Embed Size (px)
Citation preview

Gerald C. IhraJudith LehbergerHelene HochrieserPeter BauerRene SchmutzBarbara MetnitzPhilipp G. H. Metnitz
Development of demographics and outcomeof very old critically ill patients admittedto intensive care units
Received: 1 June 2011Accepted: 30 December 2011Published online: 22 February 2012� Copyright jointly held by Springer andESICM 2012
Philipp G. H. Metnitz: senior author.
G. C. Ihra ()) � J. Lehberger �R. Schmutz � P. G. H. MetnitzDepartment of Anesthesiology and GeneralIntensive Care, Medical Universityof Vienna, Vienna, Austriae-mail: [email protected].: ?43-1-404004100Fax: ?43-1-404004028URL: http://www.ihra.at
H. Hochrieser � P. BauerDepartment of Medical Statistics,Medical University of Vienna,Vienna, Austria
B. MetnitzAustrian Center for Documentationand Quality Assurance in IntensiveCare (ASDI), Vienna, Austria
Abstract Purpose: To evaluatethe development of demographics andoutcome of very old ([80 years)critically ill patients admitted tointensive care units. Setting: Allconsecutive patients admitted to 41Austrian intensive care units (ICUs)over an 11-year period. Meth-ods: We performed a retrospectivecohort study of prospectively col-lected data. To compare parametersover time, patients were divided intothree groups (group I from 1998 until2001, group II from 2002 to 2004,and group III from 2005 to 2008).Results: A total of 17,126 patientsolder than 80 years of age wereadmitted over the study period. Theproportion of very old patientsincreased from 11.5% (I) to 15.3%(III) with a significant higher preva-lence of females in all groups (onaverage 63.2%). Severity of illnessalso increased over time, even whencorrected for age. Use of noninvasivemechanical ventilation increased over
the years. However, risk-adjustedmortality rates [observed-to-expected(O/E) ratios] decreased from 1.14[confidence interval (CI) 1.11–1.18]to 1.02 (CI 0.99–1.05). Thisimprovement in outcome was con-firmed on multivariate analysis: forevery year delay in ICU admission,the odds to die decreased by 3%.Moreover, females exhibited a betteroutcome compared with males. Con-clusions: The relative and absolutenumbers of very old patientsincreased over the study period, asdid the severity of illness. Despitethis, risk-adjusted hospital mortalityimproved over the study period.Females dominated in the very oldpatients and exhibited moreover abetter outcome compared with males.
Keywords Outcome �ICU mortality � Very old patients
Introduction
Improvements in sanitation, healthcare, and environ-mental factors are considered to be responsible for therising number of elderly patients. United Nations’ offi-cials predict a further increase in the aged populationthroughout the world [1]. This demographic transitionmay be attributed to the enhancement of life expectancyin conjunction with a decrease in fertility [2]. Despitedifferences in regional patterns of aging, the median age
of the world’s population will markedly increase and theproportion of the elderly is expected to rise [3]. This shiftof balance from young to old is observed in industrializedcountries as well as in less developed regions, althoughthe highest proportions of old persons are found in moredeveloped countries [1]. Moreover, the elderly populationis growing at a faster rate than the world’s totalpopulation.
As age is considered an important factor in functionalimpairment and morbidity, and older patients are more
Intensive Care Med (2012) 38:620–626DOI 10.1007/s00134-012-2474-7 ORIGINAL

likely to suffer morbid events [4, 5], the number of elderlypatients requiring intensive care is also expected to rise[6]. All adult prognostic models have highlighted theimportance of age, and increased ICU and hospital mor-tality rates have been reported for elderly patients.However, some studies were either unable to identify ageas a predictor of survival [7] or found other factors suchas functional status to be of more importance for theprognosis of these patients [8]. Thus, decisions to admitelderly patients to intensive care units during the initialtriage process are controversially discussed with respectto functional outcome and costs [7–9].
To investigate prognosis and outcome of very oldcritically ill patients admitted to intensive care units overtime, we performed a multicenter retrospective analysis ofprospectively collected data.
Materials and methods
Data collection
Data were collected prospectively by the Austrian Centerfor Documentation and Quality Assurance in IntensiveCare Medicine (ASDI). ASDI is a nonprofit organiza-tion that has established an intensive care databaseand benchmarking project (http://www.asdi.ac.at). Afterinstitutional review board approval, the followingparameters were analyzed: sociodemographic data, suchas age, sex, and chronic conditions; the reason foradmission, which was recorded according to a predefinedlist of medical and surgical diagnoses [10, 11]; severity ofillness, as measured by the Simplified Acute PhysiologyScore II (SAPS II) [12]; level of care in the ICU, asmeasured by the Simplified Therapeutic InterventionScoring System (TISS-28) [13]; length of ICU and hos-pital stay; and outcome data, including survival status atICU and hospital discharge. Reliability and completenessof the data in the ASDI database are assessed at regularintervals as described previously; results have beenreported elsewhere [14]. In general, both reliability andcompleteness are excellent, since these data are used forgovernmental purposes.
Study population
All patients admitted to 87 Austrian ICUs from 1 January1998 to 31 December 2008 were enrolled in this study.However, to be able to evaluate prognosis over the years,only those ICUs which participated for at least 9 yearswere included for data analysis (n = 41). During thestudy period 146,116 patients were admitted to these41 ICUs. For patients who were admitted more thanonce (n = 9,408) only the first admission was included.
Patients aged \18 years (n = 2,621), or patients withrecords that lacked an entry in the field ‘‘hospitaloutcome’’ (n = 1,019), or those without a valid SAPS IIscore (n = 5,914) were excluded. Finally a total of127,154 patients remained. In this group 17,126 patientswere aged [80 years (13.5%, very old patients) and thuseligible for analysis. To compare parameters over thestudy period, patients were divided into three groups:group I including patients from 1998 until 2001(n = 5,098), group II from 2002 to 2004 (n = 4,588),and group III from 2005 to 2008 (n = 7,440). Since noadditional interventions were performed, the need forinformed consent was waived by the institutional reviewboard.
Statistical analysis
Statistical analysis was performed using the SAS Systemversion 9.1.3. (SAS Institute Inc., Cary, NC). Lineartrends over calendar time for quantitative variables weretested by linear regression analysis; for dichotomousvariables logistic regression was used accordingly. Mann–Whitney U test and v2 test were applied for comparison ofquantitative and dichotomous variables between twogroups, respectively. Observed-to-expected (O/E) mor-tality ratios were calculated by dividing the numberof observed deaths per group by the number ofSAPS II-predicted deaths per group. Confidence intervals(CIs, 95%) were calculated according to the formuladescribed by Hosmer and Lemeshow [15]. Unless other-wise indicated, values in the tables are expressed asmedian and interquartile range.
To evaluate the severity of illness in the very oldpatients without the impact of age, we calculated an age-corrected SAPS II score for each patient in such a waythat those score points which were attributed because ofage were subtracted from the overall score. We thenperformed a multiple logistic regression analysis to findfactors influencing hospital mortality and to look fora trend over the years. The following parameterswere included: age-corrected SAPS II, year, sex, renalreplacement therapy, ventilation, comorbidities, admis-sion type, and ICUs. To account for overfitting in themodel, a p value \0.01 was considered significant [16].No other correction for multiplicity of testing has beenapplied.
Results
Data of a total of 127,154 adults admitted to 41 ICUsbetween January 1998 and December 2008 were ana-lyzed. Mean age in the overall cohort was 62.4 ±17.4 years [mean ± standard deviation (SD)] with 41.9%
621

of the patients exhibiting female gender. Very old patientsexhibited a higher severity of illness with and withouttaking age into account (SAPS II and age-correctedSAPS II, Table 1). Moreover, they exhibited a shorterlength of stay (LOS) on the ICU and a shorter duration ofmechanical ventilation, as indicated by the number ofventilated days (55% versus 50%, for patients aged B80versus [80 years, respectively). Hospital mortality washigher in very old patients for both raw and risk-adjustedmortality rates.
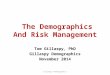
The cumulative proportion over all years of very oldpatients was 13.5% (n = 17,126). Demographic charac-teristics, type of admission, and SAPS II values of allpatients (B80 years,[80 years) are presented in Table 1.Over the years the proportion of patients admitted to ICUwho were very old increased from 11.5% (group I) to13.4% (group II) and 15.3% (group III) (Fig. 1). Inter-estingly, there were more females in the very old patientgroup (63.2%). ICU length of stay (LOS) was shorter inthe group of very old patients, but raw mortality rateswere higher for both ICU and hospital mortality. More-over, risk-adjusted mortality (O/E ratio) was higher in thevery old (1.08 [1.06–1.1] versus 0.93 [0.92–0.94]). Fur-thermore, mechanical ventilation was less frequently usedin the very old patients (Table 1).
Demographic data, comorbidities, and reasons foradmission of very old patients assigned to groups I–III arelisted in Table 2. In contrast to patients aged less than80 years, women outnumbered men in all groups of veryold patients. Severity of illness (as expressed by SAPS IIscore) increased over the years from 39.2 ± 14.8 (I) to41.3 ± 15.8 (III). To see if this was just an effect of age(which is already included in SAPS II), we calculatedSAPS II scores without age score. Age-corrected SAPS IIvalues increased from 21.2 ± 14.8 (I) to 23.3 ± 15.8 (III)(p \ 0.0001), giving evidence of a rise of the severity ofillness over time. Finally, length of stay in the ICU ofvery old ICU patients also increased over the study
period. Furthermore, use of mechanical ventilation in veryold patients increased significantly. Even more pro-nounced, the use of noninvasive mechanical ventilationtripled (Table 2).
In the cohort of very old patients, several differencesbetween males and females were present: female patientswere slightly older (85.5 ± 3.8 versus 84.8 ± 3.6 years),underwent less often mechanical ventilation (48% versus54%, p \ 0.0001), and exhibited a shorter ICU LOS(5.4 ± 7.4 versus 6.4 ± 8.9 days). In addition, despite asimilar severity of illness, females exhibited a betteroutcome: raw mortality rates were 29.7% versus 33.4%,and risk-adjusted mortality rates were 1.06 (1.03–1.08)and 1.12 (1.09–1.15) for females and males, respectively.
Table 1 ICU patient cohort: demographics, admission types, SAPS II, and mortality
B80 years (n = 110,028) 80 years (n = 17,126) p value
Age, years median (quartiles) 62 (49–72) 84 (82–87) \0.0001Female gender, % 38.6 63.2 \0.0001ICU LOS, days 3.0 (2–7) 3.0 (2–6) \0.0001Mechanical ventilation, patients, % 55.0 50.3 \0.0001Type of admission, %Medical 53.0 55.1 \0.0001Scheduled surgical 28.1 19.5 \0.0001Unscheduled surgical 18.9 25.5 \0.0001
SAPS II score 26 (18–38) 36 (29–48) \0.0001SAPS II score age-corrected 15 (8–27) 18 (11–30) \0.0001ICU mortality, % 11.4 20.2 \0.0001Hospital mortality, % 15.9 31.0 \0.0001SAPS II O/E ratio (95% CI) 0.93 (0.92–0.94) 1.08 (1.06–1.1)
CI confidence intervalp values from Mann–Whitney U test or v2 test
Fig. 1 Numbers and percentages of very old ICU patients ([80years) over the study period (1998–2008). The graphs display thenumbers of very old patients aged [80 years per year of ICUadmission (bars). The line presents the percentage (%) of very oldpatients in relation to the total cohort of patients admitted to theICUs per year
622

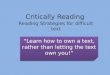
Despite the increase in severity of illness of very oldpatients over time, risk-adjusted mortality rates (O/Eratios) significantly decreased over the years (Fig. 2).
Multivariate analysis identified several factors beingassociated with hospital mortality: First of all, severity ofillness without age (age-corrected SAPS II) was signifi-cantly associated with a worse outcome. Even moreimportant negative predictors were acute and chronicrenal failure and the use of mechanical ventilation.However, year of admission was negatively correlatedwith mortality, indicating a reduction of the odds ratio of3% for every year later admitted [odds ratio (OR) 0.97;p \ 0.0001; Table 3].
Table 2 Very old patients ([80 years): demographic data in the different time groups
Group I(n = 5,098)
Group II(n = 4,588)
Group III(n = 7,440)
p value
Age, years median (quartiles) 85 (83–88) 84 (82–88) 84 (82–87) \0.0001Female gender, % 64.4 62.9 62.5 0.0072Mechanical ventilation, ICU days, % 46.6 54.7 58.4 \0.0001Noninvasive ventilation, ICU days, % 3.1 5.4 9.7 \0.0001SAPS II score 35 (28–46) 35 (28–47) 37 (30–50) \0.0001SAPS II score age-corrected 17 (10–28) 17 (10–29) 19 (12–32) \0.0001SAPS II-predicted mortality, % 27.2 27.3 30.7 \0.0001Observed ICU mortality, % 20.3 19.4 20.6 0.5484Observed hospital mortality, % 31.1 30.5 31.2 0.9461SAPS II O/E ratio (95% CI) 1.14 (1.11–1.18) 1.12 (1.08–1.16) 1.02 (0.99–1.05)Comorbidities, %Chronic renal insufficiency 10.1 11.6 13.6 \0.0001Chronic resp. insufficiency 11.3 10.1 9.3 0.0001Cardiac insufficiency 34.2 30.6 18.5 \0.0001Nonmetastatic cancer 7.0 6.4 5.2 \0.0001Metastatic cancer 3.8 3.3 2.2 \0.0001Insulin-dependent diabetes mellitus 4.5 5.1 4.9 0.4792Comorbidities, others 6.7 5.8 6 0.1034
Reasons for admission, %Cardiovascular disease 29.3 29.9 28.9 0.1663Trauma surgery 17.7 15.8 14.8 0.0001Trauma (not operated) 2.7 1.8 2.3 0.8051Abdominal surgery 16.6 14.4 14.3 0.0122Respiratory disease 6.7 8.8 10.1 \0.0001Surgery, NOS 8.8 8.7 6.1 \0.0001Cardiovascular surgery 4.3 4.4 6.5 \0.0001Neurologic disease 3.2 3.5 3.8 0. 0834Shock 2.4 2.8 3.3 0.0009Diagnosis missing 8.2 5.2 7.6 0.0065
NOS not otherwise specifiedp values calculated by linear regression or logistic regression over years as appropriate
Fig. 2 Risk-adjusted mortality rates in very old ICU patients([80 years) over the study period (1998–2008). The graph displaysthe O/E ratios of old patients over time. Bars indicate 95%confidence intervals. CI confidence interval
Table 3 Logistic regression analysis for hospital mortality in veryold ICU patients (n = 17,126)
Variable Oddsratio
95% CI p value
Age-corrected SAPS II(per unit)
1.069 (1.065–1.073) \0.001
Acute renal failure 1.720 (1.393–2.123) \0.001Chronic renal failure 1.267 (1.127–1.424) \0.001Hematologic disease 0.628 (0.447–0.880) 0.007Mechanical ventilation 1.049 (1.041–1.058) \0.001Calendar time (per year) 0.97 (0.958–0.983) \0.001
Hospital mortality was used as dependent variable. Analysis wasadjusted for sex and center effects (see ‘‘Materials and methods’’section)
623

Discussion
To our best knowledge, we present the largest cohortstudy including the greatest number of observations aswell as the longest observation period, on very oldpatients admitted to intensive care units so far. The agestructure of the world population clearly shows a pre-ponderance of the elderly [1], and this trend isaccompanied with an increasing demand for intensivecare for the elderly [9, 17]. Our results provide someevidence that this is reflected through the increasingnumbers of very old patients admitted to intensive careunits: the proportion of very old patients rose from 11.5%to 15.3% over the study period. Although this is a sig-nificant increase, it is still less than the rate reported byBagshaw et al., who found that admission rates of veryold patients increased annually by 5.6% [6]. This is ofcourse of interest to hospital managers, since these figuresare used for prediction of further needs of intensive carefor upcoming years.
As in other Western countries, the life expectancy ofthe Austrian population has steadily increased. Lifeexpectancy at age 60 years in 1998 was 19.1 and23.5 years for men and women, respectively, and furtherincreased to 21.3 and 25.1 years in 2008 [18]. The per-centage of inhabitants older than 80 years rose from 1.7%in 1961 to 3.6% in 2001 [18]. In accordance with thesefigures we observed an increase of the mean age of thecohort of critically ill patients (from 61.7 to 63.0 years)over the study period. However, the mean age in the veryold patients remained quite stable (for medians andquartiles see Table 2). This may be attributed to the factthat very old patients are already at the relative end oftheir lifespan and thus a marked increase in this group isunlikely to be discovered over the study period.
The growing number of very old patients admitted toICUs might be due to several factors: First, the increasinglife span as already discussed above. Second, a change inadmission policies of very old patients to intensive careunits might be responsible for this observation. In thiscontext patient age has been shown to influence deci-sions concerning the provision of life-sustaining support,independent of medical appropriateness or patientpreferences [19]. The triage of elderly patients wasinvestigated in several studies where advanced age wascited as a reason to refuse ICU admission [19–21]. Morethan two-thirds of patients aged over 80 years weredenied admission or received less treatment in the ICUthan younger patients in two French cohort studies[19, 22]. However, in view of an aging population, therestrictive treatment policy based on advanced age seemsto change over the years [23].
In view of the increasing number of elderly patientsrequiring intensive care [8], the need for mechanicalventilation in the elderly is also expected to rise [6, 24].
Although very old patients were less likely to receivemechanical ventilation, in a large Canadian cohort theauthors recognized a yearly increase of more than 3%;this rate was higher than the annual increase in thenumber of all ventilated patients [6]. Similarly, we founda lower rate of mechanical ventilation in the very oldpatients (Table 1), but an increase in its use over the years(Table 2). Interestingly, mechanical ventilation was cor-related with a higher mortality in this patient group, whichhas been also observed by others [6, 25]. An experimentalstudy revealed a more injurious effect of mechanicalventilation on pulmonary function to be associated withage [26], and survival rates in patients with acute respi-ratory failure have also been shown to decrease with age[27, 28].
In our study, very old patients were subjected morefrequently to noninvasive ventilation (NIV) (6.66% ver-sus 5.98%), and moreover the rate of NIV tripled over theyears (Table 2). Potential beneficial effects and indica-tions for NIV have been discussed [29], and an increasedgeneral use within the last decade has been described[30]. Notably, it has been suggested that use of NIV in theelderly may reduce the rate of intubation in the presenceof respiratory failure and may thus reduce mortality [31].Our results point towards the possibility that new tech-nologies, especially less invasive treatment options, maylead to increased use of intensive care treatment in veryold patients. Some authors suggested that avoidance ofinherent risks should be one of the major goals of ICUadmission for elderly patients [9]. Thus, one mightspeculate that the increased use of NIV in this cohortmight be regarded as more beneficial for very old patients.
One of the main findings of the present study is theimprovement of prognosis of very old patients over theyears. Although raw mortality rates did not differ inrelation to time (Table 2), the severity of illness in veryold ICU patients increased during the study period. Risk-adjusted mortality on the other hand decreased over thestudy period (Fig. 2). We used multivariate analysis toevaluate this effect in the presence of possible con-founders and confirmed these results. After adjustment forgender and treatment centers (ICUs as fixed effects), theeffect of admission year on mortality was even morepronounced than indicated by univariate comparison ofrisk-adjusted mortality rates: prognosis of very oldpatients improved by 3% for each year (Table 3).
The impact of age on mortality has been widelydemonstrated and is well known [32, 33]. However,several studies have found other more important riskfactors, such as the severity of illness [7, 25]. Factorscorrelating with higher mortality rates in our study wereacute or chronic renal failure (OR 1.72 and 1.27,respectively), which has been mentioned in previousstudies as well [14, 25]. Moreover, functional status ofvery old patients before ICU admission has recently been
624

found to be of more importance for the prognosis than agealone [8].
The predominance of the female gender among thevery old population has been observed in many countries[24, 34]. Interestingly, the continuous rise in life expec-tancy is associated with an increasing gap between menand women [34]. In our study the proportion of femaleswas markedly different between patients aged B80 yearsand very old patients: the proportion was more than 1.5-fold higher in the cohort of very old patients (38.6%versus 63.2%, respectively). This difference may beexplained by women’s prolonged life expectancy.
Female patients had lower raw and risk-adjustedmortality rates, compared with males. This is interesting,since published reports about differences in mortalityrates between genders are contradictory. Higher hospitalmortality rates have been reported for septic females [35]as well as generally for critically ill women [36]. How-ever, other authors have reported a lesser risk in femalepostoperative ICU patients [37], or no difference inmortality rates between critically ill men and womendespite differences in treatment modalities [38]. Thesedifferences merit further and specific investigationsdirected towards possible reasons for an improved out-come in one or the other gender. Understanding of thesemechanisms might help us to treat our patients better.
Several limitations of our epidemiologic study have tobe considered. First, in contrast to a single-center study,multicenter studies include different institutions which all
have different characteristics. In this context we do nothave data about admission and triage decisions, as well asend-of-life decisions. Therefore, we entered ICUs aseffects into the logistic regression analysis, thus adjustingfor differences between them. Second, for evaluation ofparameters over the years, we included only those ICUsthat could report data on a substantial time span (definedas 9 out of 11 years). We thus missed several ICUs whicheither joined the data collection in later years or droppedout for various reasons. Thus, only a part of AustrianICUs have been included in this study. Despite the con-siderable number of evaluated patients, results have to beinterpreted with caution.
In this large cohort study of very old patients admittedto intensive care units, an increase in the proportion ofvery old patients over the years was found with a pre-ponderance of female gender. Although severity of illnessincreased over the years, risk-adjusted prognosis of veryold patients improved. The use of noninvasive mechanicalventilation tripled. These results point out that admissionand discharge policies of intensive care units with respectto very old patients should be carefully revisited. Furtherstudies are needed to determine the optimal duration andlevel of intensive care treatment for these patients in orderto optimize the benefit for patients and relatives.
Acknowledgments We thank the members of the ASDI studygroup and their study coordinators in each ICU for their valuablecontribution.
References
1. Department of Economic and SocialAffairs: World population ageing 2009.United Nations, New York.www.un.org/esa/population/publications/WPA2009. Accessed 26April 2011
2. Bongaarts J (2009) Human populationgrowth and the demographic transition.Phil Trans R Soc B 364:2985–2990
3. Lutz W, Sanderson W, Scherbov S(2008) The coming acceleration ofglobal population ageing. Nature451:716–719
4. Rosenthal GE, Kaboli PJ, Barnett MJ,Sirio CA (2002) Age and the risk of in-hospital death: insights from amultihospital study of intensive carepatients. J Am Geriatr Soc50:1205–1212
5. Creditor MC (1993) Hazards ofhospitalization of the elderly. AnnIntern Med 118:219–222
6. Bagshaw SM, Webb SAR, Delaney A,George C, Pilcher D, Hart GK, BellomoR (2009) Very old patients admitted tointensive care in Australia and NewZealand: a multi-centre cohort analysis.Crit Care 13:R45
7. Somme D, Maillet JM, Gisselbrecht M,Novara A, Ract C, Fagon JY (2003)Critically ill old and the oldest-oldpatients in intensive care: short- andlong-term outcomes. Intensive CareMed 29:2137–2143
8. Boumendil A, Somme D, Garrouste-Orgeas M, Guidet B (2007) Shouldelderly patients be admitted to theintensive care unit? Intensive Care Med33:1252–1262
9. Nguyen YL, Angus DC, Boumendil A,Guidet B (2011) The challenge ofadmitting the very elderly to intensivecare. Ann Intensive Care 1:29
10. Metnitz PhGH, Vesely H, Valentin A,Popow C, Hiesmayr M, Lenz K, KrennCG, Steltzer H (1999) Evaluation of aninterdisciplinary data set for nationalICU assessment. Crit Care Med27:1486–1491
11. Metnitz PhGH, Steltzer H, Popow C,Valentin A, Lenz K, Neumark J,Sagmuller G, Schwameis F, UrschitzM, Hiesmayr M (1997) Definition andevaluation of a documentation standardfor intensive care medicine: the ASDIpilot project. Wien Klin Wochenschr109:132–138
12. Le Gall JR, Lemeshow St, Saulnier F(1993) A new simplified acutephysiology score (SAPS II) based on aEuropean/North American multicenterstudy. JAMA 270:2957–2963
13. Miranda DR, De Rijk A, Schaufeli W(1996) Simplified therapeuticinterventions scoring system: the TISS-28 items—results from a multicenterstudy. Crit Care Med 4:64–73
14. Metnitz PhGH, Krenn CG, Steltzer H,Lang Th, Ploder J, Lenz K, Le Gall JR,Druml W (2002) Effect of acute renalfailure requiring renal replacementtherapy on outcome in critically illpatients. Crit Care Med 30:2051–2058
625

15. Hosmer DW, Lemeshow S (1995)Confidence interval estimates of anindex of quality performance based onlogistic regression models. Stat Med14:2161–2172
16. Bauer P, Poetscher BM, Hackl P (1988)Model selection by multiple testprocedures. Statistics 19:39–44
17. Angus DC, Kelley MA, Schmitz RJ,White A, Popovich J (2000) Currentand projected workforce requirementsfor care of the critically ill and patientswith pulmonary disease. JAMA284:2762–2770
18. Statistik Austria, Bundesanstalt StatistikOsterreich, A 1110 Vienna.http://www.statistik.at. Accessed 26April 2011
19. Garrouste-Orgeas M, Timsit JF,Montuclard L, Colvez A, Gattoliat O,Philippart F, Rigal G, Misset B, Carlet J(2006) Decision-making progress,outcome, and 1-year quality of life ofoctogenarians referred for intensivecare unit admission. Intensive CareMed 32:1045–1051
20. Hamel MB, Teno JM, Goldmann L,Lynn J, Davis RB, Galanos AN,Desbiens N, Connors AF, Wenger N,Phillips RS (1999) Patient age anddecisions to withhold life-sustainingtreatments from seriously ill,hospitalized adults. Ann Intern Med130:116–125
21. Garrouste-Orgeas M, Boumendil A,Pateron D, Aergerter P, Somme D,Simon T, Guidet B, ICE-CUB Group(2009) Selection of intensive care unitadmission criteria for patients aged80 years and over and compliance ofemergency and intensive care unitphysicians with the selected criteria: Anobservational, multicenter, prospectivestudy. Crit Care Med 37:2919–2928
22. Boumendil A, Aegerter P, Guidet B, theCUB-Rea Network (2005) Treatmentintensity and outcome of patients aged80 and older in intensive care units: amulticenter matched-cohort study.J Am Geriatr Soc 53:88–93
23. Lerolle N, Trinquart L, Bornstain C,Tadie JM, Imbert A, Diehl JL, FagonJY, Guerot E (2010) Increased intensityof treatment and decreased mortality inelderly patients in an intensive care unitover a decade. Crit Care Med 38:59–64
24. Needham DM, Bronskill SE, CalinawanJR, Sibbald WJ, Pronovost PJ, LaupacisA (2005) Projected incidence ofmechanical ventilation in Ontario to2026: preparing for the aging babyboomers. Crit Care Med 33:574–579
25. Van Den Noorgate N, Vogelaers D,Afschrift M, Colardyn F (1999)Intensive care for elderly patients:outcome and risk factors for in-hospitalmortality. Age Ageing 28:253–256
26. Nin N, Lorente JA, Paula M, FernandezSegoviano P, Penuelas O, SanchezFerrer A, Martinez Caro L, Esteban A(2008) Ageing increases thesusceptibility to injurious mechanicalventilation. Intensive Care Med34:923–931
27. Behrendt CE (2000) Acute respiratoryfailure in the United States: Incidenceand 31-day survival. Chest118:1100–1105
28. Ely EW, Wheeler AP, Thompson BT,Ancukiewicz M, Steinberg KP, BernardGR (2002) Recovery rate and prognosisin older persons who develop acute lunginjury and the acute respiratory distresssyndrome. Ann Intern Med 136:25–36
29. Evans TW (2001) Internationalconsensus conferences in intensive caremedicine: non-invasive positivepressure ventilation in acute respiratoryfailure. Intensive Care Med 27:166–178
30. Demoule A, Girou E, Richard JC, TailleS, Brochard L (2006) Increased use ofnoninvasive ventilation in Frenchintensive care units. Intensive Care Med32:1747–1755
31. Nava S, Grassi M, Fanfulla F,Domenighetti G, Carlucci A, Perren A,Dell’orso D, Vitacca M, Ceriana P,Karakurt Z, Clini E (2011) Non-invasive ventilation in elderly patientswith acute hypercapnic respiratoryfailure: a randomized controlled trial.Age Ageing 40:444–450
32. Nicolas F, Le Gall JR, Alperovitch A,Loirat P, Villers D (1987) Influence ofpatients’ age on survival, level oftherapy and length of stay in intensivecare units. Intensive Care Med 13:9–13
33. Goldhill DR, Sumner A (1998)Outcome of intensive care patients in agroup of British intensive care units.Crit Care Med 26:1337–1345
34. Oeppen J, Vaupel JW (2002) Brokenlimits to life expectancy. Science296:1029–1031
35. Pietropaoli AP, Glance LG, Oakes D,Fisher SG (2010) Gender differences inmortality in patients with sever sepsis orseptic shock. Gend Med 7:422–437
36. Fowler RA, Sabur N, Li P, Juurlink DN,Pinto R, Hladunewich MA, AdhikariNKJ, Sibbald WJ, Martin CM (2007)Sex- and age-based differences in thedelivery and outcomes of critical care.CMAJ 177:1513–1519
37. Reinikainen M, Niskanen M, Uusaro A,Ruokonen E (2005) Impact of genderon treatment and outcome of ICUpatients. Acta Anaesthesiol Scand49:984–990
38. Valentin A, Jordan B, Lang T,Hiesmayr M, Metnitz PGH (2003)Gender-related differences in intensivecare: a multiple center cohort study oftherapeutic interventions and outcomein critically ill patients. Crit Care Med31:1901–1907
626