Embed Size (px)
Citation preview

Development of the All Patient Refined DRGs(APR-DRGs)
Richard F. Averill, M.S., Norbert Goldfield, M.D., Barbara Steinbeck, ART, Thelma Grant, RRA, John Muldoon, M.H.A., A. Joseph Brough, M.D., James Gay, M.D.
The Diagnosis Related Groups (DRGs)are a patient classification system thatprovides a means of relating the type ofpatients a hospital treats (i.e., its casemix)to the costs incurred by the hospital. Thereare currently three major versions of theDRG in use. The basic DRGs are used bythe Health Care Financing Administration(HCFA) for hospital payment for Medicarebeneficiaries. The All Patient DRGs (AP-DRGs) are an expansion of the basicDRGs to be more representative of non-Medicare populations such as pediatricpatients. The All Patient Refined DRGs(APR-DRG) incorporate severity of illnessand risk of mortality subclasses into theDRGs.
The original objective of the DRGs wasto develop a patient classification systemthat related the types of patients treated tothe resources they consumed. Thus, theDRGs focused exclusively on resourceintensity. The HCFA DRGs and the AP-DRGs have remained focused on this lim-ited objective. As the health care industryhas evolved there has been increaseddemand for a patient classification systemthat can be used for applications beyondresource use, cost and payment. In partic-ular, a patient classification system isneeded for
• The comparison of hospitals across awide range of resource and outcomemeasures. Such comparisons are typi-cally disseminated to the public by statedata commissions
• The evaluation of differences in inpatientmortality rates
• The implementation and support of criti-cal pathways
• The identification of continuous qualityimprovement projects
• The basis of internal management andplanning systems
• The management of capitated paymentarrangements
In order to meet these needs, the objec-tive of the DRG system needed to beexpanded in scope to address patientseverity of illness and risk of mortality aswell as resource intensity. These patientattributes have the following meaning
Severity of illness: The extent of physi-ologic decompensation or organ systemloss of function
Risk of mortality: The likelihood ofdying
Resource intensity: The relative vol-ume and types of diagnostic, therapeuticand bed services used in the managementof a particular disease
The APR-DRGs expand the basic DRGstructure by adding four subclasses toeach DRG. The addition of the four sub-classes address patient differences relat-ing to severity of illness and risk ofmortality. Severity of illness and risk ofmortality relate to distinct patientattributes. Severity of illness relates to theextent of physiologic decompensation ororgan system loss of function experiencedby the patient while risk of mortality relatesto the likelihood of dying. For example, apatient with acute cholecystitis as the only
3M HIS Research Report 8-97 1
secondary diagnosis is considered a majorseverity of illness but a minor risk of mor-tality. The severity of illness is major sincethere is significant organ system loss offunction associated with acute cholecysti-tis. However, it is unlikely that the acutecholecystitis alone will result in patientmortality and thus, the risk of mortality forthis patient is minor. If additional diag-noses are present along with the acutecholecystitis, patient severity of illness andrisk of mortality may increase. For exam-ple, if peritonitis is present along with theacute cholecystitis, the patient is consid-ered an extreme severity of illness and amajor risk of mortality. Since severity of ill-ness and risk of mortality are distinctpatient attributes, separate subclasses areassigned to a patient for severity of illnessand risk of mortality. Thus, in the APR-DRG system a patient is assigned threedistinct descriptors.
• The base APR-DRG (e.g., APR-DRG194 - Heart Failure or APR-DRG 440 -Kidney Transplant)
• The severity of illness subclass• The risk of mortality subclass
The four severity of illness subclassesand the four risk of mortality subclassesare numbered sequentially from 1 to 4indicating respectively, minor, moderate,major or extreme severity of illness or riskof mortality. For applications such as eval-uating resource use or establishing patientcare guidelines, the APR-DRGs in con-junction with severity of illness subclass isused. For evaluating patient mortality theAPR-DRG in conjunction with the risk ofmortality subclass is used.
Although the subclasses are numbered1-4, the numeric values represent catego-ries and not scores. Thus, severity sub-class 4 congestive heart failure patients,are not comparable to severity subclass 4fractured leg patients. Thus, it is not mean-
ingful to average the numeric values (i.e.,1-4) of the severity of illness or risk of mor-tality subclasses across a group ofpatients to compute an average severityscore. However, the APR-DRG severityand risk of mortality subclasses can beused to compute an expected value for ameasure of interest (e.g., length of stay,cost, mortality). Expected values can becomputed using statistical techniquessuch as indirect rate standardization.
The underlying clinical principle of APR-DRGs is that the severity of illness or riskof mortality subclass of a patient is highlydependent on the patient’s underlyingproblem and that patients with high sever-ity of illness or risk of mortality are charac-terized by multiple serious diseases. In theAPR-DRGs, the assessment of the sever-ity of illness or risk of mortality of a patientis specific to the base APR-DRG to whicha patient is assigned. In other words, thedetermination of the severity of illness andrisk of mortality is disease-specific. Thus,the significance attributed to complicatingor comorbid conditions is dependent onthe underlying problem. For example, cer-tain types of infections are considered amore significant problem in a patient whois immunosuppressed than in a patientwith a fractured arm. In APR-DRGs, highseverity of illness or risk of mortality areprimarily determined by the interaction ofmultiple diseases. Patients with multiplecomorbid conditions involving multipleorgan systems constitute the difficult- to-treat patients who have poor outcomes.
The process used in the development ofthe APR-DRGs involved an iterative pro-cess of formulating clinical hypothesesand then testing the hypotheses with his-torical data. Separate clinical models weredeveloped for each of the 355 base APR-DRGs. Once the clinical model for severityof illness and risk of mortality was devel-
2 3M HIS Research Report 8-97
oped for each base APR-DRG, it wasevaluated with historical data. Patientswith a high severity of illness are, in gen-eral, expected to incur greater costs andpatients with a higher risk of mortality areexpected to die more frequently. Historicaldata was used to review the clinicalhypotheses. If there were discrepanciesbetween clinical expectations and the dataresults, the clinical expectations werealways utilized as the basis of the APR-DRGs. Thus, the APR-DRGs are a clinicalmodel that has been extensively reviewedwith historical data. The historical dataused in the development of version 15 ofthe APR-DRGs was a random, nation-wide, database of 5.7 million dischargeswhich included data from 657 hospitals, in35 states, from all payers. In addition, adatabase drawn from all discharges fromchildren’s hospitals in the United Stateswas also utilized.
Development of the APR-DRGs
The AP-DRGs were initially used as thebase DRGs in the formation of the APR-DRGs. A series of consolidations, addi-tions and modifications were made tothese initial APR-DRGs to create the baseAPR- DRGs. The first step in forming theAPR-DRGs was to consolidate all splitsbased on age and the presence of a com-plication or comorbidity. The APR-DRGsalso consolidated all splits based on dis-charge status of death. In addition to theseuniform consolidations of the initial APR-DRGs the following modifications to theinitial APR-DRGs were made.
Consolidate APR-DRGs Based onComplicated Principal Diagnosis
APR-DRGs that were defined based oncomplicated principal diagnoses were alsoconsolidated. For example, the initial APR-DRGs for appendectomies are differenti-
ated by whether or not there is a compli-cated principal diagnosis (e.g., withperitonitis). The APR-DRGs for appendec-tomies were consolidated and recognitionof the complicated principal diagnosis wassubsequently incorporated into the sub-class assigned within the APR-DRGs.
Pediatric Additions
While the AP-DRGs incorporated someof the pediatric modifications from the PM-DRGs, the APR-DRGs incorporated theremaining significant pediatric modifica-tions in the PM-DRGs. In addition, in con-junction with NACHRI the APR-DRGswere reviewed with a national pediatricdatabase. As a result of this review, addi-tional APR-DRGs were created. Forexample, scoliosis is one of the primaryreasons spinal fusions are performed onpediatric patients. Spinal fusions for scoli-osis tend to be more complex than spinalfusions for other clinical reasons such as aherniated disk. Thus, the APR-DRG forspinal fusions was subdivided based on aprincipal diagnosis of scoliosis.
Restructure Newborn APR-DRGs
The base APR-DRGs for newbornswere completely restructured. Surgicaland medical hierarchies were createdwithin each birthweight range. A medicalhierarchy is necessary because newbornsdo not have a principal diagnosis in theusual sense. Most newborns have a livenewborn status code as their principaldiagnosis. This does not permit assign-ment to a medical APR-DRG based onprincipal diagnosis. Thus, it was neces-sary to create a medical hierarchy for new-borns. The end result of this restructuringis the creation of 35 base APR-DRGs for newborns.
Consolidate APR-DRGs Based on Volume
The general trend toward outpatient sur-gery made some initial APR-DRGs
3M HIS Research Report 8-97 3

extremely low in volume. Such APR-DRGswere consolidated into other related APR-DRGs. For example, carpal tunnelreleases are now rarely performed on aninpatient basis. Thus, the APR-DRG forcarpal tunnel release was consolidatedinto the APR-DRG for nervous systemprocedures for peripheral nerve disorderswhich includes procedures such as tarsaltunnel release.
Add APR-DRGs for Mortality
The same base APR-DRGs are used inconjunction with both the severity of illnesssubclasses and risk of mortality sub-classes. Thus, some new APR-DRGswere necessary in order to reflect differ-ences in mortality. For example, initialAPR-DRG 45 (specific cerebrovasculardisorders except TIA) was subdivided intoAPR-DRG 45 (CVA with infarct) and APR-DRG 44 (intracranial hemorrhage) as aresult of the significantly higher mortalityrate for intracranial hemorrhage patients.
The end result of the consolidation pro-cess was to create 355 base APR-DRGs.The extensive modifications to base APR-DRGs required a complete renumbering ofthe base APR-DRGs. Once the baseAPR-DRGs were completed then fourseverity of illness subclasses and four riskof mortality subclasses were defined foreach of the APR-DRGs.
Overview of APR-DRG Subclass Assignment
The process of determining the sub-classes for an APR-DRG begins by firstassigning a severity of illness level and arisk of mortality level to each secondarydiagnosis. The term level is used whenreferring to the categorization of a second-ary diagnosis while the term subclass isused when referring to one of the subdivi-sions of an APR-DRG. For secondary
diagnoses there are four distinct severityof illness levels and four distinct risk ofmortality levels. The four levels are num-bered sequentially from 1 to 4 indicating,respectively, minor, moderate, major orextreme severity of illness or risk of mor-tality. Each secondary diagnosis isassigned to one of the four severity of ill-ness levels and one of the four risk of mor-tality levels. The severity of illness leveland risk of mortality level associated with apatient’s secondary diagnoses is just onefactor in the determination of a patient’soverall severity of illness subclass and riskof mortality subclass.
The assignment of a patient to a severityof illness or risk of mortality subclass takesinto consideration not only the level of thesecondary diagnoses but also the interac-tion among secondary diagnoses, age,principal diagnosis, and the presence ofcertain OR procedures and non-OR proce-dures. The subdivision of each of the 355APR-DRGs into the four subclasses, com-bined with the two error APR-DRGs (955,956), which are not subdivided, results in1422 APR-DRGs.
The process of determining the severityof illness or risk of mortality subclass of apatient consists of three phases. In thefirst phase, the level of each secondarydiagnosis is determined. Once the level ofeach secondary diagnosis is established,the second phase determines a base sub-class for the patient based on the patient’ssecondary diagnoses. In Phase III, thefinal subclass for the patient is determinedby incorporating the impact of principaldiagnosis, age, OR procedures, non-ORprocedures and combinations of catego-ries of secondary diagnoses. A detaileddescription of the determination of theseverity of illness subclass and risk ofmortality subclass will be presented sepa-rately.
4 3M HIS Research Report 8-97
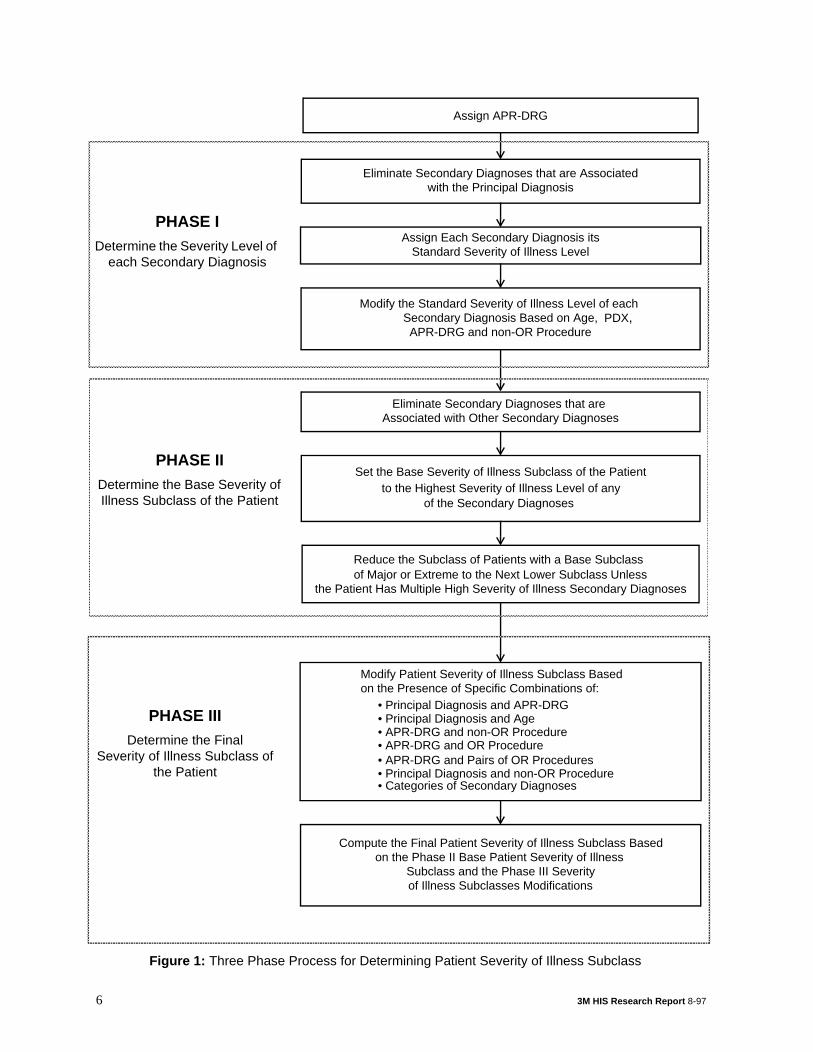
Determination of the Severity of Illness Subclass
The three phase process of determiningthe severity of illness subclass is summa-rized in Figure 1.
Phase I - Determining the Severity ofIllness Level of each SecondaryDiagnosis
Eliminate secondary diagnoses associ-ated with the principal diagnosis
If a secondary diagnosis is closelyrelated to the principal diagnosis, then thesecondary diagnosis is excluded from thedetermination of the severity of illnesssubclass. For example, a secondary diag-nosis of urinary retention is excluded fromthe determination of the severity of illnesssubclass if the principal diagnosis isbenign prostatic hypertrophy but isincluded for other principal diagnoses.
Assign each Secondary Diagnosis to its Standard Severity of Illness Level
Each secondary diagnosis is assignedto one of the four distinct severity of illnesslevels. Examples of the different severityof illness levels are contained in Table 1.
The severity of illness level for diabetesprogresses from minor for uncomplicateddiabetes to extreme for diabetes withhyperosmolar coma. Similarly, the severityof illness level for respiratory diagnosesprogresses from minor for bronchitis toextreme for respiratory failure.
The process of determining the severityof illness subclass for a patient begins byassigning each secondary diagnosis itsstandard severity of illness level. The nextstep is to modify the standard severity ofillness level based on other patientattributes. The patient attributes which canmodify the standard severity of illnesslevel of a secondary diagnosis are the
APR-DRG, the age of the patient and thepresence of certain nonoperating roomprocedures.
Modify the Standard Severity of Illness Level of a Secondary Diagnosis Based on the Principal Diagnosis
The standard severity of illness level forthe same secondary diagnoses will bemodified depending on the principal diag-nosis of the patient. For example, theseverity level of a secondary diagnosis ofacute anterolateral myocardial infarction,initial is moderate for patients with a princi-pal diagnosis of acute anterior wall myo-cardial infarction, initial. In general,secondary diagnoses that are closelyrelated to the principal diagnosis areexcluded from the determination of theseverity of illness subclass. However, anacute anterolateral myocardial infarction,initial represents an extension of the acuteanterior wall myocardial infarction, initialand is therefore not excluded and isassigned a severity of illness level of mod-erate.
Modify the Standard Severity of Illness Level of a Secondary Diagnosis Based on the APR-DRG
The standard severity of illness level forsome secondary diagnoses will be modi-fied depending on the APR-DRG to whichthe patient is assigned. Some examples ofAPR-DRG modifications are shown inTable 2. Stridor is common for patientswith bronchitis and asthma and is an inte-gral part of the disease. Thus, stridor isreduced to a minor severity of illness levelfor patients in the APR-DRG for bronchitisand asthma. Chronic renal failure signifi-cantly increases the severity of illnesslevel for patients with diabetes and, thus,is increased to a major severity of illnessfor the APR-DRG for diabetes. Cardiome-galy is not only common for CHF patients,
3M HIS Research Report 8-97 5
Eliminate Secondary Diagnoses that are Associatedwith the Principal Diagnosis
Assign Each Secondary Diagnosis itsStandard Severity of Illness Level
Modify the Standard Severity of Illness Level of each Secondary Diagnosis Based on Age,
Eliminate Secondary Diagnoses that are Associated with Other Secondary Diagnoses
Set the Base Severity of Illness Subclass of the Patient to the Highest Severity of Illness Level of any
Reduce the Subclass of Patients with a Base Subclass of Major or Extreme to the Next Lower Subclass Unless
Compute the Final Patient Severity of Illness Subclass Based
of the Secondary Diagnoses
APR-DRG and non-OR Procedure
the Patient Has Multiple High Severity of Illness Secondary Diagnoses
on the Phase II Base Patient Severity of Illness Subclass and the Phase III Severity
PHASE IDetermine the Severity Level of
each Secondary Diagnosis
PHASE IIDetermine the Base Severity of Illness Subclass of the Patient
PHASE IIIDetermine the Final
Severity of Illness Subclass of the Patient
Assign APR-DRG
of Illness Subclasses Modifications
Modify Patient Severity of Illness Subclass Based on the Presence of Specific Combinations of:
• Principal Diagnosis and Age• APR-DRG and non-OR Procedure• APR-DRG and OR Procedure• APR-DRG and Pairs of OR Procedures
• Principal Diagnosis and APR-DRG
• Principal Diagnosis and non-OR Procedure• Categories of Secondary Diagnoses
PDX,
6 3M HIS Research Report 8-97
Figure 1: Three Phase Process for Determining Patient Severity of Illness Subclass
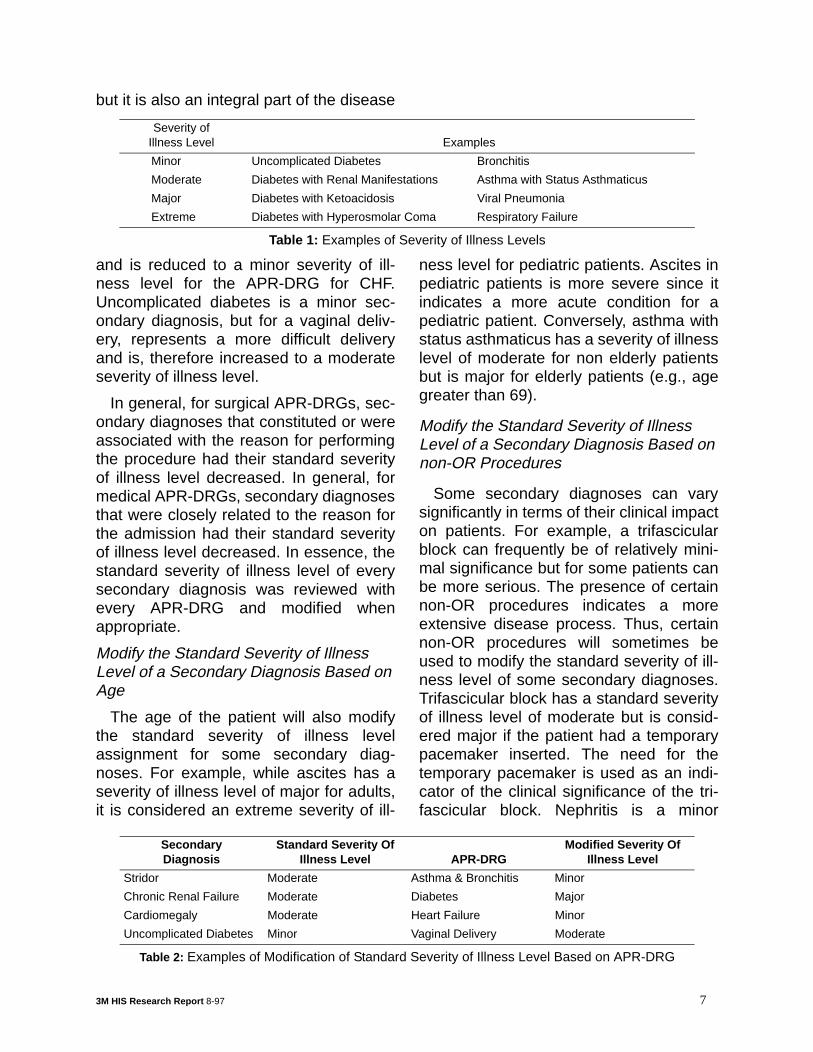
but it is also an integral part of the disease
and is reduced to a minor severity of ill-ness level for the APR-DRG for CHF.Uncomplicated diabetes is a minor sec-ondary diagnosis, but for a vaginal deliv-ery, represents a more difficult deliveryand is, therefore increased to a moderateseverity of illness level.
In general, for surgical APR-DRGs, sec-ondary diagnoses that constituted or wereassociated with the reason for performingthe procedure had their standard severityof illness level decreased. In general, formedical APR-DRGs, secondary diagnosesthat were closely related to the reason forthe admission had their standard severityof illness level decreased. In essence, thestandard severity of illness level of everysecondary diagnosis was reviewed withevery APR-DRG and modified whenappropriate.
Modify the Standard Severity of Illness Level of a Secondary Diagnosis Based on Age
The age of the patient will also modifythe standard severity of illness levelassignment for some secondary diag-noses. For example, while ascites has aseverity of illness level of major for adults,it is considered an extreme severity of ill-
ness level for pediatric patients. Ascites inpediatric patients is more severe since itindicates a more acute condition for apediatric patient. Conversely, asthma withstatus asthmaticus has a severity of illnesslevel of moderate for non elderly patientsbut is major for elderly patients (e.g., agegreater than 69).
Modify the Standard Severity of Illness Level of a Secondary Diagnosis Based on non-OR Procedures
Some secondary diagnoses can varysignificantly in terms of their clinical impacton patients. For example, a trifascicularblock can frequently be of relatively mini-mal significance but for some patients canbe more serious. The presence of certainnon-OR procedures indicates a moreextensive disease process. Thus, certainnon-OR procedures will sometimes beused to modify the standard severity of ill-ness level of some secondary diagnoses.Trifascicular block has a standard severityof illness level of moderate but is consid-ered major if the patient had a temporarypacemaker inserted. The need for thetemporary pacemaker is used as an indi-cator of the clinical significance of the tri-fascicular block. Nephritis is a minor
Severity of Illness Level Examples
Minor Uncomplicated Diabetes Bronchitis
Moderate Diabetes with Renal Manifestations Asthma with Status Asthmaticus
Major Diabetes with Ketoacidosis Viral Pneumonia
Extreme Diabetes with Hyperosmolar Coma Respiratory Failure
Table 1: Examples of Severity of Illness Levels
SecondaryDiagnosis
Standard Severity OfIllness Level APR-DRG
Modified Severity Of Illness Level
Stridor Moderate Asthma & Bronchitis Minor
Chronic Renal Failure Moderate Diabetes Major
Cardiomegaly Moderate Heart Failure Minor
Uncomplicated Diabetes Minor Vaginal Delivery Moderate
Table 2: Examples of Modification of Standard Severity of Illness Level Based on APR-DRG
3M HIS Research Report 8-97 7

severity of illness level but is considered amajor severity of illness if dialysis is per-formed. The dialysis is used to indicatethat the nephritis is more extensive.
Phase II - Determine the Base Severityof Illness Subclass for the Patient
Once each secondary diagnosis hasbeen assigned its standard severity of ill-ness level and the standard severity of ill-ness level of each secondary diagnosishas been modified based on the APR-DRG, age and presence of certain non-OR procedures, then the base severity ofillness subclass for the patient can bedetermined. The process of determiningthe base patient severity of illness sub-class begins with the elimination of certainsecondary diagnoses that are closelyrelated to other secondary diagnoses. Theelimination of these diagnoses preventsthe double counting of clinically similardiagnoses in the determination of theseverity of illness subclass of the patient.Once redundant diagnoses have beeneliminated, the base severity of illnesssubclass is determined based on theremaining secondary diagnoses.
Eliminate Certain Secondary Diagnoses from the Determination of the Severity of Illness Subclass of the Patient
Combinations of secondary diagnoses,which are closely related, are eliminated.Groups of closely related secondary diag-noses have been identified. If more thanone secondary diagnosis from the samegroup is present then only the secondarydiagnosis with the highest severity of ill-ness level is preserved. All other second-ary diagnoses in the group are eliminated.For example, the secondary diagnoses ofCVA and precerebral occlusion are in thesame secondary diagnosis group. Sincethe CVA is an extreme severity of illnesslevel and the precerebral occlusion is a
moderate severity of illness level the CVAwill be preserved and the precerebralocclusion will be eliminated if they are bothpresent as secondary diagnoses.
Combine all Secondary Diagnoses to Determine the Base Severity of Illness Subclass of the Patient
Once secondary diagnoses that arerelated to other secondary diagnoses havebeen eliminated, then the base patientseverity of illness subclass is set equal tothe maximum severity of illness levelacross all of the remaining secondarydiagnoses. For example, if there are fiveremaining secondary diagnoses and oneis a major severity of illness level and fourare a moderate severity of illness levelthen the base patient subclass is major.
Reduce the Base Severity of Illness Sub-class of Patients with a Major or Extreme Subclass unless the Patient has Multiple Secondary Diagnoses at a High Severity Level
In order to be assigned to the major orextreme severity of illness subclass apatient must have multiple secondarydiagnoses at a high severity of illnesslevel. High severity of illness patients arecharacterized by the presence of multiplehigh severity of illness secondary diag-noses. Patients with an extreme baseseverity of illness subclass must have twoor more secondary diagnoses that are anextreme severity of illness level or onesecondary diagnoses at an extreme sever-ity of illness level plus at least two othersecondary diagnoses at a major severityof illness level, otherwise the base severityof illness level is reduced to major.Patients with a major base severity of ill-ness subclass must have two or more sec-ondary diagnoses that are a major severityof illness level or one secondary diagnosisat a major severity of illness level plus at
8 3M HIS Research Report 8-97
least two other secondary diagnoses at amoderate severity of illness level. Other-wise the base severity of illness level isreduced to moderate. Thus, a secondarydiagnosis of AMI is not sufficient to assigna patient to an extreme severity of illnesssubclass. In addition to the AMI, theremust be at least one additional extremeseverity of illness secondary diagnosis(e.g., acute renal failure) or two or moreadditional major severity of illness second-ary diagnoses (e.g., CHF and diabeticketoacidosis).
Phase III - Determine the Final Severity of Illness Subclass of the Patient
Once the base patient severity of illnesssubclass is computed then the patientseverity of illness subclass may beincreased or decreased based on specificvalues of the following patient attributes.
• Combinations of principal diagnosis andAPR-DRG
• Combinations of age and principal diag-nosis
• Combinations of non-OR proceduresand principal diagnoses
• Combinations of non-OR proceduresand APR-DRGs
• Combinations of APR-DRGs and ORprocedures
• Combinations of APR-DRGs and pairsof OR procedures
• Combinations of categories of second-ary diagnoses
Previously, age and non-OR procedureswere used to modify the standard severityof illness level of a secondary diagnosis.However, age and non-OR procedurescan also be associated with the principaldiagnosis or the APR- DRG of the patient.Thus, the impact of age and non-OR pro-cedures is reassessed as part of the deter-mination of the severity of illness subclass
of the patient. Based on the patientattributes listed above, a series of modifi-cations to the base patient severity of ill-ness subclass are made during Phase III.The final patient severity of illness sub-class is computed based on the Phase IIbase patient severity of illness subclassand the modification to the base severityof illness subclass made in Phase III.
Modify Severity of Illness Subclass for the Patient Based on Combinations of Princi-pal Diagnosis and APR-DRG
The ICD-9-CM coding system will some-times include in a single diagnosis codeboth the underlying disease and an asso-ciated manifestation of the disease. Forexample, the code 25020 is diabetes withhyperosmolar coma. When this code isused as principal diagnosis the patient isassigned to the APR-DRG for diabetes. Ifthe patient has no secondary diagnosesthen the patient severity of illness sub-class would be minor. However, a diabeticpatient with hyperosmolar coma should beat a higher patient severity of illness sub-class than minor. In order to accommodatethis ICD-9-CM idiosyncrasy, if an ICD-9-CM diagnosis code that represents multi-ple diagnoses is principal diagnosis theseverity of illness subclass of the patient isincreased by a specified increment up to aspecified maximum subclass. For exam-ple, if diabetes with hyperosmolar coma isthe principal diagnosis, the severity of ill-ness subclass of the patient is increasedby 1 up to a maximum of a major subclass.
Within specific APR-DRGs some princi-pal diagnoses are indicative of higherseverity of illness relative to the other prin-cipal diagnoses in the APR-DRG. Forexample, the severity of illness subclass ofpatients in APR-DRG 221 (major smalland large bowel procedures) with a princi-pal diagnosis of acute vascular insuffi-ciency of the intestine is increased by 1 up
3M HIS Research Report 8-97 9
to a maximum of a moderate subclass.Relative to the other principal diagnosesassociated with the procedures in APR-DRG 221 (e.g., bowel malignancies) acutevascular insufficiency of the intestine rep-resents a more severely ill patient.
Conversely, within specific APR-DRGssome principal diagnoses are indicative oflower severity of illness relative to theother principal diagnoses in the APR-DRG. For example, the severity of illnesssubclass of patients in APR-DRG 404(thyroid, parathyroid & thyroglossal proce-dures) with a principal diagnosis of non-toxic uninodular goiter is decreased by 1for patients with a severity of illness sub-class that is major or lower. Relative to theother principal diagnoses associated withthe procedures in APR-DRG 404 (e.g.,malignant neoplasm of thyroid) nontoxicuninodular goiter represents a lessseverely ill patient.
Modify Severity of Illness Subclass for the Patient Based Combinations of APR-DRG, Age and Principal Diagnosis
For some principal diagnoses in specificAPR-DRGs, the patient’s age essentiallyrepresents a complicating factor. For spe-cific principal diagnoses and age combina-tions in certain APR-DRGs, the severity ofillness subclass of the patient is increasedby a specified increment up to a specifiedmaximum subclass. For example, for pedi-atric patients in APR-DRG 344 (osteomy-elitis) if bone infection is principaldiagnosis the severity of illness subclassis increased by 1 up to a maximum of amoderate subclass. The increase in theseverity of illness subclass indicates thatbone infection in a pediatric patient repre-sents a more severely ill patient.
Modify the Severity of Illness Subclass for the Patient Based on Combinations of non-OR Procedure and APR-DRG or Prin-
cipal Diagnosis
For some APR-DRGs the presence ofcertain non-OR procedures represents acomplicating factor. For certain APR-DRGand non-OR procedure combinations, thepatient severity of illness subclass isincreased by a specific increment up to aspecified maximum severity of illness sub-class. For example, for patients in APR-DRG 220 (major stomach, esophagealand duodenal procedures) the severity ofillness subclass is increased to the nexthigher subclass up to a maximum of majorif a gastrostomy is performed. In addition,specific principal diagnoses with an APR-DRG in combination with certain non-ORprocedures will increase the severity of ill-ness subclass by a specified increment upto a specified maximum severity of illnesssubclass. For example, principal diag-noses of malignancy in APR-DRG 343(pathological fractures and musculoskele-tal and connective tissue malignancy) areincreased by one level up to a maximumof major if radiation therapy or chemother-apy is performed.
Modify the Severity of Illness Subclass for the Patient Based on Combinations of OR Procedure and APR-DRG
Within specific APR-DRGs some ORprocedures are indicative of higher sever-ity of illness relative to the other OR proce-dures in the APR-DRG. For example, theseverity of illness subclass of patients inAPR-DRG 362 (mastectomy procedures)with an OR procedure of bilateralextended radical mastectomy is increasedby 1 up to a maximum of a moderate sub-class. Relative to the other OR proceduresin APR-DRG 362 (e.g., unilateral simplemastectomy) a bilateral extended radicalmastectomy represents a patient that ismore severely ill.
Conversely, within specific APR-DRGs
10 3M HIS Research Report 8-97

some OR procedures are indicative oflower severity of illness relative to theother OR procedures in the APR-DRG.For example, the severity of illness sub-class of patient in APR-DRG 21 (craniot-omy except for trauma) with an ORprocedure of skull biopsy is decreased by1 for patients with a severity of illness sub-class that is major or lower.
Modify the Severity of Illness Subclass for the Patient Based on Combinations of APR-DRGs and Pairs of OR Procedures
Within specific APR-DRGs some pairsof OR procedures are indicative of higherseverity of illness relative to the OR proce-dures in the APR-DRG. For example, theseverity of illness subclass of a patient inthe APR-DRG 172 (amputation for circula-tory system disorder) with both a periph-eral vascular bypass and an above theknee amputation is increased by 1 up to amaximum of a major subclass. Relative tothe other amputation patients in APR-DRG172, those with a peripheral vascularbypass followed by an above the kneeamputation are more severely ill.
Establish a Minimum Severity of Illness Subclass for the Patient Based on Combi-nations of Secondary Diagnoses
The presence of certain combinations ofsecondary diagnoses has great clinicalsignificance. The interaction of specificcombinations of secondary diagnosesmake treatment more difficult and typicallyindicate a more extensive disease pro-cess. Therefore, a minimum patient sever-ity of illness subclass is established ifcertain combinations of secondary diag-noses are present. The presence of multi-ple interacting diagnoses is characteristicof high severity of illness patients. A sub-set of secondary diagnoses will interactwith each other causing patient severity ofillness to be increased. This subset ofdiagnosis codes consists of 4068 individ-ual codes that have been assigned to oneof 60 secondary diagnosis categories. Thesecondary diagnoses in each category aresimilar clinically and have the same stan-dard severity of illness level. A completelist of the secondary diagnosis categoriesis in Table 4. The secondary diagnosis cat-egories listed in Table 4 apply only to non-newborn patients. A separate set of cate-gories is used for newborns. The severityof illness level of the secondary diagnosesin each category is shown in parenthesesin Table 4. As summarized in Table 3 thereare six different types of combinations of
Combination Type Combination of Categories
Additional Secondary Diagnoses Required
Minimum Severity of Illness
1 Specified combinations of two major categories
At least two additional secondary diagnoses of major or higher
Extreme (4)
2 Specified combinations of a major and moderate category
At least two additional secondary diagnoses of major or higher
Extreme (4
3 Specified combinations of two moderate categories
At least two additional secondary diagnoses of moderate or higher
Major (3)
4 Specified combinations of a mod-erate and minor category
At least two additional secondary diagnoses of moderate or higher
Major (3)
5 Specified combinations of two minor categories
At least two additional secondary diagnoses of minor or higher
Moderate (2)
6 Specified combination of two mod-erate categories
None Major (3)
Table 3: Combinations of Secondary Diagnosis Categories
3M HIS Research Report 8-97 11
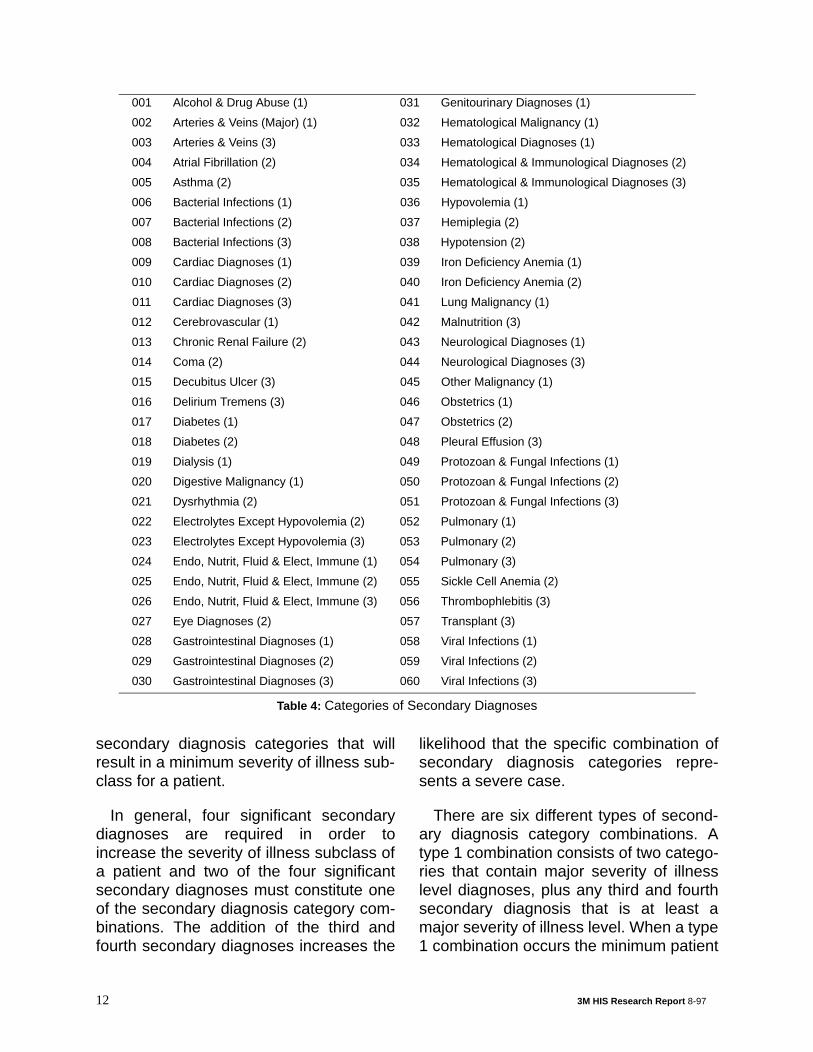
secondary diagnosis categories that willresult in a minimum severity of illness sub-class for a patient.
In general, four significant secondarydiagnoses are required in order toincrease the severity of illness subclass ofa patient and two of the four significantsecondary diagnoses must constitute oneof the secondary diagnosis category com-binations. The addition of the third andfourth secondary diagnoses increases the
likelihood that the specific combination ofsecondary diagnosis categories repre-sents a severe case.
There are six different types of second-ary diagnosis category combinations. Atype 1 combination consists of two catego-ries that contain major severity of illnesslevel diagnoses, plus any third and fourthsecondary diagnosis that is at least amajor severity of illness level. When a type1 combination occurs the minimum patient
001 Alcohol & Drug Abuse (1) 031 Genitourinary Diagnoses (1)
002 Arteries & Veins (Major) (1) 032 Hematological Malignancy (1)
003 Arteries & Veins (3) 033 Hematological Diagnoses (1)
004 Atrial Fibrillation (2) 034 Hematological & Immunological Diagnoses (2)
005 Asthma (2) 035 Hematological & Immunological Diagnoses (3)
006 Bacterial Infections (1) 036 Hypovolemia (1)
007 Bacterial Infections (2) 037 Hemiplegia (2)
008 Bacterial Infections (3) 038 Hypotension (2)
009 Cardiac Diagnoses (1) 039 Iron Deficiency Anemia (1)
010 Cardiac Diagnoses (2) 040 Iron Deficiency Anemia (2)
011 Cardiac Diagnoses (3) 041 Lung Malignancy (1)
012 Cerebrovascular (1) 042 Malnutrition (3)
013 Chronic Renal Failure (2) 043 Neurological Diagnoses (1)
014 Coma (2) 044 Neurological Diagnoses (3)
015 Decubitus Ulcer (3) 045 Other Malignancy (1)
016 Delirium Tremens (3) 046 Obstetrics (1)
017 Diabetes (1) 047 Obstetrics (2)
018 Diabetes (2) 048 Pleural Effusion (3)
019 Dialysis (1) 049 Protozoan & Fungal Infections (1)
020 Digestive Malignancy (1) 050 Protozoan & Fungal Infections (2)
021 Dysrhythmia (2) 051 Protozoan & Fungal Infections (3)
022 Electrolytes Except Hypovolemia (2) 052 Pulmonary (1)
023 Electrolytes Except Hypovolemia (3) 053 Pulmonary (2)
024 Endo, Nutrit, Fluid & Elect, Immune (1) 054 Pulmonary (3)
025 Endo, Nutrit, Fluid & Elect, Immune (2) 055 Sickle Cell Anemia (2)
026 Endo, Nutrit, Fluid & Elect, Immune (3) 056 Thrombophlebitis (3)
027 Eye Diagnoses (2) 057 Transplant (3)
028 Gastrointestinal Diagnoses (1) 058 Viral Infections (1)
029 Gastrointestinal Diagnoses (2) 059 Viral Infections (2)
030 Gastrointestinal Diagnoses (3) 060 Viral Infections (3)
Table 4: Categories of Secondary Diagnoses
12 3M HIS Research Report 8-97

severity of illness subclass is extreme. Anexample of a type 1 combination would bea major bacterial infection (Category 8)with a transplanted organ (Category 57). Ifa diagnosis from both these categories ispresent plus at least two other secondarydiagnoses that are at least a major sever-ity of illness level, then the minimumpatient severity of illness subclass will beextreme. A type 2 combination is the sameas a type one combination except that thetwo categories consist of a major severityof illness category and a moderate sever-ity of illness category. A type 3 combina-tion consists of two categories that containmoderate severity of illness level diag-noses plus any third and fourth secondarydiagnosis that is at least a moderate level.When a type 3 combination occurs, theminimum patient severity of illness sub-class is major. An example of a type 3combination would be a moderate viralinfection (category 59) with asthma (cate-gory 5).
A type 4 combination consists of a mod-erate severity of illness category and aminor severity of illness category plus anythird and fourth diagnosis that is at least amoderate severity of illness level. When atype 4 combination occurs, the minimumpatient severity of illness subclass ismajor. An example of a type 4 combinationwould be minor obstetrics (category 46)with moderate diabetes (category 18). Atype 5 combination consists of two catego-ries that contain minor severity of illnesslevel diagnoses plus two additional minorseverity of illness level diagnoses. When atype 5 combination occurs the maximumpatient severity of illness subclass is mod-erate. An example of a type 5 combinationwould be diabetes (category 17) withminor bacterial infection (category 6).Combination type 6 is a special combina-tion type for normal newborns (APR-DRGs626 and 640).
Compute the Final Patient Severity of Ill-ness Subclass
The final patient severity of illness sub-class is computed based on the Phase IIbase patient severity of illness subclassand the Phase III modified patient severityof illness subclasses. If all the modifiedPhase III modified severity subclasses aregreater than or equal to the Phase II baseseverity of illness subclass, then the finalseverity of illness subclass is computed asthe maximum of the Phase II and III sever-ity subclasses. If all of the modified PhaseIII severity of illness subclasses are lessthan or equal to the Phase II base severityof illness subclass the final severity of ill-ness subclass is computed as the Phase IIbase severity of illness subclass minusone. If the Phase III modified severity of ill-ness subclasses includes modified sever-ity of illness subclasses that are bothgreater and less than the Phase II basedseverity of illness subclass, then the modi-fied Phase III subclass relating to combi-nations of secondary diagnoses andprocedures will take priority in determiningthe final severity of illness subclass. Thecombination of the APR-DRG and the finalpatient severity of illness subclass consti-tute the complete APR-DRG description ofthe severity of illness of the patient.
Summary of APR-DRG Severity of Ill-ness Subclass Assignment Logic
The following is a summary of the stepsinvolved in computing the APR-DRGseverity of illness subclass of a patient.
Phase I - Determine the Severity of Illness Level of Each Secondary Diagnosis
1. Eliminate secondary diagnoses thatare associated with the principal diag-nosis.
2. Assign each secondary diagnosis itsstandard severity of illness level.
3M HIS Research Report 8-97 13
3. Modify the standard severity of illnesslevel of each secondary diagnosisbased on the age of the patient.
4. Modify the standard severity of illnesslevel of each secondary diagnosisbased on the principal diagnosis andthe APR-DRG to which the patient isassigned.
5. Modify the standard severity of illnesslevel of each secondary diagnosisbased on the APR-DRG to which thepatient is assigned.
6. Modify the standard severity of illnesslevel of each secondary diagnosesbased on the presence of certain non-OR procedures.
Phase II - Determine the Base Severity of Illness Subclass of the Patient
7. Eliminate all secondary diagnoses thatare in the same secondary diagnosisgroup except the secondary diagnosiswith the highest severity of illnesslevel.
8. Compute the base patient severity ofillness subclass as the maximum of allthe secondary diagnosis severity of ill-ness levels.
9. If the base patient severity of illnesssubclass from Step 8 is major orextreme, then reduce the base patientseverity of illness subclass to the nextlower severity of illness subclassunless there are multiple secondarydiagnoses at a high severity of illnesslevel.
Phase III - Determine the final severity of illness subclass of the patient
10.Modify the patient severity of illnesssubclass based on the principal diag-nosis.
11. Modify the patient severity of illnesssubclass based on the age of thepatient.
12.Modify the patient severity of illness
subclass based on a combination ofthe APR-DRG and the presence of cer-tain non-OR procedures.
13.Modify the patient severity of illnesssubclass based on combinations ofAPR-DRGs and OR procedures.
14.Modify the patient severity of illnesssubclass based on combinations ofAPR-DRGs and pairs of OR proce-dures.
15.Modify the patient severity of illnesssubclass based on the combination ofprincipal diagnosis and the presence ofcertain non-OR procedures.
16.Modify the patient severity of illnesssubclass based on the presence ofspecific combinations of categories ofsecondary diagnoses.
17.Compute the final patient severity of ill-ness subclass based on the Phase IIbase patient severity of illness sub-class from Step 9 and the modifica-tions of the patient severity of illnesssubclasses from Steps 10-16.
Determination of the Risk of Mortality Subclass
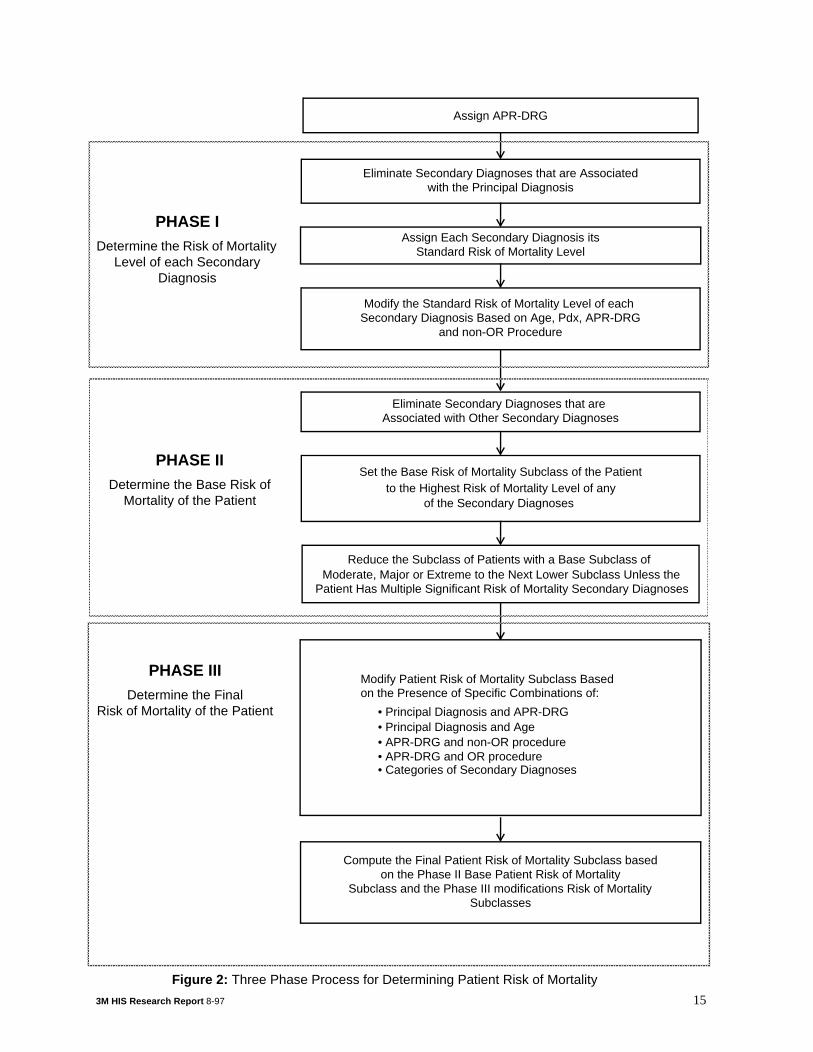
The three phase process of determiningthe risk of mortality subclass is summa-rized in Figure 2. The three phase processof determining the risk of mortality sub-class parallels the three phases in thedetermination of the severity of illnesssubclass. In the first phase, the risk ofmortality of each secondary diagnosis isdetermined. Once the risk of mortalitylevel of each secondary diagnosis isestablished, the second phase determinesa base risk of mortality subclass for thepatient based on the patient’s secondarydiagnoses. In Phase III the final subclassfor the patient is determined by incorporat-ing the impact of principal diagnosis, ORprocedures, non-OR procedures and com-binations of categories of secondary diag-
14 3M HIS Research Report 8-97
Eliminate Secondary Diagnoses that are Associatedwith the Principal Diagnosis
Assign Each Secondary Diagnosis itsStandard Risk of Mortality Level
Modify the Standard Risk of Mortality Level of each Secondary Diagnosis Based on Age, Pdx, APR-DRG
Eliminate Secondary Diagnoses that are Associated with Other Secondary Diagnoses
Set the Base Risk of Mortality Subclass of the Patient to the Highest Risk of Mortality Level of any
Reduce the Subclass of Patients with a Base Subclass of Moderate, Major or Extreme to the Next Lower Subclass Unless the
Compute the Final Patient Risk of Mortality Subclass based
of the Secondary Diagnoses
and non-OR Procedure
Patient Has Multiple Significant Risk of Mortality Secondary Diagnoses
on the Phase II Base Patient Risk of MortalitySubclass and the Phase III modifications Risk of Mortality
PHASE IDetermine the Risk of Mortality
Level of each Secondary Diagnosis
PHASE IIDetermine the Base Risk of
Mortality of the Patient
PHASE IIIDetermine the Final
Risk of Mortality of the Patient
Assign APR-DRG
Subclasses
Modify Patient Risk of Mortality Subclass Based on the Presence of Specific Combinations of:
• Principal Diagnosis and APR-DRG
• APR-DRG and OR procedure
• Principal Diagnosis and Age• APR-DRG and non-OR procedure
• Categories of Secondary Diagnoses
3M HIS Research Report 8-97 15
Figure 2: Three Phase Process for Determining Patient Risk of Mortality
noses.
Phase I - Determining the Risk ofMortality Level of each SecondaryDiagnosis
Eliminate Secondary Diagnoses Associ-ated with the Principal Diagnosis
This step is identical to the correspond-ing step in the determination of the sever-ity of illness subclass.
Assign each Secondary Diagnosis its Standard Risk of Mortality Level
Each secondary diagnosis is assignedone of four distinct risk of mortality levels.In general, except for malignancies andcertain extreme acute diseases such asacute renal failure, the risk of mortalitylevel tends to be lower than the severity ofillness level for the same diagnosis. Mor-tality is relatively rare. There are a limitednumber of diagnoses that significantlyincrease the risk of mortality. For example,traumatic amputation of the arm, acutecholecystitis and acute osteomyelitis areall at a major severity of illness level sincethey represent serious disease with signifi-cant loss of organ function. However, theypresent relatively low risk of mortality andtherefore are assigned to a minor risk ofmortality level. Example of secondarydiagnoses that would have an extremerisk of mortality are intracranial hemor-rhage, acute vascular insufficiency ofintestine, AMI and acute renal failure.
Modify the Standard Risk of Mortality of a Secondary Diagnosis Based on the APR-DRG
The standard risk of mortality level forsome secondary diagnoses will be modi-fied depending on the APR-DRG to whichthe patient is assigned. For example, aminor risk of mortality diagnosis such asright bundle branch block is increased to amoderate risk of mortality for the APR-
DRG for circulatory disorders with AMI.
Modify the Standard Risk of Mortality Level of a Secondary Diagnosis Based on Age
The age of the patient modifies the stan-dard risk of mortality level of some diag-noses. In general, the risk of mortality islower for pediatric patients. For example,the risk of mortality for diabetes withketoacidosis is lowered from moderate tominor for pediatric patients. Conversely, ingeneral, the risk of mortality is higher forelderly patients. For example, the risk ofmortality for atrial flutter is increased froma minor risk of mortality to a moderate riskof mortality for patients with age greaterthan 69.
Modify the Standard Risk of Mortality Level of a Secondary Diagnosis Based on the Principal Diagnosis
The standard risk of mortality level forsome secondary diagnoses will be modi-fied depending on the principal diagnosisof the patient. For example, the risk ofmortality of a secondary diagnosis ofacute anterolateral myocardial infarction,initial is moderate for patients with a princi-pal diagnosis of acute anterior wall myo-cardial infarction, initial. In general,secondary diagnoses that are closelyrelated to the principal diagnosis areexcluded from the determination of the riskof mortality subclass. However, an antero-lateral acute myocardial infarction repre-sents an extension of the anterior wallmyocardial infarction and is therefore notexcluded and is assigned a risk of mortal-ity level of moderate.
Modify the Standard Risk of Mortality Level of a Secondary Diagnosis Based on non-OR Procedures
Certain non-OR procedures will some-times be used to modify the standard risk
16 3M HIS Research Report 8-97

of mortality level of some secondary diag-noses. Subendocardial infarction has astandard risk of mortality level of moderatebut is considered extreme if the patienthad a pulsation balloon implanted. Theneed for the pulsation balloon is used asan indicator of the clinical significance ofthe subendocardial infarction.
Phase II - Determine the Base Risk of Mortality Subclass for the Patient
Once each secondary diagnosis hasbeen assigned its standard risk of mortal-ity level and the standard risk of mortalitylevel of each secondary diagnosis hasbeen modified based on the APR-DRG,principal diagnosis, non-OR procedureand age, then the base risk of mortalitysubclass for the patient can be deter-mined. The process of determining thebase patient risk of mortality subclassbegins with the elimination of certain sec-ondary diagnoses that are closely relatedto other secondary diagnoses. The elimi-nation of these diagnoses prevents thedouble counting of clinically similar diag-noses in the determination of the risk ofmortality subclass of the patient. Onceredundant diagnoses have been elimi-nated, the base risk of mortality subclassis determined based on the remaining sec-ondary diagnoses.Eliminate Certain Sec-ondary Diagnoses from the Determinationof the Risk of Mortality Subclass of thePatient
This step is identical to the correspond-ing step in the determination of the sever-ity of illness subclass.
Combine all Secondary Diagnoses to Determine the Base Risk of Mortality Sub-class of the Patient
Once secondary diagnoses that arerelated to other secondary diagnoses havebeen eliminated, then the base patient risk
of mortality subclass is set equal to themaximum risk of mortality level across allof the remaining secondary diagnoses.For example, if there are five remainingsecondary diagnoses and one is a majorrisk of mortality level and four are a mod-erate risk of mortality level then the basepatient risk of mortality subclass is major.
Except for Certain Secondary Diagnoses Reduce the Base Risk of Mortality Sub-class unless the Patient has Multiple Sec-ondary Diagnoses with a Significant Risk of Mortality
In general, high risk of mortality patientsare characterized by multiple secondarydiagnoses with a significant risk of mortal-ity. In order for the base risk of mortalitysubclass to be extreme, there must be twoor more extreme risk of mortality second-ary diagnoses present or a single extremerisk of mortality secondary diagnosis plustwo or more major risk of mortality second-ary diagnoses. The only exception is thatfor a limited set of extreme risk of mortalitysecondary diagnoses such as rupturedaortic aneurysm no additional secondarydiagnoses are necessary or only one addi-tional major risk of mortality secondarydiagnosis is necessary. If the above multi-ple high risk of mortality criteria is not metthen the base patient subclass is reducedto major or moderate depending on thespecific additional diagnoses that arepresent. Patients with a base risk of mor-tality subclass of major are reduced tomoderate unless in addition to the majorrisk of mortality secondary diagnosis thereare at least one additional major risk ofmortality secondary diagnosis or two moreadditional secondary diagnoses with amoderate risk of mortality. The only excep-tion is that for a limited set of major risk ofmortality secondary diagnoses such asacute pulmonary edema. no additionalsecondary diagnoses are necessary.
3M HIS Research Report 8-97 17
Patients with a base risk of mortality sub-class of moderate are reduced to minorunless there are two or more additionalmoderate risk of mortality secondary diag-noses present.
Phase III - Determine the Final Risk of Mortality Subclass of the Patient
Once the base patient risk of mortalitysubclass is computed then the risk of mor-tality subclass may be increased ordecreased based on specific values of thefollowing patient attributes.
• Combinations of principal diagnosis andAPR-DRG
• Combination of age and principal diag-nosis
• Combinations of non-OR proceduresand APR-DRG
• Combinations of APR-DRGs and ORprocedures
• Combinations of categories of second-ary diagnoses
Previously, age and non-OR procedureswere used to modify the standard risk ofmortality level of a secondary diagnosis.However, age and non-OR procedurescan also be associated with the principaldiagnosis or the APR-DRG of the patient.Thus, the impact of age and non-OR pro-cedures is reassessed as part of the deter-mination of the risk of mortality subclass ofthe patient. Based on the patient attributeslisted above, a series of modifications tothe base patient risk of mortality subclasswill be made during Phase III. The finalpatient risk of mortality subclass will becomputed based on the Phase II basepatient risk of mortality subclass and themodification to the base risk of mortalitysubclass made in Phase III.
Modify the Risk of Mortality Subclass for the Patient Based on Principal Diagnosis
Within specific APR-DRGs some princi-pal diagnoses are indicative of higher riskof mortality relative to the other principaldiagnoses in the APR-DRGs. For exam-ple, the risk of mortality subclass ofpatients in APR-DRG 309 (hip and femurprocedures except major joint for non-trauma) with a principal diagnosis of sec-ondary malignant neoplasm of bone isincreased by 1 up to a maximum of a mod-erate subclass. Relative to the other prin-cipal diagnoses associated with theprocedures in APR-DRG 309, secondarymalignant neoplasm of bone represents agreater risk of mortality.
Modify the Risk of Mortality Subclass for the Patient Based on Combinations of APR-DRG, Age and Principal Diagnosis
For some principal diagnoses in specificAPR-DRGs, the patient’s age essentiallyrepresents a complicating factor. For spe-cific principal diagnoses and age combina-tions in certain APR-DRGs, the risk ofmortality subclass of the patient isincreased by a specified increment up to aspecified maximum subclass. For exam-ple, for elderly patients more than 80 yearsold in APR-DRG 44 (intracranial hemor-rhage) if intracerebral hemorrhage is theprincipal diagnosis, the risk of mortalitysubclass is increased by 1 up to a maxi-mum of a moderate subclass. Theincrease in the risk of mortality subclassindicates that intracranial hemorrhage inan elderly patient represents a higher riskof mortality.
Modify the Risk of Mortality Subclass for the Patient Based on Combinations of non-OR Procedure and APR-DRG
For some APR-DRGs the presence ofcertain non-OR procedures represents acomplicating factor. For certain APR-DRGand non-OR procedure combinations, therisk of mortality subclass is increased by a
18 3M HIS Research Report 8-97
specific increment up to a specified maxi-mum risk of mortality subclass. For exam-ple, for patients in APR-DRG 194 (heartfailure) the risk of mortality subclass isincreased by two up to a maximum ofextreme if mechanical ventilation greaterthan 96 hours is performed.
Modify the Risk of Mortality Subclass for the Patient Based on Combinations of OR Procedure and APR-DRG
Within specific APR-DRGs some ORprocedures are indicative of higher risk ofmortality relative to the other OR proce-dures in the APR-DRG. For example, therisk of mortality subclass of patients inAPR-DRG 443 (kidney and urinary tractprocedures for non-malignancy), isincreased by 2 up to a maximum of majorif the procedure bilateral nephrectomy isperformed. Relative to other procedures inDRG 443, a bilateral nephrectomy repre-sents a patient that has a higher risk ofmortality.
Modify the Risk of Mortality Subclass for the Patient Based on Combinations of Secondary Diagnoses
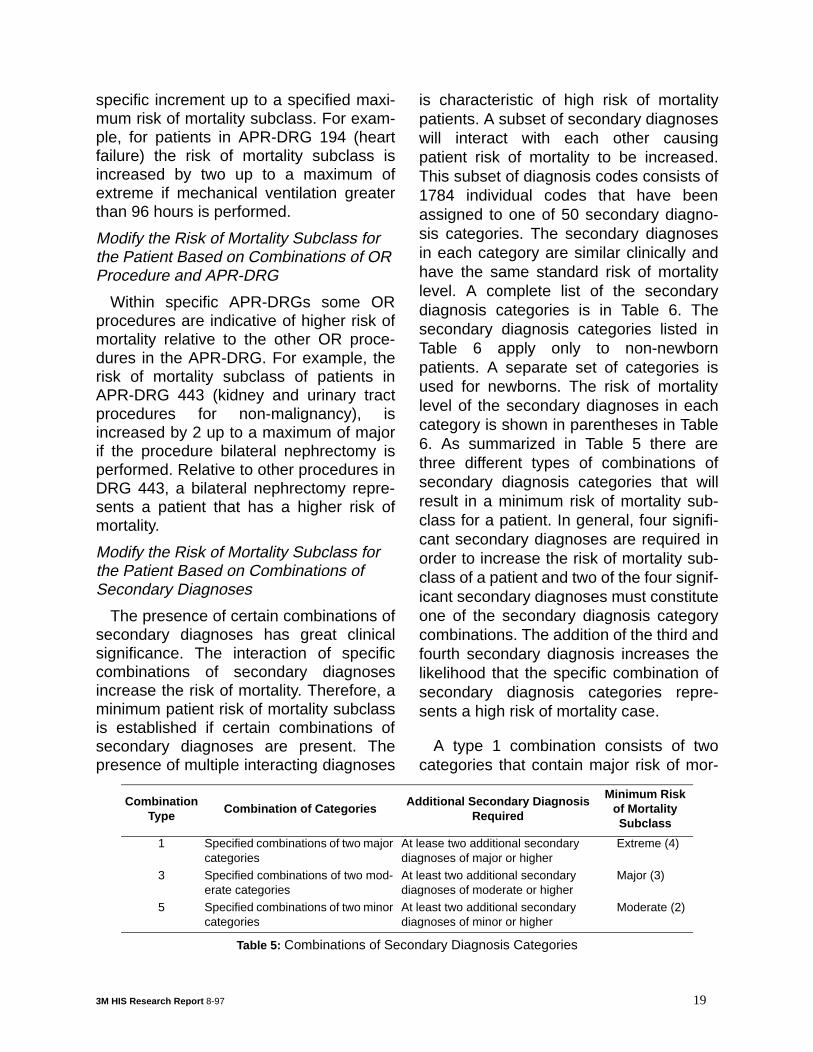
The presence of certain combinations ofsecondary diagnoses has great clinicalsignificance. The interaction of specificcombinations of secondary diagnosesincrease the risk of mortality. Therefore, aminimum patient risk of mortality subclassis established if certain combinations ofsecondary diagnoses are present. Thepresence of multiple interacting diagnoses
is characteristic of high risk of mortalitypatients. A subset of secondary diagnoseswill interact with each other causingpatient risk of mortality to be increased.This subset of diagnosis codes consists of1784 individual codes that have beenassigned to one of 50 secondary diagno-sis categories. The secondary diagnosesin each category are similar clinically andhave the same standard risk of mortalitylevel. A complete list of the secondarydiagnosis categories is in Table 6. Thesecondary diagnosis categories listed inTable 6 apply only to non-newbornpatients. A separate set of categories isused for newborns. The risk of mortalitylevel of the secondary diagnoses in eachcategory is shown in parentheses in Table6. As summarized in Table 5 there arethree different types of combinations ofsecondary diagnosis categories that willresult in a minimum risk of mortality sub-class for a patient. In general, four signifi-cant secondary diagnoses are required inorder to increase the risk of mortality sub-class of a patient and two of the four signif-icant secondary diagnoses must constituteone of the secondary diagnosis categorycombinations. The addition of the third andfourth secondary diagnosis increases thelikelihood that the specific combination ofsecondary diagnosis categories repre-sents a high risk of mortality case.
A type 1 combination consists of twocategories that contain major risk of mor-
Combination Type
Combination of CategoriesAdditional Secondary Diagnosis
Required
Minimum Risk of Mortality Subclass
1 Specified combinations of two major categories
At lease two additional secondary diagnoses of major or higher
Extreme (4)
3 Specified combinations of two mod-erate categories
At least two additional secondary diagnoses of moderate or higher
Major (3)
5 Specified combinations of two minor categories
At least two additional secondary diagnoses of minor or higher
Moderate (2)
Table 5: Combinations of Secondary Diagnosis Categories
3M HIS Research Report 8-97 19
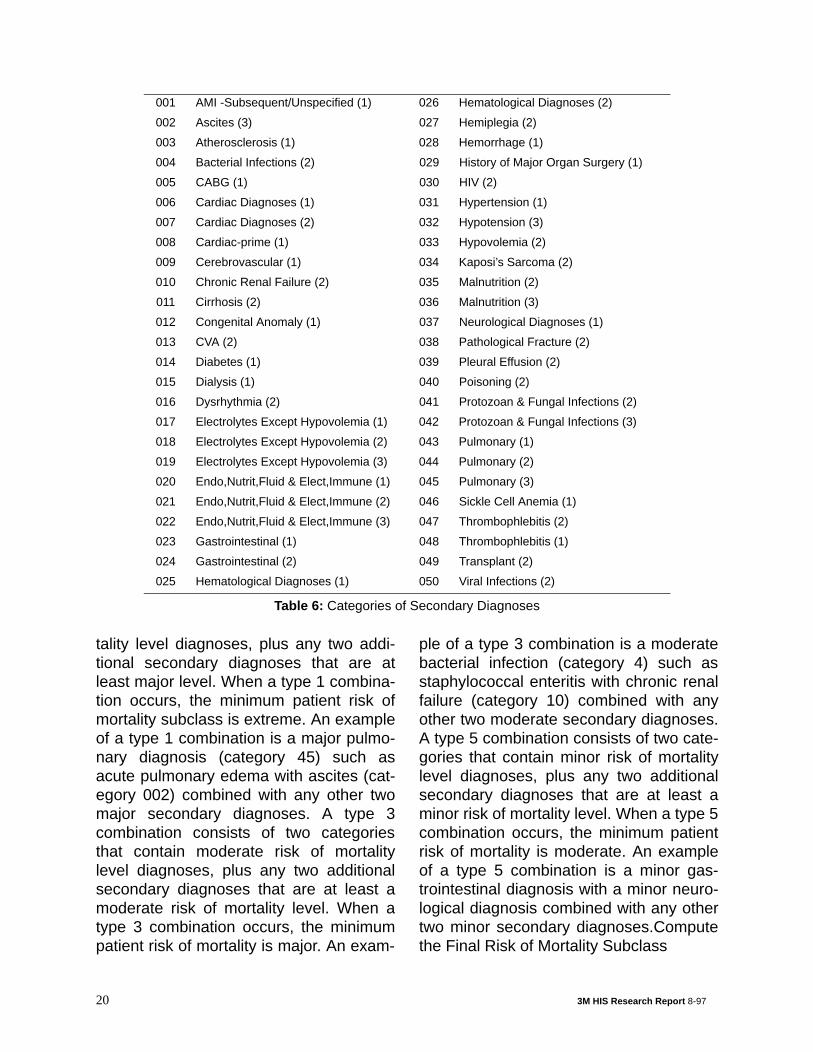
tality level diagnoses, plus any two addi-tional secondary diagnoses that are atleast major level. When a type 1 combina-tion occurs, the minimum patient risk ofmortality subclass is extreme. An exampleof a type 1 combination is a major pulmo-nary diagnosis (category 45) such asacute pulmonary edema with ascites (cat-egory 002) combined with any other twomajor secondary diagnoses. A type 3combination consists of two categoriesthat contain moderate risk of mortalitylevel diagnoses, plus any two additionalsecondary diagnoses that are at least amoderate risk of mortality level. When atype 3 combination occurs, the minimumpatient risk of mortality is major. An exam-
ple of a type 3 combination is a moderatebacterial infection (category 4) such asstaphylococcal enteritis with chronic renalfailure (category 10) combined with anyother two moderate secondary diagnoses.A type 5 combination consists of two cate-gories that contain minor risk of mortalitylevel diagnoses, plus any two additionalsecondary diagnoses that are at least aminor risk of mortality level. When a type 5combination occurs, the minimum patientrisk of mortality is moderate. An exampleof a type 5 combination is a minor gas-trointestinal diagnosis with a minor neuro-logical diagnosis combined with any othertwo minor secondary diagnoses.Computethe Final Risk of Mortality Subclass
001 AMI -Subsequent/Unspecified (1) 026 Hematological Diagnoses (2)
002 Ascites (3) 027 Hemiplegia (2)
003 Atherosclerosis (1) 028 Hemorrhage (1)
004 Bacterial Infections (2) 029 History of Major Organ Surgery (1)
005 CABG (1) 030 HIV (2)
006 Cardiac Diagnoses (1) 031 Hypertension (1)
007 Cardiac Diagnoses (2) 032 Hypotension (3)
008 Cardiac-prime (1) 033 Hypovolemia (2)
009 Cerebrovascular (1) 034 Kaposi’s Sarcoma (2)
010 Chronic Renal Failure (2) 035 Malnutrition (2)
011 Cirrhosis (2) 036 Malnutrition (3)
012 Congenital Anomaly (1) 037 Neurological Diagnoses (1)
013 CVA (2) 038 Pathological Fracture (2)
014 Diabetes (1) 039 Pleural Effusion (2)
015 Dialysis (1) 040 Poisoning (2)
016 Dysrhythmia (2) 041 Protozoan & Fungal Infections (2)
017 Electrolytes Except Hypovolemia (1) 042 Protozoan & Fungal Infections (3)
018 Electrolytes Except Hypovolemia (2) 043 Pulmonary (1)
019 Electrolytes Except Hypovolemia (3) 044 Pulmonary (2)
020 Endo,Nutrit,Fluid & Elect,Immune (1) 045 Pulmonary (3)
021 Endo,Nutrit,Fluid & Elect,Immune (2) 046 Sickle Cell Anemia (1)
022 Endo,Nutrit,Fluid & Elect,Immune (3) 047 Thrombophlebitis (2)
023 Gastrointestinal (1) 048 Thrombophlebitis (1)
024 Gastrointestinal (2) 049 Transplant (2)
025 Hematological Diagnoses (1) 050 Viral Infections (2)
Table 6: Categories of Secondary Diagnoses
20 3M HIS Research Report 8-97
The final patient risk of mortality sub-class is computed based on the Phase IIbase patient risk of mortality subclass andthe Phase III modified patient severity ofillness subclasses. If all the modifiedPhase III modified risk of mortality aregreater than or equal to the Phase II baserisk of mortality subclass, then the finalrisk of mortality subclass is computed asthe maximum of the Phase II and III risk ofmortality subclasses. If all of the modifiedPhase III risk of mortality subclasses areless than or equal to the Phase II base riskof mortality subclass the final risk of mor-tality subclass is computed as the Phase IIbase risk of mortality subclass minus one.If the Phase II modified risk of mortalitysubclasses includes modified risk of mor-tality subclasses that are both greater andless than the Phase II based risk of mortal-ity subclass, then the modified Phase IIIsubclass relating to combinations of sec-ondary diagnoses and procedures willtake priority in determining the final risk ofmortality subclass. The combination of theAPR-DRG and the final patient risk of mor-tality subclass constitute the completeAPR-DRG description of the risk of mortal-ity of the patient.
Summary of APR-DRG Risk of Mortality Subclass Assignment Logic
The following is a summary of the stepsinvolved in computing the APR- DRG riskof mortality subclass of a patient.
Phase I - Determine the Risk of MortalityLevel of each Secondary Diagnosis
1. Eliminate all secondary diagnoses thatare associated with the principal diag-nosis of the patient.
2. Assign each secondary diagnosis itsstandard risk of mortality.
3. Modify the standard risk of mortalitylevel of each secondary diagnosis
based on the age of the patient.4. Modify the standard risk of mortality
level of each secondary diagnosisbased on the principal diagnosis andthe APR-DRG to which the patient isassigned.
5. Modify the standard risk of mortalitylevel of each secondary diagnosisbased on the APR-DRG to which thepatient is assigned.
6. Modify the standard risk of mortalitylevel of each secondary diagnosisbased on the presence of certain non-OR procedures.
Phase II - Determine the Base Risk of Mortality Subclass of the Patient
7. Eliminate all secondary diagnoses thatare in the same secondary diagnosisgroup except the secondary diagnosiswith the highest risk of mortality level.
8. Compute the base patient risk of mor-tality subclass as the maximum of allthe secondary diagnosis risk of mortal-ity levels.
9. Reduce the base patient risk of mortal-ity subclass unless there are multiplesecondary diagnoses at a significantrisk of mortality.
Phase III - Determine the Final Risk of Mortality Subclass of the Patient
10.Modify the patient risk of mortality sub-class based on the principal diagnosis.
11. Modify the patient risk of mortality sub-class based on the age of the patient.
12.Modify the patient risk of mortality sub-class based on a combination of theAPR-DRG and the presence of certainnon-OR procedures.
13.Modify the patient risk of mortality sub-class based on combinations of APR-DRGs and OR procedures.
14.Modify the patient risk of mortality sub-class based on the presence of spe-cific combinations of categories of
3M HIS Research Report 8-97 21
secondary diagnoses.15.Compute the final patient risk of mor-
tality subclass based on the Phase IIbase patient severity of illness sub-class from Step 9; and the modifica-tions of the patient risk of mortalitysubclasses from Steps 10-14.
Conclusion
The APR-DRGs form a clinically coher-ent set of severity of illness and risk ofmortality adjusted patient groups. TheAPR-DRGs are designed to describe thecomplete cross-section of patients seen inacute care hospitals.
Through APR-DRGs hospitals, consum-ers, payers and regulators can gain anunderstanding of the patients beingtreated, the costs incurred and within rea-sonable limits, the services and outcomesexpected. Through APR-DRGs, areas forimprovement in efficiency and areas withpotential quality problems can be identi-fied. The classification of patients intoAPR-DRGs is constantly evolving. As theICD-9-CM coding scheme changes or asmedical technology or practice changes,the APR-DRG definitions will be updatedto reflect these changes.
© 3M 1997
22 3M HIS Research Report 8-97