Embed Size (px)
Citation preview
INTERNATIONAL JOURNAL OF GERIATRIC PSYCHIATRY
Int J Geriatr Psychiatry 2008; 23: 1306–1311.
Published online 9 July 2008 in Wiley InterScience
(www.interscience.wiley.com) DOI: 10.1002/gps.2070
Depressive symptoms and suicidal ideation among olderadults receiving home delivered meals
Jo Anne Sirey1*, Martha L. Bruce1, Mae Carpenter3, Diane Booker3, M. Carrington Reid2,Kerry-Ann Newell1 and George S. Alexopoulos1
1Department of Psychiatry, Weill Medical College of Cornell University, NY, USA2Departments of Geriatrics and Gerontology, Weill Medical College of Cornell University, NY, USA3Westchester Department of Senior Programs and Services, NY, USA
SUMMARY
Objective Homebound older adults may be vulnerable to the deleterious impact of untreated depression. Yet because theseelders are difficult to reach, there is little data on the rates of depressive symptoms and suicidal ideation among this group.The objective of this study is to document the rates of depression and correlates among a population of homebound elders.Methods Using a community based participatory research partnership, we implemented a routine screening for depressivesymptoms and suicidal ideation among older recipients of Westchester County’s home meal program. Older adults enrolledin the home delivered meal program were administered the Physician Health Questionnaire–9 (PHQ-9), and questions toassess pain, falls, alcohol abuse and perceived emotional distress.Results In our sample of 403 meal recipients, 12.2% of older adults reported clinically significant depression (PHQ-9> 9)and 13.4% reported suicidal thoughts. One-third of recipients with significant depressive symptoms were currently taking anantidepressant. Almost one-third of older adults who endorsed suicide ideation did not report clinically significant depressivesymptoms. Among men, suicidal thoughts were associated with chronic pain and greater depression severity, whereas painwas not a predictor of suicidal thoughts among women.Conclusion More than one in nine elders suffer from depression; most are untreated with one-third undertreated. Throughpartnerships between public agencies that provide age related services and academic investigators there is an opportunity forimproved detection of unmet mental health needs. Future research should explore innovative models to improve access tomental health services once unmet need is detected. Copyright # 2008 John Wiley & Sons, Ltd.
key words—geriatric depression; suicide ideation; homebound; home delivered meals
INTRODUCTION
Depressive symptoms are common and depression isexpected to be second to heart disease in globaldisease burden (Chapman and Perry, 2008). Amongthe elderly, depressive symptoms usually occur in thecontext of multiple medical illnesses and disabilities(Alexopoulos, 2005). In primary care settings 6–8% ofpatients have major depression (Schulberg et al.,1998; Unutzer et al., 2000). One-quarter of patients inrehabilitation centers for respiratory diseases have
*Correspondence to: Dr J. A. Sirey, Department of Psychiatry,WeillMedical College of Cornell University, 21 Bloomingdale Rd, WhitePlains, NY 10605, USA. E-mail: [email protected]
Copyright # 2008 John Wiley & Sons, Ltd.
major depression (Borson et al., 1998; Koenig et al.,2006). Using a SCID diagnostic interview, over 14%of older medical patients have major depression andanother 20% have less severe forms of depression(Bruce et al., 2002). These rates are consistent withdata from other studies documenting one-quarter toone-third of elders receiving home services sufferfrom depression (Banerjee and Macdonald, 1996;Beekman et al., 2002b; Buys et al., 2008). Depressionamong community elders has an unremitting courseand is associated with greater disability, inappropriateservice use and mortality (Beekman et al., 2002a;Andreescu et al., 2008).
Despite improvements in routine screening anddetection of depression in mental health and primary
Received 14 August 2007Accepted 28 April 2008

depression and suicidal ideation among homebound elderly 1307
care settings, significant sub-pockets of high-risk olderadults are not reached (Bruce et al., 2005; Choi et al.,2007). These elders tend to be ‘hidden’ from view oftraditional care providers and face transportation,stigma and financial barriers to care (Bruce et al.,2005; Druss, 2006). As a consequence, their depres-sive symptoms often go untreated. For those reasons,alternative strategies are needed to integrate screeninginto other routine services provided to homeboundelders to ensure access to quality mental health carefor those in need.
To improve the detection of depression amonghomebound elders we developed a community-basedresearch partnership using the Evidence-BasedCommunity/Partnership Model proposed by Wellset al. (2004). This model relies on a partnershipbetween communities and researchers, blendingtechniques of community participatory research andevidence-based quality improvement programs. Itsgoal is to identify problems with both agency andpublic health significance, and to address them bytailoring evidence-based strategies to fit the con-straints, needs, and life circumstances of the targetedcommunity setting and developing alternativeapproaches that are sustainable.
The partnership developed an easily integrateddepression screening protocol to evaluate seniors whoreceive home delivered meals. The sociodemographicand clinical characteristics of this population putthem at high risk for depression while their home-bound status limits access to routine depressionscreening and treatment. The Administration onAging’s (AOA’s) Elderly Nutrition Program (ENP)serves about 3.1 million community dwelling olderadults (age� 60) annually. Compared to the elderlyUS population, older adults receiving meals tend tobe older, poorer, minority and live alone; they havegreater difficulty caring for themselves and haveincreased health and nutrition risks (Ponza et al.,1996; Administration on Aging, 2004; Sharkey, 2005)
In this paper we describe the rates of clinicallysignificant depressive symptoms and endorsement ofpassive and active suicidal ideation among seniorsreceiving home delivered meals. We hypothesized thatthe rates of depressive symptoms among this group ofhomebound elders would be comparable to the ratesdocumented in other populations of elders withcomplex medical illnesses and disabilities, such ashomecare and assisted living (Bruce et al., 2002;Gruber-Baldini et al., 2004). Additionally we hypoth-esized that the rates of depressive symptoms andsuicidal thoughts would be comparable across racialgroups and gender, and associated with chronic pain.
Copyright # 2008 John Wiley & Sons, Ltd.
METHODS
The study was supported by an NIH grant-fundedcollaboration between the Westchester CountyDepartment of Senior Programs and Services (DSPS),an AoA agency, and the Weill Cornell Institute forGeriatric Psychiatry (P30 MH68638). The partnershipdeveloped procedures that were consistent withDSPS’s system and utilized standardized methodsbrought by the academic research group. The analyseswere approved by the Weill Cornell Medical CollegeInternal Review Board.
Sample
A senior is eligible for the home meal program if thatindividual has a condition, due to illness or injury, thatrestricts the individual’s ability to leave the homeexcept with the assistance of another individual or theaid of a supportive device (such as a cane or awheelchair), or if the individual has a condition suchthat leaving his or her home is contraindicated. Eldersreceiving home meals who were eligible for acertification interview from December 2004–June2006 were eligible for the screening protocol. Wecontacted 523 elders consecutively for this wave ofour project.
Measures
Standardized questions to assess depressive symp-toms, cognitive status, alcohol abuse and the presenceof chronic pain were added to the meal certificationinterview. The Physician Health Questionnaire (PHQ-9) was added to assess depressive symptoms. ThePHQ-9 assesses the symptoms used to assess DSM-IVcriteria for Major Depressive Disorder (Kroenke andSpitzer, 2002). The frequency of each symptom israted on a four-point scale (‘from not at all’ to ‘nearlyevery day’). The scale is easy to administer and hasbeen used reliably by non-psychiatric interviewers inprimary care (Oxman et al., 2002; Lowe et al., 2004;Ell et al., 2005), home healthcare settings (Ell et al.,2005) and in community samples (Martin et al., 2006).Suicidal thoughts are assessed with a single item onthe PHQ-9 (e.g. ‘How often have you been botheredby thoughts that you would be better off dead orof hurting yourself in some way’). The PHQ-9 iswidely used because it offers a measure of symptomseverity, rates the pervasiveness of each symptom usedas criteria to establish DSM IV Major DepressiveDisorder, and has established treatment planningguidelines. Clinically significant, moderate depressive
Int J Geriatr Psychiatry 2008; 23: 1306–1311.
DOI: 10.1002/gps

1308 j. a. sirey ET AL.
symptoms (PHQ-9> 9) warrant the development of atreatment plan (Kroenk and Spitzer, 2002).In addition to the PHQ-9, interviewees were asked
whether they were experiencing depression or emotionaldistress. This measure of perceived distress comp-lements the formal assessment of depressive symptoms.Current antidepressant treatment was determined as partof the standard review of current medications.Cognitive functioning was assessed using the
Blessed Orientation, Memory and Concentration(BOMC) scale (Katzman et al., 1983) where cognitiveimpairment was defined as a score greater than 15(Bartels et al., 2004; Levkoff et al., 2004). Chronicpain was assessed using self-report questions toevaluate the presence of painful sensations for thepreceding 3 months (Elliot et al., 1999). Finally, theassessors administered the four-item CAGE to assessfor alcohol problems (Ewing, 1984) and recordedwhether the interviewee had sustained a fall in the last6 months.
Training and supervision
Training and supervision on the protocol measureswas provided by the academic collaborators. Monthlysupervision was provided to review administrationand scoring. Older adults with clinically significantsymptoms (PHQ-9> 9) were offered a referral formental health services. Elders who endorsed suicidalthoughts were administered our standardized riskprotocol (Raue et al., 2006).
Data analysis
Interviews were conducted from December 2004–June 2006 with all consecutive and willing elderseligible for a meal certification interview. Chi-squareanalyses and ANOVA comparisons were conductedto examine the relation of depressive symptoms (e.g.none, mild and moderate to severe) with socio-demographic factors, clinical characteristics (e.g.pain, alcohol use), and a recent fall.To identify a model of factors associated with
suicidal thoughts, we conducted a forward logisticregression analysis with the endorsement of suicidalthoughts as the dependent variable. Analyses con-trolled for other depressive symptoms (the sum of theremaining PHQ-9 items). Interaction terms werecreated to capture potential differences betweenmen and women in the relation of pain to suicidalthoughts. This approach was taken based on theliterature supporting gender differences in both the
Copyright # 2008 John Wiley & Sons, Ltd.
experience and impact of chronic pain across thelifespan (Unruh, 1996).
RESULTS
Data were available on 403 older adults receivinghome meals. The analytic sample represents 77% oftotal eligible meal recipients during the study period(n¼ 523). Seniors were excluded due to inability tounderstand the purpose of the interview due to severecognitive impairment (6%), being too medically ill(9%), or having a language barrier (1%). A smallnumber of older adults (7%) refused to be interviewed.There was no difference in the gender, race or age ofseniors who were and were not interviewed. Thedemographics for the sample are presented in Table 1.
Almost half (47%) of the elders endorsed chronicpain with an average duration of 5 years. In thesample, almost one-quarter (24%) sustained a fallwithin the last 6 months. Only one in five seniors(20%) reported having had an alcoholic drink in thelast month.
Depressive symptoms were common; more thanone-third (36%) of the sample reported being‘bothered by feeling down, depressed or hopeless’in the prior two weeks; 12% reported moderate tosevere depression symptoms (Kroenke and Spitzer,2002). An additional 17% had mild symptoms (PHQ-9scores 5–9). In sum, 29% of this sample of homeboundseniors reported at least mild symptoms of depression.
Correlates of depression
There were no differences in the prevalence of clinicallysignificant depressive symptoms associated with race,gender, age or years of education. There was asignificant relationship between chronic pain anddepression severity levels (x2¼ 16.25, df¼ 2, p<0.001) among the entire sample. The prevalence ofchronic pain was higher (69% vs 40%) among seniorsreporting moderate to severe depression as compared tothose elders without any depressive symptoms.
Almost one in five (19%) elders in this sample weretaking an antidepressant. Among the elders withmoderate to severe symptoms, one-third (33%) weretaking an antidepressant and still reported significantdepression. The remaining elders on antidepressantshad mild to no symptoms. Among the depressedseniors with significant symptoms, only half (51%)viewed themselves as suffering from emotionaldifficulties or depression. There was no relationbetween depressive symptoms and cognitive statusalcohol use, or a recent fall.
Int J Geriatr Psychiatry 2008; 23: 1306–1311.
DOI: 10.1002/gps
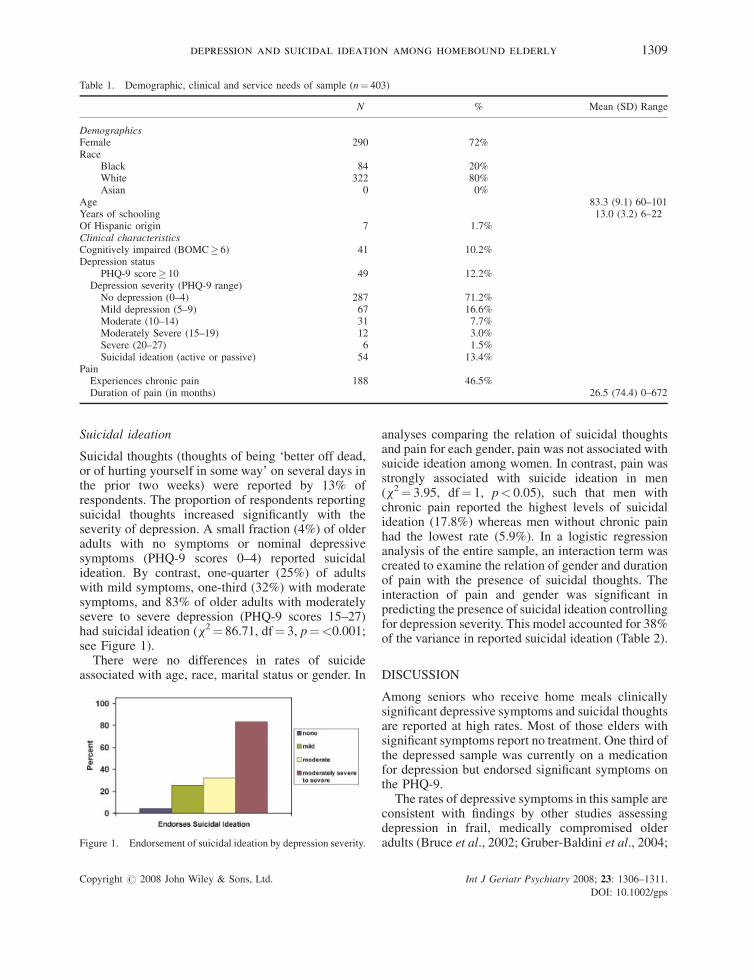
Table 1. Demographic, clinical and service needs of sample (n¼ 403)
N % Mean (SD) Range
DemographicsFemale 290 72%Race
Black 84 20%White 322 80%Asian 0 0%
Age 83.3 (9.1) 60–101Years of schooling 13.0 (3.2) 6–22Of Hispanic origin 7 1.7%Clinical characteristicsCognitively impaired (BOMC� 6) 41 10.2%Depression status
PHQ-9 score� 10 49 12.2%Depression severity (PHQ-9 range)No depression (0–4) 287 71.2%Mild depression (5–9) 67 16.6%Moderate (10–14) 31 7.7%Moderately Severe (15–19) 12 3.0%Severe (20–27) 6 1.5%Suicidal ideation (active or passive) 54 13.4%
PainExperiences chronic pain 188 46.5%Duration of pain (in months) 26.5 (74.4) 0–672
depression and suicidal ideation among homebound elderly 1309
Suicidal ideation
Suicidal thoughts (thoughts of being ‘better off dead,or of hurting yourself in some way’ on several days inthe prior two weeks) were reported by 13% ofrespondents. The proportion of respondents reportingsuicidal thoughts increased significantly with theseverity of depression. A small fraction (4%) of olderadults with no symptoms or nominal depressivesymptoms (PHQ-9 scores 0–4) reported suicidalideation. By contrast, one-quarter (25%) of adultswith mild symptoms, one-third (32%) with moderatesymptoms, and 83% of older adults with moderatelysevere to severe depression (PHQ-9 scores 15–27)had suicidal ideation (x2¼ 86.71, df¼ 3, p¼<0.001;see Figure 1).
There were no differences in rates of suicideassociated with age, race, marital status or gender. In
Figure 1. Endorsement of suicidal ideation by depression severity.
Copyright # 2008 John Wiley & Sons, Ltd.
analyses comparing the relation of suicidal thoughtsand pain for each gender, pain was not associated withsuicide ideation among women. In contrast, pain wasstrongly associated with suicide ideation in men(x2¼ 3.95, df¼ 1, p< 0.05), such that men withchronic pain reported the highest levels of suicidalideation (17.8%) whereas men without chronic painhad the lowest rate (5.9%). In a logistic regressionanalysis of the entire sample, an interaction term wascreated to examine the relation of gender and durationof pain with the presence of suicidal thoughts. Theinteraction of pain and gender was significant inpredicting the presence of suicidal ideation controllingfor depression severity. This model accounted for 38%of the variance in reported suicidal ideation (Table 2).
DISCUSSION
Among seniors who receive home meals clinicallysignificant depressive symptoms and suicidal thoughtsare reported at high rates. Most of those elders withsignificant symptoms report no treatment. One third ofthe depressed sample was currently on a medicationfor depression but endorsed significant symptoms onthe PHQ-9.The rates of depressive symptoms in this sample are
consistent with findings by other studies assessingdepression in frail, medically compromised olderadults (Bruce et al., 2002; Gruber-Baldini et al., 2004;
Int J Geriatr Psychiatry 2008; 23: 1306–1311.
DOI: 10.1002/gps
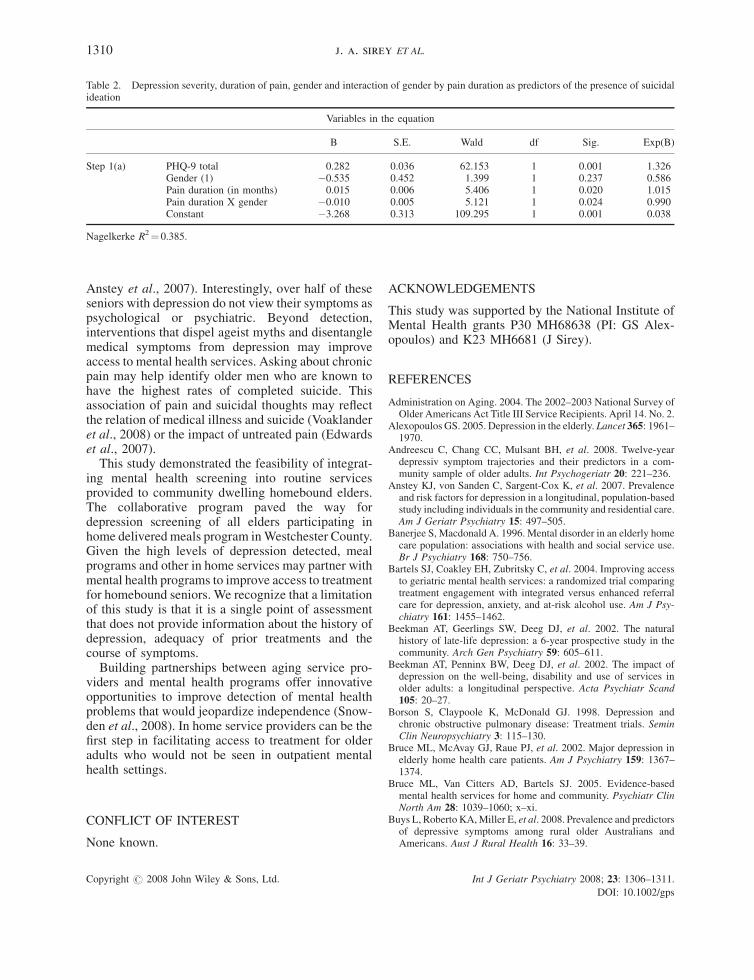
Table 2. Depression severity, duration of pain, gender and interaction of gender by pain duration as predictors of the presence of suicidalideation
Variables in the equation
B S.E. Wald df Sig. Exp(B)
Step 1(a) PHQ-9 total 0.282 0.036 62.153 1 0.001 1.326Gender (1) �0.535 0.452 1.399 1 0.237 0.586Pain duration (in months) 0.015 0.006 5.406 1 0.020 1.015Pain duration X gender �0.010 0.005 5.121 1 0.024 0.990Constant �3.268 0.313 109.295 1 0.001 0.038
Nagelkerke R2¼ 0.385.
1310 j. a. sirey ET AL.
Anstey et al., 2007). Interestingly, over half of theseseniors with depression do not view their symptoms aspsychological or psychiatric. Beyond detection,interventions that dispel ageist myths and disentanglemedical symptoms from depression may improveaccess to mental health services. Asking about chronicpain may help identify older men who are known tohave the highest rates of completed suicide. Thisassociation of pain and suicidal thoughts may reflectthe relation of medical illness and suicide (Voaklanderet al., 2008) or the impact of untreated pain (Edwardset al., 2007).This study demonstrated the feasibility of integrat-
ing mental health screening into routine servicesprovided to community dwelling homebound elders.The collaborative program paved the way fordepression screening of all elders participating inhome delivered meals program inWestchester County.Given the high levels of depression detected, mealprograms and other in home services may partner withmental health programs to improve access to treatmentfor homebound seniors. We recognize that a limitationof this study is that it is a single point of assessmentthat does not provide information about the history ofdepression, adequacy of prior treatments and thecourse of symptoms.Building partnerships between aging service pro-
viders and mental health programs offer innovativeopportunities to improve detection of mental healthproblems that would jeopardize independence (Snow-den et al., 2008). In home service providers can be thefirst step in facilitating access to treatment for olderadults who would not be seen in outpatient mentalhealth settings.
CONFLICT OF INTEREST
None known.
Copyright # 2008 John Wiley & Sons, Ltd.
ACKNOWLEDGEMENTS
This study was supported by the National Institute ofMental Health grants P30 MH68638 (PI: GS Alex-opoulos) and K23 MH6681 (J Sirey).
REFERENCES
Administration on Aging. 2004. The 2002–2003 National Survey ofOlder Americans Act Title III Service Recipients. April 14. No. 2.
Alexopoulos GS. 2005. Depression in the elderly. Lancet 365: 1961–1970.
Andreescu C, Chang CC, Mulsant BH, et al. 2008. Twelve-yeardepressiv symptom trajectories and their predictors in a com-munity sample of older adults. Int Psychogeriatr 20: 221–236.
Anstey KJ, von Sanden C, Sargent-Cox K, et al. 2007. Prevalenceand risk factors for depression in a longitudinal, population-basedstudy including individuals in the community and residential care.Am J Geriatr Psychiatry 15: 497–505.
Banerjee S, Macdonald A. 1996. Mental disorder in an elderly homecare population: associations with health and social service use.Br J Psychiatry 168: 750–756.
Bartels SJ, Coakley EH, Zubritsky C, et al. 2004. Improving accessto geriatric mental health services: a randomized trial comparingtreatment engagement with integrated versus enhanced referralcare for depression, anxiety, and at-risk alcohol use. Am J Psy-chiatry 161: 1455–1462.
Beekman AT, Geerlings SW, Deeg DJ, et al. 2002. The naturalhistory of late-life depression: a 6-year prospective study in thecommunity. Arch Gen Psychiatry 59: 605–611.
Beekman AT, Penninx BW, Deeg DJ, et al. 2002. The impact ofdepression on the well-being, disability and use of services inolder adults: a longitudinal perspective. Acta Psychiatr Scand105: 20–27.
Borson S, Claypoole K, McDonald GJ. 1998. Depression andchronic obstructive pulmonary disease: Treatment trials. SeminClin Neuropsychiatry 3: 115–130.
Bruce ML, McAvay GJ, Raue PJ, et al. 2002. Major depression inelderly home health care patients. Am J Psychiatry 159: 1367–1374.
Bruce ML, Van Citters AD, Bartels SJ. 2005. Evidence-basedmental health services for home and community. Psychiatr ClinNorth Am 28: 1039–1060; x–xi.
Buys L, Roberto KA,Miller E, et al. 2008. Prevalence and predictorsof depressive symptoms among rural older Australians andAmericans. Aust J Rural Health 16: 33–39.
Int J Geriatr Psychiatry 2008; 23: 1306–1311.
DOI: 10.1002/gps

depression and suicidal ideation among homebound elderly 1311
Chapman DP, Perry GS. 2008. Depression as a major component ofpublic health for older adults. Prev Chronic Dis 5: A22.
Choi NG, McDougall GJ. 2007. Comparison of depressive symp-toms between homebound older adults and ambulatory olderadults. Aging & Mental Health 11: 310–322.
Druss BG. 2006. Mental health parity, access, and quality of care.Med Care 44: 497–498.
Edwards RR, Magyar-Russell G, Thombs B, et al. 2007. Acute painat discharge from hospitalization is a prospective predictor oflong-term suicidal ideation after burn injury. Arch Phys MedRehabil 88: S36–42.
Ell K, Unutzer J, Aranda M, et al. 2005. Routine PHQ-9 depressionscreening in home health care: depression, prevalence, clinicaland treatment characteristics and screening implementation.Home Health Care Serv Q 24: 1–19.
Elliott AM, Smith BH, Penny KI, et al. 1999. The epidemiology ofchronic pain in the community. Lancet 354: 1248–1252.
Ewing JA. 1984. Detecting alcoholism: The CAGE questionnaire.JAMA 252: 1905–1907.
Gruber-Baldini AL, Boustani M, Sloane PD, et al. 2004. Behavioralsymptoms in residential care/assisted living facilities: prevalence,risk factors, and medication Management. J Am Geriatr Soc 52:1610–1617.
Katzman R, Fud BT, Peck A, et al. 1983. Validation of a shortOrientation-Memory-Concentration Test of cognitive impair-ment. Am J Psychiatry 140: 734–739.
Koenig HG, Johnson JL, Peterson BL. 2006. Major depression andphysical illness trajectories in heart failure and pulmonarydisease. J Nerv Ment Dis 194: 909–916.
Kroenke K, Spitzer RL. 2002. The PHQ-9: A new depressiondiagnostic and severity measure. Psychiatric Ann 32: 509–521.
Levkoff SE, Chen H, Coakley E, et al. 2004. Design and samplecharacteristics of the PRISM-E multisite randomized trial toimprove behavioral health care for the elderly. J Aging Health16: 3–27.
Copyright # 2008 John Wiley & Sons, Ltd.
Lowe B, Unutzer J, Callahan CM, et al. 2004. Monitoring depres-sion treatment outcomes with the patient health questionnaire-9.Med Care 42: 1194–1201.
Martin A, Rief W, Klaiberg A, et al. 2006. Validity of the BriefPatient Health Questionnaire Mood Scale (PHQ-9) in the generalpopulation. Gen Hosp Psychiatry 28: 71–77.
Oxman TE, Dietrich AJ, Williams JW Jr, et al. 2002. A three-component model for reengineering systems for the treatment ofdepression in primary care. Psychosomat 43: 441–450.
Ponza M, Ohls JC, Millen BE, et al. 1996. Serving elders at risk theolder American acts nutrition program 1993–1995. In Title IIIEvaluation Findings. Mathematic Policy Research, Inc.:Princeton, NJ.
Raue PJ, Brown EL, Meyers BS, et al. 2006. Does every allusion tosuicide carry the same response? J Fam Practice 55: 605–612.
Sharkey JR. 2005. Longitudinal examination of homebound olderadults who experience heightened food insufficiency: effect ofdiabetes status and implications for service provision. Gerontol-ogist 45: 773–782.
Schulberg HC, Mulsant B, Schulz R, et al. 1998. Characteristics andcourse of major depression in older primary care patients. Int JPsychiatry Med 28: 421–436.
Snowden M, Steinman L, Frederick J. 2008. Treating depression inolder adults: challenges to implementing the recommendations ofan expert panel. Prev Chronic Dis 5: A26.
Unruh AM. 1996. Gender variations in clinical pain experience.Pain 65: 123–167.
Unutzer J, Simon G, Belin TR, et al. 2000. Care for depression inHMO patients aged 65 and older. J Am Geriatr Soc 48: 871–878.
Voaklander DC, Rowe BH, Dryden DM, et al. 2008. Medical illness,medication use and suicide in seniors: a population-based casecontrol study. J Epidemiol Commun Health 62: 138–146.
Wells K, Miranda J, Bruce ML, et al. 2004. Bridging communityintervention and mental health services research. Am J Psychiatry161: 955–963.
Int J Geriatr Psychiatry 2008; 23: 1306–1311.
DOI: 10.1002/gps





























