Embed Size (px)
Citation preview
Vol. 14: e31-e41, June-September 2009
e31
REWIEWARTICLE
Key words:Anorexia nervosa, bulimianervosa, eating disorders,day treatment, day hospital,partial hospitalisation.Correspondence to:Prof. Secondo Fassino,Neurosciences Department,Psychiatry Section,Via Cherasco 11,10126 Torino.E-mail:[email protected]: March 12, 2008Accepted: December 5, 2008
Day hospital programmes for eatingdisorders: A review of the similarities,differences and goals
INTRODUCTION
In the last years eating disorders (EDs)have received greater attention because oftheir diffusion (1) and social and healthcosts (2, 3).
Currently, treatment of EDs is performedin outpatient, inpatient and day hospital(DH) settings without a shared knowledgeabout the best and most effective treatmentfor each patient (4). Further studies arerequired to clear this issue, specially asregards DH treatments.
DH treatment usually involves medicallystable patients who require intensive treat-ment with frequent contact and involve-ment in groups, as recommended by theAmerican Psychiatric Association guide-lines (5) and the National Institute forHealth and Clinical Excellence (NICE) (6).
The DH has unique characteristics: inten-sive daily care is provided but, unlike inpa-tient units, patients return home and main-
tain their social relations, allowing a dailytest of the improvements made and a pro-gressive work on environmental risk factors.
Although DH treatments are widespread,their description in the literature is lacking,except for the pioneering descriptions of theToronto (7) and Munich programmes (8).
Recently, Zipfel et al. (9) and Lammers etal. (10) reviewed the international DH treat-ment programmes for EDs, underscoringtheir advantages and disadvantages.Nonetheless, these reviews have several lim-itations: Zipfel et al. (9) describe only threecentres and Lammers et al. (10) underscorewith more detail the similarities than the dif-ferences of the different models of care.
The first aim of this review is to comparethe different types of DH programme fullydescribed in the literature and to discusstheir similarities and differences. The sec-ond aim of the article is to describe our DHexperience in Turin, Italy, and to compareits features with the other centres found.
G. Abbate-Daga, C. Gramaglia, S. Preda, E. Comba, A. Brustolin, and S. Fassino
Eating Disorders Centre, Neurosciences Department, University of Turin, Turin
ABSTRACT. Day hospital (DH) treatments for eating disorders (EDs) provide intensive dailycare and allow patients to maintain and test their social relations and coping skills at homeand outside. Although widespread, their description is lacking. This review compares the dif-ferent types of DH described in the literature and presents our DH experience in Turin, Italy.We searched Psychinfo and Pubmed with the following keywords: anorexia nervosa, bulimianervosa, EDs, DH, day treatment and partial hospitalisation. We found and reviewed the DHprogrammes of eleven specialised centres, which have some shared features but also manydifferences, suggesting that DH treatments are still largely experimental. Briefly, the sharedelements are: biopsychosocial model as reference frame; cognitive-behavioural model ortechniques; behavioural contract; patients’ selection; body image therapy; involvement offamily; weight normalisation/weight gain and modification/normalisation of eating behaviouras objectives. Nonetheless, shared opinions concerning inclusion criteria are lacking; theduration of DH treatment is surprisingly different among centres (from 3 to 39 weeks); theapproach to eating and compensation behaviours ranges from control to autonomy; follow-up and psychometric assessment can be either performed or not; psychological and behav-ioural objectives can be different. This review suggests the existence of two different DHmodels: the first has a shorter duration and is mainly symptom-focused; the second is moreindividual-focused, has a longer duration and is focused on patients’ relational skills, psycho-dynamic understanding of symptoms and more gradual changes in body weight. Furtherinvestigation is required to make DH treatment programmes measurable and comparable.(Eating Weight Disord. 14: e31-e41, 2009). ©2009, Editrice Kurtis

G. Abbate-Daga, C. Gramaglia, S. Preda, et al.
MATERIALS AND METHODS
We searched the literature using Psychinfo(1980-2007) and Pubmed (Medline 1980-2007),with the following keywords: anorexia nervosa(AN), bulimia nervosa (BN), EDs, DH, day treat-ment and partial hospitalisation. We limitedour search to articles in English and to adultpatients. The reference list of the suitable arti-cles was checked to identify additional interest-ing studies.
Overall, we found 20 articles (two of thesewere reviews) and 13 centres fully describingtheir treatment programmes for EDs. Three ofthem were excluded: the Bern Day Treatmentbecause the article was in German (11); theLeicester Day Programme Treatment (12)because the description of the DH treatmentwas too limited; the Victoria article (13)because it was only a letter to the editor andtherefore too limited.
This left 10 centres:- Day Hospital Program (DHP) of the Toronto
Hospital in Canada (9, 10, 14);- Treatment Centre for Eating Disorders (TCE)
in Munich, Germany (8, 9, 10, 15);- Our Lady of the Lake Eating Disorders Pro-
gram in Baton Rouge, USA (9, 10, 16, 17);- Eating Disorder Program (EDP) in Hoffman
Estates, USA (10, 18);- Cullen Centre (CC) in Edinburgh, United
Kingdom (19);- Amarum in Zutphen, The Netherlands (10);- Oxford Adult Eating Disorders Service
(OAEDS) in Oxford, United Kingdom (10, 20);- Day Clinic Programme (DCP) in Freiburg,
Germany (21);- Day Treatment Programme (DTP) in Chonan
City, South Korea (22),- Wesley Private Hospital (WPH) in Sydney,
Australia (10, 23, 24).Three papers (25-27) about the Day Clinic
Programme in Freiburg and the Day Treat-ment Programme in Chonan City wereexcluded because in German and Korean,respectively.
THE DAY HOSPITALPROGRAMME OF THE EATINGDISORDERS CENTRE, TURIN
The DH of the EDs Centre of Turin Universityopened in July 2006 and is part of a more thor-ough treatment programme, including alsooutpatient and inpatient care.
DH treatment has a bio-psycho-social frame-work with psychodynamic orientation. Psycho-dynamic group therapy, with an open structureof groups, and Adlerian individual psychother-apy (28-30) are the main treatment tools (Tables1 and 2). The psychodynamic groups encour-age patients to examine their interpersonalfunctioning, inner problems and the psychody-namic meaning of symptoms. Cognitive-behav-ioural techniques are used in a group setting tohelp patients in developing strategies to chal-lenge their irrational cognitions and exploringalternatives to their unhealthy behaviours (31).
The DH of the EDs Centre of Turin Universityfollows a single model (the psychodynamicone) and combines different strategies and pro-cedures. Being based on a psychodynamicmodel, the specific therapeutic agents are notthe core symptoms of EDs, but instead relation-ships, the individual’s personality and the clas-sic psychodynamic tools (clarification, con-frontation, interpretation). The advantage ofadopting broad tecniques versus a morefocused treatment is the possibility to plan indi-vidualised care, avoiding the well known risksof clinical trial in EDs (32). Furthermore, in thepsychodynamic theory the therapeutic agentdepends on the conscious use of the relation-ship and not simply on single techniques.
The disadvantage of using broad tecniques isthe likelihood of including elements which arenot so essential in the treatment plan. On theother hand, currently it is not clear which arethe most effective treatments for AN (4).
Goals of treatment are both nutritional andpsychological. The first include nutritionalrehabilitation, weight gain, modification of dis-turbed eating behaviours, and identification of
e32 Eating Weight Disord., Vol. 14: N. 2-3 - 2009
TABLE 1Brief Adlerian Psychodynamic Psychotherapy (B-APP).
Referencial paradigms Objects Elements of the therapeutic process
Individual = psychosomatic unity integrated in the society Resolution of the focus problem Establish encouraging relationship with the therapist
Individual = build and regulate self’s image Decrease/non-increase of symptoms Identify the focus; relate symptoms with currentlife situation
Bond and symbolic patterns regulate human relationships Increase of subject’s quality of life Detect, in the focus problem, the areas for possiblechanges

TABLE 2The week’s organization of the Turin treatment day hospital.
Day hospital for eating disorders: A review
perpetuating factors. The latter include anincrease of patients’ awareness of the disorderand of motivation to treatment, a psychody-namic understanding of symptoms, a deeperawareness and understanding of emotions, animprovement in relational skills and socialadjustment, self-esteem and mood regulation.
The treatment programme aims to enhancethe maturation of personality together with thechange of symptomatic behaviours. The core oftreatment is represented by the association of atherapeutic work focused on personality and onthe eating disordered symptom together with atreatment setting where patients live, work andeat together. Another important element is thework on family and with the family (counseling).
Individual psychotherapy (weekly sessions)with a psychodynamic Adlerian orientationoffers patients an opportunity of reflection andelaboration of their experiences.
Group psychotherapy sessions take placeevery day and enhance the expression of emo-tions. The group setting allows to work on therelational dynamics which take place hic etnunc. This is particularly relevant in patientswith EDs, who have difficulties in recognizingand understanding their emotions and buildingsignificant and intimate relationships. The elabo-ration of patients’ experiences and the mirroringand empathic identification mechanisms activat-ed by group therapy increase patients’ coopera-tion skills and reduce their competitiveness.
The psychodynamic approach could also beuseful to strengthen patients’ improvementafter discharge, as described for outpatientswith other psychiatric disorders (33, 34).
The Turin DH can treat about ten patients atthe same time. Patients are admitted after diag-nostic sessions and after signing a behaviouralcontract; they are usually referred from outpa-tient units, previous failed treatments or frominpatient care. Inclusion criteria are a Diagnos-
tic and Statistical Manual of Mental Disorders -fourth edition (DSM-IV) diagnosis of ED, eitherAN or BN, medical stability and a body massindex (BMI) >13.5 kg/m². Patients must showmotivation for treatment and have some capac-ity to relate in a group setting. Exclusion crite-ria are an acute suicide or medical risk, sub-stance abuse or dependence, comorbid psy-chotic symptoms or BMI<13.5 kg/m². Patientswith a BMI <13.5 kg/m² are excluded becauseinpatients treatments is more suitable for theseverity of their clinical status.
The average length of stay is 24-26 weeks,from Monday to Friday for about 7 hours perday. In DH, patients eat lunch and a snack inthe mid-morning with the assistance of nursesand dietician (assisted eating), who help andsupport patients facing difficulties duringmeals. All patients have an individually bal-anced meal plan prescribed by the dietician.Patients are weighed in underwear before thesnack, from three times to once a week; whenunderweight, their target weight is set individ-ually and the medical staff can decide whetherto use or not intravenous feeding.
The staff consists of a psychiatrist, 2 half-daypsychiatrists, a half-day clinic psychologist, 2psychiatry trainees, 5 nurses, a dietician, a con-sultant nutritionist, a consultant supervisor anda consultant music therapist. Every week a con-sultant nutritionist evaluates patients’ physicalhealth status. Psychiatric drugs (antidepres-sants, antipsychotics, BDZ and mood stabilis-ers) for comorbid psychiatric symptoms(depression, anxiety, mood instability) are pre-scribed when indicated.
RESULTS
Eighteen suitable articles and two reviewswere analyzed. The main features of each cen-
e33Eating Weight Disord., Vol. 14: N. 2-3 - 2009
Monday Tuesday Wednesday Thursday Friday
8.30-9.30 Welcome and Welcome and Welcome and Body image therapy Welcome andpharmacologic therapy pharmacologic therapy pharmacologic therapy phfarmacologic therapy
9.30-10.30 Dietistic visits Individual psycotherapy Music therapy Nutritional visits Cognitive behaviouraltecniques
10.30-11.00 Assisted snack Assisted snack Assisted snack Assisted snack Assisted snack
11.30-12.30 Psychodinamic group Psychodinamic group Psychodinamic group Psychodinamic group Psychodinamic group
13.00-13.45 Assisted eating Assisted eating Assisted eating Assisted eating Assisted eating
14.00-15.00/30 Psychiatric visits Reading group Creative group Psychiatric visits Recreation
G. Abbate-Daga, C. Gramaglia, S. Preda, et al.
tre included in this study are listed in Table 3.The DCP in Freiburg and the CC in Edin-
burgh are the only centres treating ED patientstogether with patients suffering from otherpsychiatric disorders.
The main variables of the centres studied arethe following:•Main features of the programmes:
- the centres opened in different years (from1980 to 2006);
- treatment orientation: cognitive behaviouralin most cases (9/11), psychodynamic in 2/11cases. The WPH began as psychodynamicbut after 4 years turned to cognitive behav-ioural;
- duration of treatment: highly variable, from3 to 39 weeks (mean 15,04 weeks; standarddeviation=10,22);
- behavioural contract: in all centres exceptfor CC and DTP.
•Treatment goals: modification and normalisa-tion of eating behaviour (10/11), nutritionalrehabilitation and weight gain (8/11), relapseprevention (3/11), promotion of autonomy,social adjustment, self-control and self-esteem(4/11), understanding of symptoms (4/11),identification and resolution of perpetuatingprocesses (6/11), reduction of over-evaluationof shape and weight (5/11).
•Group activities:- treatment type: mostly group (5/11), only
group (2/11), group and individual (4/11);- treatment tools: bio-psycho-social frame-
work (6/11) and cognitive behaviouralgroups (10/11) are the main treatment tools.
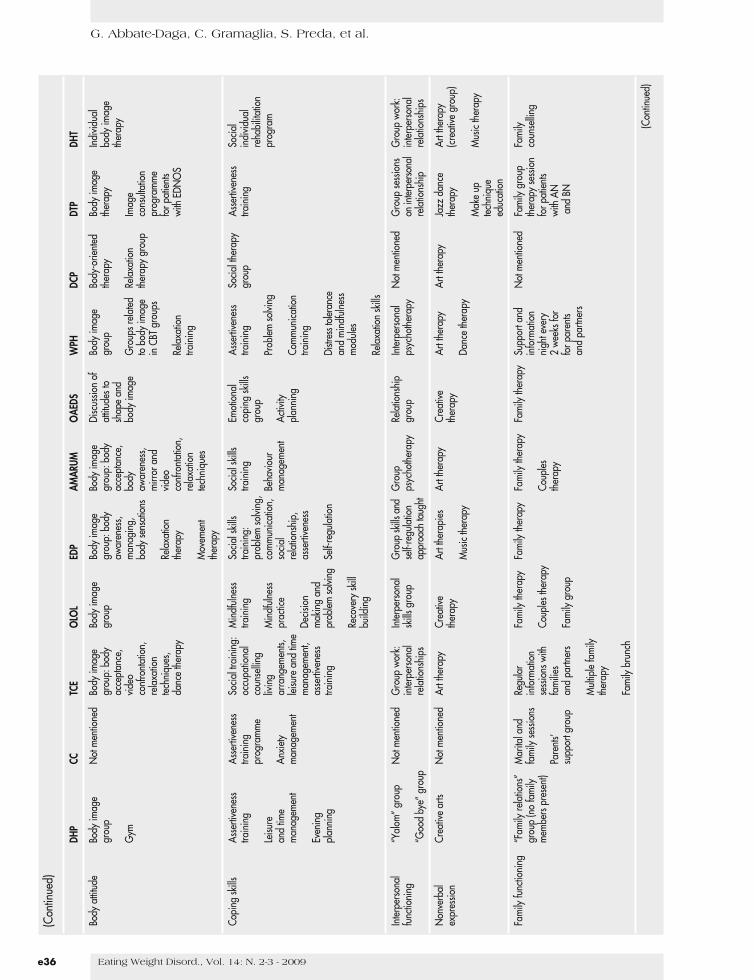
• Issues addressed in individual and groupactivities:- body attitude: (missing for CC) body-image
group (10/11) in every centre, often associat-ed with other body-shape oriented activities;
- coping skills: the most common activities areassertiveness training (6/11) and social skillstraining (4/11);
- interpersonal functioning: (missing for CCand DCP) group work on interpersonal rela-tionship (6/11), interpersonal psychotherapy(2/11), “Yalom” group (1/11), “Good bye”group (1/11);
- nonverbal expression: art, creative and mu-sic therapy (9/11);
- family functioning: all the centres involvefamily in treatment (missing datum for DCP)and the most common approach is familytherapy (6/11);
- other issues: housing facilities (2/11), EDpatients with other psychiatric patients(2/11), vegetarian menu (1/11), operantbehaviour methods (10/11), residence groupwith apartment-like housing (1//11), explicit
use of operant principles and of mindfulness(1/11), recreation (2/11), 2-day camp (1/11),readiness and motivational therapy (1/11),structural process-model and related skills(1/11); CC is close to shops and restaurants.
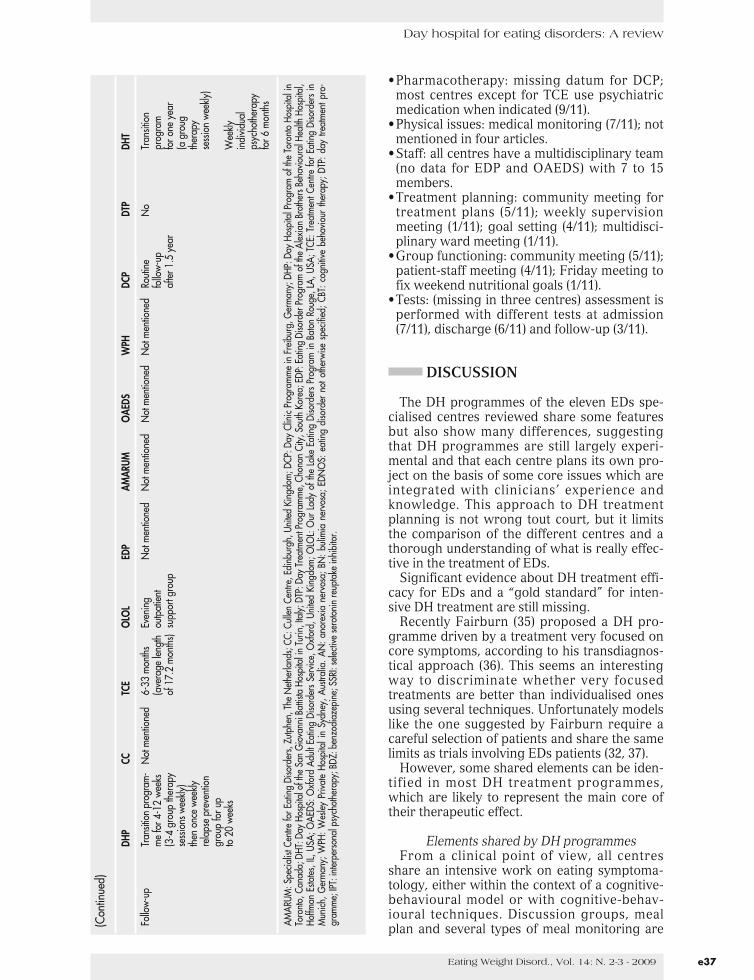
•Follow-up:- only five centres perform a follow-up (5/11):
outpatient support group (1/11); monthlyoutpatients visits (1/11); weekly group thera-py sessions (2/11); weekly individual psy-chotherapy for 6 months (1/11); weeklyrelapse prevention group (1/11).
Other variables studied (not listed in tables)are:•Conditions for admission:
- inclusion criteria: diagnosis of ED accordingto DSM-IV criteria (6/11), failure of previoustreatments (3/11); motivation to change/fortreatment (7/11); medical stability (3/11);capacity to relate in a group (4/11);
- exclusion criteria: suicide risk (10/11), med-ical risk (6/11), substance dependence (8/11),psychosis (4/11).
•Treatment of eating disordered behaviours:meal plan (9/11), assisted eating (6/11), self-monitoring (5/11), nutrition group (8/11), psy-choeducation (4/11), CBT (7/11), cooking(4/11).
•Day treatment is part of a larger eating disor-der programme in all centres (11/11).
•Group size: from 5 to 20 (mean 9,8; standarddeviation 3,68); missing for CC.
•Group structure: half open (1/11), closed(1/11), open (7/11); missing for CC and DCP.
•Days a week: three (1/11), four (3/11), five(7/11), seven (1/11). The WPH has 5-day or 3-day treatments; the DHP in the years 1995-2000 lasted 4 days/week.
•Patients’ features:- diagnosis: mostly AN (3/11); mostly BN
(1/11); only BN (1/11); AN, BN and ED nototherwisw specified (EDNOS; 1/11). Missingdatum for five centres;
- average duration of patients’ illness: from4.19 to 9.4 years (7.42±1.86 years). Missingdatum for five centres;
- BMI: highly variable according to the rate ofanorexic and bulimic patients, from 17.03 to23.9 kg/m² (20.49±2.41 kg/m²). Missingdatum for five centres.
•Weight control: (missing for CC and DCP)daily weighing (3/11), weighing group (2/11),weekly weighing (3/11), individual weighing:3, 2, 1 time/week (2/11).
•When underweight: most centres (8/11) fix anobjective for weight gain/week (which can varyand in the DHP is fixed only for anorexics); liq-uid nutritional supplements (2/11); individualtarget weight range (2/11).
e34 Eating Weight Disord., Vol. 14: N. 2-3 - 2009

Day hospital for eating disorders: A review
e35Eating Weight Disord., Vol. 14: N. 2-3 - 2009
TABL
E3
The
mai
nfe
atur
esof
the
day
hosp
ital(
DH)o
fthe
eatin
gdi
sord
erss
pecia
lised
cent
res.
DHP
CCTC
EO
LOL
EDP
AMAR
UMO
AEDS
WPH
DCP
DTP
DHT
Ope
rativ
e19
85La
te19
80s
1989
1990
1992
,rev
ised
1993
1994
1994
1998
2000
2006
since
in19
99
Trea
tmen
tCo
gniti
veCo
gniti
veCo
gniti
veCo
gniti
veCo
gniti
veCo
gniti
veCo
gniti
ve(1
994-
98Ps
ycho
dina
mic
Cogn
itive
Psyc
hodi
nam
icor
ient
atio
nbe
havio
ural
beha
viour
albe
havio
ural
beha
viour
albe
havio
ural
beha
viour
albe
havio
ural
Psyc
hodi
nam
ic)be
havio
ural
Cogn
itive
beha
viour
al
Dura
tion
ofAN
:10-
11Ab
out2
4we
eks
13-1
6we
eks
10we
eks
4-5
week
s26
-39
week
sUp
to9
No
fixed
lengt
h,12
week
s8-
14we
eks
24-2
6we
eks
treat
men
twe
eks
mon
ths
(ave
rage
BN:6
-8we
eks
8-9
week
s)
Beha
viora
lcon
tract
Yes
Not
men
tione
dYe
sYe
sYe
sYe
sYe
sYe
sYe
sN
otm
entio
ned
Yes
Trea
tmen
tgoa
lsW
eigh
tgai
nfo
rPr
omot
ion
ofW
eigh
tgai
nRe
ach
and
Inter
rupt
ion
ofN
orm
alisa
tion
Nor
mal
isatio
nW
eigh
tgai
nM
odifi
catio
nof
Wei
ghtc
hang
eW
eigh
tgai
npa
tient
swith
feeli
ngso
fm
aint
ain
goal
the
mos
tof
weig
htof
weig
htdi
sturb
edBM
I<18
.5au
tono
my,
Mod
ifica
tion
weig
htra
nge
delet
erio
usN
orm
alisa
tion
eatin
gM
odifi
catio
nM
odifi
catio
nse
lfco
ntro
lm,
ofdi
sturb
edas
pects
ofth
eN
orm
alisa
tion
Nor
mal
isatio
nof
eatin
gbe
havio
urof
distu
rbed
ofdi
sturb
edN
orm
aliz
atio
nof
self
estee
mea
ting
Stab
ilizat
ion
ofea
ting
diso
rder
ofdi
sturb
edof
eatin
gbe
havio
ur;
eatin
gea
ting
distu
rbed
eatin
gbe
havio
urhe
alth
yea
ting
eatin
gbe
havio
urco
ntai
nea
ting
Unde
rsta
ndin
gbe
havio
urs
beha
viour
sbe
havio
urTa
rget
weig
htpa
ttern
sN
orm
aliz
atio
nbe
havio
urdi
sord
ered
ofco
nflic
tsar
eno
tgive
nUn
ders
tand
ing
eatin
gpa
ttern
sM
odifi
catio
nof
beha
viour
orpe
rson
ality
Unde
rsta
ndin
gPs
ycho
dina
mic
Iden
tifica
tion
of(p
atie
ntsa
reof
sym
ptom
sM
odifi
catio
nof
Redu
ction
ofov
er-e
valua
tion
defic
itsof
unde
rsta
ndin
gpe
rpetu
atin
gno
tref
ed)
body
imag
eId
entif
icatio
nof
over
-eva
luatio
nof
cont
rol
Redu
ction
ofps
ycho
logi
cal
ofsy
mpt
oms
proc
esse
sSt
reng
then
distu
rban
cepe
rpetu
atin
gof
eatin
g,ov
erea
ting,
over
-eva
luatio
nsy
mpt
oms
Lear
nto
hand
lese
lfwo
rkfa
ctors
body
shap
esh
ape
and
ofea
ting,
Iden
tifica
tion
Restr
uctu
ring
offo
odId
entif
icatio
nof
and
weig
htwe
ight
shap
ean
dDe
pres
sion
ofpe
rpetu
atin
gdi
sturb
edth
ough
tsap
prop
riatel
yCh
ange
sin
perp
etuat
ing
Enha
ncem
ento
fas
part
ofse
lfwe
ight
aspa
rtfa
ctors
and
attitu
des
psyc
hopa
tolo
gyfa
ctors
self
regu
latio
n,co
ncep
tIm
prov
emen
tsof
self
conc
ept
Prom
otio
nof
rela
tedto
shap
eAw
aren
esso
fan
dso
cial
deve
lopm
ento
fin
socia
lse
lf-es
teem
Impr
ovem
ents
and
weig
htth
eird
ifficu
lties
outco
mes
Enha
ncem
ento
fse
lf-re
gula
tory
Iden
tifica
tion
ofad
justm
ent,
Iden
tifica
tion
ofin
socia
lfa
mily
and
socia
lsk
illspe
rpetu
atin
gse
lf-es
teem
perp
etuat
ing
adju
stmen
t,Ch
ange
isW
ork
onfu
nctio
ning
facto
rsan
dm
ood
facto
rsse
lf-es
teem
resp
onsa
bility
inter
actio
nal
Arra
ngem
ento
fre
gula
tion
and
moo
dof
the
patie
ntpr
oblem
sRe
laps
ea
secu
rean
dRe
laps
ere
gula
tion
prev
entio
nsu
ppor
tive
prev
entio
nou
tpat
ient
envir
onm
ent
Gro
up/i
ndivi
dual
Onl
ygr
oup
Gro
upan
dO
nly
grou
pM
ostly
grou
p;M
ostly
grou
pM
ostly
grou
pM
ostly
grou
p;G
roup
and
Gro
upan
dM
ostly
grou
p;G
roup
and
treat
men
tin
divid
ual
som
eon
ewe
ekly
indi
vidua
lin
divid
ual
som
ein
divid
ual
indi
vidua
lin
divid
ual
indi
vidua
l
(Con
tinue
d)
G. Abbate-Daga, C. Gramaglia, S. Preda, et al.
e36 Eating Weight Disord., Vol. 14: N. 2-3 - 2009
(Con
tinue
d)
DHP
CCTC
EO
LOL
EDP
AMAR
UMO
AEDS
WPH
DCP
DTP
DHT
Body
attitu
deBo
dyim
age
Not
men
tione
dBo
dyim
age
Body
imag
eBo
dyim
age
Body
imag
eDi
scus
sion
ofBo
dyim
age
Body
-orie
nted
Body
imag
eIn
divid
ual
grou
pgr
oup:
body
grou
pgr
oup:
body
grou
p:bo
dyat
titude
sto
grou
pth
erap
yth
erap
ybo
dyim
age
acce
ptan
ce,
awar
enes
s,ac
cept
ance
,sh
ape
and
ther
apy
Gym
video
man
agin
g,bo
dybo
dyim
age
Gro
upsr
elated
Rela
xatio
nIm
age
conf
ront
atio
n,bo
dyse
nsat
ions
awar
enes
s,to
body
imag
eth
erap
ygr
oup
cons
ultat
ion
rela
xatio
nm
irror
and
inCB
Tgr
oups
prog
ram
me
techn
ique
s,Re
laxa
tion
video
forp
atie
nts
danc
eth
erap
yth
erap
yco
nfro
ntat
ion,
Rela
xatio
nwi
thED
NO
Sre
laxa
tion
train
ing
Mov
emen
ttec
hniq
ues
ther
apy
Copi
ngsk
illsAs
serti
vene
ssAs
serti
vene
ssSo
cialt
rain
ing:
Min
dfuln
ess
Socia
lskil
lsSo
cials
kills
Emot
iona
lAs
serti
vene
ssSo
cialt
hera
pyAs
serti
vene
ssSo
cial
train
ing
train
ing
occu
patio
nal
train
ing
train
ing:
train
ing
copi
ngsk
illstra
inin
ggr
oup
train
ing
indi
vidua
lpr
ogra
mm
eco
unse
lling
prob
lemso
lving
,gr
oup
reha
bilita
tion
Leisu
reliv
ing
Min
dfuln
ess
com
mun
icatio
n,Be
havio
urPr
oblem
solvi
ngpr
ogra
man
dtim
eAn
xiety
arra
ngem
ents,
prac
tice
socia
lm
anag
emen
tAc
tivity
man
agem
ent
man
agem
ent
leisu
rean
dtim
ere
latio
nshi
p,pl
anni
ngCo
mm
unica
tion
man
agem
ent,
Decis
ion
asse
rtive
ness
train
ing
Even
ing
asse
rtive
ness
mak
ing
and
plan
ning
train
ing
prob
lemso
lving
Self-
regu
latio
nDi
stres
stole
ranc
ean
dm
indf
ulnes
sRe
cove
rysk
illm
odule
sbu
ildin
gRe
laxa
tion
skills
Inter
pers
onal
“Yal
om”g
roup
Not
men
tione
dG
roup
work
:In
terpe
rson
alG
roup
skills
and
Gro
upRe
latio
nshi
pIn
terpe
rson
alN
otm
entio
ned
Gro
upse
ssio
nsG
roup
work
:fu
nctio
ning
inter
pers
onal
skills
grou
pse
lf-re
gula
tion
psyc
hoth
erap
ygr
oup
psyc
hoth
erap
yon
inter
perso
nal
inter
pers
onal
“Goo
dby
e”gr
oup
rela
tions
hips
appr
oach
taug
htre
latio
nshi
pre
latio
nshi
ps
Non
verb
alCr
eativ
ear
tsN
otm
entio
ned
Artt
hera
pyCr
eativ
eAr
tthe
rapi
esAr
tthe
rapy
Crea
tive
Artt
hera
pyAr
tthe
rapy
Jazz
danc
eAr
tthe
rapy
expr
essio
nth
erap
yth
erap
yth
erap
y(cr
eativ
egr
oup)
Mus
icth
erap
yDa
nce
ther
apy
Mak
eup
Mus
icth
erap
ytec
hniq
ueed
ucat
ion
Fam
ilyfu
nctio
ning
“Fam
ilyre
latio
ns”
Mar
itala
ndRe
gula
rFa
mily
ther
apy
Fam
ilyth
erap
yFa
mily
ther
apy
Fam
ilyth
erap
ySu
ppor
tand
Not
men
tione
dFa
mily
grou
pFa
mily
grou
p(n
ofa
mily
fam
ilyse
ssio
nsin
form
atio
nin
form
atio
nth
erap
yse
ssio
nco
unse
lling
mem
bers
pres
ent)
sess
ions
with
Coup
lesth
erap
yCo
uples
nigh
teve
ryfo
rpat
ient
sPa
rent
s’fa
milie
sth
erap
y2
week
sfor
with
ANsu
ppor
tgro
upan
dpa
rtner
sFa
mily
grou
pfo
rpar
ents
and
BNan
dpa
rtner
sM
ultip
lefa
mily
ther
apy
Fam
ilybr
unch
(Con
tinue
d)
Day hospital for eating disorders: A review
•Pharmacotherapy: missing datum for DCP;most centres except for TCE use psychiatricmedication when indicated (9/11).
•Physical issues: medical monitoring (7/11); notmentioned in four articles.
•Staff: all centres have a multidisciplinary team(no data for EDP and OAEDS) with 7 to 15members.
•Treatment planning: community meeting fortreatment plans (5/11); weekly supervisionmeeting (1/11); goal setting (4/11); multidisci-plinary ward meeting (1/11).
•Group functioning: community meeting (5/11);patient-staff meeting (4/11); Friday meeting tofix weekend nutritional goals (1/11).
•Tests: (missing in three centres) assessment isperformed with different tests at admission(7/11), discharge (6/11) and follow-up (3/11).
DISCUSSION
The DH programmes of the eleven EDs spe-cialised centres reviewed share some featuresbut also show many differences, suggestingthat DH programmes are still largely experi-mental and that each centre plans its own pro-ject on the basis of some core issues which areintegrated with clinicians’ experience andknowledge. This approach to DH treatmentplanning is not wrong tout court, but it limitsthe comparison of the different centres and athorough understanding of what is really effec-tive in the treatment of EDs.
Significant evidence about DH treatment effi-cacy for EDs and a “gold standard” for inten-sive DH treatment are still missing.
Recently Fairburn (35) proposed a DH pro-gramme driven by a treatment very focused oncore symptoms, according to his transdiagnos-tical approach (36). This seems an interestingway to discriminate whether very focusedtreatments are better than individualised onesusing several techniques. Unfortunately modelslike the one suggested by Fairburn require acareful selection of patients and share the samelimits as trials involving EDs patients (32, 37).
However, some shared elements can be iden-tified in most DH treatment programmes,which are likely to represent the main core oftheir therapeutic effect.
Elements shared by DH programmesFrom a clinical point of view, all centres
share an intensive work on eating symptoma-tology, either within the context of a cognitive-behavioural model or with cognitive-behav-ioural techniques. Discussion groups, mealplan and several types of meal monitoring are
e37Eating Weight Disord., Vol. 14: N. 2-3 - 2009
(Con
tinue
d)
DHP
CCTC
EO
LOL
EDP
AMAR
UMO
AEDS
WPH
DCP
DTP
DHT
Follo
w-up
Tran
sitio
npr
ogra
m-
Not
men
tione
d6-
33m
onth
sEv
enin
gN
otm
entio
ned
Not
men
tione
dN
otm
entio
ned
Not
men
tione
dRo
utin
eN
oTr
ansit
ion
me
for4
-12
week
s(a
vera
gelen
gth
outp
atie
ntfo
llow-
uppr
ogra
m(3
-4gr
oup
ther
apy
of17
.2m
onth
s)su
ppor
tgro
upaf
ter1.
5ye
arfo
rone
year
sess
ions
week
ly)(a
grou
gth
enon
cewe
ekly
ther
apy
rela
pse
prev
entio
nse
ssio
nwe
ekly)
grou
pfo
rup
to20
week
sW
eekly
indi
vidua
lps
ycho
ther
apy
for6
mon
ths
AMAR
UM:S
pecia
listC
entre
forE
atin
gDi
sord
ers,
Zutp
hen,
The
Neth
erla
nds;
CC:C
ullen
Cent
re,E
dinb
urgh
,Uni
tedKi
ngdo
m;D
CP:D
ayCl
inic
Prog
ram
me
inFr
eibu
rg,G
erm
any;
DHP:
Day
Hosp
italP
rogr
amof
the
Toro
nto
Hosp
itali
nTo
ront
o,Ca
nada
;DHT
:Day
Hosp
italo
fthe
San
Gio
vann
iBat
tista
Hosp
itali
nTu
rin,I
taly;
DTP:
Day
Trea
tmen
tPro
gram
me,
Chon
anCi
ty,So
uth
Kore
a;ED
P:Ea
ting
Diso
rder
Prog
ram
ofth
eAl
exia
nBr
othe
rsBe
havio
ural
Heal
thHo
spita
l,Ho
ffman
Esta
tes,I
L,US
A;O
AEDS
:Oxf
ord
Adult
Eatin
gDi
sord
ers
Serv
ice,O
xfor
d,Un
ited
King
dom
;OLO
L:O
urLa
dyof
the
Lake
Eatin
gDi
sord
ers
Prog
ram
inBa
ton
Roug
e,LA
,USA
;TCE
:Tre
atm
entC
entre
forE
atin
gDi
sord
ers
inM
unich
,Ger
man
y;W
PH:W
esley
Priva
teHo
spita
lin
Sydn
ey,A
ustra
lia.A
N:a
nore
xia
nerv
osa;
BN:b
ulim
iane
rvos
a;ED
NO
S:ea
ting
diso
rder
noto
ther
wise
spec
ified
;CBT
:cog
nitiv
ebe
havio
urth
erap
y;DT
P:da
ytre
atm
entp
ro-
gram
me;
IPT:i
nter
pers
onal
psyc
hoth
erap
y;BD
Z:be
nzod
iaze
pine
;SSR
I:se
lectiv
ese
roto
nin
reup
take
inhi
bito
r.

G. Abbate-Daga, C. Gramaglia, S. Preda, et al.
the main treatment tools. The behavioural con-tract (which can show different degrees ofstrictness) (10) and motivation assessment areconsidered necessary by all centres.
The importance of motivation is supported bythe growing number of studies in literatureabout the prognostic importance of the assess-ment of patients’ stage of change and motiva-tion (38). Another shared issue is body imagetherapy, since body image disturbances play arelevant role in maintaining EDs. Body image isalmost always disturbed in ED patients (5, 39,40) and dissatisfaction with body image is apredictor of suicide attempts (41). The increasein body weight during DH treatment canincrease patients’ difficulties with their bodyimage, if these are not properly addressed (42).
Another relevant issue for treatment is familyinvolvement, which can take place in differentways. The onset of EDs often takes place dur-ing adolescence and parents of ED patientsshow some typical relational and personalitypatterns at the questionnaires, which mightplay a pathogenic role (43, 44). Outpatients tri-als showed the efficacy of family therapy (45).As regards DH treatment, the family needs helpto understand and support patients’ psycholog-ical, physical and eating changes. On the otherhand, patients’ understanding of family dynam-ics is part of the therapeutic process (46).
As regards group functioning, all the centresexcept one (including 20 patients) work withsmall groups (8-12 patients) and share the opin-ion that this is the proper number of patients toallow positive group interactions and to workon individual problems (10).
Differences among DH treatmentsGiven the shared issues discussed above, one
would expect not to find relevant differencesamong the centres. Nonetheless, differencesare several.
Only few centres fix a BMI. Overall, theimpression is that decisions about BMI aremade according to patients’ clinical assess-ment. Since a low BMI predicts the failure ofDH treatment (47), it should be carefullyaccounted for. Other inclusion criteria are con-tradictory: for example, three centres requirestable clinical conditions, while another acceptspatients undergoing a fast weight loss.
Only four centres mention the assessment ofpatients’ capacity to relate in a group settingand this suggests that group relational dynam-ics are not always properly accounted for.
Moreover, most centres work with patientswho have failed to respond to other treatments,while other ones accept patients when a DHtreatment is recommended, also as first treat-
ment attempt. In some cases patients areadmitted in DH after discharge from inpatienttreatment, making DH a sort of “prolongation”of care in the context of a wider stepped careprogramme.
The most striking difference is the durationof DH treatment, which ranges from a mini-mum of 3 weeks to a maximum of 39. A criticalreview of data identifies 7 centres treatingpatients for 2-3 months and 4 centres treatingpatients for 6-9 months. This suggests thehypothesis that, despite the shared elementsdescribed above, two different levels of treat-ment intensity exist in DH care. A first model ofDH has a shorter duration and is mainly symp-tom-focused while a second one has a longerduration and is focused on patients’ relationalskills, psychodynamic symptom understandingand more gradual changes in body weight. Thishypothesis is supported by the fact that the 4centres with a longer treatment duration workalso with individual psychotherapy, while 6 outof the other 7 centres work mostly/only withgroup therapy. Moreover, it is likely that short-er treatments address patients in less severeconditions.
Differences in treatment intensity emergealso in the number of days/week, ranging from3 to 7 days/week of DH treatment.
The approach to eating disordered and com-pensation behaviours is included in all DHtreatment programmes and though some basicprinciples are shared, it is quite different fromone centre to another. Some adopt a more con-trolling approach, while others promote auton-omy; several self-monitoring techniques areused and some centres include activities asbuying and cooking food. No univocal indica-tions exist for the frequency of weight con-trols/week.
Though the importance of dieticians’ work isacknowledged and despite the AmericanDietetic Association guidelines (48), it is notclear which are the best techniques to use.
DH programmes use a variety of techniquesfor social skills and creative activities, includingassertiveness training, mindfulness training,dance therapy and different types of art thera-py. Each centre makes its own choices accord-ing to theory of reference and availableresources, but these activities do not seem toplay a specific therapeutic role. Their meaningseems to be that of supporting and lighteningthe symptom-focused interventions which oth-erwise would be monothematic and oppressing.
A last consideration is that no centre per-forms interventions addressing perfectionism,and despite its widely acknowledged role in thepathogenesis of EDs (35, 36, 49, 50) this psy-
e38 Eating Weight Disord., Vol. 14: N. 2-3 - 2009

Day hospital for eating disorders: A review
chopathological core is often unchanged afterDH treatment (42).
Treatment goalsA particular attention must be paid to treat-
ment goals. Apart from the Edinburgh CC,which lacks recent publications, almost all cen-tres share the objective of weight normalisationor weight gain and of modification/norma-lisation of eating behaviour. Only 4 centres outof 11 work specifically on ED perpetuating fac-tors and relapses.
As regards psychological and behaviouralobjectives, there are several differences. Somecentres (4/11) focus attention on the psychologi-cal issues of self-esteem, control and autonomy,according to the cognitive theory about EDs.Other centres underscore the importance of thepsychodynamic or cognitive understanding ofthe symptom itself (5/11), which is relevant fortheir healing process (46). Last, other centresunderscore the need to improve social (3/11) andfamily (2/11) functioning.
Differences in treatment goals seem to reflectthe different emphasis the centres pose onintrapsychic dynamics, relational dynamics andsocial issues.
In conclusion, the work on symptoms is con-sidered an essential and primary objective, butall centres share the opinion that the intensivetreatment of patients is not complete if otherissues than symptoms are not addressed.
ConclusionsThe DH therapeutic programmes reviewed do
not allow to identify univocal guidelines for typeof intervention, treatment intensity and dura-tion. A consensus conference of experts isrequired to define some shared concepts inorder to make DH treatment programmes morehomogenous, measurable and comparable.
Overall, two types of DH treatment can beidentified: a shorter, more symptom-focusedone, and a longer, more person-focused one.
In both cases, attention needs to be paid topatients’ selection, motivation to change andidentification of treatment goals. Coherenceamong treatment model, treatment tools, sever-ity of clinical status and treatment goals needsto be carefully checked.
Moreover, attention to patients’ groupdynamics, equipe group dynamics andpatients/staff dynamics needs to be under-scored and emphasised.
A focus on psychodynamic formulation andresistance to treatment is needed in those cen-tres with a psychodynamic approach and aspecific attention on group dynamics (51). Per-sonalisation of treatment programmes should
consider the study and assessment of personal-ity (52), which is a specific treatment tool of theTurin Centre.
In a multi-disciplinary équipe only somemembers have a psychological training, andthe supervision on group dynamics is neces-sary to increase the relational awareness ofequipe members. How one talks to patients canbe therapeutic or iatrogenic but the importanceof this fact is often underestimated by modernpsychiatry. Indeed, it is necessary for each staffmember to share and discuss his/her impres-sions, emotions and behaviours with the otherones in order to modulate his/her treatmentapproach.
Last, further studies about outcome and fol-low-up of DH treatment are required.
e39Eating Weight Disord., Vol. 14: N. 2-3 - 2009
REFERENCES
1. Van Son G.E., van Hoeken D., Bartelds A.I., van FurthE.F., Hoek H.W.: Time trends in the incidence of eatingdisorders: a primary care study in The Netherlands.Int. J. Eat. Disord., 39, 565-569, 2006.
2. Crow S.J., Nyman J.A.: The cost-effectiveness of ano-rexia nervosa treatment. Int. J. Eat. Disord., 35, 155-160, 2004.
3. Simon J., Schmidt U., Pilling S.: The health service useand cost of eating disorders. Psychol. Med., 35, 1543-1551, 2005.
4. Fairburn C.G., Harrison P.J.: Eating disorders. Lancet,361, 407-416, 2003.
5. American Psychiatric Association: Treatment ofpatients with eating disorders, third edition. AmericanPsychiatric Association. Am. J. Psychiatry, 163, 7Suppl., 4-54, 2006.
6. Wilson G.T., Shafran R.: Eating disorders guidelinesfrom NICE. Lancet, 365, 79-81, 2005.
7. Piran N., Kaplan A., Kerr A., Shekter-Wolfson L.,Winocur J., Gold E., Garfinkel P.E.: A day hospital pro-gram for anorexia and bulimia. Int. J. Eat. Disord., 8,511-521, 1989.
8. Gerlinghoff M., Backmund H., Franzen U.: Evaluationof a day treatment program for eating disorders. Eur.Eat. Disord., 6, 96-106, 1998.
9. Zipfel S., Reas D.L., Thornton C., Olmsted M.P.,Williamson D.A., Gerlinghoff M., Herzog W., BeumontP.J.: Day hospitalisation programs for eating disor-ders: a systematic review of the literature. Int. J. Eat.Disord., 31, 105-117, 2002.
10. Lammers M.W., Exterkate C.C., De Jong C.A.J.: ADutch day treatment program foe anorexia andbulimia nervosa in comparison with internationallydescribed programs. Eur. Eat. Disord. Rev., 15, 98-111, 2007.
11. Reisch T., Thommen M., Csontos Z., Tschacher W.: DieBerner Psychotherapie-Tagesklinik: evaluation undeinordnung in die psychiatrische versor-gungskette[Evaluation of the Bern Day Treatmetn Program andist position in the psychiatric network]. Psychother.Psychosom. Med. Psychol., 52, 56-63, 2002.
12. Birchall H., Palmer R.L., Waine J., Gadsby K., GatwardN.: Intensive day programme treatment for severe
G. Abbate-Daga, C. Gramaglia, S. Preda, et al.
anorexia nervosa - the Leicester experience.Psychiatric Bulletin, 26, 334-336, 2002.
13. Rodriguez C., Fernandez-Corres B., Perez M.J., IruinA., Gonzalez-Pinto A.: Partial hospitalization and out-come of anorexia nervosa. Eur. Psychiatry, 17, 236-237, 2002.
14. Olmsted M.P., Kaplan A.S., Rockert W.: Relative effica-cy of a 4-day versus 5-day day hospital program. Int. J.Eat. Disord., 43, 441-449, 2003.
15. Franzen U., Backmund H., Gerlinghoff M.: Day treat-ment group programme for eating disorders: reasonsfor drop-out. Eur. Eat. Disord. Rev., 12, 153-158, 2004.
16. Stewart T.M., Williamson D.A.: Multidisciplinary treat-ment of eating disorders, part 1. Behav. Modif., 28,812-830, 2004.
17. Stewart T.M., Williamson D.A.: Multidisciplinary treat-ment of eating disorders, part 2. Behav. Modif., 28,831-853, 2004.
18. Levitt J.L., Sansone R.A.: The treatment of eating dis-order clients in a community-based partial hospitaliza-tion program. Journal of Mental Health Counselling,25, 140-151, 2003.
19. Freeman C.: Day patient treatment for anorexia ner-vosa. British Review of Bulimia and Anorexia Nervosa,6, 3-8, 1992.
20. Peake K.J., Limbert C., Whitehead L.: An evaluationof the Oxford adult eating disorders service between1994 and 2002. Eur. Eat. Disord. Rev., 13, 427-435,2005.
21. Zeeck A., Herzog T., Hartmann A.: Day clinic or inpa-tient care for severe bulimia nervosa? Eur. Eat. Disord.Rev., 12, 79-86, 2004.
22. Kong S.: Day treatment programme for patients witheating disorders: randomised controlled trial. J. Adv.Nur., 51, 5-14, 2005.
23. Touyz S., Thornton C., Rieger E., George L., BeumontP.: The incorporation of the stage of change model inthe day hospital treatment of patients with anorexianervosa. Eur. Child. Adolesc. Psychiatry, 12, Suppl. 1,I65-71, 2003.
24. Thornton C., Beumont P., Touyz S.: The Australianexperience of the day programs for patients with eat-ing disorders. Int. J. Eat. Disord., 32, 1-10, 2002.
25. Zeeck A., Hartmann A., Wetzler-Burmeister E.,Wirsching M.: [Comparison of inpatient and day clinictreatment of anorexia nervosa.]. Z. Psychosom. Med.Psychother., 52, 190-203, 2006. German.
26. Zeeck A., Herzog T., Kuhn K., Hartmann A., ScheidtC., Wirsching M.: [Partial hospitalisation -- indicationand characteristic aspects of the setting, shown by theexample of the day clinic in Freiburg/Germany]Psychother. Psychosom. Med. Psychol., 52, 492-9,2002. German.
27. Kong S.S.: [The study for development of day hospitalprogram of eating disorders.] Taehan Kanho HakhoeChi., 34, 25-34, 2004. Korean.
28. Fassino S., Abbate Daga G., Amianto F., Leombruni P.,Fornas B., Garzaro L., D'Ambrosio G., Rovera G.G.:Outcome predictors in anorectic patients after 6months of multimodal treatment. Psychother.Psychosom., 70, 201-208, 2001.
29. Fassino S., Abbate Daga G., Delsedime N., Busso F.,Pierò A., Rovera G.G.: Baseline personality character-istics of responders to 6-month psychotherapy in eat-ing disorders: preliminary data. Eat. Weight Disord.,10, 40-50, 2005.
30. Ferrero A., Pierò A., Fassina S., Massola T., Lanteri A.,Daga G.A., Fassino S.: A 12-month comparison of briefpsychodynamic psychotherapy and pharmacotherapytreatment in subjects with generalised anxiety disor-ders in a community setting. Eur. Psychiatry, 22, 530-539, 2007.
31. Garner D.M., Garfinkel P.E.: Handbook of treatmentfor eating disorders, 2nd ed. New York, GuilfordPress, 1997.
32. Halmi K.A., Agras W.S., Crow S., Mitchell J., WilsonG.T., Bryson S.W., Kraemer H.C.: Predictors of treat-ment acceptance and completion in anorexia nervosa:implications for future study designs. Arch. Gen.Psychiatry, 62, 776-781, 2005.
33. Maina G., Rosso G., Crespi C., Bogetto F.: Combinedbrief dynamic therapy and pharmacotherapy in thetreatment of major depressive disorder: a pilot study.Psychother. Psychosom., 76, 298-305, 2007.
34. Abbass A.A., Hancock J.T., Henderson J., Kisely S.:Short-term psychodynamic psychotherapies for com-mon mental disorders. Cochrane Database Syst. Rev.,8, CD004687, 2006.
35. Fairburn C.G: Cognitive behaviour therapy and Eatingdisorder. New York, Guilford Press; 2008.
36. Wade T.D., Bergin J.L., Martin N.G., Gillespie N.A.,Fairburn C.G.: A transdiagnostic approach to under-standing eating disorders. J. Nerv. Ment. Dis., 194,510-517, 2006.
37. Halmi K.A: The perplexities of conducting randomized,double-blind, placebo-controlled treatment trials inanorexia nervosa patients. Am. J. Psychiatry, 165,1227-1228, 2008.
38. Castro-Fornieles J., Casulà V., Saura B., Martínez E.,Lazaro L., Vila M., Plana M.T., Toro J.: Predictors ofweight maintenance after hospital discharge in ado-lescent anorexia nervosa. Int. J. Eat. Disord., 40, 129-135, 2007.
39. Ruuska J., Kaltiala-Heino R., Rantanen P., KoivistoA.M.: Are there differences in the attitudinal bodyimage between adolescent anorexia nervosa andbulimia nervosa? Eat. Weight Disord., 10, 98-106,2005.
40. Benninghoven D., Tetsch N., Kunzendorf S., JantschekG.: Perceptual body image of patients with anorexia orbulimia nervosa and their fathers. Eat. Weight Disord.,12, 12-19, 2007.
41. Stein D., Orbach I., Shani-Sela M., Har-Even D.,Yaruslasky A., Roth D., Meged S., Apter A.: Suicidaltendencies and body image and experience in anorexianervosa and suicidal female adolescent inpatients.Psychother. Psychosom., 72, 16-25, 2003.
42. Manara F., Manara A., Todisco P.: Correlationbetween psychometric and biological parameters inanorexic and bulimic patients during and after anintensive day hospital treatment. Eat. Weight Disord.,10, 236-244, 2005.
43. Fassino S., Svrakic D., Abbate-Daga G., Leombruni P.,Amianto F., Stanic S., Rovera G.G.: Anorectic familydynamics: temperament and character data. Compr.Psychiatry, 43, 114-120, 2002.
44. Fassino S., Amianto F., Daga G.A., Leombruni P.,Garzaro L., Levi M., Rovera G.G.: Bulimic familydynamics: role of parents’ personality: a controlledstudy with the Temperament and Character Inventory.Compr. Psychiatry, 44, 70-77, 2003.
45. Lock J., le Grange D.: Family-based treatment of eatingdisorders. Int. J. Eat. Disord., 37, Suppl., S 64-67, 2005.
e40 Eating Weight Disord., Vol. 14: N. 2-3 - 2009

Day hospital for eating disorders: A review
46. Fassino S., Pierò A., Levi M., Gramaglia C., AmiantoF., Leombruni P., Abbate Daga G.: Psychological treat-ment of eating disorders. A review of the literature.Panminerva Med., 46, 189-98, 2004.
47. Howard W.T., Evans K.K., Quintero-Howard C.V.,Bowers W.A., Andersen A.E.: Predictors of success orfailure of transition to day hospital treatment for inpa-tients with anorexia nervosa. Am. J. Psychiatry, 156,1697-1702, 1999.
48. Duyff R.: American Dietetic Association. CompleteFood and Nutrition Guide. John Wiley and Sons,Inc., 2006.
49. Bulik C.M., Tozzi F., Anderson C., Mazzeo S.E., Aggen
S., Sullivan P.F.: The relation between eating disor-ders and components of perfectionism. Am. J.Psychiatry, 160, 366-368, 2003.
50. Bardone-Cone A.M., Wonderlich S.A., Frost R.O.,Bulik C.M., Mitchell J.E., Uppala S., Simonich H.:Perfectionism and eating disorders: current status andfuture directions. Clin. Psychol. Rev., 27, 384-405, 2007.
51. Mace C., Binyon S.: Teaching psychodynamic formula-tion to psychiatric trainess. Part 1: Basics of formulation.Advances in Psychiatric Treatment, 11, 416-423, 2005.
52. Mezzich J.E.: Psychiatry for the person: articulatingmedicine’s science and humanism. World Psychiatry,6, 65-67, 2007.
e41Eating Weight Disord., Vol. 14: N. 2-3 - 2009





























