Embed Size (px)
Citation preview
APPRAISAL OF WOUNDCARE
OF PRESSURE ULCERS IN
LEPROSY: A STUDY IN NEPAL.
Study at Green Pastures Hospital and Rehabilitation
Centre Pokhara, Nepal
Contact:
Author: Marisa van de Mortel – 2512363 – Master Health Science AM_471106 International Public Health – 27 ECTS [email protected]
Date of submission: January 25, 2015
Number of words: 8322
VU- supervisor: J.W. Brandsma, PhD Athena Institute, Faculty of Earth and Life Sciences – VU University
De Boelelaan 1085 – 1081 HV Amsterdam – Netherlands
On-site supervisor: P.W. Roche, PhD – Hospital superintendent
Green Pastures Hospital and Rehabilitation Centre Pokhara – Nepal

M. van de Mortel ― VU University Amsterdam/ January 2015 2
Appraisal of woundcare of pressure ulcers in leprosy: a study in Nepal.
Marisa van de Mortel
Abstract
Introduction: The worldwide affected leprosy population with permanent impairments such
as loss of protective sensation is estimated to be three million. A well-known complication of
this condition is plantar ulceration. Autonomic nerve damage results in loss of sweating and
dryness in the hands and feet which increases the risk of ulceration. Pressure ulcers are
defined as lesions caused by unrelieved pressure, resulting in damage to the underlying
tissue. The patient’s self-awareness and self-care is crucial in order to minimize ulceration
and to facilitate healing when ulceration has already occurred. Therefore, this research aims
to assess at what extent woundcare and self-care is practiced conform to recommended
practice and, secondly, to evaluate the knowledge of patients and staff about the cause,
treatment, and prevention of leprosy and pressure ulcers.
Methods: Annual reports were reviewed to obtain an overview of the magnitude of the ulcer
care problem. The woundcare protocol was also audited. Three focus group discussions each
consisting of 5-6 leprosy participants or healthcare professionals were conducted with the
objective of answering beliefs about woundcare. In addition, ten leprosy affected persons
were interviewed about leprosy and the important aspects related to woundcare. Finally,
two ulcer management experts were interviewed about the outcome of this research.
Results: A six years trend in leprosy ulcer care showed a reduction of 33 days in average
healing time, a decrease of 30% in first time ulcer admissions and new ulcer sites in patients
who previously had an ulcer, and a decline of 39% of complicated ulcers requiring surgery.
Woundcare practice did not follow the protocol. Participants in the focus group discussions
and interviewees were well aware of the cause of leprosy, and cause, treatment and
prevention of ulcers.
Discussion & conclusion: The reduction in healing time could suggest that ulcers were
smaller and therefore healed faster. Self-care has been shown to be very effective and
Woundcare of pressure ulcers in leprosy 3
reduces the number of admissions as well as admission time. Leprosy affected persons have
adequate knowledge about the disease and about cause, treatment and prevention of
ulcers. Early detection of leprosy and loss of protective sensation are important in the
prevention of ulceration. This research identified areas where woundcare and self-care
management can be improved.
Keywords: leprosy, disability, rehabilitation, woundcare, pressure ulcers, beliefs, self-care,
Nepal.
Introduction
Leprosy is a chronic granulomatous infection of the skin and superficial peripheral nerves caused by
Mycobacterium leprae (Britton & Lockwood, 2004). The damage to peripheral nerves may result in
sensory and motor impairment with characteristic deformities and disability (Britton & Lockwood,
2004). Early diagnosis and treatment with multidrug therapy (MDT) remain the key to eliminate the
disease as a public health concern. Green Pastures Hospital and Rehabilitation Centre (GPH&RC) in
the Western region of Nepal in Kaski district was established as a specialist leprosy hospital. Nepal is
the fifth leading country in incidence of leprosy (Britton & Lockwood, 2004; WHO, 2012). The new
case detection rate in leprosy in Kaski is 0.73%, prevalence rate is 0.53%, and the proportion of
patients with visible disability among new cases is 2.70% (Leprosy annual report, 2012/13). Leprosy
can cause progressive and permanent damage to the skin, limbs and eyes (WHO, 2014). The
proportion of new patients with visible disability, such as ulceration, or muscle paralysis and muscle
contractures, is determined by the extent of nerve damage which is often caused by a delay in
diagnosis and/or inadequate treatment of nerve complications (Lockwood & Saunderson, 2012). The
delay in diagnosis and treatment can lead to the development of neuropathy which can lead to
extensive nerve damage (Van Veen, Meima, & Richardus, 2006), but nerve function impairment (NFI)
can also develop as a complication after diagnosis. An estimated three million leprosy patients have
completed MDT and have permanent impairments such as loss of protective sensation and paralysis
as a result of NFI. These patients need continuing (self-) care to limit further secondary complications
like ulcers. Autonomic nerve damage increases the risk of ulceration because of dryness of feet
(Lockwood & Saunderson, 2012). Pressure ulcers are defined as lesions caused by unrelieved
pressure, resulting in damage to the underlying tissue. They usually occur over bony prominences,
high pressure areas (e.g. forefoot). The aetiology of pressure ulcers is multifactorial. Pressure, shear,
friction, lack of moisture, and poor nutrition contribute to the aetiology of pressure ulcers (Garber &
Rintale, 2003; Krause & Broderick, 2004). Other factors associated with the development of pressure
ulcers include immobility and psychosocial factors, such as inadequate personal and financial
resources (e.g. lack of transportation for medical check-up, low self-esteem, and compulsory work

M. van de Mortel ― VU University Amsterdam/ January 2015 4
commitment) and noncompliance with acknowledged preventive behaviours (Garber & Rintale, 2003;
Krause & Broderick, 2004). It is believed that pressure ulcers may be prevented with appropriate
health maintenance behaviours including protective footwear. For example, rehabilitation programs
commit substantial time on education to help in the prevention of pressure ulcers (Krause & Broderick,
2004). Patient’s self-awareness and self-care is crucial. A patient with an anaesthetic hand or foot
needs to understand the importance of daily self-care, especially protection when undertaking
potentially harmful activities (Lockwood & Saunderson, 2012). Detail on the process of ulcer causation
and treatment has been provided by Hugh Cross (2012) in a guideline for woundcare in leprosy.
Ulcers are a major, to a large extent preventable, complication in leprosy affected persons (LAP) and
(re)admissions for this complications are greatly affecting the budget of the hospital while maintaining
negative attitudes about the disease. Knowledge about ulcer prevention and ‘best’ care practice in
addition to sound knowledge about prevention and care principles can reduce the burden of this
complication. Overall, woundcare in ulcers is practice-based. It is relevant for GPH&RC to get more
insights in woundcare since many LAP are suffering from ulcers. This research aims to identify areas
where care can be improved.
This research aims to:
- assess to what extent woundcare and self-care is practiced conform recommended practice and
- evaluate if patients and staff have adequate knowledge about cause, treatment, and prevention of
leprosy and pressure ulcers.
Conceptual Model
The conceptual model of theory of planned behaviour (TPB) of Azjen (1991) has been used because
this explains how certain behaviour in relation to ulcers in leprosy can be viewed. Ajzen argues that a
person will spend more effort to perform a desired health behaviour when his perception of
behavioural control, together with intention, is high. This can provide a focus in targeting those
specific environmental factors in which control beliefs are most strongly associated with intention or
behaviour (Montaño & Kasprzyk, 2002). The model of Ajzen has been modified by adding two
concepts (e.g. knowledge and supplies). The adjusted concept knowledge may be important because
it has a strong influence on behaviour change. The practice of woundcare is influenced by the
knowledge of health professionals and the supply of woundcare materials. This has been evaluated in
the first research aim. Then, depending on the knowledge of LAP and staff, practical
recommendations in woundcare and self-care can be given. This concerns the second research aim.
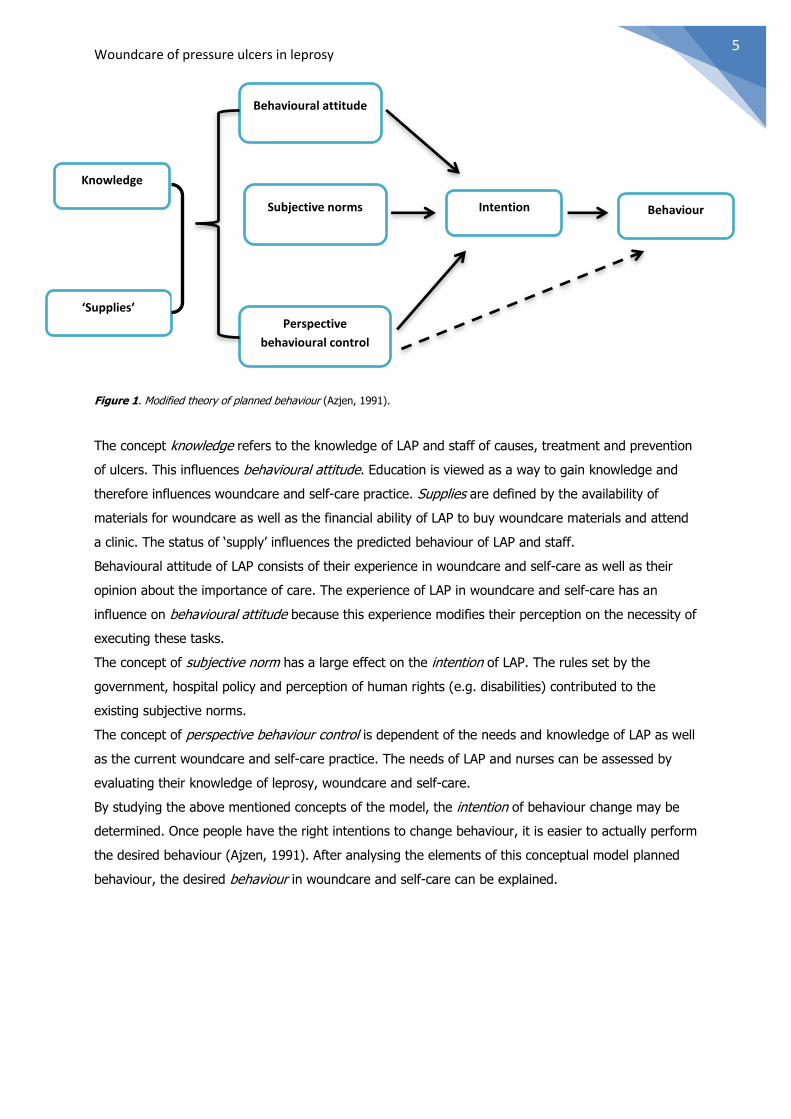
Figure 1 shows how the TPB model fits this research.
Woundcare of pressure ulcers in leprosy 5
Figure 1. Modified theory of planned behaviour (Azjen, 1991).
The concept knowledge refers to the knowledge of LAP and staff of causes, treatment and prevention
of ulcers. This influences behavioural attitude. Education is viewed as a way to gain knowledge and
therefore influences woundcare and self-care practice. Supplies are defined by the availability of
materials for woundcare as well as the financial ability of LAP to buy woundcare materials and attend
a clinic. The status of ‘supply’ influences the predicted behaviour of LAP and staff.
Behavioural attitude of LAP consists of their experience in woundcare and self-care as well as their
opinion about the importance of care. The experience of LAP in woundcare and self-care has an
influence on behavioural attitude because this experience modifies their perception on the necessity of
executing these tasks.
The concept of subjective norm has a large effect on the intention of LAP. The rules set by the
government, hospital policy and perception of human rights (e.g. disabilities) contributed to the
existing subjective norms.
The concept of perspective behaviour control is dependent of the needs and knowledge of LAP as well
as the current woundcare and self-care practice. The needs of LAP and nurses can be assessed by
evaluating their knowledge of leprosy, woundcare and self-care.
By studying the above mentioned concepts of the model, the intention of behaviour change may be
determined. Once people have the right intentions to change behaviour, it is easier to actually perform
the desired behaviour (Ajzen, 1991). After analysing the elements of this conceptual model planned
behaviour, the desired behaviour in woundcare and self-care can be explained.
Knowledge
‘Supplies’
Behaviour Intention
Behavioural attitude
Subjective norms
Perspective
behavioural control
M. van de Mortel ― VU University Amsterdam/ January 2015 6
Methods
Study setting
The research took place in a tertiary leprosy referral hospital in Pokhara, Western region of Nepal.
The International Nepal Fellow’s (INF) GPH&RC is the only known leprosy referral centre in Kaski
district. For over 50 years, INF and GPH&RC has been working with the government of Nepal to
reduce the incidence of leprosy in the Western region. GPH&RC provides rehabilitation services for
people with disabilities as result of leprosy. GPH&RC continues to provide medical support to leprosy
patients and strives to help LAP to have an independent and productive life in their own communities.
Each year approximately 8 to 10,000 out-patient visit the GPH&RC of which about 800 are admitted
(INF, n.d.). The hospital offers 48 beds for leprosy patients and for the self-care 15 beds are
available.
Study design and subjects
A quantitative and qualitative approach known as mixed method has been used to explore the
research aims. Triangulation of methods has been used to gain an overall and holistic picture of the
research and to validate findings (Verschuren & Doorewaard, 2010). The study subjects were LAP
from GPH&RC either admitted with ulcers or with an ulcer history. Literature review was performed in
order to acquire information about best practice woundcare in ulcers and this was compared with the
current woundcare protocol at GPH&RC. Following the interviews and focusgroup discussion (FGD) the
findings were discussed with two ulcer management experts.
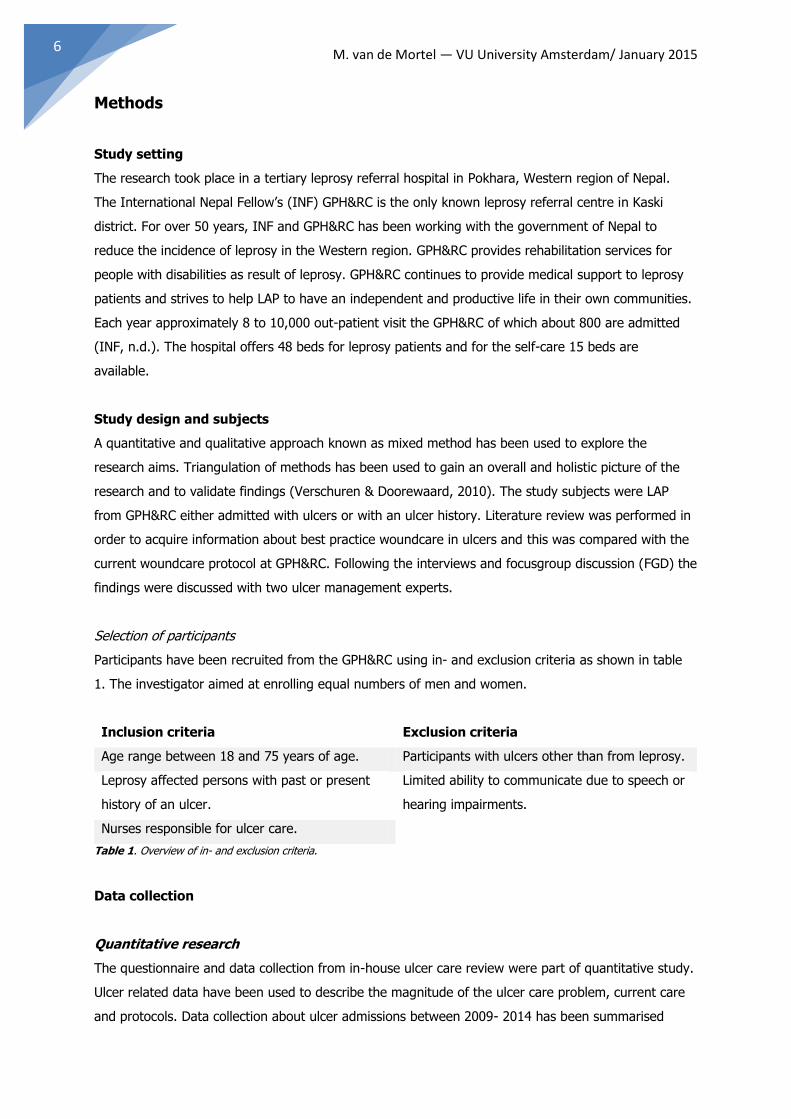
Selection of participants
Participants have been recruited from the GPH&RC using in- and exclusion criteria as shown in table
1. The investigator aimed at enrolling equal numbers of men and women.
Inclusion criteria Exclusion criteria
Age range between 18 and 75 years of age. Participants with ulcers other than from leprosy.
Leprosy affected persons with past or present
history of an ulcer.
Limited ability to communicate due to speech or
hearing impairments.
Nurses responsible for ulcer care.
Table 1. Overview of in- and exclusion criteria.
Data collection
Quantitative research
The questionnaire and data collection from in-house ulcer care review were part of quantitative study.
Ulcer related data have been used to describe the magnitude of the ulcer care problem, current care
and protocols. Data collection about ulcer admissions between 2009- 2014 has been summarised
Woundcare of pressure ulcers in leprosy 7
through reviewing annual reports to obtain an overview of the magnitude of the ulcer care problem.
This would show how many LAP were (re)admitted for ulcer care, whether there was a trend in
average healing time for ulcers, and a reduction of the frequency of new ulcers and severity.
Qualitative research
The knowledge and beliefs of LAP were researched in a qualitative study through FGD and semi-
structured interviews. The interviews with experts in ulcer management were also part of the
qualitative research.
Focus Group Discussions
FGD explores knowledge and experiences of participants (Lucassen & Olde Hartman, 2007). FGD were
applicable since the research aims are socially and culturally focused. In this case it was specifically
important to gather an understanding of the subjects’ perceptions about woundcare principles.
The FGD were selected by ‘purposeful sampling’ and homogeneity. The participants should have
something in common (Krueger and Casey, 2000), but with sufficient variation among participants in
age to allow for contrasting opinions. The purposeful sample were patients who have or had pressure
ulcers with an age range between 18 and 75 years, and nurses who perform woundcare. There were
two FGD’s, one each for LAP divided by gender and one for nurses to minimise bias and ‘false’ FGD
consensus. The three groups consisted of five or six participants each. At the start of the FGD, the aim
of the study was explained and verbal consent was obtained. The themes were risk factors, causes,
treatment, and prevention of ulcers.
Interviews
The interviews were semi-structured. The information acquired by the FGD was used for developing
the interview guide. Interviews can provide in-depth information related to participants experiences
and opinion on a particular topic. In total ten LAP were interviewed. These interviews were conducted
after a pilot interview had taken place. Accuracy of translation was checked by a healthcare
professional. The open ended interviews were conducted by the principal study investigator. At the
start of the interview, the aim of the study was explained in Nepali language. Interviews ranged from
45-60 minutes. The forms were kept by the researcher for confidentiality.
Two semi-structured interviews were conducted with experts in ulcer management. The first interview
was held at the self-care unit with DG, health educator with 26 years of working experience at
GPH&RC. The second interview was held with HC, podiatrist and woundcare specialist in leprosy, to
generate ideas regarding self-care and best practice in leprosy woundcare and for validation of
research results.
Translators
Two translators with an excellent understanding in English collaborated in this research. One
translator held a bachelor in public health and the other one is following a bachelor degree in Botany.
M. van de Mortel ― VU University Amsterdam/ January 2015 8
Prior to the FGD’s, the translators were educated in the research related topics and FGD methods. The
translators participated in the FGD as translator and note keeper. They also practised transcribing
data by doing a pilot interview. Moreover, they gathered questionnaires and interviews. Recordings
were translated from Nepali into English by the translators.
Data analysis
Quantitative data from questionnaires were analysed using SPSS Statistics version 21.0. Ulcer related
data were also used from previous conducted research and review of annual reports.
An open coding method for the transcripts of the FGD and interviews were used for the analyses of
qualitative data (Mason, 1996). Important information, views and experiences of the participants were
selected and labelled with keywords or concepts. Axial coding was followed, to make connections
between the different concepts. Conclusions of the FGD and interviews followed after axial coding,
which allows to provide answers to the research aims. Both interview and FGD were audio-taped and
transcribed verbatim. The transcriptions were read several times by the principal investigator. The codes
were reviewed and compared, in order to identify recurring patterns and emerging themes related to
woundcare practice. Codes and themes were reviewed by the co-investigator, and any discrepancies
were discussed and reconciled. Express Scribe and MAXQDA 10 and 11.0.9 were used for analysing the
qualitative data.
Ethical considerations
Verbal informed consent was asked prior to the FGD. Written informed consent was obtained from the
interviewees. Identities of all participants were coded and recorded anonymously. Ethics approval was
obtained from the Research Ethics Committee of the International Nepal Fellowship. Permission for
research was given by the Nepal Health Research Council. No incentives were offered to the participants.
Results
The ulcer problem - a six year review
Table 2 summarizes the review that has been performed on unpublished hospital documents (i.e.
hospital reports to ministry of health). A total of 576 participants were included in this in-house ulcer
care review. The table shows an average healing time for ulcers of 67 days in 2009 and 14 days in
2014. This is a reduction of 53 days in a six year period. The proportion of recurrent ulcers is 60% in
2009 against 24% in 2014. This is a decline of 36% in six years. Complication requiring surgery is
51% in 2009 while this percentage in 2014 is 12%. This is a reduction of 39%.
Woundcare of pressure ulcers in leprosy 9
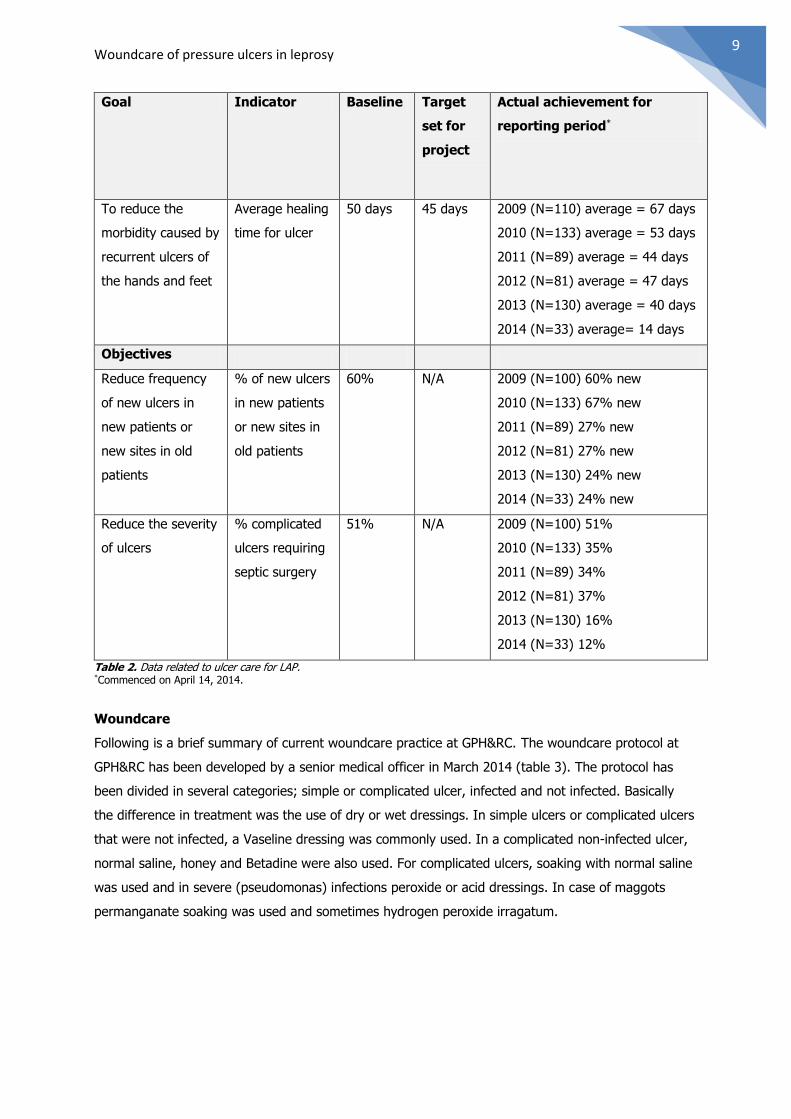
Goal Indicator Baseline Target
set for
project
Actual achievement for
reporting period*
To reduce the
morbidity caused by
recurrent ulcers of
the hands and feet
Average healing
time for ulcer
50 days 45 days 2009 (N=110) average = 67 days
2010 (N=133) average = 53 days
2011 (N=89) average = 44 days
2012 (N=81) average = 47 days
2013 (N=130) average = 40 days
2014 (N=33) average= 14 days
Objectives
Reduce frequency
of new ulcers in
new patients or
new sites in old
patients
% of new ulcers
in new patients
or new sites in
old patients
60% N/A 2009 (N=100) 60% new
2010 (N=133) 67% new
2011 (N=89) 27% new
2012 (N=81) 27% new
2013 (N=130) 24% new
2014 (N=33) 24% new
Reduce the severity
of ulcers
% complicated
ulcers requiring
septic surgery
51% N/A 2009 (N=100) 51%
2010 (N=133) 35%
2011 (N=89) 34%
2012 (N=81) 37%
2013 (N=130) 16%
2014 (N=33) 12%
Table 2. Data related to ulcer care for LAP. *Commenced on April 14, 2014.
Woundcare
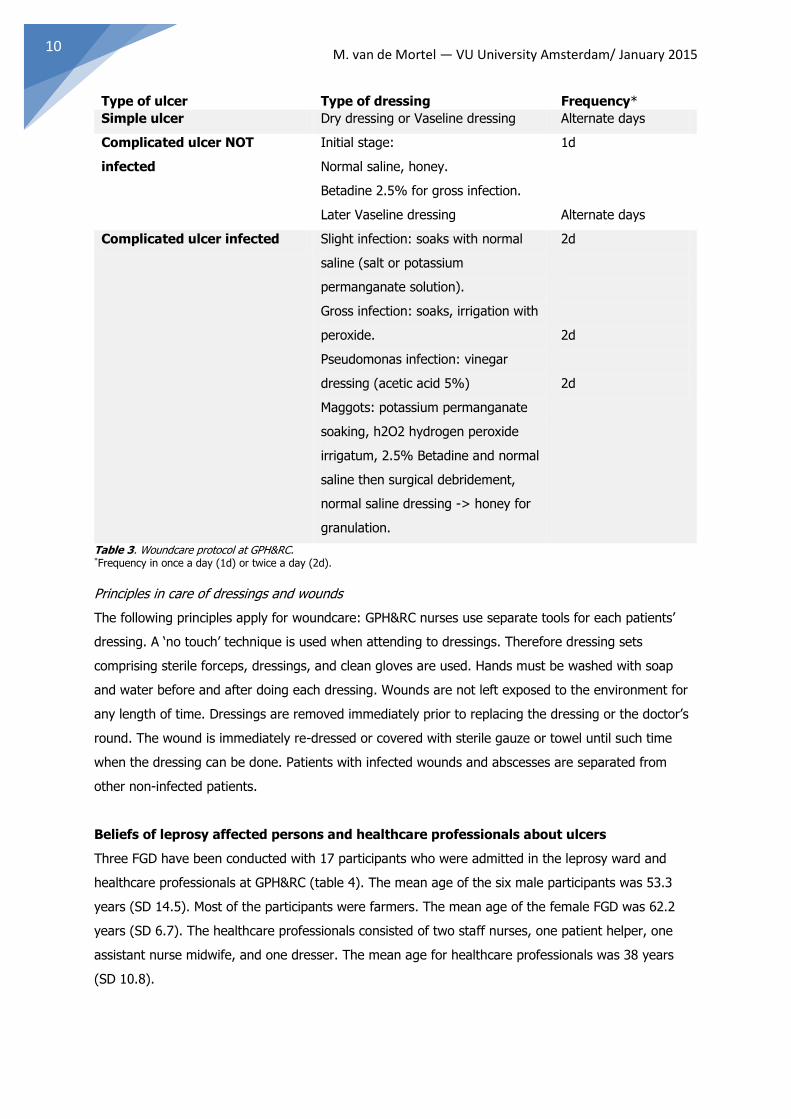
Following is a brief summary of current woundcare practice at GPH&RC. The woundcare protocol at
GPH&RC has been developed by a senior medical officer in March 2014 (table 3). The protocol has
been divided in several categories; simple or complicated ulcer, infected and not infected. Basically
the difference in treatment was the use of dry or wet dressings. In simple ulcers or complicated ulcers
that were not infected, a Vaseline dressing was commonly used. In a complicated non-infected ulcer,
normal saline, honey and Betadine were also used. For complicated ulcers, soaking with normal saline
was used and in severe (pseudomonas) infections peroxide or acid dressings. In case of maggots
permanganate soaking was used and sometimes hydrogen peroxide irragatum.
M. van de Mortel ― VU University Amsterdam/ January 2015 10
Type of ulcer Type of dressing Frequency*
Simple ulcer Dry dressing or Vaseline dressing Alternate days
Complicated ulcer NOT
infected
Initial stage:
Normal saline, honey.
Betadine 2.5% for gross infection.
Later Vaseline dressing
1d
Alternate days
Complicated ulcer infected Slight infection: soaks with normal
saline (salt or potassium
permanganate solution).
Gross infection: soaks, irrigation with
peroxide.
Pseudomonas infection: vinegar
dressing (acetic acid 5%)
Maggots: potassium permanganate
soaking, h2O2 hydrogen peroxide
irrigatum, 2.5% Betadine and normal
saline then surgical debridement,
normal saline dressing -> honey for
granulation.
2d
2d
2d
Table 3. Woundcare protocol at GPH&RC. *Frequency in once a day (1d) or twice a day (2d).
Principles in care of dressings and wounds
The following principles apply for woundcare: GPH&RC nurses use separate tools for each patients’
dressing. A ‘no touch’ technique is used when attending to dressings. Therefore dressing sets
comprising sterile forceps, dressings, and clean gloves are used. Hands must be washed with soap
and water before and after doing each dressing. Wounds are not left exposed to the environment for
any length of time. Dressings are removed immediately prior to replacing the dressing or the doctor’s
round. The wound is immediately re-dressed or covered with sterile gauze or towel until such time
when the dressing can be done. Patients with infected wounds and abscesses are separated from
other non-infected patients.
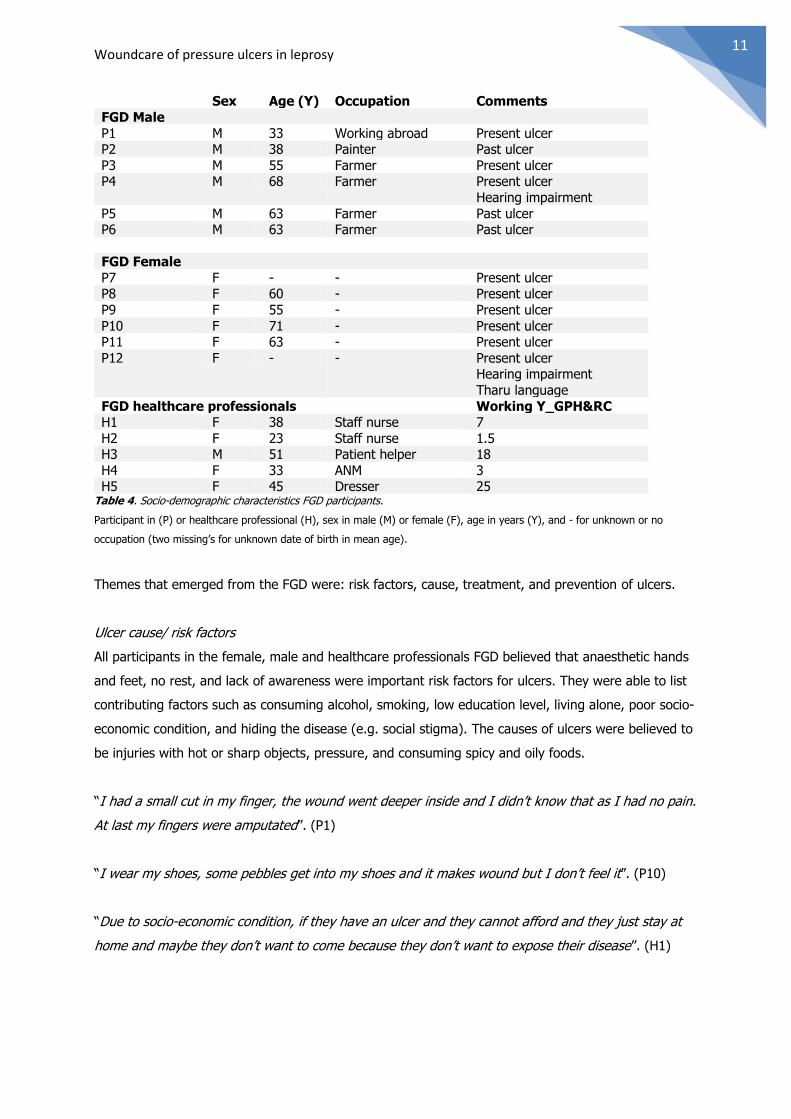
Beliefs of leprosy affected persons and healthcare professionals about ulcers
Three FGD have been conducted with 17 participants who were admitted in the leprosy ward and
healthcare professionals at GPH&RC (table 4). The mean age of the six male participants was 53.3
years (SD 14.5). Most of the participants were farmers. The mean age of the female FGD was 62.2
years (SD 6.7). The healthcare professionals consisted of two staff nurses, one patient helper, one
assistant nurse midwife, and one dresser. The mean age for healthcare professionals was 38 years
(SD 10.8).
Woundcare of pressure ulcers in leprosy 11
Sex Age (Y) Occupation Comments
FGD Male
P1 M 33 Working abroad Present ulcer P2 M 38 Painter Past ulcer
P3 M 55 Farmer Present ulcer P4 M 68 Farmer Present ulcer
Hearing impairment
P5 M 63 Farmer Past ulcer P6 M 63 Farmer Past ulcer
FGD Female
P7 F - - Present ulcer P8 F 60 - Present ulcer
P9 F 55 - Present ulcer
P10 F 71 - Present ulcer P11 F 63 - Present ulcer
P12 F - - Present ulcer Hearing impairment
Tharu language
FGD healthcare professionals Working Y_GPH&RC H1 F 38 Staff nurse 7
H2 F 23 Staff nurse 1.5 H3 M 51 Patient helper 18
H4 F 33 ANM 3 H5 F 45 Dresser 25
Table 4. Socio-demographic characteristics FGD participants.
Participant in (P) or healthcare professional (H), sex in male (M) or female (F), age in years (Y), and - for unknown or no
occupation (two missing’s for unknown date of birth in mean age).
Themes that emerged from the FGD were: risk factors, cause, treatment, and prevention of ulcers.
Ulcer cause/ risk factors
All participants in the female, male and healthcare professionals FGD believed that anaesthetic hands
and feet, no rest, and lack of awareness were important risk factors for ulcers. They were able to list
contributing factors such as consuming alcohol, smoking, low education level, living alone, poor socio-
economic condition, and hiding the disease (e.g. social stigma). The causes of ulcers were believed to
be injuries with hot or sharp objects, pressure, and consuming spicy and oily foods.
“I had a small cut in my finger, the wound went deeper inside and I didn’t know that as I had no pain.
At last my fingers were amputated”. (P1)
“I wear my shoes, some pebbles get into my shoes and it makes wound but I don’t feel it”. (P10)
“Due to socio-economic condition, if they have an ulcer and they cannot afford and they just stay at
home and maybe they don’t want to come because they don’t want to expose their disease”. (H1)
M. van de Mortel ― VU University Amsterdam/ January 2015 12
“Hands are feet become anaesthetic, they don’t use appropriate shoes but plastic slippers from the
market that get heated fast and can cause blisters”. (H5)
Treatment
All participants in the FGD mentioned several aspects of woundcare. The answers varied from
antibiotics, dressings (e.g. honey, normal saline, Betadine, Vaseline, hydrogen peroxide, camphor),
and tools (e.g. scissor, sponge, gauze). An operation was mentioned for complicated ulcers.
The male and female FGD included self-care management (e.g. wearing socks and shoes, taking rest,
healthy food, regular soaking, scrubbing, and oiling) as treatment.
“I get pressure on the wound during sleeping. The nurses put a sponge around the ankle to relief
pressure so that the wound can heal”. (P10)
“First soaking their hands and feet in Potassium Permanganate and ask them to scrub after that we
do dressings”. Most of the time we do normal saline dressing because it helps in granulation and
tissue recovery”. (H1)
Prevention
Participants in the FGD believed that prevention actions were related to self-care management such as
rest, soaking, oiling, skin inspection, personal hygiene, safety precautions when handling hot/ sharp
objects, not walking bare footed and/ or for a long distance, sun protection, balanced bodyweight,
and eating iron containing and nutritious food (e.g. protein).
“We can soak our feet every day and using oil afterwards”. (P1)
“The preventive methods taught by the doctor are not walking for a long distance and taking rest”.
(P11)
“It’s according to the condition of the wound, but the first thing is the rest”. (H1)
“Checking hands and legs every day, to see if there are blisters or wounds or thorns after getting back
from work”. (H5)
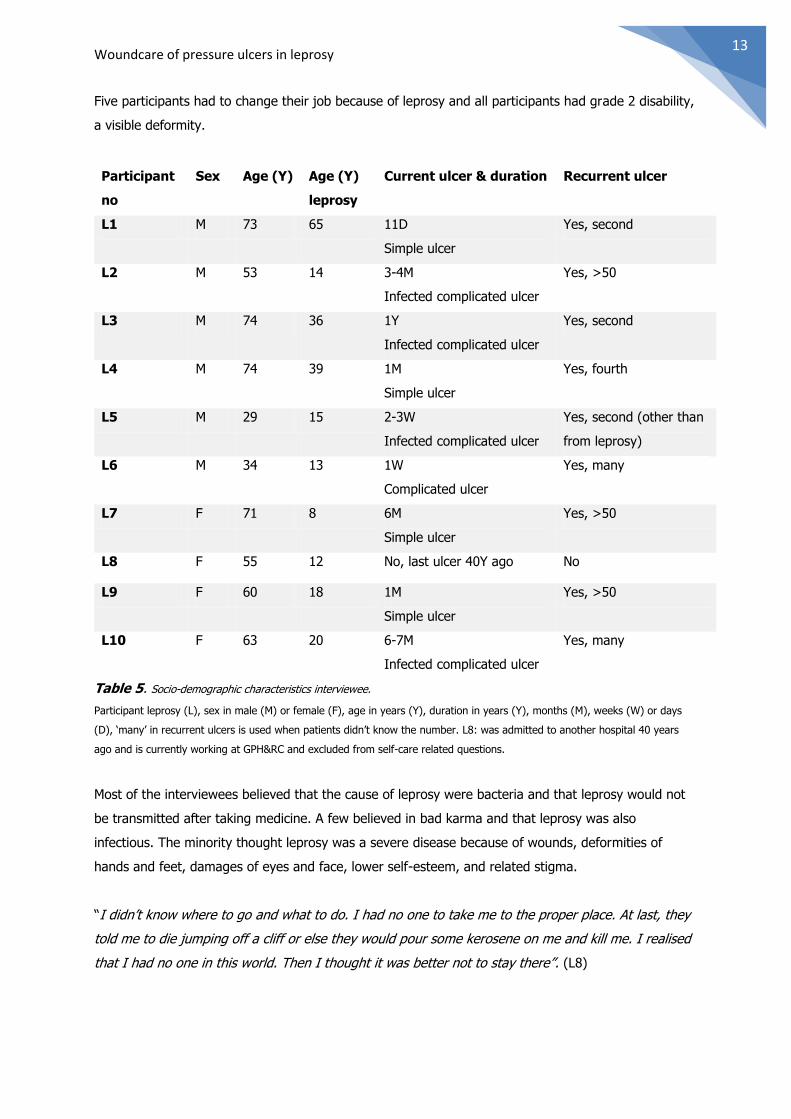
Beliefs of leprosy affected persons about leprosy
Ten leprosy affected persons have been interviewed. The mean age of the leprosy interview group
was 58.6 years (SD 16.2), and mean age at diagnosis was 24 years (SD 17.6) (table 5). All participant
were released from treatment and one participant has never had an ulcer. Six participants were living
in villages and four in the city. Seven participants were literate. In none of the subjects was the family
or a close relationship affected. Four of the subjects had somebody in the neighbourhood affected.
Woundcare of pressure ulcers in leprosy 13
Five participants had to change their job because of leprosy and all participants had grade 2 disability,
a visible deformity.
Participant
no
Sex Age (Y) Age (Y)
leprosy
Current ulcer & duration Recurrent ulcer
L1 M 73 65 11D
Simple ulcer
Yes, second
L2 M 53 14 3-4M
Infected complicated ulcer
Yes, >50
L3 M 74 36 1Y
Infected complicated ulcer
Yes, second
L4 M 74 39 1M
Simple ulcer
Yes, fourth
L5 M 29 15 2-3W
Infected complicated ulcer
Yes, second (other than
from leprosy)
L6 M 34 13 1W
Complicated ulcer
Yes, many
L7 F 71 8 6M
Simple ulcer
Yes, >50
L8 F 55 12 No, last ulcer 40Y ago No
L9 F 60 18 1M
Simple ulcer
Yes, >50
L10 F 63 20 6-7M
Infected complicated ulcer
Yes, many
Table 5. Socio-demographic characteristics interviewee.
Participant leprosy (L), sex in male (M) or female (F), age in years (Y), duration in years (Y), months (M), weeks (W) or days
(D), ‘many’ in recurrent ulcers is used when patients didn’t know the number. L8: was admitted to another hospital 40 years
ago and is currently working at GPH&RC and excluded from self-care related questions.
Most of the interviewees believed that the cause of leprosy were bacteria and that leprosy would not
be transmitted after taking medicine. A few believed in bad karma and that leprosy was also
infectious. The minority thought leprosy was a severe disease because of wounds, deformities of
hands and feet, damages of eyes and face, lower self-esteem, and related stigma.
“I didn’t know where to go and what to do. I had no one to take me to the proper place. At last, they
told me to die jumping off a cliff or else they would pour some kerosene on me and kill me. I realised
that I had no one in this world. Then I thought it was better not to stay there”. (L8)
M. van de Mortel ― VU University Amsterdam/ January 2015 14
Most of the participants used to think that leprosy was a severe disease, but nowadays with medicine
it is like a normal disease. They believed in the regulations set by the government to control leprosy
and the free provision of medicine.
Everybody was aware of the common signs and symptoms of the disease. However, many were still
concerned about the (re)occurrence of ulcers because of personal experiences with amputations and
recurrent wounds.
Practice of self-care
All the FGD participants were aware of the existence of the self-care unit. Several male participants
had been advised to attend the self-care training.
Many of the interviewed LAP did go to the self-care unit. The participants learned at the self-care unit
how to recognise ‘hot spots’, indicating a pending skin break-down, and how to prevent injuries from
unsafe cooking. Many of the participants had previously not received any guidance in basic woundcare
and the need for resting a foot ulcer. Self-care attendees were taught how to work safely in the field,
inspect their feet, not to walk barefooted, and about general cleanliness. Few patients only had
received home follow-ups.
The main reasons for readmission at the self-care unit were re-ulceration. Few LAP were able to
continue with soaking, scrubbing and oiling at home, some indicated that they could not rest because
of housekeeping duties. Many LAP found it hard to believe that ulcers could be prevented.
“If we have lots of money then only we can rest and eat”. (L3)
“No matter how much I follow the things I learned. I really try hard to prevent wounds, but I still get
them”. (L10)
Most of the participants were able to follow what was learned and found self-care training beneficial
for ulcer care and prevention.
“I can teach the things learned to other new patients”. (L5)
A few participants told it was difficult to follow self-care training due to economic problems or non-
availability of material to treat wounds (e.g. scissors, blades, and bowls for soaking). Most patients
accepted current treatment but would like to have treatment opportunities near their home or
financial support to visit the hospital.
Two interviews have been conducted with experts in self-care and woundcare practice. The GPH&RC
interviewee showed that the self-care unit used a register of patients with name, age, record number,
address, district, learning contents, discharge dates, and readmissions, if applicable. Patients who
Woundcare of pressure ulcers in leprosy 15
were referred from the hospital or OPD to, or admitted to the self-care unit were patients with healed
ulcers and new leprosy cases with a simple ulcer and neuritis. At times other patients than for self-
care were admitted which defeats the purpose of the self-care unit. Patients with a severe ulcer
received hospital based bed side education. The medical doctors refer patients to the self-care unit.
There were 15 beds for male and female patients. The self-care educational program is two weeks but
has recently been reduced to one week to lower the costs.
“One week is not enough. Some talented young people can capture the things they learn here, but for
the illiterate, elderly people, it’s really hard to capture in a week time. Because, they need two or
three days to adjust in the environment here. Then, in the remaining two or three days learning about
self-care. Because of our financial problems, we had to reduce the days”. (DG)
The content of the self-care program consists of a pre-test to test knowledge and this is repeated
before discharge. The day program at the self-care unit during the morning session: soaking,
trimming, oiling, gauze bandaging, eye, hand and foot exercise, and theoretical teaching. In the
afternoon practical teaching such as safety in cooking, gardening, and brick making as an income
generating project are taught. The LAP at the self-care watch thrice a week a self-care video program
about leprosy and other videos about, HIV, TB, diabetes, and nutrition as health education. The
patients are encouraged to share feelings and experiences together.
The health educator teaches about the risk factors (e.g. anaesthetic limbs) and trainees learned about
the cause of ulcers like fire, cracks, sharp objects, and unwanted skin pressures which can cause
ulceration. The LAP receive training about prevention of ulcers by avoiding fire, safe cooking, and the
daily rituals of soaking, trimming, and oiling. Patients who did manual labour learn that blisters easily
appear by pressure from handling working tools. Therefore, patients learn how to handle these tools
with padding in order to avoid ulcers.
This ‘primary prevention’ education is followed by a secondary prevention (e.g. when an ulcer is
formed). The ulcer treatment consists of three steps: cleaning, bandaging and resting. Further, self-
care ‘trainees’ learn how to prepare homemade medicine (e.g. honey, aloe vera, neem leaf, oil and
turmeric paste) as well as gauze bandage with re-used linen cloths by boiling it into salt water.
Patients learn that an ulcer will heal by itself when rested. Finally, the health educators or partnership
for rehabilitation (PFR) occasionally provided vocational income in own locality for some patients.
Reason to refuse admission to the self-care unit were loss of income when admitted and family
responsibilities. Patients with no indications for hospitalisation or admission to the self-care unit are
transferred back to their own health post. Overall, there is a decline in leprosy incidence which also
influences the admission rate.
GPH&RC has financial problems and therefore policy was changed to shorten the duration of
admission and no admission for simple ulcers, only for new cases. In conclusion, less patients were
referred to the self-care unit. Another problem occurs with the attitude of healthcare professionals.
Some patients are ‘scared’ of health professionals and this may lower self-esteem and compliance.
M. van de Mortel ― VU University Amsterdam/ January 2015 16
“The staff scold the patients in front of everyone saying why they get wounds again and again”. (DG)
Patients were discharged from the hospital and sent home instead of being admitted to the self-care
unit due to communication problems between healthcare professionals. While, patients could be
admitted for more intensive education and practical sessions to the self-care unit. Patients were not
motivated to go the self-care unit since they already had bed-site education and thought this was
enough. Patients received bed-site education because the health educator was afraid that patients
were discharged without knowledge of self-care. Patients should be encouraged by staff and be
motivated to go to the self-care unit.
“Few staff ever visit the self-care unit”. (DG)
The second expert-interviewee told that self-care was important because patients will then adopt
more responsibilities themselves. Self-care promotes that patients actually take responsibility of their
wounds and that they are observant about skin breakdown, and take quick action to address it. In the
last ten years self-care has generally been accepted as the key approach for patients with ulcers. In
prevention it is necessary that patients understand the need for protected foot wear.
“Self-care is becoming mainstream and that is different from before. I have seen very good results
and good published results in self-care”. (HC)
Observations in woundcare
The basic principle for healing is rest – ‘home-made’ dressings can be applied. Recently developed
wound dressing materials are costly and not suitable in low resource settings. The main important
principle in treatment is pressure relief and keeping wounds clean and secluded from the ‘problem’
environment to prevent infection.
“We can actually get very good results with principle based healing. If you just assist the body to do
what it can do very well. Any ulcer will heal if you rest it, no ulcer will heal if you don't”. (HC)
HC explained that treatment to some extent also depends on the wound stage. Hydro-colloid
dressings are used in granulating wounds but this is often not sustainable because it is too expensive.
Some natural products can be useful because it is locally available, but patients do not value it.
Patients prefer manufactured products more than natural products. Honey is a good healing agent, it
enhances re-granulation and stimulates epithelisation, but is not used widely. HC is not in favour of
Betadine because it delays healing. The use of Vaseline would maintain skin suppleness. The Unna
ointment appears to be useful and is widely used since it is easy to make and could be applied to
wounds, according to HC. A major issue is insufficient education and teaching of patients. However, it
is often much more difficult to educate and teach healthcare professionals. Healthcare professionals
Woundcare of pressure ulcers in leprosy 17
provide care, incl. ‘education’, and are often not aware of the positive influence they can have in
educating of patients.
Healthcare professionals want to apply colorful medication on the wound because it looks like magic.
Patients are misled because they are not aware that it is not the colour of drugs or soaking in
‘coloured’ water that facilitates wound healing but rest and minimising pressure – education rather
than drugs.
“If you ask the nurses to apply normal saline simple water, there's no magic in it and they don't like
it”. (HC)
Discussion
The improvements in healing time for ulcers, the reduction of new ulcers occurrence and the decrease
of complicated ulcers were not the result of major changes in admission criteria or changed treatment
regimens, but is instead due to the overall improved access to medical care, earlier reporting time
with an ulcer, and more effective self-care. However, reliable data of time between first development
of an ulcer and reporting for treatment is missing which determines size of ulcer and thereby
influences rate of healing.
The original goal of the hospitals ulcer treatment policy was to decrease the recurrence of treated
ulcers. But thereafter, the reduction of the apparition of new ulcers (in new patients or in new sites on
old patients) was considered to be more important.
The current study was limited by data from hospitalised patients because the size of the ulcers was
not recorded in the hospital records. It is reasonable to assume that smaller, uncomplicated ulcers
need shorter admission time than larger ulcers. Still, ulcers have a minimum healing time. Smaller
ulcers can explain the reduction in admission time and the need of surgery. Smaller ulcers are most
likely the result of education and a better understanding of how ulcers can be healed.
One of the aims of the study was to find out to what extent self-care and woundcare is practiced in a
low resource country conform recommended global practice compared to local available protocol.
Observation of ulcer care practice and study of the protocol reveals that there is a difference in actual
and recommended practice. This is mainly seen in the lack of use of Eusol (e.g. sodium hypochlorite)
and magnesium sulphate glycerin acriflavin dressings as prescribed in the woundcare protocol. In
practice turpentine is used instead of potassium permanganate and hydrogen peroxide irrigatum.
Vaseline, normal saline, and Betadine is also used widely. HC states that Betadine causes delay in
wound healing and therefore is not recommended for a long period but should only be used as
surface disinfectants. His opinion differs from a study by Goldenheim (1993), where he describes no
delay in wound healing, even when gel-type occlusive dressings are used to cover the wounds.

M. van de Mortel ― VU University Amsterdam/ January 2015 18
Moreover, bandage time is shortened in those patients treated with PVP-I ointment (e.g. Betadine
preparations).
The mainstay of ulcer treatment is the control of oedema by experienced personnel, especially in
neuropathic ulcers as well as application of compression therapy with caution (Mekkes, Loots, Van der
Wal, & Bos, 2003). The Unna Boot combination of medication (e.g. zinc oxide) and compression is
helpful in hastening the healing process (Cross, 2012). A study performed by Adler et al. (1997),
showed among subjects with neuropathy, compared with subjects without neuropathy, that they had
lower ankle-arm indexes, and were more likely to have a history of lower extremity oedema and ulcer.
It is recommended that arterial insufficiency is ruled out before applying a compression bandage,
especially when elastic bandages are used. This can be done by measuring the ankle–brachial
pressure index which should be more than 0,8 (Mekkes, Loots, Van der Wal, & Bos, 2003). Another
recommendation would be the use of honey as an approved effective dressing (Güneş & Eşer, 2007).
Honey properties have been reported to achieve a rapid rate of healing, a debriding effect, a rapid
clearance of bacteria and a reduced malodour from colonized and infected wounds. Honey will also
start the healing process in recalcitrant chronic wounds (Molan, 2001). Honey is easy to use and
allows patients to manage their own wounds at home, thus lowering nursing costs. Moreover, it
reduces costs of dressing materials, antibacterial agents, surgical debridement, and skin grafting
(Molan, 1999).
When considering admission of patients for ulcer care a ‘rule of thumb’ could be used. If the wound
does not meet the admission criteria when first reporting at the OPD, then the patient should not be
admitted. Hypergranulation needs to be treated with care; it is an indication of irritation in or on the
wound. Attempts should be made to address the cause of irritation before using interventions to treat
hypergranulation. Moreover, the in-house observations in woundcare suggests that the influence of
dressing nurses is high because of their daily contact with patient’s ulcer.
The study reveals that participants in FGD had a great understanding of causes, treatment and
prevention of pressure ulcers. A limitation of the FGD with the health professionals was the dominant
influence of one nurse which often led to agreed upon answers and opinions. Participants in the male
and female mentioned self-care as part of treatment and prevention whereas the healthcare
professionals only referred it in prevention. This is the only difference between the three FGD.
Participants in the FGD did not know the exact difference between the concept ‘risk factor’ and ‘cause’
because ‘anaesthetic’ was mentioned in both themes. Plantar ulceration is the cause of increased
pressure mostly over bony prominences, exacerbated by the loss of protective sensation or deformity
(Britton & Lockwood, 2004). FGD participants seemed to be able to list contributing factors to the risk
factors of an ulcer. The results of this study indicates that participants named the main causes of
pressure ulcers (e.g. thermal or mechanical) but were ignorant of warning signs such as redness and
or swelling. Beliefs of the participants agreed with findings of Kazen (1999) that ulcers should be
Woundcare of pressure ulcers in leprosy 19
treated with rest because ulcers in leprosy heal if they are protected from weight-bearing. This is
consistent with a study by Cross (2012). He states that ulcers in leprosy are often the result of
moderate pressure or shearing stress that is applied repeatedly over a long period of time. In addition
to pressure-ulceration, the protective response to minor trauma and pain, is lacking because nerve
impairment is limited in leprosy which may lead to lack of awareness in skin break-down (no pain) and
hence (re)ulceration.
Good footwear is important to reduce plantar pressures in neuropathic feet and attention to proper
foot-wear is crucial. Research by Britton and Lockwood (2004), emphasises the need of protective
footwear in anaesthetic feet, but special shoes are difficult to produce and often contribute to stigma.
Although participants are aware of foot care principles and wearing protective footwear, they often
seem not able to perform care at home due to economic circumstances (e.g. work commitment).
The interviews revealed that most interviewees know the cause and treatment of leprosy and all
participants knew one or more symptoms. Only a few participants found leprosy a severe disease
which was surprising seeing their deformities. The interviews showed that participants had learned
how to prepare dressings, but did not follow-up on scrubbing, soaking and oiling at home because of
fear of social stigma, predisposing the foot to re-ulceration.
The interview with the experts shows that older patients with (re)current ulcers may have problems
remembering the importance of care principles. When resources are limited priority should always be
given to younger motivated patients with ulcers because of the ability to learn healthy life style. An
implication of these findings is that follow-up is needed at home for elderly patients. Moreover, PFR
goes every month into the field and the staff could easily follow-up on the patients who received self-
care training. The results in self-care showed a reduction in hand and foot ulcers when patients were
trained (Cross & Newcombe, 2001). This differs from other research by Benbow and Tamiru (2001),
who conducted a trial on the effect of self-help groups in the community in Ethiopia. The traditional
approach for the prevention and management of ulcers, the didactic, health education talk or lecture
which might or might not include a practical demonstration of soaking, oiling, scraping, wound
trimming and dressing, gives disappointing results. The dressing of wounds is time consuming for the
leprosy workers, who also express concern about the dependency of the people upon this service. The
trial by Benbow and Tamiru (2001) successfully established a number of self-help groups for LAP. The
main function of the groups was to encourage the members to take responsibility for ulcer
management. The number of wounds reduced most notably during the first six months of joining a
group. The group members reported a number of qualitative benefits, in particular improved self-
respect and dignity and increased participation in society (Benbow & Tamiru, 2001). Cross and
Newcombe (2001) confirm that ulcer prevention relies on skill or knowledge but impacts attitudes and
self-esteem. This is confirmed by HC who states that the personal conviction that self-care works, is
missing. The attitude ‘we can do it’ is needed, but LAP usually have a low self-esteem and self-control.
If healthcare professionals convince patients psychologically and emotionally to take control then self-

M. van de Mortel ― VU University Amsterdam/ January 2015 20
care will be effective. If patients believe in self-efficacy then self-care is sustainable. The study by
Cross and Newcombe (2001) states that an intense period of self-care training does appear to have a
positive effect in lower admission rates for (complicated) ulcer treatment and lowers costs as
consistent with this research. Studies of self-care showed a reduction in ulcers when patients are
trained (Britton & Lockwood, 2004). However, a ‘prevention mind set’ is needed to reduce the
recurrence and severity of ulcers.
Self-care groups have been established for a long time, some were 15 years old (e.g. Dhanusha,
Nepal). The main benefit of staying 15 years together was no recurrence in ulcer formation. There is
social control - the patients keep each other accountable. Furthermore, the leprosy control
department of the government of Nepal is encouraging the development of self-care groups. The
government tries to establish self-care groups in health posts and offers self-care groups RS 10,000
(±€82). But self-care groups do not get any further assistance. Self-care groups need some help,
advice, mentoring, and monitoring for all activities. Self-care groups can develop a micro-credit
system to make loans available. That may also keep the group together, but it needs to contain the
self-care for LAP to prevent ulcers.
The self-care training at other hospitals in Nepal in Lalgadh and Anandaban are hospital and
community based, GPH&RC is only hospital based. The self-care unit in Anandaban hospital was
visited during this research. LAP were admitted when they suffered from a superficial ulcer or
following treatment of a severe ulcer. Anandaban organised self-care groups in the field and takes
care of follow-up. Anandaban has approx. 220 admissions every year of which 50 are re-admissions in
the self-care unit. Compared to GPH&RC the number of admission is much higher which may be due
to a higher prevalence of ulcers. Research by Chen, DeVivo, and Jackson (2005) suggests the need
for information on factors that contribute to increasing pressure ulcer prevalence in the recent period.
This information may help to guide prevention efforts particularly for patients with risk factors.
Nevertheless, the likelihood that any given person with loss of protective sensation will get a pressure
ulcer varies widely (Krause & Broderick, 2004).
GPH&RC should develop a criteria list which states when patients should be admitted to the self-care
unit either directly from the OPD or following initial treatment at the hospital. Support for suitable
vocational or low scale income generating training is needed for financially poor patients. This will
increase patients’ independency, avoid readmission and may be cost-effective compared to
(re)admissions for treatment. But the funding for this operation may be a problem.
Limitations and strengths
A limitation of this study is the number of participants that could be interviewed or were part of a FGD
which limits generalisation of the findings. Much information was obtained from the clinical records,
but additional needed information could only be obtained through the FGD’s and interviews which may
have resulted in recall bias. Researchers from a Western culture have certain aspects of woundcare in
mind but the culture, physical environment are substantially different in Nepal and this may makes it

Woundcare of pressure ulcers in leprosy 21
difficult to interpret and appreciate beliefs about leprosy and woundcare. The FGD and interviews
were conducted by native speaking translators which could have influenced the validity of the results.
However, the translators had the same cultural background and made practical relevant
recommendations related to woundcare and self-care for GPH&RC.
Conclusion
This study has led to more knowledge about woundcare, self-care and beliefs in leprosy about
wounds, prevention and care. There was a reduction in average healing time, percentage of new
ulcers and complications in ulcers. Furthermore, the use of costly and high-tech bandages is not
applicable in low resource settings, basic wound healing principals should be applied. This study
concludes that leprosy affected persons have adequate knowledge about the disease and about
causes, treatment and prevention of ulcers. Early detection of leprosy and loss of protective sensation
are important in the prevention of ulceration. Self-care has shown to be very effective and reduces
readmissions and admission time. In conclusion, “prevention is better than cure”.
Recommendations
Woundcare
Enhance awareness of existence of woundcare protocol that needs updating because practice
does not follow protocol.
Encourage the use of available home-made basic dressings in wound healing.
Encourage use of honey and Unna ointment as evidence based effective dressing technique.
Use compression bandage as therapy and train nurses in these techniques.
Use the ankle/arm index as prognostic indicator of foot ulceration and healing time.
Consider pus culture in wound infection when an ulcer is not healing.
Earlier preparation for discharge should be applied for patients with simple ulcers.
Attempts should be made to address the cause of irritation of hypergranulation before
applying styptics.
Self-care
Footwear should be checked on ward rounds and a system needs to be in place for regular
provision and control of footwear.
Close relatives should receive health education to encourage support and compliance of
patients.
Content of health education sessions and printed material should include the main cause of
pressure ulcers and warning signs.
Compliance and self-advocacy of LAP needs to be strengthened and stimulated by healthcare
professionals.
Development of a clear criteria list/ referral system for admission to the self-care unit.

M. van de Mortel ― VU University Amsterdam/ January 2015 22
Support of suitable vocation or low scale income generating as part of the self-care program.
Establishment of self-care groups in the community (note: self-care groups are only feasible
when LAP live close to each other).
Follow-up at home (through coordination with PFR) of leprosy affected persons.
Further research should try to include all regions or hospitals in Nepal. A national study in the leprosy
field may lead to the formulation of a national health policy and recommendations on agreed protocols
and guidelines. Usefulness of natural products (e.g. papaya because of the protein components which
breaks down sloppy tissue and works as a debriding agent) needs to be also undertaken due to their
easy availability and cheapness in low research countries. Research is further needed on factors that
contribute to the increase of pressure ulcer prevalence in a short period. Other approaches such as a
randomised control study might be able to distinguish different kind of wound materials in several
stages of wound healing.
Acknowledgments
The author expresses gratitude to the staff of the Green Pastures Hospital and Rehabilitation Centre,
Pokhara. Special thanks to Dr Paul Roche, Mr Isaac Gurung, Ms Deepa Parajuli, Dr Ruth Russell, Ms
Peggy Franks, Dr Biswa Mohan Bhattarai, Mr Dhanu Giri, Dr Jas Gurung, Dr Kamal Nepali, Mrs Laati
Laxmi, Mrs Mahima Bhattarai, Mr Balaram Bhandari. VU-supervisor Dr Wim Brandsma and the
Netherlands Leprosy Relief.
References
Adler, A.I., Boyko, E.J., Ahroni, J.H., Stensel, V., Forsberg, R.C., Smith, D.G. (1997). Risk Factors for
Diabetic Peripheral Sensory Neuropathy. Diabetes care, 20(7), 1162-1167.
Benbow, C., & Tamiru, T. (2001). The experience of self-care groups with people affected by leprosy:
ALERT, Ethiopia. Leprosy review, 72, 311-321.
Britton, W.J., & Lockwood, D.N.J. (2004). Leprosy. Lancet, 363, 1209–19.
Chen, Y., DeVivo, M.J., & Jackson, A.B. (2005). Pressure Ulcer Prevalence in People with Spinal Cord
Injury: Age-Period-Duration Effects. Archives of physical medicine and rehabilitation, 86(6), 1208-
1213.
Cross, H. (2012). Woundcare for people affected by leprosy: A guide for low resource situations.
International Federation of Anti-Leprosy Association (ILEP).
Woundcare of pressure ulcers in leprosy 23
Cross, H., & Newcombe, L. (2001). An intensive self-care training programme reduces admissions for
the treatment of plantar ulcers. Leprosy Review, 72, 276-284.
Garber, S.L., & Rintale, D.H. (2003). Pressure ulcers in veterans with spinal cord injury: A
retrospective study. Journal of Rehabilitation Research and Development, 40(5), 433-442.
Goldenheim, P.D. (1993). An appraisal of povidone-iodine and wound healing. Post graduate medicine
journal, 69(3), 97-105.
Güneş, Y., & Eşer, U. (2007). Effectiveness of a Honey Dressing for Healing Pressure Ulcers. Journal
of Wound, Ostomy & Continence Nursing, 34(2), 184–190.
INF, (n.d.). Green Pastures Hospital & Rehabilitation Centre leaflet.
Kazen, R.O. (1999). Management of plantar ulcers in leprosy. Leprosy review, 70, 63–69.
Krause, J.S., & Broderick, L. (2004). Patterns of recurrent pressure ulcers after spinal cord injury:
identification of risk and protective factors 5 or more years after onset. Archives physical medicine and
rehabilitation, 85, 1257-64.
Krueger, R.A., & Casey, M.A. (2000). Focus Groups. A Practical Guide for Applied Research (3rd
Edition). Thousand Oaks, CA: Sage Publications.
Leprosy annual report (2012/13). Government of Nepal, Ministry of Health & Population, department
of Health Services. Leprosy Control Division, Teku, Kathmandu: Nepal.
Lockwood, D.N., & Saunderson, P.R. (2012). Nerve damage in leprosy: a continuing challenge to
scientists, clinicians and service providers. International Health, 4, 77– 85.
Lucassen, P.L.B.J., & Olde Hartman, T.C. (2007). Kwalitatief onderzoek. Houten: Bohn Stafleu van
Loghum.
Mason, J. (1996). Qualitative researching. Thousand oaks: Sage publication.
Mekkes, J.R., Loots, M.A.M., Van der Wal, A.C., & Bos, J.D. (2003). Causes, investigation and
treatment of leg ulceration. British Journal of Dermatology, 148, 388–401.
Molan, P.C. (2001). Potential of Honey in the Treatment of Wounds and Burns. American Journal of
Clinical Dermatology, 2(1), 13-19.
M. van de Mortel ― VU University Amsterdam/ January 2015 24
Molan, P.C. (1999). The role of honey in the management of wounds. Journal of wound care, 8(8),
415-418.
Montaño, D.E., & Kasprzyk, D. (2002). Chapter 4. The theory of reasoned action and planned
behaviour. In: Glanz, K., Rimer, B.K., Lewis, F.M. (2002). Health Behaviour and Health Education:
theory, research and practice, 3rd edition, John Wiley & Sons, Inc., 67-98.
Van Veen, N.H., Meima, A., & Richardus, J.H. (2006). The relationship between detection delay and
impairment in leprosy control: a comparison of patient cohorts from Bangladesh and Ethiopia. Leprosy
Review, 77, 356–65.
Verschuren, P., & Doorewaard, H. (2010). Designing a research project. The Hague: Eleven
international publishing.
WHO, (2012). Retrieved on February 2, 2014, from
http://www.searo.who.int/entity/leprosy/data/data2012/en/index.html
WHO, (2014). Retrieved on April 23, 2014, from
http://www.who.int/mediacentre/factsheets/fs101/en/





























