Embed Size (px)
Citation preview

Detecting the effect of Alzheimer’s diseaseon everyday motion behavior
Thomas Kirste1, Andre Hoffmeyer2, Alexandra Bauer1, Susanne Schubert1,and Stefan Teipel1,2
1 University of Rostock, Germany; [email protected] German Center for Neurodegenerative Diseases (DZNE), Rostock, Germany;
Abstract. We report preliminary results of a study on the viability ofaccelerometric motion protocols of everyday behavior as biomarker forthe in-vivo diagnosis of Alzheimer’s disease.Based on data collected from 20 dyads (40 subjects) with one partnersuffering from dementia and one healthy partner, we provide evidencethat Alzheimer’s disease manifests itself in changes of everyday behaviorthat are detectable in accelerometric behavior protocols.
1 Motivation
Alzheimer’s disease (AD) leads to significant changes in the temporal structureof activities. Abnormal motion behavior and degeneration of the sleep-wakingcycle are among the most severe behavioral symptoms. An early detection andeven a prediction of these behaviors would allow a timely onset of interventionsthat aim to delay the manifestation or exacerbation of symptoms and reduce theneed of institutionalized care. Behavioral rating scales are the only diagnosticmarkers to detect the onset of abnormal motion behavior, but their reliability andaccuracy is limited. Using behavioral cues as diagnostic instrument is interestingfor two reasons: (i) data can be acquired in a person’s everyday environment,(ii) once behavior analysis is in place, assistive functionality can be added forcompensating errors in daily routine activities and for other forms of ambientassisted living.
There is a number of projects aiming at establishing correlations betweenmotion behavior and cognitive state – see for instance [1,2,3]. However, it seemsthat current research focuses on studies with small numbers of test subjects,thus making it difficult to establish statistical models of motion behavior. Inthis paper, we present first results of an ongoing study that includes the datafrom 40 subjects. Aim of this study is to establish, whether motion protocolsfrom persons diagnosed with AD exhibit changes that allow to discriminate themfrom motion protocols of healthy controls. We thereby focus on unlabeled motionprotocols of unconstrained everyday behavior.
As the structure of unconstrained everyday behavior is subject to a verylarge number of confounding factors concerning life style, physical fitness, health

state, etc., it is not clear that such a concept should work at all. However,the preliminary results we present in this paper give some evidence that thisapproach indeed may be viable.
2 Data Acquisition
Data recording setup. We recruited 20 dyads (n = 40 subjects) with one part-ner diagnosed with AD and one partner with no cognitive abnormality detected(NAD); AD patients fulfilled the NINCDS-ADRDA criteria for clinically prob-able AD. Severity of cognitive impairment was assessed by a comprehensive setof instruments including the MMSE score [4] and the CERAD cognitive battery.The MMSE score serves as widely established measure for the severity of overallcognitive impairment. Subject selection has been balanced with respect to thevariables “Gender”, “Diagnosis”, and “Age”. The average age of subjects was74.4 (SD = 8.96), the overall average MMSE score was 24.23 (SD = 7.02). Av-erage MMSE score for AD subjects was 19.8 (SD = 7.6) and 28.65 (SD = 1.53)for NAD subjects. It is important to note that none of the patients or care-giversreported severe behavioral symptoms in the patient.
The partners in a dyad were asked to simul-taneously record 50 continuous hours of every-day activity using an ankle-mounted accelero-metric sensor (cf. Fig. 1). Recording sessions tookplace in the time frame of three days; in day 1a medical student would attach the sensor, in-struct the subjects on sensor handling, and col-lect the data on cognitive state. During day 3
also systems for the special needs of persons with demen-tia. These solutions can be classified into four groups. Thecompensation of cognitive skills [10], for example remembertaking the medication[16], the support in the activities ofdaily living, for example washing hands [11], the stabilityof social contacts [13] and last the feeling of safety/security[12]. Kasteren [17] studied in his thesis temporal probabilis-tic models to recognize activities of daily living for elderypeople by using di↵erent sensor types and wireless sensornetwork. The approach was verified in three houses andwith Hierarchical Hidden Markov Models he gets the bestclassification results to recognize ADL.
Biological markers [5] for dementia are established in partto be explored in studies. A novel approach is to use meth-ods from activity recognition as diagnostic marker. Kearns[7] used Ubisense, an indoor localization system, to recordmovement trajectories of people with dementia. In his stud-ies the cognitive status of subjects correlated with the tor-tuosity of the movement trajectories.
3. STUDY DESGINThe DZNE is a research institute studying neurodegenera-tive diseases. One research topic in the DZNE Rostock is anearly diagnosis of dementia in high risk populations and insubjects with demand for medical and social care support.This study has the following three aims:
• The prediction of problem behaviour in the stage of de-mentia: How strong is the abnormal behavior formed?
• The prediction of dementia in early stages: Is it pos-sible to detect motion patterns which are typical fordementia in early stages?
• Review of the e�cacy of therapeutic interventions.
To verify our aims we recruited elderly couples and dividedthe subjects into two groups of couples. In group A one part-ner su↵ers from dementia and the other is healthy, in groupB both partners are cognitively healthy. To determine thecognitive performance of subjects we are using the CERADbattery [4].
The a↵ected subjects were examined by a doctor and di-agnosed with a light or mild dementia. Exclusion criteriafor the study are diseases of Nervous system, neoplastic dis-eases, Restlesslegs-Syndrome or obstructive sleep apnea syn-drome. The interesting point is that we can analyze thecaregiver e↵ect too. Are existing strains of healthy partnersin group A measurable?
The record of the movement behavior of subjects is in theirdomesticity. Both partners have a motion sensor foot-moun-ted for round about 50 hours. We use this sensor position be-cause it is the most comfortable position. As subjects wearthe sensor for three days continuously a position at the hipfor example is not acceptable because it would disturb thesubject while sleeping. The combination with the foot posi-tion and comfortable bandage has been found to be the bestalternative. Furthermore Atallah et. al. [2] evaluated di↵er-ent accelerometer positions(ear,chest,arm,wrist,waist,knee,ankle/foot-mounted) for detecting di↵erent activities of daily living.
Figure 1: The foot-mounted sensor worn by a volun-teer. The bandage has a velcro closure and a open-ing for the sensor.
day night day daynight
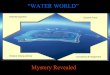
Figure 2: The illustration shows a frequency analysisof a subject with the ground truth of day and night.(Using R and seewave [14] for the illustration.)
For low activities and the ankle position they got good re-sults.
The shimmer sensor is a 3-axis accelerometer sensor. Weused a 50 Hertz sampling and a range of -4/4G. The sensoroperates autonomous. It requires no infrastructure and thesubjects can follow their usual activities. The data is log onthe sensor flash memory. 1
4. DATAHANDLINGEach subject of the study generated approximately 9 milliondata points (timestamp, and the x, y, z acceleration.) – atotal of 900 MByte. Before the data is used it is checked forits validity. So records are excluded where the sensor hasfailed or the subject has not taken the device. Furthermore,the data is normalized by the raw sensor values in g.
The first step of any signal processing is to analyze the rawdata before further processing steps are made. Figure 2presents a Fourier transform (windowsize = 256) of a sub-ject. The record includes 2 nights. Even at the di↵erentamplitude of the frequency spectrum it can be distinguishedbetween day and night. Walk sequences are also visible at ahigh frequency. One advantage of the selected sensor posi-
1The shimmer sensors have no ability for geo coding. Werecord no GPS data or similar data. An important point forall subjects is that their privacy is always protected.
Fig. 1. Physical sensor setup
the student would again visit the dyad, collect-ing the sensors and the recorded data. This recording schedule guaranteed thatwe were able to record a complete day-night cycle for each subject (from 22:00at day 1 to 22:00 at day 2).
As sensor system we used the Shimmer product, providing a 3 axis accelero-meter using Freescale MMA7260Q 1.5/2/4/6g MEMs devices giving 12 bits ofresolution with sensor data storage to on-board MicroSD card. We used a sensorsampling rate of 50 Hz and a 4g value range. The average recording duration was52 hours (SD = 8.4 hours), resulting in an average number of 9.4× 106 samplesin a subject’s motion protocol. In total, 2088 hours of data were recorded, witha total volume of 8.86 GByte binary data.
Preprocessing. Our underlying assumption for the analysis of motion protocolshas been that the temporal structure of activity intensity correlates with a per-son’s diagnosis as AD or NAD. As activity intensity, we considered the amplitudeof the envelope of the carrier band in the range of 0.5 Hz to 5 Hz. The rationalebehind the carrier band selection is the assumption that typical motion cycles(walking, . . . ) occur in roughly this frequency range. Higher frequencies includeincreasing levels of noise, lower frequencies begin to exhibit influences from gravi-tation. To isolate the activity envelope, we used the following detection method:

X024GFD1 : 17.08.11, 17:08 -- 19.08.11, 16:19Acceleration
0 10 20 30 40
1030
50
X024GMD0 : 17.08.11, 17:20 -- 19.08.11, 16:19
Acceleration
0 10 20 30 40
040
80
Fig. 2. Preprocessed data sample from a dyad. Left: female person, diagnosis AD(GFD1). Right: male person, diagnosis NAD (GMD0). X axis: recording hours, Y axis:activity level. Grey regions signify night (22:00–7:00).
Label Duration Objective
night.day 22:00–22:00 capture circadian activity cyclecal.day 24:00–24:00 check susceptibility of circadian cycle to temporal positionnight 22:00–05:00 check for effects of nightly unrestcore.night 24:00–05:00 focus on deep nightmorning 05:00–12:00 morning activityafternoon 12:00–24:00 afternoon activity
Table 1. Time windows used in spectral analysis
First, we removed orientation information by computing the acceleration mag-
nitude am =√
a2x + a2y + a2z. To the acceleration magnitude signal we applied
a sinc bandpass filter with lower band edge at 0.5 Hz and upper band edge at5 Hz to remove gravitation and noise. Finally, we rectified the resulting signaland applied a sinc low pass. We experimented with two cutoff frequencies forthe low pass filter, F1 = 0.025 Hz and F2 = 0.25 Hz, corresponding to 40 sec.resp. 4 sec. temporal resolution for the activity envelope. Two examples for theoutput signal resulting from F1 are given in Fig. 2.
3 Prediction Models
Core objective of data analysis has been to classify persons as AD or NAD basedon the activity envelopes. In addition, we were interested in the possibility ofpredicting the MMSE score from activity envelopes. Finally, in order to estimatethe usefulness of activity envelopes for predicting other variables, we looked atmodels using a subject’s gender as classification target.
Spectral features. Our assumption is that the temporal structure of activitymanifests itself in specific characteristics of the envelope’s frequency spectrum.Therefore, we computed the Fourier transform for the envelopes, discarding thephase information and retaining the magnitude. We focused on the coefficientsfor wave numbers k = 1 . . 200, dropping the DC coefficient at k = 0 and ignoringall higher harmonics. As it was of interest to analyze whether there are specific

accuracy
0.87
0.88
0.89
0.90
0.91
0.92
afternoon cal.day core.night morning night night.day
: Target Diagnosis : Target Diagnosis
afternoon cal.day core.night morning night night.day
: Target Gender : Target Gender
M1
M2M3 Index
Index
Index
Fig. 3. Left: classification accuracy achieved for quadratic discriminant models usingfive pc-spectra and different time windows, for classification targets “Diagnosis” and“Gender”. (+): results for all subjects (n = 40). (◦): results without person A (n = 39).Right: Reconstructed motion profiles for the five pc-spectra selected for Model M1sorted by magnitude of eigenvalues. X axis represents 24h.
time windows within a day where AD-induced changes are especially visible, weperformed the spectral analysis for the six different time windows in Table 1.As one of the test subjects, person A, had stopped the recording prematurelyin the morning of day two, the analysis for the complete population of n = 40subjects had to concentrate on the windows “night” and “core.night”. For areduced subject set of size n = 39, all windows could be tested. From the set ofsubject spectra we computed the principal component spectra (pc-spectra) byprinciple component analysis. The idea is that pc-spectra identify characteristicgeneral “temporal activity structures” from which daily routines are composed.For each subject, the factor loadings for the pc-spectra were computed.
Classification models for Diagnosis and Gender. We built classification modelsthat were allowed to use up to five factor loadings to discriminate between ADand NAD subjects. In a cursory first investigation using linear discriminantanalysis, quadratic discriminant analysis (QDA), and support vector machines,QDA emerged as showing the best classification performance in leave-one-outcross-validation. Furthermore, the pc-spectra factor loadings did show betterperformance than the raw Fourier coefficients, so we concentrated on pc-spectrafor further classification analysis.
We built models for all combinations of time window (six windows for n = 39subjects, two windows for n = 40), classification target (“Diagnosis” and “Gen-der”), and filter setting (F1 and F2), giving 32 model configurations. For eachmodel, the optimal combination of five pc-spectra was selected by exhaustivesearch. Comparing the 16 F1 models with the 16 F2 models using a Wilcoxonsigned rank test indicated a significantly better performance for the F1 setting(V=72.5, p=0.0094), so we concentrate on this filter setting for the further clas-sification analysis. Fig. 3 compares the resulting classification accuracies.
In Table 2 we give the confusion matrices for some typical models. In ouropinion, the achieved accuracies indicate that the temporal structure of the acti-vity envelope indeed shows correlation with the medical diagnosis. Furthermore,we see that – at least at this level of analysis – also gender specific differences inmotion behavior are detectable, indicating possible further applications for ac-tivity envelope data. Finally, as M2 indicates, it seems possible to achieve evenbetter results concentrating just on the night (which also would significantly re-

M1 M2 M3 Performance
n = 39 Truth
Class. AD NAD
AD 17 2
NAD 3 17
n = 40 Truth
Class. AD NAD
AD 19 2
NAD 1 18
n = 39 Truth
Class. F M
F 18 2
M 2 17
M1 M2 M3
acc 0.872 0.925 0.897
sens 0.85 0.95 0.9
spec 0.895 0.9 0.895
Table 2. Confusion matrices for selected models (M1: Diagnosis night.day, M2: Diag-nosis night, M3: Gender night.day) and resulting values for accuracy (acc), sensitivity(sens), and specificity (spec).
adju
sted
R2
0.4
0.5
0.6
0.7
0.8
0.9
afternoon cal.day core.night morning night night.day
Models for all subjectsModels for all subjects
afternoon cal.day core.night morning night night.day
Models for subjects with diagnosis ADModels for subjects with diagnosis AD
M4
True MMSE
Pred
icted
MM
SE
0
10
20
30
0 5 10 15 20 25 30
Fig. 4. Left: Adjusted R2 values achieved for linear models of MMSE (◦) resp.√
MMSE(+) using five spectral components as predictor variables, selecting different data timeranges. Right: True vs. predicted MMSE values for model M4 (“night.day” windowand
√MMSE prediction), (◦): AD, (+): NAD. This model is able to explain 81% of
the variance in√
MMSE (adjusted R2 = 0.78, R2=0.81, F(5,33)=27.93, p<0.001)
duce the time required for sensor data recording). However, as the appreciablevariations in accuracy caused by adding another subject show, the models rightnow are not yet robust enough to warrant a reduction of recording time.
For interest, in Fig. 3, right, we give the activity envelopes of the five pc-spectra selected by model M1. These envelopes were computed by applying aninverse Fourier transform to the respective pc-spectra. Since phase informationhad been removed from the spectral features, there is no easy way to interpretthese curves as indicating activity at a specific time of day – further analysisis required to develop an understanding of the possible meaning of these recon-structed envelopes.
Regression models for MMSE. With respect to predicting the MMSE, we foundFourier coefficients to perform better than pc-spectra. Based on the Fouriercoefficients as predictor variables, we built linear models using either MMSEor√
MMSE as regression target. The latter target choice had been motivatedby a preliminary residual analysis, indicating a nonlinear behavior of higherMMSE values, in agreement with the non-linear behavior of MMSE scores inlarge normative samples. For both targets, we built models with respect to dif-ferent choices of time window, population (all subjects resp. only AD subjects)and filter setting (resulting in 96 configurations). For the filter setting we foundthat – in contrast to the finding for classification – the F2 setting was able toprovide better results (using a Wilcoxon test on the adjusted R2 for the differentregression models). Predictor variables for a model were selected by applying the

step function of the statistics system R to an initially empty model. To avoidoverfitting, we restricted the number of predictor variables to at most five. Thevalues for adjusted R2 of the resulting models are compared in Fig. 4, left. Notethat we were able to achieve promising results; if we concentrate on just the ADsubset, an even better fit can be achieved. A comparison of predicted and trueMMSE values using the model M4 for the full population is given in Fig. 4, right.
4 Discussion
In general, we think our results show that effects of AD are detectable in ac-celerometric motion protocols, even at early stages of AD (corresponding to highMMSE scores). It is important to note that the approach presented here does notaim to increase the accuracy of the diagnosis of AD, but to determine whetherthe diagnosis of AD is associated with changes in everyday motion behavior.Although the resulting surrogate markers of motion behavior do not easily offeran interpretation in clinical terms, the overall concept of an impairment of thetemporal structure of everyday motion behavior agrees with a range of neurobio-logical and clinical studies in AD. The easily accessible assessment of early signsof forthcoming decline of motion behavior using automated sensors will have amajor impact on the development and application of interventions to prevent orattenuate behavioral impairment in AD.
Further analysis will concentrate on increasing the robustness: given thesample size, we do not think that enough data is available to identify sets ofpc-spectra that are robust across a population. The effect on M2 of leaving outperson A (see Fig. 3, left) clearly indicates high susceptibility to sample variation.Possible solutions include increasing sample size and integrating prior knowledgeon activity structures; both options are subject of further research.
References
1. Kearns, W., Algase, D., Moore, D., Ahmed, S.: Ultra wideband radio: A novelmethod for measuring wandering in persons with dementia. Gerontechnology 7(1)(2008) 48–57
2. Grunerbl, A., Bahle, G., Lukowicz, P., Hanser, F.: Using indoor location to assessthe state of dementia patients: Results and experience report from a long term,real world study. In: Proc 7th Intl. Conf. on Intelligent Environments (IE 2011),Nottingham, UK (2011) 32–39
3. Tung, J.Y., Semple, J.F.L., Woo, W.X., Hsu, W.S., Sinn, M., Roy, E.A., Poupart,P.: Ambulatory assessment of lifestyle factors for Alzheimer’s disease and related de-mentias. In: Proc. AAAI Spring Symposium: Computational Physiology, Stanford,CA (2011)
4. Folstein, M.F., Folstein, S.E., McHugh, P.R.: Mini-mental-state: A practical methodfor grading the cognitive state of patients for the clinician. J Psychiatr Res 12 (1975)189–198