ophthalmol. 6(5), 517–528 (2011)
Medscape:ContinuingMedicalEducationOnline
This activity has been planned and implemented in accordance with the Essential Areas and policies of the Accreditation Council for Continuing Medical Education through the joint spon-sorship of Medscape, LLC and Expert Reviews. Medscape, LLC is accredited by the ACCME to provide continuing medical education for physicians.
Medscape, LLC designates this Journal-based CME activity for a maximum of 1 AMA PRA Category 1 Credit(s)™. Physicians should claim only the credit commensurate with the extent of their participation in the activity.
All other clinicians completing this activity will be issued a certificate of participation. To partici-pate in this journal CME activity: (1) review the learning objectives and author disclosures; (2) study the education content; (3) take the post-test with a 70% minimum passing score and com-plete the evaluation at www.medscape.org/journals/expertophth; (4) view/print certificate.
Learningobjectives
Upon completion of this activity, participants will be able to:• Describe the clinical presentation of CMV-associated anterior segment infection
• Describe the diagnosis of CMV-associated anterior segment infection
• Describe the treatment of CMV-associated anterior segment infection
Releasedate: October6, 2011;Expirationdate:October6, 2012
For reprint orders, please contact [email protected]
Exp
ert R
evie
w o
f O
phth
alm
olog
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y W
ashi
ngto
n St
ate
Uni
vers
ity o
n 10
/25/
14Fo
r pe
rson
al u
se o
nly.

Expert Rev. Ophthalmol. 6(5), (2011)518
Review CMEJap & Chee
Cytomegalovirus (CMV) is a member of the herpes virus family and, as with other DNA viruses, life-long latency is a hallmark of CMV infection. Primary CMV infection in immunocompetent individuals is often asymptomatic or may present with only mild nonspecific systemic symptoms, such as fever, generalized fatigue, myalgia and sore throat. However, in patients with AIDS, it can cause severe disease, including encephalitis and pneumonia.
Ocular infection from reactivation of latent CMV was originally described in patients with AIDS, where it manifests predominantly as retinitis. In recent years, more and more cases of CMV infection of the anterior segment have been recognized in immunocompetent people also. In developed countries, the seroprevalence of CMV is approximately 50%, whereas it is approximately 90% in less-developed regions [1–4]. Hence, not surprisingly, most of these cases have been from Asian countries, where there is a large reservoir of dormant CMV. In these immunocompetent individuals, ocular involvement consists predominantly of a unilateral anterior uveitis, which may have either an acute recurrent or a chronic persistent course, or as a corneal endotheliitis.
Clinical featuresAnterior uveitisIn the past 5 years, 113 cases (110 patients) of CMV-positive anterior uveitis were reported [5–12]; of which, only 13 (11.5%) were from non-Asian populations [7,9,11], and CMV-positive anterior uveitis constituted 23% of all hypertensive uveitis eyes seen in one institution [13]. Of these 113 cases, 72 (64%) had an acute recurrent course, 30 eyes (27%) had chronic persistent uveitis, one had sector iris atrophy resembling herpes simplex virus (HSV)/varicella zoster virus (VZV) anterior uveitis and ten had an unknown course [5–14]. Although these eyes shared certain common features, such as elevated intraocular pressure (IOP; 106 eyes [94%]), diffuse iris atrophy (29 eyes [26%]), absence of both posterior synechiae (100%) and posterior segment involvement (99%), there were also important differences between these two entities (Table 1) [5–14].
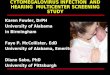
Acute recurrent uveitisOut of 72 eyes, 71 with acute recurrent disease had been diag-nosed previously as having Posner–Schlossman syndrome, as the clinical features of both entities were very similar. It typically presents with recurrent episodes of mild iritis with a few keratic precipitates (KPs), a grade of less than 2+ for anterior chamber (AC) cells and epithelial edema from elevated IOP. The eye is quiet with normal IOP inbetween attacks. KPs are usually white and fine-to-medium sized (Figure 1), although one-quarter of the eyes (nine eyes) were also noted to have nodular endothelial lesions [14], which consist of white medium-sized nodular depos-its on the endothelium, surrounded by a translucent halo and occasionally accompanied by a spot of brown pigment.
Chronic persistent uveitisThe KPs in eyes with chronic persistent uveitis are more numerous and diffusely distributed. There is usually a mix of different-sized KPs, ranging from fine stellate or filiform to medium-sized, and occasionally, even of mutton fat appearance [7,8,15]. Nodular endothelial lesions (Figure 2) were seen in 60% (nine eyes) [14]. The AC cellular reaction, again, is generally mild, with 2+ cells or less. Elevated IOP was also a promi-nent feature, being present in all except seven eyes (76.7%). However, the maximum pressure elevation (mean: 32 mmHg) was lower than that seen in eyes with acute recurrent uveitis (mean: 49 mmHg). Diffuse iris atrophy and cataracts were more common in eyes with chronic persistent disease (67 and 75%, respectively) than in acute recurrent disease (39 and 15%, respectively), and patients with chronic uveitis tended to be older (mean: 55 years) than those with acute recurrent uveitis (mean: 39 years) [14].
One eye also developed arteriolar attenuation with diffuse pigmentary changes, despite the absence of any overt retini-tis. This was attributed to possible subclinical CMV retini-tis or an auto immune retinopathy, as the patient antiretinal autoantibodies [15].
Financial & competing interests disclosureediTor
Elisa ManzottiEditorial Director, Future Science Group, London, UK. Disclosure: Elisa Manzotti has disclosed no relevant financial relationships.CME AuthorLaurie Barclay, MDFreelance writer and reviewer, Medscape, LLC.Disclosure: Laurie Barclay, MD, has disclosed no relevant financial relationships.Authors and CredentialsAliza Jap, FRCOphthSingapore National Eye Centre, Division of Ophthalmology, Changi General Hospital, Singapore.Disclosure: Aliza Jap, FRCOphth, has disclosed no relevant financial relationships.Soon-Phaik Chee, FRCOphthSingapore National Eye Centre, Department of Ophthalmology, Yong Loo Lin School of Medicine, National University of Singapore; Singapore Eye Research Institute, Singapore.Disclosure: Soon-Phaik Chee, FRCOphth, has disclosed no relevant financial relationships.
Exp
ert R
evie
w o
f O
phth
alm
olog
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y W
ashi
ngto
n St
ate
Uni
vers
ity o
n 10
/25/
14Fo
r pe
rson
al u
se o
nly.

www.expert-reviews.com 519
ReviewCME Cytomegalovirus-associated anterior segment infectionTa
ble
1. L
iter
atu
re r
evie
w o
f cl
inic
al f
eatu
res
of
cyto
meg
alo
viru
s an
teri
or
uve
itis
in n
on
-HIV
-po
siti
ve p
atie
nts
.
Stu
dy
(yea
r)Ey
es (
n)
Ker
atic
pre
cip
itat
es/
ante
rio
r ch
amb
er
infl
amm
atio
n
Intr
aocu
lar
pre
ssu
re
>21
mm
Hg
Iris
atr
op
hy
Clin
ical
co
urs
eG
lau
com
a su
rger
y/g
lau
com
ato
us
atro
ph
y
Co
mm
ents
Ref
.
Che
e et
al.
(201
0,
200
8,
200
8)
72
(70
patie
nts)
Few
and
fine
in a
cute
re
curr
ent
dise
ase
Dif
fuse
ste
llate
in c
hron
ic
pers
iste
nt d
isea
seN
odul
ar e
ndot
helia
l les
ions
: 18
eye
sM
ild in
flam
mat
ion
14 c
hron
ic
pers
iste
nt
All
acut
e re
curr
ent
Dif
fuse
: 24
eyes
Sect
or ir
is a
trop
hy: 1
eye
Abs
ent:
26
eyes
Unk
now
n: 2
1 ey
es
21 c
hron
ic p
ersi
sten
t50
acu
te r
ecur
rent
1 pr
esum
ed H
SV/V
ZV
21 e
yes
7 ey
es w
ere
posi
tive
only
on
repe
at t
aps
No
clin
ical
dif
fere
nce
betw
een
CM
V-
posi
tive
and
-neg
ativ
e ey
es
[5,13,14]
Hw
ang
et a
l. (2
011)
19
(18
patie
nts)
Non
-HSV
/VZV
infla
mm
ator
y oc
ular
hyp
erte
nsio
n sy
ndro
me
All
Unk
now
n16
acu
te r
ecur
rent
3 un
know
n5
eyes
2
had
pers
iste
nt
corn
eal e
dem
a[6]
van
Boxt
el
et a
l. (2
007
)
7Fi
ne: 3
eye
s M
utto
n fa
t: 1
eye
Trac
e to
1+
cel
lsFo
cal c
orne
al e
dem
a (e
ndot
helii
tis):
2 e
yes
All
Pres
ent:
3 e
yes
Abs
ent:
4 e
yes
6 ch
roni
c pe
rsis
tent
1 ac
ute
recu
rren
t2
eyes
2
eyes
wer
e po
sitiv
e fo
r C
MV
DN
A o
nly
at
seco
nd t
ap
[7]
Miy
anag
a et
al.
(201
0)
7Fi
ne: 2
eye
sM
utto
n fa
t: 5
eye
s1–
2+ c
ells
All
Pres
ent:
2 e
yes
Abs
ent:
5 e
yes
Unk
now
n2
eyes
Ass
ocia
tion
betw
een
vira
l loa
d an
d co
rnea
l en
doth
elia
l cel
ls lo
ss
[8]
de S
chry
ver
et a
l. (2
00
6)
5G
rey–
whi
te o
r br
own
med
ium
-to
-larg
e ke
ratic
pr
ecip
itate
sC
orne
al e
dem
a: 2
eye
sM
ild-t
o-m
oder
ate
infla
mm
atio
n
All
Abs
ent
3 ch
roni
c pe
rsis
tent
2 ac
ute
recu
rren
t2
eyes
[9]
Kaw
aguc
hi
et a
l. (2
007
)
1W
hitis
h sm
all m
utto
n fa
tYe
sA
bsen
tA
cute
rec
urre
ntYe
sC
orre
latio
n be
twee
n la
ser
flare
pho
tom
etry
w
ith v
iral l
oad
[10]
Sira
et
al.
(20
07)
1Si
ngle
whi
te k
erat
ic
prec
ipita
tes
1+ c
ells
Yes
Abs
ent
Acu
te r
ecur
rent
0[11]
Chu
ng
et a
l. (2
00
6)
1M
ediu
m-s
ized
ste
llate
ke
ratic
pre
cipi
tate
sM
ild in
flam
mat
ion
Yes
Unk
now
nA
cute
rec
urre
nt0
[12]
CM
V: C
ytom
egal
oviru
s; H
SV: H
erpe
s si
mpl
ex v
irus;
VZV
: Var
icel
la z
oste
r vi
rus.
Exp
ert R
evie
w o
f O
phth
alm
olog
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y W
ashi
ngto
n St
ate
Uni
vers
ity o
n 10
/25/
14Fo
r pe
rson
al u
se o
nly.

Expert Rev. Ophthalmol. 6(5), (2011)520
Review CMEJap & Chee
Corneal endotheliitisDuring the same period, 51 eyes of 48 patients with CMV endotheliitis (Figure 3) were analyzed, and all were from Asian populations [6,8,16–24]. Unlike eyes with anterior uveitis, the KPs in eyes with corneal endotheliitis tended to be pigmented, and were often arranged in a linear or coin-shaped pattern (Table 2). The linear KPs tended to occur at the leading edge of the stro-mal edema. The coin-shaped KPs are usually medium sized, and arranged in a circular pattern around an area of corneal edema [17]. Owl’s eyes lesions were seen in two eyes: one on confocal micro-scopy [20] and one on histology [21]. These owl’s eye lesions consist of intranuclear inclusion bodies, and are characteristic of CMV infection [25]. The cornea edema may be localized or diffuse, and the AC inflammation is very mild, having cells less than 1+, and may be absent in some eyes. Rarely, KPs may also be absent [24].
Elevated IOP was a less prominent feature than in anterior uvei-tis, with only 37 eyes (73%) having elevated IOP and nine eyes (18%) requiring glaucoma surgery. Iris atrophy was less obvious in these eyes, being noted in only 12 eyes (24%). One patient had a simultaneous onset of localized areas of retinitis [19].
Endotheliitis in eyes with previous anterior uveitis It is interesting that 20 eyes had been treated previously for hypertensive anterior uveitis and were receiving corticosteroids at the time of diagnosis of the endotheliitis [6,16–18,23]. Furthermore, two eyes with anterior uveitis had been noted to have concomi-tant endotheliitis lesions [7]. This suggests that endotheliitis and anterior uveitis are part of the same spectrum of possible clinical presentation of CMV anterior segment infection, and that the particular pattern of manifestation may depend on the host’s immune status and/or viral load. The younger age and tendency to a lower viral load in eyes with acute uveitis [14] suggest that it may represent an inflammatory response to a small or short-lived release of viral load, whereas endotheliitis represents direct tis-sue damage, and the prior use of corticosteroids may have been responsible for transformation in these eyes.
Post-corneal graft endotheliitisOf further interest, 14 eyes were diagnosed following corneal graft surgery [6,17–19,22] and one eye had a history of both previ-ous uveitis and graft [21]. These eyes had initially been thought to display endothelial rejection, until linear or coin-shaped KPs were noted, the endothelial cell count decreased unexpectedly or the edema worsened despite an increase in immunosuppressive therapy [19,22]. The source of the CMV infection in these eyes is uncertain. The indications for the initial graft included kera-toconus [22], posterior polymorphous dystrophy, pseudophakic bullous keratopathy [18,19], herpetic keratouveitis, Fuchs uveitis syndrome [19], Fuchs endothelial dystrophy [17], recurrent corneal endotheliitis [17] and corneal opacities [17]. Other than the eye that received a graft for keratoconus, whether these eyes already had CMV endotheliitis prior to the graft, the CMV was transmitted from the donor or the prolonged immunosuppressive therapy caused a reactivation of latent CMV, cannot be determined. However, these cases demonstrate that the possibility of CMV infection should be excluded prior to performing a graft or when graft rejection occurs, especially in the presence of atypical KPs.
Complications of CMV anterior segment infectionGlaucomaAt least 42 eyes (26%) required glaucoma surgery or had glaucoma-tous optic neuropathy [5–10,16,18,19]. However, these figures may under-represent the prevalence of glaucomatous damage as, although glaucoma surgery was indicated when required, most authors did not define nor systemically describe the presence of any glaucomatous optic neuropathy.
Endothelial cell loss &/or corneal decompensationAnshu et al. [19] and Miyanaga et al. [8] found severe endo thelial cell loss in their patients, ranging from 35 to 77% (15 eyes [9%]), and, particularly for the 48 treatment episodes of eyes with endotheliitis, 12 (25%) had significant persistent corneal edema despite resolution of inflammation [6,16–19,22,23]. In addi-tion, persistent edema was also seen in two eyes with anterior uveitis [6], of which one was severe enough to require a corneal graft. Focal areas of endotheliitis were also seen in two eyes with anterior uveitis [7].
Cataract formationThe prevalence of cataract was also not systemically recorded in most of the studies. However, it was seen in 23 (32%) of the eyes in a large series [5] and, not unexpectedly, it was more prevalent in eyes with chronic uveitis [14].
PathogenesisThe reactivation of CMV in the eye causing ocular disease in immunocompetent patients, especially in Asia, is not unex-pected given its high seroprevalence and the life-long latency of this virus in hematopoietic and endothelial cells [26]. Similar to the other herpetic infections, recurrent disease is well docu-mented, and has been attributed to a temporary breakdown in the ocular immune defense mechanisms, as in times of stress
Figure 1. Slit-lamp photograph of an eye with acute recurrent cytomegalovirus anterior uveitis showing a few fine- to medium-sized keratic precipitates.
Exp
ert R
evie
w o
f O
phth
alm
olog
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y W
ashi
ngto
n St
ate
Uni
vers
ity o
n 10
/25/
14Fo
r pe
rson
al u
se o
nly.

www.expert-reviews.com 521
ReviewCME Cytomegalovirus-associated anterior segment infection
or other illnesses. Furthermore, in eyes with endotheliitis that had a history of prior uveitis or corneal graft, the use of cortico-steroids or other immunosuppressants may have enhanced viral replication, resulting in a more severe manifestation of the dis-ease. However, owing to the existence of the blood–ocular bar-rier, the cellular-mediated response to the infection is limited and, hence, it is difficult to control or suppress CMV, even in immunocompetent patients.
Differential diagnosis Idiopathic hypertensive anterior uveitisAcute recurrent CMV anterior uveitis has many features in com-mon with Posner–Schlossman syndrome, and constituted half of the cases of presumed Posner–Schlossman syndrome in one series [14]. The chronic persistent form also has features that resemble Fuchs uveitis syndrome, and CMV was found in 42% of such eyes by Chee and Jap [14]. One eye also presented with sector iris atrophy and was initially diagnosed as HSV/VZV anterior uveitis [13]. The lack of distinguishing features between the CMV-positive and -negative cases in eyes with acute recur-rent uveitis [14], as well as the 95% positive predictive value of these features in the series from Hwang et al. [6], suggests that, in Asia certainly, CMV infection should be excluded in eyes with hypertensive anterior uveitis.
Endothelial rejection post corneal graftIn eyes with previous grafts, the KPs occurred on both the donor and host corneas [17,19], unlike in endothelial rejection, where the KPs are seen on the donor.
Idiopathic endotheliitisIn the series from Kandori et al., none of the eyes with epithelial or stromal keratitis were positive for CMV, but seven out of 29 cases (24%) of endotheliitis were CMV-positive [18], and CMV was found in at least 90% of cases of endotheliitis in two studies [6,16]. Hence, CMV needs to be excluded in eyes with an apparently idiopathic cause of endotheliitis.
Diagnostic tests Although there are certain clinical features that may be useful in increasing the positive-predictive values of aqueous sampling, such as the presence of coin-shaped KPs in eyes with endotheliitis, anterior uveitis with ocular hypertension, diffuse iris atrophy and absence of epithelial or stromal keratitis [6,18], there are no clinical features with sufficient sensitivity nor specificity for the diagno-sis of CMV infection to be made on purely clinical grounds [14]. Hence, the diagnosis can only be confirmed on aqueous sampling for evidence of intraocular CMV. However, aqueous ana lysis is an invasive procedure and, therefore, is not practiced for this reason, even in some developed countries. In cases of anterior uveitis, we routinely tap all eyes after having excluded other common causes, such as syphilis, TB, sarcoidosis or HLA-B27-associated anterior uveitis, or unless they have an obvious cause for the inflamma-tion, for example, those with corneal or skin lesions or iris changes typical of HSV/VZV uveitis. Specifically, we would tap those that
present as an acute mild uveitis with ocular hypertension or as a chronic, persistent uveitis with the features described previously. These criteria are applied regardless of the descent of the patient.
The presence of intraocular CMV may be established by qualitative or quantitative PCR methods [27,28], or by compar-ing the intraocular CMV-specific antibody levels to serum levels (Goldmann–Witmer coefficient). By combining these two tech-niques the yield may be improved, since, in some of the eyes, the PCR was positive only at repeat taps. This could possibly be owing to a small viral load in a small volume of aqueous avail-able for ana lysis or a short-lived release of the virus, which may be missed on PCR alone, whereas antibody production remains throughout the course of the disease [29]. On the other hand, in immunocompromised patients, PCR may be a more sensitive test [30–32]. Hence, ideally, both of these tests should be done if they are available, as they complement each other.
Figure 2. A 73-year-old male with chronic persistent cytomegalovirus anterior uveitis of the right eye presents with mild redness and a raised intraocular pressure. (A) Slit-lamp photograph of an eye with chronic persistent cytomegalovirus anterior uveitis showing nodular endothelial lesions (arrows) and diffuse iris atrophy. (B) Confocal microscopy of the same eye showing the nodular endothelial lesion (arrow).
Exp
ert R
evie
w o
f O
phth
alm
olog
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y W
ashi
ngto
n St
ate
Uni
vers
ity o
n 10
/25/
14Fo
r pe
rson
al u
se o
nly.

Expert Rev. Ophthalmol. 6(5), (2011)522
Review CMEJap & Chee
ManagementThe optimal therapy of CMV anterior segment infection has yet to be established. Current therapy protocols have been based on the results of treatment of CMV retinitis in patients with AIDS. In patients with AIDS, ganciclovir or, more recently, valganci-clovir therapy, is efficacious and can often be discontinued as immune recovery occurs in patients on retroviral therapy.
Ganciclovir is a synthetic purine nucleoside analogue with good anti-CMV activity and relatively fewer adverse effects. It has been used for the treatment of CMV retinitis since the late 1980s in intravenous, oral or intravitreal formulations, with the route being determined by the location, severity of the retinitis, immune status of the patient, costs and occurrence of side effects. Valganciclovir is a prodrug of ganciclovir, which is rapidly converted to ganciclovir following oral administration, and is able to achieve similar plasma levels with a once-daily dosing as ganciclovir.
In accordance with the management of CMV retinitis in AIDS patients, systemic ganciclovir or valganciclovir has been the first line of treatment of CMV anterior segment infection in most centers, with intravitreal ganciclovir as a second-line therapy. The ganciclovir implant (Vitrasert®, Bausch and Lomb Inc., CA, USA), which releases 4.5 mg of ganciclvoir over 5–8 months, is an alternative modality for patients who have recurrent inflam-mation following previous response to systemic therapy but had issues with side effects. Topical ganciclovir was originally devel-oped for the treatment of herpetic keratitis, but it has been found to achieve high concentrations in the cornea, iris tissue and aque-ous, especially with the 0.2% gel [33]. It is commercially available as an ophthalmic gel under the trade names of Virgan® and Zirgan® from Laboratories Thea (Clermont-Ferrand, France).
However, various concentrations of ganciclovir eye drops have also been used in the literature for the treatment of CMV anterior uveitis [18,20,21].
The results of treatment are difficult to evaluate as they are derived from nonrandomized case series or single case reports, and there is considerable variation in the route, dose and duration of treatment. Furthermore, the outcome measures are not well defined, with most authors reporting a clinical improvement, and the duration of follow-up post-treatment has been relatively short in most studies. However, what has been a consistent out-come in these studies is the fact that, in these immunocompetent patients, although the response to antiviral therapy is high, the relapse rate has also been high, and a prolonged period of treat-ment may be required (Tables 3 & 4). In particular, the relapse rate with intravitreal ganciclovir has been 100%. On the other hand, it may be a useful adjunct to systemic therapy, although the number of cases in this series is small and the follow-up period is relatively short [6].
Ganciclovir gel has a relatively low response rate, but it also has a lower relapse rate and, more importantly, owing to its low cost and minimal adverse effects, it may be considered for use as maintenance therapy for prolonged periods. The potential role of valaciclovir is uncertain as it was noted to be effective in only a single case report [11].
Another result that has been consistent is the potential need for adjunctive measures, whereby, although the inflammation and/or viral load is controlled with antiviral therapy, the compli-cations, such as IOP elevation, glaucomatous optic neuropathy and corneal decompensation, may still ensue and require surgical management, as evidenced by the 34 eyes (21%) who had either glaucomatous optic neuropathy or required glaucoma surgery, and the 14 eyes (12 with endotheliitis [24%]) that had persistence of significant corneal edema.
Moreover, not all CMV-positive eyes require antiviral treat-ment. Among the eyes with anterior uveitis, approximately half who had milder disease refused treatment without any appar-ent disadvantage [5]. Similarly, two eyes with small areas of endotheliitis also refused antiviral therapy without any adverse outcome [16].
Expert commentaryInfection by CMV of the anterior segment in the immuno-competent is a spectrum of diseases that varies from an acute relapsing somewhat self-limiting disease to an endotheliitis. Two of the features commonly seen in all these cases were elevated IOP and iris atrophy. CMV has been found in the smooth mus- CMV has been found in the smooth mus-CMV has been found in the smooth mus-cle cells of the iris and ciliary body [34]. The exact mechanisms whereby it causes the IOP rise remain unknown, but it may cause a trabeculitis, as is the case with HSV [35]. There may be an overlap in the signs; for example, some of the eyes with anterior uveitis may also have patches of endotheliitis. These differences in manifestations of the same disease in different eyes, as well as in the same eye over time, is probably a result of an interac-tion between the viral load and the immune status of the eye, as discussed previously.
Figure 3. Slit-lamp photograph of an eye with cytomegalovirus endotheliitis showing edema of the superior two-thirds of the cornea and a few small keratic precipitates.
Exp
ert R
evie
w o
f O
phth
alm
olog
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y W
ashi
ngto
n St
ate
Uni
vers
ity o
n 10
/25/
14Fo
r pe
rson
al u
se o
nly.

www.expert-reviews.com 523
ReviewCME Cytomegalovirus-associated anterior segment infection
The current practice of therapy is to use systemic ganciclovir as a first-line treatment. However, the results of the various studies suggest that a longer duration of treatment may be required, as the recurrence rate is high. This is not only costly, but also may not be tolerated owing to adverse reactions, such as neutropenia. Other modes of therapy, such as administering a loading dose of an intravitreal injection of ganciclovir together with valganciclo-vir, have been tried, with apparently good outcomes. However,
the numbers treated in this manner is small, and the duration of follow-up is relatively short [6,12].
PCR and/or CMV-specific antibody tests are not widely availa-ble at present, and aqueous sampling is also an invasive procedure, which not all patients are willing to undergo. On the other hand, since the prevalence of CMV infection is rather high in Asia, it may be prudent to limit the use of corticosteroids in eyes with idiopathic hypertensive anterior uveitis, in cases where there is no
Table 2. Literature review of clinical features of cytomegalovirus endotheliitis in non-HIV-positive patients.
Study (year)
Eyes (n) Keratic precipitates/anterior chamber inflammation
Intraocular pressure >21 mmHg
Iris atrophy
Comments Ref.
Chee et al. (2007)
12 (10 patients)
Filiform, fine-to-medium in sizePigmented with linear and/or circular pattern+0.5–2+ cells
All 8 eyes 4 eyes required glaucoma surgery11 eyes had had previous hypertensive anterior uveitisAll had been receiving steroids at the time of diagnosis of endotheliitis
[16]
Hwang et al. (2011)
10 Coin-shaped keratic precipitates Mild inflammation
5 eyes 2 eyes 2 presented as Posner–Schlossman syndrome1 noted post corneal graft1 had glaucoma surgery
[6]
Koizumi et al. (2008)
8 Linear and coin-shaped keratic precipitates at leading edgeLocalized stromal edemaMinimal inflammation
6 eyes Unknown 3 had previous uveitis4 had previous corneal grafts
[17]
Kandori et al. (2010)
8 (7 patients) Localized or diffuse edemaLinear or coin-shaped keratic precipitates at leading edgeZero-to-mild inflammation
2 eyes Unknown 4 had previous corneal graft3 had previous uveitis1 had glaucoma surgery
[18]
Miyanaga et al. (2010)
4 Diffuse stromal edema: 3 eyesLocalized edema: 1 eyeFine and mutton fat: 1 to 2+ cells
All 2 eyes Association between viral load and corneal endothelial cells lossNo glaucoma
[8]
Anshu et al. (2009)
4 Pigmented keratic precipitatesLinear pattern0–1+ cells
All Unknown All were post-corneal graft3 had glaucoma surgery1 patient also had retinitis
[19]
Shiraishi et al. (2007)
1 Coin-shaped lesionsMultiple keratic precipitatesLocalized edema
Yes Unknown Confocal microscopy showed owl’s eye endothelial cells
[20]
Shimazaki et al. (2010)
1 Diffuse edemaPigmented keratic precipitatesCoin-shaped keratic precipitates0 cells
Yes Unknown Post corneal graft and previous uveitisHistology: owl’s eye endothelial cells
[21]
Sonoyama et al. (2010)
1 Diffuse edemaCoin-shaped keratic precipitates at leading edgeMild inflammation
Yes Unknown Previous corneal graft [22]
Yamauchi et al. (2007)
1 Diffuse edemaFine pigmented keratic precipitates
Yes 0 Previous recurrent uveitis [23]
Chiang et al. (2011)
1 Temporal 2/3 edemaNo keratic precipitates or cells
No Unknown [24]
Exp
ert R
evie
w o
f O
phth
alm
olog
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y W
ashi
ngto
n St
ate
Uni
vers
ity o
n 10
/25/
14Fo
r pe
rson
al u
se o
nly.

Expert Rev. Ophthalmol. 6(5), (2011)524
Review CMEJap & CheeTa
ble
3. L
iter
atu
re r
evie
w o
f o
utc
om
es o
f tr
eatm
ent
of
cyto
meg
alo
viru
s an
teri
or
uve
itis
in n
on
-HIV
-po
siti
ve p
atie
nts
.
Stu
dy
(yea
r)Tr
eatm
ent
epis
od
es (
n)
Trea
tmen
t m
od
alit
y an
d d
ura
tio
n (
mo
nth
s)O
utc
om
eD
ura
tio
n o
f fo
llow
-up
(m
on
ths)
Ref
.
Syst
emic
th
erap
y
Che
e an
d Ja
p (2
010
)19
Intr
aven
ous
ganc
iclo
vir
10 m
g/k
g/d
ay f
or 6
wee
ks f
ollo
wed
by
oral
ga
ncic
lovi
r 3
g/d
ay f
or a
noth
er 6
wee
ks o
r V
alga
ncic
lovi
r 18
00
mg
/day
for
6 w
eeks
fol
low
ed b
y 9
00
mg
/day
fo
r an
othe
r 6
wee
ks
17 r
espo
nded
, but
14
had
recu
rren
ces
2 ha
d no
res
pons
e
4.9
–54.
8 po
st-t
reat
men
t[5]
Miy
anag
a et
al.
(201
0)
7V
alga
ncic
lovi
r 18
00
mg
/day
for
mor
e th
an 3
wee
ksA
ll re
spon
ded
Unk
now
n[8]
de S
chry
ver
et a
l. (2
00
6)
5In
trav
enou
s ga
ncic
lovi
r or
fos
carn
et f
or 2
wee
ks f
ollo
wed
by
valg
anci
clov
ir 9
00
mg
/day
for
8 w
eeks
: 4 t
reat
men
t ep
isod
esV
alga
ncic
lovi
r 9
00
mg
/day
for
10
wee
ks: 1
tre
atm
ent
epis
ode
All
resp
onde
d, b
ut 3
had
rec
urre
nces
Re
trea
ted
with
val
ganc
iclo
vir
for
6 m
onth
s, r
espo
nded
with
no
recu
rren
ce
9–2
4[9]
van
Boxt
el e
t al
. (2
00
6)
5O
ral v
alga
ncic
lovi
r 18
00
mg
/day
for
3 w
eeks
fol
low
ed b
y 9
00
mg
/day
for
3–1
2 m
onth
sA
ll re
spon
ded,
1 h
ad a
rec
urre
nt
epis
ode
18–2
46[7]
Hw
ang
et a
l. (2
011)
3V
alga
ncic
lovi
r 18
00
mg
/day
for
3–1
3 m
onth
s A
ll re
spon
ded,
but
1 h
ad r
ecur
renc
es
and
1 ha
d pe
rsis
tent
cor
neal
ede
ma
1–36
[6]
Sira
and
Mur
ray
(20
07)
111
mon
ths
oral
val
acic
lovi
r 2
g/d
ay
Resp
onde
d w
ith n
o re
curr
ence
11[11]
Intr
avit
real
gan
cicl
ovi
r
Hw
ang
et a
l. (2
011)
91
dose
intr
avitr
eal g
anci
clov
ir 2
mg
All
resp
onde
d 1–
36[6]
Che
e et
al.
(201
0)
7In
trav
itrea
l gan
cicl
ovir
2 m
g pe
r w
eek
for
12 w
eeks
3
had
no r
espo
nse
4 re
spon
ded,
but
all
had
recu
rren
ces
4.9
–54.
8 po
st-t
reat
men
t[5]
Chu
ng e
t al
. (20
06
)1
1 do
se in
trav
itrea
l gan
cicl
ovir
2 m
gRe
spon
ded
with
no
recu
rren
ceU
nkno
wn
[12]
Oth
er t
reat
men
t re
gim
ens
Hw
ang
et a
l. (2
011)
71
dose
of
intr
avitr
eal g
anci
clov
ir 2
mg
with
va
lgan
cicl
ovir
180
0 m
g/d
ay f
or 0
.5–6
mon
ths
All
resp
onde
d, b
ut 1
had
per
sist
ent
corn
eal e
dem
a1–
36[6]
Che
e an
d Ja
p (2
010
)17
Gan
cicl
ovir
gel 0
.15%
fou
r-tim
es d
aily
for
at
leas
t 3
mon
ths
6 ha
d no
res
pons
e11
res
pond
ed, b
ut 5
rec
urre
d4.
9–5
4.8
post
-tre
atm
ent
[5]
Che
e an
d Ja
p (2
010
)4
Gan
cicl
ovir
impl
ant
All
resp
onde
d, b
ut a
ll ha
d re
curr
ence
s4.
9–5
4.8
post
-tre
atm
ent
[5]
Exp
ert R
evie
w o
f O
phth
alm
olog
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y W
ashi
ngto
n St
ate
Uni
vers
ity o
n 10
/25/
14Fo
r pe
rson
al u
se o
nly.

www.expert-reviews.com 525
ReviewCME Cytomegalovirus-associated anterior segment infection
access to such tests. Endothelial rejection following corneal graft should be carefully examined for a possible CMV etiology, as early treatment can result in restoration of graft clarity. Glaucoma is another important complication of CMV anterior segment infec-tion, with at least 26% of the eyes either requiring surgery or having glaucomatous damage. Hence, glaucoma therapy is an essential component in the management of these eyes.
Five-year viewAlthough the diagnosis of CMV infection will still require aque-ous sampling, we look toward more readily available, cheaper and more sensitive confirmatory tests. Subsequently, less inva-sive tests may then be used to monitor the effects of treatment, for example, flare values [10] endothelial cell loss [8] or confocal microscopy to look for owl’s eye changes in the cornea.
Table 4. Literature review of outcomes of treatment of cytomegalovirus endotheliitis in non-HIV-positive patients.
Study (year) Treatment episodes (n)
Treatment modality and duration (months)
Outcome Duration of follow-up (months)
Ref.
Systemic therapy
Chee et al. (2007) 10 Intravenous ganciclovir 10 mg/kg for 6 weeks followed by oral ganciclovir 3 g/day for another 6 weeks, or valganciclovir 1800 mg/day for 6 weeks followed by 900 mg/day for another 6 weeks
All responded, but 3 eyes had persistent corneal edema
4.9–54.8 post-treatment
[16]
Koizumi et al. (2008)
8 Ganciclovir 10 mg/kg/day for 10 days Responded, but 2 had persistent corneal edema
20–24 [17]
Kandori et al. (2010) 7 Intravenous ganciclovir 5 or 10 mg/kg/day for 5–21 days with topical ganciclovir 0.15, 0.3 or 0.5%
All responded, but 2 had persistent edema
7–14 [18]
Miyanaga et al. (2010)
4 Valganciclovir 1800 mg/day for more than 3 weeks
All responded Unknown [8]
Anshu et al. (2009) 4 Valganciclovir 1800 mg/day for 6 weeks followed by 900 mg/day for another 6 weeks
All responded, but 2 had recurrences1 had persistent corneal edema
4–9 [19]
Hwang et al. (2011) 1 Valganciclovir 1800 mg day for 3–13 months Responded, but needed corneal graft for persistent corneal edema
1–36 [6]
Sonoyama et al. (2010)
1 Intravenous ganciclovir 10 mg/kg/day for 10 days
Responded, but had persistent edema
21 [22]
Chiang et al. (2011) 1 Valganciclovir 1800 mg/day for 4 months Responded Unknown [24]
Yamauchi et al. (2007)
1 Valganciclovir 1800 mg/day for 4 months Responded, but had persistent corneal edema
16 months post-treatment
[23]
Other treatment regimens
Hwang et al. (2011) 6 1 dose of intravitreal ganciclovir 2 mg with valganciclovir 1800 mg/day for 0.5–5 months
Responded, but 1 eye needed corneal graft for persistent corneal edema
2–17 [6]
Hwang et al. (2011) 2 1 dose intravitreal ganciclovir 2 mg Responded [6]
Shiraishi et al. (2007)
1 Topical ganciclovir 0.5% eight-times daily and intravenous ganciclovir 500 mg/day for 2 weeks followed by topical ganciclovir 0.5% four-times daily for 3 months
Responded 3 [20]
Shimazaki et al. (2010)
1 Ganciclovir 10 mg/kg/day for 7 days followed by topical ganciclovir 0.5% six-times daily, then three-times daily for 20 months
Responded 20 [21]
Kandori et al. (2010) 1 Topical ganciclovir 0.5% Responded 7–14 [18]
Exp
ert R
evie
w o
f O
phth
alm
olog
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y W
ashi
ngto
n St
ate
Uni
vers
ity o
n 10
/25/
14Fo
r pe
rson
al u
se o
nly.

Expert Rev. Ophthalmol. 6(5), (2011)526
Review CMEJap & Chee
Another important area of development is to have improved sustained local drug-delivery systems that can deliver consistent levels of medication over a longer term without being invasive and costly. One such potential technique is to use nanoparticles to deliver the drug.
More research into understanding the role of AC-associated immune deviation in the pathogenesis of CMV in the anterior segment of the eye will be useful in order to provide us with other means of preventing or treating this disease, such as by modifying the immune response.
Key issues
• Cytomegalovirus (CMV) infection in the immunocompetent patient manifests predominantly in the anterior segment and, generally, the posterior segment is uninvolved.
• It may present as an acute recurrent hypertensive anterior uveitis, a chronic anterior uveitis with or without ocular hypertension, an endotheliitis or a combination of the uveitis with endotheliitis.
• CMV endotheliitis may develop following penetrating keratoplasty or Descemet’s membrane automated endothelial keratoplasty, and may be mistakenly diagnosed as an endothelial rejection episode.
• Both the acute and chronic CMV anterior uveitis eyes may develop patchy or diffuse iris atrophy, but do not develop posterior synechiae.
• In most cases, diagnosis was made by PCR ana lysis of aqueous for CMV DNA and by CMV-specific antibody ana lysis in a few centers.
• CMV anterior segment infection responds to specific antiviral therapy, but is associated with a tendency to relapse in 75% of cases.
• Eyes with CMV anterior uveitis may lose vision as a result of glaucomatous optic neuropathy.
• Eyes with CMV endotheliitis may develop visual loss from endothelial failure, despite control of infection with antiviral therapy.
• Topical and systemic immunosuppressive therapy in the absence of specific antiviral therapy should be avoided, as the disease may progress.
ReferencesPapers of special note have been highlighted as:• of interest•• of considerable interest
1 Wong A, Tan KH, Tee CS, Yeo GS. Seroprevlance of cytomegalovirus, toxoplasma and parvovirus in pregnancy. Singapore Med. J. 41(4), 151–155 (2000).
2 Taechowisan T, Sutthent R, Louisirirotchanakul S, Puthavathana P, Wasi C. Immune status in congenital infections by TORCH agents in pregnant Thais. Asian Pac. J. Allergy Immunol. 15(2), 93–97 (1997).
3 Tookey PA, Ades AE, Peckham CS. Cytomegalovirus prevalence in pregnant women: the influence of parity. Arch. Dis. Child. 67(7), 779–783 (1992).
4 Gratacap-Cavallier B, Bosson JL, Morand P et al. Cytomegalovirus seroprevalence in French pregnant women: parity and place of birth as major predictive factors. Eur. J. Epidemiol. 14(2), 147–152 (1998).
5 Chee SP, Jap A. Cytomegalovirus anterior uveitis: outcome of treatment. Br. J. Ophthalmol. 94(12), 1648–1652 (2010).
•• Largeseriesanalyzingtheoutcomeoftreatmentwithvariousmodalitiesofganciclovir.
6 Hwang YS, Shen CR, Chang SH et al. The validity of clinical feature profiles for cytomegaloviral anterior segment infection. Graefes Arch. Clin. Exp. Ophthalmol. 249(1), 103–110 (2011).
7 van Boxtel LA, van der Lelij A, van der Meer J, Los LI. Cytomegalovirus as a cause of anterior uveitis in immunocompetent patients. Ophthalmology 114(7), 1358–1362 (2007).
• Oneoftheearliestpaperstodescribecytomegalovirus(CMV)anteriorsegmentinfection.
8 Miyanaga M, Sugita S, Shimizu N et al. A significant association of viral loads with corneal endothelial cell damage in cytomegalovirus anterior uveitis. Br. J. Ophthalmol. 94(3), 336–340 (2010).
9 de Schryver I, Rozenberg F, Cassoux N et al. Diagnosis and treatment of cytomegalovirus iridocyclitis without retinal necrosis. Br. J. Ophthalmol. 90(7), 852–855 (2006).
10 Kawaguchi T, Sugita S, Shimizu N, Mochizuki M. Kinetics of aqueous flare, intraocular pressure and virus-DNA copies in a patient with cytomegalovirus iridocyclitis without retinitis. Int. Ophthalmol. 27(6), 383–386 (2007).
11 Sira M, Murray PI. Treatment of cytomegalovirus anterior uveitis with oral valaciclovir. Ocul. Immunol. Inflamm. 15(1), 31–32 (2007).
12 Chung RS, Chua CN. Intravitreal ganciclovir injections in aqueous cytomegalovirus DNA positive hypertensive iritis. Eye 20(9), 1080 (2006).
13 Chee SP, Bacsal K, Jap A, Se-Thoe SY, Cheng CL, Tan BH. Clinical features of cytomegalovirus anterior uveitis in immunocompetent patients. Am. J. Ophthalmol. 145(5), 834–840 (2008).
14 Chee SP, Jap A. Presumed Fuchs heterochromic iridocyclitis and Posner–Schlossman syndrome: comparison of cytomegalovirus-positive and negative eyes. Am. J. Ophthalmol. 146(6), 883–889 (2008).
• ThereisahighprevalenceofCMVinfectionineyeswithhypertensiveuveitis,andtherearenoclinicalfeaturesthatareeithersensitiveorspecificenoughtomakepossibleadiagnosisofCMVinfection.
15 Cheung CM, Chee SP. Anti-retinal autoantibodies-positive autoimmune retinopathy in cytomegalovirus-positive anterior uveitis. Br. J. Ophthalmol. 94(3), 380–381 (2010).
16 Chee SP, Bacsal K, Jap A, Se-Thoe SY, Cheng CL, Tan BH. Corneal endotheliitis associated with evidence of cytomegalovirus infection. Ophthalmology 114(4), 798–803 (2007).
• ImmunosuppressivetherapymaycauseachangeinpatternofmanifestationofCMVinfectionfromananterioruveitistoanendotheliitis.
17 Koizumi N, Suzuki T, Uno T et al. Cytomegalovirus as an etiologic factor in corneal endotheliitis. Ophthalmology 115(2), 292–297 (2008).
Exp
ert R
evie
w o
f O
phth
alm
olog
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y W
ashi
ngto
n St
ate
Uni
vers
ity o
n 10
/25/
14Fo
r pe
rson
al u
se o
nly.

www.expert-reviews.com 527
ReviewCME Cytomegalovirus-associated anterior segment infection
• OneoftheearliestpapersonCMVendotheliitis.Describesthecharacteristiccoin-shapedpatternofkeraticprecipitates.
18 Kandori M, Inoue T, Takamatsu F et al. Prevalence and features of keratitis with quantitative polymerase chain reaction positive for cytomegalovirus. Ophthalmology 117(2), 216–222 (2010).
19 Anshu A, Chee SP, Mehta JS, Tan DT. Cytomegalovirus endotheliitis in Descemet’s stripping endothelial keratoplasty. Ophthalmology 116(4), 624–630 (2009).
• CMVendotheliitismaypresentasanapparentcornealgraftrejection.
20 Shiraishi A, Hara Y, Takahashi M et al. Demonstration of ‘owl’s eye’ morphology by confocal microscopy in a patient with presumed cytomegalovirus corneal endotheliitis. Am. J. Ophthalmol. 143(4), 715–717 (2007).
21 Shimazaki J, Harashima A, Tanaka Y. Corneal endotheliitis with cytomegalovirus infection of corneal stroma. Eye 24(6), 1105–1107 (2010).
22 Sonoyama H, Araki-Sasaki K, Osakabe Y et al. Detection of cytomegalovirus DNA from cytomegalovirus corneal endotheliitis after penetrating keratoplasty. Cornea 29(6), 683–685 (2010).
23 Yamauchi Y, Suzuki J, Sakai J, Sakamoto S, Iwasaki T, Usui M. A case of hypertensive keratouveitis with
endotheliitis associated with cytomegalovirus. Ocul. Immunol. Inflamm. 15(5), 399–401 (2007).
24 Chiang CC, Lin TH, Tien PT, Tsai YY. Atypical presentation of cytomegalovirus endotheliitis: a case report. Ocul. Immunol. Inflamm. 19(1), 69–71 (2011).
25 Herriot R, Gray ES. Images in clinical medicine. Owl’s-eye cells. N. Engl. J. Med. 331(10), 649 (1994).
26 Koffron AJ, Hummel M, Patterson BK et al. Cellular localization of latent murine cytomegalovirus. J. Virol. 72(1), 95–103 (1998).
27 Sugita S, Shimizu N, Watanabe K et al. Use of multiplex PCR and real-time PCR to detect human herpes virus genome in ocular fluids of patients with uveitis. Br. J. Ophthalmol. 92(7), 928–932 (2008).
28 Brantsaeter AB, Holberg-Petersen M, Jeansson S, Goplen AK, Bruun JN. CMV quantitative PCR in the diagnosis of CMV disease in patients with HIV-infection – a retrospective autopsy based study. BMC Infect. Dis. 6(7), 127 (2007).
29 De Groot-Mijnes JD, Rothova A, Van Loon AM et al. Polymerase chain reaction and Goldmann–Witmer coefficient analysis are complimentary for the diagnosis of infectious uveitis. Am. J. Ophthalmol. 141(2), 313–318 (2006).
30 Doornenbal P, Seerp Baarsma G, Quint WG, Kijlstra A, Rothbarth PH, Niesters HG. Diagnostic assays in cytomegalovirus retinitis: detection of herpesvirus by simultaneous application of the polymerase chain reaction and local antibody analysis on ocular fluid. Br. J. Ophthalmol. 80(3), 235–240 (1996).
31 de Boer JH, Verhagen C, Bruinenberg M et al. Serologic and polymerase chain reaction analysis of intraocular fluids in the diagnosis of infectious uveitis. Am. J. Ophthalmol. 121(6), 650–658 (1996).
32 Fardeau C, Romand S, Rao NA et al. Diagnosis of toxoplasmic retinochoroiditis with atypical clinical features. Am. J. Ophthalmol. 134(2), 196–203 (2002).
33 Castela N, Vermerie N, Chast F et al. Ganciclovir ophthalmic gel in herpes simplex virus rabbit keratitis: intraocular penetration and efficacy. J. Ocul. Pharmacol. 10(2), 439–451 (1994).
34 Daicker B. Cytomegalovirus panuveitis with infection of corneo-trabecular endothelium in AIDS. Ophthalmologica 197(4), 169–175 (1988).
35 Amano S, Oshika T, Kaji Y, Numaga J, Matsubara M, Araie M. Herpes simplex virus in the trabeculum of an eye with corneal endotheliitis. Am. J. Ophthalmol. 127(6), 721–722 (1999).
Exp
ert R
evie
w o
f O
phth
alm
olog
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y W
ashi
ngto
n St
ate
Uni
vers
ity o
n 10
/25/
14Fo
r pe
rson
al u
se o
nly.

Expert Rev. Ophthalmol. 6(5), (2011)528
Review CMEJap & Chee
Cytomegalovirus-associated anterior segment infectionx
To obtain credit, you should first read the journal article. After reading the article, you should be able to answer the following, related, multiple-choice questions. To complete the questions (with a minimum 70% passing score) and earn continuing medi-cal education (CME) credit, please go to www.medscape.org/journals/expertophth. Credit cannot be obtained for tests com-pleted on paper, although you may use the worksheet below to keep a record of your answers. You must be a registered user on Medscape.org. If you are not registered on Medscape.org, please click on the New Users: Free Registration link on the left hand side of the website to register. Only one answer is correct for each question. Once you successfully answer all post-test questions you will be able to view and/or print your certificate. For ques-tions regarding the content of this activity, contact the accredited provider, [email protected]. For technical assistance, contact [email protected]. American Medical Association’s Physician’s Recognition Award (AMA PRA) credits are accepted in the US as evidence of participation in CME activities. For further information on this award, please refer to http://www.ama-assn.org/ama/pub/category/2922.html. The AMA has determined
that physicians not licensed in the US who participate in this CME activity are eligible for AMA PRA Category 1 Credits™. Through agreements that the AMA has made with agencies in some countries, AMA PRA credit may be acceptable as evidence of participation in CME activities. If you are not licensed in the US, please complete the questions online, print the AMA PRA CME credit certificate and present it to your national medical association for review.
Activity EvaluationWhere 1 is strongly disagree and 5 is strongly agree
1 2 3 4 5
1. The activity supported the learning objectives.
2. The material was organized clearly for learning to occur.
3. The content learned from this activity will impact my practice.
4. The activity was presented objectively and free of commercial bias.
2. Based on the review by Drs Jap and Chee, which of the following statements about diagnosis of CMV-associated anterior segment infection in the patient described in question 1 is most likely correct?
£ A Diagnosis can be made exclusively on clinical grounds
£ B Diagnosis requires CMV-specific antibody analysis
£ C Aqueous analysis is noninvasive
£ D Ideally, diagnosis is made both by polymerase chain reaction methods and by comparing the intraocular CMV-specific antibody levels to serum levels
1. Your patient is a 45-year-old, immunocompetent Asian man thought to have cytomegalovirus (CMV)-associated ocular infection. Based on the review by Drs Jap and Chee, which of the following features would be most likely consistent with that diagnosis?
£ A Exclusive involvement of the posterior segment
£ B Acute recurrent hypertensive anterior uveitis
£ C Posterior synechiae
£ D Associated encephalitis and pneumonia
3. Based on the review by Drs Jap and Chee, which of the following statements about treatment of CMV-associated anterior segment infection is most likely correct?
£ A Response to specific antiviral therapy is poor
£ B Relapse rate after specific antiviral therapy is low
£ C Glaucoma therapy is an important adjunctive modality of management
£ D Topical and systemic immunosuppressive therapy should be given without specific antiviral therapy
Exp
ert R
evie
w o
f O
phth
alm
olog
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y W
ashi
ngto
n St
ate
Uni
vers
ity o
n 10
/25/
14Fo
r pe
rson
al u
se o
nly.







![Cytomegalovirus Infection Causes an Increase of Arterial ... · found an association between HCMV infection and vascular atherosclerosis [13–17]. It remains an important investigational](https://img.pdfslide.net/doc/110x75/5d4fe36688c993ce438bdbac/cytomegalovirus-infection-causes-an-increase-of-arterial-found-an-association.jpg)