Embed Size (px)
Citation preview
Diabetes Knowledge as a Moderator of Reactions to Illness by Patients With Insulin-Dependent Diabetes Mellitus'
MICHAEL J STRUBE,' JOHN H. YOST, AND DEBRA HAIRE-JOSHU Washington University
We examined patient knowledge as a moderator of psychological reactions to illness among patients with insulin-dependent diabetes mellitus. We reasoned that knowledgeable patients would have the most severe reactions to their illness because the causal implications of good or poor metabolic control would be most apparent. Accordingly, we expected that more knowledgeable patients would react more nega- tively than less knowledgeable patients to poor metabolic control but would react more positively to good metabolic control. Results from a sample of 46 patients with insulin-dependent diabetes mellitus supported this hypothesis. These findings suggest that increased patient knowledge may not produce uniformly positive results. Patient education programs must consider the psychological implications of patient knowl- edge in addition to the physiological consequences.
Diabetes mellitus is the third leading cause of death in the United States, affecting over 5 million people (Cox, Gonder-Frederick, Pohl, & Penne- baker, 1986; Karam, 1981; Wing, Epstein, Nowalk, & Lamparski, 1986). The essential deficit in diabetes is the body's inability to regulate blood sugar level precisely. Accordingly, the treatment of diabetes emphasizes the careful and coordinated regulation of diet, exercise, and insulin (cf. Surwit, Fein- glos, & Scovern, 1983). In essence, the patient must replace a sophisticated biological regulator with a vigilant and volitional strategy. Not surprisingly, there is wide individual variability in the course of the disease because it is difficult for patients to approximate closely the delicate metabolic balance that is achieved automatically in individuals without diabetes. Indeed, studies of diabetes self-care indicate that patients often administer insulin incorrectly, do not conduct or interpret urine or blood glucose tests cor- rectly, and do not eat prescribed foods or eat with sufficient regularity (Watkins, Roberts, Williams, Martin, & Coyle, 1967; Watkins, Williams, Martin, Hogan, & Anderson, 1967; Williams, Anderson, Watkins, & Coyle, 1967; see also Johnson, Freund, Silverstein, Hansen, & Malone, 1990). Con- sequently, researchers have attempted to identify the predictors of patients' ability to adhere to a strict and complicated treatment regimen.
'We thank two anonymous reviewers for their helpful comments on a n earlier version of this
'Correspondence concerning this article should be addressed to Michael J Strube, Depart- paper.
ment of Psychology, Washington University, St. Louis, M O 63130.
944
Journal of Applied Social Psychology, 1993,23, 12, pp. 944-958. Copyright @ 1993 by V. H. Winston & Son, Inc. All rights reserved.
DIABETES KNOWLEDGE AND REACTIONS TO ILLNESS 945
One of the most commonly identified predictors, and the focus of this investigation, is patient knowledge about diabetes and its treatment. Interest in patient knowledge follows from the sensible assumption that a patient cannot be expected to carry out a complicated treatment plan unless that patient has a sound understanding of treatment components and their rela- tion to the disease. This knowledge requirement is particularly acute for the diabetes patient because all treatment components are interdependent. Blood glucose level is influenced by diet, exercise, and exogenous insulin so that a change in one component necessitates a precise change in other com- ponents. Surprisingly, however, the presumed importance of knowledge has not been sustained by consistent positive relations between knowledge and treatment adherence or between knowledge and metabolic control (e.g., Ludvigsson, 1977; McCaul, Glasgow, & Schafer, 1987; Watkins, Williams et al., 1967; see also Fisher, Delamater, Bertelson, & Kirkley, 1982; Goodall & Halford, 1991; Wilkinson, 1987).
These inconsistent findings suggest a t least three possible roles for patient knowledge as a determinant of patient adherence and well-being. First, patient knowledge may be unimportant, at least beyond some minimal level of information needed for survival. If most patients have acquired this min- imum information, then little relation between knowledge and metabolic control could be expected. Second, the effects of patient knowledge may be indirect, influencing other variables that then determine adherence and con- trol. Some support for this view is provided by the demonstration that knowledge affects attitudes and beliefs about diabetes, which, in turn, influ- ence adherence and self-care (e.g., de Weerdt, Visser, Kok, & Van der Veen, 1990; de Weerdt, Visser, & Van der Veen, 1989; see also Glasgow et al., 1989; Hampson, Glasgow, & Toobert, 1990). Finally, increased knowledge may not have uniformly positive effects. The regulation gains that greater knowl- edge may produce could be offset by psychological deficits. We investigated this latter possibility.
One consequence of increased knowledge is that more knowledgeable patients are in a better position to interpret and understand their current level of metabolic control. Given the central role that the patient plays in regulating diet, exercise, and insulin intake, the causal implications of good or poor control are potentially more apparent to the patient who under- stands better the importance of self-regulation. As a result, relatively more knowledgeable patients may have stronger psychological reactions to their illness than patients with less knowledge. When blood glucose is under good control, a knowledgeable patient should benefit more psychologically be- cause the causal implication is that the control is due to careful self- regulation. On the other hand, a knowledgeable patient should suffer more psychologically from knowing that blood glucose is under poor control. In

946 STRUBE, YOST, AND HAIRE-JOSHU
this case, knowledge of the many ways that the patient can affect metabolic outcome implicates the patient as the cause of poor control. By contrast, less knowledgeable patients should be influenced less psychologically by know- ing their level of blood glucose control. In the present study, we tested this hypothesized interaction of knowledge and blood glucose control on psycho- logical responses to illness among patients with insulin-dependent diabetes mellitus.
Because our hypotheses rest on attributional assumptions, we also exam- ined the patients’ causal ascriptions for their level of blood glucose control. We expected knowledgeable patients to make more internal attributions for their level of metabolic control, particularly if that control was poor. Attri- butional processing is most likely for unexpected or negative events (e.g., Frieze, 1976; Wong & Weiner, 1981; for a review see Fiske & Taylor, 1991), and the important role of the patient in metabolic control should be more apparent as a causal source for knowledgeable patients. By contrast, self- serving attributions (a common response to good and poor outcomes) were not expected because outcomes in this study were open to public scrutiny (see Fiske & Taylor, 1991).
Methods
Subjects
Subjects were 46 outpatients (12 men, 34 women) with insulin-dependent diabetes mellitus. The participants were sampled from a diabetes research center at a large midwestern university hospital and from the private practice of a diabetologist. Average age of the sample was 32.91 years ( S D = 11.34, Range: 15-61). The majority of the sample was Caucasian (76. I%), relatively well educated (9 1.3% completed high school, 60.9% some college), currently married (54.3%), and employed in white-collar occupations (52.2%). The patients had known of their diagnoses for an average of 18.43 years ( S D = 8.76, Range: 5-48).
Procedure
Patients were contacted by phone within 2 weeks following a scheduled visit to the diabetes clinic. Those agreeing to participate (70.77%) completed a packet containing a measure of diabetes knowledge, a measure of their psychological reactions to diabetes, and an attribution m e a ~ u r e . ~
We also collected several individual difference measures: The Krantz Health Opinion Survey (Krantz, Baum, & Wideman, 1980), the Jenkins Activity Survey (Jenkins, Zyzanski, & Rosen- man, 1979), the Psychological Adjustment to Illness Scale (Derogatis, 1977, 1983), and the
DIABETES KNOWLEDGE AND REACTIONS TO ILLNESS 947
Diabetes knowledge. We measured knowledge about diabetes with Form A of the Diabetes Knowledge Test (DKT; Hess & Davis, 1983). The DKT contains 38 true-false and multiple-choice items that assess factual knowl- edge about diabetes and its treatment. Reported overall internal consistency for the DKT is high (a! = .89). Validation evidence indicates that the measure is sensitive to instructional interventions, correlates predictably with type of diabetes, but is not highly correlated with general education level (Hess & Davis, 1983). The DKT can be scored for five subscales: carbohydrates, blood sugar, basics, food exchanges, and insulin. We examined the total knowledge score as well as each subscale as moderators of patients’ reactions to their illness.
Reactions to illness. Patients also completed the Reactions to Illness Scale (RIS; Pritchard, 1973). The RIS contains 50 items that measure cognitive, behavioral, and emotional reactions by patients to their illness. Each item is a statement reflecting an illness reaction (e.g., “I am defenseless against it,” “It is a punishment which I do not deserve,”“I think of it as a problem to be tackled”); patients rated their agreement with the statements on a scale ranging from not at all (1) to extremely (4). The RIS has been used success- fully in a previous study of coping with illness among patients with diabetes (Rhodewalt & Marcroft, 1988) as well as studies of illness reactions by other patient groups (e.g., Rhodewalt & Strube, 1985).
Illness attributions. To test our assumptions about the role of attributions in reactions to illness, we asked patients to complete a five-item attribution questionnaire. We modeled the measure after the Attributional Style Ques- tionnaire (Peterson et al., 1982) so that the multidimensional aspects of causal attributions could be assessed. The patients were first asked to indi- cate what they thought was the major reason for their current level of blood glucose control. Then, patients rated those causes along five dimensions: (a) internal versus external, (b) stable versus unstable, (c) global versus specific, (d) controllable versus uncontrollable, and (e) degree of responsibility. All ratings were made on 5-point scales with higher ratings indicating external, unstable, uncontrollable, global, low-responsibility attributions.
Blood glucose control. Blood glucose control was assessed by glycosylated hemoglobin (HbA1). The percentage of glycosylated hemoglobin is propor- tional to the amount of time that red blood cells have been exposed to blood glucose. The percentage of hemoglobin that is glycosylated is an index of the
Miller Behavioral Style Questionnaire (Miller, 1987). Findings relevant to these measures are reported elsewhere (Strube, Haire-Joshu, & Yost, 1987; Strube, Yost, & Haire-Joshu, 1987). These individual differences did not interact with knowledge in the prediction of reactions to illness. Importantly, sample means for these measures were similar to those reported for non- patient samples, suggesting that patients in the present study were not atypical along several commonly measured psychological dimensions.

948 STRUBE, YOST, AND HAIRE-JOSHU
average blood glucose control over the previous 8 to 12 weeks (cf. Kennedy & Merimec, 1981; Ziel & Davidson, 1987). Reference values vary slightly by assay methods, but there is general agreement that values above 10% indi- cate poor control. Patient blood samples were taken during their visit to the clinic and patients completed the questionnaire materials within 4 weeks of having their blood samples drawn. Assays for patients’ blood samples were conducted by one laboratory.
Results
Preliminary Analyses
Overall, patients were fairly knowledgeable about diabetes; the overall average percentage of correct items on the DKT was 77.80%, and subscale performances ranged from 69.93% for the food subscale to 91.96% for the blood sugar subscale. Knowledge subscales were moderately correlated (mean r = .35). The sample also demonstrated modest blood glucose control (HbAI M = 8.84, SD = 2.19). Overall knowledge and blood glucose control were not significantly related, r(44) = .034, nor were knowledge subscale scores significantly related to blood glucose control (rs ranged from -.092 to .13). These latter results are not surprising given that past research has also failed to find a consistently positive relation between knowledge and control.
Prior to major analyses, items from the RIS were collapsed into simpler composites. Pritchard (1973) suggests that the 50 statements should be col- lapsed to 3 1 basic reactions. However, examination of the item intercorrela- tions indicated that Pritchard’s subscales are highly redundant and that a simpler set of subscales could be constructed. Accordingly, we used principal components analysis to identify the major RIS dimensions. Principal com- ponents analysis ensures that the resulting composites will be uncorrelated and will account for the maximum original score variance. Based on the scree test (see Cliff, 1988), we extracted the first three principal components, rotated these to simple structure using the varimax procedure, and calcu- lated component scores (i.e., 2 score^).^ The three components accounted for 52.60% of the variance in the original scores, indicating that the majority of original score information was retained, but with considerable savings in the number of composites needed to account for that information. The largest rotated principal component had an eigenvalue of 11.64 and accounted for
4As Cliff (1988) has noted, reliance on the traditional eigenvalues-greater-than-one rule for component retention can result in relatively trivial and unreliable components. The scree test, by contrast, is more conservative and retains components that are more likely to reflect mean- ingful and replicable dimensions. This more conservative approach was dictated by our small sample size. Note also that we use principal components analysis in this study to reduce the number of redundant significance tests; our intent is not to identify all of the basic dimensions of the RIS. That task would require much larger samples and cross-validation.
DIABETES KNOWLEDGE AND REACTIONS TO ILLNESS 949
23.76% of the original score variance. Items (k = 18) that loaded highly on this component (> .50) indicated clear negative affect (depression, fear, anger, misery, resentment), the perception of the illness as an enemy and a punishment, the desire to avoid or escape from the illness, and self-blame for the illness.' For brevity, this component will be referred to as resentment and self-blame. Note that self-blame items on the RIS refer to blame for the illness and not to current levels of blood glucose control. Thus they represent a more global self-incrimination than the internal-external ratings from the additional attribution measure. The second largest rotated principal compo- nent accounted for 20.80% of the original score variance and had an eigen- value of 10.19. Items (k = 21) that loaded highly on this component .50) also indicated clear negative affect (shame, depression, anger, misery, anx- iety). In addition, this component was defined by clear feelings of unrecover- able loss, weakness, and the desire to hide the illness from others. This component seems best labeled as shame and resignation. The third rotated principal component accounted for 8.04% of the original score variance and had an eigenvalue of 3.94. This component was defined by items (k = 5) measuring resentment of the help and sympathy of others, the desire to put thoughts of the illness out of mind, and denial of the illness as a problem to be tackled or as a challenge. The label avoidance and denial appears to capture the nature of this component adequately.
Major analyses were conducted using multiple regression with RIS princi- pal components and attributions as dependent measures and DKT, HbA1, and the product of DKT and HbAl as independent variables. The product variable tests the interaction between knowledge and blood glucose control, after the simple effects of knowledge and glucose control have been entered into the analysis (see Cohen & Cohen, 1975). In addition, the number of years since diagnosis of the disease was included as a covariate to control for length of exposure to the illness.6
Reactions to Illness
We first examined the moderating effect of total knowledge scores. A multivariate analysis of variance was conducted to assess the impact of
'We defined components based on item loadings of .5 or greater to ensure clear interpreta- tion. Such loadings are highly significant for this sample size and ensure that the item shares a t least 25% of its variance with the component.
6Preliminary analyses examined age, gender, time since diagnosis, and education as addi- tional moderators. The small sample limited the power of these tests but they indicated no significant moderator effects. We also examined more complex models relating knowledge to blood glucose control. If there is a critical knowledge level beyond which additional knowledge is unimportant, then a nonlinear relation between knowledge and control would be expected. No evidence for a nonlinear relation was found, although this does not rule out a nonlinear model because of the generally high knowledge levels in this sample (i.e., restricted range).
950 STRUBE, YOST, AND HAIRE-JOSHU
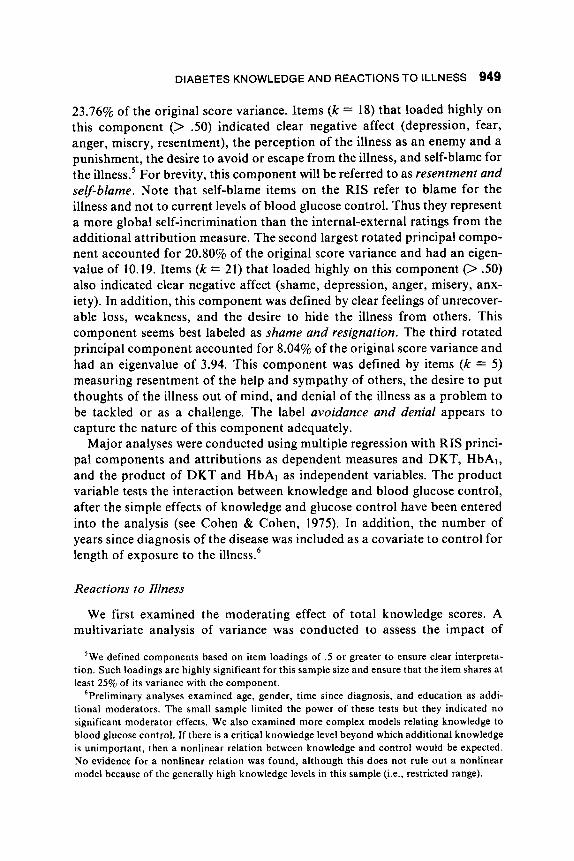
knowledge and blood glucose control on the set of RIS components. Univari- ate analyses were also conducted to assess the impact on individual RIS components. The multivariate analysis indicated a significant Knowledge X HbAl interaction, multivariate F(3, 39) = 3.36, p < .05, Wilks’s A = .80. Each RIS component contributed positively to the multivariate linear com- bination (i.e., canonical variate) represented by this interaction. The load- ings for resentment and self-blame, shame and resignation, and avoidance and denial were .66, .47, and .39, respectively. The interaction is illustrated in Figure 1; for ease of presentation, the canonical variate estimates for points along each independent variable corresponding to f .75 standard deviations were calculated (cf. Cohen & Cohen, 1975). As Figure 1 indicates, the pre- dicted impact of knowledge is quite apparent: High knowledge in the pres- ence of poor blood glucose control is accompanied by the most negative reactions to illness (higher Z scores), whereas high knowledge in the presence of good glucose control is accompanied by the most positive reactions. Univariate analyses indicated similar patterns for each RIS component, although the univariate interaction achieved significance only for the resentment and self-blame component, F(1, 41) = 4.61, p < .05.
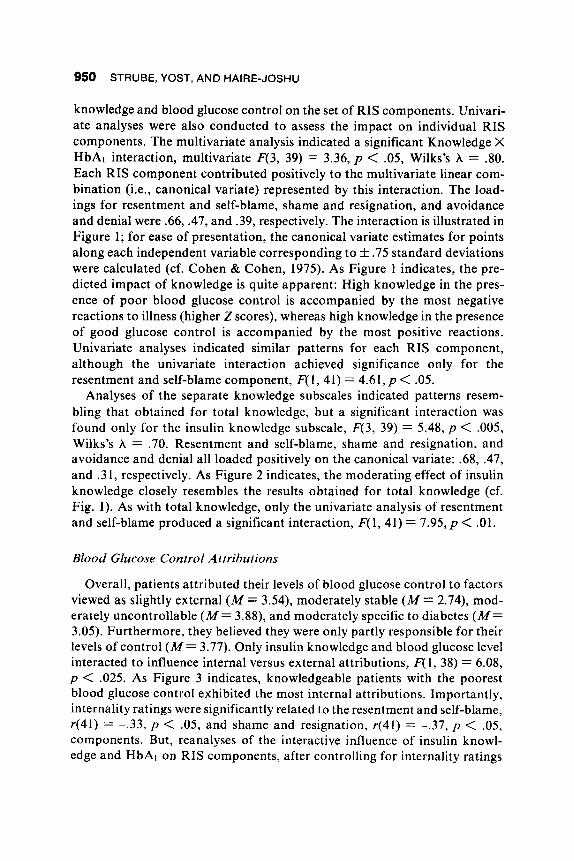
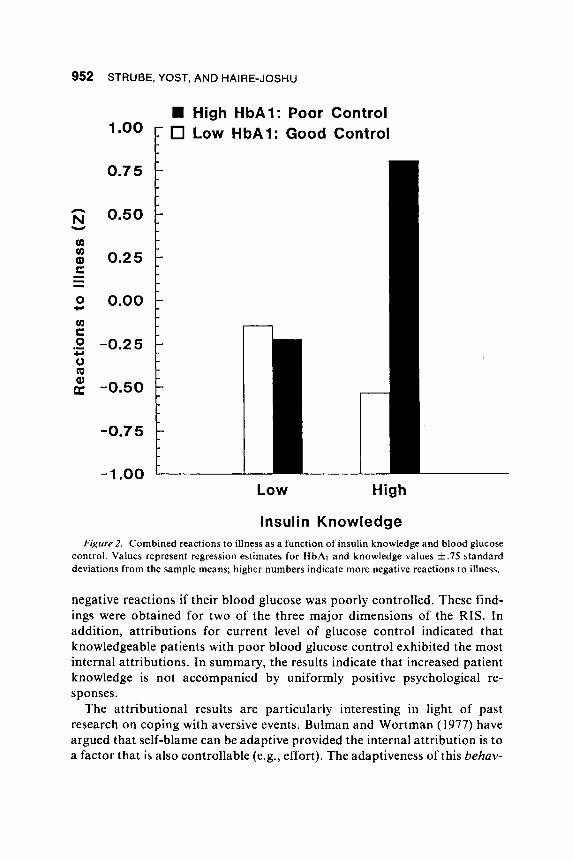
Analyses of the separate knowledge subscales indicated patterns resem- bling that obtained for total knowledge, but a significant interaction was found only for the insulin knowledge subscale, F(3, 39) = 5.48, p < .005, Wilks’s A = .70. Resentment and self-blame, shame and resignation, and avoidance and denial all loaded positively on the canonical variate: .68, .47, and .31, respectively. As Figure 2 indicates, the moderating effect of insulin knowledge closely resembles the results obtained for total knowledge (cf. Fig. 1). As with total knowledge, only the univariate analysis of resentment and self-blame produced a significant interaction, F( 1, 41) = 7.95, p < .01.
Blood Glucose Control Attributions
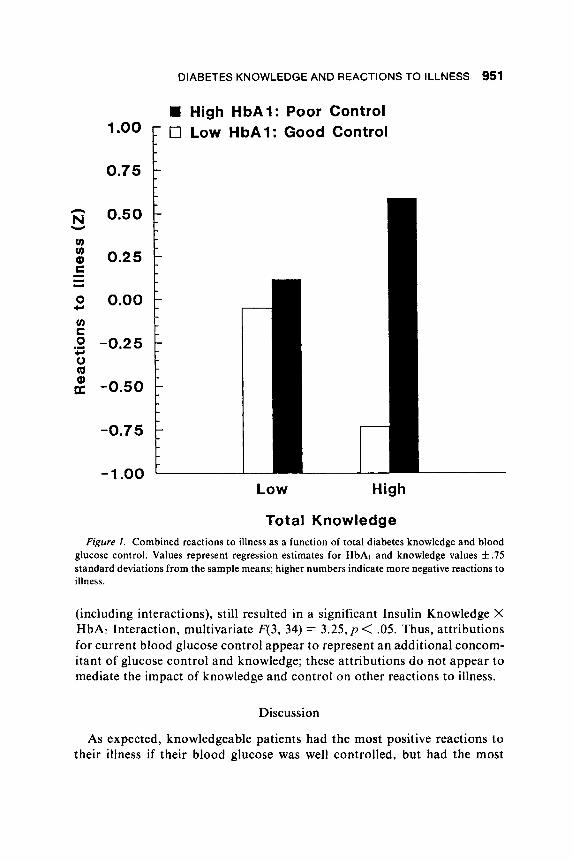
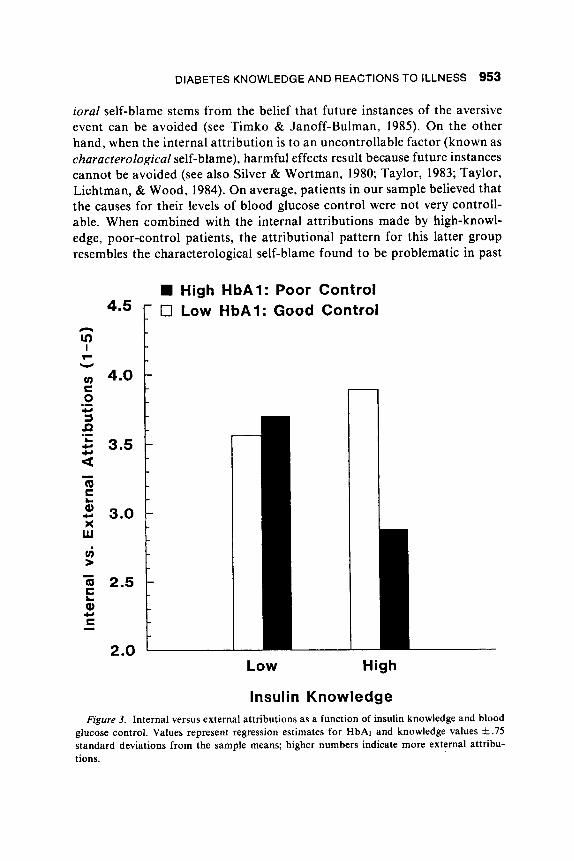
Overall, patients attributed their levels of blood glucose control to factors viewed as slightly external ( M = 3.54), moderately stable ( M = 2.74), mod- erately uncontrollable ( M = 3.88), and moderately specific to diabetes ( M = 3.05). Furthermore, they believed they were only partly responsible for their levels of control ( M = 3.77). Only insulin knowledge and blood glucose level interacted to influence internal versus external attributions, F( 1, 38) = 6.08, p < .025. As Figure 3 indicates, knowledgeable patients with the poorest blood glucose control exhibited the most internal attributions. Importantly, internality ratings were significantly related to the resentment and self-blame, r(41) = -.33, p < .05, and shame and resignation, r(41) = -.37, p < .05, components. But, reanalyses of the interactive influence of insulin knowl- edge and HbAl on RIS components, after controlling for internality ratings
DIABETES KNOWLEDGE AND REACTIONS TO ILLNESS 951
0 c,
High HbA1: Poor Control 0 Low HbA1: Good Control
0.75
0.50 1
-0.2 5
-0.50
t -0.75
- 1 .oo L Low High
Total Knowledge Figure I . Combined reactions to illness as a function of total diabetes knowledge and blood
glucose control. Values represent regression estimates for HbAl and knowledge values k .75 standard deviations from the sample means; higher numbers indicate more negative reactions to illness.
(including interactions), still resulted in a significant Insulin Knowledge X HbAl Interaction, multivariate F(3, 34) = 3.25, p < .05. Thus, attributions for current blood glucose control appear to represent an additional concom- itant of glucose control and knowledge; these attributions do not appear to mediate the impact of knowledge and control on other reactions to illness.
Discussion
As expected, knowledgeable patients had the most positive reactions to their illness if their blood glucose was well controlled, but had the most
STRUBE, YOST, AND HAIRE-JOSHU
0.50
0.25
0.00
-0.25
-0.50
-0.75
-1 .oo
High HbA1: Poor Control Low HbA1: Good Control
"0° F -
-
-
-
-
-
0.75 1
n
Low High
Insulin Knowledge Figure 2. Combined reactions to illness as a function of insulin knowledge and blood glucose
control. Values represent regression estimates for HbAl and knowledge values * .75 standard deviations from the sample means; higher numbers indicate more negative reactions to illness.
negative reactions if their blood glucose was poorly controlled. These find- ings were obtained for two of the three major dimensions of the RIS. In addition, attributions for current level of glucose control indicated that knowledgeable patients with poor blood glucose control exhibited the most internal attributions. In summary, the results indicate that increased patient knowledge is not accompanied by uniformly positive psychological re- sponses.
The attributional results are particularly interesting in light of past research on coping with aversive events. Bulman and Wortman (1977) have argued that self-blame can be adaptive provided the internal attribution is to a factor that is also controllable (e.g., effort). The adaptiveness of this behav-
DIABETES KNOWLEDGE AND REACTIONS TO ILLNESS 953
ioral self-blame stems from the belief that future instances of the aversive event can be avoided (see Timko & Janoff-Bulman, 1985). On the other hand, when the internal attribution is to an uncontrollable factor (known as characterological self-blame), harmful effects result because future instances cannot be avoided (see also Silver & Wortman, 1980; Taylor, 1983; Taylor, Lichtman, & Wood, 1984). On average, patients in our sample believed that the causes for their levels of blood glucose control were not very controll- able. When combined with the internal attributions made by high-knowl- edge, poor-control patients, the attributional pattern for this latter group resembles the characterological self-blame found to be problematic in past
High HbA1: Poor Control 0 Low HbA1: Good Control 4S
Low High
Insulin Knowledge Figure 3. Internal versus external attributions as a function of insulin knowledge and blood
glucose control. Values represent regression estimates for HbAl and knowledge values f .75 standard deviations from the sample means; higher numbers indicate more external attribu- tions.
954 STRUBE, YOST, AND HAIRE-JOSHU
research. The additional point that our findings underscore is that not all patients with poor control exhibited characterological self-blame. The mod- erating effect of knowledge indicates that it is a key component in the con- trol-related causal ascriptions made by patients with diabetes.
The study is not, however, without limitations. First, the predicted attri- butional results were obtained for only one of the knowledge subscales and attributions were not found to mediate the interactive relation of knowledge and blood glucose control on reactions to illness. This may reflect weak- nesses in the one-item internality measure or it may indicate that attributions are just another reaction to illness and not causally prior to other psycholog- ical responses. This issue will require further research. Second, only one knowledge subscale, insulin knowledge, produced a significant interaction that mimicked the total knowledge results. Several explanations seem plaus- ible. For example, some knowledge components (e.g., blood sugar) demon- strated such high rates of accuracy (i.e., 91.96%) that restricted range prob- ably obscured any relations with other measures. Also, the subscale scores necessarily are less reliable than the total knowledge score, which would also attenuate statistical relations. Alternately, it may be that insulin knowledge is a key knowledge moderator because insulin deficit and regulation is a particularly salient feature of IDDM. Future research should address further the possible distinct effects of different knowledge components, perhaps by investigating samples that provide greater ranges of scores for other compo- nents (e.g., newly diagnosed patients) or by examining patients with nonin- sulin dependent (Type 11) diabetes for whom insulin knowledge should be less important. Third, the lack of random sampling dictates caution in generalizing the results beyond the current sample. Fourth, the timing of HbAl assessment relative to measurement of illness reactions was necessarily quite variable because of the logistics of data collection. Moreover, our measure of HbAl is assumed to stand for both the patients’ level of control and their recognition of their level of control. This latter assumption seems reasonable given the patients’ required daily monitoring of their blood glu- cose regulation. Nonetheless, a more detailed and direct examination of the inferences that patients draw from information about blood glucose control would provide additional insight into the processes that underlie illness reac- tions. Finally, the single measurement period and nonexperimental design make causal inferences risky. Accordingly, longitudinal research will be a necessary next step in which metabolic control, knowledge development, and psychological responses are tracked from disease onset. Experimental manipulation of the knowledge component (when ethically and logistically feasible) will further help establish the causal role of this variable.
With these limitations in mind, it is useful to consider the implications of the present findings. As noted previously, past research has not found a

DIABETES KNOWLEDGE AND REACTIONS TO ILLNESS 955
consistent relation between knowledge and adherence. This may stem from the different short-term and long-term effects of knowledge on the physical and psychological functioning of the patient. It may be that beyond some minimum level attained by most patients, additional knowledge may have little impact on daily physical functioning. Indeed, despite the best efforts of the patient armed with the best information available, it is difficult to achieve consistently the metabolic balance found in normal individuals. Therefore, although high levels of knowledge may have beneficial long-term physical effects, the short-term physical benefits may be small. On the other hand, the short-term psychological effects of knowledge may be substantial and may have physical consequences. As the present results suggest, when blood glucose is poorly controlled, higher knowledge may be accompanied by self-blame and negative illness reactions. The resulting stress could itself disrupt metabolic control (cf. Gonder-Frederick, Carter, Cox, & Clarke, 1990; Goodall & Halford, 1991; Halford, Cuddihy, & Mortimer, 1990), either by directly increasing stress hormone levels or by indirectly altering self-management behaviors (Halford et al., 1990). These possibilities will require future attention.
Despite the potentially negative effects of higher knowledge, it would be misguided to conclude from our results that patient education is wasted effort beyond some minimal self-care requirements. Greater knowledge may, in fact, have long-term benefits. But, as the present research suggests, patient education may also need to emphasize a more realistic appraisal of short-term metabolic control. If patients recognize that metabolic balance is highly variable and will fluctuate despite their best efforts, then increased knowledge need not produce negative effects when control is poor. Thus, an expanded view of patient functioning, emphasizing more than just blood glucose level, appears appropriate (cf. Goodall & Halford, 1991). This necessarily involves an emphasis on broad-based patient education that includes information about common reactions to illness and their origin. In addition, given the attributional processes that accompany illness reactions, patient education programs might profitably explore attributional retraining (e.g., Forsterling, 1985) as a potential means of reducing the nega- tive effects of knowledge. Indeed, it is not so much the knowledge, but how that knowledge is used, that appears to produce the deleterious effects re- ported here.
References
Bulman, R., & Wortman, C . B. (1977). Attributions of blame and coping in the “real world”: Severe accident victims react to their lot. Journal of Personality and Social Psychology, 35, 35 1-363.
956 STRUBE, YOST, AND HAIRE-JOSHU
Cliff, N. (1988). The eigenvalues-greater-than-one rule and the reliability of components. Psychological Bulletin, 103, 276-279.
Cohen, J., & Cohen, P. (1975). Applied multiple regressionJcorrelation analysis f o r the behavioral sciences. Hillsdale, NJ: Erlbaum.
Cox, D. J., Gonder-Frederick, L., Pohl, S., & Pennebaker, J . W. (1986). Diabetes. In K. A. Holroyd & T. L. Creer (Eds.), Self-management of chronic diseases (pp. 305-346). Orlando, FL: Academic Press.
Derogatis, L. R. (1977). Psychological Adjustment to Illness Scale: Self- report version. Baltimore: Clinical Psychometric Research.
Derogatis, L. R. (1983). Psychological Adjustment to Illness Scale (PAIS & PAIS-SR): Scoring procedures and administration manual. Baltimore: Clinical Psychometric Research.
de Weerdt, I., Visser, A. P., Kok, G., & Van der Veen, E. A. (1990). Deter- minants of active self-care behaviour of insulin treated patients with dia- betes: Implications for diabetes education. Social Science and Medicine,
de Weerdt, I., Visser, A. P., & Van der Veen, E. A. (1989). Attitude behavior theories and diabetic education programmes. Patient Education and Counseling, 14, 3-19.
Fisher, E. B., Delamater, A. M., Bertelson, A. D., & Kirkley, B. G. (1982). Psychological factors in diabetes and its treatment. Journal of Consulting and Clinical Psychology, 50,993- 1003.
Fiske, S. T., & Taylor, S. E. (1991). Social cognition (2nd ed.). New York: McGraw-Hill.
Forsterling, F. (1985). Attributional retraining: A review. Psychological Bul- letin, 98, 495-512.
Frieze, I. (1976). Causal attributions and information seeking to explain success and failure. Journal of Research in Personality, 10, 293-305.
Glasgow, R. E., Toobert, D. J., Riddle, M., Donnelly, J., Mitchell, D. L., & Calder, D. ( 1989). Diabetes-specific social learning variables and self-care behaviors among persons with Type I1 diabetes. Health Psychology, 8,
Gonder-Frederick, L. A., Carter, W. R., Cox, D. J., & Clarke, W. L. (1990). Environmental stress and blood glucose change in insulin-dependent dia- betes mellitus. Health Psychology, 9, 503-5 15.
Goodall, T. A., & Halford, W. K. (1991). Self-management of diabetes mellitus: A critical review. Health Psychology, 10, 1-8.
Halford, W. K., Cuddihy, S., & Mortimer, R. H. (1990). Psychological stress and blood glucose regulation in Type I diabetic patients. Health Psychol-
Hampson, S. E., Glasgow, R. E., & Toobert, D. J. (1990). Personal models
30,605-615.
285-303.
ogy, 9,516-528.
DIABETES KNOWLEDGE AND REACTIONS TO ILLNESS 957
of diabetes and their relations to self-care activities. Health Psychology, 9,
Hess, G. E., & Davis, W. K. (1983). The validation of a diabetes patient knowledge test. Diabetes Care, 6, 591-596.
Jenkins, C. D., Zyzanski, S. J., & Rosenman, R. H. (1979). The Jenkins Activity Survey, Form C. New York: Psychological Corporation.
Johnson, S. B., Freund, A., Silverstein, J., Hansen, C. A., & Malone, J. (1990). Adherence-health status relationships in childhood diabetes. Health Psychology, 9, 606-63 1.
Karam, J . H. (1981). Diabetes mellitus, hypoglycemia and lipoprotein dis- orders. In M. A. Krepp & M. J . Chatton (Eds.), Current medical diag- nosis and treatment (pp. 735-762). Los Angeles: Lange.
Kennedy, A. L., & Merimec, P. J. (1981). Glycosylated serum protein and hemoglobin A1 levels to measure control of glycemia. Annals of Internal Medicine, 95, 56-58.
Krantz, D. S., Baum, A., & Wideman, M. V. (1980). Assessment of prefer- ences for self-treatment and information in health care. Journal of Per- sonality and Social Psychology, 39,977-990.
Ludvigsson, J . (1977). Socio-psychological factors and metabolic control in juvenile diabetes. Acta Paediatrica Scandinavica, 66, 43 1-437.
McCaul, K. D., Glasgow, R. E., & Schafer, L. C. (1987). Diabetes regimen behaviors: Predicting adherence. Medical Care, 25, 868-88 1.
Miller, S. M. (1987). Monitoring and blunting: Validation of a questionnaire to assess styles of information seeking under threat. Journal of Personal- ity and Social Psychology, 52, 345-353.
Peterson, C., Semmel, A., von Baeyer, C., Abramson, L. Y., Metalsky, G. I., & Seligman, M. E. P. (1982). The attributional style questionnaire. Cog- nitive Therapy and Research, 6,287-299.
Pritchard, M. (1973). Reaction to illness in long term haemodialysis. Journal of Psychosomatic Research, 18, 55-67.
Rhodewalt, F., & Marcroft, M. (1988). Type A behavior and diabetic con- trol: Implications of psychological reactance for health outcomes. Jour- nal of Applied Social Psychology, 18, 139- 159.
Rhodewalt, F., & Strube, M. J . (1985). A self-attribution-reactance model of recovery from injury in Type A individuals. Journal of Applied Social
Silver, R. L., & Wortman, C. B. (1980). Coping with undesirable life events. In J. Garber & M. E. P. Seligman (Eds.), Human helplessness: Theory and applications (pp. 279-340). New York: Academic Press.
Strube, M. J., Haire-Joshu, D., & Yost, J. H. (1987, June). Style of cognitive response to stressful situations as a moderator of bloodglucose control in
63 2-646.
Psychology, 15, 330-344.
958 STRUBE, YOST, AND HAIRE-JOSHU
Type I diabetic palients. Presented at the 47th annual meeting of the American Diabetes Association, Indianapolis, IN.
Strube, M. J., Yost, J . H., & Haire-Joshu, D. (1987, August). Health care attitudes and reactions to a chronic illness. Presented at the 95th annual meeting of the American Psychological Association, New York.
Surwit, R. S., Feinglos, M. N., & Scovern, A. W. (1983). Diabetes and behavior: A paradigm for health psychology. American Psychologist, 38,
Taylor, S . E. (1983). Adjustment to threatening events: A theory of cognitive adaptation. American Psychologist, 38, 1161-1 173.
Taylor, S. E., Lichtman, R. R., & Wood, J . V. (1984). Attributions, beliefs about control, and adjustment to breast cancer. Journal of Personality and Social Psychology, 46,489-502.
Timko, C., & Janoff-Bulman, R. (1985). Attributions, vulnerability, and psychological adjustments: The case of breast cancer. Health Psychology,
Watkins, J . D., Roberts, D. E., Williams, T. F., Martin, D. A., & Coyle, V. (1967). Observation of medication errors made by diabetes patients in the home. Diabetes, 16, 882-885.
Watkins, J. D., Williams, T. F., Martin, D. A., Hogan, M. D., & Anderson, E. (1967). A study of diabetic patients a t home. American Journal of Public Health, 37,452-459.
Wilkinson, G . (1987). The influence of psychiatric, psychological and social factors on the control of insulin-dependent diabetes mellitus. Journal of Psychosomatic Research, 31,277-286.
Williams, T. F., Anderson, E., Watkins, J. D., & Coyle, V. (1967). Dietary errors made at home by patients with diabetes. Journal of the American Dietetic Association, 51, 19-25.
Wing, R. R., Epstein, L. H., Nowalk, M. P., & Lamparski, D. M. (1986). Behavioral self-regulation in the treatment of patients with diabetes melli- tus. Psychological Bulletin, 99, 78-89.
Wong, P. T. P., & Weiner, B. (198 1). When people ask “why” questions, and the heuristics of attributional search. Journal of Personality and Social Psychology, 40,650-663.
Ziel, R. H., & Davidson, M. B. (1987). The role of glycosylated serum albumin in monitoring glycemic control in stable insulin-requiring dia- betic outpatients. Journal of Clinical Endocrinology and Metabolism, 64,
255-262.
4, 521-544.
269-273.