Embed Size (px)
Citation preview
PLACENTA : TO REGARD OR DISCARD
DEPARTMENT OF ANATOMY
HIMSR
JAMIA HAMDARD, NEW DELHI – 110062
17TH MARCH, 2015
INTRODUCTION
PROF. RAJ D. MEHRA
INTRODUCTION
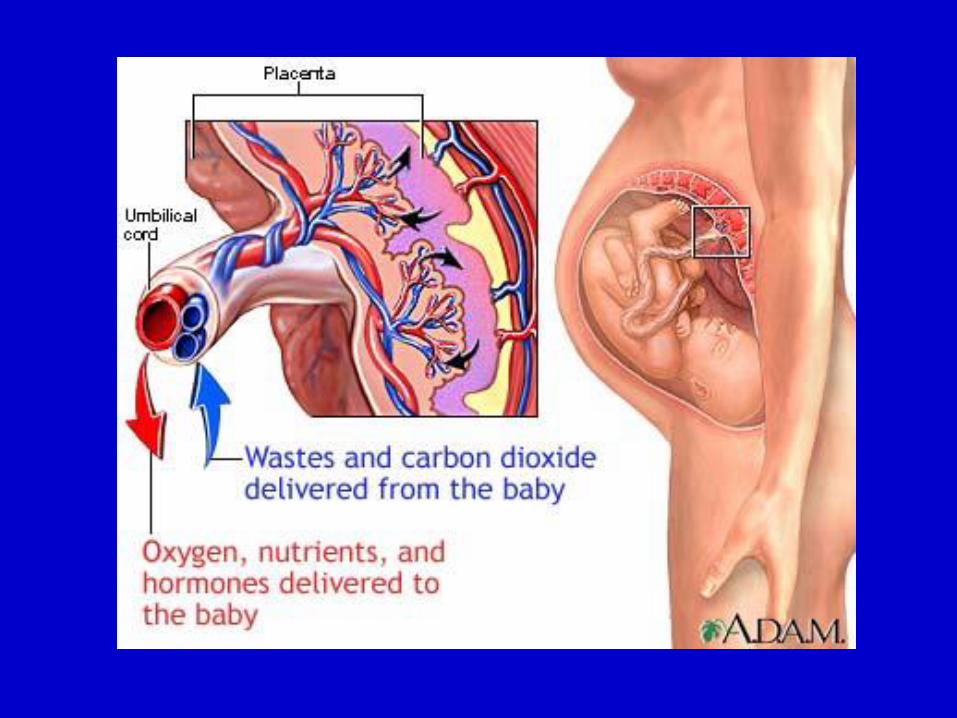
• Placenta, a fetomaternal organ that acts as acradle to the developing fetus, while alsoparticipating in fetomaternal tolerance, is aphenomenon that is fascinating, but yet notentirely understood.
• It is the least understood and arguably one of themore important human organs , not only for thehealth of a woman and her fetus duringpregnancy, but also for the lifelong health ofboth.
By increasing the understanding aboutplacenta and our ability to prevent and treatplacental abnormalities, we could improvenot only pregnancy outcome but also healthof the child and of the mother lifelong.
Further, placental function is important forlater health as poor fetal growth is associatedwith higher rates of chronic disease in adultlife.
INTRODUCTION (CONT)
• Placental structure and function affect the health of themother, as seen in the development of insulin resistanceand gestational hypertension, preeclampsia andeclampsia.
• Placental dysfunction affects the fetus, causingprematurity and fetal growth and neurodevelopmentalabnormalities.
• The concept of “placental origins of adult disease” stemsfrom studies where variations in placental developmentaffect the supply of nutrients to the fetus anddevelopment of systems linked to diseases of the adult.
PLACENTA : ABNORMALITIES
• Recent studies indicate that placenta should not be seen as a waste material, but in relation to its important role during pregnancy
• It should be regarded as a great gift from nature as a source of cells and bioactive molecules for therapeutic applications
• Placenta is considered as “the tree of life”, branches of which continue to extend from fetal development and beyond
• Indeed placenta may continue to sustain our life even outside of the womb.
HUMAN PLACENTA
ORGANIZATION OF THE CONTENTS• Introduction• Placental Structure and Development• Placental Anomalies• Clinical Case Correlations• Recent Developments in Placental Research For Healing/Placenta MedicineFor Rejuvenation/Skin CarePlacental MicrobiomePlacenta EncapsulationAs a rich source of Stem Cells
STRUCTURE & DEVELOPMENT OF PLACENTA
DR RANJANA VERMA
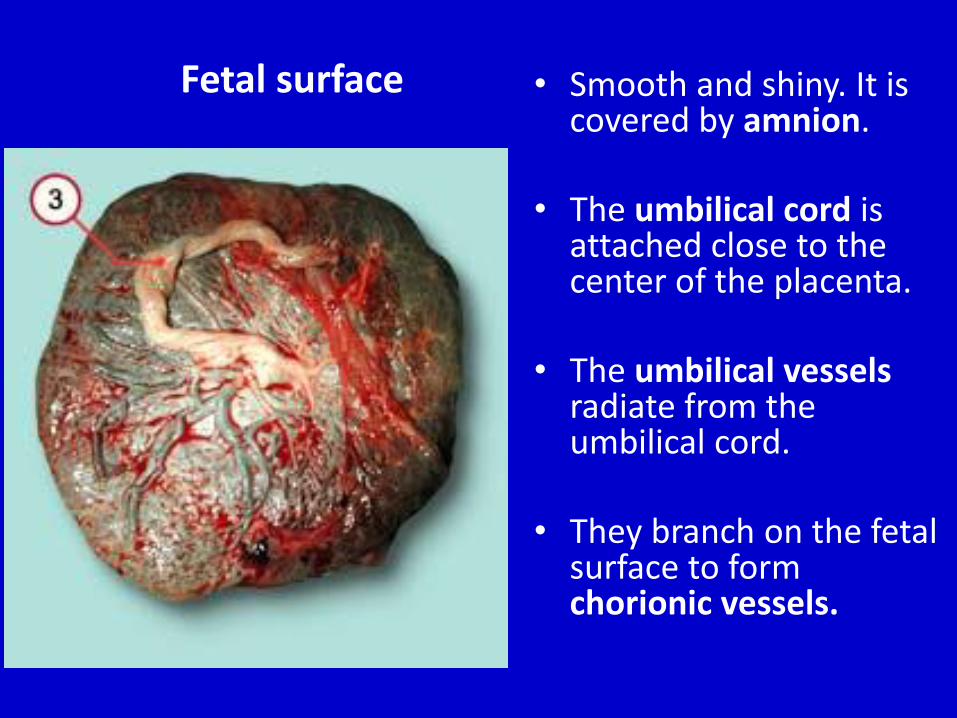
Fetal surface • Smooth and shiny. It is covered by amnion.
• The umbilical cord is attached close to the center of the placenta.
• The umbilical vesselsradiate from the umbilical cord.
• They branch on the fetal surface to form chorionic vessels.
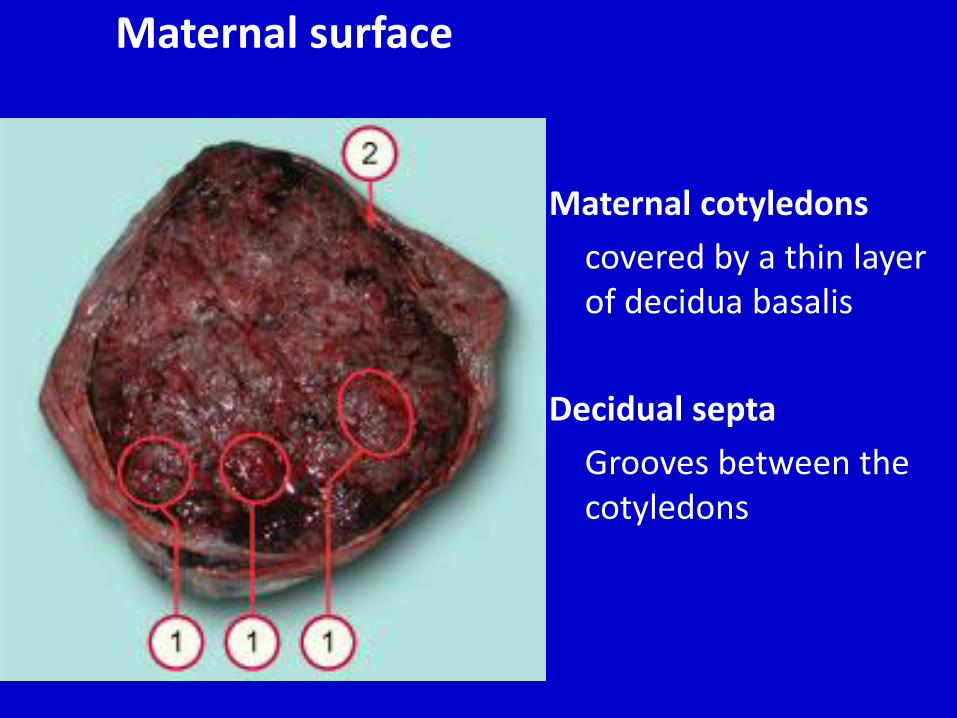
Maternal surface
Maternal cotyledons
covered by a thin layer of decidua basalis
Decidual septa
Grooves between the cotyledons
Characteristic Features of Human Placenta
• Labyrinthine
• Hemochorial
• Chorioallantoic
• Deciduate
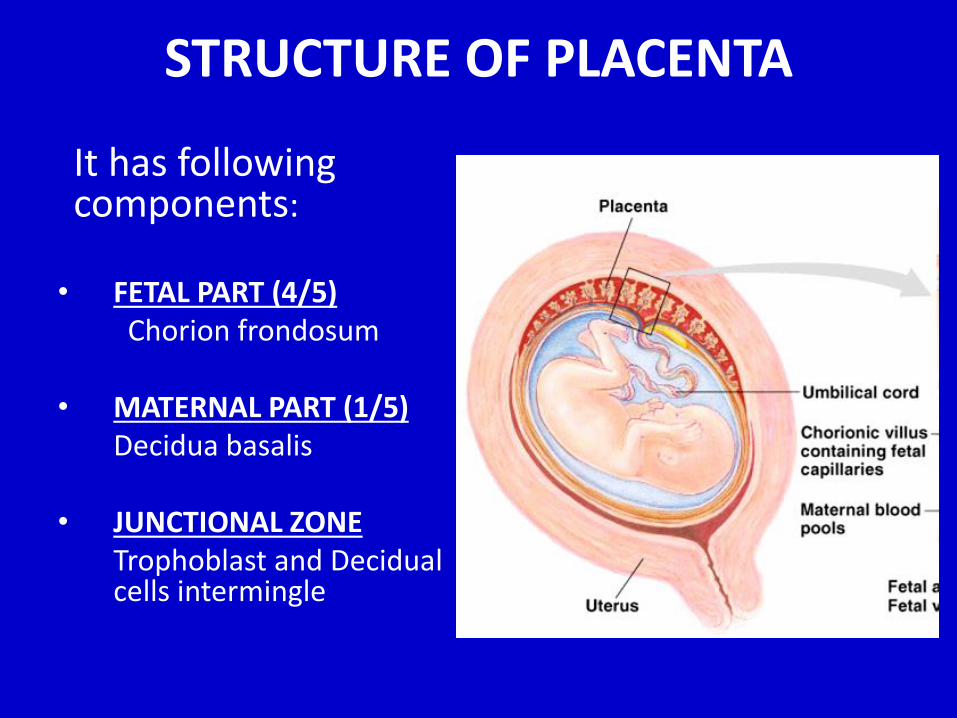
STRUCTURE OF PLACENTA
It has following components:
• FETAL PART (4/5) Chorion frondosum
• MATERNAL PART (1/5)Decidua basalis
• JUNCTIONAL ZONE Trophoblast and Decidual cells intermingle
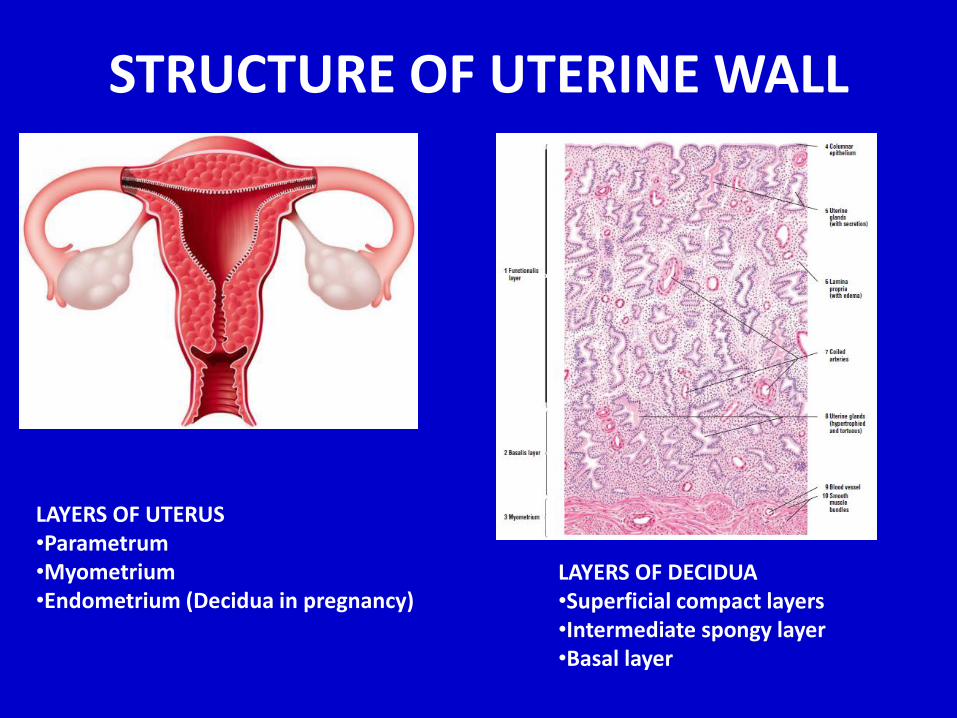
STRUCTURE OF UTERINE WALL
LAYERS OF UTERUS•Parametrum•Myometrium•Endometrium (Decidua in pregnancy)
LAYERS OF DECIDUA•Superficial compact layers•Intermediate spongy layer•Basal layer
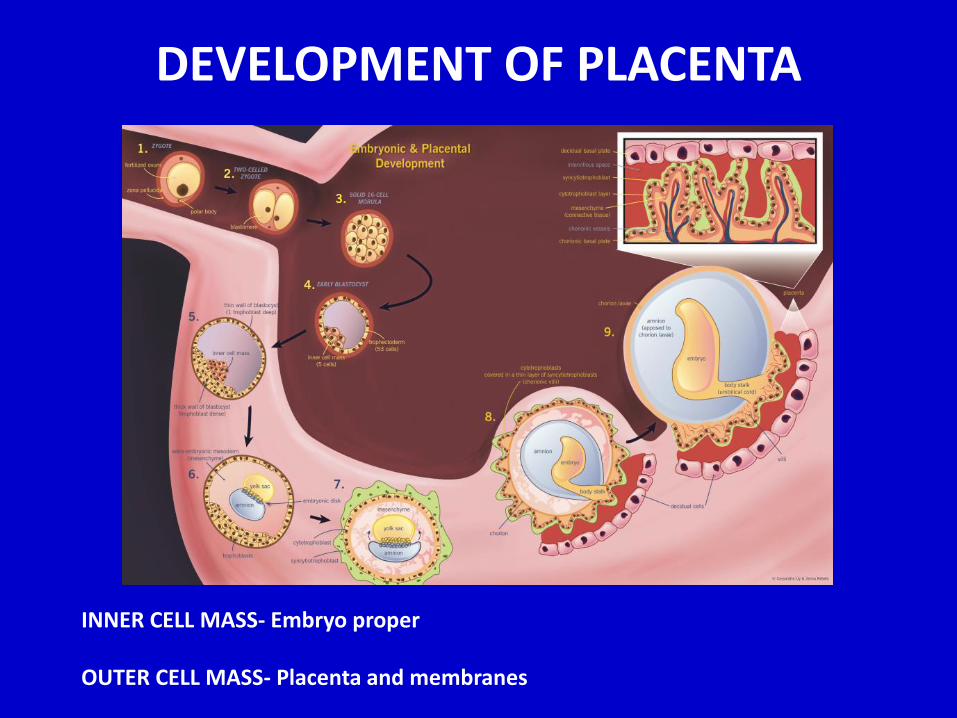
DEVELOPMENT OF PLACENTA
INNER CELL MASS- Embryo proper
OUTER CELL MASS- Placenta and membranes
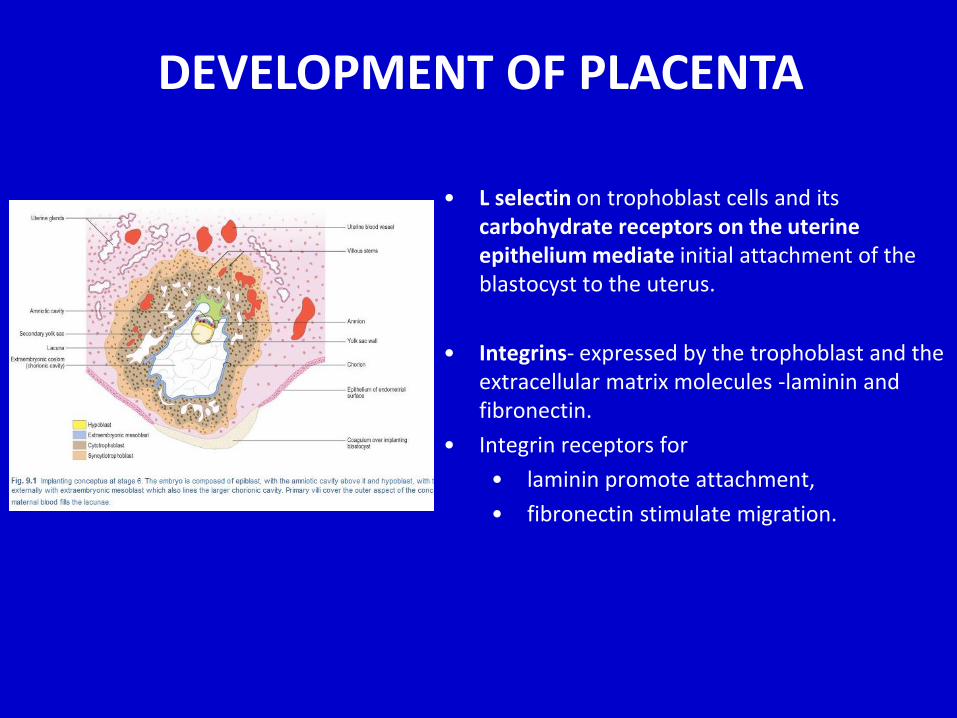
• L selectin on trophoblast cells and its carbohydrate receptors on the uterine epithelium mediate initial attachment of the blastocyst to the uterus.
• Integrins- expressed by the trophoblast and the extracellular matrix molecules -laminin and fibronectin.
• Integrin receptors for
• laminin promote attachment,
• fibronectin stimulate migration.
DEVELOPMENT OF PLACENTA
DEVELOPMENT OF PLACENTA
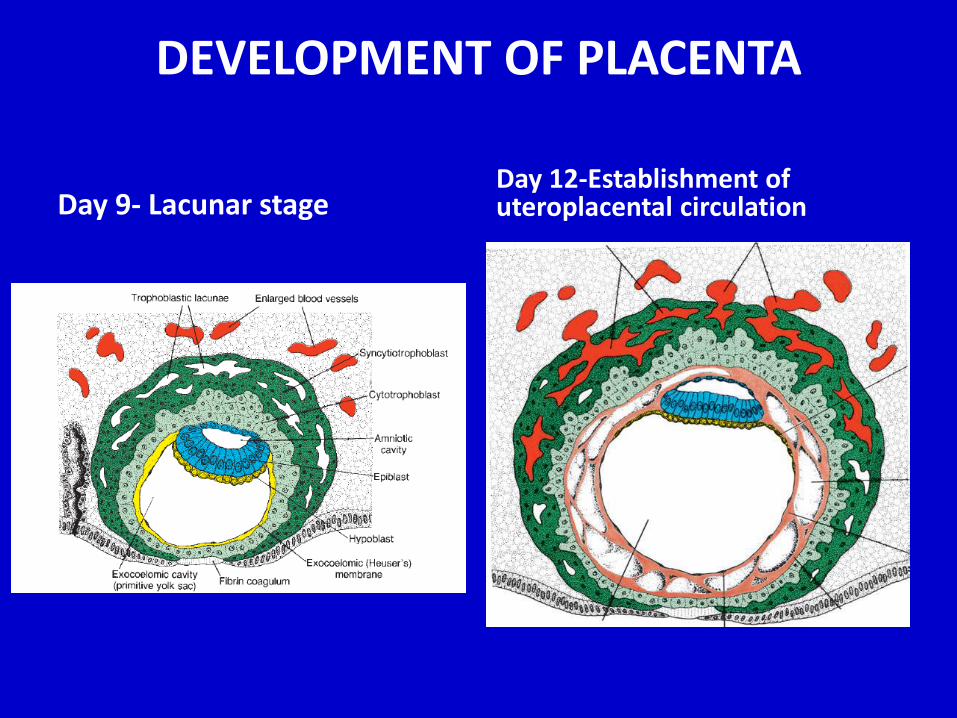
Day 9- Lacunar stageDay 12-Establishment of uteroplacental circulation

Day-13 Primary villi
Day-15 Secondary villi
Projection of syncytiotrophoblastwith core of cytotrophoblast
Core of primary villi invaded with mesoderm
DEVELOPMENT OF PLACENTA
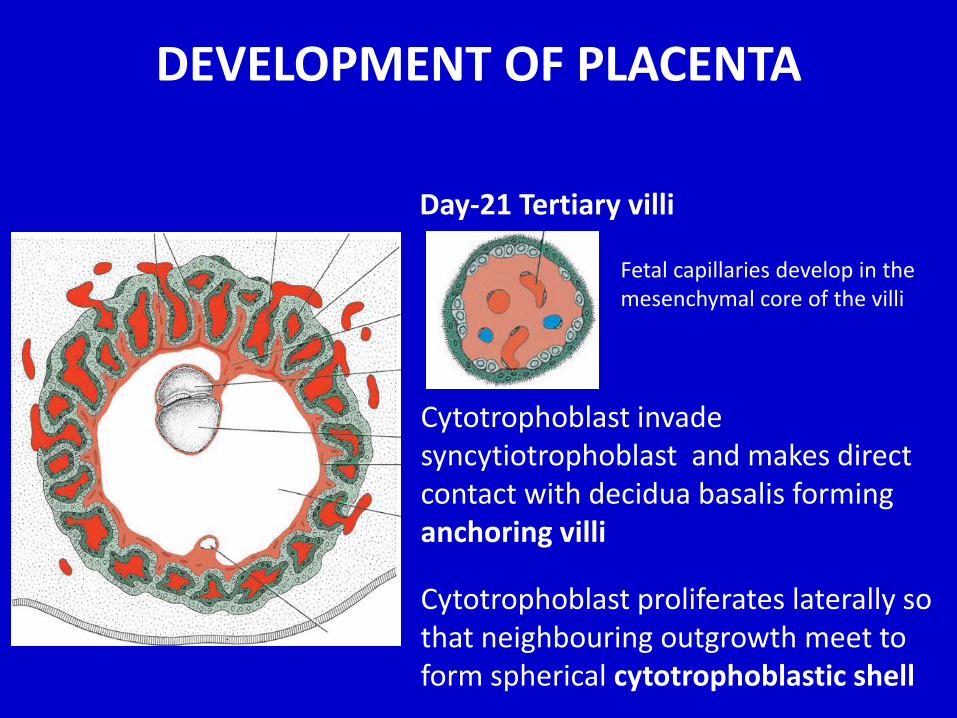
Day-21 Tertiary villi
Fetal capillaries develop in the mesenchymal core of the villi
Cytotrophoblast invade syncytiotrophoblast and makes direct contact with decidua basalis forming anchoring villi
Cytotrophoblast proliferates laterally so that neighbouring outgrowth meet to form spherical cytotrophoblastic shell
DEVELOPMENT OF PLACENTA
CHANGES IN TROPHOBLAST
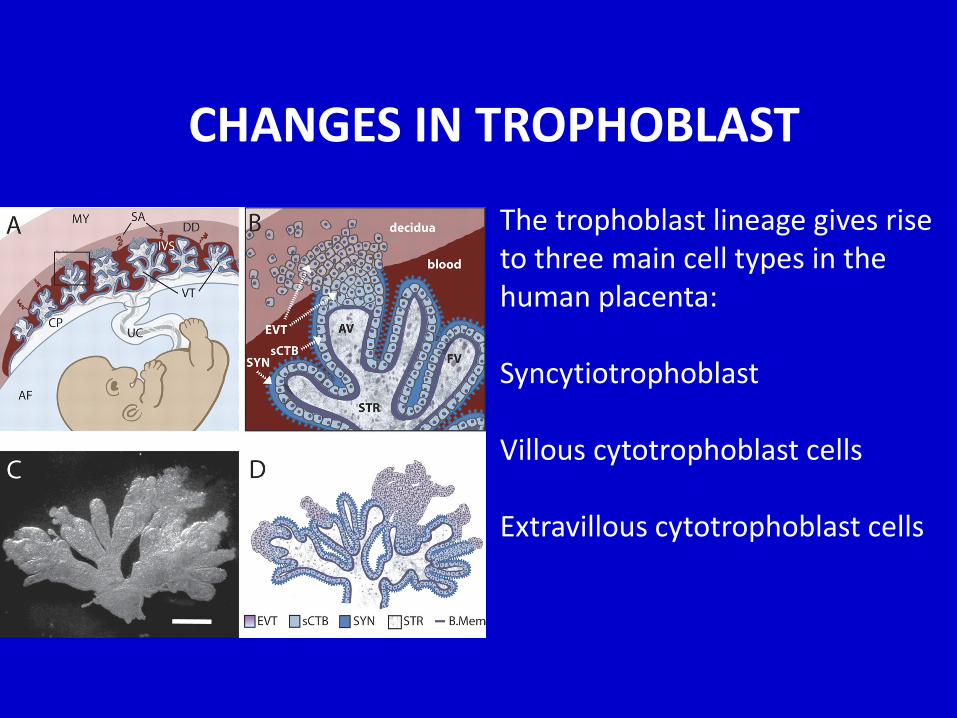
The trophoblast lineage gives rise to three main cell types in the human placenta:
Syncytiotrophoblast
Villous cytotrophoblast cells
Extravillous cytotrophoblast cells
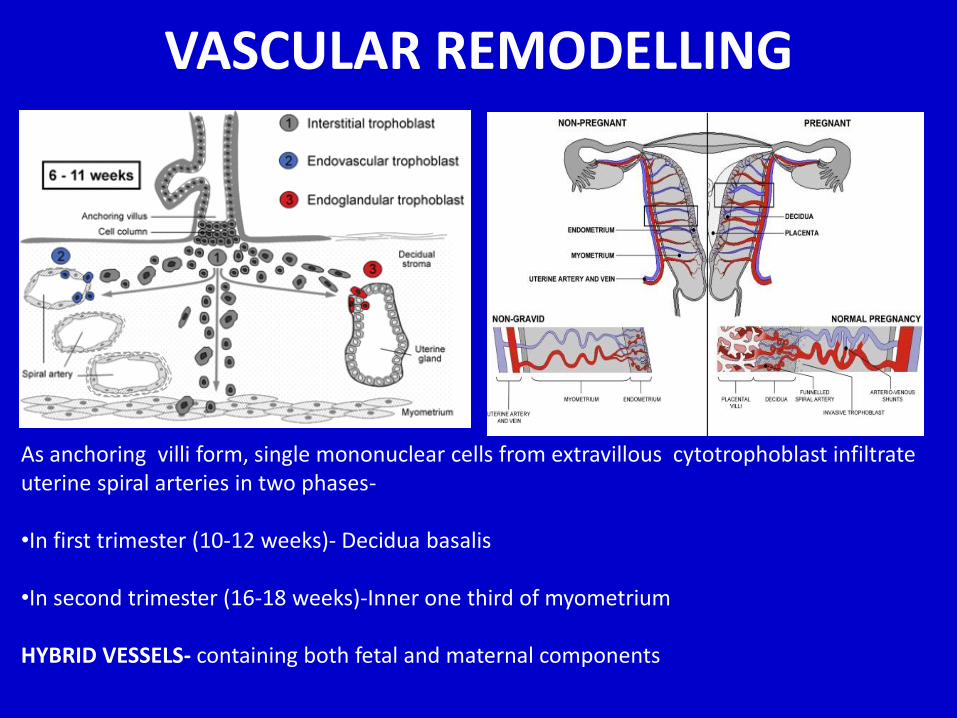
VASCULAR REMODELLING
As anchoring villi form, single mononuclear cells from extravillous cytotrophoblast infiltrate uterine spiral arteries in two phases-
•In first trimester (10-12 weeks)- Decidua basalis
•In second trimester (16-18 weeks)-Inner one third of myometrium
HYBRID VESSELS- containing both fetal and maternal components
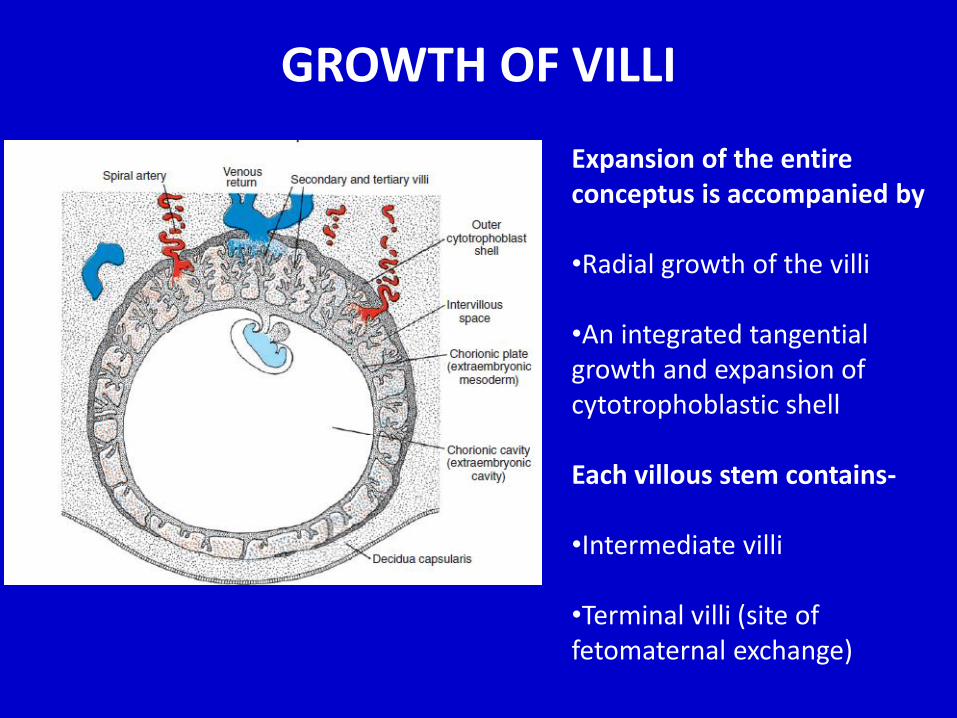
GROWTH OF VILLI
Expansion of the entire conceptus is accompanied by
•Radial growth of the villi
•An integrated tangential growth and expansion of cytotrophoblastic shell
Each villous stem contains-
•Intermediate villi
•Terminal villi (site of fetomaternal exchange)
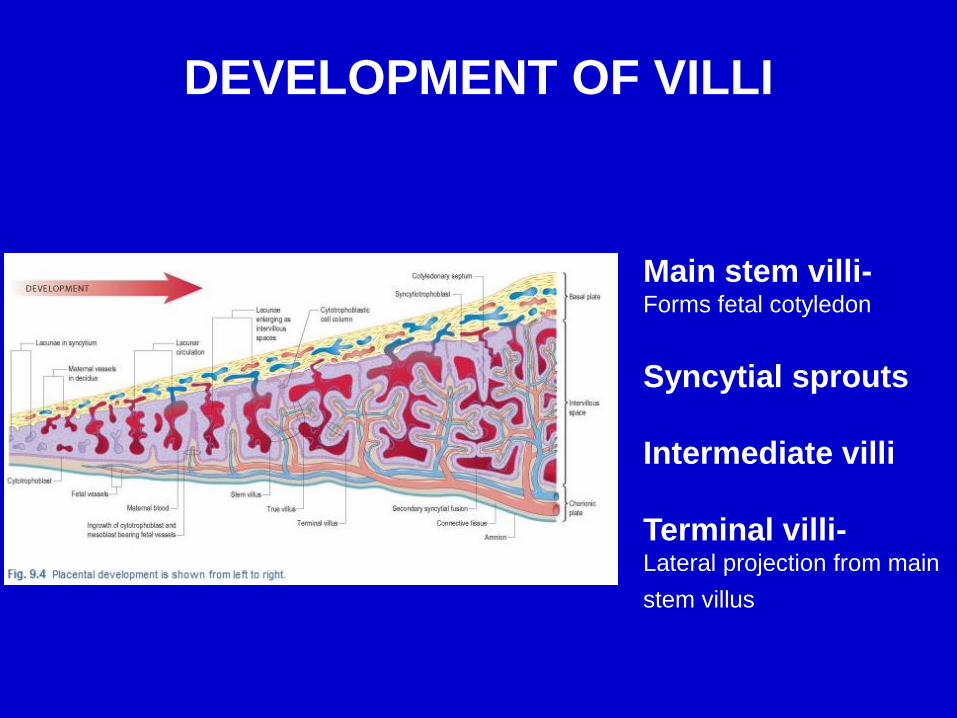
DEVELOPMENT OF VILLI
Main stem villi-Forms fetal cotyledon
Syncytial sprouts
Intermediate villi
Terminal villi-Lateral projection from main
stem villus
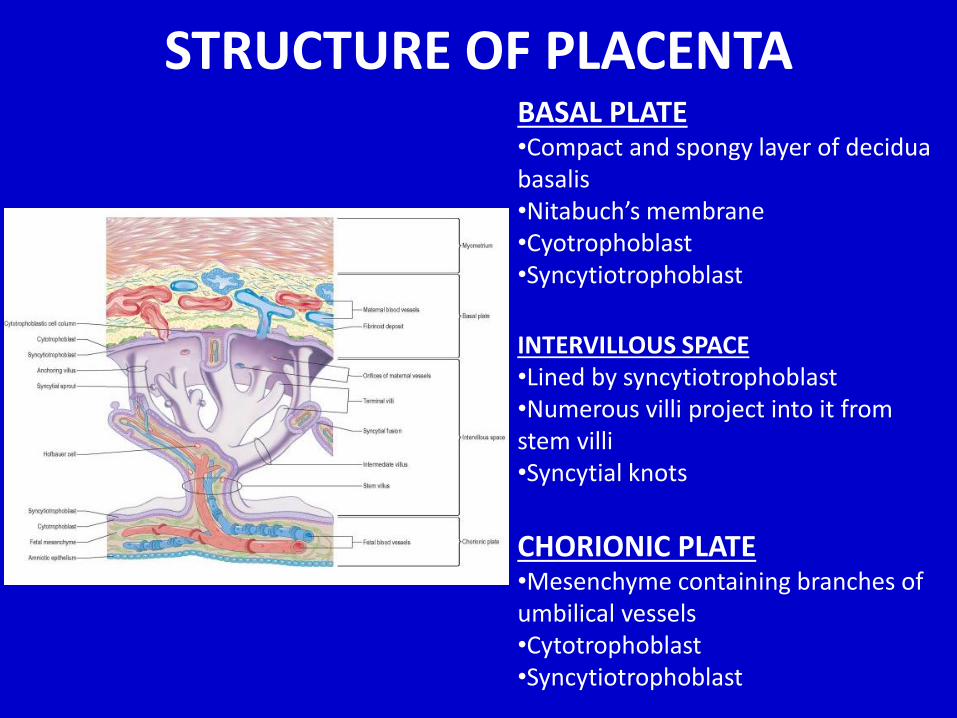
STRUCTURE OF PLACENTABASAL PLATE•Compact and spongy layer of deciduabasalis•Nitabuch’s membrane•Cyotrophoblast•Syncytiotrophoblast
INTERVILLOUS SPACE•Lined by syncytiotrophoblast•Numerous villi project into it from stem villi•Syncytial knots
CHORIONIC PLATE•Mesenchyme containing branches of umbilical vessels•Cytotrophoblast•Syncytiotrophoblast
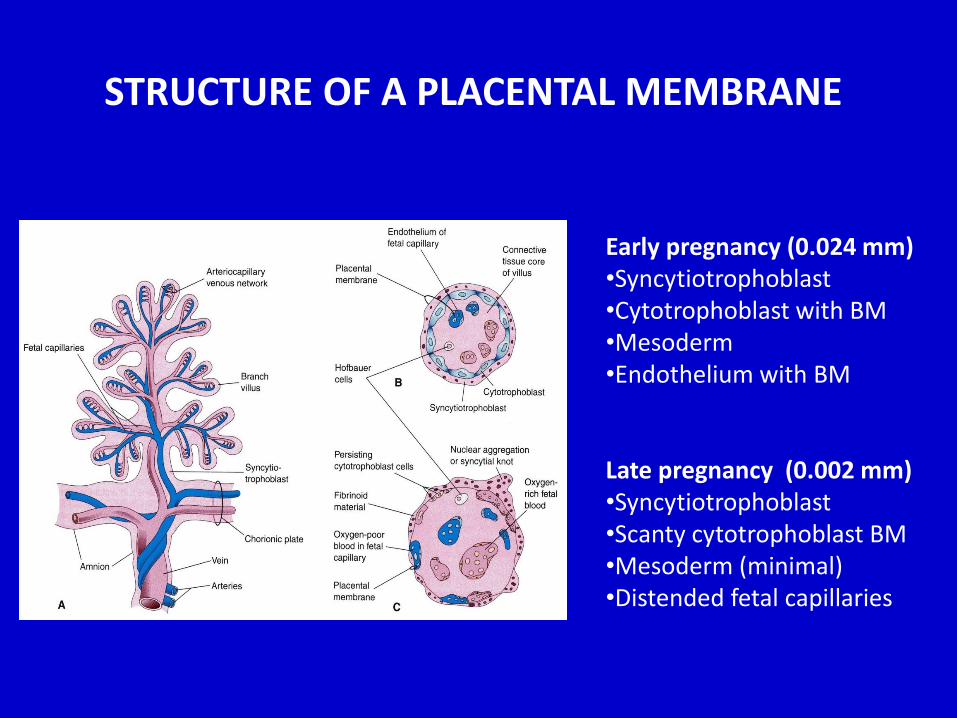
STRUCTURE OF A PLACENTAL MEMBRANE
Early pregnancy (0.024 mm)•Syncytiotrophoblast•Cytotrophoblast with BM•Mesoderm•Endothelium with BM
Late pregnancy (0.002 mm)•Syncytiotrophoblast•Scanty cytotrophoblast BM•Mesoderm (minimal)•Distended fetal capillaries
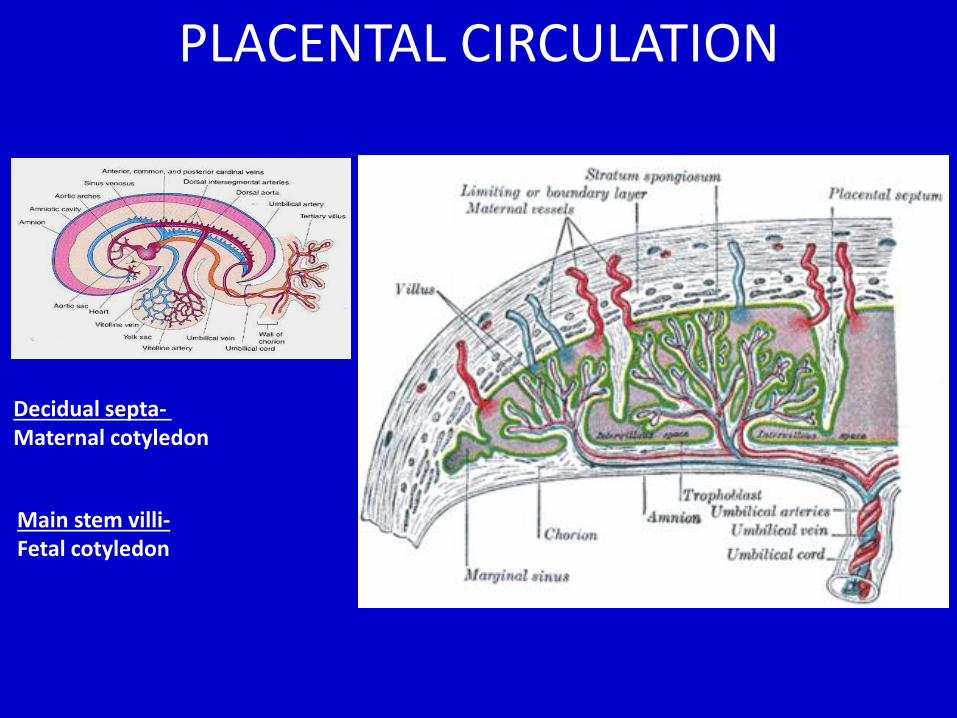
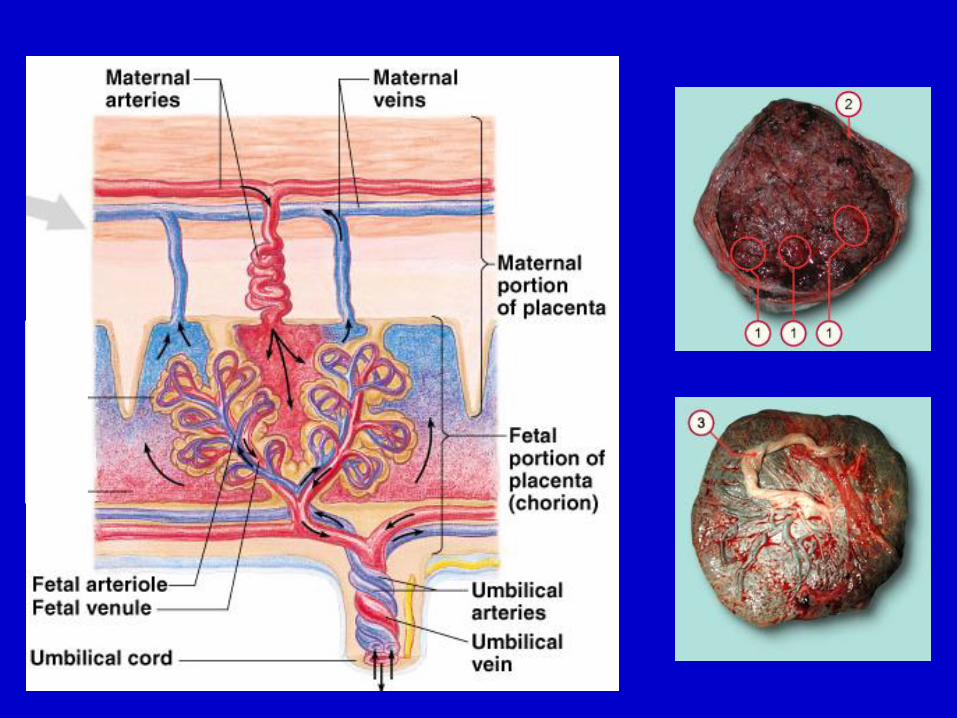
PLACENTAL CIRCULATION
Decidual septa-Maternal cotyledon
Main stem villi-Fetal cotyledon
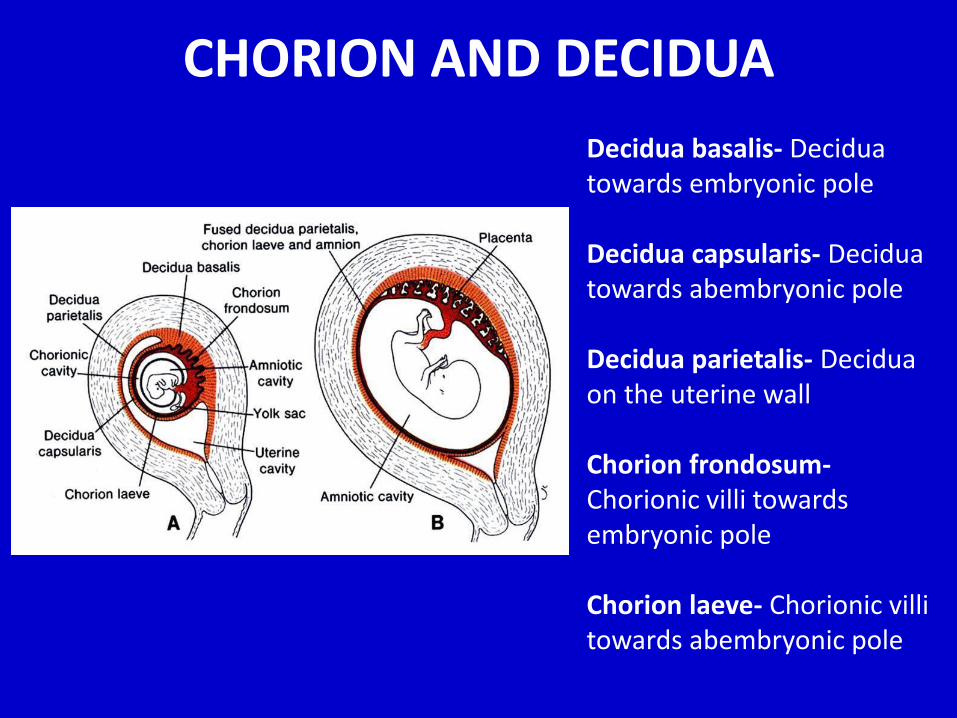
CHORION AND DECIDUA
Decidua basalis- Decidua towards embryonic pole
Decidua capsularis- Decidua towards abembryonic pole
Decidua parietalis- Decidua on the uterine wall
Chorion frondosum-Chorionic villi towards embryonic pole
Chorion laeve- Chorionic villi towards abembryonic pole
PLACENTAL AGEING– Increase in the fibrous tissue in the core of the villous
– Thickening of the basement membrane in the fetal capillary
– Obliteration of some fetal vessels and dialatation of capillaries
– Syncytial knots
– Partial disappearance of cytotrophoblast
– Decrease in mesoderm including hofbauer cell
– Deposition of fibrin on the surface of villi in the junctional zone and chorionic plate
» Decidua-Nitabuch’s membrane
» Intervillous space - white infarct & Rohr’s stria
ABNORMAL PLACENTATION
1. Abnormal implantation
2. Abnormal blastocyst
3. Defect in Nitabuch’s membrane
4. Activated chorion laeve
5. Defect in vascular remodelling
6. Passage across placental membrane/barrier
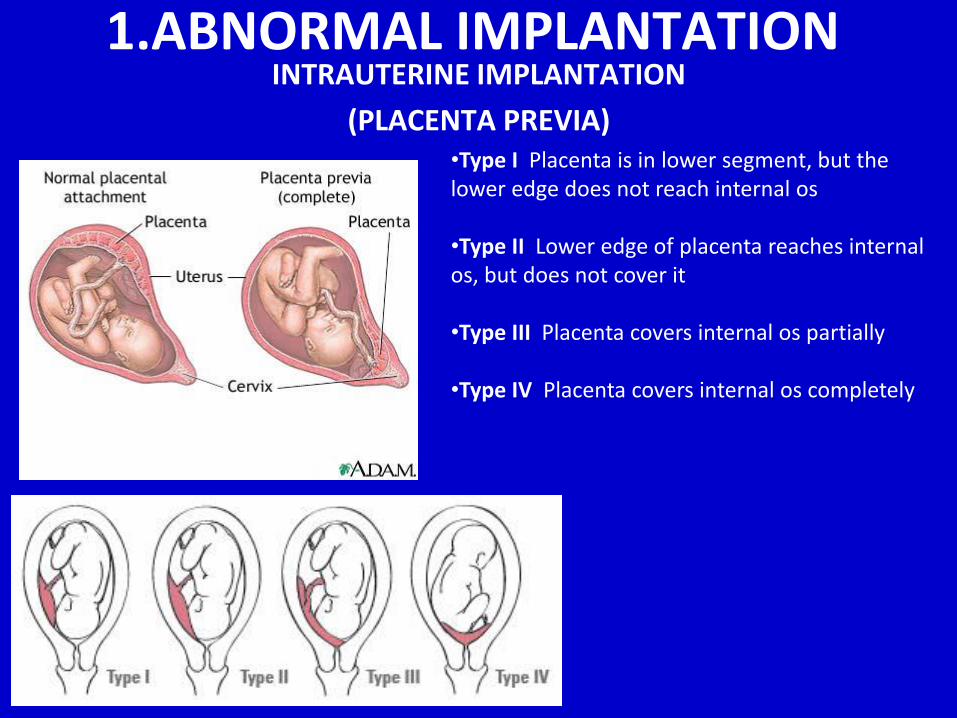
•Type I Placenta is in lower segment, but the lower edge does not reach internal os
•Type II Lower edge of placenta reaches internal os, but does not cover it
•Type III Placenta covers internal os partially
•Type IV Placenta covers internal os completely
INTRAUTERINE IMPLANTATION
(PLACENTA PREVIA)
1.ABNORMAL IMPLANTATION
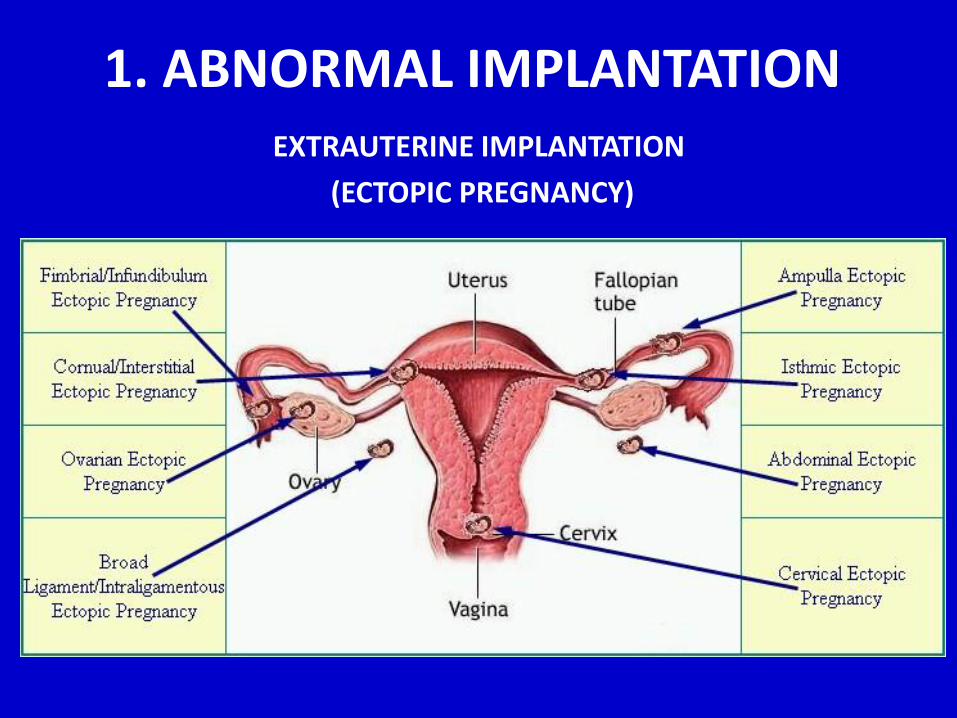
1. ABNORMAL IMPLANTATION EXTRAUTERINE IMPLANTATION
(ECTOPIC PREGNANCY)
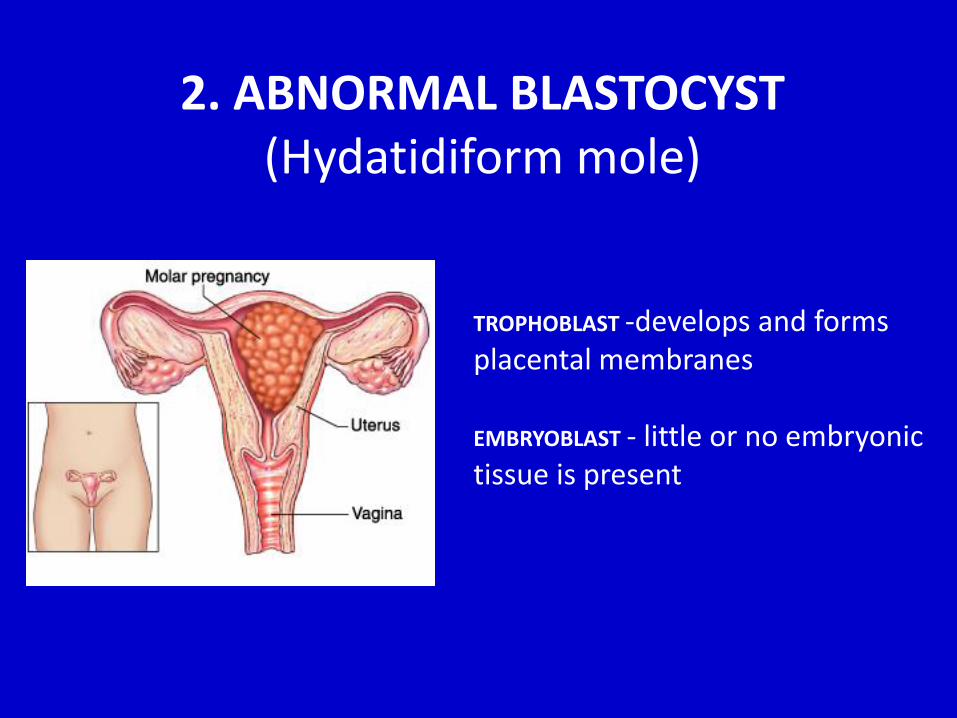
2. ABNORMAL BLASTOCYST(Hydatidiform mole)
TROPHOBLAST -develops and forms placental membranes
EMBRYOBLAST - little or no embryonic tissue is present
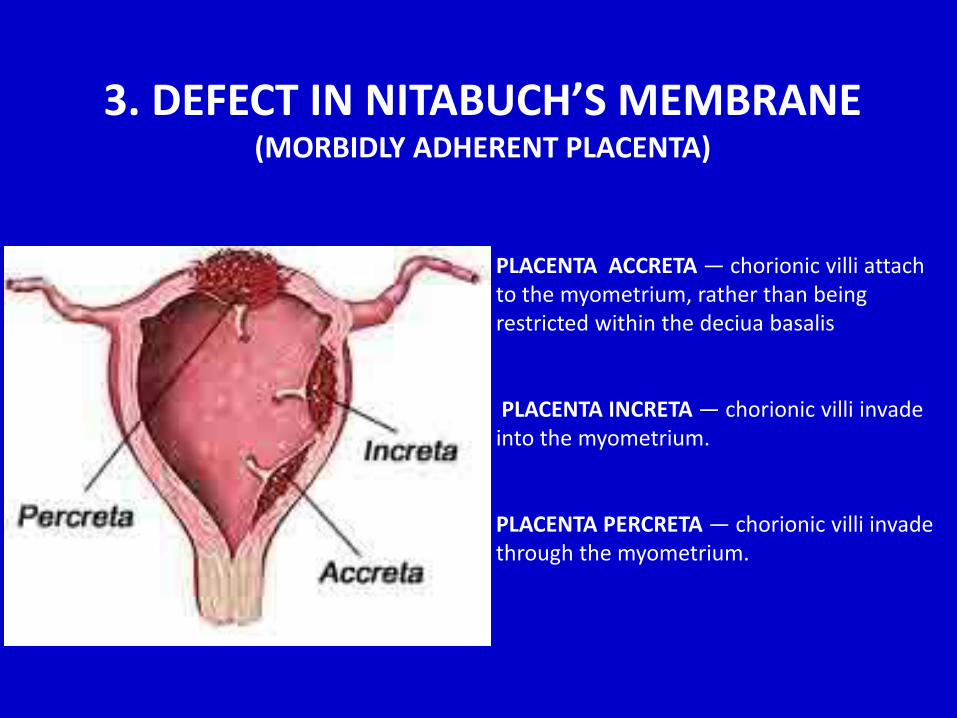
3. DEFECT IN NITABUCH’S MEMBRANE(MORBIDLY ADHERENT PLACENTA)
PLACENTA ACCRETA — chorionic villi attach to the myometrium, rather than being restricted within the deciua basalis
PLACENTA INCRETA — chorionic villi invade into the myometrium.
PLACENTA PERCRETA — chorionic villi invade through the myometrium.
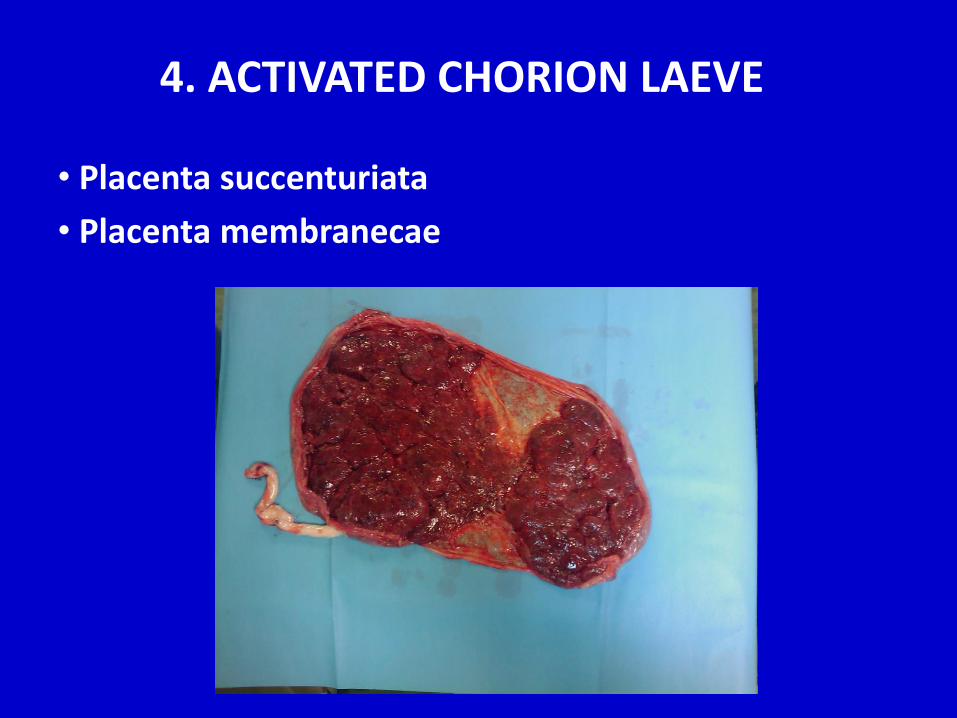
• Placenta succenturiata
• Placenta membranecae
4. ACTIVATED CHORION LAEVE
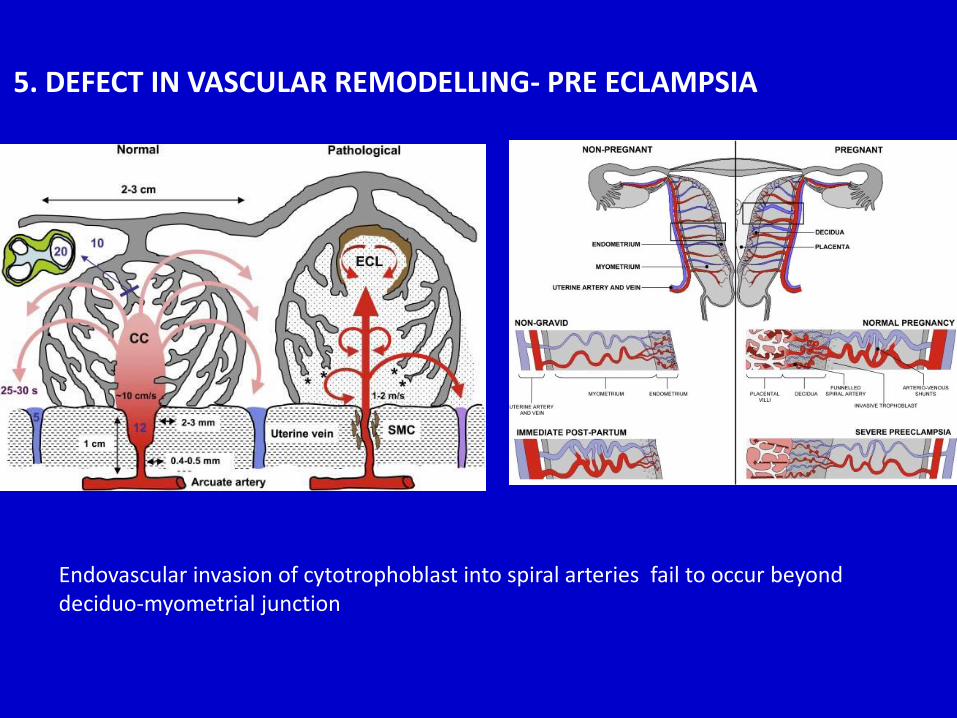
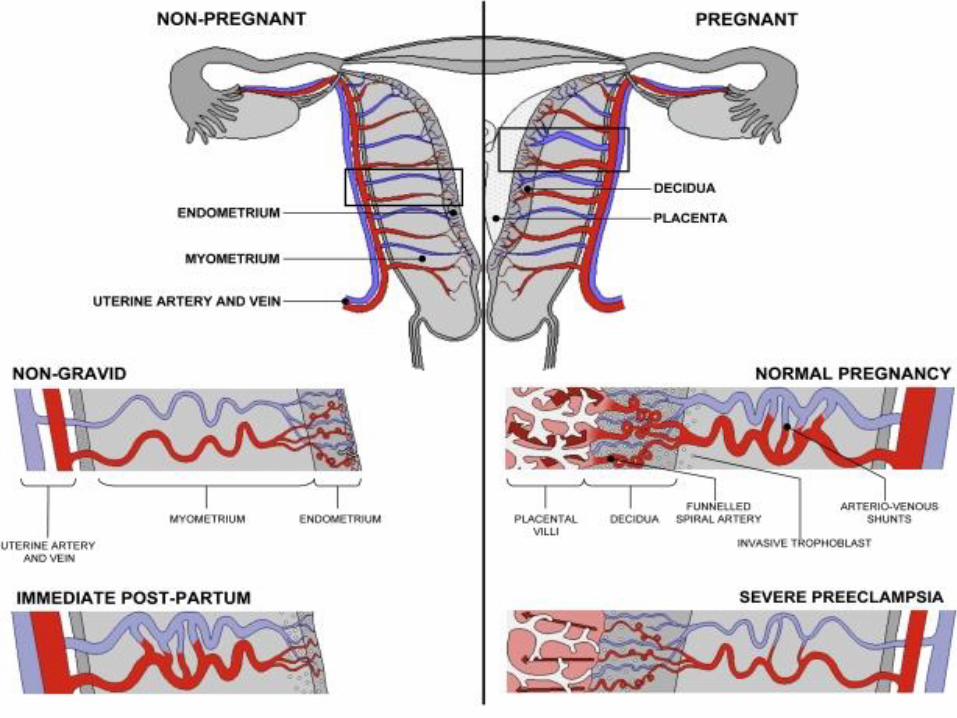
5. DEFECT IN VASCULAR REMODELLING- PRE ECLAMPSIA
Endovascular invasion of cytotrophoblast into spiral arteries fail to occur beyond deciduo-myometrial junction
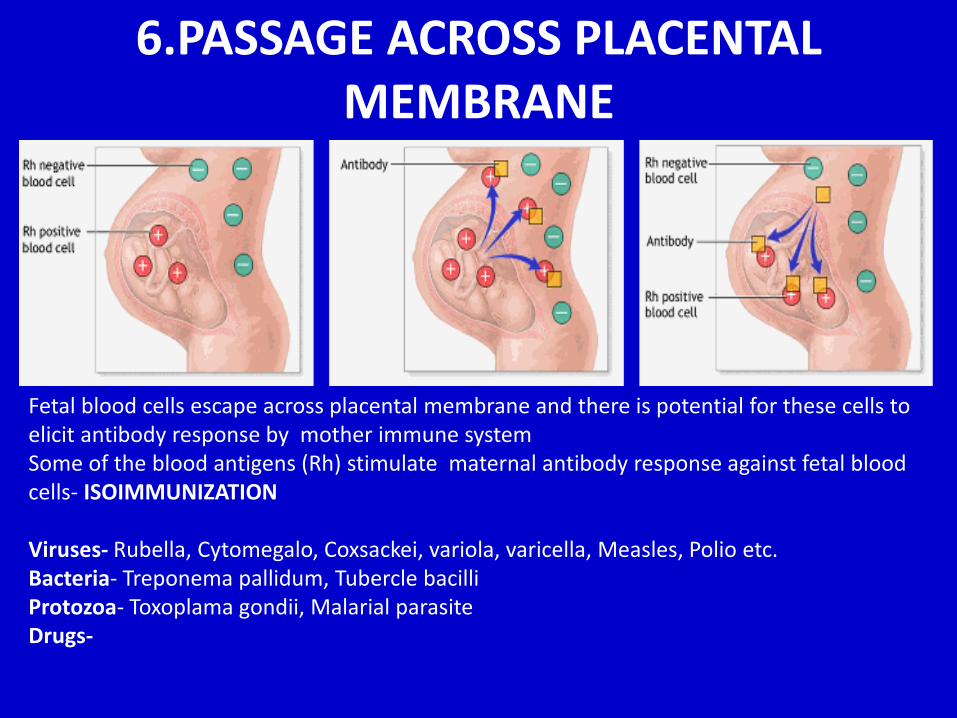
6.PASSAGE ACROSS PLACENTAL MEMBRANE
Fetal blood cells escape across placental membrane and there is potential for these cells to elicit antibody response by mother immune systemSome of the blood antigens (Rh) stimulate maternal antibody response against fetal blood cells- ISOIMMUNIZATION
Viruses- Rubella, Cytomegalo, Coxsackei, variola, varicella, Measles, Polio etc.Bacteria- Treponema pallidum, Tubercle bacilliProtozoa- Toxoplama gondii, Malarial parasiteDrugs-
Dr.Shalini KumarAssistant Professor
35 yr old female Presented with spontaneously ruptured
membranes & breech presentation for caesarean delivery at 39wks gestation
Past h/o 2 spontaneus abortion No live issue Surgical h/o dilatation & curettage for
abortions
LSCS was done Baby was delivered Intraoperatively –Irregularity in placental
attachment ~ 2 x2 cm in anterior and medial part of uterus
Area of endometrium surgically corrected to achieve hemostasis
One Hour later in post op ICU ,large clot (approx. 800ml)resulted per vagina on uterine expression
Vitals signs were normal Managed conservatively with fluids and drugs Bleeding continued Intrauterine balloon inserted to tamponade
the bleeding
2 hours later recurrence of perfuse bleeding from vagina with hypotension
2 units of blood trasfused Initially planned for uterine artery
embolisation –>couldn’t be done as vitals were unstable
Shifted to operation theater
Bleeding couldn’t be controlled (>800ml) Exploratory laparotomy,bilateral uterine
artery ligation and supracervicalhysterectomy was performed
Post operative patient was stable Histopathological report showed placenta
increta
Post Partum Haemorrhage following placenta increta
• Primary PPH – Occurs when blood loss is > 500
ml. in the first 24 hours after a vaginal delivery or
greater than 1000 ml after a cesarean birth
(Normal blood loss is about 300 - 500 ml)
• Secondary PPH – significant blood loss
between 24 hours and 6 weeks after birth
• Most cases (99%) of post partum hemorrhage are
primary
Placenta Accreta
Uterine Atony
Lacerations
Retained Placental Fragments
Inversion of the Uterus
Hematomas
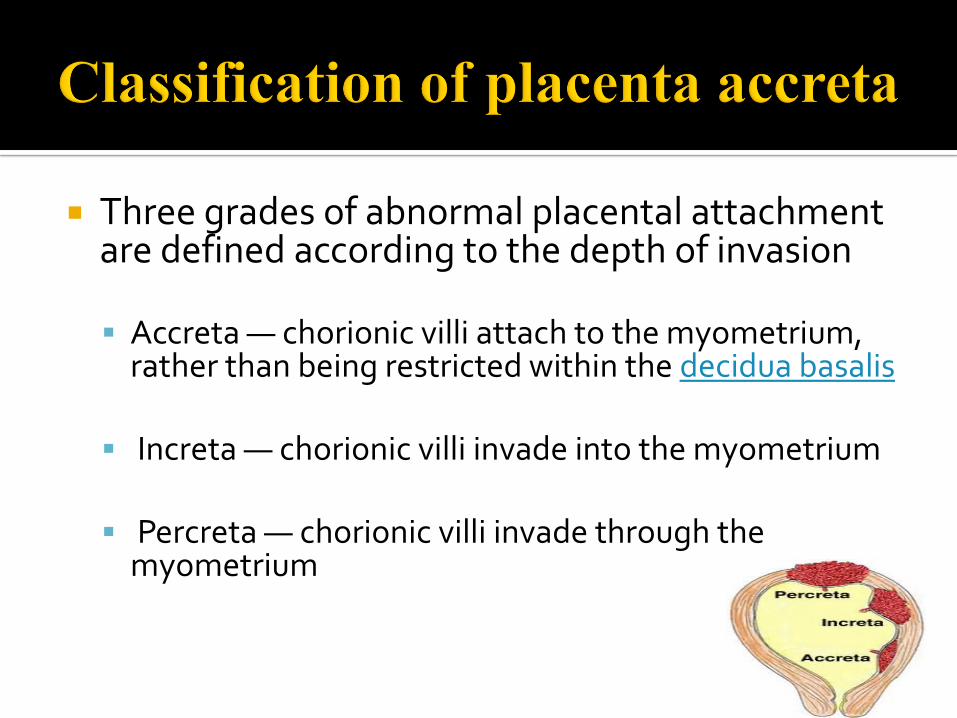
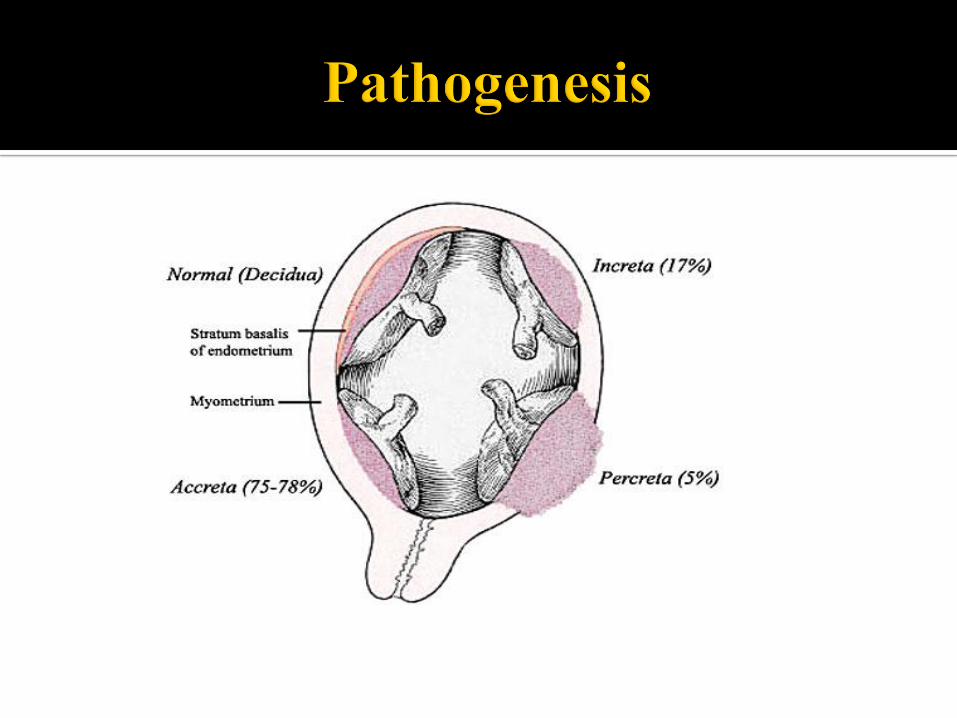
Three grades of abnormal placental attachment are defined according to the depth of invasion
Accreta — chorionic villi attach to the myometrium, rather than being restricted within the decidua basalis
Increta — chorionic villi invade into the myometrium
Percreta — chorionic villi invade through the myometrium
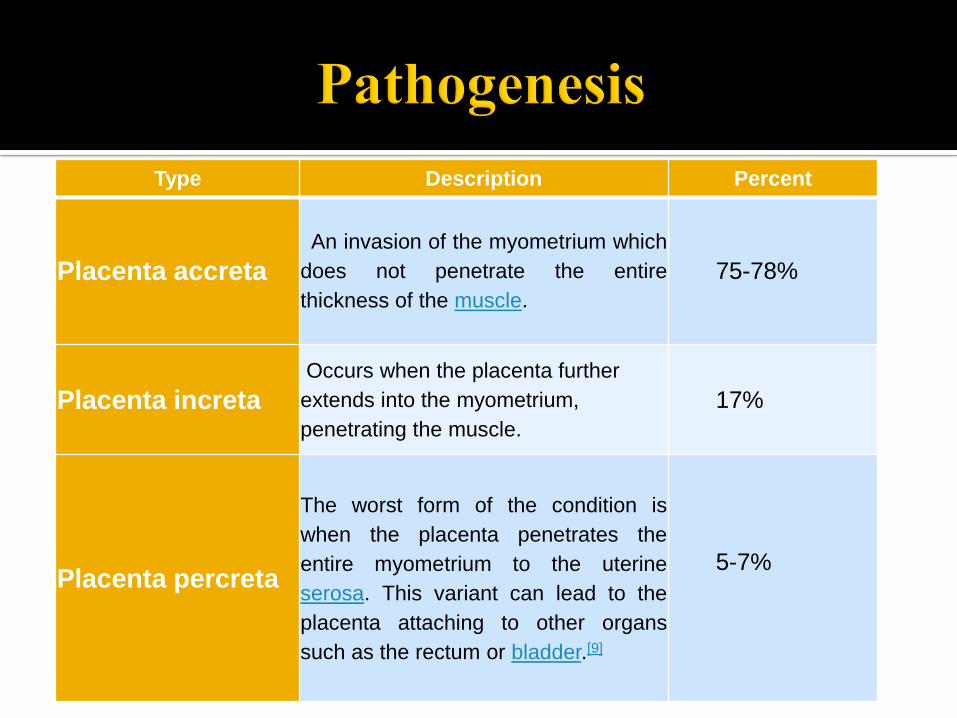
Type Description Percent
Placenta accreta
An invasion of the myometrium which
does not penetrate the entire
thickness of the muscle.
75-78%
Placenta increta
Occurs when the placenta further
extends into the myometrium,
penetrating the muscle.
17%
Placenta percreta
The worst form of the condition is
when the placenta penetrates the
entire myometrium to the uterine
serosa. This variant can lead to the
placenta attaching to other organs
such as the rectum or bladder.[9]
5-7%
In this case it is hypothetised that due to previous instrumentation in uterus leads to abnormal attachment of placenta to myometrium resulting in placenta incretawhich was associated with:
Heavy bleeding
Need for transfusion
Required hysterectomy
PRE ECLAMPSIA - ANATOMICAL PERSPECTIVE
Dr SHWETA CHAUDHARY
Pre Eclampsia
Multisystem disorder of unknown etiology characterised by
• Hypertension - blood pressures ≥ 140/90 mm Hg on 2 occasions and
• Proteinuria - with urinary protein excretion ≥ 300 mg/day (in a 24-hour urine specimen) or 100 mg/L
After 20 wks in a previously normotensive and non proteinuric woman
Edema, a classic feature of the disease
HISTORY
A 29 yr old patient came in antenatal clinic with history of two previous pregnancies with a normal outcome and no medical conditions
At 15 weeks, her BMI was 28 ( N- 25)
Blood pressure - 134/86 mmHg
At 27 weeks, she was referred to clinic with new onset hypertension
• BP- 158/102 mmHg• No other sign of pre-eclampsia• No evidence of proteinuria (negative dipstick)• In clinic, her BP settled to 145/90 mmHg
In the 32nd week• Her baby’s estimated fetal weight (EFW) on scan-
appropriate for gestational ageEFW -1,580g
By the 33rd week
• Blood pressure - 156/110 mmHg and
She was administered nifedipine
• Protein: Creatinine Ratio - 24 mg/mmol ( N- < 30 mg/mmol)
She reported headaches, but
• no visual symptoms,
• no coagulopathy, or liver dysfunction
Clinical Question:
Does she have evolving pre-eclampsia?
PLCENTAL GROWTH FACTOR(PlGF)
In the 27th week
• her plasma PlGF was - 34 pg/ml (abnormal <100 pg/mL) suggesting she had placental dysfunction
In the 33rd week
• her plasma PlGF had fallen to
• less than 12pg/ml (very abnormal <12pg/mL) suggesting she had severe placental dysfunction
Pregnancy Outcome:
Two days after commencing nifedipine, her BP decreased to 140/84 mmHg
At 34 weeks, she developed
• Proteinuria (PCR 176 mg/mmol) and a
• USG Scan - IUGR
She was induced, but was delivered by caesarean section for fetal distress.
• Her baby weighed 1,510g
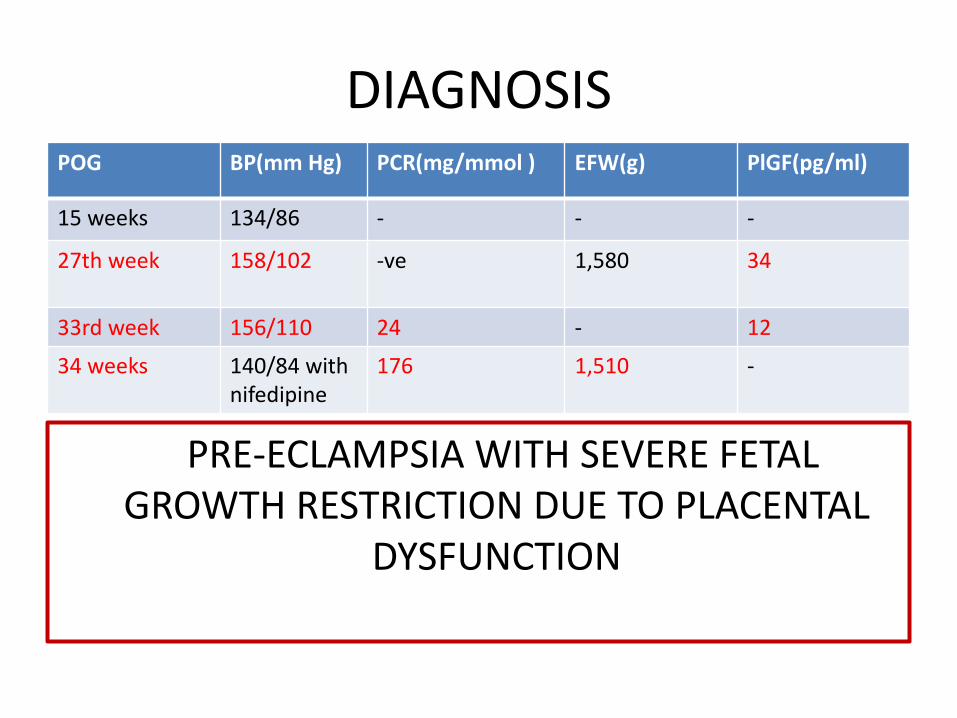
DIAGNOSIS
PRE-ECLAMPSIA WITH SEVERE FETAL GROWTH RESTRICTION DUE TO PLACENTAL
DYSFUNCTION
POG BP(mm Hg) PCR(mg/mmol ) EFW(g) PlGF(pg/ml)
15 weeks 134/86 - - -
27th week 158/102 -ve 1,580 34
33rd week 156/110 24 - 12
34 weeks 140/84 withnifedipine
176 1,510 -
TYPES
• Early-onset PET (diagnosed before 34 weeks of gestation) - necessitates delivery before 34 weeks’ gestation
• Late-onset PET (diagnosed after 34 weeks of gestation) - requires delivery at or after 34 weeks of gestation
• Involves one or more other systems, such as renal, haematological, liver, neurological, pulmonary and/or placental abruption
• Leading cause of maternal and perinatalmorbidity and mortality, particularly when it occurs at a gestational age of less than 34 weeks
DEFECT IN VASCULAR
REMODELLING
• Endovascular cytotrophoblasts fail to
migrate
• Spiral arteries remain as small-caliber
resistance vessels
• Reduction of blood supply to fetoplacental
unit
IUGR
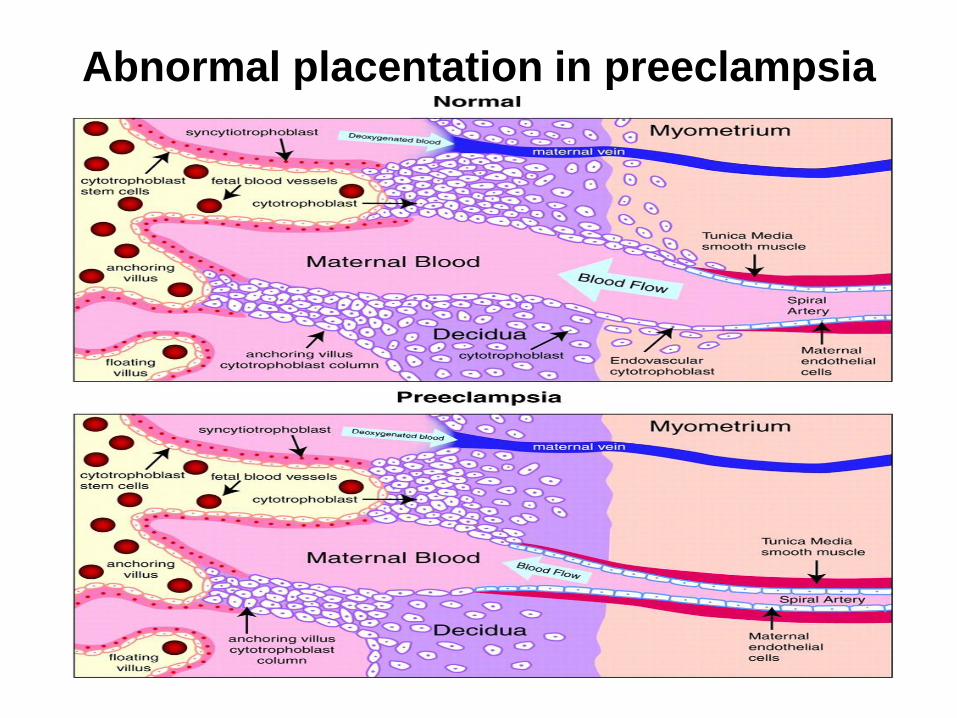
Abnormal placentation in preeclampsia
EXPLANATION• Placental Growth Factor (PlGF) is a member of the
Vascular Endothelial Growth Factor (VEGF) family of growth factors involved in the regulation of angiogenesis
• Expressed by trophoblast cells and placental villi in pregnancy
• Made by the placenta and released into maternal circulation
• Induces vasodilation of uterine, myometrial, mesenteric, and subcutaneous arteries
• Contributes to uterine vascular remodelling during pregnancy
• PlGF increases in first and second trimester and then decreases after 34 weeks suggestive of placental maturity
• Decreased circulating free PlGF during first and second trimester are seen in women diagnosed` with pre-eclampsia
• Low levels of PlGF can be detected before the onset of clinical symptoms
SCREENING PRE ECLAMPSIA
Refrences
• DOI: 10.1161/CIRCULATIONAHA.109.853127
• http://www.plgf.com/home/proposed-clinical-use-of-plgf/case-studies.htm
• http://circ.ahajournals.org/content/128/19/2121.short
RECENT ADVANCES
PROF. RAJ D. MEHRA
Placenta is usually disposed off along with other medical waste, a “forgotten organ” that typically receives little attention from scientists, clinicians, and the public at large.
However, beyond reproductive biology, placentas and associated tissues have been employed in diverse fields such as immunology, stem cell research, environmental sciences and toxicology, genetics, hypertension research, cancer research and tissue engineering.
PLACENTA : NEW APPROACHES
Chemical communications between the placenta and hypothalamus of the mother & fetus play an important role in expression of various genes.
For example, 41 genes expressed in placentas have been associated with neurological diseases.
Two genes: schizophrenia histidine triad nucleotide binding protein 1 (Hint1) and Strathmin1 (Stmn1 have been identified as placental markers for schiziophrenia. (Broad & Keverne 2011; PNAS)
PLACENTA : NEW APPROACHES
PLACENTA: SOURCE OF STEM CELLS
CD34+ve Stem cells have successfully been harvested from the placenta & umbilical cord and differentiated into tissues of choice.
Their potential to treat over 80 diseases to date, including leukemia, Hodgkin's lymphoma, sickle cell anemia and others has been documented.
Although very few placental cell transplants have taken place till date, but this appears to be a promising and upcoming field of research.
www.wombfruits.com
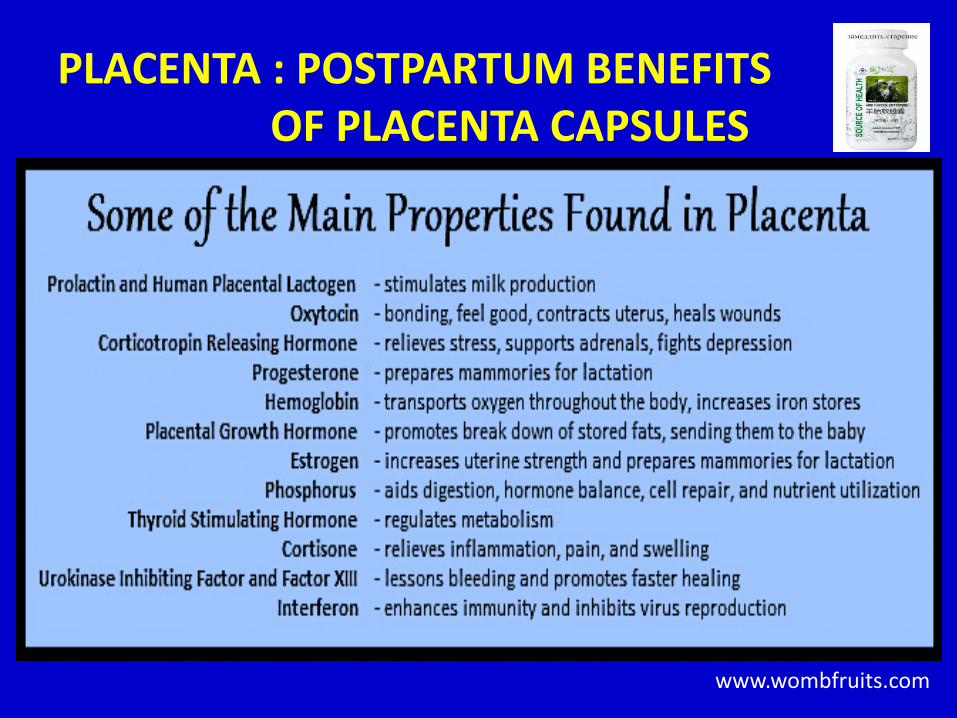
PLACENTA : POSTPARTUM BENEFITS OF PLACENTA CAPSULES
PROPOSED: SCIENTIFIC BASIS OF MATERNAL PLACENTOPHAGY
Placental tissue consumption enhances analgesic effects through a specific endogenous opioid pathway (DiPirro and Kristal 2004; Kristal
1991). Similar hypotheses have been proposed for possible comparable effects in human mothers if they were to engage in the behavior (Apari and Rózsa 2006).
CRH (Corticotropin-Releasing Hormone) Stress Reducer Hypothalamus.
During the last trimester of pregnancy, the placenta secretes so much CRH that the levels in the bloodstream increase threefold.
However, it was also discovered that postpartum women have lower than average levels of CRH, triggering depressive symptoms (NIH study).
PLACENTA : POTENTIAL BENEFITS OF
PLACENTAL CAPSULES IN OTHER DISEASES
Native Americans: dried & ground umbilical cord, given to Child when Sick.
In Central India: women of the Kol Tribe eat placenta to aid reproductive function.
Sino-Vietnamese consume placenta to aid the recovery of those suffering from tuberculosis.
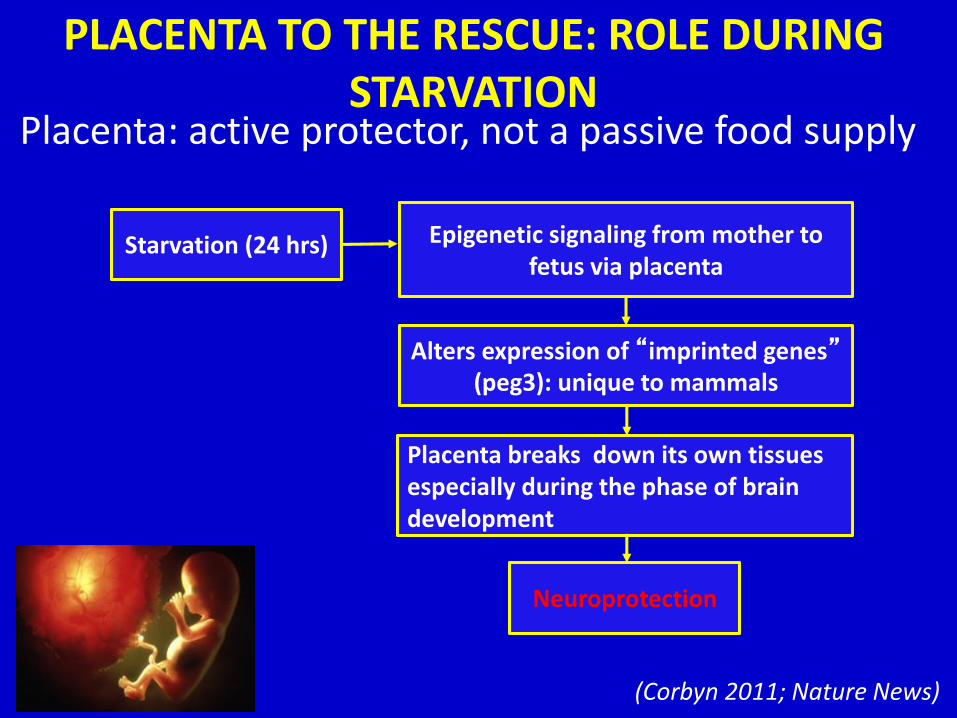
PLACENTA TO THE RESCUE: ROLE DURING STARVATION
Placenta: active protector, not a passive food supply
Starvation (24 hrs)
Alters expression of “imprinted genes”(peg3): unique to mammals
Placenta breaks down its own tissues especially during the phase of brain development
Neuroprotection
Epigenetic signaling from mother to fetus via placenta
(Corbyn 2011; Nature News)
PLACENTREX
A Drug containing Peptides (CRF), Nucleotides (NADPH) & Glutamate is actually derived from an extract of fresh term, healthy, human placenta.
Uses:
• Pelvic Inflammatory disease (Agarwal et al., 2010)
• Wound Healing (Ridley et al., 2003)
PLACENTAL MICROBIOTA: ROLE IN HUMAN HEALTH
Recent evidence suggests that Placenta, long thought to be a sterile organ is home to a bacterial community (non pathogenic, commensal microbiota) similar to the one found in the oral cavity.
Microbes are generally non-pathogenic, however variations in their composition could be the root of common but poorly understood pregnancy disorders such as preterm birth, which occurs one out of every ten pregnancies. (Moskvitch 2014; Nature News)

USE IN COSMETICS
Hydrolyzed Human & animal Placental Proteins have been used as additives in cosmetic products as skin and hair conditioning agents.
Human-derived ingredients are prohibited from use under provisions of the European Union cosmetics & Food and Drug Administration (FDA) based on concerns about transmission of human spongiform encephalopathies and viral diseases eg. human immunodeficiency virus (Nair B, Elmore AR; Cosmetic Ingredient Review Expert panel, 2002)
However, it is widely prevalent in South East Asian countries

MULTIPLE CHOICE QUESTIONS
Dr. Khalid Mehmood
Q1. Uteroplacental circulation is established by which day of development
a) 08th day
b) 10th day
c) 12th day
d) 14th day
Q2.Fetal component of placenta is formed by which of the following
a) Decidua basalis
b) Decidua parietalis
c) Chorion laeve
d) Chorion frondosum
Q3. Most common site of ectopic pregnancy is
a) Ampulla of uterine tube
b) Isthmus of uterine tube
c) Uterine cervix
d) Abdominal cavity
Q4. Exchange between maternal and fetal blood takes place at which of the following site.
a) Main stem villi
b) Intermediate villi
c) Terminal villi
d) Anchoring villi
Q5. Human placenta is
a) Hemochorial
b) Epitheliochorial
c) Endotheliochorial
d) Choriovitelline
KEY
Q1. c
Q2. d
Q3. a
Q4. c
Q5. a





























