Embed Size (px)
Citation preview

Patient Education and Counseling 88 (2012) 44–53
Review
Diabetes self-management in patients with low health literacy: Ordering findingsfrom literature in a health literacy framework
Mirjam P. Fransen a,*, Christian von Wagner b, Marie-Louise Essink-Bot a
a Department of Public Health, Amsterdam Medical Centre, University of Amsterdam, Amsterdam, The Netherlandsb Health Behaviour Research Centre, University College London, London, UK
A R T I C L E I N F O
Article history:
Received 8 July 2011
Received in revised form 2 November 2011
Accepted 30 November 2011
Keywords:
Literature review
Health literacy
Diabetes self-management
Sociocognitive determinants
Theoretical framework
A B S T R A C T
Objective: To review studies on the association between health literacy (HL), diabetes self-management
and possible mediating variables.
Methods: We systematically searched for empirical studies in PubMed. Findings were ordered by a HL
framework that outlines routes between HL, sociocognitive determinants and health actions.
Results: Of the 11 relevant studies, three reported a significant positive association between HL and
specific diabetes self-management domains. Ten studies investigated the association between HL and
knowledge (n = 8), beliefs (n = 2), self-efficacy (n = 3) and/or social support (n = 1). Significant
associations were found between HL and knowledge (n = 6), self-efficacy (n = 1) and social support
(n = 1). Of the three studies evaluating the effect of these sociocognitive variables on diabetes self-
management, only one found proof for a mediating variable (social support) in the pathway between HL
and self-management.
Conclusion: There is only limited evidence for a significant association between HL and diabetes self-
management, and for the mediating role of sociocognitive variables in this pathway.
Practice implications: Longitudinal studies, including HL, diabetes self-management and potential
mediators, are needed to substantiate possible associations between these variables. Such research is
essential to enable evidence-based development of interventions to increase adequate and sustainable
self-management in diabetic patients with low HL.
� 2011 Elsevier Ireland Ltd. All rights reserved.
Contents lists available at SciVerse ScienceDirect
Patient Education and Counseling
jo ur n al h o mep ag e: w ww .e lsev ier . co m / loc ate /p ated u co u
1. Introduction
1.1. Diabetes self-management
Self-management has become increasingly important in thetreatment of diabetes mellitus type 2 (DM2). Patients with DM2have become partners in the treatment of their own disease andself-management is crucial to obtain adequate glycaemic control.There is no universally accepted definition of self-management.Barlow et al. defined general self-management as the patient’sability to manage the symptoms, treatment, physical andpsychosocial consequences and lifestyle changes inherent in livingwith a chronic disease [1]. Diabetes self-management is generallydivided into four domains: nutritional management; exercise andphysical activity; blood glucose monitoring; and medicationutilization [2–4]. The American Association of Diabetes Educators
* Corresponding author at: Department of Public Health K2-204, Academic
Medical Centre, University of Amsterdam, PO-Box 22660, 1100 DD Amsterdam, The
Netherlands. Tel.: +31 20 5667443; fax: +31 20 6972316.
E-mail address: [email protected] (M.P. Fransen).
0738-3991/$ – see front matter � 2011 Elsevier Ireland Ltd. All rights reserved.
doi:10.1016/j.pec.2011.11.015
(ADEE) operationalized nutritional management into makinghealthy food choices, understanding portion sizes and learningthe best times to eat. Regular activity is important for overallfitness, weight management and blood glucose control. Togetherwith healthcare professionals, patients should address barriers toregular physical activity and develop an appropriate plan tobalance food and medication with the activity level. The AADE alsonote that daily self-monitoring of blood glucose provides patientswith diabetes the information they need to assess how food,physical activity and medications affect their blood glucose levels.To adequately utilize medications, patients should be knowledge-able about each medication, including its action, side effects,efficacy, toxicity, prescribed dosage, appropriate timing, frequencyof administration, effect of missed/delayed doses and instructionsfor storage, travel and safety [5].
1.2. Health literacy
To implement optimal diabetes self-management, patientsmust apply specific knowledge and decision-making skills acrossthe multiple domains of self-management. This requires adequate

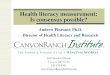
Fig. 1. Framework of health literacy and health actions.
M.P. Fransen et al. / Patient Education and Counseling 88 (2012) 44–53 45
health literacy (HL). The Institute of Medicine (IOM) defined HL asthe degree to which individuals have the capacity to obtain,process, and understand basic health information and servicesneeded to make appropriate health decisions [6]. Subjects with lowHL tend to be less likely to successfully manage chronic diseases[7,8]. They generally have less knowledge about their disease,exhibit inadequate self-management and have poor health out-comes [9–14].
1.3. Framework for health literacy and health actions
In 2007 Paasche-Orlow and Wolf developed a framework thatoutlined routes through which HL might affect health actions inthe access and utilization of health care, patient–providerinteractions and self-management [15]. Drawing upon these ideas,von Wagner et al. developed a framework for health literacy andhealth actions that was derived from health psychology (Fig. 1)[16]. This framework was developed to guide research on theprocesses through which HL affects health outcomes. Theframework proposes that health actions (access and use of healthcare, patient–provider interactions, and the management of healthand illness, e.g. diabetes self-management) determine healthoutcomes (e.g. HbA1c level) through sociocognitive motivationaland volitional determinants. Motivational determinants includetraditional social cognition constructs (e.g. beliefs and attitudes)which in turn are associated with access to health information andknowledge. For example, adequate knowledge in diabetes self-management consists of knowing the effect of food on bloodglucose. Volitional determinants on the other hand refer toobjective and subjective (e.g. self-efficacy) action control andinclude task-specific skills, such as information processing andnavigational skills to acquire specific knowledge about adherenceregimens, and cognitive skills (e.g. anticipate on glucose levels).The motivational and volitional determinants are not affected bylevels of HL alone, but form a symbiotic relationship with externalsystem factors. For example accessibility of health care informa-tion, communication skills of the health care provider, and out-of-pocket costs for health care. The motivational determinant
‘patient’s understanding of a healthy diet’ also depends on howwell the healthcare provider is able to explain what the patientshould or should not eat to maintain a healthy diet [16].
1.4. Aim
The aim of this paper is to review the literature on theassociation between HL and diabetes self-management, and thepossible mediating variables in this pathway. A secondary aim is toorder the findings in the framework proposed by von Wagner et al.In the Section 2 we explain why we chose this framework to orderour literature findings and describe the methods for our literaturereview. The findings of our literature review are schematicallyreported in the Section 3. The paper ends with a discussion of thefindings and implications for further research.
2. Methods
2.1. Literature review
In July 2011, we searched for articles on HL, diabetes, diabetesself-management and its four domains (nutritional management;exercise and physical activity; blood glucose monitoring; andmedication utilization). Relevant search terms were derived fromliterature on HL and diabetes self-management [9–14]. We usedthe following keywords and Medical Subject Headings (MeSH) tosearch in PubMed:
[Health literacy or literacy or numeracy] and [diabetes] and[self-management or self-monitor or medication adherence or dietor food or exercise or sports].
Except for ‘numeracy’ and ‘self-monitor’, all terms were MeSHterms. This means that PubMed automatically searched for paperswith equivalents of these terms. Additional articles were identifiedby reviewing the reference lists of the retrieved articles.
Inclusion criteria were:� Empirical studies among patients with DM2.� Reporting on the association between HL and diabetes self-
management tasks.

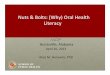
Fig. 2. Flow diagram literature search.
M.P. Fransen et al. / Patient Education and Counseling 88 (2012) 44–5346
� Published in the English language.
Exclusion criteria were:� Papers reporting on patients with comorbidity.� Reviews and case reports.� Not published as a scientific paper (e.g. abstracts or theses).
The initial search yielded 139 papers, published between 1988and June 2011. A flow diagram of the review process is presented inFig. 2. After one reviewer (MF) screened titles and abstracts on
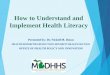
Fig. 3. Findings of literature review
relevance, this number was reduced to 32 publications. The 32abstracts were then critically reviewed by MLE, resulting in 26 fullpapers. Most excluded papers did not report on the associationbetween HL and performance of diabetes self-management tasks.Consensus was reached between MF and MLE-B by reading anddiscussing the content of 26 full-text papers. All reviews stageswere based on the same in- and exclusion criteria. Papers wererated as sufficient when MF and MLE both decided that allinclusion criteria were clearly met and exclusion criteria were notapplicable. This accounted for 10 papers. Papers were rateddoubtful when there was no consensus on sufficiency for inclusion,e.g. when papers met part of the inclusion criteria. This accountedfor 16 papers, most of these concerned intervention developmentstudies where the association between HL and self-managementwas partly studied. These doubtful papers (n = 16) were exten-sively discussed by MF and MLE, resulting in the exclusion of 15papers, leaving 11 papers for the literature study.
For each paper we reported how HL and self-management wasdefined and measured, which determinants in the pathway betweenHL and self-management were studied, and the most relevantresults. The methodological quality of the papers was based onguidelines for cohort studies as defined by the Cochrane Collabora-tion [17]. We assessed whether the characteristics of the studypopulation and the outcome measures were well defined, the appliedmeasurement tools were valid, confounders were corrected for in theanalysis and whether the results were valid and applicable. Theresults of the review were discussed in light of the HL framework.
2.2. Order findings in framework
The literature findings were ordered in von Wagner’s frame-work for HL and health actions. This framework enables theordering of variables in the pathway between HL and diabetes self-management and places HL in the context of sociocognitive
in health literacy framework.

Table 1Papers reporting on empirical studies on health literacy and diabetes self-management (n = 11).
Author, year Aim Design Population Relevant measurements Analyses Results
Bains and Egede,
2011 [18]
Assess associations
among HL, diabetes
knowledge,
self-management
and glycemic control.
Cross-
sectional
survey
Patients with DM2 in
primary care clinic
in the US (n = 125)
HL: REALM-R Spearman’s correlation
and multiple regression
analysis
HL was significantly associated with knowledge
(b= 0.55; CI 0.29, 0.82).
65+ years: 49%
Mediating variables:
Knowledge was significantly associated with
glycemic control (b = 0.12; CI 0.01–0.23).Female: 72.5%
- Knowledge (DKQ)
HL was not significantly associated with SM or HbA1c.
SM: SDSCA
Other: HbA1cl;
medication adherence
Cavanaugh
et al., 2008 [19]
Examine association
between numeracy
and diabetes control.
Cross-
sectional
survey
Patients with DM1 or
DM2 in primary care
and diabetes clinics
in the US (n = 398)
HL: DNT Cuzick nonparametric
test for trend
Lower DNT scores were associated with:
Median age: 55
Mediating variables:
- Lower median DKT (52% vs 86%, p<0.001)
Female: 51%
- Knowledge (DKT)
- Lower self-efficacy of SM (9% vs 12%, p = 0.003)
Type 2 diabetes: 86%
- Self-efficacy (self-report)
- Adjustment of insulin dose
(38% vs 75%, p<0.001)
Duration diabetes:
9 years
SM: SDSCA
- Adjustment of carbohydrate
intake (12% vs 72%, p<0.001).
Other: Diabetes
control (HbA1C)
Participation in dietary, physical
activity or medication behaviours were not
significantly associated with DNT scores.
DTN was modestly associated with HbA1c
level. A 10-percentage point decrease of
correct DNT responses predicted an increase
of HbA1c of 0.09% (95% CI 0.01–0.16, p = 0.03).
Hawthorne and
Tomlinson,
1999 [20]
Study factors affecting
diabetes control and SM.
Cross-
sectional
survey
British Pakistani patients
with DM2 (n = 201)
HL: Subjective literacy,
no measure reported
x2 test Illiterate patients had less knowledge on:
Mean age: 54 Mediating variables: - Handling raised glucose levels (9% vs 30%, p<0.01)
Female: n = 107 - Knowledge food values - Chiropodist (4% vs 17%, p = 0.01)
- Knowledge SM - Diabetes complications (19% vs
47%; 19% vs 39%, p<0.01; 13% vs 16%, p>0.05).
- Knowledge complications HL was not significantly associated with knowledge
of food values, glucose self-monitoring and HbA1c.SM: Glucose self-
monitoring
(self-reported)
Other: Diabetes
control (HbA1C)
Karter,
et al.,
2010 [21]
Investigate barriers to
insulin initiation following
a new prescription.
Cross-
sectional
survey
Insulin-naive patients with
poorly controlled type 2
diabetes in the USA (n = 169)
HL: SBSQ Not reported Compared to adherent patients,
non-adherent patients more often
reported low HL (30% vs 51%, p<0.05).
Mediating variables:
Non adherent patients:
- Provider communication
Mean age: 61
- SM training
Female: 35%
SM: Adherence of insulin
treatment (dispense of the
newly prescribed insulin
within 60 days of the
prescribing date)
Adherent patients:
Mean age: 58
Female: 47%
M.P
. Fra
nsen
et a
l. /
Pa
tient
Ed
uca
tion
an
d C
ou
nselin
g 8
8 (2
01
2)
44
–5
3
47

Table 1 (Continued )
Author, year Aim Design Population Relevant measurements Analyses Results
Kim
et al.,
2004 [22]
Examine the association
between HL and SM and
determine the effect of
diabetes education on
SM in patients with
limited and adequate HL.
Prospective
observational
study
DM1/2 patients enrolled
in diabetes education
classes at the Hospital of
the University of
Pennsylvania, USA (n = 92)
HL: s-TOFHLA Paired t-tests At baseline, patients with adequate HL had better
mean knowledge than patients with limited HL
(17.2 vs 13.9, p = 0.014). Health literacy was not
significantly associated with SM or HbA1c-levels.
Adequate HL patients:
Mediating variable:
After diabetes education, those with adequate
HL had higher knowledge scores (19.9 vs 18.0, p<0.00)
and exercised more (2.8 vs 2.1, p = 0.02). But patients
with lower HL reported better adherence to diet
(6.0 vs 5.2, p<0.00), self-glucose monitoring (6.6
vs 5.4, p = 0.002), and foot care (5.1 vs 5.0, p = 0.001).
Mean age: 58
- Diabetes knowledge (DKQ)
Female: 59%
SM: SDSCA
Duration diabetes: 7.8
Other: HbA1c
Limited HL patients:
Mean age: 67
Female: 81%
Duration diabetes: 9.3
Mancuso,
2010 [23]
Examine the impact
of HL on glycemic control.
Cross-
sectional
survey
Patients with DM1/2 in two
primary care clinics in the
USA (n = 102)
HL: TOFHLA Multiple regression
analysis and correlation
coefficients
A significant positive correlation was found between
HL and diabetes knowledge (rho 0.296, p<0.01).
Mean age: 52
Mediating variable:
HL was not significantly correlated with SM or HbA1C.
Female: 61%
- Knowledge of
diabetes (DKT)
Duration diabetes: 5.8 SM: SDSCA
Other: Glycemic control
(HbA1C); patient trust
(HCR Trust Scale);
Depression (CES-D)
Mbaezue
et al.,
2010 [24]
Examine the relationship
between HL and
self-monitoring
of blood glucose.
Cross-
sectional
survey
Diabetic patients
receiving care in a large
urban public health care
setting in the USA (n = 189)
HL: TOFHLA x2 tests and
multivariate logistic
regression analysis
There was no difference in SBMG among patients by
HL level. However, those with adequate HL more
often kept a record of their glucose levels than patients
with inadequate HL (64.6% vs 35.4%, p = 0.049). In
multivariate logistic modelling, no significant
association was found between HL and SBMG.
Mean age: 51
SM: SBMG
Female: 59%
Duration diabetes: 8.5
Osborn
et al.,
2010 [25]
Examine the relationship
between HL, determinants
of SM and glycemic control.
Cross-
sectional
study
Patients with DM2
at a university
hospital (n = 130)
HL: REALM-R Structural equation
modelling
HL did not have a direct effect on diabetes
knowledge, fatalism, SM or glycemic control.
Mean age: 62.7
Mediating variables:
More knowledge (r = 0.22, p<0.05), less fatalism
(r =�0.22, p<0.05, and more social support (r =�0.27),
p<0.01) were independent, direct predictors of
self-management and through self-management
related to glycemic control (r =�0.20, p<0.05).
Female: 72.5%
- Diabetes knowledge
(DKQ)
HL had a direct effect on social support (r = 0.02, p<0.01)
and through social support an indirect effect on SM
(r =�0.07) and an indirect effect on glycemic control
(r =�0.01).
- Diabetes fatalism
- Social support (MOS
Social Support Survey)SM: SDSCA
Other: Glycemic control
(HbA1C)
M.P
. Fra
nsen
et a
l. /
Pa
tient
Ed
uca
tion
an
d C
ou
nselin
g 8
8 (2
01
2)
44
–5
34
8

Powell
et al.,
2007 [26]
Sarkar
et al.,
2006 [27]
Explore the relationship
among HL, readiness to
take health actions
and diabetes knowledge.
Examine the relationship
between diabetes self-
efficacy and SM in a
population with
a high prevalence
of low HL.
Cross-
sectional
study
Cross-
sectional
study
Patients with DM2 receiving
care at a general internal
medicine clinic in the USA (n = 68)
HL: REALM Multiple linear
regression
analysis
Multivariate
regression
analyses
HL was associated with diabetes knowledge and
hbA1C. Those with low HL had lower DKT scores
(estimated coefficients �13.2; �18.5; �12.9 p = 0.004)
and higher hbA1C levels (estimated coefficients
1.36; 1.21; 1.24 p = 0.02).
Median age: 55
Mediating variable:
No significant association was found between DHBM
scale score and HL levels.
Female: 80%
- Diabetes knowledge (DKT)
Duration diabetes: 7
SM: Diabetes Health
Beliefs (DHBM)Other: HbA1C
Patients with DM2 at two
primary care clinics at a
public hospital in the
USA (n = 408)
HL: s-TOFHLA
Self-efficacy was associated with SM across health
literacy levels (OR 1.14; CI 1.04–1.33).Mean age: 58.1
Mediating variable:
No significant interactions were found between
self-efficacy and HL on the SM outcomes.
Duration diabetes: 9.5
- Diabetes self-efficacy
SM: SDSCA
Wallace
et al.,
2009 [28]
Evaluate the impact of a
literacy-appropriate diabetes
education guide on diabetes
SM among patients with
adequate and inadequate HL.
Intervention
study
English and Spanish speaking
DM2 patients in academic
internal medicine practices
in the USA (n = 250)
HL: s-TOFHLA Independent
t-tests
At baseline, patients with marginal or inadequate HL
scored higher on mean diabetes self-management
activities (manage medications, monitor blood
glucose, maintain a diet, exercise and conduct foot
care) than patients with
adequate HL (76.71 vs 73.52).
Mean age:56
Other:
Female: 64.8%
- Patient activation (PAM)
At baseline, patients with marginal or inadequate HL
scored lower on mean self-efficacy than patients with
adequate HL (73.13 vs 74.02).
- Self-efficacy
- Diabetes knowledge
At baseline, patients with marginal or inadequate
HL scored lower on knowledge than patients with
adequate HL (51.77 vs 60.83).
SM: Subjective scale for
diabetes self-management
activities
DM = Diabetes mellitus. HL = health literacy. DNT = diabetes numeracy test. SM = self-management. SCSCA = summary of diabetes self care activities scale. SBSQ = set of brief screening questions. REALM = rapid estimate of adult
literacy in medicine. TOFHLA = test of functional health literacy in adults. DKQ = diabetes knowledge questionnaire. SBMG = self-monitoring of blood glucose. DKT = diabetes knowledge test. HCR Trust Scale = Health Care Relationship
Trust Scale. CES-D = Centre for Epidemiological Studies Depression Scale. MOS = medical outcomes study. DHBM = Diabetes Health Belief Model Scale. PAM = patient activation measure.
M.P
. Fra
nsen
et a
l. /
Pa
tient
Ed
uca
tion
an
d C
ou
nselin
g 8
8 (2
01
2)
44
–5
3
49

Table 2Quality of the selected papers on health literacy and diabetes self-management (n = 11).
Author, year Study population
description
Outcome
measures
description
Valid
measurements
Description of
analysis
Correction for
confounders
Validity and
applicability of results
Bains and Egede, 2011 + + + + + +
Cavanaugh et al., 2008 + + + + � +
Hawthorne and Tomlinson, 1999 + � � + � +/-
Karter et al., 2010 + + + � � �Kim et al., 2004 + + + + � +
Mbaezue et al., 2010 + + + + + +
Mancuso et al., 2010 + + + + + +
Osborn et al., 2010 + + + + + +
Powell et al., 2007 + + + + + +
Sarkar et al., 2006 + + + + + +
Wallace et al., 2009 + + + + � �
+: sufficient; �: insufficient; �: doubtful.
M.P. Fransen et al. / Patient Education and Counseling 88 (2012) 44–5350
theories of health behaviour. To design specific evidence-basedinterventions to promote adequate self-management amongdiabetic patients with low HL, we need more information onhow sociocognitive and psychological variables influence self-management in patients with low HL. Von Wagner’s frameworkprovides a suitable theoretical basis for further research andintervention development.
3. Results
In this section we first summarize the content and methodo-logical quality of the papers that were included in our review(Section 3.1). We then describe findings on the associationbetween HL and diabetes self-management (Section 3.2). Weend with findings on possible mediating variables in theassociation between health literacy and self-management, dividedinto motivational and volitional determinants (Section 3.3). Fig. 3presents a schematic ordering of the findings in von Wagner’sframework.
3.1. Included papers and methodological quality
Table 1 presents the design and main findings of the papers thatwere included in the review. Ten studies were performed in theUSA, and one in the UK [18–28]. Nine studies were cross-sectional[18–21,23–27]. Two were prospective observational studies toevaluate the effect of diabetes education [22,28]. Table 2summarizes the methodological quality of each paper. Thecross-sectional design that most studies applied limits interpreta-tion of the causality between HL, determinants and self-manage-ment [18–21,23–27]. Because the beneficial effect of self-management on sociocognitive determinants (e.g. knowledge
Table 3Reported associations between health literacy and diabetes self-management activities
Author, year HL-Measure Domain of dia
Nutrition
Bains, 2011 REALM-R 0
Cavanaugh, 2008 DNT +
Hawthorne and Tomlinson, 1999 REALM *
Karter et al., 2010 SBSQ *
Kim et al., 2004 s-TOFHLA 0
Mancuso, 2010 TOFHLA 0
Mbaezue et al., 2010 TOFHLA *
Osborn et al., 2010 REALM-R 0
Sarkar et al., 2006 s-TOFHLA 0
Wallace et al., 2009 s-TOFHLA ?
+: significant positive association; 0: no significant association; ?: no statistical signifi
and self-efficacy) over time is feasible, there could be a reciprocalrelationship that can only be evaluated in prospective cohortstudies. Three studies had problems with statistical power[22,23,26]. Most studies applied valid measures to assess HL,self-management and other variables. However, it must be notedthat in all 11 studies self-management assessment was based onself-report alone and that the applied HL measures only evaluatedfunctional HL and not the broader concept of HL as defined by theIOM.
3.2. Health literacy and self-management
Three studies found a significant direct positive associationbetween HL and self-management activities (Table 3) [19,24].Mbaezue et al. reported that patients with adequate HL more oftenkept a record of their glucose levels than patients with inadequateHL (64.6% vs. 35.4%, p = 0.049). However, no significant associationwas found between HL and the frequency of self-monitoring ofblood glucose [24]. Karter et al. found that significantly more non-adherent patients in insulin treatment reported low HL comparedto adherent patients (51% vs. 30%, p < 0.05) [21]. Cavanaugh et al.found that higher diabetes-related numeracy among patientsreporting insulin use was associated with the adjustment of insulindose for blood glucose level (38% among lowest HL vs. 75% amonghighest HL, p < 0.001) and carbohydrate intake (12% among lowestHL vs. 75% among highest HL) [19]. Eight studies found no directsignificant association between HL and diabetes self-management(Table 3) [18,20,22,23,25–28]. Five of them found that HL was notsignificantly associated with self-care activities as measured by theSummary of Diabetes Self-Care Activities scale (SDSCA)[18,22,23,25,27]. This scale measures self-reported frequency ofdiabetes self-management in the past 7 days for five aspects of the
(n = 11).
betes self-management
Physical activity Glucose monitoring Medication
0 0 0
0 0 +
* 0 *
* * +
0 0 0
0 0 0
* + *
0 0 0
0 0 0
? ? ?
cance reported; *: no association measured.

M.P. Fransen et al. / Patient Education and Counseling 88 (2012) 44–53 51
diabetes regimen: diet, foot care, blood-glucose testing, exerciseand cigarette smoking [3].
In addition to the relation between HL and diabetes self-management, seven studies investigated the relationship betweenHL and HbA1c-level [18,19,22,23,25,26]. Two of them reportedsignificant associations [19,26].
3.3. Possible mediating variables in health literacy and
self-management
Eight studies reported on variables that could be ordered in themotivational determinants (knowledge, beliefs and attitudes) invon Wagner’s framework [18–20,22,23,25,26,28]. Von Wagneremphasized that motivation alone is not enough to perform self-management. Concepts such as self-efficacy (volitional determi-nants) and practical barriers (system factors) influence thetranslation of intentions into action. Three studies reported onHL, self-efficacy and diabetes self-management [19,27,28]. Onestudy reported on HL, social support and self-management [25].We found no studies on the influence of system factors in thepathway between HL and diabetes self-management. Below wedescribe the studies that report on motivational and volitionaldeterminants in the pathway between HL and diabetes self-management.
3.3.1. Motivational determinants
3.3.1.1. Knowledge. Eight studies investigated the associationbetween HL and diabetes knowledge [18–20,22,23,25,26,28]. Sixof them reported a significant positive correlation between HL anddiabetes knowledge [18–20,22,23,26]. However, none of theseactually demonstrated that inadequate knowledge in patients withlow HL influenced their diabetes self-management. Osborn et al.found that diabetes knowledge was positively associated with self-management, but did not find a direct relationship between HL anddiabetes knowledge [25].
3.3.1.2. Beliefs and attitudes. In von Wagner’s framework beliefsand attitudes are considered an important mediating factor in thepathway between HL and self-management. Two studies investi-gated the association between HL and patient beliefs in relation todiabetes self-management [25,26]. Powel et al. found that HL wasnot associated with scores on the Diabetes Health Belief Model(after controlling for educational level, age, DKT score, race) [26].Osborn et al. measured the relation between HL, diabetes fatalismand self-management. Diabetes fatalism is defined as a complexpsychological cycle characterized by perceptions of despair,hopelessness, and powerlessness. They reported that diabetesfatalism had a direct effect on diabetes self-management, but thatHL did not have a direct effect on diabetes fatalism [25]. None ofthe studies assessed the relation between knowledge and beliefs,as proposed in von Wagner’s model.
3.3.2. Volitional determinants
3.3.2.1. Self-efficacy. Three studies investigated the associationbetween HL and self-efficacy [19,27,28]. Cavanaugh et al. de-scribed that patients with higher diabetes-related numeracy weremore likely to have a greater perceived self-efficacy compared withlow numeracy patients [19]. Wallace et al. found that patients withmarginal or inadequate HL scored lower on mean self-efficacy thanpatients with adequate HL at baseline (73.13 vs. 74.02), however,they did not report any significance levels of this difference [28].Only one study investigated the role of self-efficacy in thepathway between HL and diabetes self-management [27]. Theyfound an association between increasing self-efficacy score and
self-management with regard to diet, exercise, self-monitoringand foot care across HL levels, but no significant interactionsbetween self-efficacy and HL [27].
3.3.2.2. Social support. Osborn et al. found that low HL had a directnegative effect on social support (r = �0.2, p < 0.05) and, throughsocial support, had an indirect negative effect on diabetes self-management and glycaemic control [25]. Although social supportwas not implemented in von Wagner’s model, it can be consideredas a post-intentional variable. Therefore, we added it to the modelin the volitional phase.
4. Discussion and conclusion
Below we discuss the main findings in this literature review anddescribe various gaps in research on HL and diabetes self-management. The discussion ends with a reflection on strengthsand weaknesses of this study. The discussion is followed by ageneral conclusion and implications for further research.
4.1. Discussion
4.1.1. Discussion of main findings
The results of this literature review show that evidence for theassociation between HL and diabetes self-management is verylimited and may vary within the domains of self-management. Onlythree studies reported a direct association between HL and specificdomains of diabetes self-management (recording glucose levels,treatment adherence, adjustment of insulin dose, and carbohydrateintake). Eight studies found no direct significant associationbetween HL and self-management. In contrast to what is generallyexpected, current research cannot confirm that low HL is associatedwith inadequate diabetes self-management. This is in line with thenon-consistent data on the impact of HL on glycaemic control thathave been reported over the years [9,12,19,23,25,29,30].
Furthermore, limited evidence was found for the hypothesisthat HL influences self-management via motivational and voli-tional determinants as described in von Wagner’s framework. As inother studies, significant associations were found between HL andknowledge (n = 6), self-efficacy (n = 1) and social support (n = 1)[14,31–34]. However, only three studies evaluated the effect ofthese sociocognitive variables on diabetes self-management. Twoof them found that sociocognitive determinants (knowledge andself-efficacy) influenced self-management, but found no associa-tion between HL and these determinants. Only one study foundproof for a mediating variable (social support) in the pathwaybetween HL and self-management. The very limited evidence onthe mediating role of sociocognitive variables may be attributed tothe fact that most studies did not test for causal relations betweenall variables in the pathway between HL and self-management, ascan be done by structural equation modelling. Only Osborn et al.applied this latter technique and found that social support had amediating effect in the pathway between HL and diabetes self-management [25].
4.1.2. Gaps in research on health literacy diabetes self-management
This review has identified several gaps in the research on HLand diabetes self-management. While it is generally assumed thatlow HL is associated with inadequate diabetes self-management,few studies actually investigated this association over the yearsand very few found significant associations in highly specific self-management domains. Only one study used diabetes specific HLmeasures, such as the Diabetes Numeracy Test [19]. Furthermore,the role of possible mediating variables in the pathway between HLand self-management has hardly been evaluated. Research so farhas focused on the association between HL and variables that may

M.P. Fransen et al. / Patient Education and Counseling 88 (2012) 44–5352
play a role in diabetes self-management (e.g. knowledge) and noton the possible mediating role of these variables in the relationshipbetween HL and self-management. Although several studies, forexample, demonstrated that inadequate HL is associated withinsufficient diabetes knowledge, the role of insufficient knowledgeon self-management among patients with low HL remains unclearand needs further investigation [14,31–34]. The same applies tovolitional determinants such as self-efficacy and social support.Although it is generally believed that adequate self-efficacyimproves diabetes self-management, the mediating role of self-efficacy in the pathway between HL and self-management hashardly been studied [35].
4.1.3. Strength and limitations
A limitation of the present review is that only PubMed was usedto search for studies on HL and diabetes self-management, andonly reports in English were included. However, a strength is thatwe are the first to perform a systematic literature search on theassociation between HL and diabetes self-management, andpossible mediating variables. Furthermore, we are the first toorder findings of a literature review in von Wagner’s framework forHL and health actions. The framework has been applied before astheoretical basis for research on the association between healthliteracy and self-efficacy for participation in colorectal cancerscreening and for research on the association between numeracyand quality of patient–provider communication [36,37]. It alsoformed part of a wider framework of health inequalities in cancerscreening [38]. Our study has implications for further research onthe pathway between HL and health actions as described in vonWagner’s framework and stimulates research on the impact of HLon diabetes self-management.
4.2. Conclusion
To date few empirical studies have investigated the associationbetween HL and diabetes self-management. There is only limitedevidence that low HL is associated with inadequate diabetes self-management. This evidence accounts for very specific self-management domains. The evidence for the hypothesis that HLinfluences self-management via possible mediating sociocognitivevariables (e.g. motivational and volitional determinants) is alsoweak.
4.3. Implications
More studies are needed to substantiate the associationbetween HL and diabetes self-management and to identify towhat extent mediating variables play a role in the possiblepathway between HL and diabetes self-management. Prospectivelongitudinal studies are needed to investigate possible causalrelationships between HL, mediating variables and health actions,such as self-management. The size of the research population inthese studies should be sufficient to statistically test and estimatecausal relations (e.g. structural equation modelling). This isnecessary to investigate how HL is related to possible mediatingvariables and to what extent these variables are related to diabetesself-management and, in turn, glycaemic control. Furthermore,standardized valid and diabetes specific measures are needed toassess HL and self-management in low health literate populations.The validity of self-reported measures of HL and self-managementneed to be tested among subjects with low HL. Since currentobjective HL measures only evaluate the ability to read, calculateand understand, new HL measures are needed that also measurethe skills to obtain and use information to make appropriate healthdecisions. Such developments in research on HL and diabetes self-management are essential to understand the impact of HL on
health behaviour, and health outcomes and will eventually enableevidence-based development of interventions to increase ade-quate and sustainable self-management in diabetic patients withlow HL.
Conflicts of interest
The authors have no conflicts of interest to declare.
Acknowledgements
The authors thank Petra Jellema for her constructive commentson this review.
References
[1] Barlow J, Wright C, Sheasby J, Turner A, Hainsworth J. Self-managementapproaches for people with chronic conditions: a review. Patient Educ Couns2002;48:177–87.
[2] Stetson B, Schlundt D, Peyrot M, Ciechanowski P, Austin MM, Young-Hyman D,et al. Monitoring in diabetes self-management: issues and recommendationsfor improvement. Popul Health Manag 2011;14:189–97.
[3] Toobert DJ, Hampson SE, Glasgow RE. The summary of diabetes self-careactivities measure: results from 7 studies and a revised scale. Diabetes Care2000;23:943–50.
[4] Weinger K, Butler HA, Welch GW, La Greca AM. Measuring diabetes self-care: apsychometric analysis of the self-care inventory-revised with adults. DiabetesCare 2005;28:1346–52.
[5] American Association of Diabetes Educators. Diabetes education. http://www.diabeteseducator.org/DiabetesEducation [accessed 05.07.11].
[6] Ratzan SC, Parker RM. Introduction. In: Selden CRZ, editor. National library ofmedicine current bibliographies in medicine: health literacy. Bethesda, MD:National Institutes of Health, U.S. Department of Health and Human Services;2000. Pub. No. CBM 2000-1.
[7] DeWalt DA, Berkman ND, Sheridan S, Lohr KN, Pignone MP. Literacy and healthoutcomes: a systematic review of the literature. J Gen Intern Med2004;19:1228–39.
[8] DeWalt DA, Hink A. Health literacy and child health outcomes: a systematicreview of the literature. Pediatrics 2009;124(Suppl 3):S265–74.
[9] Rothman R, Malone R, Bryant B, Dewalt D, Pignone M. Health literacy anddiabetic control. J Amer Med Assoc 2002;288:2687–8.
[10] Rothman R, Malone R, Bryant B, Horlen C, Dewalt D, Pignone M. The relation-ship between literacy and glycemic control in a diabetes disease-managementprogram. Diabetes Educ 2004;30:263–73.
[11] Rothman RL, DeWalt DA, Malone R, Bryant B, Shintani A, Crigler B, et al.Influence of patient literacy on the effectiveness of a primary care-baseddiabetes disease management program. J Amer Med Assoc 2004;292:1711–6.
[12] Schillinger D, Grumbach K, Piette J, Wang F, Osmond D, Daher C, et al.Association of health literacy with diabetes outcomes. J Amer Med Assoc2002;288:475–82.
[13] DeWalt DA, Malone RM, Bryant ME, Kosnar MC, Corr KE, Rothman RL, et al. Aheart failure self-management program for patients of all literacy levels: arandomized, controlled trial [ISRCTN11535170]. BMC Health Serv Res2006;6:30.
[14] Gazmararian JA, Williams MV, Peel J, Baker DW. Health literacy and knowledgeof chronic disease. Patient Educ Couns 2003;51:267–75.
[15] Paasche-Orlow MK, Wolf MS. The causal pathways linking health literacy tohealth outcomes. Am J Health Behav 2007;31(Suppl 1):S19–26.
[16] Von Wagner C, Steptoe A, Wolf MS, Wardle J. Health literacy and healthactions: a review and a framework from health psychology. Health Educ Behav2009;36:860–77.
[17] Dutch Cochrane Centre. Guidelines to assess the quality of cohort designs [InDutch: Beoordelen van een cohortonderzoek]. http://dcc.cochrane.org/dutch-cochrane-centre [accessed 21.06.11].
[18] Bains SS, Egede LE. Associations between health literacy, diabetes knowledge,self-care behaviors, and glycemic control in a low income population withtype 2 diabetes. Diabetes Technol Ther 2011;13:335–41.
[19] Cavanaugh K, Huizinga MM, Wallston KA, Gebretsadik T, Shintani A, Davis D,et al. Association of numeracy and diabetes control. Ann Intern Med2008;148:737–46.
[20] Hawthorne K, Tomlinson S. Pakistani moslems with Type 2 diabetes mellitus:effect of sex, literacy skills, known diabetic complications and place of care ondiabetic knowledge, reported self-monitoring management and glycaemiccontrol. Diabet Med 1999;16:591–7.
[21] Karter AJ, Subramanian U, Saha C, Crosson JC, Parker MM, Swain BE, et al.Barriers to insulin initiation: the translating research into action for diabetesinsulin starts project. Diabetes Care 2010;33:733–5.
[22] Kim S, Love F, Quistberg DA, Shea JA. Association of health literacy with self-management behavior in patients with diabetes. Diabetes Care 2004;27:2980–2.

M.P. Fransen et al. / Patient Education and Counseling 88 (2012) 44–53 53
[23] Mancuso JM. Impact of health literacy and patient trust on glycemic control inan urban USA population. Nurs Health Sci 2010;12:94–104.
[24] Mbaezue N, Mayberry R, Gazmararian J, Quarshie A, Ivonye C, Heisler M. Theimpact of health literacy on self-monitoring of blood glucose in patients withdiabetes receiving care in an inner-city hospital. J Natl Med Assoc2010;102:5–9.
[25] Osborn CY, Bains SS, Egede LE. Health literacy, diabetes self-care, and glycemiccontrol in adults with type 2 diabetes. Diabetes Technol Ther 2010.
[26] Powell CK, Hill EG, Clancy DE. The relationship between health literacy anddiabetes knowledge and readiness to take health actions. Diabetes Educ2007;33:144–51.
[27] Sarkar U, Fisher L, Schillinger D. Is self-efficacy associated with diabetes self-management across race/ethnicity and health literacy? Diabetes Care2006;29:823–9.
[28] Wallace AS, Seligman HK, Davis TC, Schillinger D, Arnold CL, Bryant-Shilli-day B, et al. Literacy-appropriate educational materials and brief counsel-ing improve diabetes self-management. Patient Educ Couns 2009;75:328–33.
[29] Williams MV, Baker DW, Parker RM, Nurss JR. Relationship of functional healthliteracy to patients’ knowledge of their chronic disease. A study of patientswith hypertension and diabetes. Arch Intern Med 1998;158:166–72.
[30] Tang YH, Pang SM, Chan MF, Yeung GS, Yeung VT. Health literacy, complicationawareness, and diabetic control in patients with type 2 diabetes mellitus. J AdvNurs 2008;62:74–83.
[31] Al-Adsani AM, Moussa MA, Al-Jasem LI, Abdella NA, Al-Hamad NM. The leveland determinants of diabetes knowledge in Kuwaiti adults with type 2diabetes. Diabetes Metab 2009;35:121–8.
[32] DeWalt DA, Boone RS, Pignone MP. Literacy and its relationship with self-efficacy, trust, and participation in medical decision making. Amer J HealthBehav 2007;31(Suppl 1):S27–35.
[33] Kandula NR, Nsiah-Kumi PA, Makoul G, Sager J, Zei CP, Glass S, et al. Therelationship between health literacy and knowledge improvement after a multi-media type 2 diabetes education program. Patient Educ Couns 2009;75:321–7.
[34] Rothman RL, Malone R, Bryant B, Wolfe C, Padgett P, DeWalt DA, et al. Thespoken knowledge in low literacy in diabetes scale: a diabetes knowledgescale for vulnerable patients. Diabetes Educ 2005;31:215–24.
[35] Sigurdardottir AK. Self-care in diabetes: model of factors affecting self-care. JClin Nurs 2005;14:301–14.
[36] Von Wagner C, Semmler C, Good A, Wardle J. Health literacy and self-efficacyfor participating in colorectal cancer screening: the role of information pro-cessing. Patient Educ Couns 2009;75:352–7.
[37] Smith SG, Wolf MS, von Wagner C. Socioeconomic status, statistical confidence,and patient-provider communication: an analysis of the Health InformationNational Trends Survey (HINTS 2007). J Health Commun 2010;15(Suppl3):169–85.
[38] Von Wagner C, Good A, Whitaker KL, Wardle J. Psychosocial determinants ofsocioeconomic inequalities in cancer screening participation: a conceptualframework. Epidemiol Rev 2011;33:135–47.