Embed Size (px)
Citation preview

Dental caries experience andprevalence of children afraid ofdental treatmentBedi R, Sutcliffe P, f)onnaii PT. Harrett N, McConnachie J: Dental earies experienceand prevalence of children afraiti of denial treatment. Communily Dent OralFpidemiol 1992: 20: 368 71.
Abstraet The aim of this study was to examine the clinical outcome with regardto dental caries of high self reported dental anxiety in a group of Seottish secondaryschoolchildren. 1103 children participated in the study, mean age 14 yr (sd 0.35 yr),and the prevalenee of high dental anxiety was 7.1% (95% CI--5.6%, 8.6%). Whenthese children were compared with their conlcinporaries their DMFT and all itscomponents were higher but only the mean MT reached statistical sigiiiricaiice afteradjusting for gender and social class. C^hildren wilh a high denial anxiely were 62'^more likely to have at least I missing tooth due to caries. In additi(-in this groupwhen compared to the rest of the study population, had a significantly lower meannumber of teeth fissure sealed and a lower proportion of ehildren wilh sealants. Nosimilar trend was obvious for ehildren who had a high general fear. The denlallyanxious more accurately perceived their treatment need and were more likely lo defer,cancel or not turn up for dental appointments.
Raman Bedi', Philip Sutcliffe\Peter Donnan^, Nicola Barrett' andJohn McConnachie^'Department of Preventive Dentistry. ^MedicalStatistics Unit. University of Edinburgh and'Community Dental services. Lothian HealthBoard, Edinburgh. UK
Key words: denlai anxiety: dentai caries;epidemioiogy
Mr. R. Bedi. Department of Chiidren's DentistryThe Denlai Schooi. University of BirminghamSt Chad's Queensway. Birmingham B4 6NNUnited Kingdoi-n
Accepted for publication 22 December 19gi
People with a high dental anxiety mayavoid visiting the dentisl or, when al-tending for dental treatment, display be-haviotiral problems (1,2). Presently thereis liltle iiifornialion on the prevalence oldental anxiety within the general popula-tion (3, 4). A telephone interview surveyof 105 American households showed thatI 1.1% of the respondenls reported a highdegree ofdental fear (5). This finding hasbeen confirmed by other surveys whichshow thai approximately 10 20% of Iheadull population have a high dental anxi-ety, and hold a belief that this fear devel-oped during their childhood (6-8). Flow-ever, lew studies exploring dental anxietyhave examined the effect that this vari-able iiiigbt have upon an individual'sdental health status (4. 9 12).
The British national children's dentalhealth survey completed in 1973 showedthat the proportion of children who weredentally anxious steadily increasedthrough the primary .school years andthen levelled off during the secondaryschool years to about 5f)"A, of the poptila-tion (13). Regular atteuders were theleast dentally anxious among the 5- andl4 + -yr-olds and allhough dental anxietyincreased with age, mothers rcpi-irted thaibehavioural problems in the deutal chairdecreased with age (13).
VI<;NI:.SA el al. (1990) claimed lo be thefirst lo evaluale the elTecl of denial fearon the oral health of children (12). Theyfound no dilTerence in dental caries acliv-ily belween the high- and low-fear Singa-porean 8 9-yr-oid primary schoolchil-dren, with lhe prevalenee of untreatedcaries being high in both grotips (12).ConiiN (1985) investigated a UnitedStates adult naval population and founda significant inerease in decayed surfacesamong lhe denlally anxious bul no differ-ences in filled or missing surfaces (II).However, a recent national British dentalhealth survey showed that adults whosaid fear was the most important barrierto allending Ihe denlist, when comparedto other adults, had fewer niliiigs but asimilar number of sound and decayedteeth (I).
The aim of this sludy was lo examinelhe denlai earies status of a group ofScottish secondary schoolchildren wilhhigh sclf-rcporlctl denial anxiely.
iVIethod and materiais
Sant/>le sclcclioti - The Lothian Fdiica-lion Atilhorily provideti a lisl of H sec-ondary .schools Ihal had been randomlyselected and stratified by social back-grotmd so as to be rcprcsciilalivc of the
Aulhorily's 51 secondary schoolsChildren in grade three were selected be-eause this was the oldest age group be-fore (hey embarked tipon work experi-ence aiitl so were nol likely lo be absentA letter was sent lo all the parents of theselected children outlining the aims andprocedures of the sUidy, and iiilbrinintrihcm thai if Ihey did nol wish theirchiklrcn U-i parlicipate, then Ihey were toinform the appropriate school admin-istrator.
'The qttcstiottnaire A self adminisleredstruetured c]uestionnaire (available onrequest from the senior author) was tised.The questionnaire had six seclions;personal/family background. dentalaiixicty/general fear, dental experienceand attendance, oral cleanliness habits,use of lluorides and lastly sugar con-sumplion.
Dental anxiely was measured on theCorah Dental Anxiely Scale (CDAS), awell eslablished index which measures re-actions on a f^wc p(-iinl scale of ascendinganxiety lo fotir differenl denial lrealmenlsituations (14-17).
In addition qucslii-iiis on perceplioii ofanxiely. fear of specific dental proeeduresand Ihc subjccls' dispi-isilioii towards fearill geueral was measured accc-irding to theGcer I'car Scale (Cil-\S) which records re-
Detital caries atiiotig detttally att.xiotis selioolcliildreti 369
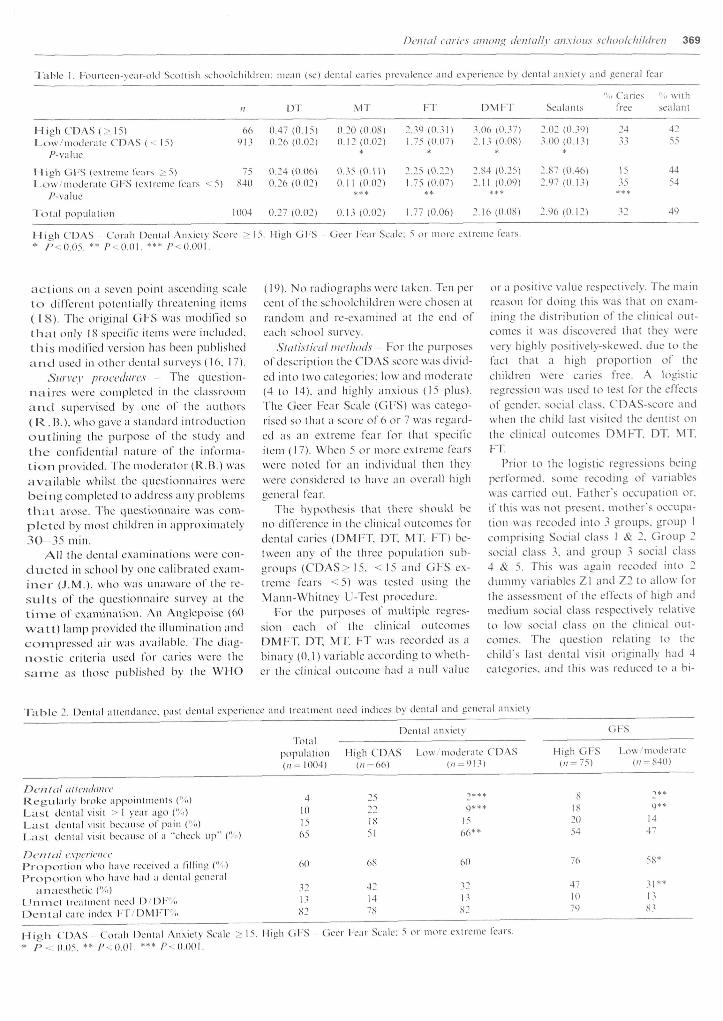
Table I, l-ourteen-year-old Scollish sehoolehililren: mean (.se) dental earies prevalence and experience by dental anxiety and general lear
"o Caries ".• wilhn n'V M'V If DMI-T Sealanls tree sealanl
66 0.47(0.15) 0.20(0.08) 2..?9 (O..^.l) .^06 (0..U) 2.02 (0..W)91.^ 0.26(0.02) 0.12(0.02) L75 (0.07) 2.I.MO.O8) 3.00(0.1.1)
High CDAS (> 15)Low/niodeiale C-DAS (•- 15)
/ ^ -va lue * * * *
H i a h G l - S ( e x t r e m e fem-s > 5) 75 0 , 2 4 ( 0 , 0 6 ) 0 , 3 5 ( 0 , 1 1 ) 2 , 2 5 ( 0 , 2 2 ) 2 , 8 4 ( 0 , 2 5 ) 2 . 8 7 ( 0 . 4 6 )
L o w ' / m o d e i - a t e G F S ( e x t r e m e fea r s < 5) 8 4 0 0 . 2 6 ( 0 . 0 2 ) 0 . 1 1 ( 0 , 0 2 ) 1 , 7 5 ( 0 , 0 7 ) 2 , 1 1 ( 0 , 0 9 ) 2 , 9 7 ( 0 , 1 3 )
/ ' - v a l u e
Tolal populalion 1004 0 . 2 7 ( 0 . 0 2 ) 0 . 1 . 1 ( 0 . 0 2 ) 1 . 7 7 ( 0 , 0 6 ) 2 , 1 6 ( 0 . 0 8 ) 2 . 9 6 ( 0 . 1 2 )
24
15
42
55
44
54
49
High CDAS Corah Dental AnxieiN Score > 15. Migh Gl-S deer l-ear Scale: 5 or more exlreme tears,* P-~^0.05. ** /'•--O.OI. *** /''.O.Ooi,
a c t i ons on a seven point ascending scalet o differenl potentially tlircalening ilcms( 1 8 ) . The original GFS was modified sot h a i only KS specific ilems were included,t h i s modified version has been publisheda n d used in olher dental surveys (16, 1 7).
Sttrycy procedures The question-naires were completed in (he classroomat-id supervised by one of (he authors(R.B.) , who gave a standard inlroduclionoutlining the purpose (-if the sludy andt h e confidential iialurc of lhe informa-t i o n provided. The modcralor (R.B.) wasavailable whilsl lhe questionnaires werebe ing conipleled to address any problemstha t arose. The questionnaire was com-ple ted by most children in approximalely3 0 - 3 5 min.
All the dental examinations were con-duc ted in school by one calibrated cxam-inei- (.LM.), who was unaware of llic rc-sult.s of lhe qucslioiiiiaire survey al thet i m e of examination. An Anglepoise ((-)0-v^'att) lamp provided the illtnninatioii andcompressed air was available. The diag-n o s t i c criteria tised lor caries were thesan-ic as llio.se published by lhe WHO
(19). No t-adiograplis were taken. Ten percent of (he schoolchildren were chosen atrandoiii and re-examined al llic end ofeach school stn-vcy.
Statistical methods 1-br the purposesof descriplion lhe CDAS score was divid-ed inlo two calegories: low and moderate(4 to 14), and highly anxious (15 plus).The Geer Fear Scale (GFS) was catego-rised so that a .score of 6 or 7 vxas regard-ed as an extreme fear for thai specifici(em (17). When 5 or more exlreme fearswere iioled for an individual llicn theywere considered lo have an (-iverall highgeneral fear.
The hypothesis that there should beno difference in (he clinical ou(comcs lordenial caries (DMFT, DT, MT. FT) be-tween any of the three population sub-groups (CDAS> 15, < 15 and GFS ex-lreme fears <5) was tested using llicMann-Whilncy U-Tcsl procedure.
1-br (he purposes of multiple regres-sion each of (lie clinical ou(comesDMFT, DT. MT, FT was recorded as abinary (0.1) variable according (o wheth-er (he clinicai outcome had a null value
or a positive value respectively. The mainreason for doing this was that on exam-ining the distribution of (he clinical out-comes it was discovered (ha( (hey were\cvy highly positively-skewed, due lo thefact that a high proportion of thechildren were caries free. A logisticregression was used to test for the effectsof gender, social class, CDAS-score andwhen lhe child iasl visited (he dentist onthe clinical outcomes DMFT, DT. MT.in.
Prior (o (he logistic regressions beingperformed, some recoding of variableswas carried ou(. Father's occupation or.if (his w-as no( present, mother's occupa-(ion was recodcd in(o 3 groups, group 1comprising Social class 1 & 2, Group 2social class 3, and group 3 social class4 & 5. This was again recoded into 2dummy variables Zl and Z2 to allow- forthe assessment of (he effects of high andmedium social class respectively relativeto low soeial class on the clinical out-comes. The question rclaling (o (hechild's last dental visit originally had 4calecories. and (his was reduced lo a bi-
Tablc 2. Dental atteiulatice. past denlai experienee and Ireatmeni need indices by dental and general anxieU
1-otalDental anxielv Cil-S
populalion High CDAS Low moderate CDAS913
High GFS Low moderate•" 840 )
E)c'ttttil iittettilatteeKeyiilarly broke appoinlments ("<.)L a s t denlai visil > I year ago ("o)La.sl dental visil beeau.se of pain ("u)La.st dental visit because ofa "eheck up" ('/o)
OctttttI c.\/)crii'tticPrdporllon who have reeeived a IHling ("̂ i)Proportion who have had a denial general
iinaeslhelic i%)L'nmcl lrealmenl need D/DI-'"liD e n t a l care index 1-l7f:)Ml-T%
4101565
60
1851
68
321382
421478
1566*
60
321382
8182054
1
y1447
76 58*
471079
311383
M I e h C D A S Cotah Denial Anxiely .Scale -- 15. High Gl-S C'leer l-ear Scale: 5 or more exlreme fears,
* P • 0.05. ** / ' - .0 , ( ) l , *** / ' - 0,001,
370 BRDI I: I AL.
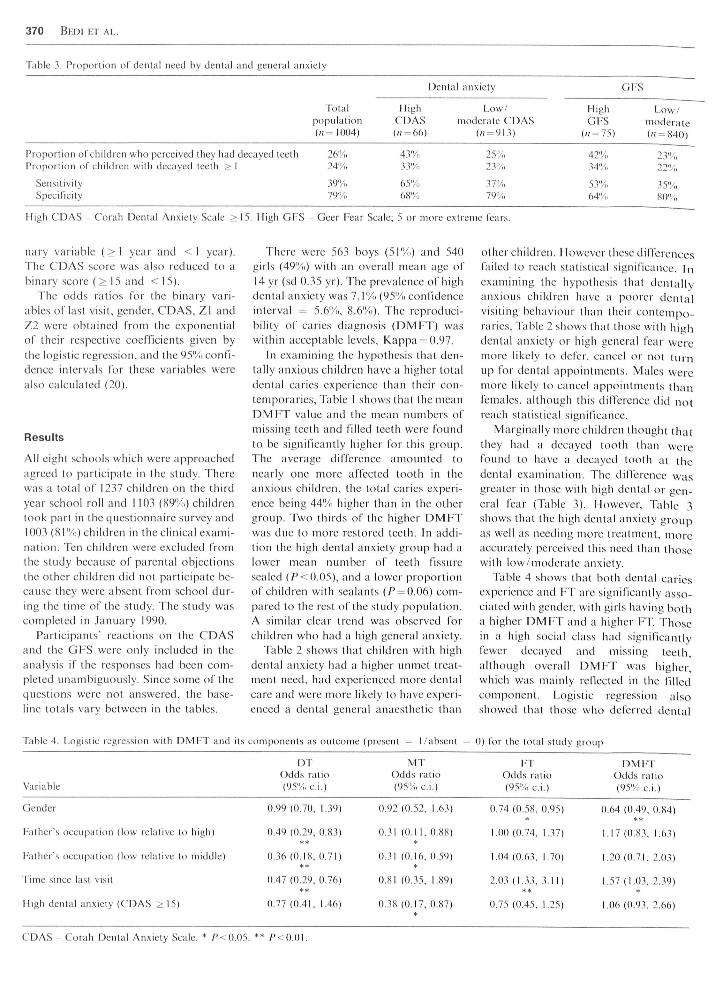
Table 3. Proporlion of denial need by dental and general anxiely
Denial anxiely
Tolal High Low/population CDAS moderate CDAS(/;=I004) (/( = 66) (/7
GI-'S
High Low/Gl-'S moderate
(;i = 75)
Proportion of children who perceived they had decayed leelh 26'>iiProportion of children wilh decayed teeth >1 24"A,
Sensitivity 39%Specincity 79%
43'y;.33%
65'yo6»"A,
25"A~23'/.,
37%79'V;,
34%
53%64"-;,
High CDAS Corah Denial Anxiely Scale > 15. High GFS Geer Fear Scale: 5 or more exlreme fears.
nary variable (>1 year and <1 year).The CDAS seore was also reduced [o abinary score ( > 15 and < 15).
Tbe odds ratios for tbe binary vari-ables of last visit, gender, CDAS, Zl andZ2 were obtained from the exponentialof Iheir respective coefficients given bythe logistie regression, and the 95'Xi confi-dence intervals for these variables wereal.so calculated (20).
Results
All eight schools which were approachedagreed to parlicipate in the study. Therewas a total of 1237 children on the thirdyear school roll and 1103 (89'^) childrentook part in the questionnaire survey and1003 (81"/,) children in (he clinical exami-nalion. Ten children were excluded fromihc sludy because of parental objections(he o(her children did iio( par(icipa(e be-cause they were absent from school dur-ing (he time of the study. The study wascompleted in January 1990.
Participants' reactions on the CDASand the GFS were only included in theanalysis if the resp(-)nses had been com-pleted unambiguously. Since some of thequestions were nc-it answered, the base-line totals vary between in the tables.
There were 563 b(-iys (51%) and 540girls (49%) with an overall mean age of14 yr (sd 0.35 yr). The prevalence of highdental anxiety was 7.^^ (95% confidenceinterval = 5.6%, 8.6'̂ !,). The reproduei-bility of caries diagnosis (DMFT) waswithin acceptable levels. Kappa = 0.97.
In examining the hypothesis thai den-tally anxious children have a higher lolaldenial caries experienee than (heir c(-in-(cmporaries. Table I shows (hat Ihc meanDMFT value and the tnean numbers ofmissing teeth and filled teeth were foundto be significantly higher for this group.The average dilTerence amounted tonearly one more affected loolh in theanxious children, the total earies experi-ence being 44'!/, higher Ihan in lhe olhergroup. Two thirds (-if the higher DMFTwas due to more restored teeth. In addi-tion the high dental anxiety group had alower mean number of teelh fissuresealed (/''<().O5), and a lower pr(-)por(ioiiof children wilh sealants (/•' = 0.06) com-pared to the rest of the study populalion.A similar clear trend was observed forchildren who had a high general anxiety.
Table 2 shows that children wilh highdental anxiety had a higher unmet treat-ment need, had experienced iiK-ire dentalcare and were more likely to have experi-enced a dental general anaesthetic than
olher children. However these differencesfailed (o reach slatistical significance. Inexamining lhe hypothesis ihal dentallyanxious ehildren have a poorer dentalvisiting behaviour than their contempo-raries. Table 2 sbows that those with highdenial anxiety or high general fear weremore likely (o defer, eaiicel or not turnup Ibr denial appointments. Males weremore likely lo cancel appoinlmenls thanfemales, although this difference did notreaeh statistieal significance.
Marginally more children lliouglii Ihatthey had a decayed loolh than wereIbuud (o have a decayed (oo(li a( thedental examination. The dilTerence wasgreater in those with high dental or gen-eral fear (Table 3). However. Table 3shows that the high dental anxiety grc-iupas well as needing more Irealment, moreaecurately perceived this need than (hosewith low/moderale anxiety.
Table 4 sbows that both denial cariesexperience and FV are significaiidy asso-ciated with gender, with girls having botha higher DMFT and a higher FT. Thosein a high social class had significantlyfewer decayed and missing teeth,allhotigh overall DMFT was higher,which was mainly renected in Ilie filledc(-inip(-inen(. Logistic regression als(-)showed Ihal Ihose who deferred denlai
Table 4. Logistic regression wilh DMI-T and its components as outcome (present = I/abseni = 0) for lhe tolal study group
Variable
DTOdds ratio(95'/, ci.)
MTOdds ratio(9.5'/, ci.)
0.92 (0.52. 1.63)
0.31 (0.11. 0.88)*
0,31 (0.16. 0,59)*
0.81 (0.35. 1.89)
0.38 (0,17. 0,87)
FTOdds ratii(95% ci.)
0.74 (0.58. 0.
1,00 (0,74, 1.
1.04 (0.63. 1,
2.03 (1.33, 3.**
0.7-'̂ (0.45, 1.
)
95)
37)
70)
11)
25)
DMFTOdds ralio(95'/, ci.)
0.64 (0.49. 0.84)
1,17 (0,83. 1.63)
1,20 (0.71. 2.03)
1,57 (1.03. 2..19)*
1,06 (0,93, 2,66)
Gender 0.99 (0.70, 1.39)
Father's occupa(ion (low relative (o high) 0,49 (0.29, 0,83)
l-'ather's occupation (low relative to middle) 0.36 (0,18, 0.71)
Time since lasl visit 0.47 (0,29. 0.76)
High dental anxiety (CDAS >15) 0.77 (0.41. 1.46)
CDAS Corah Dental Anxiety Scale. * P<().05. ** /'<O.OI.

Dctital earies aiiions; dentally anxious seltaolehildrcn 371
visits had higher DL and Uiwer FT andD M F T . However, it is clear that at (hisa y e children widi high denial anxiely donci\. have a significanlly lower prevalenceo f caries experience (i.e. percenlage wilhD M F T = O), bul only a higher MT, thant h a t for the rest of the population.
Discussion
It has been eslablished from a number ofstudies thai dentally anxious adulls avoiddental trealment vvliencver possible andprefer teeth lo be extracted rallier (liaiire.storcd. They are also mote likely (oh a v e decayed leelli present (6, 9, 1 1). Thiswould appear lo be the inevitable conse-quence of personal neglecl and avoidingdenta l care as the result of au anxielyt h a t is perceived to have been acquireddur ing childhood (5. 6).
The denial health of young primaiyschoolchildren with a high dental anxielyhiis been reported (o be iiol differenlIVom (ha( of other children (10, 12). Thiss t u d y of 14-yr-olds from Lothian hasshown ihal 7",, of the children had highden ta l anxiety, thai is. with scores of 15o r more on ihc Corah Denial AnxielySeale . The.se anxious children had a high-e r DML'T and lower mean numbers offissuie sealed teeth Ihan Iheir eontempo-lar ics .
The clinical oiilcoiiie associated withh i y h dental fear in Ihc 14-yr-olds was anaverage of nearly one more loolh wilh ahistory of carious attack. However, theaverage increa.se in permanent tooth ex-traet ion in lhe anxious children was onlyapproximately one Icnih of a tooth.Therefore, in this study population, highden t a l anxiety had not been associatedw i t h an irretrievable clinical outcome bulnegalive attitudes to dental heallli weteei-i-ierging. The children had a poor .selfimage , in Ihal they Ihotighl (ha( (hey hadn-i(-)rc decayed (eelh lliaii llicy acliiallyh a d . The last denial visil for denlallyanxious children was more likely lo bea s a result of pain and less likely to haveb e e n for a dental check-up only.
Tlic findings show thai dentally anx-i o u s children were iiK-ire likely lo haveh a d a tlcnlal general anacslhelic and weren-iorc likely (o have had a filling. The
la((er finding is surprising, one w-otildhave expected more carious teeth, sinceihcsc children were afraid and w-enl tothe denlisi less often than Ihc others.
The (-idds ratios analysis (Table 4)showed thai for dental anxiely lheDMFT (i.e. pereentage caries free) oddsratio is 1.06, so thai the overall DMFTis approximately equal in the two groups.Therefore there is no obvious relation-ship between dental anxiely and thosewh(-i arc earies free, and yet it is signi-ficanlly more likely thai those with a highdental anxiety have missing teeth (i.e.62",, more likely) relalive ((-> (he low/moderale gr(-iup.
In summary, this sltidy shows thaidenial anxiely is a barrier to dentalcare for a small proportion of the sec-ondary schoolchild population. Theclinical slalus of Ihc anxious childrenwas not markedly W(-)i-se than thai ofllic remaining children but llic anxiouschildren displayed certain negative atti-tudes (o dciKal heahh suggesting that(heir den(al health will continue to de-(eriorale dtiring adulthood. This studyalso indicates lhe same finding as therecent AduU Dental Health survey (ha(fear as a barrier to dental care may bemore associaled with (he (realmenl thatpeople receive than with llic diseaselevel they experienee (I).
Acknowlcdgcniettt 1 he pi-(-ijeet was funded bya grant from the Seottish Deparlment ofHome and Heallh. The aulhors wish to ihankfirst and foremost all the children and schoolswho participated in this projecl. withoiilwhose help Ihis sludy would nol have beenpossible. We are grateful to Mr .1 CRAIU (ChiefAdniinislralive Dental Officer). Mrs CWKUiiii (Senior Denlai Offieer) bolh from theFothian Heallh Hoard and Miss H MooKi(Research assislanO for their help and supporlthroughout lhe survey. We are also gralelullo Miss B WourciiMinu (Computing Officer.l'|-e\-enli\-e Dentislry) and the slalT of the Med-ical Slatislics Unit from the Lniversity ofFdinbiirgh for their help.
References
1. Tonu .IE. LAOIIR D. Adttit dctital ttealthI9SS United Kitigdont. London: HMSO.1991,
2. CoR.Mi NL. O'Slii A RM. Avi R. WA. Den-lisls' management of palienls' fear andanxielv. ./.-(b.-l 1985: //(), 734 6.
3, Ki.i:iMAN MB, Fear of dentists as an inhib-iting factor in children's use of denial ser-vices, ./ Detu Child 1982: 49: 209 13,
4, A-ihR WA, CoRAii NL. Behavioural fac-tors inllueneing dental treatnient. hi:Coin:N LK, BRYANT PS, eds. Social scien-ces and dentistry. Vol. 11, London: Quinte-ssenee. 1984: 267-322.
5, GAITHI:!, R.1. R(-)BERT.SON MC. lN(a;RSOi,iBD. WALKI:R C . BOWMAN L. The prev-alence of denial fear and avoidance: a re-eent survey sludy. .lADA 1983: 107:609 10. '
6, MiKiROM P, Fi.sFT L. Mi:i,NirK S.WHINSTHIN P. The prevalence and practicemanagemenl eonseqiienees of denial fearin a major LIS cily. .lADA 1988: 116:641 7,
7, DoMoro PK. WMNSTHIN P. Mi:iNirK S ctal. Resulls of a dental fear survey in .la-pan: iniplicalions for dental public heallhin Asia. Cotitniunity Dent Oral Epidetniol1988: 16: 199 201.
8, BI:R(-.(;RI:N Ll. MirVNrRi G. Dental fearand avoidanee: eauses. symploms. andcon.sequences. ./.4D.4 1984: /()9,-247 51.
9, HAI tSTROM T. HAI.LINC; A. Prevalence ofdenlislry ph(-ibia and its relation to miss-ing teeth, alveolar bone loss and dentalcare habits in an urban community sam-ple. Acta Psvchiatr Scatid 1984: 70:438 46,
10. WRKfllT F'AC. LU(AS JO. MCMURRAVNF. Dental anxiety in five to nine yearold children, ./ Paedodontics 1980: 4: 99-115.
11. CoHFN ME. Dental anxiely and DMFSstatus: association within a US navalpopulalion versus differences betv\-eengroups, Contttttinitv Detu Oral Epidetttiol1985: 13: 75 8.
12. ViGNi;nsA H. CHKI.LAI'PAH N K . MILC^ROMP, GOING R. T):O CS. A elinieal evaluationof high- and low-fear children in Singa-pore .V Dent Child 1990: .̂ 7,- 224-9.
13. Toni-) .IE. Children's dental heatth iti Eng-land and Wales 1973. London: HMSO.1975.
14. CoRAU NL, DevclopmenI ofa dental anx-iely scale, ./ Dent Res 1969: 4S: 596.
15. CoRAii NL. GALI: EN. \\\K, S.I, Assess-meni of a denial anxiely seale. .1.4 DA1978: 9': 816 9,
16. Bi-RGGRi-,N U, CARLSSON S G . Psvehomel-ric measures of dental fear. CottinttinityDent Otal Epidctniol 1984: 12: 319-24,
17. BI:RGGRI:N II. CARI.SSON SG. Usefulnessof two psychometric seales in Swedish pa-lients with se\-ei-e dental fear. ConuttunityDent Otal Epidemiol 1985: 13: 70 4.
18. CII;I:R .IH, The de\-elopment ofa scale tomea.sure fear, Beliav Res Therapy 1965: 3:45-53.
19. WoRin HEALrH ORGANIZATION. Oralhealth surveys, hasic tttcthods, 3rd edn. Ge-neva: WHO. 1988,
20. DixoN W.I. ed, B.MDP statisttcal softwatctttatttiiil. Los Angeles: I'niversily of Cali-loniia Press, 1988.








