Embed Size (px)
Citation preview
Am J Geriatr Psychiatry 10:5, September-October 2002 521
Depressive Symptoms and Mortality in aProspective Study of 2,558 Older Adults
Jurgen Unutzer, M.D., M.P.H., Donald L. Patrick, Ph.D., M.S.P.H.Tonya Marmon, M.S., Gregory E. Simon, M.D., M.P.H.
Wayne J. Katon, M.D.
Objective: The authors report results from a 7-year prospective study of depressionand mortality in 2,558 Medicare recipients age 65 and older. Methods: This report isbased on a secondary data analysis of a randomized controlled trial that evaluatedthe cost-effectiveness of preventive services for older enrollees in an HMO. Results:Subjects with mild-to-moderate depression at baseline did not have an increased riskof mortality compared with those without significant depression. The 3% of olderadults with the most severe depressive syndromes, however, had significant increasesin mortality, even after adjusting for demographics, health risk behaviors, and chronicmedical disorders. Conclusion: The increase in mortality in this group of older adultswas comparable to that in participants with chronic medical disorders such as em-physema or heart disease. (Am J Geriatr Psychiatry 2002; 10:521–530)
Received October 5, 2000; revised January 8, 2001; accepted January 30, 2001. From the Center for Health Services Research, UCLA Neuropsy-chiatric Institute, Los Angeles, CA (JU,TM), the Department of Health Services, University of Washington. Seattle, WA (DLP), the Center for HealthStudies, Group Health Cooperative of Puget Sound, Seattle, WA (GES), and the Department of Psychiatry and Behavioral Sciences, University ofWashington, Seattle, WA (WJK). Address correspondence to Dr. Unutzer, Center for Health Services Research, UCLA Neuropsychiatric Institute,10920 Wilshire Blvd., Suite 300, Los Angeles, CA 90024. e-mail: [email protected]
Copyright � 2002 American Association for Geriatric Psychiatry
The prevalence of major depressive disorder inhealthy, non-institutionalized older adults is only
about 1%, but as many as 15% of older adults experiencesignificant depressive symptoms that are below the se-verity threshold for a DSM-IV diagnosis of major de-pression.1 A number of earlier studies have shown thatmajor depression and subthreshold depressive symp-toms have a significant impact on older individuals’ abil-ity to function and on their quality of life.2–8 Late-lifedepression has also been associated with other adverseoutcomes, such as increased medical morbidity,9–11 in-creased use of health services,12 and, in some studies,mortality.13–16 According to the Global Burden of Dis-ease Study, major depression ranks fourth in the worldamong causes of early death and disability.17
Research findings about the association between de-pression and mortality have been contradictory.15,16,18,19
A number of research teams have reported statisticallysignificant associations between depressive symptomsand mortality. Some of these studies have not been ableto control for differences in a number of demographic,medical, and behavioral health risk factors that may beassociated with both depression and the risk of deathand thus might confound this relationship. However,Schulz et al.18 and Covinsky et al.14 found a statisticallysignificant relationship between increased depressivesymptoms and mortality after adjustment for comor-bidity, functional impairment, and cognitive impair-ment. A subset of studies has focused on the relation-ship of depression and cardiovascular mortality or the

Depressive Symptoms and Mortality
522 Am J Geriatr Psychiatry 10:5, September-October 2002
relationship between depression and mortality in pa-tients with cardiovascular disease. These studies havereported significant associations between depressionand mortality.20–25
In this report, we describe the results of a 7-yearprospective study of 2,558 older adults in a staff modelhealth maintenance organization (HMO). Our study hasthe following objectives:
1. To examine the association between depressionand subsequent mortality.
2. To examine the association between depressionand mortality in patients with preexisting cardiacdisease.
3. To examine whether these associations remain sig-nificant after adjusting for other known risk fac-tors.
METHODS
This report is based on a secondary data analysis of arandomized controlled trial that evaluated the cost-ef-fectiveness of preventive services for older enrollees inan HMO. The study was conducted by Patrick and col-leagues between 1989 and 1993 and has been reportedelsewhere.26–29 It was approved by the Institutional Re-view Boards of the University of Washington and theGroup Health Cooperative of Puget Sound. All subjectsgave informed consent.
Study Setting
Subjects were recruited from all HMO enrolleesover 65 who were receiving their care in one of fouroutpatient clinics of the Group Health Cooperative ofPuget Sound (GHC). GHC is a large-staff model HMOserving approximately 400,000 residents of westernWashington State, including 45,000 Medicare enrollees.The HMO provides medical and specialty mental healthservices using salaried staff providers.
Study Subjects
A total of 5,012 Medicare enrollees from four clinicsof the HMO were invited to participate in the originalstudy; 2,558 members (51%) consented to participateand were successfully randomized to a treatment and acontrol group. Those who did not participate in the
study were somewhat older, lived further away from theclinic, had a higher level of chronic medical illness, andhad a higher number of outpatient visits in the yearbefore the study.28 The treatment group received apackage of preventive services that included a visit witha health-promotion nurse, follow-up visits with theirprimary care clinician, and invitations to attend health-promotion classes targeted to each individual’s healthrisk factors. The control group received usual care bytheir primary care physicians. About 90% of those inthe intervention group had intervention-related health-promotion and disease-prevention visits in the first yearof the intervention.27 When compared with usual care,the intervention was not associated with lasting im-provements in health status or health-related quality oflife, but it was associated with slightly higher mortalityover 4 years.26,27 For the purpose of this secondary dataanalysis, we included subjects from both the interven-tion and the control group in the analyses. Because ear-lier analyses26,27 had found a higher mortality rate inintervention patients, we included intervention statusas a covariate in our survival analyses to adjust for thepotential effect of the intervention on mortality.
Measures
All subjects completed a mail survey and a 30-min-ute telephone interview at baseline in 1989. The mailsurveys collected information on demographics, healthstatus, chronic medical illnesses, and depressive symp-toms. Severity of depression was measured with theCenter for Epidemiological Studies Depression Scale(CES–D).30 This is a 20-item self-rating scale that wasdeveloped to screen for depression in primary care set-tings. Its reliability and validity have been found to begood when used for this purpose,31,32 and the scale hasalso been used to measure changes in depressive symp-toms over time.33 For the purpose of our analyses, wedefined four subject groups by depression severity: 1) agroup of patients with little or no depression (CES–D�16), using a cutoff of 16, as recommended by Radloff30
and Myers and Weissman31 to define a significant level ofdepression; 2) a group of patients with mild depression(CES–D 16–20); 3) a group of patients with moderatedepression (CES–D 21–26), based on a cutoff of 21 sug-gested in earlier work by Lyness and colleagues;34 and 4)the 3% of participants with the most severe depressivesyndrome (CES–D �26).
We used two methods to assess the extent of co-

Unutzer et al.
Am J Geriatr Psychiatry 10:5, September-October 2002 523
morbid chronic medical illness. We asked all partici-pants whether a doctor had told them that they hadone or more of eight chronic medical conditions. Theseincluded bronchitis or emphysema, arthritis or rheu-matism, high blood pressure, heart disease, stroke, can-cer, diabetes, or chronic foot problems (i.e., bunions oringrown toenails). We also used the HMO’s automatedpharmacy data from the year before enrollment into thestudy to calculate a “chronic disease score” accordingto a method developed by Von Korff and colleagues.35
This score classifies each patient according to the num-ber of medications used to treat chronic medical con-ditions, and it is therefore a measure of recognized andtreated medical illness. Psychotropic medications andmedications used primarily for symptom management(e.g., analgesics) are not included in the index. In pre-vious research in the GHC population, the chronic dis-ease score was strongly correlated with physician rat-ings of physical disease severity; it predicted mortalityand hospital use over the subsequent year.35
We also inquired about a number of other healthrisk factors. Excessive alcohol use was defined as threedrinks or more per day, following the approach used byPenninx and colleagues.13 Body mass index (BMI) wascalculated from self-reported weights and heights, con-verted to the metric scale and then calculated as theweight in kilograms divided by the height in meterssquared, similar to the approach used by Penninx etal.13 Smoking risk was defined as currently smoking orhaving recently quit smoking (within the past 6months).36 Exercise risk is defined as no exercise/insuf-ficient exercise, defined as less than 20 minutes ofphysical activity at least 3 times per week.37 Nutritionrisk was defined as having greater than 40% of dailycalories from fat or less than 19 grams of soluble fiberper day.38
We obtained information on mortality from the au-tomated data files of the HMO. These files are regularlyupdated from a database maintained by the state ofWashington. We were able to get mortality data on all2,558 study subjects through the end of 1996 (7 yearsafter study enrollment).
Statistical Analyses
We used t-tests and ANOVAs to examine the asso-ciation of demographic and clinical characteristics withdepression severity as measured by the CES–D score.We used Cox proportional-hazard regression models
with fixed covariates to study the association of de-pression severity, demographic, and clinical and healthrisk factors, and mortality over a 7-year follow-up pe-riod. First, we determined the unadjusted associationbetween depression severity and mortality. Second, wemeasured the unadjusted association between demo-graphic, clinical, and health risk factors and mortality.Clinical and demographic factors to be entered into thefinal model were chosen on the basis of p values �0.25in univariate Cox regression models. Excessive alcoholuse, nutrition risk, and chronic foot trouble had p values�0.25 and therefore were left out of the final model.Adjusted and unadjusted relative risks of death were ob-tained using Cox proportional-hazard regression mod-els. The survival probabilities for the four severitygroups, controlling for the effects of the covariates,were also obtained to plot the survival curves. We ex-amined the first-order interactions of depression sever-ity and all other covariates in the final model, and noneof the interactions tested were statistically significant.The proportionality assumption was tested for all themodels. All variables met the proportional-hazards as-sumption. The final model measures the association be-tween depression severity and mortality, controlling fordemographic characteristics as well as clinical andhealth risk factors.
Adjustment for Comorbid Medical Illness
We modeled the severity of comorbid medical ill-ness in three ways. First, we entered all seven condi-tions that were significantly associated with mortality inunivariate analyses in the regression model. In anothermodel, we entered a summary score (0–8) of the totalnumber of self-reported chronic illnesses, and, in a thirdmodel, we entered the chronic disease score.35 The as-sociation of depression and mortality was not sensitiveto the particular method used to control for chronicmedical illness. Therefore, we present the final modelusing the seven individual medical conditions.
RESULTS
The mean age of the 2,558 GHC members who enrolledinto the study in 1989 was 73 years (standard deviation[SD]: 5.5). The group was 61% female and 97% Cauca-sian. They exceeded the national average in total yearsof education (13; SD: 2.8) and mean household income
Depressive Symptoms and Mortality
524 Am J Geriatr Psychiatry 10:5, September-October 2002
TABLE 1. Association between baseline samplecharacteristics and CES–D score
% F[df] (p)
Age-group65–70 41.4% 15.22[2] (0.0001)71–75 30.6%�75 28%
EducationLess than high school 19.2% 17.61[3] (0.0001)High school graduate 26.3%Some college 35.5%College 18.9%
Body Mass Index�20 9.2% 5.03[2] (0.0066)20–28 68%�28 22.8%
t[df] (p)
SexMale 39% �6.5[2282] (0.0001)Female 61%
Marital statusMarried 64.3% 7.33[1687] (0.0001)Not married 35.7%
Intervention group 50.1% �1.43[2556] (0.1534)
Chronic diseasesBronchitis or emphysema 10.5% �6.02[313] (0.0001)Arthritis or rheumatism 51% �5.61[2552] (0.0001)High blood pressure 29.4% �2.94[1266] (0.0033)Heart disease 16.3% �3.58[2547] (0.0003)Stroke 2.9% �3.85[77] (0.0002)Cancer 8.2% �1.46[2547] (0.1446)Diabetes 6.1% �2.93[2549] (0.0035)Chronic foot trouble 29.3% �5.89[1210] (0.0001)
Excessive alcohol use 6.5% �1.39[182] (0.1675)Exercise risk 60.9% �1.22[2556] (0.2242)Smoking risk 9.2% �2.96[274] (0.0033)Nutrition risk 58.8% 3.34[2151] (0.0008)
Note: CES–D: Center for Epidemiological Studies DepressionScale.
($22,300; SD: $13,000, in 1989 dollars). At baseline,64% were married, and 30% were living alone; 82% ofthe subjects described their overall health as “excellent,very good, or good,” and, on average, subjects reported1.5 (SD: 1.2) of eight chronic medical conditions. Themean CES–D score at baseline was 8.6 (SD: 7.2); 86%of subjects (2,199/2,558) had no significant depression(CES–D �16); 14% (359/2,558) met criteria for a clini-cally significant depressive syndrome (CES–D �16);7.6% (194/2,558) had mild depression (CES–D 16–20);3.2% (83/2,558) had moderate depression (CES–D 21–26); and 3.2% (82/2,558) had severe depression (CES–D�26). Table 1 shows the association between baselinesample characteristics and CES–D score.
Depression and Mortality
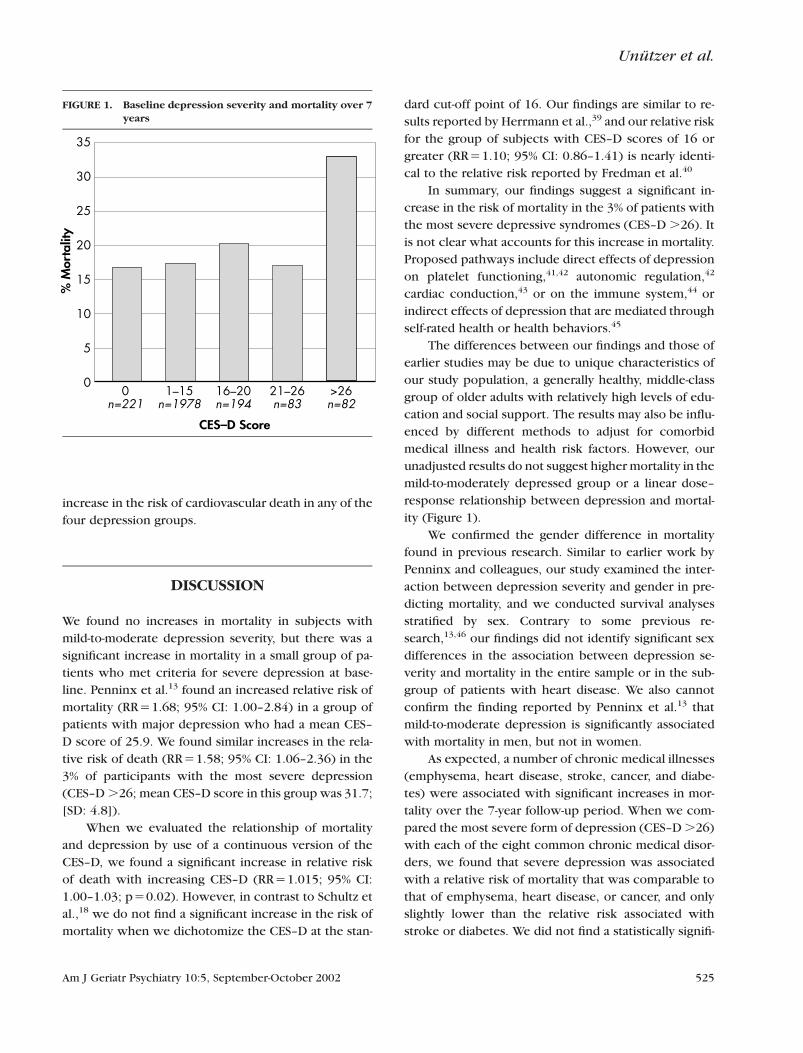
There were 460 deaths from all causes in our studycohort, including 215 deaths from cardiovascular dis-eases. Our unadjusted regression models indicate thatsubjects with mild-to-moderate depression had nohigher risk of dying over the 7-year observation periodthan those without significant depression. The groupwith severe depression (CES–D �26), however, had astatistically significant increase in the relative risk (RR)of dying (RR�2.12; 95% confidence interval [CI]: 1.44–3.14) compared with the group who had no significantdepression. Mortality varied from 17% to 20% in all butthe most severely depressed group, which had a mor-tality rate of 33% (Figure 1).
Other factors that were significantly associatedwith mortality included age, sex, marital status, smok-ing, BMI, and a number of chronic medical diseases,including emphysema, hypertension, heart disease,stroke, cancer, and diabetes. The chronic disease scoreand the sum of the eight self-reported chronic medicalillnesses were also significantly associated with mortal-ity. As reported previously,26,27 intervention groupstatus was also associated with mortality, with the sub-jects assigned to the intervention group experiencing aslightly higher relative risk of mortality (RR�1.19; 95%CI: 1.01–1.38).
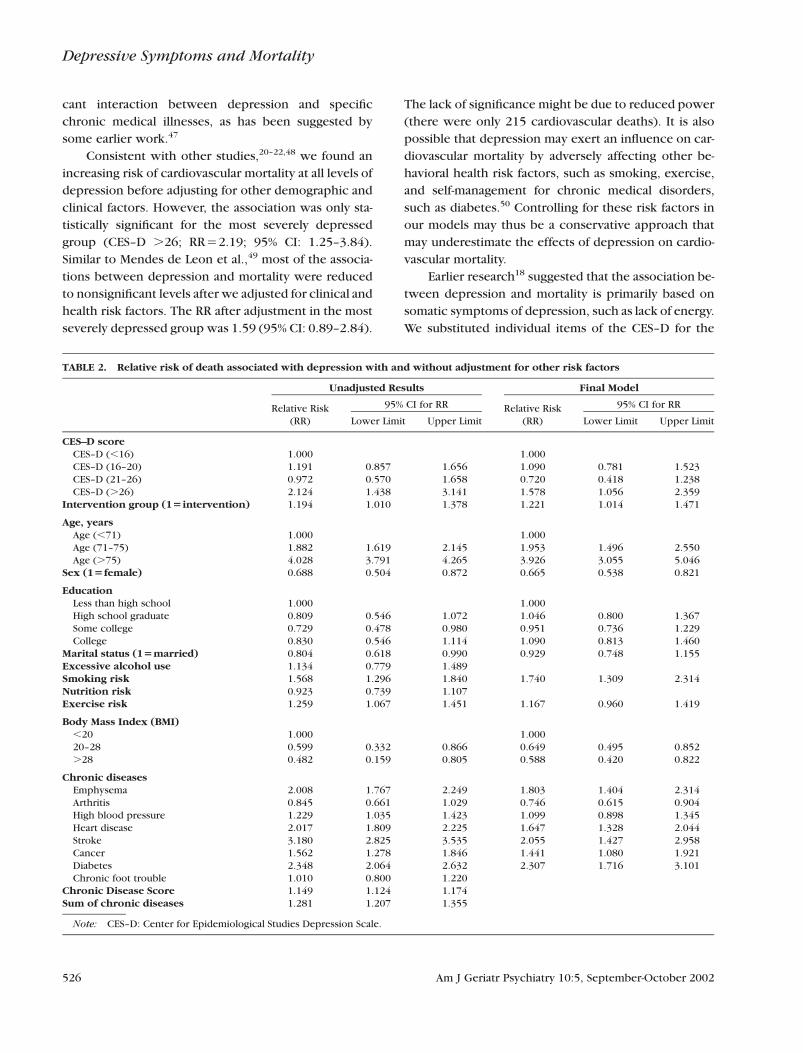
Our final model included the four depressiongroups, intervention group, age, sex, education, maritalstatus, and all clinical factors that had an associationwith mortality with a p �0.25 in the univariate analyses.In the final model (Table 2), we confirmed our findingsfrom univariate analyses that there is no significant in-crease in all-cause mortality associated with mild-to-
moderate depression, but that there is a significant in-
crease in the relative risk of mortality for the 3% with
the most severe depressive syndromes (CES–D �26).
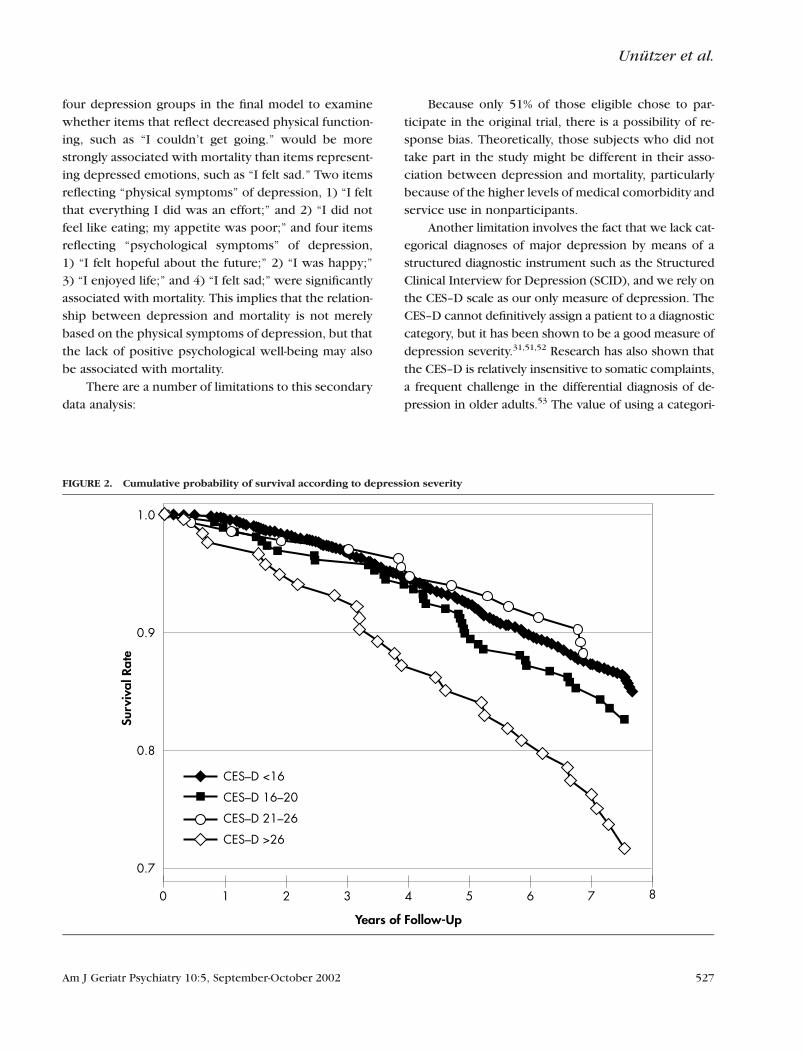
Figure 2 shows the proportion of patients in the
four depression severity groups who died during the 7-
year follow-up period.
Because earlier research had suggested that depres-
sion might be particularly associated with mortality in
patients with cardiovascular disease, we examined the
risk of mortality in the group of 416 people with heart
disease at baseline. We found a relative risk of death of
2.19 (95% CI: 1.07–4.50) in the group with severe de-
pression, compared with those without significant de-
pression. We also examined the risk of cardiovascular
mortality in all subjects, and we did not find a significant
Unutzer et al.
Am J Geriatr Psychiatry 10:5, September-October 2002 525
FIGURE 1. Baseline depression severity and mortality over 7years
% M
orta
lity
CES–D Score
00 1–15 16–20 21–26 >26
n=221 n=1978 n=194 n=83 n=82
5
10
15
20
25
30
35
increase in the risk of cardiovascular death in any of thefour depression groups.
DISCUSSION
We found no increases in mortality in subjects withmild-to-moderate depression severity, but there was asignificant increase in mortality in a small group of pa-tients who met criteria for severe depression at base-line. Penninx et al.13 found an increased relative risk ofmortality (RR�1.68; 95% CI: 1.00–2.84) in a group ofpatients with major depression who had a mean CES–D score of 25.9. We found similar increases in the rela-tive risk of death (RR�1.58; 95% CI: 1.06–2.36) in the3% of participants with the most severe depression(CES–D �26; mean CES–D score in this group was 31.7;[SD: 4.8]).
When we evaluated the relationship of mortalityand depression by use of a continuous version of theCES–D, we found a significant increase in relative riskof death with increasing CES–D (RR�1.015; 95% CI:1.00–1.03; p�0.02). However, in contrast to Schultz etal.,18 we do not find a significant increase in the risk ofmortality when we dichotomize the CES–D at the stan-
dard cut-off point of 16. Our findings are similar to re-sults reported by Herrmann et al.,39 and our relative riskfor the group of subjects with CES–D scores of 16 orgreater (RR�1.10; 95% CI: 0.86–1.41) is nearly identi-cal to the relative risk reported by Fredman et al.40
In summary, our findings suggest a significant in-crease in the risk of mortality in the 3% of patients withthe most severe depressive syndromes (CES–D �26). Itis not clear what accounts for this increase in mortality.Proposed pathways include direct effects of depressionon platelet functioning,41,42 autonomic regulation,42
cardiac conduction,43 or on the immune system,44 orindirect effects of depression that are mediated throughself-rated health or health behaviors.45
The differences between our findings and those ofearlier studies may be due to unique characteristics ofour study population, a generally healthy, middle-classgroup of older adults with relatively high levels of edu-cation and social support. The results may also be influ-enced by different methods to adjust for comorbidmedical illness and health risk factors. However, ourunadjusted results do not suggest higher mortality in themild-to-moderately depressed group or a linear dose–response relationship between depression and mortal-ity (Figure 1).
We confirmed the gender difference in mortalityfound in previous research. Similar to earlier work byPenninx and colleagues, our study examined the inter-action between depression severity and gender in pre-dicting mortality, and we conducted survival analysesstratified by sex. Contrary to some previous re-search,13,46 our findings did not identify significant sexdifferences in the association between depression se-verity and mortality in the entire sample or in the sub-group of patients with heart disease. We also cannotconfirm the finding reported by Penninx et al.13 thatmild-to-moderate depression is significantly associatedwith mortality in men, but not in women.
As expected, a number of chronic medical illnesses(emphysema, heart disease, stroke, cancer, and diabe-tes) were associated with significant increases in mor-tality over the 7-year follow-up period. When we com-pared the most severe form of depression (CES–D �26)with each of the eight common chronic medical disor-ders, we found that severe depression was associatedwith a relative risk of mortality that was comparable tothat of emphysema, heart disease, or cancer, and onlyslightly lower than the relative risk associated withstroke or diabetes. We did not find a statistically signifi-
Depressive Symptoms and Mortality
526 Am J Geriatr Psychiatry 10:5, September-October 2002
TABLE 2. Relative risk of death associated with depression with and without adjustment for other risk factors
Unadjusted Results Final Model
Relative Risk 95% CI for RR Relative Risk 95% CI for RR
(RR) Lower Limit Upper Limit (RR) Lower Limit Upper Limit
CES–D scoreCES–D (�16) 1.000 1.000CES–D (16–20) 1.191 0.857 1.656 1.090 0.781 1.523CES–D (21–26) 0.972 0.570 1.658 0.720 0.418 1.238CES–D (�26) 2.124 1.438 3.141 1.578 1.056 2.359
Intervention group (1�intervention) 1.194 1.010 1.378 1.221 1.014 1.471
Age, yearsAge (�71) 1.000 1.000Age (71–75) 1.882 1.619 2.145 1.953 1.496 2.550Age (�75) 4.028 3.791 4.265 3.926 3.055 5.046
Sex (1�female) 0.688 0.504 0.872 0.665 0.538 0.821
EducationLess than high school 1.000 1.000High school graduate 0.809 0.546 1.072 1.046 0.800 1.367Some college 0.729 0.478 0.980 0.951 0.736 1.229College 0.830 0.546 1.114 1.090 0.813 1.460
Marital status (1�married) 0.804 0.618 0.990 0.929 0.748 1.155Excessive alcohol use 1.134 0.779 1.489Smoking risk 1.568 1.296 1.840 1.740 1.309 2.314Nutrition risk 0.923 0.739 1.107Exercise risk 1.259 1.067 1.451 1.167 0.960 1.419
Body Mass Index (BMI)�20 1.000 1.00020–28 0.599 0.332 0.866 0.649 0.495 0.852�28 0.482 0.159 0.805 0.588 0.420 0.822
Chronic diseasesEmphysema 2.008 1.767 2.249 1.803 1.404 2.314Arthritis 0.845 0.661 1.029 0.746 0.615 0.904High blood pressure 1.229 1.035 1.423 1.099 0.898 1.345Heart disease 2.017 1.809 2.225 1.647 1.328 2.044Stroke 3.180 2.825 3.535 2.055 1.427 2.958Cancer 1.562 1.278 1.846 1.441 1.080 1.921Diabetes 2.348 2.064 2.632 2.307 1.716 3.101Chronic foot trouble 1.010 0.800 1.220
Chronic Disease Score 1.149 1.124 1.174Sum of chronic diseases 1.281 1.207 1.355
Note: CES–D: Center for Epidemiological Studies Depression Scale.
cant interaction between depression and specificchronic medical illnesses, as has been suggested bysome earlier work.47
Consistent with other studies,20–22,48 we found anincreasing risk of cardiovascular mortality at all levels ofdepression before adjusting for other demographic andclinical factors. However, the association was only sta-tistically significant for the most severely depressedgroup (CES–D �26; RR�2.19; 95% CI: 1.25–3.84).Similar to Mendes de Leon et al.,49 most of the associa-tions between depression and mortality were reducedto nonsignificant levels after we adjusted for clinical andhealth risk factors. The RR after adjustment in the mostseverely depressed group was 1.59 (95% CI: 0.89–2.84).
The lack of significance might be due to reduced power(there were only 215 cardiovascular deaths). It is alsopossible that depression may exert an influence on car-diovascular mortality by adversely affecting other be-havioral health risk factors, such as smoking, exercise,and self-management for chronic medical disorders,such as diabetes.50 Controlling for these risk factors inour models may thus be a conservative approach thatmay underestimate the effects of depression on cardio-vascular mortality.
Earlier research18 suggested that the association be-tween depression and mortality is primarily based onsomatic symptoms of depression, such as lack of energy.We substituted individual items of the CES–D for the
Unutzer et al.
Am J Geriatr Psychiatry 10:5, September-October 2002 527
FIGURE 2. Cumulative probability of survival according to depression severity
Surv
ival
Rat
e
Years of Follow-Up
1.0
0.9
0.8
0.7
80 1 2 3 54 6 7
CES–D >26
CES–D 21–26
CES–D 16–20
CES–D <16
four depression groups in the final model to examinewhether items that reflect decreased physical function-ing, such as “I couldn’t get going.” would be morestrongly associated with mortality than items represent-ing depressed emotions, such as “I felt sad.” Two itemsreflecting “physical symptoms” of depression, 1) “I feltthat everything I did was an effort;” and 2) “I did notfeel like eating; my appetite was poor;” and four itemsreflecting “psychological symptoms” of depression,1) “I felt hopeful about the future;” 2) “I was happy;”3) “I enjoyed life;” and 4) “I felt sad;” were significantlyassociated with mortality. This implies that the relation-ship between depression and mortality is not merely
based on the physical symptoms of depression, but that
the lack of positive psychological well-being may also
be associated with mortality.
There are a number of limitations to this secondary
data analysis:
Because only 51% of those eligible chose to par-ticipate in the original trial, there is a possibility of re-sponse bias. Theoretically, those subjects who did nottake part in the study might be different in their asso-ciation between depression and mortality, particularlybecause of the higher levels of medical comorbidity andservice use in nonparticipants.
Another limitation involves the fact that we lack cat-egorical diagnoses of major depression by means of astructured diagnostic instrument such as the StructuredClinical Interview for Depression (SCID), and we rely onthe CES–D scale as our only measure of depression. TheCES–D cannot definitively assign a patient to a diagnostic
category, but it has been shown to be a good measure of
depression severity.31,51,52 Research has also shown that
the CES–D is relatively insensitive to somatic complaints,
a frequent challenge in the differential diagnosis of de-
pression in older adults.53 The value of using a categori-

Depressive Symptoms and Mortality
528 Am J Geriatr Psychiatry 10:5, September-October 2002
cal, rather than a dimensional, approach to assessing de-pression has been debated in the literature.11 In recentyears, data from the Medical Outcomes Study54,55 andother work56–59 have shown that patients with sub-threshold depressive syndromes that fall short of DSMseverity criteria for major depression have substantiallimitations in functioning and quality of life.
Half of the study participants were assigned to a pre-ventive intervention. Baseline depression levels were notsignificantly different among patients and control sub-jects, but it is theoretically possible that the interventionaffected mortality by decreasing depression severity. Wedo not believe that this is likely, however, because moreintervention patients than control patients died duringthe 7-year study follow-up. We included interventionstatus as a covariate in our survival analyses to adjust forthe effect of the intervention on mortality.
Although we have made substantial efforts to con-trol for health risk factors such as comorbid medicalillness and health risk behaviors, it is possible that thereare unaccounted-for differences in other health risk fac-tors associated with both depression and mortality thatmight be responsible for the increased relative risk ofdepression we observed in our group of severely de-pressed patients. However, the inclusion of health riskbehaviors in our models might also underestimate therelative risk associated with having severe depression.Depression may directly affect such health risk behav-iors as smoking or adherence to special diets in patientswith diabetes.50
We rely on patient self-reports of chronic medicalillness, and it is possible that depressed patients weremore likely to report comorbid medical illnesses thanthose who were not depressed. This could lead to anunderestimate of the association between depressionand mortality. However, when we replaced the self-reported chronic illnesses in our model with thechronic disease score, a more objective measure ofchronic medical illness,35 we also did not find increasedmortality rates except in the small group of severelydepressed patients.
We do not have information on specific causes ofdeath, with the exception of the distinction betweencardiovascular and other deaths. It is possible, for ex-ample, that suicide accounts for some of the deathsamong the depressed patients, but we do not have anaccurate estimate of this. In all but one of the 26 com-munity and medical samples reviewed by Wulsin,19 sui-cide accounts for less than 1% of reported mortality. A
recent study by Simon et al.60 also found that suicideaccounted for an exceedingly small fraction of overallmortality in a large sample of depressed primary carepatients from the same HMO.
Our findings are based on the association betweendepression at baseline and mortality over a 7-year pe-riod, but the severity of depression may have variedsubstantially during the 7-year follow-up. More researchis needed to look at the relationship between mortalityand exposure to depression over time. Wassertheil-Smoller et al.,61 for example, found no association be-tween baseline depression scores and mortality in agroup of hypertensive patients, whereas they found thatan increase in depression scores over time predictedmortality.
On the basis of this study, we cannot conclude thattreating depression in this population of older adultswould reduce mortality. Data suggesting an increasedmortality risk associated with depression do, however,add to the growing evidence regarding the burden ofdepression in older adults. In earlier research with thisgroup, we demonstrated that even moderate levels ofdepression were associated with substantial losses inhealth-related quality of life,12 but that only a small mi-nority of patients in this cohort received any treatmentfor depression.62 Only 4% of the patients in the entiresample and 10% of those with clinically significant de-pressive syndromes received any treatment for depres-sion during a 1-year period surrounding the assessmentof depression.62 Even when patients were treated fordepression, the intensity of treatments was generally be-low levels suggested by available treatment guidelines.While we await definitive information regarding de-pression and mortality, sufficient reasons exist to makerecognition and treatment of depression in older adultsa priority. There is good evidence for the efficacy ofboth antidepressant medications and psychotherapiesin the treatment of late-life depression,1,63 and a numberof studies (including an unpublished one by two of thecurrent authors [Unutzer et al.]) are currently underway to test the effectiveness of population-based inter-vention models for depression in late life.6465
This research was funded by the Health Care Fi-nancing Administration (HCFA) under CooperativeAgreement No. 95-C-99161 to the University of Wash-ington and Group Health Cooperative of Puget Sound,and by a grant from the W.K. Kellog Foundation toGroup Health Cooperative of Puget Sound.
Unutzer et al.
Am J Geriatr Psychiatry 10:5, September-October 2002 529
References
1. Lebowitz MD: Age, period, and cohort effects: influences on dif-ferences between cross-sectional and longitudinal pulmonaryfunction results. Am J Respir Crit Care Med 1996; 154:S273–S277
2. Craig TJ, Van Natta PA: Disability and depressive symptoms intwo communities. Am J Psychiatry 1983; 140:598–601
3. Kennedy GJ, Kelman HR, Thomas C: The emergence of depres-sive symptoms in late life: the importance of declining healthand increasing disability. J Community Health 1990; 15:93–104
4. Gurland BJ, Wilder DE, Berkman C: Depression and disability inthe elderly: reciprocal relations and changes with age. Int J Ger-iatr Psychiatry 1988; 3:163–179
5. Bruce ML, Seeman TE, Merrill SS, et al: The impact of depressivesymptomatology on physical disability: MacArthur Studies of Suc-cessful Aging. Am J Public Health 1994; 84:1796–1799
6. Forell Y, Jorm AF, Winblad B: Association of age, sex, cognitivedysfunction, and disability with depressive symptoms in an el-derly sample. Am J Psychiatry 1994; 151:1600–1604
7. Alexopoulos GS, Vrontou C, Kakuma T, et al: Disability in geri-atric depression. Am J Psychiatry 1996; 153:877–885
8. Unutzer J, Patrick DL, Diehr P, et al: Quality-adjusted life-years inolder adults with depressive symptoms and chronic medical dis-orders. Int Psychogeriatr 2000a; 12:15–33
9. Murphy E: The prognosis of depression in old age. Br J Psychiatry1983; 142:111–119
10. Baldwin RC: The outcome of depression in old age, special issue:affective disorders in old age. Int J Geriatr Psychiatry 1991;6:395–400
11. Alexopoulos GS: Methodology of treatment studies in geriatricdepression. Am J Geriatr Psychiatry 1995; 3:280–289
12. Unutzer J, Patrick D, Simon G, et al: Depressive symptoms andthe cost of health services in HMO patients age 65 and over: afour-year prospective study. JAMA 1997; 277:1618–1623
13. Penninx BW, Geerlings SW, Deeg DJH, et al: Minor and majordepression and the risk of death in older persons. Arch Gen Psy-chiatry 1999; 56:889–895
14. Covinsky KE, Kahana E, Chin MH, et al: Depressive symptomsand three-year mortality in older hospitalized medical patients.Paper presented at the Annual Meeting of the Society of GeneralInternal Medicine, Chicago, IL, 1998
15. Pulska T, Pahkala K, Laippala P, et al: Six-year survival of de-pressed elderly Finns: a community study. Int J Geriatr Psychiatry1997; 12:942–950
16. Whooley MA, Browner WS: Association between depressivesymptoms and mortality in older women. Arch Intern Med 1998;158:2129–2135
17. Murray CJL, Lopez AD: Global mortality, disability, and the con-tribution of risk factors: Global Burden of Disease study. Lancet1997; 349:1436–1442
18. Schulz R, Beach SR, Ives DG, et al: Association between depres-sion and mortality in older adults. Arch Intern Med 2000; 160:1761–1768
19. Wulsin LR: Does depression kill? Arch Intern Med 2000; 160:1731–1732
20. Barefoot JC, Helms MJ, Mark DB, et al: Depression and long-termmortality risk in patients with coronary artery disease. Am J Car-diol 1996; 78:613–617
21. Barefoot JC, Schroll M: Symptoms of depression, acute myocar-dial infarction, and total mortality in a community sample. Cir-culation 1996; 93:1976–1980
22. Murberg TA, Bru E, Svebak S, et al: Depressed mood and subjec-
tive health symptoms as predictors of mortality in patients withcongestive heart failure: a two-year follow-up study. Int J Psychi-atry Med 1999; 29:311–326
23. Frasure-Smith N, Lesperance F, Juneau M, et al: Gender, depres-sion, and one-year prognosis after myocardial infarction. Psycho-som Med 1999; 61:26–37
24. Frasure-Smith N, Lesperance F, Talajic M: Depression followingmyocardial infarction. JAMA 1993; 270:1819–1825
25. Kaufmann MW, Fitzgibbons JP, Sussman EJ, et al: Relation be-tween myocardial infarction, depression, hostility, and death. AmHeart J 1999; 138:549–554
26. Patrick DL, Beresford SA, Ehreth J, et al: Interpreting excess mor-tality in a prevention trial for older adults. Int J Epidemiol 1995;24(suppl1):S27–S33
27. Patrick DL, Grembowski DE, Durham ML, et al: Cost and out-comes of Medicare reimbursement for HMO preventive services.Health Care Financing Review 1999; 20:25–43
28. Durham ML, Beresford S, Diehr P, et al: Participation of higherusers in a randomized trial of Medicare reimbursement for pre-ventive services. Gerontologist 1991; 31:603–606
29. Grembowski D, Patrick D, Diehr P, et al: Self-efficacy and healthbehavior among older adults. J Health Soc Behav 1993; 34:89–104
30. Radloff LS: The CES–D Scale: a self-report depression scale forresearch in the general population. Applied Psychological Mea-surement 1977; 1:385–401
31. Myers JK, Weissman MM: Use of a self-report symptoms scale todetect depression in a community sample. Am J Psychiatry 1980;137:1081–1084
32. Husaini BA, Neff JA, Harrington JB, et al: Depression in ruralcommunities: validating the CES–D scale. J Community Psychia-try 1980; 8:20–27
33. Weissman MM, Sholomskas D, Pottenger M, et al: Assessing de-pressive symptoms in five psychiatric populations: a validationstudy. Am J Epidemiol 1977; 106:203–214
34. Lyness JM, Duberstein PR, King DA, et al: Medical illness burden,trait neuroticism, and depression in older primary care patients.Am J Psychiatry 1998; 155:969–971
35. Von Korff M, Wagner EH, Saunders K: A chronic disease scorefrom automated pharmacy data. J Clin Epidemiol 1992; 1:197–203
36. Adams PF, Benson V: Current estimates from the National HealthInterview survey. Vital Health Stat–10 1989; 176:1–221
37. Buchner DM, Reed RL, Pearlman RA: Risk factors for early un-planned hospital readmission in the elderly. J Gen Intern Med1991; 6:223–228
38. Kristal AR, Abrams BF, Thomquist MD, et al: Development andvalidation of a food use checklist for evaluation of communitynutrition interventions. Am J Public Health 1990; 80:1318–1322
39. Herrmann C, Brand-Driehorst S, Buss U, et al: Effects of anxietyand depression on 5-year mortality in 5,057 patients referred forexercise testing. J Psychosom Res 2000; 48:455–462
40. Fredman L, Magaziner J, Hebel JR, et al: Depressive symptomsand 6-year mortality among elderly community-dwelling women.Epidemiology 1999; 10:54–59
41. Nair GV, Gurbel PA, O’Connor CM, et al: Depression, coronaryevents, platelet inhibition, and serotonin reuptake inhibitors. AmJ Cardiol 1999; 84:321–323
42. Roose SP, Spatz E: Treatment of depression in patients with heartdisease. J Clin Psychiatry 1999; 60(suppl20):34–37

Depressive Symptoms and Mortality
530 Am J Geriatr Psychiatry 10:5, September-October 2002
43. Yeragani VK, Pohl R, Jampala VC, et al: Increased QT variabilityin patients with panic disorder and depression. Psychiatr Res2000; 93:225–235
44. Miller GE, Cohen S, Herbert TB: Pathways linking major depres-sion and immunology in ambulatory female patients. PsychosomMed 1999; 61:850–860
45. Idler EL, Benyamini Y: Self-rated health and mortality: a reviewof 27 community studies. J Health Soc Behav 1997; 38:21–37
46. Abbey SE, Stewart DE. Gender and psychosomatic aspects of is-chemic heart disease. J Psychosom Res 2000; 48:417–423
47. Black SA, Markides KS: Depressive symptoms and mortality inolder Mexican-Americans. Ann Epidemiol 1999; 9:45–52
48. Pokorski RJ: Mortality risk in patients with coronary artery diseaseand depression. Journal of Insurance Medicine 1999; 31:4–7
49. Mendes de Leon CF, Krumholz HM, Seeman TS, et al: Depressionand risk of coronary heart disease in elderly men and women:New Haven EPESE, 1982–1991. Established Populations for theEpidemiologic Studies of the Elderly. Arch Intern Med 1999;158:2341–2348
50. Ciechanowski P, Katon W: Depression and diabetes: impact ofdepressive symptomatology on adherence, function, and costs.Arch Internal Med 2000; 160:3278–3285
51. Zich JM, Attkisson CC, Greenfield TK: Screening for depressionin primary care clinics: the CES–D and the BDI. Int J PsychiatryMed 1990; 20:259–277
52. Wetzler S, Van Praag HM: Assessment of depression, in MeasuringMental Illness. Edited by Wetzler S. Washington, DC, AmericanPsychiatric Press, 1989, pp 71–88
53. Foelker GA Jr, Shewchuck RM: Somatic complaints and the CES–D. J Am Geriatr Soc 1992; 40:259–262
54. Wells KB, Burnam MA, Rogers W, et al: The course of depressionin adult outpatients: results from the Medical Outcomes Study.Arch Gen Psychiatry 1992; 49:788–794
55. Hays RD, Wells KB, Donald Sherbourne C, et al: Functioning andwell-being outcomes of patients with depression compared withchronic general medical illnesses. Arch Gen Psychiatry 1995;52:11–19
56. Broadhead WE, Blazer DG, George LK, et al: Depression, disabil-ity days, and days lost from work in a prospective epidemiolog-ical survey. JAMA 1990; 264:2525–2528
57. Horwath E, Johnson J, Klerman GL, et al: Depressive symptomsas relative and attributable risk factors for first-onset major de-pression. Arch Gen Psychiatry 1992; 49:817–823
58. Kennedy GJ, Kelman HR, Thomas C: Persistence in remission ofdepressive symptoms in late life. Am J Psychiatry 1991; 148:174–178
59. Katz IR, Parmelee PA, Streim JE: Depression in older patients inresidential care: significance of dysphoria and dimensional as-sessment. Am J Geriatr Psychiatry 1995; 3:161–169
60. Simon GE, Von Korff M, Barlow W: Health care costs of primarycare patients with recognized depression. Arch Gen Psychiatry1995; 52:850–856
61. Wassertheil-Smoller S, Applegate WB, Berge K, et al: Change indepression as a precursor of cardiovascular events: SHEP Coop-erative Research Group (Systolic Hypertension in the Elderly).Arch Intern Med 1996; 156:553–561
62. Unutzer J, Simon G, Belin TR, et al: Care for depression in HMOpatients age 65 and older. J Am Geriatr Soc 2000; 48:871–878
63. Unutzer J, Katon WJ, Sullivan M, et al: Treating depressed olderadults in primary care: narrowing the gap between efficacy andeffectiveness. Milbank Q 1999; 77:225–256
64. Katz IR, Coyne JC: The public health model of mental health carefor the elderly. JAMA 2000; 283:2844–2845
65. Unutzer J, Katon W, Williams JW Jr, et al: Improving primary carefor depression in late life: the design of a multicenter randomizedtrial. Med Care 2001; 39:785–799